Whooping cough
25
WHOOPING COUGH Dr. Rajalekshmy.P.R Dept of Swasthavritta Amrita School of Ayurveda
-
Upload
drrajalekshmy-arun -
Category
Health & Medicine
-
view
391 -
download
0
Transcript of Whooping cough

WHOOPING COUGH
Dr. Rajalekshmy.P.RDept of Swasthavritta
Amrita School of Ayurveda


INTRODUCTION• Pertussis, also known as whooping cough is a highly contagious
bacterial disease mainly caused by Bordetella pertussis.
• Clinically characterized by an insidious onset with mild fever and an irritating cough, gradually becoming paroxysmal with characteristic whoop often with cyanosis and vomiting.
• Also known as hundred day cough.
• Habit pattern of coughing may last for longer or subsequent weeks & months.
DERIVATION• Following a fit of coughing a high-pitched whoop
sound or gasp may occur as the person breathes in.
• The coughing may last for more than a hundred days or ten weeks.
• A person may cough so hard they vomit, break ribs, or become very tired from the effort.
• Children less than one year old may have little or no cough and instead have periods where they do not breathe.

PROBLEM STATEMENT• Important cause of death of infants worldwide.• Public health concern even in countries with high vaccination coverage.• 2010- about 1.29 lac cases were reported to WHO globally.• Most lethal disease of infants and young children who have not been
immunized, particularly those with underlying malnutrition and other respiratory infections.• India- Marked decline of disease after launch of UIP.• 1987: incidence-1.63 lakh cases• 2011- 39,091 cases (decline-76%)

AGENT• Bordetella pertussis• Gram negative organism • Small, ovoid, cocobacillus.• Length - 0.5 microns• Have bipolar metachromatic granules
when stained with Toludine blue.• Occurs in smooth and rough phases,
capsulated and non-capsulated forms.

• Loose clumps of bacilli appear as thumb print appearence with clear space between the organisms.• Freshly isolated strains have
fimbria.
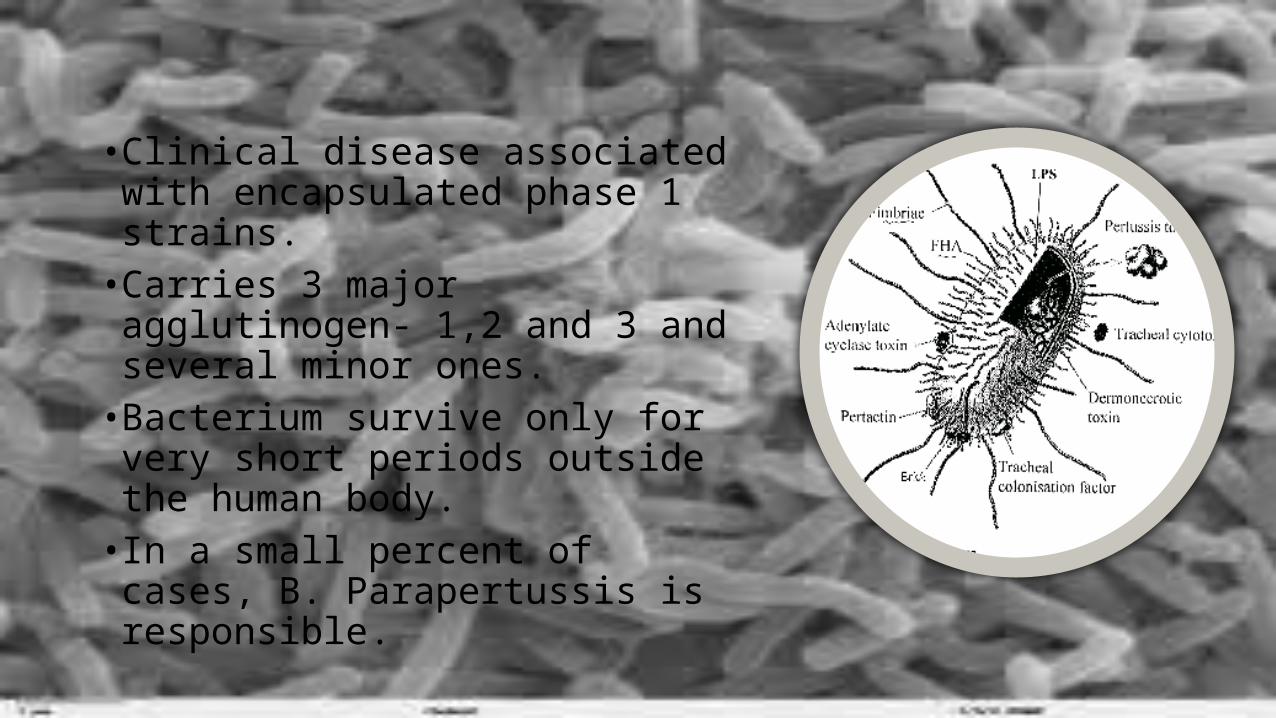
• Clinical disease associated with encapsulated phase 1 strains.• Carries 3 major agglutinogen- 1,2
and 3 and several minor ones.• Bacterium survive only for very
short periods outside the human body.• In a small percent of cases, B.
Parapertussis is responsible.

SOURCE OF INFECTION• B.Pertussis infects only man.• Source of infection is a case of
pertussis.• Chronic carrier does not exist.

INFECTIVE MATERIAL• Infective bacilli occurs abundantly in the nasopharyngeal and
bronchial secretions.•Objects freshly contaminated by discharge are also infective.

INFECTIVE PERIOD
•Most infectious during catarrhal stage.• Extends from a week after exposure to about 3 weeks after
the onset of paroxysmal stage.
SECONDARY ATTACK RATE
• 90% in unimmunized household contacts.

HOST FACTORS
SEX
Incidence and fatality more among females than males.
AGE
Infants and pre-school childrenHighest incidence-below 5 yrs.
Highest mortality-infants below 6 months.
IMMUNITY
• Recovery from pertussis or adequate immunization is followed by immunity.• Second attacks may occur in persons with declining immunity.• Maternal antibodies does not appear to give them protection.

ENVIRONMENTAL FACTORS
•Occurs throughout the year.•Disease shows seasonal trends with more cases in winter and
spring due to overcrowding.• Socio economic conditions and way of life influences
epidemology.

MODE OF TRANSMISSION• Spread through droplet infection and direct contact.• Bacilli spread into air through cough, sneezes or talks.

INCUBATION PERIOD• 7-14 days, but not more than 3 weeks.

PATHOGENESIS• The bacterium contains a surface
protein, filamentous haemagglutinin adhesin, which binds to the sulfatides found on cilia of epithelial cells.
• Once anchored, the bacterium produces tracheal cytotoxin, which stops the cilia from beating.
• This prevents the cilia from clearing debris from the lungs, so the body responds by sending the host into a coughing fit.
• These coughs expel some bacteria into the air, which are free to infect other hosts.


CLINICAL COURSECATARRHAL STAGE
Lasts for about 10 daysInsidious onset, lacrimation, sneezing,
coryza, anorexia, malaise, hacking night cough
PAROXYSMAL STAGE
Lasts for 2-4 weeksBursts of rapid, consecutive coughs followed by
deep, high pitched inspiration(whoop).Followed by vomiting
Young infants- cyanosis and apnoeaAdults & adolescent-persistent cough
CONVALESCENT STAGE
Lasts for 1-2 weeksIllness generally lasts for 6-8 weeks.

COMPLICATIONS• Occurs in 5-6% cases, most frequent in infants less than 6 months.
• Complications-bronchitis, bronchopneumonia, bronchiectasis
• Violent paroxysm precipitate subconjunctival haemorrhage, epistaxis, haemoptysis and cerebral haemorrhage which may cause convulsions and coma.
• Broncho pneumonia occurs in 5.2% cases.

CONTROL CASES
• Early diagnosis, isolation and treatment of cases, disinfection of discharges from nose and throat
• Drug of choice- erythromycin• dose-:30-50mg/kg of body weight in 4
divided doses for 10 days.• Alternatives- ampicillin, septran or
tetracycline
CONTACTS
• Infants and young children should be kept away from cases.
• Known contacts should be given prophylactic antibiotic (erythromycin/ ampicillin) treatment for 10 days to prevent infecting bacteria become established.

ACTIVE IMMUNIZATION• Combined DPT, DTwP or DTaP vaccines• DPT vaccine-3 doses(0.5 ml) intramuscularly at
one month interval, starting at 6 weeks.• Booster dose at 18-24 months.• Acellular pertussis vaccines are used in older
children and adults.• Pertussis vaccination affects pharyngeal
colonization resulting in reduction of bacterial transmission.• Duration of protection: 6-12 years

CONTRA-INDICATIONS
Anaphylatic reactions, H/O epilepsy, convulsions, CNS disorders, reaction to triple
vaccine injectionsUNTOWARD REACTIONS
Local reactions at site of injectionMild feverIrritability
Persistent inconsolable screaming, seizures, anaphylactic reactions, encephalopathy

PASSIVE IMMUNIZATION• Merits of immunoglobulins in pertussis has yet to be established.• No evidence of its efficacy in controlled trials.