Wiring of-mandible
46
WIRING OF MANDIBLE GROUP 2 (SECTION C) PRESENTED TO: DR. ASAD MANZOOR , DR. MISBAH
-
Upload
zohaib-saleem -
Category
Science
-
view
129 -
download
11
Transcript of Wiring of-mandible

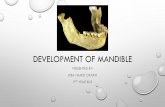
WIRING OF MANDIBLE
GROUP 2 (SECTION C)PRESENTED TO: DR. ASAD MANZOOR , DR. MISBAH

OUTLINE: Introduction Anatomy Etiology Signs and symptoms Diagnosis Treatment Repair of fracture

INTRODUCTION Fracture of the mandible are very common due to its prominence and location. Mandibular fracture also known as fracture of jaw, are breaks through the
mandibular bone . Although any breeds and species can be affected . The pattern and type of fracture is determined by the a) Direction of force b) Mechanism of injury.

Three most common mandibular fractures are:1) Mandibular symphysis2) Mandibular body3) Mandibular ramus
SITES FOR MANDIBULAR FRACTURE

Lateral view

MEDIAL VIEW

MUSCLES

BLOOD SUPPLY
Mental. A Facial .A Transverse facial .A Lingual .A External carotid .A Cranial laryngeal .A



ORTHODONTIC SURGICAL INSTRUMENTS1. Scalpels:Used for incision
(i) Small general purpose blade
(ii) Blade for opening abscesses
(iii) Blade for fine dissection
2. Diagonal Wire Cutter
3. Wire Bending Used for bending wire

ORTHODONTIC SURGICAL INSTRUMENTS
4. Light Wire Bird Beak Used for forming precise loops
5. BABCOCK Suture Wire, Stainless Steel B&S Gauge Diameter 18 GA .040” 20 GA .032” 22 GA .025” 24 GA .020” 25 GA .018” 26 GA .016” 28 GA .012” 30 GA .010” 32 GA .008” 34 GA .006” 36 GA .004”
18- to 20-gauge (for dogs) 20- to 22-gauge (for cats) orthopedic wire

6. Lip retractor
7. Drill machine

8.Wire passer
9. Mouth gags

SIGNS AND SYMPTOMS Pain Drooling of saliva Inability in eating Malocclusion of teeth Bleeding Difficulty in opening of jaw Swelling of the faceFractured teeth

CAUSES OF MANDIBLE FRACTURE Physical factors▪Trauma ▪ Road accident ▪Gunshot wound to the face
Pathological factors Neoplasia Metabolic bone disease Infection

DIAGNOSIS History of physical Trauma or Injury. Physical Examination and Clinical Signs X-ray of Mandible Radiographs from lateral, ventrodorsal, oblique and open mouth view for full
extent examination of the fractured part of the mandible.

Treatment of Mandible Fractures
• Primary Goal:1. Restoration of proper dental occlusion.
• Basic Principles:1. Stable anatomic or functional fixation of fracture fragments
2. Avoidance of soft tissue entrapment and dental trauma
3. Assessment of tissue viability

Different Scenarios of Mandibular Fracture

Firstly, airway regulation to help the patient for successful respiration. Rapid acting intravenous induction is necessary. Oral intubation is necessary for initial approach . endotracheal intubation will help to prevent the suffocation during surgery.
INITIAL APPROACH

1) The oral cavity is rinsed with dilute antiseptic solution such as 1percent povidone -iodine. 2) If an open fracture is present, antibiotics are used before surgery to avoid the risk of infection. 3) Ampicillin with sulbactam (10-20mg \ kg)or third generation cephalosporin are effective.
PREOPERATIVE CARE

Treatment of mandibular symphysis
Type of fracture Treatment options
separation • Cerclage wire• Hemicerclage wire• screw

1) TREATMENT OF MANDIBULAR SYMPHYSIS FRACTURES VIA CERCLAGE WIRE: Separation of Mandibular Symphysis is very common in dogs. Following the manipulative reduction of the symphysis, a single 6 inch to 8 inch
long, 18- to 22-gauge stainless steel wire is threaded through a prebent needle and then introduced caudal to canine tooth lateral to the horizontal ramus through the mucosa and out through the skin on the midline ventral to the mandible.
The other end of the wire is introduced in a similar manner and the orthopedic wire is directed ventral chin incision ,twisted as they exit the skin.
Reduction of the fracture is obtained while the wire is tightened. The wire is cut off, leaving approximately three twists. It is usually allowed to remain in place for 12 weeks. Removal can be accomplished with a wire cutter by snipping the wire between the canine teeth and pulling it out ventrally.

Mandibular Symphysis Fractures


HEMICERCLAGE WIRE Technique prevents shearing. Can be used for revision surgeries. Ventral approach to mandibular symphysis is performed and fracture is reduced ,
hole is drilled just caudal to the roots of canine teeth , perpendicular to the symphysis.
A hemicerclage wire is inserted through the hole and is tightened ventrally.

2) FRACTURES OF THE BODY OF THE MANDIBLE

INTERDENTAL WIRING Holes are predrilled in the alveolar border of the mandible between the teeth with a
small krischner wire. A piece of 0.4 to 0.5mm orthopedic wire is inserted into these holes in loops. The wire is passed through the loops intraorally.
The loops are tightened individually over the intraoral wire. Alternatively , a 0.6 mm Krischner wire can be used as an intraoral splint , around which the wire loops are anchored. The oral part of the splint can be reinforced with dental composite if deemed necessary.



3) FRACTURES OF MANDIBULAR RAMUS

INTERFRAGMENTARY WIRING An orthopedic wire is inserted on the oral side of the mandible through two
predrilled holes , around 5mm away from fracture line .
The location of the drill holes is also dictated by the location of the tooth roots,
which should be avoided. An additional wire can be placed at the aboral side of the
mandible to enhance neutralization of shear and rotational forces.
In case of butterfly fracture , the directly from the oral cavity , provided the fracture
stability is judged to be sufficient for only one suture to be placed at the rostral
mandibular angle.


INTERARCUATE WIRING Valid alternative to primary fracture repair, especially in multifragmentary fractures. 0.6 or 0.8mm wire is inserted through predrilled holes in the oral border of maxilla
mandible, and is tightened just enough for the cat/dog to open the mouth a few millimeters.
The holes are usually drilled between the premolar and molar tooth roots. It is mostly done bilaterally but sometimes applied sometimes for correction of
lateral deviation of lower jaw. Release the fixation immediately in case of vomiting.




COMPLICATIONSLower jaw heals in wrong alignment. The patient may suffer from a malocclusion . May injure the tooth roots and neurovascular bundle within the mandible. Incisional dehiscence.Infections.Mandibular drift and instability.

POST OPERATIVE CARE Analgesics for at least 48-72 hours after surgery. Post operative antibiotics are also recommended for first 5-7 days. Moist food to protect surgical incisions. Access to chew toys or bones should be restricted until incision is healed.

Repair of a Fracture

STAGES IN THE HEALING OF A BONE FRACTURE Hematoma formation
Torn blood vessels hemorrhage A mass of clotted blood (hematoma) forms at the fracture site Site becomes swollen, painful, and inflamed 3-4 hours
Hematoma

FIBROCARTI LAGINOUS CALLUS FORMS Granulation tissue (soft callus) forms a few days after the fractureCapillaries grow into the tissue and phagocytic cells begin cleaning debris
2 Fibrocartilaginous callus formation
Internal callus (fibrous tissue and cartilage)
External callus
New blood vessels
Spongy bone trabeculae

Bony callus formationNew bone trabecular appear in the fibro
cartilaginous callusFibro cartilaginous callus converts into a bony
(hard) callusBone callus begins 3-4 weeks after injury, and
continues until firm union is formed 2-3 months later
3 Bony callus formation
Bony callus of spongy bone

CONT.The fibro cartilaginous callus forms when:
Osteoblasts and fibroblasts migrate to the fracture and begin reconstructing the bone
Fibroblasts secrete collagen fibers that connect broken bone endsOsteoblasts begin forming spongy boneOsteoblasts furthest from capillaries secrete an externally bulging cartilaginous
matrix that later calcifies

Bone remodelingExcess material on the bone shaft
exterior and in the medullary canal is removed
Compact bone is laid down to reconstruct shaft walls
4 Bone remodeling
Healing fracture