Choanal Atresia
40
Choanal Atresia Choanal Atresia Essie Fine Essie Fine May 31, 2007 May 31, 2007
Transcript of Choanal Atresia

Choanal AtresiaChoanal Atresia
Essie FineEssie Fine
May 31, 2007May 31, 2007

Case PresentationCase Presentation
You are asked to see a neonate born at 36 You are asked to see a neonate born at 36 weeks for intermittent cyanosis.weeks for intermittent cyanosis.
Birth history: born to G4P3 mother, by c-Birth history: born to G4P3 mother, by c-section for placenta previa. Apgars are 8, section for placenta previa. Apgars are 8, 9. The neonate then desaturates at 7 9. The neonate then desaturates at 7 minutes of life. She is bag ventilated and minutes of life. She is bag ventilated and recovers. recovers.
History: No birth defects in family. History: No birth defects in family. Uneventful pregnancy. No exposures. Uneventful pregnancy. No exposures.

ExamExam
Mouth breathing, retracting slightly at neckMouth breathing, retracting slightly at neck Shortened palpebral fissures with no visible globeShortened palpebral fissures with no visible globe Left cleft nareLeft cleft nare AnkyloglossusAnkyloglossus Low set earsLow set ears Normal fingersNormal fingers RRR no murmursRRR no murmurs Abdomen soft, no organomegalyAbdomen soft, no organomegaly Cannot pass catheter or FFO scope either nareCannot pass catheter or FFO scope either nare

Nasopharyngeal obstruction Nasopharyngeal obstruction DDxDDx
Vascular - hemangiomaVascular - hemangioma Infectious - ChlamydiaInfectious - Chlamydia Traumatic- septal hematoma, dislocated nasal septumTraumatic- septal hematoma, dislocated nasal septum Autoimmune – sarcoid, RA, churg-straussAutoimmune – sarcoid, RA, churg-strauss Metabolic – cystic fibrosisMetabolic – cystic fibrosis Iatrogenic/idiopathic – septal hematoma, dislocated nasal septum, Iatrogenic/idiopathic – septal hematoma, dislocated nasal septum,
kartagenerskartageners Neoplasia – hamartoma, nasopharyngeal mass hairy polyp, Neoplasia – hamartoma, nasopharyngeal mass hairy polyp,
teratoma, chordoma, rhabdomyosarcoma, angiofibroma, teratoma, chordoma, rhabdomyosarcoma, angiofibroma, hemangiopericytoma, scchemangiopericytoma, scc
Congenital - Choanal stenosis/atresia, Piriform aperture stenosis, Congenital - Choanal stenosis/atresia, Piriform aperture stenosis, Nasal glioma, Encephalocele, Meningocele, dermoid, Micrognathia, Nasal glioma, Encephalocele, Meningocele, dermoid, Micrognathia, Macroglossia, Treacher collins, Down’s syndrome, Cystic Hygroma, Macroglossia, Treacher collins, Down’s syndrome, Cystic Hygroma, Lingual thyroid, incisive canal cysts, nasolacrimal duct cyst, Lingual thyroid, incisive canal cysts, nasolacrimal duct cyst, dentigerous cystsdentigerous cysts

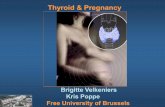
Nasal endoscopyNasal endoscopy
Right Left

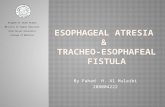
CT scanCT scan
Her scan
Different Pathology

CT scan evaluationCT scan evaluation
Choanal airspace measurement: Choanal airspace measurement: mean normal is 0.67cm. Mixed mean normal is 0.67cm. Mixed atresia is 1/3 of normal, bony atresia atresia is 1/3 of normal, bony atresia measures 0.measures 0.
Vomer width – Mean 0.23cm, bony Vomer width – Mean 0.23cm, bony atresia mean 0.6cm, membranous atresia mean 0.6cm, membranous atresia 0.3 cm. atresia 0.3 cm.
Slovis TL et al. Choanal Atresia: Precise CT Evaluation. Radiology. 1985;155:345-348.

EpidemiologyEpidemiology
1:5000-1:8000 live births1:5000-1:8000 live births 50% with other anomalies50% with other anomalies 65-75% unilateral. 75% of bilateral cases have 65-75% unilateral. 75% of bilateral cases have
other anomalies.other anomalies. Polydactyly, nasal-auricular and palatal Polydactyly, nasal-auricular and palatal
deformities, crouzon’s, craniosynostosis, deformities, crouzon’s, craniosynostosis, microencephaly, meningocele, microencephaly, meningocele, meningoencephalocele, facial asymmetry, meningoencephalocele, facial asymmetry, hypoplasia of orbit and midface, hypertelorism, hypoplasia of orbit and midface, hypertelorism, cleft palatecleft palate
29% bony, 71% mixed (brown et al)29% bony, 71% mixed (brown et al)

Typical presentationTypical presentation
Bilateral – cyclic cyanosis relieved by Bilateral – cyclic cyanosis relieved by cryingcrying
Unilateral – chronic nasal obstruction, Unilateral – chronic nasal obstruction, thick tenatious mucousthick tenatious mucous

anatomyanatomy
Bounderies of the atresia Bounderies of the atresia plate:plate:
Superior: sphenoidSuperior: sphenoid Lateral: medial Lateral: medial
pterygoid lamina pterygoid lamina Medial: vomerMedial: vomer Inferior: horizontal Inferior: horizontal
portion of the palatal portion of the palatal bone bone

AnatomyAnatomy
Narrow nasal cavity lateral Narrow nasal cavity lateral obstruction by lat pterygoid obstruction by lat pterygoid plate, Vomer thickening, plate, Vomer thickening, membranous obstructionmembranous obstruction
Medial pterygoid plate and Medial pterygoid plate and posterior vomer are posterior vomer are expanded by endochondral expanded by endochondral bone formation and bone formation and fibroepithelial membrane fibroepithelial membrane that obstructs the choanaethat obstructs the choanae

Further work upFurther work up
As always, AIRWAY firstAs always, AIRWAY first Genetics evaluationGenetics evaluation Cardiology (EKG, Echo)Cardiology (EKG, Echo) Opthalmology evaluationOpthalmology evaluation HearingHearing UA (kidney)UA (kidney)

ManagementManagement
Unilateral delayed to allow Unilateral delayed to allow the patient to grow, and the patient to grow, and reduce risk of restenosisreduce risk of restenosis
Bilateral – creating oral Bilateral – creating oral airway- Mcgovern nipple with airway- Mcgovern nipple with enlarged hole or two side enlarged hole or two side holes, surgical correction vs holes, surgical correction vs tracheostomytracheostomy
Stimulate infant to cry, Stimulate infant to cry, intubate, bag ventilate if intubate, bag ventilate if obstructing in an emergencyobstructing in an emergency
Genetics consult, work up for Genetics consult, work up for other anomaliesother anomalies

Surgical ApproachesSurgical Approaches
TransnasalTransnasal TranspalatalTranspalatal TransseptalTransseptal

Transnasal/transseptalTransnasal/transseptal
Most common repair strategy now Most common repair strategy now that endoscopes are usedthat endoscopes are used
Multiple techniques – all use either Multiple techniques – all use either mucosal flaps or stenting to prevent mucosal flaps or stenting to prevent restenosisrestenosis

TransnasalTransnasal

Transnasal pros/consTransnasal pros/cons
Punching through the atretic plate is Punching through the atretic plate is essentially blind process – important to go essentially blind process – important to go inferomedial to avoid sphenopalatine artery, inferomedial to avoid sphenopalatine artery, and drill parallel to palate to avoid entering and drill parallel to palate to avoid entering clivus, sphenoidclivus, sphenoid
Risks include all those of FESS, but anatomy is Risks include all those of FESS, but anatomy is abnormal and less predictableabnormal and less predictable
Does not impair development of dental archesDoes not impair development of dental arches Uses equipment/techniques similar to FESSUses equipment/techniques similar to FESS

Transnasal/transseptalTransnasal/transseptal
Cedin AC, Fujita R, Cruz OL: Endoscopic transeptal surgery for choanal atresia with a stentless folded-over-flap technique. Otolaryngol Head Neck Surg 2006 Nov; 135(5): 693-8

TranspalatalTranspalatal
Tewfik et al., 2007
•Include greater palatine for blood supply to Include greater palatine for blood supply to flapflap•Subperiosteal elevation to leading edge of hard palate•Cutting burr used to drill the posterior vomer and atretic plate.•Stents placed•Incision made 5 mm from dental archIncision made 5 mm from dental arch

Transpalatal drawbackTranspalatal drawback
52% incidence of dental malocclusion resulting from narrowed maxillary dental arches in patients younger than 5 years
Palatal flap necrosis Palatal fistula Persistent submucous tunnel Restenosis Upside: success rate of over 80% is
comparable to all other approaches

SyndromesSyndromes
CHARGECHARGE Treacher CollinsTreacher Collins Crouzon’sCrouzon’s

CHARGE syndromeCHARGE syndrome
Coloboma and/or CNS abnormalitiesColoboma and/or CNS abnormalities Heart abnormalityHeart abnormality Atresia choanaeAtresia choanae Retardation of growthRetardation of growth Genital defects (males)Genital defects (males) Ear anomalies/deafnessEar anomalies/deafness
Mutations on the CHD7 gene (located on Chromosome 8) Mutations on the CHD7 gene (located on Chromosome 8) were found in 10 of 17 patients in a study conducted in the were found in 10 of 17 patients in a study conducted in the Netherlands (Vissers, et al., 2004). Netherlands (Vissers, et al., 2004).
A study in the US of 110 individuals with CHARGE syndrome A study in the US of 110 individuals with CHARGE syndrome showed that 60% of those tested had a mutation on the showed that 60% of those tested had a mutation on the CHD7 gene (Lalani et al., 2006). CHD7 gene (Lalani et al., 2006).

CHARGECHARGE
The percentages of the different The percentages of the different anomalies in CHARGE association are as anomalies in CHARGE association are as follows: follows:
Coloboma - 80% Coloboma - 80% Heart defect - 58% Heart defect - 58% Atresia of choanae - 100% Atresia of choanae - 100% Mental retardation - 94% Mental retardation - 94% Growth deficiency - 87% Growth deficiency - 87% Genital hypoplasia in males - 75% Genital hypoplasia in males - 75% Ear anomalies - 88%Ear anomalies - 88%

CHARGECHARGE
Other features: kidney anomalies, Other features: kidney anomalies, OCDOCD Palmar crease, esophageal Palmar crease, esophageal atresia, tracheoesophageal fistula, atresia, tracheoesophageal fistula, scoliosis, chronic middle ear scoliosis, chronic middle ear problems, cleftsproblems, clefts

Treacher CollinsTreacher Collins
Malar hypoplasiaMalar hypoplasia ColobomasColobomas Medial 2/3 lash without lashesMedial 2/3 lash without lashes Retrusive chinRetrusive chin Class 2 malocclusionClass 2 malocclusion External ear anomaliesExternal ear anomalies SNHLSNHL Rarely choanal atresiaRarely choanal atresia


Which of the following are true Which of the following are true of Treacher collins syndromeof Treacher collins syndrome
A. Autosomal RecessiveA. Autosomal Recessive B. Mutation in the TCOF gene, coding B. Mutation in the TCOF gene, coding
treacletreacle C. Abnormal third branchial arch C. Abnormal third branchial arch
developmentdevelopment D. External ear anomolies are present but D. External ear anomolies are present but
there is no hearing lossthere is no hearing loss E. Surgical correction typically at 7 years E. Surgical correction typically at 7 years
of age. of age.

EmbryogenesisEmbryogenesis
Nasal placodes invaginate to form Nasal placodes invaginate to form nasal pits 3-4 weeks of nasal pits 3-4 weeks of gestationgestation
These enlarge and burrow into These enlarge and burrow into underlying mesoderm, forming underlying mesoderm, forming nasal pouchesnasal pouches
Floor between nasal and buccal Floor between nasal and buccal cavity thins to form nasobuccal cavity thins to form nasobuccal membranemembrane
Membrane ruptures at 6 weeks Membrane ruptures at 6 weeks gestationgestation
Choanal atresia – cause unknown, Choanal atresia – cause unknown, thought to be due either to thought to be due either to persistence of nasobuccal persistence of nasobuccal membrane, buccopharngeal membrane, buccopharngeal membrane, or due to errors in membrane, or due to errors in mesoderm migrationmesoderm migration






EpidemiologyEpidemiology
1:5000-1:8000 live births1:5000-1:8000 live births 50% with other anomalies50% with other anomalies 65-75% unilateral. 75% of bilateral cases 65-75% unilateral. 75% of bilateral cases
have other anomalieshave other anomalies Polydactyly, nasal-auricular and palatal Polydactyly, nasal-auricular and palatal
deformities, crouzon’s, craniosynostosis, deformities, crouzon’s, craniosynostosis, microencephaly, meningocele, microencephaly, meningocele, meningoencephalocele, facial asymmetry, meningoencephalocele, facial asymmetry, hypoplasia of orbt and midface, hypoplasia of orbt and midface, hypertelorism, cleft palatehypertelorism, cleft palate



EmbryogenesisEmbryogenesis


Hemifacial microsomiaHemifacial microsomia
OrbitOrbit MandibleMandible EarEar Facial nerveFacial nerve Soft tissueSoft tissue Defect of first and second branchial Defect of first and second branchial
arches - ? Vascular insult arches - ? Vascular insult

Treacher CollinsTreacher Collins
Malar hypoplasiaMalar hypoplasia ColobomasColobomas Medial 2/3 lash without lashesMedial 2/3 lash without lashes Retrusive chinRetrusive chin Class 2 malocclusionClass 2 malocclusion External ear anomaliesExternal ear anomalies SNHLSNHL
![Syndromic choanal atresia: The example of CHARGE Syndrome · CHARGE syndrome is a rare but serious genetic disease [1]. The real incidence of this syndrome is not known;with estimates](https://static.fdocuments.us/doc/165x107/5eded24fad6a402d666a2c8a/syndromic-choanal-atresia-the-example-of-charge-syndrome-charge-syndrome-is-a-rare.jpg)




![THREE NOVEL MUTATIONS OF CHD7 GENE IN TWO TURKISH … · syndrome [16]. Choanal atresia or stenosis is found in approximately half of the patients and noticed due to respiratory difficulty](https://static.fdocuments.us/doc/165x107/5f0d1c4d7e708231d438bad3/three-novel-mutations-of-chd7-gene-in-two-turkish-syndrome-16-choanal-atresia.jpg)