Virtual R&D Day September 29, 2021
118
Virtual R&D Day September 29, 2021
Transcript of Virtual R&D Day September 29, 2021

Virtual R&D Day
September 29, 2021

Forward Looking Statements
This presentation contains forward-looking statements, including, but not limited to, statements related to Horizon’s full-year 2021 net sales and adjusted EBITDA
guidance; expected financial performance and operating results in future periods, including potential growth in net sales of certain of Horizon’s medicines;
development, manufacturing and commercialization plans and strategies; expected timing of clinical trials, studies and regulatory approvals; potential market
opportunity for and benefits of Horizon’s medicines and medicine candidates; and business and other statements that are not historical facts. These forward-looking
statements are based on Horizon’s current expectations and inherently involve significant risks and uncertainties. Actual results and the timing of events could differ
materially from those anticipated in such forward-looking statements as a result of these risks and uncertainties, which include, without limitation, risks that Horizon’s
actual future financial and operating results may differ from its expectations or goals; Horizon’s ability to grow net sales from existing medicines; impacts of the COVID-
19 pandemic and actions taken to slow its spread, including impacts on supplies and net sales of Horizon’s medicines and potential delays in clinical trials; the fact that
Horizon’s full-year 2021 net sales, adjusted EBITDA and TEPEZZA net sales guidance and the expected timing of certain TEPEZZA clinical trials assume that future
committed manufacturing slots for TEPEZZA are not cancelled and are run successfully, which could be impacted by additional government-mandated COVID-19
vaccine production orders and other risks associated with the manufacture of biologic medicines; risks associated with acquisitions, such as the risk that the
businesses will not be integrated successfully, that such integration may be more difficult, time-consuming or costly than expected or that the expected benefits of the
transaction will not occur; the availability of coverage and adequate reimbursement and pricing from government and third-party payers; risks relating to Horizon’s
ability to successfully implement its business strategies, including its manufacturing and global expansion strategy; risks inherent in discovering new medicine targets
and candidates and in developing novel medicine candidates and existing medicines for new indications; risks associated with regulatory approvals; risks in the ability
to recruit, train and retain qualified personnel; competition, including potential generic competition; the ability to protect intellectual property and defend patents;
regulatory obligations and oversight, including any changes in the legal and regulatory environment in which Horizon operates and those risks detailed from time-to-
time under the caption "Risk Factors" and elsewhere in Horizon’s filings and reports with the SEC. Horizon undertakes no duty or obligation to update any forward-
looking statements contained in this presentation as a result of new information.
Dr. Dinesh Khanna, Dr. Martin Kolb and Dr. Bobby Korn serve as consultants to Horizon Therapeutics plc.

Horizon Therapeutics Virtual R&D Day Agenda
CD40L: Cluster of differentiation 40 ligand. | LPAR1: Lysophosphatidic acid receptor 1. | pDC: Plasmacytoid dendritic cell. | TED: Thyroid Eye Disease.
Topic Speakers
Introduction: Vision and Strategy Tim Walbert, Chairman, President and Chief Executive Officer
R&D StrategyElizabeth Thompson, Ph.D., EVP Research & DevelopmentSrini Ramanathan, Ph.D., SVP Research & Development Sciences
Daxdilimab (HZN-7734): First and Only pDC Depleter in Clinical Development; Now Pursuing Five Indications
Bill Rees, Ph.D., VP Translational SciencesTheresa Podrebarac, M.D., M.Sc., SVP Clinical Development
Dazodalibep (HZN-4920): CD40L Antagonist Designed to Block a Central Pathway Involved in Many Autoimmune and Inflammatory Diseases
Bill ReesTheresa Podrebarac
Q&A Session
HZN-825: LPAR1 Antagonist with Early Signals of Benefit in Fibrotic Diseases, Areas with High Unmet Need
Srini RamanathanDinesh Khanna, M.D., M.Sc., Professor, University of Michigan Health
UPLIZNA: Next-Generation B-cell Depleter with a Novel, Targeted ApproachKristina Patterson, M.D., Ph.D., Medical Director, NeuroimmunologyTheresa Podrebarac
Q&A Session
TEPEZZA: Building Evidence to Help Treat More Patients with Chronic TEDBobby S. Korn, M.D., Ph.D., FACS, Professor of Ophthalmology & Plastic Surgery, University of California, San Diego
Q&A Session
Conclusion Tim Walbert

Horizon Leadership Team and Clinical Experts Participating Today
Tim WalbertChairman, President and Chief Executive Officer
Elizabeth Thompson, Ph.D.Executive Vice President, Research & Development
Theresa Podrebarac, M.D., M.Sc.Senior Vice President, Clinical Development
Srini Ramanathan, Ph.D.Senior Vice President, Research & Development Sciences
Bill Rees, Ph.D.Vice President, Translational Sciences
Horizon Participants Key Opinion Leaders
Dinesh Khanna, M.D., M.Sc.ProfessorUniversity of Michigan Health
Bobby S. Korn, M.D., Ph.D., FACSProfessor of Ophthalmology & Plastic SurgeryUniversity of California, San Diego
Tina VenturaSenior Vice President, Investor Relations
Kristina Patterson M.D., Ph.D. Medical Director, Neuroimmunology
Martin Kolb, M.D., Ph.D.Director, Division of RespirologyProfessor, Department of Medicine McMaster University

Tim WalbertChairman, President and Chief Executive Officer
Sept. 29, 2021 | Horizon R&D Day | 5

Key Takeaways for Today
(1) Horizon estimate.
We are building a
•
• announced today and starting in 2022
• anticipated in 2021-2023
• in second half of the decade
Horizon is a with best-in-class commercial execution and a rapidly growing pipeline
We are to bolster our ability to continuously innovate
Our current in total peak annual net sales potential(1)

Horizon is One of the Fastest Growth and Transformation Stories in Biotechnology
(1) Midpoint of full-year 2021 net sales guidance as of Aug. 4, 2021. By this presentation Horizon is not updating or confirming its prior guidance.
$297M
2014 2021E
Inflammation Segment Orphan Segment
$3.075B
10x
Net Sales(1)

Strong Track Record of Execution While Increasing R&D Investment
CAGR: Compound annual growth rate. | DD: Double-digit. | EBITDA: Earnings before interest, taxes, depreciation, and amortization. Adjusted EBITDA is a non-GAAP measure; see reconciliations at the end of the presentation for a reconciliation of GAAP to non-GAAP measures. (1) Midpoint of full-year 2021 net sales guidance as of Aug. 4, 2021. By this presentation Horizon is not updating or confirming its prior guidance.
R&D Investment ($M)
2018 2019 2020 2021E
+37% CAGR
$1,208 $1,300
$2,200
$3,075
Inflammation SegmentOrphan Segment
(1) 2018 2019 2020 2021E
$451 $483
$999
$1,280
+42% CAGR
(1)
2018 2019 2020 2021E
$73
6% of sales
$85
7% of sales
$115
5% of sales
Low DD as % of sales
(1)
Adj. EBITDA Growth ($M)Net Sales Growth ($M)

Consistently Delivering Significant Value for Our Shareholders
NBI: NASDAQ Biotechnology Index. Source: Bloomberg. Note: Peer Index is an equally weighted index of ALXN, ALKS, ALNY, BMRN, BLUE, EXEL, INCY, IONS, JAZZ, NBIX, SRPT, SGEN, RARE, UTHR, VRTX; ALXN was acquired Aug. 2021.
$0
$5
$10
$15
$20
$25
Market Cap in $B
$24.9B
-100%
0%
100%
200%
300%
400%
500%HZNP: 487%
NBI: 85%
Peer Index: 67%
Data through Sept. 24, 2021 Data through Sept. 24, 2021
5-Year Shareholder Return Significantly Exceeded NBI and Peer Index
Driving an Eight-Fold Increasein Our Market Cap

Horizon’s Vision
EBITDA: Earnings before interest, taxes, depreciation, and amortization.(1) Horizon’s goals are to achieve strong double-digit net sales growth and EBITDA margin growth for 3-year CAGR [2021 to 2024].
Strategic Goals Financial Goals
A Top-Tier Biotech Company Focused on Researching, Developing and Commercializing
Medicines for Rare, Autoimmune and Severe Inflammatory Diseases
• Maximize value of on-market medicines through commercial execution and clinical investment
• Invest aggressively in our current pipeline medicines
• Expand our pipeline through focused internal innovation and business development
- Expand beyond rare diseases into areas with high unmet need and alignment with Horizon commercial and development strengths
• Build a global presence
• Generate strong double-digit net sales growth(1)
• Generate strong double-digit adjusted EBITDA growth(1)
• Generate meaningful adjusted EBITDA margin expansion
• Maintain R&D investment at double-digits as a percent of sales
• Generate top-tier performance for our shareholders

Excellence in Commercial Execution
We accelerate the growth trajectory and maximize the
potential of our medicines through best-in-class commercial execution
Proven & Disciplined Business Development
We acquire and license medicines through our strong in-house
business development capability, focused on opportunities where
we are uniquely positioned to drive value
Strong Research & Development Capability
We leverage deep drug development experience and an
agile approach to continually innovate with our
existing medicines and bring new ones to market
What Sets Horizon Apart

(1) Full-year 2021 KRYSTEXXA net sales guidance as of Aug. 4, 2021. By this presentation Horizon is not updating or confirming its prior guidance. (2) Horizon estimate.
2015 2021 Peak Annual Net SalesGuidance
>$500M(1)
>$1B(2)
~$60M
HZNPPre-HZNP
>8x
Increasing Annual Net Sales More Than 8x in Five Years Exemplifies Our Industry-Leading Patient-Centric Approach
• KRYSTEXXA was an underperforming and undervalued medicine when acquired in 2016
• We transformed its growth trajectory through strong commercial execution
• We invested in clinical development to drive our immunomodulation strategy;immunomodulation use >40% at 2Q21
• We redefined the market and repositioned KRYSTEXXA as a medicine with >$1B(2) potential and are driving continued growth
KRYSTEXXA: Example of Horizon’s Ability to Drive the Right Strategy and Execute FlawlesslyApproved in 2010; Relaunched by Horizon in 2016

KRYSTEXXA: Significant Opportunity Exists to Exceed $1B in U.S. Annual Peak Net Sales
Uncontrolled gout: Chronic gout refractory (unresponsive) to conventional therapies.(1) Prevalence of gout and hyperuricemia in the U.S. general population: The National Health and Nutrition Examination Survey (NHANES) 2007-2016. Arthritis Rheum. 2019 Jun;71(6):991-999. (2) Approximate number of patients in our annual addressable target market in rheumatology and nephrology; Horizon estimate. (3) Horizon estimate of patients treated in 2020.
9.5MU.S. gout patients; growing low-single digits(1)
>100K uncontrolled
gout patients(2)
• Growth in use of KRYSTEXXA plus immunomodulation
- Improves physician clinical conviction
- Increases patient’s ability to stay on therapy longer
• Growth in new and existing rheumatology accounts
• Accelerating growth in nephrology
Growth Drivers: Objective to Increase Total Patients and Vials Per Patient
<5% penetration(3); significant opportunity exists

TEPEZZA: Another Example of Best-in-Class Commercial Execution; One of the Most Successful Rare Disease Medicine Launches
(1) Full-year 2021 TEPEZZA net sales guidance as of Aug. 4, 2021. By this presentation Horizon is not updating or confirming its prior guidance. (2) Horizon estimate of TEPEZZA peak U.S. annual net sales of >$3B and TEPEZZA ex-U.S. estimate of >$500M peak annual net sales. (3) In the OPTIC Phase 3 confirmatory trial, 83 percent of patients treated with TEPEZZA achieved the primary endpoint of a 2 mm or more reduction in proptosis at week 24. In the OPTIC-X open-label extension trial, 89 percent of OPTIC placebo patients treated with TEPEZZA achieved the primary endpoint of a 2 mm or more reduction in proptosis at week 24.
Initial 2020Guidance
2020 2021E Peak
>$3.5B(2)
>$1.55B(1)
Exceptional Launch and Significant Net Sales Opportunity
$820M
$30M-40M
Growth Drivers: Objective to Drive Continued Strong Uptake and Expand TEPEZZA to More Patients
• TEPEZZA efficacy is impressive at 83-89%; broad indication(3)
• Severity and disfiguring nature of disease a motivating factor for patients to seek treatment
• Pre-launch, launch and new expansion efforts to drive strong awareness and high demand
- High-touch, patient-centric model
- Investing significantly in direct-to-consumer campaigns

TEPEZZA: Significant Opportunity Exists to Exceed $3.5B in Global Annual Peak Net Sales
TED: Thyroid Eye Disease. (1) Horizon estimate.
More Than $500M Opportunity Outside the U.S. and Europe(1)
• Continuing to advance our clinical program in Japan
• ~3K-5K: Estimated addressable annual patient incidence of acute TED in Japan(1)
• Evaluating launch in several additional countries
More Than $3B Opportunity in the U.S.;Significant Opportunity Exists(1)
• ~15-20K patients: Estimated U.S. annual incidence of acute moderate to severe TED patients (1)
- Acute TED lasts one to three years
• >70K patients: Estimated U.S. prevalence of chronic TED patients(1)
- Symptoms no longer changing but persisting; typically includes patients who have had chronic TED for five years or less

UPLIZNA through Focused Commercial Execution
the Value of UPLIZNA through Collaborative and Clinical Research
UPLIZNABeginning with Europe
• Invest in sales and marketing organization to expand reach and share of voice
• Establish best-in-class patient services, site of care and payer support
• Raise awareness of the benefits of UPLIZNA versus other therapies
• Invest in medical and scientific engagement;establish scientific leadership
• Conduct further analysis of UPLIZNA NMOSD data to expand understanding of differentiation
• Continue to build base of compelling real-world evidence
• Building out European infrastructure to support the potential launch of UPLIZNA for NMOSD
• Adding key capabilities to support UPLIZNA as well as additional medicines
UPLIZNA: Applying Our Success with KRYSTEXXA and TEPEZZA to Relaunch UPLIZNA for NMOSD
NMOSD: Neuromyelitis optica spectrum disorder.

Business Development is a Critical Part of Our Strategy to Build a Robust Pipeline
(1) As of June 30, 2021, cash and cash equivalents were $812.3M, gross debt was $2.614B and the gross debt-to-last-12-months adjusted EBITDA leverage ratio was 2.3x. Adjusted EBITDA is a non-GAAP measure; see reconciliations at the end of the presentation for a reconciliation of GAAP to non-GAAP measures.
Expanding our presence beyond rare diseases
• Autoimmune and severe inflammatory diseases
• Open to larger patient populations
Maintaining strong focus in rare diseases with significant unmet need
Balancing across early to late-stage programs
• E.g., preclinical, clinical, platform technologies
Increasing research-based partnerships and collaborations
• Focused; supported by sound rationale and compelling data
Strong financial position provides flexibility to pursue future business development opportunities(1)

Acquisition Cost Net Sales Achieved Through 2021
Business Development: Strong Track Record Based on a Disciplined Approach and Smart Commercial Perspective
(1) KRYSTEXXA net sales from 2016 through 2021; net sales in 2021 based on Horizon guidance of >$500M as of Aug. 4, 2021. (2) Does not include milestone payments or royalties. (3) Assumes net sales in 2021 based on Horizon guidance of >$1.55B as of Aug. 4, 2021. By this presentation Horizon is not updating or confirming its prior guidance.
>$1.755B(1)
$510M
3x
KRYSTEXXA: Total Net Sales Achieved to Date is Already More Than 3x the Acquisition Cost
Upfront Payment Net Sales Achieved Through 2021
>$2.37B(3)
$145M(2)
16x
TEPEZZA: Total Net Sales Achieved to Date is Already More Than 16x the Upfront Acquisition Cost

Leveraging our combined unique strengths
to make Horizon an even stronger, high-growth,
profitable biotech with the ability to continuously innovate
Horizon: A Leading Biotech
Bringing additional treatments to patients across a wide range of rare, autoimmune and severe inflammatory diseases
Talented R&D team with early-stage research, clinical development
capabilities and a deep, mid-stage biologics
pipeline
Experienced team with proven track record of
late-stage development and commercial expertise
to maximize value of pipeline and on-market medicines
Acquisition of Viela Significantly Expanded the Horizon Pipeline and R&D Talent

Pipeline Added deep, mid-stage biologics pipeline with four candidates now in 13 development programs
Target AreasAdvanced Horizon’s position in rare diseases and key therapeutic areas (i.e., rheumatology, nephrology), including UPLIZNA, a biologic medicine for the rare autoimmune disease NMOSD
Innovation Platform
Added early-stage research and translational capabilities that enhance Horizon’s ability to continuously innovate
R&D TalentEnhanced our accomplished R&D team adding deep scientific knowledge of autoimmune and severe inflammatory diseases
Leadership Position
Advanced Horizon’s position as a leading profitable biotech company by meaningfully adding pipeline breadth, depth and R&D investment to levels approaching profitable biotech peers
How Viela Advanced Horizon’s Transformation
NMOSD: Neuromyelitis Optica Spectrum Disorder.

Phase 2 Preclinical Phase 4
KRYSTEXXA(PROTECT Trial)
Phase 1
TEPEZZA(3)
(Diffuse Cutaneous Systemic Sclerosis)
HemoShear(2)
(Gout)
KRYSTEXXA(MIRROR: Immunomodulation)
HZN-003(Uncontrolled Gout)
HZN-007(1)
(Uncontrolled Gout)
2019 R&D Pipeline
MIRROR: Immunomodulation program evaluating the use of KRYSTEXXA in combination with methotrexate to increase response rate. PROTECT: Clinical trial evaluating the effect of KRYSTEXXA on serum uric acid levels in kidney transplant patients with uncontrolled gout.(1) Being developed under a collaboration agreement with XL Protein GmbH. (2) Gout discovery program in partnership with HemoShear. (3) Exploratory study.
Phase 3
TEPEZZA(Thyroid Eye Disease)

Preclinical
HemoShear(2)
(Gout)
HZN-003(Uncontrolled Gout)
HZN-007(1)
(Uncontrolled Gout)
Phase 3
UPLIZNA(Myasthenia Gravis)
UPLIZNA(IgG4-Related Disease)
Phase 2
UPLIZNA(Kidney Transplant Desensitization)
HZN-825(Diffuse Cutaneous Systemic Sclerosis)
Daxdilimab (HZN-7734)(Systemic Lupus Erythematosus)
HZN-825(Interstitial Lung Diseases)
Dazodalibep (HZN-4920 )(Rheumatoid Arthritis)
Dazodalibep (HZN-4920)(Sjögren’s Syndrome)
Dazodalibep (HZN-4920)(Kidney Transplant Rejection)
Horizon
Viela
Phase 1
TEPEZZA(3)
(Subcutaneous Administration)
TEPEZZA(4)
(Diffuse Cutaneous Systemic Sclerosis)
Daxdilimab (HZN-7734)(COVID-19 Acute Lung Injury)
HZN-1116(Autoimmune Diseases)
Phase 4
KRYSTEXXA(Shorter Infusion Duration)
TEPEZZA(Chronic Thyroid Eye Disease)
KRYSTEXXA(PROTECT Trial)
KRYSTEXXA(MIRROR: Immunomodulation)
KRYSTEXXA(Retreatment)
KRYSTEXXA(Monthly Dosing)
TEPEZZA(Chronic Thyroid Eye Disease)
TEPEZZA(OPTIC-X: Phase 3 Extension Trial)
2021 R&D Pipeline – March 2021Viela Added Significant Breadth and Depth to Horizon’s Pipeline
MIRROR: Immunomodulation program evaluating the use of KRYSTEXXA in combination with methotrexate to increase response rate. | PROTECT: Clinical trial evaluating the effect of KRYSTEXXA on serum uric acid levels in kidney transplant patients with uncontrolled gout. | OPTIC-X: Open-label extension trial of the Phase 3 trial evaluating TEPEZZA for the treatment of Thyroid Eye Disease. | IgG4: Immunoglobulin G4. (1) Being developed under a collaboration agreement with XL Protein GmbH. (2) Gout discovery program in partnership with HemoShear. (3) Including collaboration agreement with Halozyme. (4) Exploratory study.

Preclinical Phase 4
KRYSTEXXA(Shorter Infusion Duration)
TEPEZZA(Chronic Thyroid Eye Disease)
KRYSTEXXA(PROTECT Trial)
HemoShear(2)
(Gout)
KRYSTEXXA(MIRROR: Immunomodulation)
HZN-003(Uncontrolled Gout)
HZN-007(1)
(Uncontrolled Gout)
Phase 3
UPLIZNA(Myasthenia Gravis)
UPLIZNA(IgG4-Related Disease)
KRYSTEXXA(Retreatment)
KRYSTEXXA(Monthly Dosing)
ARO-XDH(Uncontrolled Gout)
2021 R&D Pipeline – September 2021Six New Programs for a Total of 27 Programs
MIRROR: Immunomodulation program evaluating the use of KRYSTEXXA in combination with methotrexate to increase response rate. | PROTECT: Clinical trial evaluating the effect of KRYSTEXXA on serum uric acid levels in kidney transplant patients with uncontrolled gout. | IgG4: Immunoglobulin G4.(1) Being developed under a collaboration agreement with XL Protein GmbH. (2) Gout discovery program in partnership with HemoShear. (3) Including collaboration agreement with Halozyme. (4) Exploratory study.
Phase 2
UPLIZNA(Kidney Transplant Desensitization)
Daxdilimab (HZN-7734)(Discoid Lupus Erythematosus)
HZN-825(Diffuse Cutaneous Systemic Sclerosis)
Daxdilimab (HZN-7734)(Systemic Lupus Erythematosus)
Daxdilimab (HZN-7734)(Alopecia Areata)
Daxdilimab (HZN-7734)(Lupus Nephritis)
HZN-825(Interstitial Lung Diseases)
Dazodalibep (HZN-4920)(Rheumatoid Arthritis)
Daxdilimab (HZN-7734)(Dermatomyositis)
Dazodalibep (HZN-4920)(Sjögren’s Syndrome)
Dazodalibep (HZN-4920)(Kidney Transplant Rejection)
Dazodalibep (HZN-4920)(Focal Segmental Glomerulosclerosis)
Existing Indications/ Programs
New Indications/ Programs
Phase 1
TEPEZZA(3)
(Subcutaneous Administration)
TEPEZZA(4)
(Diffuse Cutaneous Systemic Sclerosis)
HZN-1116(Autoimmune Diseases)
TEPEZZA(Chronic Thyroid Eye Disease)

2021 Net Sales Potential Peak Net Sales of Growth Drivers and Pipeline Medicines
$3.075B(2)
TEPEZZA
KRYSTEXXA
UPLIZNA
Daxdilimab (HZN-7734)
Dazodalibep (HZN-4920)
HZN-825
ARO-XDH
KRYSTEXXA
Other Medicines
UPLIZNA
Significant Future Potential Driven by Seven Potential Blockbuster Medicines(1)
(1) Blockbuster defined as medicine with >$1B in estimated potential peak net sales. (2) Midpoint of full-year 2021 net sales guidance as of Aug. 4, 2021. By this presentation Horizon is not updating or confirming its prior guidance. (3) Horizon estimates. Assumes each development program successfully completes clinical development, attains regulatory approval for Horizon's intended indications and is successfully commercialized.
~$10B(3)
TEPEZZA

Elizabeth Thompson, Ph.D.EVP, Research & Development
Sept. 29, 2021 | Horizon R&D Day | 25

R&D Strategy: Building and Expanding Our Pipeline by Broadening Our Ambitions
Foundational Element
Building for the Future
Maximize potential of on-market medicines (e.g., KRYSTEXXA immunomodulation)
Expand our pipeline through business development
Add top talent to R&D function
Maximize pipeline molecules (e.g., five indications for daxdilimab (HZN-7734))
Expand pipeline through earlier-stage partnerships and collaborations
Build research capabilities to generate discovery stage candidates
Expand therapeutic areas of focus to build on established areas of expertise
Significantly Increasing R&D Investment

Theresa Podrebarac, M.D. , M.Sc., Senior Vice President, Clinical Development
• 20+ years clinical development and strategy
• Dr. Podrebarac joined Horizon in early 2021 where she leads the clinical development function
• Prior to Horizon, she served as CMO for two biotech companies. She also served as VP, immunology clinical development for AbbVie, Biogen and EMD Serono leading to several approved therapies
Elizabeth H. Z. Thompson, Ph.D., Executive Vice President, Research and Development
• 20+ years of experience leading the development of multiple novel medicines in the United States and globally
• In her time at Horizon, Dr. Thompson led the expedited filing and approval of TEPEZZA and its successful FDA Advisory Committee meeting
• Prior to Horizon, Dr. Thompson was the clinical lead for SKYRIZI at AbbVie. She also has had a career spanning clinical development, business development and medical communications and has worked at Raptor, InterMune and Amgen
We Have an Experienced R&D Leadership Team
Srini Ramanathan, Ph.D., Senior Vice President, Research and Development Sciences
• 20+ years spanning research and drug development, contributing to 10 new drug approvals
• At Horizon, Dr. Ramanathan leads discovery research, translational sciences and biometrics, and led the scientific discussion at the FDA Advisory Committee meeting and supported the approval of TEPEZZA
• Prior to Horizon, led multiple immunology programs at AbbVie and was global head of clinical pharmacology at Gilead
Melanie Gloria, Senior Vice President, Development Operations
• 20+ years of experience leading operations functions across research and development
• At Horizon, Melanie leads Clinical Operations, Regulatory, Project Management and Pharmacovigilance
• Prior to Horizon, Melanie worked at AbbVie and Abbott. Melanie supported the development programs across the Immunology, Oncology, Women’s Health, and Virology Therapeutic areas
Eliezer Katz, M.D. FACS• Vice President,
Clinical Development • Previously worked at Viela Bio,
MedImmune, Pfizer, CTI Clinical Trial and Consulting Services and University of Massachusetts
Betsy O’Neill, Ph.D.• Vice President, External
Research and Development• Previously worked at BioMarin,
Elan Pharmaceuticals and Tularik
Lisa Pitt, PharmD, M.S.J.• Vice President, Regulatory Affairs• Previously worked at Viela Bio,
Premier Research, FDA, MedImmune, Parexel and Novartis
Bill Rees, Ph.D. • Vice President,
Translational Sciences• Previously worked at Viela
Bio, MedImmune, Amgen and Corixa
Gábor Illei, M.D. • Vice President, Clinical
Development• Previously worked at Viela Bio,
REGENXBIO Inc., MedImmune andNational Institutes of Health
Dewei She, Ph.D.• Vice President, Biometrics• Previously worked at Viela Bio,
MedImmune/AstraZeneca, The EMMES Corporation, Orchid Biosciences, The Degge Group

San Francisco, CA
Deerfield, IL
Rockville, MD
Waterford, Ireland
Dublin, Ireland
Global R&D Presence in Locations to Build and Attract Top TalentNearly Quadrupled R&D Organization Since 2018

MIRROR: Randomized, placebo-controlled trial underway evaluating KRYSTEXXA plus immunomodulator MTX
• Primary and secondary endpoint results after trial completes, expected Q4 2021
• Expect to submit sBLA in 1H 2022
ImproveResponse Rate
Shorter infusion duration (AGILE): Open-label trial underwayevaluating KRYSTEXXA plus MTX at shorter durations (current duration is 2+ hours)
Improve Patient Experience
Monthly dosing (FORWARD): Open-label trial underway to evaluate 16mg monthly dosing of KRYSTEXXA plus MTX (current dosing is 8mg 2x/month)
PROTECT: Open-label trial underway evaluating KRYSTEXXA for uncontrolled gout in kidney transplant patients (most severe)
Demonstrate Benefit in Broader
Populations
Retreatment (ADVANCE): Open-label trial underway to evaluate KRYSTEXXA plus MTX in patients who have previously failed KRYSTEXXA alone
Maximizing the Long-Term Potential of KRYSTEXXA Five Trials Underway
MTX: Methotrexate. | sBLA: Supplemental Biologics License Application.

• Randomized, placebo-controlled trial of TEPEZZA underway in chronic TED patients
• Objective is to generate data supporting TEPEZZA adoption in the already indicated chronic TED patient population
Chronic Disease Subcutaneous Administration Diffuse Cutaneous Systemic Sclerosis
• Pharmacokinetic trial underway to explore subcutaneous TEPEZZA dosing
• Objective is to assess the potential for additional administration options for TEPEZZA
• Partnered with Halozyme to leverage proprietary ENHANZE® drug delivery technology
• Exploratory study to investigate the safety, tolerability and effect on IGF-1/IGF-1R inflammatory/fibrotic biomarkers
• Preclinical data implicate IGF-1/IGF-1R signaling in diffuse cutaneous systemic sclerosis pathology
• Expect to initiate Phase 1 trial in Q4 2021
Thyroid Eye Disease (TED) Programs Maximizing the Future and Long-Term Potential
of TEPEZZA for TED Patients
Potential Additional IndicationHigh Unmet Need in a Rare, Chronic
Autoimmune Disease; Core Therapeutic Area
Maximizing the Long-Term Potential of TEPEZZAAdvancing Three R&D Programs
IGF-1R: Insulin-like growth factor 1 receptor.

Expanding Our Pipeline: How We Think About Choosing New Indications
Unmet Need /Patient Perspective
Competitive Landscape
Scientific Rationale
Feasibility
Horizon Focus

KRYSTEXXA Combination with Immunomodulation in Uncontrolled Gout(1)
UPLIZNA
Myasthenia Gravis (MG)
IgG4-Related Disease (IgG4-RD)
Kidney Transplant Desensitization
HZN-825Diffuse Cutaneous Systemic Sclerosis (dcSSc)(3)
Idiopathic Pulmonary Fibrosis (IPF)(3)
Daxdilimab (HZN-7734)
Systemic Lupus Erythematosus (SLE)
Alopecia Areata (AA)(3)
Discoid Lupus Erythematosus (DLE)(3)
Lupus Nephritis (LN)(3)
Dermatomyositis (DM)(3)
Dazodalibep (HZN-4920)
Sjögren’s Syndrome
Rheumatoid Arthritis
Kidney Transplant Rejection
Focal Segmental Glomerulosclerosis (FSGS)(3)
TEPEZZASubcutaneous Administration
Diffuse Cutaneous Systemic Sclerosis (dcSSc)(3)
HZN-1116 Autoimmune Diseases
ARO-XDH
Next-Gen Uncontrolled GoutHZN-003
HZN-007
HemoShear Novel Gout Targets
Program Potential Indication
New programs announced today
Ongoing programs
Horizon Pipeline Today: 27 Programs; Five New Indications Announced Today
Preclinical Phase 1 Phase 2 Phase 3
• 27 programs in total(2)
• Five new programs announced today and starting in 2022
• 10 data readouts anticipated in 2021-2023
• 10 potential approvals in second half of the decade
IgG4: Immunoglobulin G4. (1) KRYSTEXXA MIRROR trial is a Phase 4 trial. (2) There are five additional Phase 4 programs included in our pipeline, but not shown here. (3) Planned programs; not yet initiated.

KRYSTEXXA Combination with Immunomodulation in Uncontrolled Gout(1)
UPLIZNA
Myasthenia Gravis (MG)
IgG4-Related Disease (IgG4-RD)
Kidney Transplant Desensitization
HZN-825Diffuse Cutaneous Systemic Sclerosis (dcSSc)(3)
Idiopathic Pulmonary Fibrosis (IPF)(3)
Daxdilimab (HZN-7734)
Systemic Lupus Erythematosus (SLE)
Alopecia Areata (AA)(3)
Discoid Lupus Erythematosus (DLE)(3)
Lupus Nephritis (LN)(3)
Dermatomyositis (DM)(3)
Dazodalibep (HZN-4920)
Sjögren’s Syndrome
Rheumatoid Arthritis
Kidney Transplant Rejection
Focal Segmental Glomerulosclerosis (FSGS)(3)
TEPEZZASubcutaneous Administration
Diffuse Cutaneous Systemic Sclerosis (dcSSc)(3)
HZN-1116 Autoimmune Diseases
ARO-XDH
Next-Gen Uncontrolled GoutHZN-003
HZN-007
HemoShear Novel Gout Targets
Program Potential Indication
New programs announced today
Ongoing programs
Horizon Pipeline: Our Programs We Will Discuss Today
Preclinical Phase 1 Phase 2 Phase 3
• 27 programs in total(2)
• Five new programs announced today and starting in 2022
• 10 data readouts anticipated in 2021-2023
• 10 potential approvals in second half of the decade
IgG4: Immunoglobulin G4. (1) KRYSTEXXA MIRROR trial is a Phase 4 trial. (2) There are five additional Phase 4 programs included in our pipeline, but not shown here. (3) Planned programs; not yet initiated.
• 27 programs in total(2)
• 5 new programs announced today and starting in 2022
• 6 data readouts anticipated in 2021-2023
• 9 potential approvals in second half of the decade
Daxdilimab (HZN-7734)
• SLE• AA• DLE• LN• DM
Dazodalibep (HZN-4920)
• Sjogren’s Syndrome• FSGS
HZN-825
• dcSSc• IPF
UPLIZNA
• MG• IgG4-RD
TEPEZZA
• Chronic TED

Core Therapeutic Areas Areas of Expansion
We Have Meaningfully Expanded Our Therapeutic Areas of Focus
SLE: Systemic Lupus Erythematosus. | AA: Alopecia Areata. | DLE: Discoid Lupus Erythematosus. | DM: Dermatomyositis. | FSGS: Focal Segmental Glomerulosclerosis. | SC: subcutaneous. | IPF: Idiopathic pulmonary fibrosis. | IgG4: Immunoglobulin G4.dcSSc: Diffuse cutaneous systemic sclerosis. | ILD: Interstitial lung diseases. | MG: Myasthenia Gravis.
RheumatologyDeep knowledge and expertise,
market leader in gout; clinical programs:
KRYSTEXXA MIRROR, daxdilimab
(HZN-7734) in SLE and dazodalibep
(HZN-4920) in Sjögren’s Syndrome
NephrologyGrowing presence with KRYSTEXXA;
clinical programs: KRYSTEXXA PROTECT,
dazodalibep (HZN-4920) in kidney
transplant rejection and FSGS
Growing capabilities in ophthalmology, ophthalmology subspecialists
and endocrinology as a pioneer in Thyroid Eye Disease (TED);
clinical programs: TEPEZZA Chronic TED, TEPEZZA SC
Ophthalmology Endocrinology
NeuroimmunologyDeep research and translational
capabilities, academic collaborations
and protein engineering expertise;
clinical programs: UPLIZNA in MG and
IgG4-related disease
RespiratoryFocused investments in areas that fit our research strategy (e.g., ILDs a
large area with high unmet need and mechanistic rationale supports
evaluation); clinical programs: HZN-825 in IPF and dcSSc
DermatologyGrowing field with high unmet need;
immune dysfunction and fibrosis central
to many diseases; clinical programs:
daxdilimab (HZN-7734) in AA, DLE and DM

Earlier-Stage Innovation is Critical for Building a Sustainable and Diversified Pipeline
Internal research to generate innovation in core areas of expertise
Externalcollaborations and business development
to access promising innovation

SVP, Research & Development Sciences
Srini Ramanathan, Ph.D.
Sept. 29, 2021 | Horizon R&D Day | 36

Building a Robust Research Organization and Discovery Engine to Drive Long-Term Growth
IND: Investigational New Drug. | IP: Intellectual property.
Building an internal engine to begin to generate high-quality INDs over the next few years
Balanced between internal and external opportunities
Aligned with our therapeutic areas of focus
Focused on matching the right modality to scientific / patient
needs
Built by growing our talented research team and capabilities
Projects Driven by Horizon Research
Areas where Horizon has internal capabilities, insights and IP that make it best equipped to deliver
Projects Driven by External Partnerships
• Seek out specific partners with unique capabilities and expertise that can translate Horizon’s technical vision
• Form collaborations with high-value transformational potential and improved likelihood of success

Example of How Our Research and Translational Teams Partner with Business Development to Build a Next-Generation Gout Franchise
sUA: Serum Uric Acid. | RNAi: Ribonucleic acid interference. (1) Approximate number of patients in addressable target market; Horizon estimates.
• Using RNAi, ability to silence the gene associated with high sUA
• Subcutaneously administered medicine candidate
• Using cell-based models of gout; identified and validated two novel targets for reducing uric acid
• Orally administered medicine candidates• Starting with KRYSTEXXA, built leadership
position in gout
• Built deep expertise via best-in-class commercial and clinical teams
• Realized unmet need for >500K(1) patients who do not respond to standard of care or are not candidates for KRYSTEXXA
Horizon Sought Out External Collaborations to Fill this Unmet Need
As a leader in gout, Horizon is uniquely positioned to successfully develop and
commercialize candidates that result from these programs

CD40/CD40LCo-stimulatory
Pathway
CD40L
T cell
Dazodalibep(HZN-4920)
Plasmablast
Plasma cells
CD19
CD19
Viela Clinical Approach: Focused on Three Biological Pathways Shared Across Various Diseases
CD19: Cluster of Differentiation 19. | CD40: Cluster of Differentiation 40. | CD40L: Cluster of differentiation 40 Ligand. IFNα: Interferon-α. | IL6: Interleukin 6. | ILT7: Immunoglobulin-Like Transcript 7. | mDC: Myeloid Dendritic Cell. MO: Monocytes. | pDC: Plasmacytoid Dendritic Cell | TNF: Tumor Necrosis Factor.
Innate Immunity Pathway
pDC
ILT7
IL-6
TNF
IFNα
Inflammatorymediators
Daxdilimab(HZN-7734)
Tissue Damage,Inflammation and
Fibrosis
Autoimmunity
CD40
B-cell/Autoantibody Pathway
UPLIZNA
CD19
B cell

Daxdilimab (HZN-7734) First and Only pDC Depleter in Clinical Development; Now Pursuing Five Indications
Sept. 29, 2021 | Horizon R&D Day | 40
Theresa Podrebarac, M.D., M.Sc., SVP Clinical Development
Bill Rees, Ph.D., VP Translational Sciences

Daxdilimab is an anti-ILT7 fully human monoclonal antibody with a
Plasmacytoid dendritic cells across many autoimmune and inflammatory diseases
provide clear rationale to pursue daxdilimab in multiple diseases
Systemic lupus erythematosus (SLE) is the first indication in development, which in cutaneous lupus erythematosus (CLE)
Today, we are announcing as part of our strategy to fully realize its potential
ILT7: Immunoglobulin-like transcript 7.
Daxdilimab (HZN-7734) Key TakeawaysFirst and Only pDC Depleter in Clinical Development; Now Pursuing Five Indications

• In healthy individuals, pDCs are present in low numbers, driving an appropriate immune response to fight infection
• In individuals with certain autoimmune diseases, pDCs are found in high concentrations in target tissue, which results in significant inflammation and tissue damage that are a hallmark of autoimmune disease
• Daxdilimab was designed to be an efficient pDC depleter, targeting a main driver of inflammation without impairing the body’s overall antiviral response
What are pDCs and Why are They Important in Autoimmune Diseases?
ILT7: Immunoglobulin-like transcript 7.
pDCs, Inflammation and Autoimmune Disease
Immune complexes containing nucleic acids bind to pDC
Production of inflammatory molecules
PlasmacytoidDendritic Cell (pDC)
Daxdilimab binds to ILT7

pDCs Play a Critical Role in Driving Inflammation; Daxdilimab (HZN-7734) Directly Targets pDCs
pDCs: Plasmacytoid Dendritic Cells.

DaxdilimabControl H 4 Control H 4Control
Preclinical Evidence Demonstrated Daxdilimab (HZN-7734) is an Efficient Depleter of pDCs with a Similar Impact on Type 1 Interferon
IFN: Interferon. | PBMC: Peripheral blood mononuclear cell. | pDC: Plasmacytoid Dendritic Cell.Source: Karnell et al (2021) Sci Transl Med, 13(595), 14.
Daxdilimab Had a Similar Impact on Type 1 InterferonDaxdilimab Efficiently Depleted pDCs
Study Day
pD
Cs
(pe
r m
illio
n P
BM
Cs)
Pre-dose Dosing Sustained Effect
Study Day
IFN
α (
pg
/ml)
Pre-dose Dosing Sustained Effect

Clinical Evidence Demonstrated Daxdilimab (HZN-7734) Efficiently Depleted Circulating pDCs
Arrows represent when dosing occurred. | pDC: Plasmacytoid Dendritic Cell. | BL: Baseline. | PBMC: Peripheral blood mononuclear cell.Source: Karnell et al (2021) Sci Transl Med, 13(595), 14.
Rates of adverse events were similar between daxdilimab and placebo
Daxdilimab Rapidly Depleted pDCs and Had a Sustained Effect
Dosing Sustained Effect%
pD
Cs
(of
PB
MC
s)
Study Day
Daxdilimab 50 mg (n=8) lacebo H 4, 0 mg H 4, 1 0 mgPlacebo (n=9)Daxdilimab 150 mg (n=8) lacebo H 4, 0 mg H 4, 1 0 mg

pDCs are Important Drivers of Disease Across Multiple Autoimmune and Inflammatory Diseases
pDC: Plasmacytoid Dendritic Cell.
Systemic autoimmune diseases
Autoimmune kidney diseases
Autoimmune skin diseases
Other inflammatory diseases

Clinical Evidence in Cutaneous Lupus Erythematosus (CLE) Patients Showed that Daxdilimab (HZN-7734) Reduced pDCs and Type 1 Interferon Activity in Target Tissue Based on Skin Biopsies
pDC: Plasmacytoid Dendritic Cell. | IFN: Interferon.Source: Karnell et al (2021) Sci Transl Med, 13(595), 14.
Skin biopsies shown above
Day
85
Bas
elin
e
pDCs IFN response protein
98% Reduction of Skin pDCs with DaxdilimabDaxdilimab Profoundly Reduced pDCs and
Type 1 Interferon in the Skin
% c
han
ge f
rom
Bas
elin
e t
o D
ay 8
5 (
skin
pD
Cs)
Placebo(n=6)
Daxdilimab(n=16)

Daxdilimab (HZN-7734) Demonstrated a Dose Dependent Improvement in Cutaneous Lupus
CLASI-A: Cutaneous Lupus Erythematosus Area and Severity Index-Activity. | BL: Baseline.Source: Karnell et al (2021) Sci Transl Med, 13(595), 14.
Treatment with Daxdilimab Resulted in Clinically Significant Reduction in Skin
Disease Activity
Higher % of Daxdilimab Patients Achieved ≥7 Point Reduction in CLASI-A
vs. Placebo
% C
han
ge f
rom
BL:
CLA
SI-A
Sco
re
% ≥
7-p
oin
t re
du
ctio
n in
CLA
SI-A
Study Day
Higher % of Daxdilimab Patients Achieved ≥50% Reduction in CLASI-A vs.
Placebo
% w
ith
≥5
0%
re
du
ctio
n in
CLA
SI-A
Time (days) Time (days)
Daxdilimab 50 mg (n=8)
(Last Dose)
Daxdilimab 150 mg (n=8) lacebo H 4, 0 mg H 4, 1 0 mg Placebo (n=9) lacebo H 4, 0 mg H 4, 1 0 mg

Daxdilimab (HZN-7734) Phase 2 Trial in Systemic Lupus Erythematosus (SLE) Initiated in June 2021
CLASI-A: Cutaneous Lupus Erythematosus Area and Severity Index-Activity. | LLDAS: Lupus Low Disease Activity State. | PD: Pharmacodynamic(s). | PK: Pharmacokinetic(s). | SRI: SLE Responder Index. | SubQ: Subcutaneous.(1) Defined as oral glucocorticoid (OGC) dose ≤ . mg/day and ≤ Baseline (Day 1) dose of prednisone or equivalent at Week 48.
• proportion of participants achieving a BILAG 2004 Index-based Combined Lupus Assessment (BICLA) response and a reduction in glucocorticoid use(1)
• CLASI-A score at Week 12, SRI-4, LLDAS, sustained steroid reduction, PK/PD, safety and tolerability
Key Inclusion Criteria
• Adults aged ≥ 18 to ≤ 0 years
• Moderate to Severely Active SLE as Defined By: - SLE Disease Activity Index 2000 (SLEDAI-2K)- British Isles Lupus Assessment Group (BILAG) 2004 Index- Physician Global Assessment (PGA)
Phase 2 Trial Design in SLE
Safety Follow-Up
19
5 p
atie
nts
1:1
:1 r
an
do
miz
ati
on
Cohort 1: Daxdilimab 200 mgSubQ Monthly Dosing
Cohort 2: Daxdilimab 200 mgSubQ Dosing Every 12 Weeks + additional 200 mg SubQ at Week 4
PlaceboSubQ Monthly Dosing
Study Week 0
Week 48Primary Endpoint
Week 56Safety Follow-Up

Evaluating Five Indications for Daxdilimab (HZN-7734) where pDCs are Implicated
pDC: Plasmacytoid Dendritic Cell. | IFN: Interferon. (1) Horizon estimate. (2) Werth et al. Arthritis Rheum (2020) 72 (suppl 10). (3) Furie et al. 2020 ACR Annual Meeting. (4) Rahal et al. JEADV (2014) 30(1): 119-123. (5) Ito et. al. Allergology International (2020) 69(1): 121-131. (6) Vermi et. al. Immunobiology (2009) 214: 877–886. (7) Rakhshan et al. An Bras Dermatol. 2020; 95(3): 307-13. (8) Braunstein et al. Br J. Dermatol (2012) 166(5): 971-5. (9) Fiore et al. Mol Immunology (2008) 45: 259–265. (10) Kassianos et al. Am J Physiol. (2013) 305, F1391–F1401. (11) Shimizu et al. Mod Rheum (2018) 28: 661-669. (12) Greenberg et al. Ann Neurol (2005) 57(5):664-678. (13) McNiff et al. J Cutan Pathol (2008) 35: 452-456. (14) Greenberg et al. Arth Res Ther (2010) 12:S4.
Indications Being Pursued
Scientific Rationale
Unmet Need / Competitive Landscape
U.S. Patient Population(1)
Alopecia Areata (AA)
• pDCs detected in AA lesions and Type 1 interferon signatures are elevated in AA lesions(4)
• Preclinical models implicate pDCs in AA(5)
• Treated with off label medicines, subject to significant side effects, variable efficacy
• High rate of relapse (~85%) and need for fast, robust results
>600K patients of which ~40K would be appropriate for novel
therapies including biologics
Discoid Lupus Erythematosus (DLE)
• pDCs reported to be abundant in DLE skin lesions(6-7)
• Significantly elevated Type 1 interferon activity in DLE compared to healthy tissue(8)
• High disease burden• Current standard of care not uniformly effective and is
associated with potential side effects
~30K patients would be appropriate for novel
therapies including biologics
Lupus Nephritis (LN)
• Presence of pDCs is associated with more advanced disease in LN(9-10)
• Evidence of interferon activity in renal tissue in LN(11)
• High disease burden• May progress to kidney failure• Standard of care associated with potentially dangerous side
effects
~60K patients would be appropriate for novel
therapies including biologics
Dermatomyositis (DM)
• pDCs reported to be abundant in DM muscle(12-13)
• Increased Type 1 interferon activity in DM and interferon signature is correlated with disease severity(14)
• High disease burden• Treated with off label medicines, subject to significant side
effects, variable efficacy
~35K patients would be appropriate for novel
therapies including biologics
Indications for Which Clinical Trials are Underway
Scientific Rationale
Unmet Need / Competitive Landscape
U.S. Patient Population(1)
Systemic Lupus Erythematosus (SLE)
• Early-stage clinical studies show benefit of targeting pDCs(2-3)
• Many patients have uncontrolled disease activity with available treatment options leading to increased morbidity and mortality
• Approved medicine, but not highly effective
~250-350K patients of which ~50K would be appropriate for
novel therapies including biologics

• AA: an autoimmune disorder characterized by nonscarring hair loss
• Next steps: Phase 2 trial expected to start in 1H 2022
Alopecia Areata (AA)
Five Phase 2 Trials for Daxdilimab (HZN-7734); Initiating Trials in Four New Indications in 2022
• DM: autoimmune, inflammatory disorder characterized by rashes that often burn and debilitating muscle weakness
• Next steps: Phase 2 trial expected to start in 2H 2022
Dermatomyositis (DM)
• SLE: an autoimmune disease that manifests as skin rashes, arthritis, nephritis, and serositis
• Next steps: Phase 2 trial underway, with first patient enrolled in June 2021
Systemic Lupus Erythematosus (SLE)
• LN: an autoimmune, inflammatory condition of the kidney; efficacy in LN may increase adoption of daxidilimab in SLE patients
• Next steps: Phase 2 trial expected to start in 2H 2022
Lupus Nephritis (LN)
• DLE: chronic, inflammatory skin condition characterized by sores that can result in scarring
• Next steps: Phase 2 trial expected to start in 1H 2022
Discoid Lupus Erythematosus (DLE)

Daxdilimab is an anti-ILT7 fully human monoclonal antibody with a
Plasmacytoid dendritic cells across many autoimmune and inflammatory diseases
provide clear rationale to pursue daxdilimab in multiple diseases
Systemic lupus erythematosus (SLE) is the first indication in development, which in cutaneous lupus erythematosus (CLE)
Today, we are announcing as part of our strategy to fully realize its potential
Daxdilimab (HZN-7734) Key TakeawaysFirst and Only pDC Depleter in Clinical Development; Now Pursuing Five Indications
ILT7: Immunoglobulin-like transcript 7.

Dazodalibep (HZN-4920) CD40L Antagonist Designed to Block a Central Pathway Involved in Many Autoimmune and Inflammatory Diseases
Sept. 29, 2021 | Horizon R&D Day | 53
Theresa Podrebarac, M.D., M.Sc., SVP Clinical Development
Bill Rees, Ph.D., VP Translational Sciences
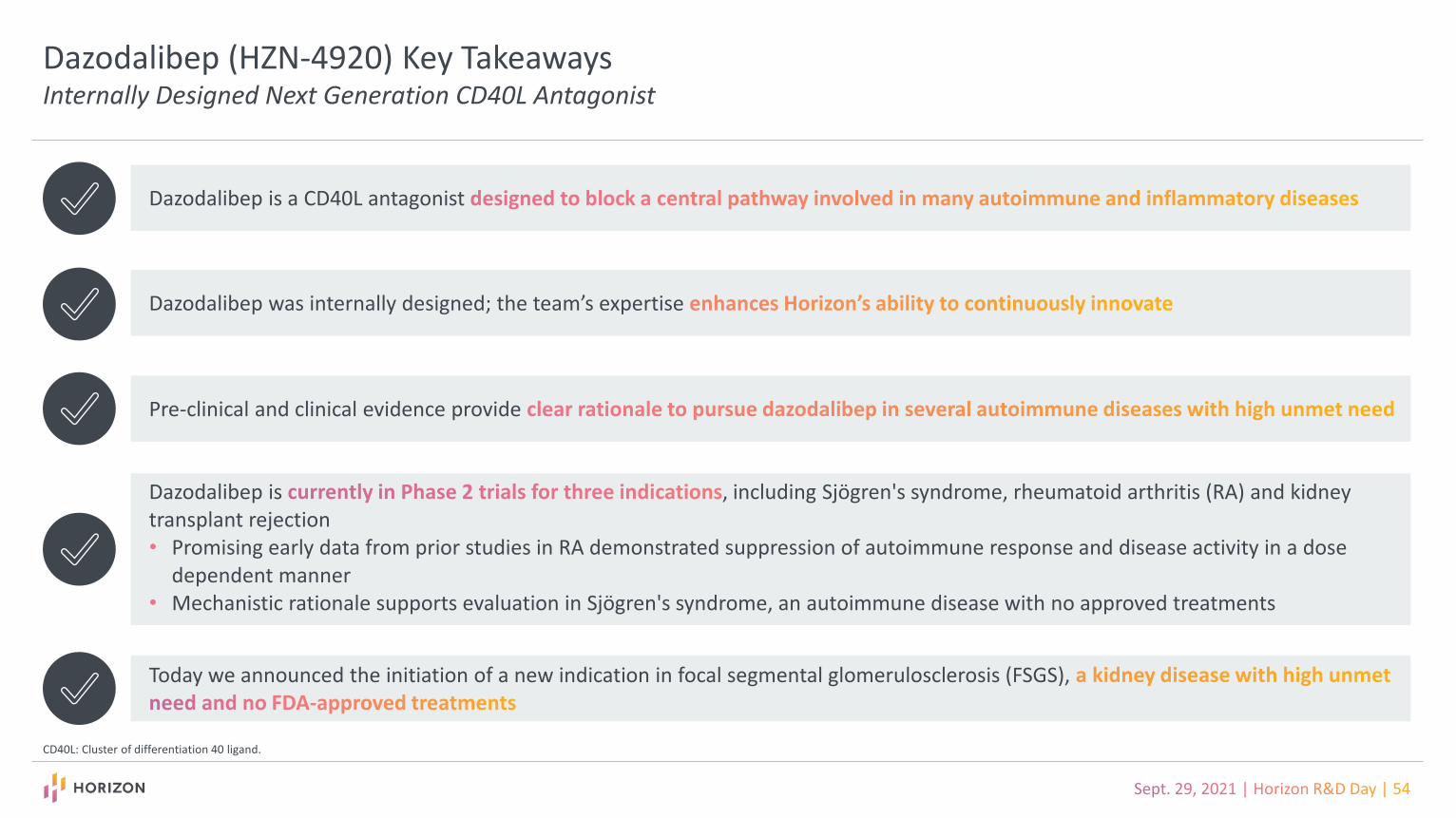
Dazodalibep (HZN-4920) Key TakeawaysInternally Designed Next Generation CD40L Antagonist
CD40L: Cluster of differentiation 40 ligand.
Dazodalibep is a CD40L antagonist
Dazodalibep was internally designed; the team’s expertise
Pre-clinical and clinical evidence provide
Dazodalibep is , including Sjögren's syndrome, rheumatoid arthritis (RA) and kidney transplant rejection• Promising early data from prior studies in RA demonstrated suppression of autoimmune response and disease activity in a dose
dependent manner• Mechanistic rationale supports evaluation in Sjögren's syndrome, an autoimmune disease with no approved treatments
Today we announced the initiation of a new indication in focal segmental glomerulosclerosis (FSGS),

• CD40/CD40L interactions play a critical role in driving immune responses, including the T-cell-dependent activation of B cells, central to the production of pathogenic autoantibodies
• CD40/CD40L can trigger overstimulation of immune cells leading to an immune response cascade and driving inflammation
• CD40L drives inflammation through its interaction with CD40 which is expressed on several tissues in the salivary gland, spleen, kidney, joint, gut and skin
• The CD40/CD40L pathway is implicated in many autoimmune diseases including Sjögren’s syndrome, RA, immune mediated kidney diseases and transplantation
CD40-CD40L Pathway Plays a Central Role in Autoimmune and Inflammatory Diseases
CD40: Cluster of differentiation 40. | CD40L: Cluster of differentiation 40 ligand. | RA: Rheumatoid arthritis.
Antibody secreting cell produces autoantibodies
APC and T cell produce inflammatory molecules
Memory B cell
Plasmablast
Autoantibodies
T cell
Cytokines
Cytokines Chemokines
Antigen Presenting Cell (APC)
T cell
CD40L
CD40
T cell
B cell
B cell

• First generation antibodies targeting CD40L were unsuccessful
• Dazodalibep is a fusion protein that binds to CD40L
• It was designed as a next-generation CD40L antagonist blocking the CD40 pathway and undesired immune responses that lead to the development of autoimmune diseases
Dazodalibep (HZN-4920) was Designed to Address Immune Overactivation Attributed to the CD40 Pathway
CD40: Cluster of differentiation 40. | CD40L: Cluster of differentiation 40 ligand.
Plasmablast
Autoantibodies
T cell
Antigen Presenting Cell (APC)
T cell
T cell
B cell
Memory B cell
B cell
CD40L
CD40
Dazodalibep

Clinical Evidence Demonstrated that Dazodalibep (HZN-4920) Can Suppress Antibody Response in a Dose Dependent Manner
Source: Karnell JL et al. Sci Transl Med. 2019 Apr 24; 11 (489).(1) Phase 1 randomized, blinded, placebo-controlled, single-ascending dose trial to evaluate the safety and tolerability of dazodalibep in healthy adults. (2) Immune responses stimulated with keyhole limpet hemocyanin (KLH), a T-dependent antigen. (3) Antibody response was measured using anti-KLH IgG titers (ng/ml).
Dazodalibep Suppressed Antibody Response in a Dose Dependent Manner(1)
DazodalibepImmune Response Stimulation(2)
An
tib
od
y R
esp
on
se(3
)
Immune Response Stimulation(2)
Visit Day
3000 mg(n=8)
1000 mg(n=8)
300 mg(n=8)
100 mg(n=8)
30 mg(n=8)
Placebo(n=2)

Dazodalibep (HZN-4920) Decreased Disease Activity in a Dose Dependent Manner in a Phase 1b Study in Patients with Active Rheumatoid Arthritis
TEAE: Treatment emergent adverse event. Source: Karnell JL et al. Sci Transl Med. 2019 Apr 24; 11 (489).DAS28-CRP is a composite clinical disease activity score used in rheumatoid arthritis that takes into account the number of swollen and tender joints, C-reactive protein (CRP) levels, and a patient global health assessment.
75.0%
50.0%
13.0%
1500 mg 1000 mg Placebo(n=12) (n=12) (n=15)
Patients Maintained Low Disease Activity Approximately Three Months Off Therapy
Half or More Patients on Dazodalibep Achieved Low Disease
Activity or Remission
• Balanced distribution of TEAEs between placebo and four active groups was observed
• No thrombotic events or significant coagulation abnormalities
Dazodalibep was Generally Safe and Well Tolerated
DA
S28
-CR
P a
t 3
.2 o
r le
ss
Me
an (
+/-)
Ch
ange
fro
m B
ase
line
in
DA
S28
-CR
P S
core
(Last Dose)
Dazodalibep 1000mg (n=12)Dazodalibep 1500mg (n=12) Placebo (n=15)

Dazodalibep (HZN-4920) is in Development for Four Indications, Each Addressing Immune Overactivation
FSGS photo source: © 1998-2021 Mayo Foundation for Medical Education and Research (MFMER); all rights reserved; https://www.mayoclinic.org/diseases-conditions/fsgs/symptoms-causes/syc-20354693.
• RA: a chronic inflammatory disorder characterized by progressive destruction of joints
• Next steps: Phase 2 trial underway; data readout in 1H 2022
Rheumatoid Arthritis (RA)
• KTR: occurs when the immune system detects an organ transplant as a threat and attacks it; results in organ rejection
• Next steps: Phase 2 open-label trial underway; data readout in 2H 2022
Kidney Transplant Rejection (KTR)
• Sjögren’s: chronic, systemic autoimmune disease attacking the salivary and tear (exocrine) glands, with severe cases affecting multiple organs
• Next steps: data readout in 2023
Sjögren’s Syndrome
• FSGS: a rare disease that attacks the kidney’s filtering units (glomeruli) and causes serious scarring, leading to permanent kidney damage and even kidney failure
• Next steps: Phase 2 trial expected to start in 2H 2022
Focal Segmental Glomerulosclerosis (FSGS)

Sjögren’s Syndrome is an Autoimmune Disease Involving Overexpression of CD40/CD40L with No FDA-Approved Treatments
CD40: Cluster of differentiation 40. | CD40L: Cluster of differentiation 40 ligand.(1) Horizon estimate.
• Chronic, systemic autoimmune disease attacking the salivary and tear (exocrine) glands, with severe cases affecting multiple organs
• Disease manifestations include dry eyes, dry mouth, arthritis and kidney or lung dysfunction
• Overexpression of CD40/CD40L observed at site of inflammation and in circulation
• ~250K-350K patients with Sjögren’s syndrome in the U.S. of which ~50k would be appropriate for novel therapies including biologics(1)
Sjögren’s Syndrome
• No FDA-approved treatments
• Current treatments: palliative care (artificial tears, medicines for dry mouth); topical cyclosporine; steroids/immunosuppressants used off-label as needed to manage systemic symptoms
Unmet Need

Phase 2 Trial Evaluating the Safety and Efficacy of Dazodalibep (HZN-4920) in Sjögren’s Syndrome
ESSDAI: European League Against Rheumatism. | EULAR: Sjögren’s Syndrome Disease Activity Index: A Sjögren’s specific disease activity index composed of 12 system domains. | ESSPRI: EULAR Sjögren’s Syndrome Patient Reported Index: Patient reported indexcomposed of three questions assessing dryness, fatigue and pain. | FACIT: Functional Assessment of Chronic Illness Therapy. | PGIS: atient’s Global Impression of Severity. | IV: Intravenous.
Placebo (n=36) 1500mg dazodalibep
1500mg dazodalibep (n=36) Placebo
Day 169: Primary EndpointDay 1 Day 281
Induction followed by monthly IV dosing
Population One (n=72)Moderate-to-High Systemic Disease Activity
• Subjects with ESSDAI ≥
• Primary endpoint: change from baseline in ESSDAI at Day 169
• Secondary endpoint: change from baseline in ESSPRI at Day 169
Population Two (n=102)Moderate-to-Severe Patient-Reported Symptoms
• Subjects with ESS RI score ≥ and residual stimulated salivary flow but with mild systemic disease activity defined by ESSDAI score < 5
• Primary endpoint: change from baseline in ESSPRI at Day 169
change from baseline in FACIT-Fatigue score at Day 169, change from baseline in PGIS at Day 169, safety and tolerability of multiple IV doses of dazodalibep and anti-drug antibodies until the study completion
Placebo (n=51) 1500mg dazodalibep
1500mg dazodalibep (n=51) Placebo
Day 169: Primary EndpointDay 1 Day 281
Induction followed by monthly IV dosing

Indication Being Pursued
Scientific Rationale(1)
Unmet Need / Competitive Landscape
U.S. Patient Population(2)
Focal Segmental Glomerulosclerosis (FSGS)
A rare disease that attacks the kidney’s filtering units (glomeruli)
and causes serious scarring, leading to permanent kidney damage and
even kidney failure
• Overactivity of the CD40-CD40L pathway likely a key driver of pathogenesis
• CD40-CD40L pathway involved in podocyte damage in FSGS kidney biopsies(3)
• Animal models support blocking CD40-CD40L pathway against renal injury(4)
• Most common glomerular disease resulting in end-stage renal disease in the U.S.
• No FDA-approved treatments; limited treatment options used off-label with moderate efficacy, undesirable side effects and high rates of relapse
~50K patients with primary FSGS and chronic
kidney disease, and not on dialysis
Focal Segmental Glomerulosclerosis (FSGS) is a Compelling Indication with High Unmet Need and No FDA-Approved Treatments
FSGS photos source: © 1998-2021 Mayo Foundation for Medical Education and Research (MFMER); all rights reserved; https://www.mayoclinic.org/diseases-conditions/fsgs/symptoms-causes/syc-20354693.(1) Doublier et al., PLoS One 2017 12(11):e0188045. (2) Horizon estimate. (3) Delville, et al., Sci Transl Med 6 (256) (2014) 256ra136. (4) Kairaitis et al., Kidney Int. 2003 64(4):1265-72.
Blood with impurities is filtered creating urine
Kidney with normal glomerulus
Scarring impairs kidney function
Kidney with FSGS

Dazodalibep (HZN-4920) Key TakeawaysInternally Designed Next Generation CD40L Antagonist
CD40L: Cluster of differentiation 40 ligand.
Dazodalibep is a CD40L antagonist
Dazodalibep was internally designed; the team’s expertise
Pre-clinical and clinical evidence provide
Dazodalibep is , including Sjögren's syndrome, rheumatoid arthritis (RA) and kidney transplant rejection• Promising early data from prior studies in RA demonstrated suppression of autoimmune response and disease activity in a dose
dependent manner• Mechanistic rationale supports evaluation in Sjögren's syndrome, an autoimmune disease with no approved treatments
Today we announced the initiation of a new indication in focal segmental glomerulosclerosis (FSGS),

Q&A
Sept. 29, 2021 | Horizon R&D Day | 64

HZN-825
Sept. 29, 2021 | Horizon R&D Day | 65
LPAR1 Antagonist with Early Signals of Benefit in Fibrotic Diseases, Areas with High Unmet Need
Srini Ramanathan, Ph.D., SVP Research & Development Sciences
Dinesh Khanna, M.D., M.Sc., Professor, University of Michigan

HZN-825 Key TakeawaysHZN-825 is an LPAR
1Antagonist with Early Signals of Benefit in Fibrotic Diseases, Areas with High Unmet Need
LPA: Lysophosphatidic acid. | LPAR: Lysophosphatidic acid receptor. | IPF: Idiopathic pulmonary fibrosis. | ILD: Interstitial lung diseases. | dcSSc: Diffuse cutaneous systemic sclerosis.
HZN-825 is an that blocks LPA signaling, and has including reversal of established fibrosis in animal studies
Preclinical evaluation and clinical data support the
We are pursuing HZN-825 in : dcSSc and IPF
Our Phase 2a exploratory study of HZN-825 , and such as IPF

The Role of Lysophosphatidic Acid (LPA) and the LPAR1 Receptor in the Pathogenesis of Fibrotic Diseases
• LPA are bioactive molecules
• In healthy individuals, LPA enables beneficial cellular events such as cell growth, migration and survival
• LPA signaling takes place through multiple receptors, including LPAR1
• In people with fibrotic disease, LPAR1 signaling is dysregulated, resulting in inflammation and fibrosis mediated by:
- Vascular leakage
- Epithelial damage
- Fibroblast recruitment
LPAR: Lysophosphatidic acid receptor.
The Role of LPAR1 in Fibrosis
Vascular leakage
Fibroblast recruitment
Epithelial damage
LPAR1
Inflammation and fibrosis
LPA

HZN-825 Selectively Blocks LPAR1 and May Provide Therapeutic Benefit in Fibrotic Diseases
LPAR: Lysophosphatidic acid receptor.
• HZN-825 blocks the LPAR1 pathway and has potential to impact fibrotic diseases
• In preclinical and / or clinical studies, LPAR1 antagonism has been shown to:
- Reduce immune cell infiltration
- Protect against development of fibrosis
- Reverse established fibrosis
HZN-825 Blocks the LPAR1 Pathway; Potential Impact on Fibrotic Diseases
LPAR1
HZN-825
Reduced immune cell infiltration
Reversed established fibrosis
Protected against development of fibrosis

Preclinical Evidence Supports the Broad Anti-Fibrotic Potential of LPAR1 AntagonismAdditionally, HZN-825 Was Proven Safe and Well Tolerated Across Several Phase 1 Studies
LPAR: Lysophosphatidic acid receptor.(1) Castelino et al Arthritis Rheum 63(5):1405–15. (2) Internal HZN Data. (3) Ledein et al Br J Pharmacol. 177:4296–4309. (4) Tager et al Nat Med 14(1):45-54. (5) Swaney et al Br J Pharmacol 160:1699-713. (6) Ninou et al Front Med Volume 5 Article 180. (7) Murphy et al Eur Respir J. 2019; 54(suppl 63):PA5383. (8) Pradere et al J Am S Nephrol 18:3110-3118. (9) Lee et al BBA Molecular Basis of Disease 1865:1332-1340.
HZN-825 was safe and well tolerated in >160 healthy volunteers across several Phase 1 studies
• LPAR1 deletion prevented dermal fibrosis(1)
in mouse models
• LPAR1 antagonism reversed dermal fibrosis(2, 3) in mouse models
Skin
• LPAR1 deletion prevented lung fibrosis(4) in mouse models
• LPAR1 antagonism reduced inflammation, fibrosis, vascular leakage, tissue injury and more(5-7) in mouse models
Lungs
• LPAR1 deletion reduced kidney fibrosis(8) in mouse models
• LPAR1 antagonism reduced fibrosis, improved cardiac and/or kidney function and more(2, 9) in multiple rodent models
Kidney and Heart

Systemic Sclerosis is the Hallmark Disease of Fibrosis Spanning Multiple Organ Systems
PAH: Pulmonary arterial hypertension.Source: Nie LY et al. 2019
• Estimated U.S. prevalence of systemic sclerosis: ~70K-80K
• ~60% limited cutaneous systemic sclerosis (lcSSc)
- Distal skin sclerosis – face, hands, forearms, feet, legs principally
- Pulmonary arterial hypertension and severe gut disease frequent and serious
- Late-stage complications frequent
• ~40% diffuse cutaneous systemic sclerosis (dcSSc)
- Diffuse disease involves the same areas as lcSSc but also more proximal skin areas: chest, thighs, upper arms and back
- High frequency of internal organ involvement including severe lung fibrosis
- Increased risk of renal crisis and cardiac involvement
Organ Complications Associated with Systemic Sclerosis
Interstitial lung diseases
Renal crisis
Gastrointestinal diseases
Digital ulcersRaynaud phenomenonSkin fibrosis
Musculoskeletal problems
Arrhythmias
Pericardial diseases
Valvular Disease
PAH
Myocardial Dysfunction

Interstitial Lung Disease (ILD) is the Leading Cause of Death in Patients with Systemic Sclerosis, and Idiopathic Pulmonary Fibrosis (IPF) is the Most Common ILD
SSc: Systemic sclerosis. (1) Perelas A. et al. 2020.
• ILD is a common comorbidity of SSc
• ILD is also the leading cause of death in patients with SSc with 10-year mortality of up to 40%(1)
SSc-ILD
• IPF is the most common ILD; IPF is a rare progressive lung disease characterized by dyspnea, chronic cough and potentially death
IPF

The Many Physical Characteristics of Systemic Sclerosis
Christopher P Denton ▪ Dinesh Khanna ▪ www.thelancet.com ▪ Published online April 13, 2017.
Digital vasculopathy Gastrointestinal
Lung Fibrosis Pulmonary hypertension
Cardiac Renal Musculoskeletal Calcinosis Acro-osteolysis

Usual Timing of Internal Organ Involvement in Systemic Sclerosis
RP: Raynaud's phenomenon. Arthritis Rheumatol. 2020 Jul;72(7):1049-1058. doi: 10.1002/art.41246. Epub 2020 May 18. Current and Future Outlook on Disease Modification and Defining Low Disease Activity in Systemic SclerosisVivek Nagaraja 1 , Marco Matucci-Cerinic 2 , Daniel E Furst 3 , Masataka Kuwana 4 , Yannick Allanore 5 , Christopher P Denton 6 , Ganesh Raghu 7 , Vallerie Mclaughlin 1 , Panduranga S Rao 1 , James R Seibold 8 , John D Pauling 9 , Michael L Whitfield 10 , Dinesh Khanna 1.
DIFFUSE CUTANEOUS VARIANT
LIMITED CUTANEOUS VARIANT
TIME
Raynaud, digital ischemia
SKIN
TH
ICK
NES
S
2-5 years after first non-RP symptom/sign
Limited Diffuse
tendon/bursal friction rubs;joint contractures
skeletal myopathy
interstitial lungdisease
myocardial involvement “renal crisis”pulmonary
hypertension
interstitial lung disease
esophageal disease
pulmonary hypertension
malabsorption

The Physical and Emotional Impact of Early Systemic Sclerosis
https://journals.sagepub.com/doi/full/10.1177/2397198319866615.
Initial symptoms• Skin thickening
• Raynaud’s phenomenon
• Swelling of hands
• Fatigue
• Pain
Diagnosis• Delays reaching
appropriate specialist
• Shock at severity of disease
• Poor prognosis
Treatment• High treatment
burden
• Limited options
• No cure
Worsening symptoms• Loss of mobility/
dexterity
• Pain
• Exhaustion
• Changed appearance
• Depression/anxiety
• Worry about organ involvement
Fearful Complicated
UnpredictableHopeful
Supported
DepressedWeak
BurdenedIsolated
Tightness Pain
Limiting
Sad
ExhaustedConfused
Frustrated

HZN-825 Showed Early Signals of Benefit in dcSSc Patient Population in a Phase 2a 24-Week Exploratory Study
NS: Not significant. | LPA: Lysophosphatidic acid. | dcSSc: Diffuse cutaneous systemic sclerosis. | mRSS: Modified Rodnan Skin Score is a measure of skin thickness intended to measure disease severity and mortality. The minimal clinically important difference (MCID) is an improvement of 5 units. Source: Allanore et al, Arth & Rheum. Oct 2018. SAR100842 was renamed HZN-825. (1) Responder rate defined as ≥ point improvement/reduction in mRSS.
Clinical Outcomes: Median Decrease in mRSS Responder Rate(1)
24-weeks of continuous HZN-825 treatment -7.5 78.6%
Subjects switched from placebo to HZN-825 -7.0 69.2%
Eight-Week Double-Blind Period (n=32) 16-week Open-Label Extension Period (n=30)
Numerically greater median reduction in mRSS (0-51); baseline to week eightBoxes represent the 25th to 75th percentiles, dark lines in boxes represent the median, the lines outside the box represent 10th and 90th percentiles, and the open circles are outliers
Imp
rove
me
nt
• After week eight, all patients were placed on HZN-825 treatment for 16 weeks
• Biomarker analysis of skin biopsies showed reductions in LPA-related genes
• Similar proportions of adverse events in active and placebo arms
• No safety concerns seen on laboratory parameters
Safety
Ch
ange
in m
RSS
fro
m b
ase
line
P=NS

Evaluating Two Fibrotic Diseases with Significant Unmet Need: dcSSc and IPF (ILDs)
Disease dcSSc IPF
Treatment Options
• No FDA-approved treatment for dcSSc• Two FDA approved therapies for SSc-related lung fibrosis • Current treatments provide symptomatic relief without compelling
evidence of slowing disease progression for overall disease- Exception: Stem cell transplant but associated with toxicity
• Treatment options include immunomodulators, NSAIDs, ACE inhibitors, vasodilators
• First-line options include nonpharmacologic management (oxygen, rehabilitation) and symptomatic care (steroids, beta-2 agonists)
• As IPF progresses, FDA-approved anti-fibrotic treatments can be tried
• Lung transplant is final option
A more comprehensive treatment is needed to address the inflammation and fibrosis that drive dcSSc and IPF
Shortcomings of Current Therapies
• Current treatments slow disease progression but do not stabilize or reverse disease
• Significant tolerability and compliance issues with current anti-fibrotic therapies
• Patients often need multiple treatments• Ineffective at halting disease progression, resulting in high
morbidity and mortality rates
U.S. Prevalence • ~30K dcSSc patients in the U.S.(1) • ~100K IPF patients in the U.S.(2)
Rationale• Clinical proof of concept demonstrated for LPAR1 antagonism in IPF• In a 24-week exploratory study, HZN-825 showed early signals of
benefit in dcSSc patient population
dcSSc: Diffuse cutaneous systemic sclerosis. | IPF: Idiopathic pulmonary fibrosis. | ILD: Interstitial lung diseases. | ACE: Angiotensin-converting enzyme. | NSAID: Nonsteroidal anti-inflammatory drug. | LPAR: Lysophosphatidic acid receptor.(1) Chifflow H Semin Arthritis Rheum 37:223-235. (2) Barratt SL, Creamer A, Hayton C, Chaudhuri N. Idiopathic pulmonary fibrosis (IPF): an overview. J Clin Med. 2018;7(8):201.

Phase 2b Pivotal Trial in Diffuse Cutaneous Systemic Sclerosis (dcSSc) Expected to Initiate Q4 2021
QD: Once daily. | BID: Twice daily. | SSC: Systemic sclerosis
• Change in forced vital capacity (FVC) % predicted after 52 weeks of treatment
• HAQ-DI (Health Assessment Questionnaire Disability Index), Physician Global Assessment (MDGA), Patient Global Assessment (PTGA), SSPRO-18, mRSS (modified Rodnan skin score), ACR-CRISS (American College of Rheumatology Composite Response Index in Systemic Sclerosis)
Key Inclusion Criteria
• Early, active disease with inflammation
• Stable immunosuppressive use
• <36 months since onset of first non-Raynaud's SSc manifestation
Phase 2 Trial Design in dcSSc
Safety Follow-Up
30
0 p
atie
nts
1:1
:1 r
an
do
miz
ati
on Cohort 1: HZN-825 300 mg QD
Cohort 2: HZN-825 300 mg BID
Placebo
Study Week 0
Week 52Primary Endpoint
Week 56Safety Follow-Up

Phase 2b Pivotal Trial in Interstitial Pulmonary Fibrosis (IPF) Expected to Initiate Q4 2021
QD: Once daily. | BID: Twice daily.
• Change in forced vital capacity (FVC) % predicted after 52 weeks of treatment
• Decline in FVC % predicted ≥10%, 6-Minute Walk Test (6MWT), King's Brief Interstitial Lung Disease (K-BILD), Living with IPF (L-IPF), Leicester Cough Questionnaires (LCQ), hospitalization due to respiratory distress, composite endpoint of progression-free survival (PFS)
Key Inclusion Criteria
• Diagnosis of I F ≥1 year to ≤ years
• Not currently treated with IPF therapy
Phase 2 Trial Design in IPF
36
0 p
atie
nts
1:1
:1 r
an
do
miz
ati
on Cohort 1: HZN-825 300 mg QD
Cohort 2: HZN-825 300 mg BID
Placebo
Study Week 0
Week 52Primary Endpoint
Week 56Safety Follow-Up
Safety Follow-Up

HZN-825 Key TakeawaysHZN-825 is an LPAR
1Antagonist with Early Signals of Benefit in Fibrotic Diseases, Areas with High Unmet Need
LPA: Lysophosphatidic acid. | LPAR: Lysophosphatidic acid receptor. | IPF: Idiopathic pulmonary fibrosis. | ILD: Interstitial lung diseases. | dcSSc: Diffuse cutaneous systemic sclerosis.
HZN-825 is an that blocks LPA signaling, and has including reversal of established fibrosis in animal studies
Preclinical evaluation and clinical data support the
We are pursuing HZN-825 in : dcSSc and IPF
Our Phase 2a exploratory study of HZN-825 , and such as IPF

UPLIZNA® (inebilizumab-cdon)Next-Generation B-Cell Depleter with a Novel, Targeted Approach
Sept. 29, 2021 | Horizon R&D Day | 80
Kristina Patterson, M.D., Ph.D., Medical Director, Neuroimmunology
Theresa Podrebarac, M.D., M.Sc., SVP Clinical Development

UPLIZNA Key Takeaways A Next-Generation B-Cell Depleter with a Novel Targeted Approach
AChR+: Acetylcholine receptor. | MuSK+: Muscle-specific kinase. | CD19: Cluster of differentiation 19. | CD20: Cluster of differentiation 20. | IgG4: Immunoglobulin G4.
UPLIZNA is an anti-CD19, humanized monoclonal antibody with potential in multiple autoimmune diseases
Targets the CD19 antigen, which including plasmablasts and certain plasma cells that anti-CD20 therapies do not target
, which include:
Neuromyelitis optica spectrum disorder (NMOSD), where UPLIZNA is already indicated
, where UPLIZNA has the potential for differentiation; our robust Phase 3 trial is the first with clearly delineated AChR+ and MuSK+ patient populations
, where UPLIZNA has the potential to be the first-ever FDA-approved therapy

B Cells Contribute to the Damaging Pathology of Multiple Autoimmune and Autoinflammatory Diseases
CD19: Cluster of differentiation 19.
• B cells are a white blood cell type, and an integral component of the adaptive immune system
• An important immune system function of B cells is making antibodies
− In a normal state, these antibodies attack foreignpathogens such as bacteria and viruses
− In autoimmune disorders, antibodies attack the body’s own tissues, leading to disease
• B cells also play a role in healthy inflammatory responses through the production of cytokines and chemokines and interactions with T cells
− In excess, this response can lead to prolonged activation of T cells and tissue destruction
B-Cell Dysregulation Plays a Central Role in Many Diseases
Production of Autoantibodies
Production of pro-fibrotic chemokines and cytokines that recruit immune cells with fibrotic potential
Production of long-lived pool of memory T cells
Memory T cell
T cell
B cell
Plasmablast
Plasma cells
CD19
CD19
CD19

UPLIZNA: Next-Generation Humanized Monoclonal Antibody Engineered for Differentiated Mechanistic and Clinical Profile
CD19: Cluster of differentiation 19. | F(ab): Fragment antigen-binding. | Fc: FcγRIIIa; type III Fcy receptor a.
Optimized for human CD19 binding
• Selectively binds to CD19 with high affinity, targeting a broad lineage of B cells for depletion – including plasmablasts and plasma cells
Humanized F(ab) portion
• Humanized structure designed to decrease immunogenicity, improve tolerability and reduce the risk of infusion reactions
Afucosylated Fc portion
• Afucosylated design allows for enhanced therapeutic efficiency with lower doses of the drug, with the potential to improve the efficacy and safety profile

UPLIZNA: Anti-CD19 Provides More Complete B-Cell Depletion
CD19: Cluster of differentiation 19. | CD20: Cluster of differentiation 20. | IgG: Immunoglobulin G. | IgM: Immunoglobulin M. | IgD: Immunoglobulin D.(1) Adapted from Cree et al. Poster presented at the American Association of Neurology 2021 Virtual Annual Meeting, April 17–22, 2021.
Stem cell Pro-B cell Pre-B cell Immature B cell
NaïveB cell
Mature B cellMemory B cell
Plasmablast Plasma cell
Bone marrow Periphery
CD19 expression
IgM IgD
Secreted IgG
IgM
Directly targeted by UPLIZNA but not by anti-CD20 agents
CD19 expression
CD20 expression
IgG
Targets a broader range of B cells for depletion
Demonstrated depletion of B cells to <1 cell/μL
Shown to be effective at preventing attacks for at least four years in the
open-label period(1)

NMOSD is a Chronic Autoimmune Disease of the Central Nervous System
NMOSD: Neuromyelitis optica spectrum disorder. | MS: Multiple sclerosis.
What is NMOSD?
• NMOSD is an autoimmune, inflammatory disease of the central nervous system
• Attacks the optic nerve, spinal cord and can also affect the brain and brainstem
• Severe, rare, relapsing
• Attacks result in accumulation of neurological damage and can result in blindness, paralysis and death
What causes NMOSD?
• Discovery of autoantibodies to aquaporin-4 (AQP4) in 2004 differentiated NMOSD from MS
• In ~80% of cases antibodies to AQP4 are present
• U.S. NMOSD population: ~10K; ~8K AQP4+
Optic neuritis
Myelitis
Brain/brain stem

UPLIZNA is a Well-Studied, Well-Understood Medicine in NMOSD that Prevents Attacks
NMOSD: Neuromyelitis optica spectrum disorder. | HR: hazard ratio. | CI: confidence interval. | NNT: number needed to treat. | RCT: Randomized controlled trial. | CI: Confidence interval. | AQP4-IgG: Aquaporin-4 Immunoglobulin G.(1) Cree et al. Long-term efficacy outcomes with inebilizumab treatment in neuromyelitis optica spectrum disorder: the N-MOmentum trial. Neurology (AAN) 2021 Virtual Annual Meeting April 17-22, 2021. ACTRIMS Forum 2021; February 15-27, 2021.
Phase 3 Data: B-Cell Depletion with UPLIZNA Decreases Attacks and Reduces Possibility of Disability
AQP4-IgG seropositive population
Pro
bab
ility
of
no
att
ack
Time (days)
PlaceboUPLIZNA
87.6%
56.6%Patients with NMOSD attacks (n/N)Inebilizumab, 18/161 (11.2%)Placebo, 22/52 (42.3%)HR (95% CI), 0.227 (0.121, 0.423); p < 0.0001NNT at Day 197 (95% CI), 3.23 (2.72, 4.54)
• UPLIZNA treatment generally well tolerated
Long-Term Data: UPLIZNA Provided Sustained Reduction in NMOSD Attack Risk At Least 4 Years(1)
Originally on UPLIZNA in the RCT and on UPLIZNA during
the open-label period
Originally on placebo in the RCT and on UPLIZNA during
the open-label period
87.7%
% of patients who remained attack-free
83.4%
0
20
40
60
80
100

UPLIZNA is a Well-Studied, Well-Understood Medicine in NMOSD; Positive Disability Data; Positive Rituximab-Switch Data and Sustained B-Cell Depletion
EDSS: Expanded Disability Status Scale. | NMOSD: Neuromyelitis optica spectrum disorder. | CD19: Cluster of differentiation 19. | CD20: Cluster of differentiation 20. | RCT: Randomized controlled trial. (1) Marignier et al. Disability outcomes in the N-MOmentum trial of inebilizumab in neuromyelitis optica spectrum disorder. Neurol Neuroimmunol Neuroinflamm 2021;8:e978. (2) Levy et al. The safety and efficacy of inebilizumab in those with previous rituximab exposure. ACTRIMS Forum 2021; February 15-27, 2021. (3) Cree et al. Lancet. 2019 Oct 12;394(10206):1352-1363. (4) N-Momentum measured CD20 B cells because UPLIZNA specifically binds CD19, which interferes with the CD19 assay. Therefore, once a patient receives UPLIZNA, CD20 B cells are measured. Likewise, studies in anti-CD20 agents, CD19 cells are measured because the anti-CD20 agents bind CD20.
Disability: UPLIZNA Improved Disability Outcomes Regardless of Baseline Status,
Attack History or Disease Duration(1)
Subgroup analysis
Baseline EDSS <5
Baseline EDSS ≥
Number of prior attacks, <2
Number of prior attacks, ≥2
Disease duration <5 years
Disease duration ≥ years
UPLIZNAbetter
Placebobetter Circulating CD20 B cells at each study visit (3,4)
CD
20
B c
ells
(ce
lls p
er µ
L)
Durability: In the NMOSD Phase 3 Trial, B-Cell Depletion in the UPLIZNA Group vs.
Placebo was Rapid and Sustained (p<0.0001)
Rituximab Switching: Patients with Prior Rituximab Exposure Saw Significant Attack
Reduction on UPLIZNA(2)
Of seven patients with confirmed attacks while treated with rituximab,
, with mean follow-up period of
Time (days)
PlaceboUPLIZNA

• Characteristics and symptoms: Rare autoimmune disease caused by breakdown in communication between nerves and muscles
− Two main types of MG: AChR+ and MuSK+
− Symptoms include weakness, drooping eyelid(s), double vision, difficulties with speech and swallowing, and respiratory impairment
− A hallmark of MG is patient variability and fluctuation in symptoms/impact
• U.S. prevalence: ~55K with generalized MG; 20K-25K appropriate for novel therapies, including a biologic(1)
• Current standard of care: steroids, immunosuppressants (including off-label use of rituximab, a CD20+ B-cell depleter), cholinesterase inhibitors, IVIG, plasmapheresis, complement inhibition
MG is a Debilitating Rare Disease with Significant Unmet Need
AChR+: Acetylcholine receptor. | MuSK+: Muscle-specific kinase. | MG: Myasthenia Gravis. | IVIG: Intravenous immunoglobulin.(1) Horizon estimate.
A Common MG Symptom is Drooping Eyelids (Ptosis)

GERMINAL CENTER
Plasma cell
B cell
T cell
NEUROMUSCULAR JUNCTION
Neuron
Muscle
MG is Caused by Autoantibodies Attacking the Postsynaptic Neuromuscular Junction, Leading to Muscle Weakness
AChR: Acetylcholine receptor. | MuSK: Muscle-specific kinase. | Lrp4: Low density lipoprotein receptor-related protein 4. | MG: Myasthenia gravis.
MG
Anti-Lrp4
Anti-MuSKAnti-AchR
NORMAL
AchR
Lrp4Ach
MuSK
• In MG, autoantibodies target functional proteins (e.g., AChR and MuSK) in the post-synaptic neuromuscular junction
• This interrupts the normal synaptic function needed to signal muscle contraction, and:
• Results in neuromuscular junction damage and remodeling
• Affects voluntary muscles of the body, especially those that control the eyes, mouth, throat, breath and limbs

Phase 3 MG TrialLarge, Robust Pivotal Trial with Clearly Delineated Patient Populations
AChR+: Acetylcholine receptor autoantibody positive. | MuSK+: Muscle-specific kinase autoantibody positive. | MG: Myasthenia Gravis. | ADL: Activities of Daily Living.| QMG Score: Quantitative Myasthenia Gravis score.
Change from Baseline in MG-ADL Profile score at 52 weeks (AChR+) and 26 weeks (MuSK+)
Data readout expected in 2023
Key Inclusion Criteria
• MG-ADL Score ≥6 with > 0% non-ocular symptoms
• QMG Score ≥11
• On standard of care:
- Corticosteroids only; or - One allowed non-steroidal immunosuppressant; or- Corticosteroids plus one allowed immunosuppressant
Phase 3 Trial Design in MG: Aim is to Assess Whether UPLIZNA Can Reduce MG-Related Disability in Two Different Patient Populations
AC
hR
+1
88
p
ati
ents
Mu
SK+
82
pa
tien
ts
18-Month Optional Open-Label Period
UPLIZNA Three infusions (Days 1, 15 and 183); 300mg per infusion
PlaceboThree infusions (Days 1, 15 and 183)
18-Month Optional Open-Label Period
UPLIZNA Two infusions (Days 1 and 15); 300mg per infusion
PlaceboTwo infusions (Days 1 and 15)
Day 1 Week 26MuSK+ Primary Endpoint
Week 52AChR+ Primary Endpoint
+18 MonthsOpen-Label Optional Period

IgG4-Related Disease (IgG4-RD) is a Chronic, Debilitating Rare Disease
IgG4: Immunoglobulin G4.(1) ACR-EULAR 2019 IgG4-RD Classification Criteria, from Perugino, C. A. and Stone, John. IgG4-related disease: an update on pathophysiology and implications for clinical care. Nature Reviews Rheumatology. September 2020. (2) Horizon estimate.
• Characteristics and symptoms(1): Chronic, debilitating rare disease characterized by tumor-like inflammatory and fibrotic mass formation in affected organs
• Affects mostly men (75%)
• Progressive; waxes and wanes; attendant morbidity; potential mortality. Specific symptoms depend on which organs are affected; multiple organ involvement is typical
• Major causes for mortality include liver cirrhosis, portal hypertension, retroperitoneal fibrosis, etc.
• U.S. prevalence: ~20K-40K(2); large variance due to limited epidemiology data
• Current standard of care: steroids, rituximab (off-label)
IgG4-RD is Caused by Multiple Mechanisms of B-Cell Dysfunction
IgG4-RD: Multiple Organ Disease
• Lacrimal glands
• Parotid glands
• Lymph nodes
• Pancreas
• Lungs
• Aorta
• Submandibular glands
• Retroperitoneum
• Biliary tree
• Thyroid
• Kidneys
• Orbits
• Others

• B cells trigger and perpetuate pathogenic processes in IgG4-RD, including:
IgG4 class switch and oligoclonal expansion of CD19+ IgG4+ plasmablasts; massive tissue infiltration and swollen lesions
Production of IL-1 and other factors, driving tissue inflammation
Production of profibrotic molecules (TGFβ, LOXL2, PDGF-B); fibroblast activation, increased collagen production and fibrosis
Autoantibody production and interactions with CD4+ and CD8+ T cells, leading to cycle of CTL-mediated tissue destruction
.
IgG4-Related Disease is Caused by Multiple Mechanisms of B-Cell Dysfunction
CD4: Cluster of differentiation 4. | CD8: Cluster of differentiation 8. | CD19: Cluster of differentiation 19. | IgG4-RD: Immunoglobulin G4-related disease. | IL-1: Immunoglobulin-Like 1. | CTL: Cytotoxic T lymphocytes. TGFβ: Transforming growth factor beta. | LOXL2: Lysyl Oxidase Like 2. | PDGF-B: Platelet-derived growth factor subunit B.Hsieh SC, Shen CY, Liao HT, et al. The Cellular and Molecular Bases of Allergy, Inflammation and Tissue Fibrosis in Patients with IgG4-related Disease. Int J Mol Sci. 2020;21(14):5082.Perugino CA, Stone JH. IgG4-related disease: an update on pathophysiology and implications for clinical care. Nat Rev Rheumatol. 2020 Dec;16(12):702-714.Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012 Sep;25(9):1181-92.
CD4+ and CD8+ T cells
CD19+ B cells
IgG4 class switch and oligoclonal expansion
IL-1 production
Profibrotic factorproduction
Autoantibodies
T follicular
helper cells
• Cell damage, death• Tissue destruction• Self-antigen release• More autoantibodies
Plasmacytic infiltration and tissue
enlargement
1 2 3 4
Inflammation of tissues
Fibrosis
1
2
3
4

Examples of IgG4-RD Manifestations
IgG4-RD: Immunoglobulin G4-related disease.Source: Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med 2012; 366:539.

Phase 3 IgG4-RD TrialFirst Pivotal Randomized Controlled Trial in IgG4-RD
RCT: Randomized controlled trial. | GC: Glucocorticoid. | IgG4-RD: Immunoglobulin G4-related disease. | ACR: American College of Rheumatology. | EULAR: European Alliance of Associations for Rheumatology.
Time to first adjudication committee-determined, investigator-treated disease flare during RCT
Event-based endpoint; data readout expected in 2023
Key Inclusion Criteria
• Clinical diagnosis of IgG4-RD
• Fulfillment of 2019 ACR/EULAR IgG4-RD classification criteria
• Experiencing or recently experienced an IgG4-RD flare that requires GC treatment
• IgG4-RD affecting >2 organs/sites during course of IgG4-RD
Phase 3 Trial Design: Aim is to Define the Efficacy and Safety of UPLIZNA for Prevention of IgG4-RD-Related Flares
~16
0 p
ati
ents
52-Week Optional Open-Label Period
UPLIZNA Three infusions (Days 1, 15 and 183); 300mg per infusion
PlaceboThree infusions (Days 1, 15 and 183)
Day 1 Week 52 +52 WeeksOpen-Label Optional Period

UPLIZNA Key Takeaways A Next-Generation B-Cell Depleter with a Novel Targeted Approach
AChR+: Acetylcholine receptor . | MuSK+: Muscle-specific kinase. CD19: Cluster of differentiation 19. | CD20: Cluster of differentiation 20. | IgG4: Immunoglobulin G4.
UPLIZNA is an anti-CD19, humanized monoclonal antibody with potential in multiple autoimmune diseases
Targets the CD19 antigen, which including plasmablasts and certain plasma cells that anti-CD20 therapies do not target
, which include:
Neuromyelitis optica spectrum disorder (NMOSD), where UPLIZNA is already indicated
, where UPLIZNA has the potential for differentiation; our robust Phase 3 trial is the first with clearly delineated AChR+ and MuSK+ patient populations
, where UPLIZNA has the potential to be the first-ever FDA-approved therapy

Q&A
Sept. 29, 2021 | Horizon R&D Day | 96

TEPEZZABuilding the Evidence to Help Treat More Patients with Chronic TED
Sept. 29, 2021 | Horizon R&D Day | 97
Bobby S. Korn, M.D., Ph.D., FACS, Professor of Ophthalmology & Plastic Surgery, University of California, San Diego

Thyroid Eye Disease (TED): Debilitating, Vision-Threatening; Severely Impacts Quality of Life
Inflammation and tissue expansion behind the eye causes proptosis, the most disfiguring sign of TED
Can impair ability to close eyes, resulting in pain and corneal ulceration
Associated with diplopia (double vision), which is a result of misalignment of eyes
Impacts quality of life: Working, driving, reading, and sleeping

Natural History of TED – Acute to Chronic
TED: Thyroid Eye Disease.(1) Douglas RS, et al. N Engl J Med. 2020;382(4):341-352. (2) Ozzello DJ, et al. Am J Ophthalmol Case Rep. 2020;19:100744.
Time
Chronic TED
Acute TED
Sign
s &
Sym
pto
ms
Acute inflammatory
<9 months(1)
Chronic noninflammatory
3 years(2)
Inflammatory signs and symptoms, such as pain, redness, swelling, proptosis, diplopia, and eyelid
retraction are at peak levels
Inflammatory signs such as redness and swelling are reduced but the pain, proptosis, diplopia, and eyelid
retraction are persistent throughout life

Acute and Chronic TED Have Similar Signs and Symptoms
TED: Thyroid Eye Disease.Wang, Y et al., Active Versus Inactive Thyroid Eye Disease: Symptom and Quality of Life Comparison in US Patients. ACE May 26-29, 2021, Virtual.
0%
50%
100%
0%
50%
100%
Most commonly reported signs and symptoms of acute TED
Most-commonly reported signs and symptoms of chronic TED

Acute and Chronic TED Have a Similar Impact on Mental Health
TED: Thyroid Eye Disease.(1) US adult population statistics for 2017 as reported by the National Institutes of Health.
19% 19%
7%
37%
28%
19%
36%
26%
17%
0%
10%
20%
30%
40%
Any mental health issue Anxiety Depression
US adult population Acute TED population Chronic TED population
• Mental health issues (anxiety and/or depression) were higher in both the acute and chronic TED populations
• The prevalence of mental health issues was not significantly different between patients with acute and chronic disease
(1) (1) (1)

TE E A’s Mechanism of Action: Common athway in Acute and Chronic TED
TED: Thyroid Eye Disease.Eye Pathology – Eagle R.C. 2017
• Insulin-like growth factor-1 receptor (IGF-1R)/Thyroid stimulating hormone receptor (TSHR) signaling key in TED
• Teprotumumab is a human monoclonal antibody inhibitor of IGF-1R
• Binds to IGF-1R/TSHR complex and blocks downstream signaling
• Targets the pathology at TED’s source, reducing production of hyaluronic acid, halting inflammation and retro-orbital tissue expansion
• Pathway is common in both acute and chronic TED
TEPROTUMUMAB
IGF-1R/TSHR COMPLEX
B CELL
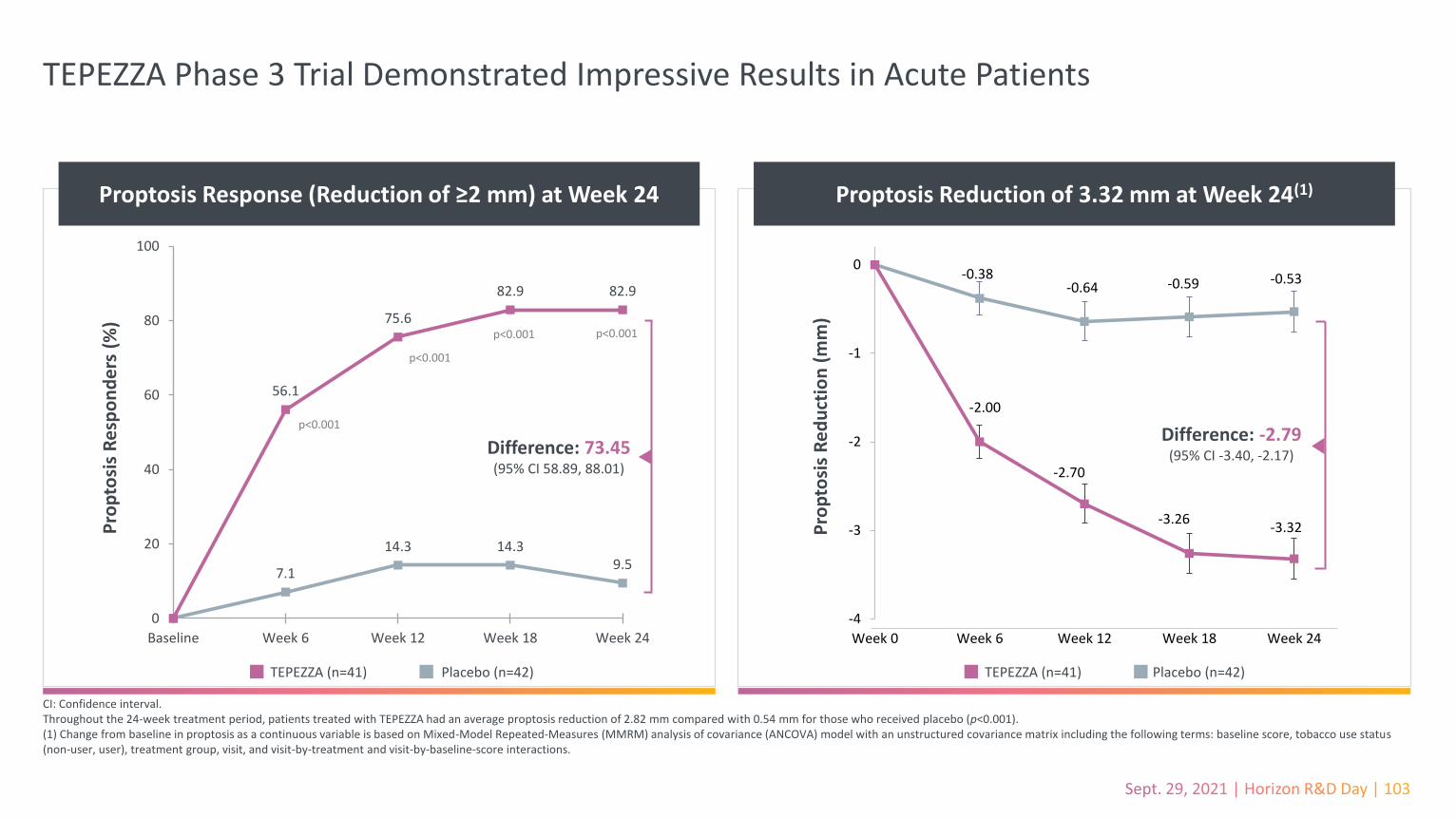
TEPEZZA Phase 3 Trial Demonstrated Impressive Results in Acute Patients
CI: Confidence interval.Throughout the 24-week treatment period, patients treated with TEPEZZA had an average proptosis reduction of 2.82 mm compared with 0.54 mm for those who received placebo (p<0.001).(1) Change from baseline in proptosis as a continuous variable is based on Mixed-Model Repeated-Measures (MMRM) analysis of covariance (ANCOVA) model with an unstructured covariance matrix including the following terms: baseline score, tobacco use status (non-user, user), treatment group, visit, and visit-by-treatment and visit-by-baseline-score interactions.
Proptosis Response (Reduction of ≥2 mm) at Week 24
Pro
pto
sis
Re
spo
nd
ers
(%
)
7.1
14.3 14.39.5
56.1
75.6
82.9 82.9
0
20
40
60
80
100
Baseline Week 6 Week 12 Week 18 Week 24
p<0.001
p<0.001
p<0.001 p<0.001
Difference: 73.45(95% CI 58.89, 88.01)
TEPEZZA (n=41) Placebo (n=42)
Proptosis Reduction of 3.32 mm at Week 24(1)
-0.38-0.64 -0.59 -0.53
-2.00
-2.70
-3.26-3.32
-4
-3
-2
-1
0
Week 0 Week 6 Week 12 Week 18 Week 24
Pro
pto
sis
Re
du
ctio
n (
mm
)
Difference: -2.79(95% CI -3.40, -2.17)
TEPEZZA (n=41) Placebo (n=42)

OPTIC-X Shows Efficacy Across Short- and Long-Term Thyroid Eye Disease
TED: Thyroid Eye Disease.Douglas RS, et al., Teprotumumab for the Treatment of Active Thyroid Eye Disease. N Engl J Med 2020; 382:341-52. DOI: 10.1056/NEJMoa1910434
Phase 3 OPTIC-X
Timing<9 months since diagnosis of acute TED (average 6 months)
Average of 12 months since diagnosis of TED (up to 16 months)
Response
• 89% proptosis responder rate • 3.5-mm reduction in proptosis at Week 24
Before
After-2.00
-2.70
-3.26 -3.32
-1.78
-2.58
-3.23-3.47
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0 6 12 18 24
Pro
pto
sis
Ch
ange
fro
m B
asel
ine
(mm
)
TEPEZZA (OPTIC, N =41) Placebo --> TEPEZZA (OPTIC-X, N=37)

First Published Case Report in AJO with TEPEZZA in a Chronic TED Patient
TED: Thyroid Eye Disease. | CAS: Clinical Activity Score.Ozzello DJ, et al. Am J Ophthalmol Case Rep. 2020 May 15;19:100744. doi: 10.1016/j.ajoc.2020.100744.
• 50-year-old female
• 3-year history of disease
• CAS score of 1
• Nonsurgical candidate
• 6mm proptosis reduction achieved after 3 infusions
• Reduction of extraocular muscles suggest TEPEZZA can modify disease course in chronic disease

Update – First Published Case Report in AJO on TEPEZZA in a Chronic TED Patient
Pre-TEPEZZA After 3 infusions 1 year after 8 infusions
TED: Thyroid Eye Disease. | AJO: American Journal of Ophthalmology.Ozzello DJ, et al. Am J Ophthalmol Case Rep. 2020 May 15;19:100744. doi: 10.1016/j.ajoc.2020.100744.

Ugradar – Eye – 2020: Mean proptosis reduction of 2.6 mm(1)
(N = 4 non-inflammatory TED patients; on average 7 months from diagnosis)
Davis – NANOS – 2021 (Poster): Proptosis reduction of 5-6 mm from baseline after
completing treatment of 8 infusions(N = 1; patient diagnosed with Graves in 1997)
Ozzello – AJO – 2020: Proptosis reduction of 5 mm and 6 mm in the right and left eye
respectively after 3 infusions (N = 1; 24 months of stable eye disease)
Diniz – OPRS – 2021: 71% overall proptosis response rate (proptosis reduction ≥2 mm(2);
N = 6; on average 16 months from onset of TED)(3)
Illustrative Case Studies Demonstrating Efficacy in Chronic TED Patients
TED: Thyroid Eye Disease. | AJO: American Journal of Ophthalmology. | OPRS: Ophthalmic Plastic and Reconstructive Surgery. | NANOS: North American Neuro-Opthalmology Society.(1) After completing treatment of 8 infusions. | (2) After range of 3-8 infusions; photo taken after 3 infusions. | (3) 71% response rate refers to the 21 patients in the study. 6 refers to patients with chronic TED. (4) Mean of 7 infusions.
Ozzello - Orbit - 2021: 78% proptosis reduction of ≥2 mm in at least one eye(1)
(N = 9; on average of 75 months from diagnosis)
Ugradar - Eye - 2021: 90% of study experienced clinically significant improvement
(≥2 mm) in proptosis(4)
(N = 31; on average of 81 months from diagnosis)

Growing Body of Patient Case Studies Supporting the Use of TEPEZZA in Chronic TED
TED: Thyroid Eye Disease.(1) Ozzello DJ, et al. Am J Ophthalmol Case Rep. 2020 May 15;19:100744. doi: 10.1016/j.ajoc.2020.100744. (2) Ugradar S, et al. Eye (Lond). 2020 Nov 21. doi: 10.1038/s41433-020-01297-w. (3) Davis R, et al. NANOS 2021 Feb annual meeting abstract. https://collections.lib.utah.edu/ark:/87278/s6gz077j. (4) Diniz SB, et al. Ophthalmic Plast Reconstr Surg. 2021 Mar 8. doi: 10.1097/IOP.0000000000001959. (5) Ozzello DJ, et al. Orbit. 2021 Jun 1:1-8. doi: 10.1080/01676830.2021.1933081. (6) Ugradar S, et al. Eye (Lond). 2021 Jul 9. doi: 10.1038/s41433-021-01593-z. Note: Data from separate clinical trials may not be directly comparable due to differences in trial protocols, endpoints, conditions and patient populations.
Nu
mb
er o
f TE
PEZ
ZA P
atie
nts
Stu
die
d
41
Chronic Patient Case Studies to Date Acute Patients on TEPEZZA Studied
in Phase 3 Clinical Trial
52
Total Number of Chronic TED Patients Across Case Studies Compared to Number of Acute Patients on TEPEZZA from Phase 3 Clinical Trial
654321Legend (Color-to-Article):

Real World Examples of TEPEZZA in Chronic TED
Before Treatment with TEPEZZA After Treatment with TEPEZZA
TED: Thyroid Eye Disease.Image on right is after 8 TEPEZZA infusions.

First Published Case Report in American Journal of Ophthalmology on TEPEZZA Impact in Chronic TED Patient
TED: Thyroid Eye Disease.Ozzello DJ, et al. Am J Ophthalmol Case Rep. 2020 May 15;19:100744. doi: 10.1016/j.ajoc.2020.100744.

Clinical Trial: A Study Evaluating TEPEZZA Treatment in Patients with Chronic Thyroid Eye Disease; Data Anticipated 2H 2022
Q3W: once every 3 weeks. | TED: Thyroid Eye Disease. | QoL: Quality of Life.
• Change from Baseline at Week 24 in proptosis in the study eye
• roptosis responder rate (% of participants with ≥2-mm reduction from baseline in proptosis in the study eye, without deterioration [≥2-mm increase] of proptosis in the fellow eye) at Week 24
• Additional endpoints on diplopia, QoL, orbital pain, MRI muscle volume
Key Inclusion Criteria
• Initial diagnosis of TED ≥ years but <8 years prior to screening
• Clinical diagnosis of stable, chronic (inactive) TED, as determined by participant medical records indicating a Clinical Activity Score (CAS) ≤1 in both eyes for at least 1 year prior to screening
• CAS ≤1 at the screening and baseline visits
• roptosis ≥ -mm increase from participant’s baseline or roptosis ≥ -mm above normal for race and gender
Randomized, Placebo-Controlled Trial
Safety Follow-Up
57
pat
ien
ts2
:1 r
an
do
miz
ati
on TEPEZZA 10 mg/kg for the first infusion and 20 mg/kg for the remaining 7
infusions Q3W
Placebo
Study Week 0
Week 24Primary Endpoint
Week 45Safety Follow-Up

TEPEZZA: Building the Evidence to Treat More Patients with Chronic TED
TED: Thyroid Eye Disease.
TE E A’s mechanism of action addresses the same underlying pathology in both the acute and chronic TED
Growing body of evidence supporting the use of TEPEZZA in chronic TED
Ongoing clinical trial in patients with chronic TED to establish clinical conviction

Closing Q&A
Sept. 29, 2021 | Horizon R&D Day | 113

Conclusion
Sept. 29, 2021 | Horizon R&D Day | 114

Key Takeaways for Today
(1) Horizon estimate.
We are building a
•
• announced today and starting in 2022
• anticipated in 2021-2023
• in second half of the decade
Horizon is a with best-in-class commercial execution and a rapidly growing pipeline
We are to bolster our ability to continuously innovate
Our current in total peak annual net sales potential(1)

Reconciliations of GAAP to Non-GAAP Measures
Sept. 29, 2021 | Horizon R&D Day | 116

Note Regarding Use of Non-GAAP Financial Measures
EBITDA, or earnings before interest, taxes, depreciation and amortization, and adjusted EBITDA are used and provided by Horizon as non-GAAP financial measures. These non-GAA measures are intended to provide additional information on Horizon’s performance, operations, expenses, profitability and cash flows. Adjustments to Horizon’s GAA figures as well as EBITDA exclude acquisition and/or divestiture-related expenses, gain or loss from divestiture, gain or loss from sale of assets, upfront, progress and milestone payments related to license and collaboration agreements, litigation settlements, loss on debt extinguishment, costs of debt refinancing, drug manufacturing harmonization costs, restructuring and realignment costs, the income tax effect on pre-tax non-GAAP adjustments and other non-GAAP income tax adjustments, as well as non-cash items such as share-based compensation, depreciation and amortization, non-cash interest expense, long-lived asset impairment charges and other non-cash adjustments. Certain other special items or substantive events may also be included in the non-GAAP adjustments periodically when their magnitude is significant within the periods incurred. Horizon maintains an established non-GAAP cost policy that guides the determination of what costs will be excluded in non-GAAP measures. Horizon believes that these non-GAAP financial measures, when considered together with the GAAP figures, can enhance an overall understanding of Horizon’s financial and operating performance. The non-GAAP financial measures are included with the intent of providing investors with a more complete understanding of the Company’s historical and expected 2021 financial results and trends and to facilitate comparisons between periods and with respect to projected information. In addition, these non-GAAP financial measures are among the indicators Horizon’s management uses for planning and forecasting purposes and measuring the Company's performance. For example, adjusted EBITDA is used by Horizon as one measure of management performance under certain incentive compensation arrangements. These non-GAAP financial measures should be considered in addition to, and not as a substitute for, or superior to, financial measures calculated in accordance with GAAP. The non-GAAP financial measures used by the Company may be calculated differently from, and therefore may not be comparable to, non-GAAP financial measures used by other companies. Horizon has not provided a reconciliation of its full-year 2021 adjusted EBITDA outlook to an expected net income (loss) outlook because certain items such as acquisition/divestiture-related expenses and share-based compensation that are a component of net income (loss) cannot be reasonably projected due to the significant impact of changes in Horizon’s stock price, the variability associated with the size or timing of acquisitions/divestitures and other factors. These components of net income (loss) could significantly impact Horizon’s actual net income (loss).

2020 2019 2018
GAAP net income 389,796$ 573,020$ (38,380)$
Depreciation 24,303 6,733 6,126
Amortization and step-up:
Intangible amortization expense 255,148 230,424 243,634
Inventory step-up expense - 89 17,312
Interest expense, net (including amortization of
debt discount and deferred financing costs) 59,616 87,089 121,692
Expense (Benefit) for income taxes 11,849 (593,244) (44,752)
EBITDA 740,712$ 304,111$ 305,632$
Other non-GAAP adjustments:
Acquisition/divestiture-related costs 49,196 3,556 4,396
Restructuring and realignment costs (141) 237 15,350
Impairment of long-lived assets 1,713 - 46,096
(Gain)/Loss on sale of assets (4,883) 10,963 (42,985)
Share-based compensation 146,627 91,215 114,860
Litigation settlements - 1,000 5,750
Upfront, progress and milestone payments related to
license and collaboration agreements 33,000 9,073 (10)
Fees related to refinancing activities 54 2,292 937
Loss on debt extinguishment 31,856 58,835 -
Drug substance harmonization costs 542 457 2,855
Charges relating to discontinuation of Friedreich's ataxia program - 1,076 (1,464)
Total of other non-GAAP adjustments 257,964 178,704 145,785
Adjusted EBITDA 998,676$ 482,815$ 451,417$
Twelve Months Ended December 31,
GAAP to Non-GAAP ReconciliationEBITDA and Adjusted EBITDA – Twelve Months Ended December 31
$ in thousands