07 Sewell GI Part 1
30
UCSF, Department of Medicine, CME 1 1 GASTROENTEROLOGY Justin L. Sewell, MD, MPH, FACP Assistant Professor of Medicine Division of Gastroenterology UC San Francisco | Zuckerberg SanFrancisco General Disclosures l No relationships or conflicts of interest to disclose 2 Agenda l Case-based overview of GI content most pertinent to IM boards l Additional boards-relevant information with guideline references l Pause for questions after each session but ask anytime 3 Highest yield GI topics for IM Boards (GI content 9-10%) l Esophagus: GERD, Barrett’s, varices, (cancer, motility) l Stomach/duodenum: H pylori, PUD, non-ulcer dyspepsia, GI bleeding, gastritis, (gastric cancer) l Small intestine: Crohn’s disease, gastroenteritis, (celiac, ischemic bowel diseases) l Colorectal: colon cancer, diverticular disease, ulcerative colitis, IBS, antibiotic colitis, appendicitis, hemorrhoids, (constipation, incontinence, polyposis syndromes) l Pancreas: acute pancreatitis, (pancreatic cancer, chronic pancreatitis) l Liver and biliary: separate session 4
Transcript of 07 Sewell GI Part 1

UCSF, Department of Medicine, CME
1
1
GASTROENTEROLOGY
Justin L.Sewell, MD,MPH,FACPAssistantProfessorofMedicineDivisionofGastroenterologyUCSanFrancisco|ZuckerbergSanFranciscoGeneral
Disclosures
l Norelationships orconflicts ofinterest todisclose
2
Agenda
l Case-based overviewofGIcontent mostpertinent to IMboards
l Additional boards-relevant informationwith guideline references
l Pauseforquestions aftereachsession butaskanytime
3
Highest yieldGItopics forIMBoards (GIcontent9-10%)l Esophagus:GERD,Barrett’s,varices,(cancer,motility)l Stomach/duodenum: Hpylori,PUD,non-ulcer
dyspepsia,GIbleeding,gastritis,(gastriccancer)l Smallintestine:Crohn’sdisease,gastroenteritis,(celiac,
ischemic boweldiseases)l Colorectal:colon cancer,diverticulardisease,ulcerative
colitis,IBS,antibioticcolitis,appendicitis,hemorrhoids,(constipation, incontinence,polyposis syndromes)
l Pancreas:acutepancreatitis,(pancreaticcancer,chronic pancreatitis)
l Liverandbiliary:separatesession
4

UCSF, Department of Medicine, CME
2
Case #1l 42 year old Caucasian man withheartburnl Intermittent retrosternal burning ~2yearsl Increasing use of antacids & OTC H2RAs, with only transient
relief of symptomsl 1-2 packs cigarettesQD, 1-2 glasseswine QHSl Regurgitation of sour material at night, but no dysphagial Elevates head of bed and has lost weight without benefit
Case #1– What isthemostappropriatenextstepinmanagement?
1. Perform upper endoscopy2. Trialofhigh-dose PPIfor4-6weeks3. Stopallcaffeine andalcohol4. Esophageal pHtesting5. TakeH2RAscheduled rather than prn
6
Case #1– What isthemostappropriatenextstepinmanagement?
1. Perform upper endoscopy2. Trialofhigh-dose PPIfor4-6weeks3. Stopallcaffeine andalcohol4. Esophageal pHtesting5. TakeH2RAscheduled rather than prn
7
Indications for endoscopy inGERD
Menandwomenwith:l Alarmsymptomsl GERDrefractorytoPPIl Severeerosiveesophagitisl Recurrentdysphagiawith
historyofstricturel KnownBarrett’sesophagus
Menonlywith:l GERD>5yearsAND
additionalriskfactorsforesophagealcancer(singlescreeningEGD)l Nocturnal reflux
l Obesityl Central adiposityl Smokingl Hiatal hernia
8Shaheen NJ.Ann Intern Med 2012; 157(11):808-16.

UCSF, Department of Medicine, CME
3
9
Case #1
l Symptoms partially improved on PPIà EGDl EGD: 2 cm tong ue of salmon colored mucosa in the distal
esophagus, otherwise unremarkablel Biopsies: intestinal metaplasia with no dysplasia
10
Case#1– Which isthe most appropriatenextstep?
1. Repeat EGD for surveillancewithin 1 year
2. Test for H. pylori infection and treat if present
3. Radiofrequency ablation of the Barrett’s mucosa
4. Refer to surgeon for anti-reflux surgery
5. Double the dose of his PPI to BID and followsymptomatically
11
1. Repeat EGD for surveillancewithin 1 year
2. Test for H. pylori infection and treat if present
3. Radiofrequency ablation of the Barrett’s mucosa
4. Refer to surgeon for anti-reflux surgery
5. Double the dose of his PPI to BID and followsymptomatically
Case#1– Which isthe most appropriatenextstep? Case #1– Barrett’s surveillance
l Riskofprogressiontocancerislow(<1%peryear)
l Nodysplasia:EGDevery3-5yearsl Lowgradedysplasia:repeat6months,thenannually
l Highgradedysplasia:confirmby2nd pathologistà ablationoresophagectomyduetoconcomitantadenocarcinomain30-40%
12ASGE Standards of Practice Committee. Gastrointest Endosc 2012;76(6):1087-94.

UCSF, Department of Medicine, CME
4
1 3
Case #1– Barrett’smanagement
l Medical orsurgical anti-reflux therapiesdo notcauseregression of Barrett’s; goalistocontrol symptoms andminimize cancer risk
l Radiofrequency ablation (RFA) eradicates80-95% ofdysplasia andreduces lifetimecancer riskfrom 9%to1%
l Anti-reflux surgeryreservedfor failures ofoptimalmedical therapyor patientpreference
14
Case #1
l Eradicate Hpylori whendiagnosedl Reduces riskof PUD,gastriccancer
l However thisdoesnotaffect progression ofBarrett’s andcouldtheoretically worsen GERD
15
GERD
l Cardiac versusGERD-induced chest paincan bedifficulttodifferentiatel PPItriall Cardiactestinginhigher-riskpatients
l GERDcancauseglobusanddysphagiaàPPItriall Functionalheartburnandnonerosiverefluxdiseaseare
commonandarelessresponsivetoacidsuppressionl Esophageal pHmonitoring required todiagnose
l PPIshouldbetaken30-60minutesbeforeeatingforoptimalacidsuppression
16
GERD
l GERD can beexacerbated byl Impairedsalivaryflow(Sjögrens,XRT)l Esophagealdysmotility(scleroderma)l Gastricdistension(gastroparesis,dietaryhabits)l ReducedLESpressure(chocolate,alcohol,nicotine,CCBs,nitrates,antidepressants,progesterone, benzodiazepines)
l Atypical(extraesophageal) GERDmanifestationsinclude: chronic cough, hoarseness, laryngitis,asthma

UCSF, Department of Medicine, CME
5
1 7
Dysphagia
l Dysphagia:sourcesuggestedbysymptomsl Intermittent solid: Schatzki ring, eosinophilic esophagitisl Progressive solid: stricture/achalasia (slow) orneoplasm (rapid)l Solid and liquid: dysmotility
l EGDusuallyfirsttestthoughcanconsideresophagraml Manometry testing ifEGDnondiagnostic
18
Dysphagia
l Dysphagia:sourcesuggestedbysymptomsl Intermittent solid: Schatzki ring, eosinophilic esophagitisl Progressive solid: stricture/achalasia (slow) orneoplasm (rapid)l Solid and liquid: dysmotility
l EGDusuallyfirsttestthoughcanconsideresophagraml Manometry testing ifEGDnondiagnostic
l Achalasia:lackofperistalsisandnon-relaxingLESl Oropharyngeal dysphagiausuallyduetoneuromuscular
disorders,andisassociatedw/coughing,nasalregurgitation,choking
19
Eosinophilic esophagitis
l Eosinophilic esophagitisl Intermittent solidfooddysphagiaorfoodimpaction,M>F
l Ringedor“feline”esophagusl Eosinophilicinfiltrateonbiopsyl Treatwitheliminationdiet,swallowed inhaledsteroids,PPIs
Dellon ES.Gastroenterology 2014; 147(6):1238-54. 2 0
Case #2
l 62y/owomanwith4monthsofepigastricabdominalpain,worsepost-prandially
l IncompletelyrelievedbyOTCH2RAsl Occasionalnauseabutnovomitingl Mildanorexial 5poundweightlossl ASA81mg/dandPRNibuprofenforarthritisl PEx:mildepigastricTTP,otherwiseunremarkable

UCSF, Department of Medicine, CME
6
2 1
Case#2Whichofthefollowingisthebestapproachatthistime?1. EmpiricHpyloritreatment
2. Hpylori testingandtreatmentifpositive
3. EmpiricprotonpumpinhibitorRx
4. Upperendoscopy
5. SwitchibuprofentoaCOX-2NSAID
22
Case#2Whichofthefollowingisthebestapproachatthistime?1. EmpiricHpyloritreatment
2. Hpylori testingandtreatmentifpositive
3. EmpiricprotonpumpinhibitorRx
4. Upperendoscopy
5. SwitchibuprofentoaCOX-2NSAID
Non-invasive H.pylori testing
H.pylori negative
Chronicdyspepsia
H.pylori positive
Eradication therapy Empiric treatment:Protonpumpinhibitor
Endoscopy
Improvement ImprovementNo improvement
YES
NO
Alarmsigns or symptomsAge>55
2 4
Case #2– Hpylori testing
l Rarely treat empiricallyl Active infection: urea breath test, stoolantigen,endoscopicbiopsy
l Active/prior infection: serology

UCSF, Department of Medicine, CME
7
2 5
Case #2– EmpiricPPI
l Empiricacid-suppressionhassomeefficacyindyspepsia,andisreasonableinyoungpatientswithnoalarmsymptoms
l COX-2selectiveNSAIDshaveless GItoxicityl Newdyspepsiainpatientsoverage50,dyspepsiawithalarmsymptomsorfamilyhistoryofgastriccancer,shouldhaveEGDtoruleoutcancer
26
Hpylori
l Usuallyacquiredinchildhood,persontopersontransmissionl Inverseassociationwithsocioeconomicstatusl Oftenasymptomatic
l 10-20% PUDl <0.01%gastric CA
l Treatment:l Triple: PPI, clarithromycin, amoxicillin x10-14 daysl Quadruple: PPI,bismuth, metronidazole, tetracycline x10-14daysl Other antibiotic options include levofloxacin, rifabutin, nitazoxanide
27
Pepticulcerdisease
l GUsrequirebiopsy&repeatEGDtoexcludeCAl Multiplenon-healingulcers,orulcersw/diarrhea:suspectZES.Bestinitialtest:fastingserumgastrin
l Elevatedgastrinseeningastricoutletobstruction,PPIuse,perniciousanemia,renal insufficiency,diabetes,andgastrinoma
l Gastrinlevels>1000highlysuspiciousforZES;200-1000bestevaluatedwithsecretinstimulationtest(paradoxicalriseingastrinaftersecretinadministered)
Non-ulcer dyspepsia
l Alsocalled functional dyspepsial Symptomswithout source identifiedl TCA’sor SSRI’scanbeeffective
28

UCSF, Department of Medicine, CME
8
2 9
UGI bleed
l HighriskGIBpatientstakingNSAIDS:l KnownPUD,advancedage,warfarinl TestandtreatforHpyloril Co-prescribePPI
l Stress,caffeine,prednisonedonotcausePUD
30
UGI bleed
l UGIBmaypresent ashematochezia ifbrisk,andconversely, slow right-sided colonic bleedingmaycausemelena
l NGtube only85%sensitive inUGIBl MostUGIBwill stop spontaneouslyl MostUGIBcanbeeffectively managedbyEGDorangiography
l Surgeryindicated ifpersistent orrecurrentexsanguination
Common causes of upperGIbleeding
PUD(50%)
Mallory-Weiss tear (10%)
Varices/portalhypertension(20%)
Erosive gastritis (10%)32
UGI bleed
l Mortality risk~10%l Increasedwithadvanceage, shock,hematochezia,cirrhosis
l EGD:diagnostic, therapeutic, prognosticl IRandsurgery arebackupl Medicaltherapy with PPIbolus +continuousinfusion; octreotide ifportal HTN
l Norole forH2RA’s

UCSF, Department of Medicine, CME
9
3 3
Case #3
l 47y/omaleexecutiveadmittedwithsevereabdominalpainradiatingtohisback
l Drinks2-3cocktailsperday,occasionallymorel PExnotableformid-abdominaltendernesswithhypoactivebowelsounds
l Lipase9,200l Initialmanagement: NPO,analgesiaandhydration
Case #3
l Additional labs:lWBC11,000l Bili1.6,AST95,ALT32,AlkP120l Triglycerides220l Calcium8.5
34
Case#3What isthemost appropriate nextdiagnostic step?1. Ultrasound oftheabdomen2. Empiric antibiotics3. MRCP4. Surgical consultation5. Trend CBC andlivertests, follow exam
35
Case#3What isthemost appropriate nextdiagnostic step?1. Ultrasound oftheabdomen2. Empiric antibiotics3. MRCP4. Surgical consultation5. Trend CBC andlivertests, follow exam
36

UCSF, Department of Medicine, CME
10
3 7
Case #3
l U/S:normal GB andCBD, pancreas is“obscured byoverlying bowel gas”
l Antibiotics notrecommendedl Byhospital day#8,his lipasehasnormalized buthis abdominal pain isworsening slightly, andhehasdevelopednewfeversto101.8,with arisingWBC
Tenner S.Am JGastroenterol 2013; 108(9):1400-15. 3 8
Case#3Whichofthefollowingisthebestapproachatthistime?1. Initiate oral feeds, as lipase is normal
2. Empiric antibiotics
3. Epidural catheter and PCA
4. ERCP
5. CT scan of the pancreas
39
Case#3Whichofthefollowingisthebestapproachatthistime?1. Initiate oral feeds, as lipase is normal
2. Empiric antibiotics
3. Epidural catheter and PCA
4. ERCP
5. CT scan of the pancreas
40
Case #3– CT scanwith necrosis
Normalenhancement
Lackofenhancement

UCSF, Department of Medicine, CME
11
4 1
Case #3– Pancreatic necrosis
l Persistent symptoms withacutepancreatitis shouldraiseconcern for complications
l Pancreatic necrosis predicts poor outcomel Antibiotics not recommended unless highsuspicion
ordocumented infected necrosisl Carbapenems haveexcellent pancreatic penetrationl Ifpatient appears infected and haspancreatic
necrosis, consider FNAwithgramstain/culturel Infected necrosis (positive gramstain) predicts high
mortalityrateandrequires surgical debridement
Tenner S.Am JGastroenterol 2013; 108(9):1400-15.
Case #3– ERCP forpancreatitis
l ERCPifbiliarysourceforpancreatitissuspectedl ALTisfirsttorisefollowedbybilirubinandalkPl Biliarydilation(US,CT,MRCP)
l WaitforpancreatitistoimproveunlessobstructingCBDstoneonimagingorsuspectedcholangitis
42Tenner S.Am JGastroenterol 2013; 108(9):1400-15.
4 3
Case #3– Acutepancreatitismanagement
l Canassessprognosisw/RansonorAPACHEIIl Serialamylase/lipase levelsnotusefulinpredictingcourse
l ObtainCTifseverepancreatitisissuspected(organfailure,lackofimprovement,increasingpain,fever,WBC,hypotension)
l NecrosisonCThasworstprognosis
Tenner S.Am JGastroenterol 2013; 108(9):1400-15. 4 4
l Prophylacticantibioticsnotindicatedl Earlystudiesevaluatedagentswithpoorpancreaspenetrationandincludedpatientswithmilddisease
l Besttherapyisgoodsupportivecareandaggressivehydration(250-500mL/hour,bolusifhypovolemic)
Tenner S.Am JGastroenterol 2013; 108(9):1400-15.
Case #3– Acutepancreatitismanagement

UCSF, Department of Medicine, CME
12
4 5
Case #3– Whentofeed
l Patientscaneatwhenpain-freeandhungryl Liquiddietandlow-fatsoliddietareequivalentl Post-duodenalenteralfeedingmaybeappropriateinpatientswithacutepancreatitisbutdoesnot improveoutcomescomparedwithon-demandoralfeeding
Bakker OJ. NewEngl JMed 2014; 371(21):1983-93.Tenner S.Am JGastroenterol 2013; 108(9):1400-15.
4 6
Acutepancreatitis – etiologies
l Mostcommonetiologies:gallstonesandalcoholl Lesscommon:hypertriglyceridemia,post-ERCP,pregnancy,hypercalcemia,viral,hereditary,autoimmune
l Medications:Erythromycin,tetracycline,6-MP/AZA,sulfas,5-ASAs,NSAIDs,estrogens,thiazides
Chronicpancreatitis
l Exocrineandendocrinemanifestationsl Imaging:dilatedduct,calcificationsl Enzymesbetterforsteatorrhea thanpainl Forpaincanconsiderceliacplexusblock,surgicaloptions
l Cancausebiliaryobstructionl Pancreasdivisum:failureoffusionofdorsalandventralglands;foundin5%ofpopulation;maypredisposetochronicpancreatitis
47
Let’stakea detourinto…radiology
l Common abdominal x-raysyoumightseeonboards
48

UCSF, Department of Medicine, CME
13
What isthis?
1. Toxicmegacolon2. Smallbowel
obstruction3. Sigmoidvolvulus4. Perforatedviscus
49
What isthis?
1. Toxicmegacolon2. Smallbowel
obstruction3. Sigmoidvolvulus4. Perforatedviscus
50
What isthis?
1. Toxicmegacolon2. Smallbowel
obstruction3. Sigmoidvolvulus4. Perforatedviscus
51
What isthis?
1. Toxicmegacolon2. Smallbowel
obstruction3. Sigmoidvolvulus4. Perforatedviscus
52

UCSF, Department of Medicine, CME
14
What isthis?
1. Toxicmegacolon2. Smallbowel
obstruction3. Sigmoidvolvulus4. Perforatedviscus
53
What isthis?
1. Toxicmegacolon2. Smallbowel
obstruction3. Sigmoidvolvulus4. Perforatedviscus
54
What isthis?
1. Toxicmegacolon2. Smallbowel
obstruction3. Sigmoidvolvulus4. Perforatedviscus
55
What isthis?
1. Toxicmegacolon2. Smallbowel
obstruction3. Sigmoidvolvulus4. Perforatedviscus
56

UCSF, Department of Medicine, CME
15
5 7
Case #4
l 22y/omanc/o1yearofworsening bloating&gasl Frequentmalodorous,floating,greasystoolsl 20lbweightlossin6monthsl Deniesabdominalpain,buthasdecreasedfoodintakeasitprovokesdiarrhea
l Healsocomplainsofanitchyrashonhiskneesandelbows
58
Case #4
l Physicalexam:shortstature,mucosalpallor,angularcheilosis,scatteredpapulesandvesicleswithexcoriationoverthekneesandelbows,andmildpretibialedema
l Labtestsaresignificantformicrocyticanemiaandalowserumalbumin
59
GIrashesyouneed toknow…
DermatitisHerpetiformis E.nodosum Pyoderma
60
Case#4Whichofthefollowingisthemostlikelycauseofthispatient’ssyndromeandmalnutrition?
1. Whipple’s Disease
2. Crohn’s Disease
3. Celiac Disease
4. Pancreatic exocrine insufficiency
5. Smallbowelbacterialovergrowth

UCSF, Department of Medicine, CME
16
6 1
Case#4Whichofthefollowingisthemostlikelycauseofthispatient’ssyndromeandmalnutrition?
1. Whipple’s Disease
2. Crohn’s Disease
3. Celiac Disease
4. Pancreatic exocrine insufficiency
5. Smallbowelbacterialovergrowth
Case #4
6 2
6 3
Case #4
l Severeceliac diseasewithprofound malabsorptionl Gluten bound byparticular HLAtypesresults in
inflammatory cascade damaging SBmucosal Presentation ranges from asymptomatic tomildiron
deficiency toIBSsymptoms toseveremalabsorptionl Dx: EGD(villous atrophy, increased IELs) and/or
serologicmarkers (anti-tissue transglutaminase Ab)l Smallbowelmucosa andauto-antibodies can
normalizewithgluten freediet
Green PH. New EnglJ Med 2007; 357(17):1731-43. 6 4
Case #4l Tx:gluten-freedietl Newagent= larazotide(preventstightjunctionopeningà decreasedglutenuptake)
l Long-termcomplicationsincludeelevatedriskofSBCAs (AdenoCA,lymphoma)andosteoporosis
l Associationwithotherautoimmunediseases,suchasRAandthyroiddisease
l Whipple’sdisease,bacterialovergrowth,Crohn’sdisease&pancreaticinsufficiencycanalsocausemalabsorption
Green PH. New EnglJ Med 2007; 357(17):1731-43.
UCSF, Department of Medicine, CME
17
6 5
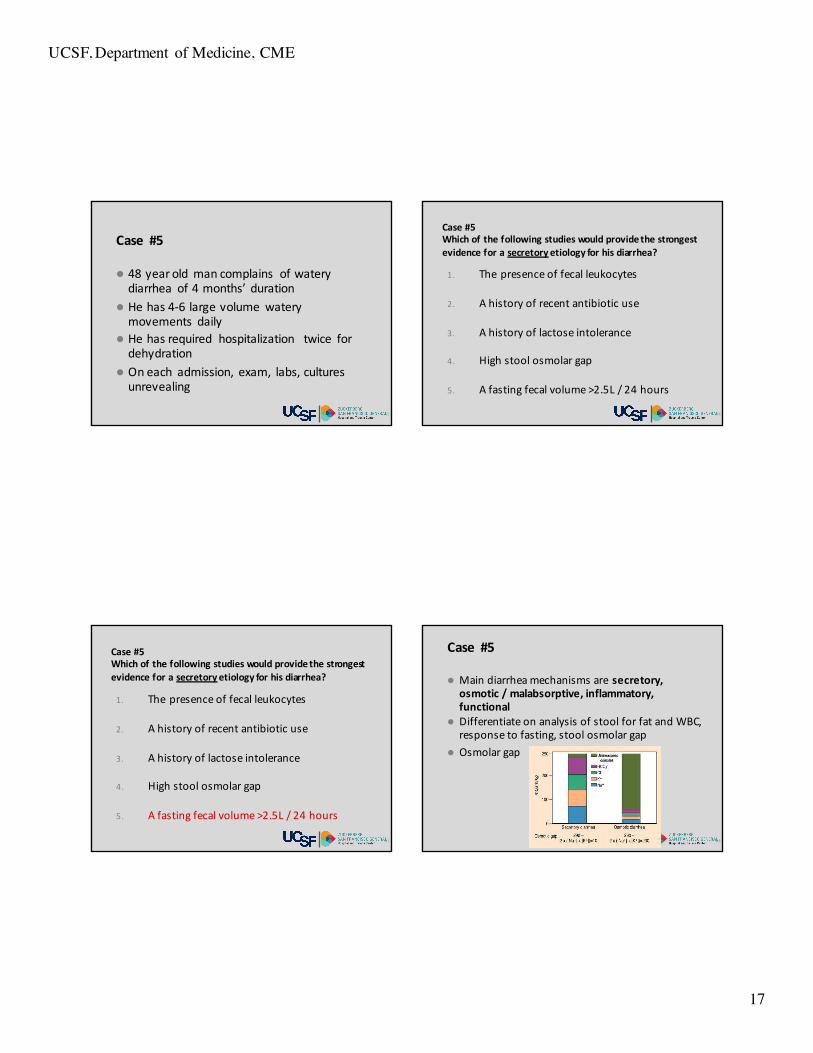
Case #5
l 48yearold mancomplains ofwaterydiarrhea of4months’ duration
l Hehas4-6largevolume waterymovements daily
l Hehasrequired hospitalization twice fordehydration
l Oneach admission, exam, labs,culturesunrevealing
66
Case#5Whichofthefollowingstudieswouldprovidethestrongestevidenceforasecretory etiologyforhisdiarrhea?
1. The presence of fecal leukocytes
2. A history of recent antibiotic use
3. A history of lactose intolerance
4. High stool osmolar gap
5. A fasting fecal volume >2.5L / 24 hours
67
1. The presence of fecal leukocytes
2. A history of recent antibiotic use
3. A history of lactose intolerance
4. High stool osmolar gap
5. A fasting fecal volume >2.5L / 24 hours
Case#5Whichofthefollowingstudieswouldprovidethestrongestevidenceforasecretory etiologyforhisdiarrhea?
6 8
Case #5
l Maindiarrheamechanismsaresecretory,osmotic/malabsorptive,inflammatory,functional
l DifferentiateonanalysisofstoolforfatandWBC,responsetofasting,stoolosmolargap
l Osmolargap

UCSF, Department of Medicine, CME
18
6 9
Case #5
l Secretorydiarrheaistypicallylargevolume(>1L/d)anddoesnotdiminishwithfasting
l Causesofsecretorydiarrhea:l Bacterialandparasiticinfections(i.e.,gastroenteritis)l Bilesaltmalabsorptionfromilealresectionl Medicationsl Smallintestinalbacterialovergrowth(SIBO)l Hormonesecretingtumorsl Microscopiccolitis
70
Diarrhea
l Celiacdiseasecancausebothsecretoryandosmotic(malabsorptive)diarrhea
l Osmoticdiarrhea:lactoseintolerance,magnesiumintake
l Inflammatorydiarrhea: usuallyduetobacterialcolitisorIBD
71
Steatorrhea
l Elevated fecal fatsuggestsmaldigestionormalabsorption
l Fattydiarrheacanbeduetodefective:l Lipolysis(pancreaticinsufficiency)l Micellarization(bilesaltinsufficiency)l Absorption(intestinalepithelium)l Delivery(lymphatics)
+ à
IBS
l Functional GIdisorder affecting 10-20% ofadults inUS
l Abdominal painordiscomfort associatedwith altered bowel habits;pain improvedwith improved bowel habits
l IBSisasyndrome – there aremanypotential causes/contributors
72

UCSF, Department of Medicine, CME
19
Functionaldisease
Abnormalmotility
Lifestress
Psycho-social
Visceralhypersensitivity
InfectionsHormones Foods
Coping
Socialsupport
Childhood
Family
Foods
Infections
Gas
IBSManagement
l Treattheprimary bowel symptoml Antidepressant therapyl Trialofantibiotics forsmallintestinalbacterial overgrowth
l Cognitive behavioral therapy
75
Otherdiarrheal syndromes
l Ecoli0157:H7associatedwithHUS(renalfailure, thrombocytopenia, hemolyticanemia)
l Diabeticwithdiarrhea:considerSIBO,osmotic(sorbitol),“diabeticdiarrhea”
l Considerfactitiousdiarrheainmedicalpersonnelwithunexplaineddiarrhea
l Inhospital-acquireddiarrhea,considerCdifficileandmedications
carbohydratesfats
proteinsmagnesium
trace elementsvitamins Water and
electrolytes
shortchainfatty acids
iron,calcium,copper
folate
vitaminB12bilesalts
Colonicdiseasedoesnotcausemalabsorption
What’s (mal)absorbed where?

UCSF, Department of Medicine, CME
20
7 7
Cdifficile
l Riskfactors:hospitalization,antibiotics,chemotherapy,immunesuppression,PPIs
l Communityacquired C.difficile increasinglycommon
l C.difficile sporesarehardyandhighlyinfectiousl Haveahighindexofsuspicionintheelderly,immunosuppressed,immunocompromised,andpatientswithIBD
Case #6
l 87y/omanwithhistoryofAFib,HTN,CAD,andDMpresentstoERwith1dayofcrampyleftlowerquadrantabdominalpainandbloodystool
l PEx:BP106/75,pulse112,mildLLQTTP,andmaroonstoolonrectalexam
l Hct36%,WBC12Kl CTAbdshowsleftcolonwallthickeningl Thepatientisadmittedtothehospitalandgentlefluidresuscitationisinitiated
79
Case#6Whichofthefollowingisthemostappropriatenextstep?
1. Visceral angiogram
2. Flexible sigmoidoscopy
3. Thrombolytic therapy
4. Renal dose dopamine
5. Stool forCdifficile toxin
80
Case#6Whichofthefollowingisthemostappropriatenextstep?
1. Visceral angiogram
2. Flexible sigmoidoscopy
3. Thrombolytic therapy
4. Renal dose dopamine
5. Stool forCdifficile toxin

UCSF, Department of Medicine, CME
21
8 1 8 2
Case #6
l Ischemiccolitis:seenwitholderage,atherosclerosis,arrhythmiasandhypotension
l Youngerindividuals:stimulantdruguse,enduranceathletes
l Classicpresentationissudden,crampyabdominalpainassociatedwithhematochezia
83
Case #6
l Watershedregionsmostcommonlyinvolvedthoughstudiessuggestmultipledistributions
l Rectalsparingduetocollateralflowviathehemorrhoidalplexus(internaliliacartery)
l Embolicdiseaseusuallymoresevere
Brandt LJ. Am JGastroenterol 2015; 110(1):18-44. 8 4
Case #6
l Flexsigwill reveal rectal sparingandlocalizedsignsofmucosalischemia(ulcerations,hemorrhage)
l Notpathognomonic,buthighlysuggestivel PresentationnotsuggestiveofCdifficile(typicallynonbloodyandwouldnotseetheseendoscopicfindings)
Brandt LJ. Am JGastroenterol 2015; 110(1):18-44.

UCSF, Department of Medicine, CME
22
8 5
Case #6
l Supportivemanagementwithgoalofeuvolemia,normotension
l Pressorsmayworsenvisceralvasoconstrictionl Worseningabdominalexamwithperitonealsigns,lacticacidosissuggesttoxicmegacolonand/orperforationà requires urgentsurgicalevaluation
l Prognosisisgenerallygoodl 80%resolve,15%chronicischemia,5%fulminant
Brandt LJ. Am JGastroenterol 2015; 110(1):18-44. 8 6
Vascular boweldisease
Ischemic colitis Acutemesentericischemia
Chronicmesentericischemia
Bowelsite Colon Smallbowel SmallbowelOnset Acute Acute Chronic/recurrentTypicalpathophysiology
Hypoperfusion EmbolismThrombosis
Atherosclerosis
Presentation Acutecramping andhematochezia
Acute,severe pain“outofproportiontoexamination”
Recurrent post-prandialpain“foodfear”
Naturalcourse 80%resolves15%chronic5%fulminant
Deathifnotrapidlytreated
Gradualchronicworsening
Treatment Conservative Emergentsurgery Elective surgicalorendovasculartherapy
Inflammatory boweldisease
l IBDresults fromuncontrolled immuneresponse inthegut
87
Inflammatory boweldisease
8 8
Environmentaltriggers
Moderatelyinflamed
Failure to down-regulate
Chronic uncontrolledinflammation = IBD
Down-regulate
Normal gutcontrolled inflammation
Normal gutcontrolled inflammation

UCSF, Department of Medicine, CME
23
Pathologicfeatures UlcerativeColitis Crohn’sdiseaseTransmuralinvolvement No(exceptfulminant) Yes“Skiplesions” No YesFibrosis Minimal CommonFistulae No CommonGranulomas No Yes,in20%Smallboweldisease No Yes,75%Rectalinvolvement Always Occasional
Clinical features UlcerativeColitis Crohn’sdiseaseDiarrhea Verycommon CommonBloodper rectum Verycommon OccasionalAbdominalpain Common VerycommonConstitutional symptoms Common CommonStrictures/abscesses/fistulae No CommonPerianaldisease No CommonExtra-intestinalmanifestations Occasional OccasionalRecurrenceaftersurgery No Common,>50%Malignancy Occasional Occasional
90
Colitis
l NSAIDusemayresultinsymptomsmimickingIBDormayexacerbateexistingIBD
l RiskCRCinIBDproportionaltoextentofcoloninvolvedanddurationofillness
l EIM: arthritis,uveitis,erythemanodosum,pyodermagangrenosum,sclerosingcholangitis
Medicaltherapy
5ASA
Antibiotics
Steroids
Immuno-modulators
Biologics
Supportiveagents
Cancerscreening inIBD
l Ulcerative colitis proximal totherectum orCrohn’s diseasewith significant colonicinvolvement
l Diseaseduration > 8yearsl Colonoscopy q1-2 yearswith targetedbiopsies plus random biopsies ORchromoendoscopy
92Laine L.Gastrointest Endosc 2015; 81(3):489-501.

UCSF, Department of Medicine, CME
24
9 3
LowerGIB
l 10%w/hematocheziahaveUGIsourcel >80%LGIBstopsspontaneously,25%recurl Diverticulosismostcommoncausel TaggedRBCscan(bloodloss0.1cc/min,6cc/hr)l Angiography(bloodloss0.5cc/min,30cc/hr)l Colonoscopycanbepursuedbutrequiresrapidprep
Diverticulardisease
l Common inelderlyl Notreatment indicatedl Complications: LGIBanddiverticulitisl Diagnosis ofdiverticulitis warrants futurecolonoscopy torule out cancer
l Consider surgeryifrecurrent diverticulitis
94
Hemorrhoids
l Hemorrhoidalveinsarevenouscushionstomaintaincontinence
l Whenlargeanddilatedtheyareclinicallyreferredtoashemorrhoids
l Management:keepstoolssoft;surgicalinterventionpossibleifrecurrentbleeding
95
Constipation
Age<50,noalarmsymptoms
l Considermedicationsassource
l Increasedfluidandfiberintake
l Stoolsofteners(polyethyleneglycol,docusatesodium)
l Anthraquinonelaxatives(senna,bisacodyl)
Age>50oralarmsymptoms;noresponsetoinitialtherapyl Colonoscopyl Defecographyandanorectal
manometryifdyssynergicdefecationislikely
Variablepatientdefinition,mostoftenduetobehavioralordietarycauses

UCSF, Department of Medicine, CME
25
9 7
Case 7
l A62y/omanhasapositiveFOBTcollectedviadigitalrectalexam
l Takesadailylow-doseASAforcardioprotectionl ReportsoccasionalBRBwhenhewipeswithtoiletpaperforyears,especiallywithstraining
l Nofamilyhistoryofcolorectalcancerl NootherGIsymptoms
98
Case7Whichofthefollowingisthebestapproachatthistime?
1. Repeat FOBT on spontaneously defecated stool
2. Colonoscopy
3. Flexible Sigmoidoscopy
4. Barium Enema
5. CT colonography
99
Case7Whichofthefollowingisthebestapproachatthistime?
1. Repeat FOBT on spontaneously defecated stool
2. Colonoscopy
3. Flexible Sigmoidoscopy
4. Barium Enema
5. CT colonography
100

UCSF, Department of Medicine, CME
26
1 0 1
Case #7
l CouldbefalsepositiveFOBTduetoDREorhemorrhoids,butapositivetestalwaysrequiresacompletecolonoscopy
l Norolefor“confirmatory”retesting
102
Colorectalcancerscreening
l ApprovedCRCscreeningmethods:l Colonoscopy(q10years)l Flexiblesigmoidoscopy(q5years)l CTcolonography (q5years)l FOBT/FIT(annually)l BEhasfallenoutoffavor(q5years)
l Anypositiveexamà colonoscopyl CEAnotusedforscreeningl FecalDNAnotwidelyused
Levin B.Gastroenterology 2008; 134(5):1570-95.
1 0 3
Polyps&colorectalcancer
l IncreasedCRCriskl Personalorfamilyhistoryofpolypsorcancer
l 10yearsbefore ageofaffected family member orage40,whichever is earlier
l IBD:after8-10years ofdiseasel Subsequentcolonoscopyintervalsifaveragerisk
l 10yearsifnopolypsl 5yearsis< 2smalladenomasl 3yearsif>2small,oranylarge(10mm+)adenomas
Lieberman DA. Gastroenterology 2012; 143(3):844-57. 1 0 4
Cancersyndromes
l FamilialAdenomatousPolyposis:AD,1/3newmutations,cancerin30sw/ocolectomy
l Gardner's =FAPw/extracolonicosteomas,desmoidtumors,congenitalhypertrophyofthepigmentedretinalepithelium
l Bothcausedbysamemutation(APC),atumorsuppressergene
l MaincauseofdeathinFAPandGardner’spatientss/pcolectomyisperiampullaryneoplasia;nextaredesmoidtumors

UCSF, Department of Medicine, CME
27
1 0 5
l Turcot's =FAPw/CNSmalignanciesl Lynch Syndrome=HereditaryNon-PolyposisColorectalCancer(HNPCC).AD,incompletepenetrance,R-sidedCRCs,betterprognosisthanFAPl Increasedriskofovarian,endometrial,breast,gastric,
ampullaryCAl CausedbymutationsinDNAmismatch-repairgenes
Cancersyndromes
1 0 6
CASE #8
l 59y/oChinesewomanrecentlyimmigrated toUSwith4monthsofprogressivedyspepsia,describedasaperiumbilicalgnawingorfullness
l 12lbweightlossandearlysatietyl EGDrevealsdiffusegastricatrophyanda1.5cmulcerinthefunduswithexophyticedgesl Ulcerbiopsies– granulationtissuel Gastricbodybiopsies–organismsconsistentwithH
pylori
1 0 7
CASE#8Whichofthefollowingisthebestapproachatthistime?
1. Treat for H pylori, then repeat EGD
2. Treat for H pylori, repeat EGD if symptoms persist
3. Treat for H pylori, check UGIS if symptoms persist
4. Treat for H pylori, noneed to repeat EGD
5. PPI BID, no need to treat forH pylori if symptoms resolve
108
CASE#8Whichofthefollowingisthebestapproachatthistime?
1. Treat for H pylori, then repeat EGD
2. Treat for H pylori, repeat EGD if symptoms persist
3. Treat for H pylori, check UGIS if symptoms persist
4. Treat for H pylori, noneed to repeat EGD
5. PPI BID, no need to treat forH pylori if symptoms resolve

UCSF, Department of Medicine, CME
28
1 0 9 1 1 0
CASE #8
l Proximal location, Hpylori, recent Asianimmigrant, exophytic marginsconcerning formalignancy
111
CASE #8
l Allgastriculcersrequirerepeatendoscopyaftermedicaltreatment toconfirmhealingandexcludeneoplasia
l Patientwithmultiple, small,antralulcers,especiallywithknownriskfactors(suchasNSAIDs)istheexception
l RepeatEGDnotrequiredfortypicalduodenalulcers,ascancerriskisverylow
ASGE Standards of Practice Committee. Gastrointest Endosc 2010; 71(4): 663-8. 1 1 2
Gastric cancer
l Riskfactors:Hpylori,achlorhydria(partialgastrectomy,atrophicgastritis),intestinalmetaplasia,adenomatousgastricpolyps,smoking,alcoholabuse
l Majorityisadenocarcinomal Gastriclymphomaisthemostcommonsiteofextranodallymphoma
l MALTlymphoma:related toHpylori,canoftenbecuredwithHP eradicationalone

UCSF, Department of Medicine, CME
29
1 1 3
Esophageal cancer
l Esophagealadenocarcinomariskfactors:malegender,Caucasian,Barrett’s,smoking,obesity,alcoholabuse
l Squamouscell esophagealcancerriskfactors:alcoholabuse,smoking,causticingestion,achalasia,tylosis,dietarynitrates
l StagewithCTscanà endoscopicultrasoundifnometsonCT
114
l Veryuncommon, butcanincludeadenocarcinoma, carcinoid, GIST,lymphoma
l Riskfactors: celiacdisease, Crohn’s disease,familial polyposis, HIV(lymphoma)
Small bowelcancer
1 1 5
Pancreatic cancer
l Incidenceincreasing,nowthe4th leadingcauseofcancerdeathinUS(lung,colon,breast)
l Riskfactors:smoking,alcoholabuse,chronicpancreatitis
l Mainlyadenocarcinoma,70%inpancreaticheadl SystemicmanifestationsofPancCA:polyarthritis,subcutaneousfatnecrosis,migratorythrombophlebitis
116
Otherpancreatic cancers
l IPMN,cystadenocarcinoma,neuroendocrinel Isletcell tumors:
l insulinomas→ hypoglycemial glucagonomas→ hyperglycemia&rash(necrolyticmigratoryerythema)
l gastrinoma→pepticulcerdisease,diarrheal VIPoma→ waterydiarrhea,hypokalemia

UCSF, Department of Medicine, CME
30
Pancreatic cysts
l Serouscystadenoma (or carcinoma),mucinous cystadenoma (orcarcinoma),IPMN,pseudocysts
l Common incidentalomas
117
Pancreatic cysts – newguidelines
l Highriskfeatures: >3cminsize, solidcomponent, dilated PD
l 0-1high-risk feature:MRIin1yearthenq2yearsx2
l >1high-risk feature:EUSwith FNAl IfEUSwithout concerning featuresàMRIl Iflesion intail, easiertoresect surgically
118Vege SS.Gastroenterology 2015; 148(4):819-22.
TheEnd
1 1 9