VIETNAM STOP TB PARTNERSHIP€¦ · 2012 TB Month with high political commitment GR R9 Phase 2...
19
Seoul, 22-23 November 2012 VIETNAM STOP TB PARTNERSHIP 1. Country TB epidemic 2. Priorities 3. Challenges, Contraints, Gaps 4. Partnership’s contribution
Transcript of VIETNAM STOP TB PARTNERSHIP€¦ · 2012 TB Month with high political commitment GR R9 Phase 2...

Seoul, 22-23 November 2012
VIETNAM STOP TB PARTNERSHIP
1. Country TB epidemic
2. Priorities
3. Challenges, Contraints, Gaps
4. Partnership’s contribution

1. TB epidemiology
225236247259
271283297
311326
341358375
113113114116118120118125120118115116
0
100
200
300
400
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
PrevalenceNotification
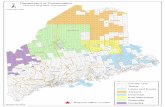
High rate in the south High TB/HIV in HCM city, Mekong river delta Low TB in mountainous, highland areas
Ho Chi Minh City
Tay Ninh An
Giang
Ha Noi
Da Nang

Ranks 12th among 22 TB HBCs Ranks 14th among 27 high MDR-TB burden countries TB prevalence in Viet Nam remains high. 1st National Prevalence Survey (2006-2007) showed that the previous estimation was underestimated by 60%.
A significant number (~40%) of tuberculosis cases remains undiagnosed or unreported.
1. TB epidemiology

2. Priorities
Priorities after Prevalence Survey 2006-2007
Increase case detection is the key PPM – PAL to engage all health care providers Encourage using chest X-ray as screening tool High risk group (closed setting, HIV, diabetes, …) Pilot & expand PMDT Novel multi-modality of A - C - SM Mobilization for local resources

3. Challenges
Human resources – Stigma, low financial compensation, and perceived risk
affect recruitment; lack of sufficient staff results in over-work; in combination these result in high staff turn-over
– Need for training on new approaches and techniques Financial resources
– GVN budget: grossly insufficient, barely covering DOTS – Heavy dependence on external funding for PMDT,
TB/HIV, PPM, ACSM, high risk groups in context of rapidly decreasing funding
– New diagnostic tools: promising but expensive

Example of financial challenge
PMDT Targets driven by financial resources

Challenge Intervention Ss(-) & EPTB increase HIV/TB Relapse/failure/default cases & reTx after default increase
DOT / PMDT
High CNR + poor Tx outcomes in congregate settings
TB control in congregate settings
High Tx success rate, but high prevalence rate and ~40% incident cases untreated each year
+ PPM
Very low CNR among children less than 14 years Childhood TB control
Strengthening of recording/reporting
Programmatic challenges

Programmatic challenges
Challenges Response Reduced international financial support Advocacy Cross-cutting issues of MDRTB, TB/HIV, PPM, closed settings … requires broad engagement of non-NTP partners
Partnership
Diagnostic delay for susceptible and resistant TB, suboptimal treatment adherence
New diagnostic tools, decentralization, shorter regimen, addl community engagement
Access barriers in mountainous areas ACF, ACSM, community DOT
SLD management Drug supply & Forcasting
Shortage of HR More incentives ($, training)
Accessibiltity (Patient charge) + Health insurance

Funding levels & gaps, 2013-15
Financial Need (USD) 2013 2,014 2,015 Total
Objective 1: High quality DOTS 48,557,537 54,067,373 49,350,967 151,975,876
Objective 2: TB/HIV, MDR-TB, Closed settings 6,449,221 7,254,870 8,267,339 21,971,429
Objective 3: HSS 3,445,845 4,310,847 4,487,344 12,244,036
Objective 4: PPM 2,814,085 2,164,900 2,154,153 7,133,138
Objective 5: ACSM 4927475 4934582 4633739 14,495,796
Objective 6: Surveillance and research 393,000 1,577,764 435,000 2,405,764
Total (in US$s) 66,587,162 74,310,335 69,328,542 210,226,039

Funding levels & gaps, 2013-15
Financial Gap (USD) 2013 2014 2015 Total
Funding needs 2013-2015 66,587,162 74,310,335 69,328,542 210,226,039
Estimated fund
Central Gov’t budget 5,500,000 6,000,000 6,500,000 18,000,000
Provincial Gov’t Fund 4,741,607 5,435,115 6,152,621 16,329,343
Global Fund 10,503,688 10,616,383 11,495,842 32,615,913
TB CARE I (PEPFAR) 3,900,171 3,900,171 3,900,171 9,600,342
EXPAND TB In-kind n/a n/a
CDC (PEPFAR) 293,000 293,000 293,000 879,000
Total in US$ 24,938,466 26,244,669 28,341,634 79,524,769
Funding Gap, US $ 41,648,696 48,065,666 40,986,908 130,701,270

VSTP Establishment as an utmost important solution for NTP
Initial concept and reason for formation: 2008
First formal VSTP meeting: April 2010, followed by regular
quarterly meetings
Strong support from MOH and local partners, now over 39
Host organization and legal status:
Vietnam Association Against TB and Lung Diseases - VATLD


13

14
18th
COORDINATIN
G BOARD
MEETING OF
THE STOP TB
PARTNERSHIP

VSTP’s Partners
Partners # members National Lung Hospital / NTP
WHO – Vietnam Office
Women’s Union ~ 14 million
Farmers’ Union > 10 million
Red Cross > 10 million
Youth Union > 6 million
Veteran’s Association > 3.5 million Other NGO/CBO/Academic and bilateral/multilateral organizations: Vietnam Association Against Tuberculosis and Lung Diseases, CDC, USAID, KNCV, MCNV, PATH, URC, FHI, PSI, University of California San Francisco, Woolcock Medical Research Institute
Other VN government organizations: Ministry of Health, Ministry of Public Security, Ministry of Labour-Invalids and Social Affairs, Ministry of Education and Training, Viet Nam Administration of HIV/AIDS Control, National Institute for Hygiene and Epidemiology
Private sector: Ha Noi Association of Private Medical Practitioners, Hai Duong Association of Private Practitioners, Hung Thinh Pharmaceutical and Medical J.S. Company, METRO Cash & Carry Company

4. Partnership’s contribution
Technical & policy advisory role to NTP Information sharing and improved coordination & collaboration
Support to NTP in developing & implementing solutions for challenges Initiate priority focus to develop ACSM and PPM advisory networks among VSTP partners Financial and technical resource mobilization from local and international organizations Quarterly full partnership meetings, TWG meetings, ad hoc one-on-one meetings

4. Partnership’s contribution
GR R9 proposal development (~60 mil. $)
NTP 2007-2011 mid-term & end-term evaluations
National TB Control Strategy 2011-2015
2012 TB Month with high political commitment
GR R9 Phase 2 proposal development
National TB Control Strategy to 2020, vision 2030
Engage business sector in Tb control

18

19