ucfsarc.files.wordpress.com€¦ · Web viewFiber types and conduction velocity. Type A fibers...
17
Powerpoint 8 – Sensory Physiology Part 1 1. Sensory Systems a. Need specific receptors b. Types of Receptors i. Photoreceptors – respond to light 1. Located in retina of eye ii. Mechanoreceptors – respond to mechanical stimulus 1. Pacinian corpuscles 2. Joint receptors 3. Stretch receptors in muscle 4. Hair cells in auditory and vestibular systems 5. Baroreceptors in carotid sinus iii. Chemoreceptors – respond to chemical stimulus 1. Olfactory 2. Taste buds 3. Osmoreceptors 4. Carotid body O 2 body iv. Nociceptors – respond to extreme temperature and pain c. Two types of Fibers i. Afferent – takes information from peripheral to CNS ii. Efferent – takes signal from CNS to peripheral d. Sensory Receptors i. Located in peripheral cells/tissues and detect 1. Pain 2. Light 3. Touch 4. Temperature 5. Vibration 2. Fiber types and conduction velocity a. Type A fibers myelinated and thickest fibers i. A-alpha 1. Large alpha-motor neurons 2. Conduction velocity a. Fastest ii. A-beta 1. Touch 2. Pressure 3. Conduction velocity
-
Upload
dinhkhuong -
Category
Documents
-
view
221 -
download
4
Transcript of ucfsarc.files.wordpress.com€¦ · Web viewFiber types and conduction velocity. Type A fibers...

Powerpoint 8 – Sensory Physiology Part 1
1. Sensory Systemsa. Need specific receptorsb. Types of Receptors
i. Photoreceptors – respond to light1. Located in retina of eye
ii. Mechanoreceptors – respond to mechanical stimulus1. Pacinian corpuscles2. Joint receptors3. Stretch receptors in muscle4. Hair cells in auditory and vestibular systems5. Baroreceptors in carotid sinus
iii. Chemoreceptors – respond to chemical stimulus1. Olfactory2. Taste buds3. Osmoreceptors4. Carotid body O2 body
iv. Nociceptors – respond to extreme temperature and painc. Two types of Fibers
i. Afferent – takes information from peripheral to CNSii. Efferent – takes signal from CNS to peripheral
d. Sensory Receptorsi. Located in peripheral cells/tissues and detect
1. Pain2. Light3. Touch4. Temperature5. Vibration
2. Fiber types and conduction velocitya. Type A fibers myelinated and thickest fibers
i. A-alpha 1. Large alpha-motor neurons2. Conduction velocity
a. Fastestii. A-beta
1. Touch2. Pressure3. Conduction velocity
a. Mediumiii. A-gamma
1. Gamma-motor neurons to muscle spindles2. Conduction velocity
a. Medium

iv. A-delta 1. Touch2. Pressure3. Temperature4. Fast pain5. Conduction velocity
a. Medium b. Type B fibers myelinated and medium thickness fibers
i. Preganglionic autonomic fibersii. Conduction velocity
1. Mediumc. Type C fibers unmyelinated and thinnest
i. Slow painii. Postganglionic autonomic fibers
iii. Conduction velocity1. Slowest
3. Receptive field of a sensory neurona. The area of the body that the sensory neuron innervates. b. Stimulating the receptive field of a sensory neuron stimulates the neuron
4. Sensory transduction stimulation of a sensory receptor to produce a signala. Steps
i. Stimulus of sensory receptorii. Ion channels open in receptor allows current flow (usually inward)
iii. Receptor is depolarizediv. This leads to change in membrane potential receptor potential (generator potential)v. Signal sent down afferent nerve fiber
5. Adaptation of Sensory Receptorsa. Slow adapting (tonic)
i. Respond repetitively to prolonged stimulusii. Examples
1. Slow pain2. Pressure3. Muscle spindle
b. Rapidly adapting (phasic)i. Show decline in action potential frequency with time for a constant stimulusii. Example
1. Pacinian corpuscle2. Light touch3. Smell4. Taste5. Temperature

6. Sensory pathway stations for sensory systema. Stimulation of receptor stimulates 1st group of neuronsb. 1st group neurons take information to the inner spinal cord
i. Some synapse in spinal cord in dorsal hornii. Some pass through spinal cord without synapsing and synapse instead in brain stem with 2nd
group of neurons in medulla oblongatac. 2nd group of neurons from brain stem (medullar oblongata) synapse on contralateral thalamus with
3rd group of neuronsd. 3rd group synapses with 4th group in the cerebral cortexe. Information to cerebral cortex results in perception of stimulus
7. Somatosensory systemsa. Detects information about touch, pain, and temperatureb. Types of receptors
i. Mechanoreceptors (touch)ii. Nociceptors (pain)
iii. Thermoreceptors (temperature)c. Two pathways
i. Dorsal column system1. Fine touch2. Pressure3. Two-point discrimination4. Vibration
ii. Anterolateral system1. Temperature2. Pain3. Light touch
d. Both pathways are similar and use general pathway previously described (Receptor Dorsal horn (spinal cord) medulla oblongata (brain stem) contralateral thalamus cerebral cortex)
8. Thalamusa. Each side of thalamus controls sensation on contralateral side of bodyb. Information from parts of body are arranged somatopically (in groups dermatomes)
i. Referred pain (because of dermatomes)1. Origin of some nerves is from same area which controls different part of body2. Important for clinical diagnosis of some diseases or disorders3. Pain is good because it tells us that something is wrong in our body and sometimes
what is wrong as wella. Myocardial infarction
i. Patient has problems in heart but have referred pain in retrosternal area, left shoulder, left arm, left forearm, and last two fingers, and neck area (submandibular region), posterior region of left shoulder
b. Pain in epigastric line (especially right side)i. Two problems
1. Could be gall bladder stone or infection of liver

2. Could be infection of right kidney
9. Pain nociceptiona. Receptors
i. Free nerve endings in skin, muscle, and viscerab. Neurotransmitter
i. Substance P1. Pain relief is inhibition of substance P (opioids inhibit substance P relieve pain)
c. Fast and slow paini. Fast pain
1. Carried by group A-delta fibers2. Rapid onset and offset3. Well localized
ii. Slow pain1. Carried by C fibers2. Aching, burning, or throbbing3. Poorly localized
10. Two-Point Touch Thresholda. If each point touches receptive field of different sensory neurons feel both pointsb. If each point touches receptive field of a single sensory neuron feels like one point
11. Taste gustationa. Chemoreceptors on tongue detect taste taste budsb. Types of taste
i. Salt1. More sensitive on anterior lateral portion of tongue (side toward the front)2. From Na+
ii. Sour1. More sensitive on lateral regions of tongue (sides of tongue)2. From protons (high acidicty)
iii. Sweet1. More sensitive on anterior of tongue (tip of tongue)2. Involves G-protein coupled receptors – GPCR’s
iv. Bitter1. More sensitive at posterior of tongue (back/base of tongue)2. Uses GPCR’s which release gustducin the G-protein is was coupled to
c. Innervation of tonguei. Anterior two thirds (front two thirds) branch of Facial nerve (Cranial Nerve 7) called
Chorda tympaniii. Posterior one third (back one third) Glossopharyngeal nerve (Cranial nerve 9)
iii. Base of tongue (Epiglotis) Vagus nerve (Cranial nerve 10)d. Disorders
i. Bell’s Palsy loss of taste

1. Facial nerve under skin of face can get paralyzed. This means that the small branch of this nerve called the Chorda tympani is paralyzed. This causes taste disorder in patient.
ii. Ageusia loss of taste1. Etiology could be…
a. Nerve problem such as in Bell’s palsyb. Irritation of tongue by foodc. Autoimmune disease of tongued. Tumor or cancer in tonguee. Damage of pathway fibers which take information to taste centerf. Glossitis – inflammation of tongue
iii. Hypogeusia decreases taste sensitivityiv. Hypergeusia increased taste sensitivityv. Glossodynia burning sensation on the tongue
vi. Benign migratory glossitis (geographic tongue)1. Irregular and inflamed patches on tongue which often have white borders2. Tongue may be generally swollen, red, and sore. 3. Cause is unknown
e. Taste Pathwayi. Stations of pathway
1. 1st station Medulla oblongataa. Has 3 nuclei…
i. Geniculate nucleusii. Petrosal nucleus
iii. Inferior ganglion of vagus nerve2. 2nd station Thalamus
a. Has 2 nuclei…i. Left Ventral posterior medial (VPM) nucleusii. Right Ventral Posterior medial (VPM) nucleus
3. 3rd station Taste centera. Located at base of central sulcus in brain
ii. Flow of pathway1. 1st group of neurons from tongue synapse with 2nd group of nuclei in medulla
oblongata. The 1st group is called Tratcus Solitarius2. 2nd group of neurons synapse with 3rd group of neurons in left VPM nucleus of
thalamus3. 3rd group travels to taste center which is located at base of central sulcus of brain
area 43 is taste centeriii. Innervation of tongue (1st group of neurons)
1. Anterior two thirdsa. By corda tympani branch of facial nerve (nerve 7) b. Travels to Geniculate nucleus in Medulla oblongata.
2. Posterior one thirda. By glossopharyngeal nerve (Nerve 9) b. Travels to Petrosal nuclei in Medulla oblongata.
3. Base of tongue (Epiglotis)a. Be Vagus nerve (Nerve 10)b. Travels to inferior ganglion of vagus nerve
iv. Vagus nerve has three nuclei
12. Olfactory System smell, olfactiona. Olfactory pathway
i. Receptors in nasal cavity detect odors
ii. Bind of odor to olfactory receptor stimulates 1st group of neurons which are connected to base of receptor
iii. 1st group pass through cribriform plate which is a bone that separates nasal cavity and olfactory bulb
iv. The 1st group travel through cribriform plate and synapses with 2nd group of neurons in the olfactory bulb located at base of brain
v. 2nd group of neurons in olfactory bulb are called mitral cells. vi. 2nd group of neurons from olfactory bulb are called Olfactory tract.vii. Wen stimulated, neurons in Olfactory tract release stimulatory neurotransmitters detected
by Olfactory center in Cerebral Cortex at base of Olfactory tract. b. Innervation of Olfactory system
i. Cranial nerve 1 olfactory nerve 1. Carries information from olfactory receptor to cells of olfactory bulb2. Axons are C fibers and are some of the smallest and slowest in the nervous system
ii. Cranial nerve 5 trigeminal nerve1. Detects noxious or painful stimuli ammonia
c. Transduction in olfactory receptor neuronsi. Odorant molecules bind to receptors on cilia of olfactory receptor neuronsii. Receptors get activated and activate G protein (G olf)
iii. G protein activates adenylate cyclase (AC)iv. AC increases cAMP which opens Na+ channels in olfactory receptors and depolarize
receptorsv. If depolarized to threshold, action potentials are generated and propagate through pathway
d. Disordersi. Anosmia loss of smell
1. Etiologya. Defect in receptors in nasal cavity
i. Irritationii. Damage
b. Head trauma that affects…i. Olfactory bulbii. Olfactory tract
iii. Olfactory centerii. Phantosmia
1. Psychological problem Something is wrong with CNS 2. Smelling odors not really present
iii. Dysosmia1. Things smell differently than they should
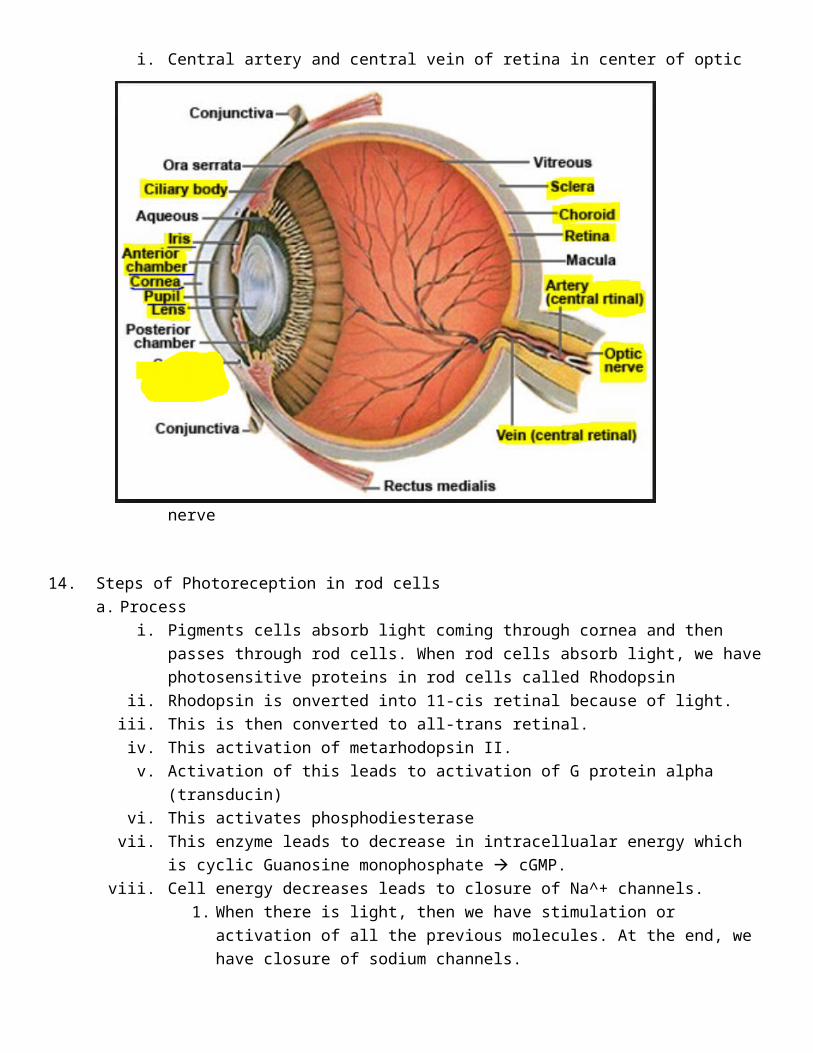
13. Anatomy of the Eyea. Wall of eye has three layers (listed from outer to inner)
i. 1st layer Schlera - External layer is fibrous tissue1. Protects eye from external trauma and covers eye externally2. Continues with anterior portion called cornea
a. Behind cornea we have anterior chamber and pupil

b. Behind pupil we have lensii. 2nd layer Choroid
1. Choroid full of blood vessel2. Gives nutrients and oxygen to eye3. Continues with iris in anterior portion of eye
a. Iris is covered by ciliary body. Ciliary body covers ciliary muscle. b. Iris is full of pigment cells.
4. Ciliary body a. Secretes a fluid which is released into posterior chamber first and then
anterior chamber. b. Intraocular fluid gets into venous system which passes through or is released
through canal of schlemmc. That canal (opening) receives ocular fluid and releases into veins.
i. Obstruction or closure of canal of schlemm leads to Glaucoma1. Obstruction of canal increases interocular fluid and pressure.
This pressure can press on or destroy retina and optic nerve. 2. Non-treated glaucoma leads to blindness. If diagnosed in
time, they can cut some ligaments of canal off by surgery.3. Etiology of glaucoma
a. Congenitalb. Tumorc. Infectiond. Head trauma
iii. 3rd layer Retina1. Layers of retina
a. 1st Pigment cellsb. 2nd photoreceptors
i. These are sensitive to lightii. Two types
1. Rods – sensitive to light. Molecules in rod are similar to the sones in cone cells.
2. Cones – sensitive to wavelength of light (detects color)iii. Blind spot is due to lack of photoreceptors
c. 3rd Bipolar cellsd. 4th horizontal cellse. 5th Amacrine cellsf. 6th Ganglion cells
i. The axon of these neurons (ganglion cells) form Optic nerve 1. Take the information about the light to the central nervous
system and it passes through different stations in CNS. 2. Fovea centralis
a. Small area on retina where the cornea and lens of eye focus lightb. Densely packed with cone cells, no rodsc. Responsible for sharp central vision
b. Posterior part of eye Optic nerve

i. Central artery and central vein of retina in center of optic nerve
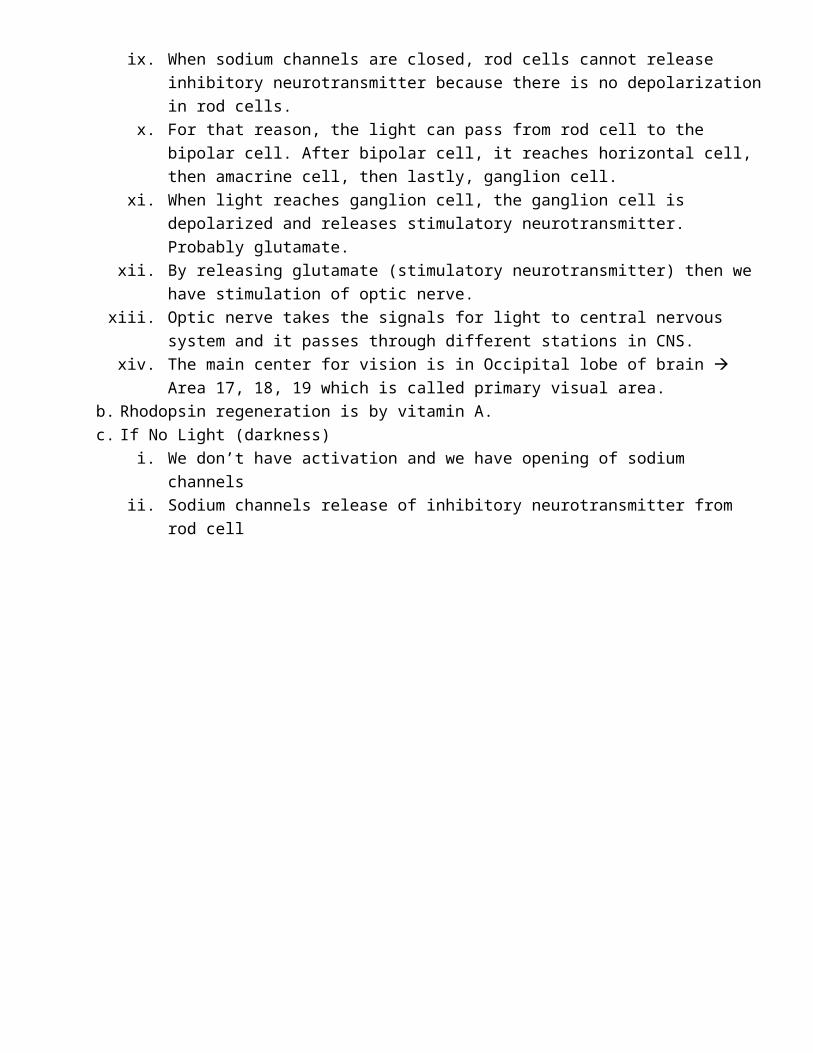
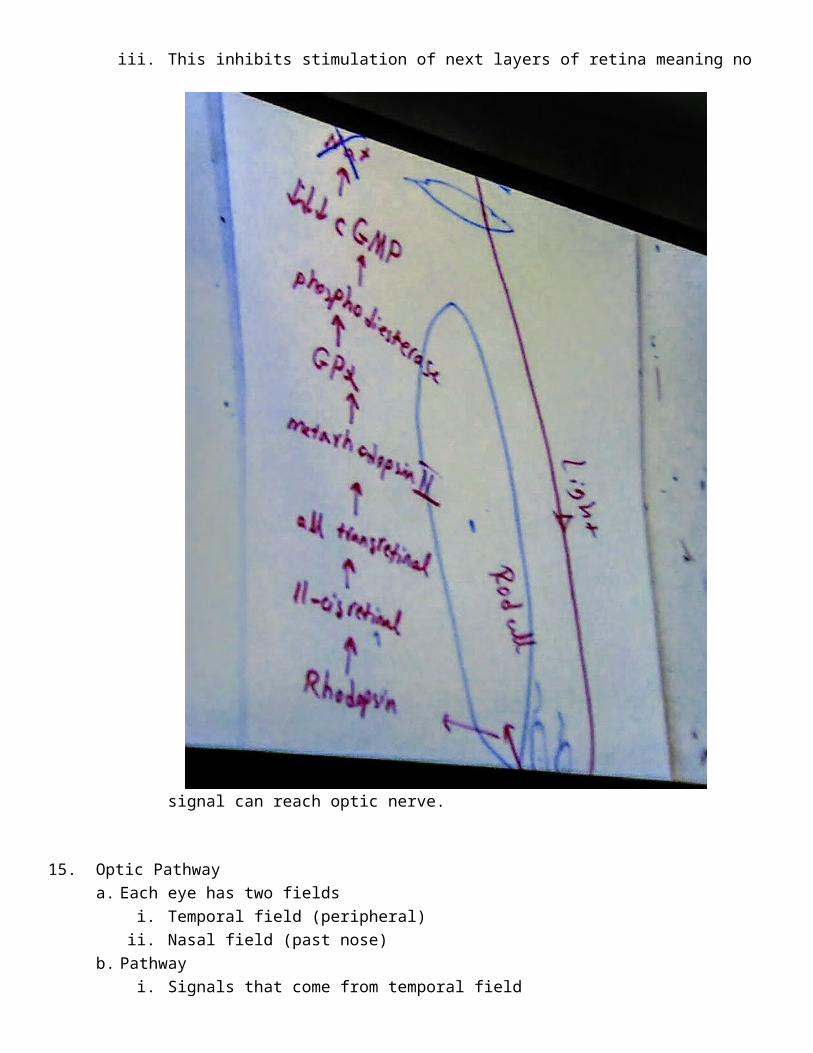
14. Steps of Photoreception in rod cellsa. Process
i. Pigments cells absorb light coming through cornea and then passes through rod cells. When rod cells absorb light, we have photosensitive proteins in rod cells called Rhodopsin
ii. Rhodopsin is onverted into 11-cis retinal because of light. iii. This is then converted to all-trans retinal. iv. This activation of metarhodopsin II. v. Activation of this leads to activation of G protein alpha (transducin)
vi. This activates phosphodiesterasevii. This enzyme leads to decrease in intracellualar energy which is cyclic Guanosine
monophosphate cGMP.viii. Cell energy decreases leads to closure of Na^+ channels.
1. When there is light, then we have stimulation or activation of all the previous molecules. At the end, we have closure of sodium channels.
ix. When sodium channels are closed, rod cells cannot release inhibitory neurotransmitter because there is no depolarization in rod cells.
x. For that reason, the light can pass from rod cell to the bipolar cell. After bipolar cell, it reaches horizontal cell, then amacrine cell, then lastly, ganglion cell.
xi. When light reaches ganglion cell, the ganglion cell is depolarized and releases stimulatory neurotransmitter. Probably glutamate.
xii. By releasing glutamate (stimulatory neurotransmitter) then we have stimulation of optic nerve.
xiii. Optic nerve takes the signals for light to central nervous system and it passes through different stations in CNS.
xiv. The main center for vision is in Occipital lobe of brain Area 17, 18, 19 which is called primary visual area.
b. Rhodopsin regeneration is by vitamin A. c. If No Light (darkness)
i. We don’t have activation and we have opening of sodium channels ii. Sodium channels release of inhibitory neurotransmitter from rod cell
iii. This inhibits stimulation of next layers of retina meaning no signal can reach optic nerve.
15. Optic Pathwaya. Each eye has two fields
i. Temporal field (peripheral) ii. Nasal field (past nose)
b. Pathwayi. Signals that come from temporal field
1. Focus on nasal portion of retina and passes through optic chiasm (contralateral), travels through contralateral optic tract
ii. Signals from nasal field 1. Focus on temporal portion of retina and travels through ipsilateral optic tract.
iii. 1st group of nerve synapse with 2nd group in ganglion of thalamus called lateral Geniculate nucleus (body)
iv. 2nd group of neurons and travel toward Occipital lobe of brain area 17, 18, and 19 which is called Primary Visual Area
1. 2nd group is called Geniculo-calcarine tract
c. Pathology Conditions of optic pathwayi. Lesions in pathway
1. Cut left optic nerve cannot receive signal from left temporal field and also left nasal field. Left eye becomes blind
2. Cut lateral or peripheral portion of left optic nerve you cannot see from left nasal field.
3. Cut optic chiasm left and right temporal fields cannot be seen4. Cut left optic tract cannot see right temporal or left nasal field5. Cut genicular calcarine tract on left side partial damage to left nasal field and
right temporal field.
ii. Color blindness can’t detect all colors1. Congenital or genetic2. Difficulty in cone cells which detect color of light3. Could be due to eye, nerve, brain damage, or due to exposure of certain chemicals
iii. Night blindness1. Difficulty in rod cells (detect light)2. Could be due to lack of Vitamin A (regenerates rhodopsin in rod cells)
iv. Glaucoma1. Obstruction of Canal of schlemm2. Intercranial pressure because of accumulation of interocular fluid in chambers
a. This leads to destruction or pressure on optic nerve and retina3. Non-treatment leads to blindness
v. Visual agnosia
1. Brain cannot recognize or identify objects (familiar faces)2. Problem with CNS, not eye.
vi. Emmetropic normal1. Light focuses on retina
vii. Hypertropia farsighted1. Light focuses behind retina2. Corrected by convex lens
viii. Myopia nearsighted1. Light focuses in front of retina2. Corrected by biconcave lens
ix. Astigmatism curvature of lens not perfect1. Corrects with cylindrical lens