VARIANCE(AND(SCOPE(OF(DESTRUCTION( IN(DELIVERYOF...
20
VARIANCE AND SCOPE OF DESTRUCTION IN DELIVERY OF RENAL CARE DURING CONFLICTS MEMA, AUB 2017 MOHAMED SEKKARIE, MD. MPH
Transcript of VARIANCE(AND(SCOPE(OF(DESTRUCTION( IN(DELIVERYOF...

VARIANCE AND SCOPE OF DESTRUCTION IN DELIVERY OF RENAL CARE DURING
CONFLICTS
MEMA, AUB 2017MOHAMED SEKKARIE, MD. MPH

Kidney Diseases
• Chronic Kidney disease (CKD) stage 1-‐5• Acute Kidney Injury• Acute on Chronic KD• Hypertension, Electrolyte problems, Related minerals and bone disorders , Anemia of CKD
• Primary and secondary preventions are more effective but in disasters situations these are usually ignored

The Worldwide Burden of CKD
• Prevalence of CKD: 13.4%• In 2010, 2.6 million people received RRT (HD, PD, TXP) for
• ESRD Patients needing RRT: 4.9 -‐ 9.7 million• Strong relationship between RRT prevalence & per capita income ( range < 10 to 3000 / M)
• Prevalence = Incidence X Duration (Coresh, J., 2017. Update on the Burden of CKD. JASN, 28(4))

Prevalence of ESRD in Syria
• Dialysis: 143 per million in 2005 (Saeed, B., Derani, R et al. 2007. Organ failure in Syria. Saudi Journal of Kidney Diseases and Transplantation)
• Dialysis: 189 per million in 2015 among Syrian refugees in Jordan
(Isreb B, Kaysi S, Rifai A, Al Kukhun H, Sultan Al-‐Adwan S, Kass-‐Hout T , Sekkarie M. 2017. The Effect of War on Syrian Refugees with ESRD. KI reports)

The Geographical Variation of Support to ESRD Patients in the Syrian Conflict• Inside Syria – Government areas (some preservation of the old system)
– Non-‐government areas ( NGO’s access)– Besieged areas (very limited access)
• Refugees

REQUIREMENTS FOR THE PROVISION OF RRT
• Human Resources• Dialysis clinics• Supplies • Medications• Safe routes• Utilities• Hospitals• Money

Literature Review ( PubMed)
• Twelve reports ( descriptive studies, letter to the editor, cover stories) up to October 2015
• HD, PD and Transplant• Wars: Kuwait, Iraq, Balkans, Afghanistan, Syria
• Isreb, M.A., Rifai, A.O., Murad, L.B., Al-‐Makki, A., Al-‐Saghir, F. and Sekkarie, M.A., 2016. Care and outcomes of end-‐stage kidney disease patients in times of armed conflict: recommendations for action.
Kuwait• Doctors: 20 to 5, Nurses: 97 to 11• Restriction of HD treatment hours• Nearly half of those patients who remained in Kuwait died
during the period of occupation (12.7% of those who left)• Failure to reach dialysis centers was a major cause of death• The incidence of new ESRD Kuwaiti patients entering dialysis
program during the occupation period and soon afterwards was only 37 per million Kuwaiti population compared to 60 per million in the previous years.
• El-‐Reshaid, K., Johny, K.V., Georgous, M., Nampoory, M.R.N. and Al-‐Hilal, N., 1993. The impact of Iraqi occupation on end-‐stage renal disease patients in Kuwait, 1990–1991.Nephrology Dialysis Transplantation, 8(1), pp.7-‐10.
The Balkans• Albania the host country: 1 hemodialysis center, 5 HD
machines, a total of 20 patients• New patients are admitted only if one of the established
patients dies or receives a kidney• Decided to treat all 75 refugees from Kosovo• 25 patients evacuated to Italy, 15 to Austria, 35 remain and
treated with donated machines, supplies, and visiting providers from France
• 2/5 refugees transplant recipient dies• 2 PD patients had to switch to HD due to infection
Barbullushi, M., Koroshi, A. and Tase, M., 2000. Albanian contribution to the treatment of refugee renal patients from Kosovo.Nephrology Dialysis Transplantation, 15(8), pp.1261-‐1261
Transplant in Syria• In Syria, the number of annual kidney transplants declined
from 385 in 2010 to 154 in 2013 (60%)
• The number of operational kidney transplant centers has decreased from 8 to 4 centers
• Difficulties in securing anti-‐rejection medications
Saeed B. The effect of the Syrian crisis on organ transplantation in Syria. ExpClin Transplant. 2015; 13: 206-‐208.
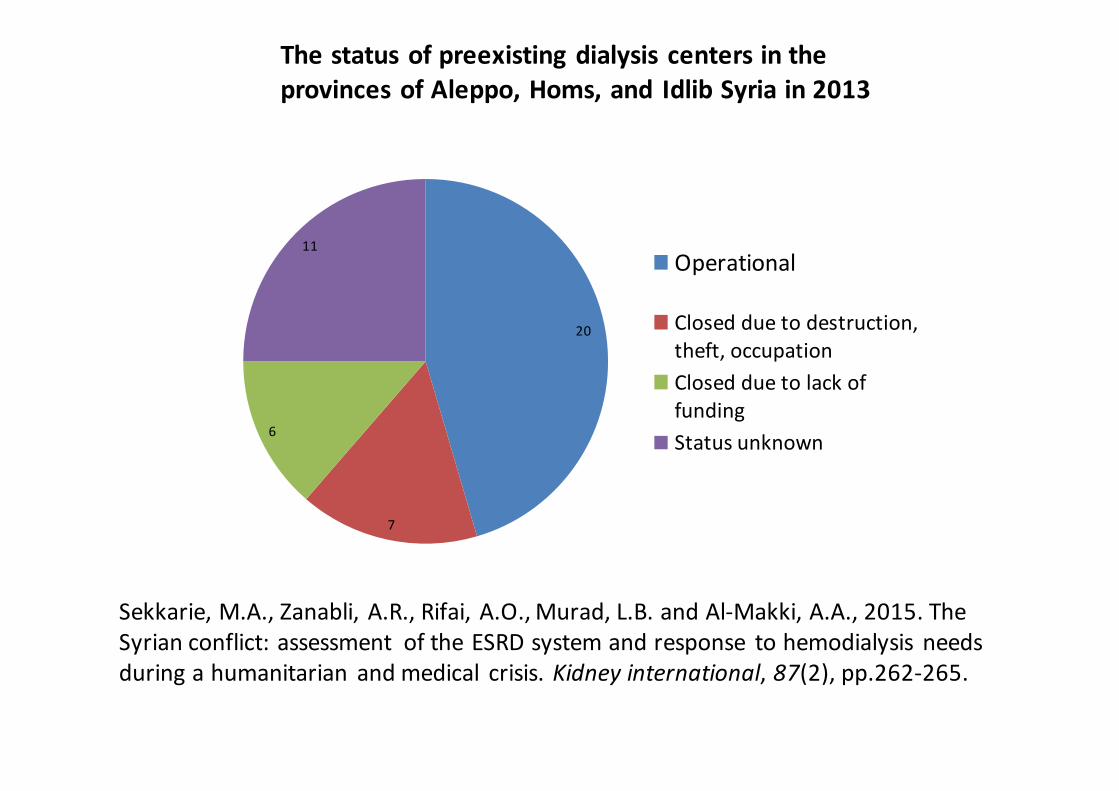
The status of preexisting dialysis centers in the provinces of Aleppo, Homs, and Idlib Syria in 2013
20
7
6
11Operational
Closed due to destruction, theft, occupationClosed due to lack of fundingStatus unknown
Sekkarie, M.A., Zanabli, A.R., Rifai, A.O., Murad, L.B. and Al-‐Makki, A.A., 2015. The Syrian conflict: assessment of the ESRD system and response to hemodialysis needs during a humanitarian and medical crisis. Kidney international, 87(2), pp.262-‐265.

Patient-‐related processes and outcomes in non-‐government areas• For many patients, blood transfusion was the only method for anemia management
• Many essential tests not available• It is common for the same patient to receive dialysis at more than one center according to safety concerns and functionality of the center
• Outdated machines• Inadequate water treatment• Most facilities had no nephrologist

Interruption of Dialysis
• Death of about half of 35 patients in 2011 from lack of dialysis after the occupation and closure of a hospital based dialysis facility by armed forces
• In one dialysis center, all 18 patients reported going at least one week without dialysis because of inability to get to a clinic
• Many patients reported various forms of harassment at checkpoints that led to inability to access facilities; confiscation of dialysis supplies, and abuse

Isreb, M., Alyousef, M., Obaid, N., Abbara, A. and Sekkarie, M., 2016. Effect of besiegement on non-‐communicable diseases: haemodialysis. The Lancet, 388(10058), p.2350.

YEMEN

Health workers and the weaponisation of health care in
Syria
a preliminary inquiry for The Lancet-‐American University of Beirut
Commission on Syria.Lancet. 2017 Mar 14. Fouad et al.



Conclusions
Patients with kidney disease during conflicts face:• The usual problems kidney disease patients face
• Difficulties resulting from limited resources • Unique issues related to lack of safe routes and war damages to themselves, providers and facilities