Valvular Heart Disease Dr. Raid Jastania. Valvular Heart Disease Congenital or Acquired Part of...
21
Valvular Heart Disease Dr. Raid Jastania
-
date post
22-Dec-2015 -
Category
Documents
-
view
222 -
download
2
Transcript of Valvular Heart Disease Dr. Raid Jastania. Valvular Heart Disease Congenital or Acquired Part of...
Valvular Heart Disease
Dr. Raid Jastania

Valvular Heart Disease
• Congenital or Acquired
• Part of congenital heart diseases
• May involve any valve: Aortic, Mitral, Pulmonary, Tricuspid

Valvular Heart Disease
• Types of Diseases:– Stenosis– Regurgitation– Endocarditis

Pathological Mechanisms of valve diseases
• Primary– Congenital/Developmental defect– Acquired Pathological process
• Infection: endocarditis• Immune disorder: Rheumatic heart disease• Degenerative (Aging) changes
• Secondary– LV dilatation– Abnormality of papillary muscle

Case
• A ten-year-old child was brought to a pediatrician because of a mild sore throat. The pediatrician noticed some redness, swabbed her throat, tested for group A streptococci in the office, sent blood for antistreptolysin O titer, and prescribed treatment.
• Three weeks later, the child returned with fever and painful swelling of the knee joints, followed by pain and swelling of elbow joints.

• Physical examination revealed a pericardial friction rub and a murmur suggestive of mitral regurgitation. The antistreptolysin O titer was elevated over the previous value. The child was hospitalized and treated with antibiotics and anti-inflammatory drugs. The patient recovered and did well over the next several decades.

• In her thirties, the patient began to have dyspnea on exertion, which slowly increased in severity in her forties. In the months prior to her hospital admission for this and related symptoms, she had awakened at night feeling short of breath. She had one fainting spell, followed by an episode of temporary loss of vision in one eye. On admission to the hospital, she was very short of breath and had coughed up some blood-tinged sputum.
• Physical examination and laboratory tests suggested narrowing of the mitral valve orifice. X-ray of her chest showed an enlarged left atrium and pulmonary edema. Cardiac surgery was offered, but she refused. She was treated medically for several days and discharged, feeling better but with some residual limitation of cardiac function.
• The week before her next admission, she went to a dentist because of tooth pain, and underwent a dental extraction. She returned to the hospital with high spiking fevers and overt signs and symptoms of heart failure.
Rheumatic Fever and Heart disease
• Acute inflammatory disease• Affecting different tissues and systems: Heart,
joints, serosal surfaces, skin…• Immune mediated• Follow pharyngitis with GroupA streptococcal
infection• Few weeks after resolution of infection• Antibody against M-protein of GroupA strep• Cross-reaction with self antigen

Rheumatic Fever and Heart disease
• <3% of GroupA strep phayngitis• Genetic susceptibility • Age affected 5-15 years• Positive anti streptolysinO, or DNAse B• Fever• Arthritis: migratory, large joints• Carditis: pericarditis, pericardial effusion,
myocarditis• CHF
Rheumatic Fever and Heart disease
• Recurrence of acute illness• Progress to chronic Rheumatic heart disease
– Years after the acute illness– Valve disease: commonly mitral stenosis and aortic
stenosis
• Complications: – CHF– Arrhythmia (atrial fibrillation)– Infective endocarditis– Thromboembolism
Rheumatic Fever and Heart disease
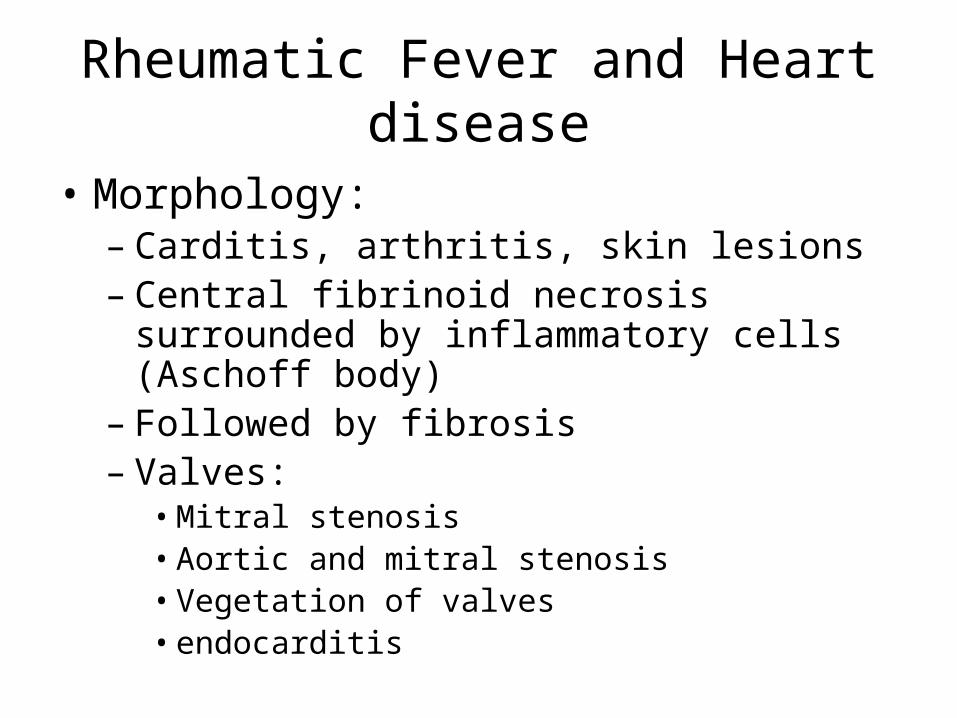
• Morphology:– Carditis, arthritis, skin lesions– Central fibrinoid necrosis surrounded by
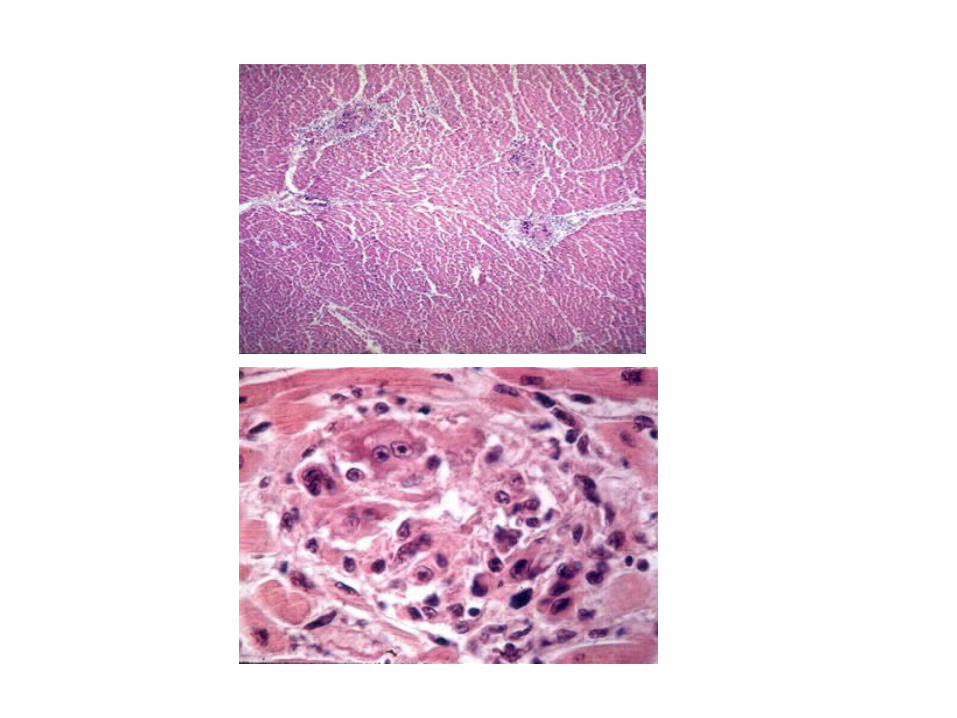
inflammatory cells (Aschoff body)– Followed by fibrosis– Valves:
• Mitral stenosis• Aortic and mitral stenosis• Vegetation of valves• endocarditis
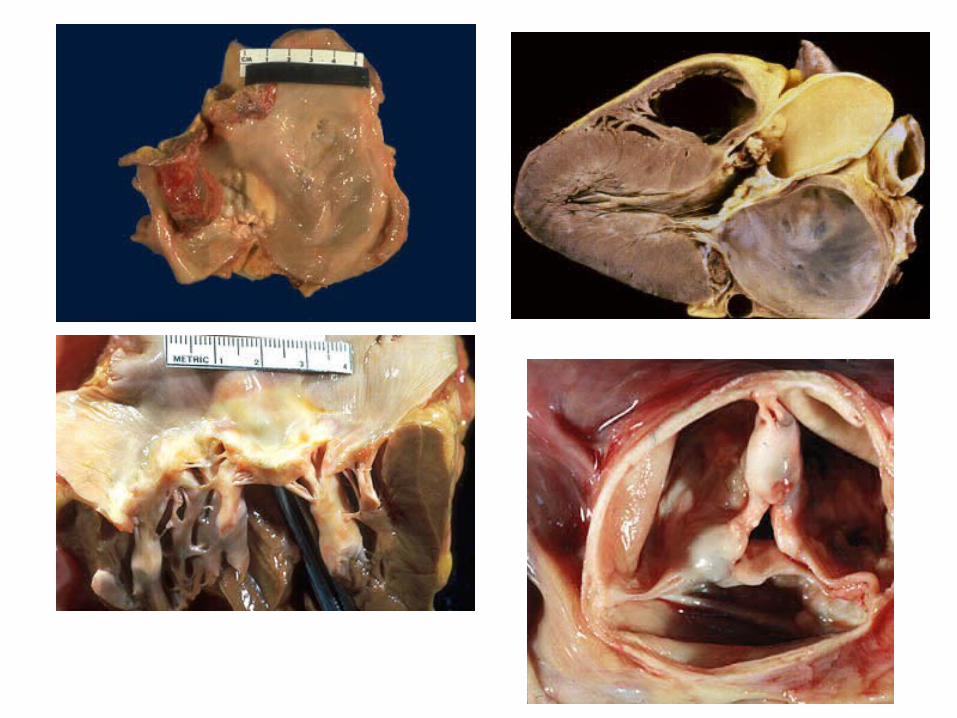

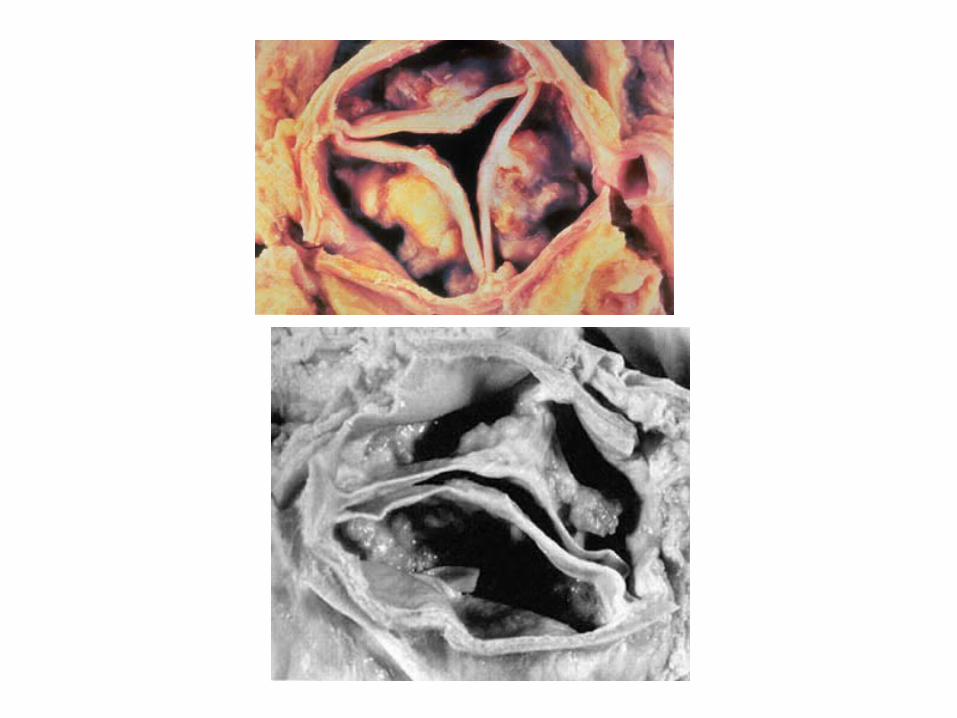
Degenerative Valve DiseaseCalcific Aortic Stenosis
• Degeneration is aging process• End by fibrosis and calcification• Common cause of isolated aortic stenosis• Affect mitral valve as well, but usually
does not result in functional abnormality• Fatigue, syncope, systolic murmur• L.V hypertrophy, ischemia, angina• CHF

Mitral Valve Prolapse
• 3-5% of the general population
• Discovered between 20-40 years
• Accumulation of loose ground substance in the leaflets and cordae of mitral valve
• Floppy valve
• Ballooning of the valve to the left atrium during systole

Mitral Valve Prolapse
• Usually asymptomatic
• Midsystolic click
• Fatigue, chest pain
• 3% develop complications– Mitral regurgitation– CHF– Infective endocarditis– Thromboembolism







![Severe valvular and congenital heart diseases in adults€¦ · term condition] scheme, severe valvular heart disease. Valvular heart diseases are very diverse and require different](https://static.fdocuments.us/doc/165x107/600678272dffc94bfc1e40e5/severe-valvular-and-congenital-heart-diseases-in-term-condition-scheme-severe.jpg)