Unusual glioma
52
Unusual Gliomas Dr vardan kulshreshtha M.cH Resident – final year Deptt. Of Neurosurgery RNT Medical College , Udaipur, INDIA 10/20/2016 1 unusual giomas
-
Upload
drvardan-ku -
Category
Health & Medicine
-
view
166 -
download
0
Transcript of Unusual glioma
Unusual Gliomas
Dr vardan kulshreshthaMcH Resident ndash final year
Deptt Of NeurosurgeryRNT Medical College Udaipur INDIA
10202016 1unusual giomas
bull These tumor deserve special considerationbull These are rare and there behaviour and
natural history is still largely less knownbull Many of these have indolent growth and
commonly reach to attention due to epilepsybull Routine use of IHC and genetic assay have led
to some understanding
10202016 2unusual giomas
Subependymal Giant Cell Astrocytomabull WHO grade 1bull Generally occur in
patients with tuberoussclerosis
bull Typical location isintraventricular
bull Present with features ofraised ICP andobstructive HCP
bull TUBEROUS Sclerosis isan autosomal dominantdisease
bull Mental retardationseizures adenomassebaceum
bull Altered skinpigmentations retinaltumors subungualfibromas tumors ofpancreas and spleen
10202016 3unusual giomas
Pathologybull Rarely undiagnosedbull Found typically in
intraventricular locationsbull Typical appearance of giant
cells mixed with cells ofastrocyte lineage
bull Well demarcated tumorswith modest infilteartioninto surrounding whitematter
bull Giant cells with abundanteosinophilic cytoplasm andspindle shaped nuclei
bull Mitoses nuclear atypianecrosis endothelialproliferation withaggressive behaviour
bull Anaplastic transformationis rare
bull IHC marker show positivityfor GFAP AND S-100
10202016 4unusual giomas
Imaging
bull CT demonstratescalcification as well ascontrast enhancement
10202016 5unusual giomas
MRI
bull Isointense tohypointense on T1 massin the periventricularlocation
bull Hyperintense signal onT2 WI
bull Strongly enhancedsignals on post contrast
10202016 6unusual giomas
Management
bull Do not require interventionunless bolck the foramen ofmonroe
bull Primary treatment issurgical total resection
bull Subtotal resection may beadequate in case totalresection is hazardous
bull Tumor rarely becomesaggressive
bull Tarnscortical transcallosalapproach
bull If surgery not possible ordenied by pt thenmanagement of HCP byshunt
bull Role of chemotherapy hasshown promises
10202016 7unusual giomas
Everolimus for Subependymal Giant-Cell Astrocytomas in Tuberous SclerosisDarcy A Krueger MD PhD Marguerite M Care MD Katherine Holland MD PhD KarenAgricola FNP Cynthia Tudor PNP Prajakta Mangeshkar MS Kimberly A Wilson MSAnna Byars PhD Tarek Sahmoud MD PhD and David Neal Franz MDN Engl J Med 2010 3631801-181
bull Backgroundbull Neurosurgical resection is the standard treatment for subependymal giant-cell astrocytomas in patients with the tuberous
sclerosis complex An alternative may be the use of everolimus which inhibits the mammalian target of rapamycin a protein regulated by gene products involved in the tuberous sclerosis complex
bull Methodsbull Patients 3 years of age or older with serial growth of subependymal giant-cell astrocytomas were eligible for this open-label
study The primary efficacy end point was the change in volume of subependymal giant-cell astrocytomas between baseline and 6 months We gave everolimus orally at a dose of 30 mg per square meter of body-surface area to achieve a trough concentration of 5 to 15 ng per milliliter
bull Resultsbull We enrolled 28 patients Everolimus therapy was associated with a clinically meaningful reduction in volume of the
primary subependymal giant-cell astrocytoma as assessed on independent central review (Plt0001 for baseline vs 6 months) with a reduction of at least 30 in 21 patients (75) and at least 50 in 9 patients (32) Marked reductions were seen within 3 months and were sustained There were no new lesions worsening hydrocephalus evidence of increased intracranial pressure or necessity for surgical resection or other therapy for subependymal giant-cell astrocytoma Of the 16 patients for whom 24-hour video electroencephalography data were available seizure frequency for the 6-month study period (vs the previous 6-month period) decreased in 9 did not change in 6 and increased in 1 (median change minus1 seizure P=002) The mean (plusmnSD) score on the validated Quality-of-Life in Childhood Epilepsy questionnaire (on which scores can range from 0 to 100 with higher scores indicating a better quality of life) was improved at 3 months (634plusmn124) and 6 months (621plusmn142) over the baseline score (578plusmn140) Single cases of grade 3 treatment-related sinusitis pneumonia viral bronchitis tooth infection stomatitis and leukopenia were reported
bull Conclusionsbull Everolimus therapy was associated with marked reduction in the volume of subependymal giant-cell
astrocytomas and seizure frequency and may be a potential alternative to neurosurgical resection in some cases though long-term studies are needed
10202016 8unusual giomas
Angiocentric glioma
bull Described by WHO in2005
bull Initially included withastroblastoma andchoroid glioma
bull Mean age at diagnosis is17 years
bull Pts present with longhistory of seizures
bull Microscopically show themonomorphous bipolarcells associated withnormal vessels of thecortex and white matter
bull Tumor cells are spindleshaped
bull Mitoses are rarebull Positive for S-100 GFAP
vimentin
10202016 9unusual giomas
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull These tumor deserve special considerationbull These are rare and there behaviour and
natural history is still largely less knownbull Many of these have indolent growth and
commonly reach to attention due to epilepsybull Routine use of IHC and genetic assay have led
to some understanding
10202016 2unusual giomas
Subependymal Giant Cell Astrocytomabull WHO grade 1bull Generally occur in
patients with tuberoussclerosis
bull Typical location isintraventricular
bull Present with features ofraised ICP andobstructive HCP
bull TUBEROUS Sclerosis isan autosomal dominantdisease
bull Mental retardationseizures adenomassebaceum
bull Altered skinpigmentations retinaltumors subungualfibromas tumors ofpancreas and spleen
10202016 3unusual giomas
Pathologybull Rarely undiagnosedbull Found typically in
intraventricular locationsbull Typical appearance of giant
cells mixed with cells ofastrocyte lineage
bull Well demarcated tumorswith modest infilteartioninto surrounding whitematter
bull Giant cells with abundanteosinophilic cytoplasm andspindle shaped nuclei
bull Mitoses nuclear atypianecrosis endothelialproliferation withaggressive behaviour
bull Anaplastic transformationis rare
bull IHC marker show positivityfor GFAP AND S-100
10202016 4unusual giomas
Imaging
bull CT demonstratescalcification as well ascontrast enhancement
10202016 5unusual giomas
MRI
bull Isointense tohypointense on T1 massin the periventricularlocation
bull Hyperintense signal onT2 WI
bull Strongly enhancedsignals on post contrast
10202016 6unusual giomas
Management
bull Do not require interventionunless bolck the foramen ofmonroe
bull Primary treatment issurgical total resection
bull Subtotal resection may beadequate in case totalresection is hazardous
bull Tumor rarely becomesaggressive
bull Tarnscortical transcallosalapproach
bull If surgery not possible ordenied by pt thenmanagement of HCP byshunt
bull Role of chemotherapy hasshown promises
10202016 7unusual giomas
Everolimus for Subependymal Giant-Cell Astrocytomas in Tuberous SclerosisDarcy A Krueger MD PhD Marguerite M Care MD Katherine Holland MD PhD KarenAgricola FNP Cynthia Tudor PNP Prajakta Mangeshkar MS Kimberly A Wilson MSAnna Byars PhD Tarek Sahmoud MD PhD and David Neal Franz MDN Engl J Med 2010 3631801-181
bull Backgroundbull Neurosurgical resection is the standard treatment for subependymal giant-cell astrocytomas in patients with the tuberous
sclerosis complex An alternative may be the use of everolimus which inhibits the mammalian target of rapamycin a protein regulated by gene products involved in the tuberous sclerosis complex
bull Methodsbull Patients 3 years of age or older with serial growth of subependymal giant-cell astrocytomas were eligible for this open-label
study The primary efficacy end point was the change in volume of subependymal giant-cell astrocytomas between baseline and 6 months We gave everolimus orally at a dose of 30 mg per square meter of body-surface area to achieve a trough concentration of 5 to 15 ng per milliliter
bull Resultsbull We enrolled 28 patients Everolimus therapy was associated with a clinically meaningful reduction in volume of the
primary subependymal giant-cell astrocytoma as assessed on independent central review (Plt0001 for baseline vs 6 months) with a reduction of at least 30 in 21 patients (75) and at least 50 in 9 patients (32) Marked reductions were seen within 3 months and were sustained There were no new lesions worsening hydrocephalus evidence of increased intracranial pressure or necessity for surgical resection or other therapy for subependymal giant-cell astrocytoma Of the 16 patients for whom 24-hour video electroencephalography data were available seizure frequency for the 6-month study period (vs the previous 6-month period) decreased in 9 did not change in 6 and increased in 1 (median change minus1 seizure P=002) The mean (plusmnSD) score on the validated Quality-of-Life in Childhood Epilepsy questionnaire (on which scores can range from 0 to 100 with higher scores indicating a better quality of life) was improved at 3 months (634plusmn124) and 6 months (621plusmn142) over the baseline score (578plusmn140) Single cases of grade 3 treatment-related sinusitis pneumonia viral bronchitis tooth infection stomatitis and leukopenia were reported
bull Conclusionsbull Everolimus therapy was associated with marked reduction in the volume of subependymal giant-cell
astrocytomas and seizure frequency and may be a potential alternative to neurosurgical resection in some cases though long-term studies are needed
10202016 8unusual giomas
Angiocentric glioma
bull Described by WHO in2005
bull Initially included withastroblastoma andchoroid glioma
bull Mean age at diagnosis is17 years
bull Pts present with longhistory of seizures
bull Microscopically show themonomorphous bipolarcells associated withnormal vessels of thecortex and white matter
bull Tumor cells are spindleshaped
bull Mitoses are rarebull Positive for S-100 GFAP
vimentin
10202016 9unusual giomas
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Subependymal Giant Cell Astrocytomabull WHO grade 1bull Generally occur in
patients with tuberoussclerosis
bull Typical location isintraventricular
bull Present with features ofraised ICP andobstructive HCP
bull TUBEROUS Sclerosis isan autosomal dominantdisease
bull Mental retardationseizures adenomassebaceum
bull Altered skinpigmentations retinaltumors subungualfibromas tumors ofpancreas and spleen
10202016 3unusual giomas
Pathologybull Rarely undiagnosedbull Found typically in
intraventricular locationsbull Typical appearance of giant
cells mixed with cells ofastrocyte lineage
bull Well demarcated tumorswith modest infilteartioninto surrounding whitematter
bull Giant cells with abundanteosinophilic cytoplasm andspindle shaped nuclei
bull Mitoses nuclear atypianecrosis endothelialproliferation withaggressive behaviour
bull Anaplastic transformationis rare
bull IHC marker show positivityfor GFAP AND S-100
10202016 4unusual giomas
Imaging
bull CT demonstratescalcification as well ascontrast enhancement
10202016 5unusual giomas
MRI
bull Isointense tohypointense on T1 massin the periventricularlocation
bull Hyperintense signal onT2 WI
bull Strongly enhancedsignals on post contrast
10202016 6unusual giomas
Management
bull Do not require interventionunless bolck the foramen ofmonroe
bull Primary treatment issurgical total resection
bull Subtotal resection may beadequate in case totalresection is hazardous
bull Tumor rarely becomesaggressive
bull Tarnscortical transcallosalapproach
bull If surgery not possible ordenied by pt thenmanagement of HCP byshunt
bull Role of chemotherapy hasshown promises
10202016 7unusual giomas
Everolimus for Subependymal Giant-Cell Astrocytomas in Tuberous SclerosisDarcy A Krueger MD PhD Marguerite M Care MD Katherine Holland MD PhD KarenAgricola FNP Cynthia Tudor PNP Prajakta Mangeshkar MS Kimberly A Wilson MSAnna Byars PhD Tarek Sahmoud MD PhD and David Neal Franz MDN Engl J Med 2010 3631801-181
bull Backgroundbull Neurosurgical resection is the standard treatment for subependymal giant-cell astrocytomas in patients with the tuberous
sclerosis complex An alternative may be the use of everolimus which inhibits the mammalian target of rapamycin a protein regulated by gene products involved in the tuberous sclerosis complex
bull Methodsbull Patients 3 years of age or older with serial growth of subependymal giant-cell astrocytomas were eligible for this open-label
study The primary efficacy end point was the change in volume of subependymal giant-cell astrocytomas between baseline and 6 months We gave everolimus orally at a dose of 30 mg per square meter of body-surface area to achieve a trough concentration of 5 to 15 ng per milliliter
bull Resultsbull We enrolled 28 patients Everolimus therapy was associated with a clinically meaningful reduction in volume of the
primary subependymal giant-cell astrocytoma as assessed on independent central review (Plt0001 for baseline vs 6 months) with a reduction of at least 30 in 21 patients (75) and at least 50 in 9 patients (32) Marked reductions were seen within 3 months and were sustained There were no new lesions worsening hydrocephalus evidence of increased intracranial pressure or necessity for surgical resection or other therapy for subependymal giant-cell astrocytoma Of the 16 patients for whom 24-hour video electroencephalography data were available seizure frequency for the 6-month study period (vs the previous 6-month period) decreased in 9 did not change in 6 and increased in 1 (median change minus1 seizure P=002) The mean (plusmnSD) score on the validated Quality-of-Life in Childhood Epilepsy questionnaire (on which scores can range from 0 to 100 with higher scores indicating a better quality of life) was improved at 3 months (634plusmn124) and 6 months (621plusmn142) over the baseline score (578plusmn140) Single cases of grade 3 treatment-related sinusitis pneumonia viral bronchitis tooth infection stomatitis and leukopenia were reported
bull Conclusionsbull Everolimus therapy was associated with marked reduction in the volume of subependymal giant-cell
astrocytomas and seizure frequency and may be a potential alternative to neurosurgical resection in some cases though long-term studies are needed
10202016 8unusual giomas
Angiocentric glioma
bull Described by WHO in2005
bull Initially included withastroblastoma andchoroid glioma
bull Mean age at diagnosis is17 years
bull Pts present with longhistory of seizures
bull Microscopically show themonomorphous bipolarcells associated withnormal vessels of thecortex and white matter
bull Tumor cells are spindleshaped
bull Mitoses are rarebull Positive for S-100 GFAP
vimentin
10202016 9unusual giomas
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Pathologybull Rarely undiagnosedbull Found typically in
intraventricular locationsbull Typical appearance of giant
cells mixed with cells ofastrocyte lineage
bull Well demarcated tumorswith modest infilteartioninto surrounding whitematter
bull Giant cells with abundanteosinophilic cytoplasm andspindle shaped nuclei
bull Mitoses nuclear atypianecrosis endothelialproliferation withaggressive behaviour
bull Anaplastic transformationis rare
bull IHC marker show positivityfor GFAP AND S-100
10202016 4unusual giomas
Imaging
bull CT demonstratescalcification as well ascontrast enhancement
10202016 5unusual giomas
MRI
bull Isointense tohypointense on T1 massin the periventricularlocation
bull Hyperintense signal onT2 WI
bull Strongly enhancedsignals on post contrast
10202016 6unusual giomas
Management
bull Do not require interventionunless bolck the foramen ofmonroe
bull Primary treatment issurgical total resection
bull Subtotal resection may beadequate in case totalresection is hazardous
bull Tumor rarely becomesaggressive
bull Tarnscortical transcallosalapproach
bull If surgery not possible ordenied by pt thenmanagement of HCP byshunt
bull Role of chemotherapy hasshown promises
10202016 7unusual giomas
Everolimus for Subependymal Giant-Cell Astrocytomas in Tuberous SclerosisDarcy A Krueger MD PhD Marguerite M Care MD Katherine Holland MD PhD KarenAgricola FNP Cynthia Tudor PNP Prajakta Mangeshkar MS Kimberly A Wilson MSAnna Byars PhD Tarek Sahmoud MD PhD and David Neal Franz MDN Engl J Med 2010 3631801-181
bull Backgroundbull Neurosurgical resection is the standard treatment for subependymal giant-cell astrocytomas in patients with the tuberous
sclerosis complex An alternative may be the use of everolimus which inhibits the mammalian target of rapamycin a protein regulated by gene products involved in the tuberous sclerosis complex
bull Methodsbull Patients 3 years of age or older with serial growth of subependymal giant-cell astrocytomas were eligible for this open-label
study The primary efficacy end point was the change in volume of subependymal giant-cell astrocytomas between baseline and 6 months We gave everolimus orally at a dose of 30 mg per square meter of body-surface area to achieve a trough concentration of 5 to 15 ng per milliliter
bull Resultsbull We enrolled 28 patients Everolimus therapy was associated with a clinically meaningful reduction in volume of the
primary subependymal giant-cell astrocytoma as assessed on independent central review (Plt0001 for baseline vs 6 months) with a reduction of at least 30 in 21 patients (75) and at least 50 in 9 patients (32) Marked reductions were seen within 3 months and were sustained There were no new lesions worsening hydrocephalus evidence of increased intracranial pressure or necessity for surgical resection or other therapy for subependymal giant-cell astrocytoma Of the 16 patients for whom 24-hour video electroencephalography data were available seizure frequency for the 6-month study period (vs the previous 6-month period) decreased in 9 did not change in 6 and increased in 1 (median change minus1 seizure P=002) The mean (plusmnSD) score on the validated Quality-of-Life in Childhood Epilepsy questionnaire (on which scores can range from 0 to 100 with higher scores indicating a better quality of life) was improved at 3 months (634plusmn124) and 6 months (621plusmn142) over the baseline score (578plusmn140) Single cases of grade 3 treatment-related sinusitis pneumonia viral bronchitis tooth infection stomatitis and leukopenia were reported
bull Conclusionsbull Everolimus therapy was associated with marked reduction in the volume of subependymal giant-cell
astrocytomas and seizure frequency and may be a potential alternative to neurosurgical resection in some cases though long-term studies are needed
10202016 8unusual giomas
Angiocentric glioma
bull Described by WHO in2005
bull Initially included withastroblastoma andchoroid glioma
bull Mean age at diagnosis is17 years
bull Pts present with longhistory of seizures
bull Microscopically show themonomorphous bipolarcells associated withnormal vessels of thecortex and white matter
bull Tumor cells are spindleshaped
bull Mitoses are rarebull Positive for S-100 GFAP
vimentin
10202016 9unusual giomas
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
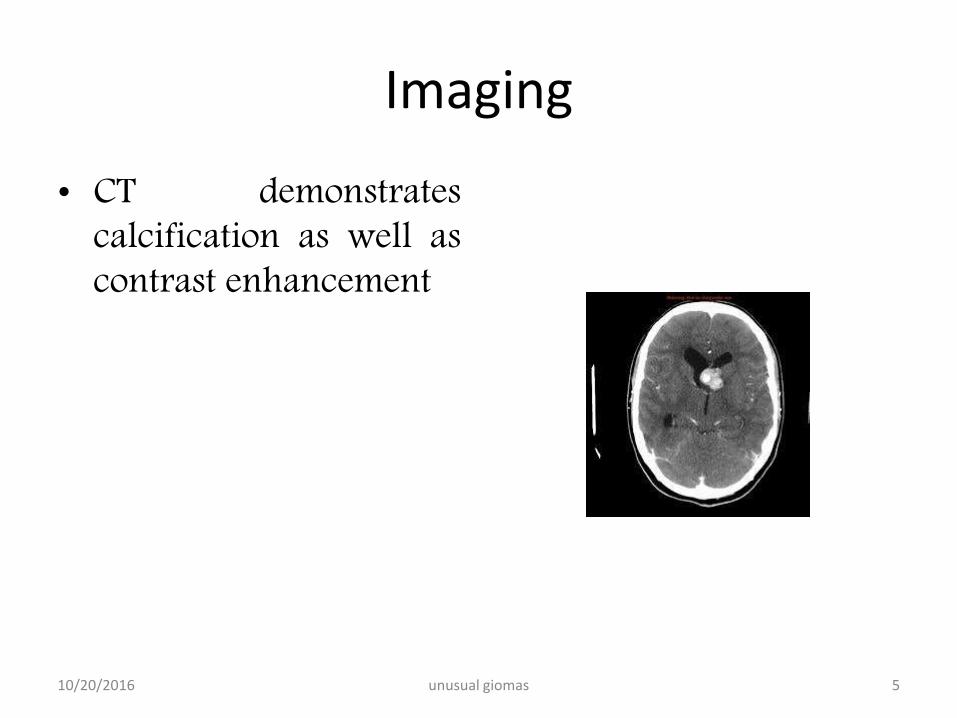
Imaging
bull CT demonstratescalcification as well ascontrast enhancement
10202016 5unusual giomas
MRI
bull Isointense tohypointense on T1 massin the periventricularlocation
bull Hyperintense signal onT2 WI
bull Strongly enhancedsignals on post contrast
10202016 6unusual giomas
Management
bull Do not require interventionunless bolck the foramen ofmonroe
bull Primary treatment issurgical total resection
bull Subtotal resection may beadequate in case totalresection is hazardous
bull Tumor rarely becomesaggressive
bull Tarnscortical transcallosalapproach
bull If surgery not possible ordenied by pt thenmanagement of HCP byshunt
bull Role of chemotherapy hasshown promises
10202016 7unusual giomas
Everolimus for Subependymal Giant-Cell Astrocytomas in Tuberous SclerosisDarcy A Krueger MD PhD Marguerite M Care MD Katherine Holland MD PhD KarenAgricola FNP Cynthia Tudor PNP Prajakta Mangeshkar MS Kimberly A Wilson MSAnna Byars PhD Tarek Sahmoud MD PhD and David Neal Franz MDN Engl J Med 2010 3631801-181
bull Backgroundbull Neurosurgical resection is the standard treatment for subependymal giant-cell astrocytomas in patients with the tuberous
sclerosis complex An alternative may be the use of everolimus which inhibits the mammalian target of rapamycin a protein regulated by gene products involved in the tuberous sclerosis complex
bull Methodsbull Patients 3 years of age or older with serial growth of subependymal giant-cell astrocytomas were eligible for this open-label
study The primary efficacy end point was the change in volume of subependymal giant-cell astrocytomas between baseline and 6 months We gave everolimus orally at a dose of 30 mg per square meter of body-surface area to achieve a trough concentration of 5 to 15 ng per milliliter
bull Resultsbull We enrolled 28 patients Everolimus therapy was associated with a clinically meaningful reduction in volume of the
primary subependymal giant-cell astrocytoma as assessed on independent central review (Plt0001 for baseline vs 6 months) with a reduction of at least 30 in 21 patients (75) and at least 50 in 9 patients (32) Marked reductions were seen within 3 months and were sustained There were no new lesions worsening hydrocephalus evidence of increased intracranial pressure or necessity for surgical resection or other therapy for subependymal giant-cell astrocytoma Of the 16 patients for whom 24-hour video electroencephalography data were available seizure frequency for the 6-month study period (vs the previous 6-month period) decreased in 9 did not change in 6 and increased in 1 (median change minus1 seizure P=002) The mean (plusmnSD) score on the validated Quality-of-Life in Childhood Epilepsy questionnaire (on which scores can range from 0 to 100 with higher scores indicating a better quality of life) was improved at 3 months (634plusmn124) and 6 months (621plusmn142) over the baseline score (578plusmn140) Single cases of grade 3 treatment-related sinusitis pneumonia viral bronchitis tooth infection stomatitis and leukopenia were reported
bull Conclusionsbull Everolimus therapy was associated with marked reduction in the volume of subependymal giant-cell
astrocytomas and seizure frequency and may be a potential alternative to neurosurgical resection in some cases though long-term studies are needed
10202016 8unusual giomas
Angiocentric glioma
bull Described by WHO in2005
bull Initially included withastroblastoma andchoroid glioma
bull Mean age at diagnosis is17 years
bull Pts present with longhistory of seizures
bull Microscopically show themonomorphous bipolarcells associated withnormal vessels of thecortex and white matter
bull Tumor cells are spindleshaped
bull Mitoses are rarebull Positive for S-100 GFAP
vimentin
10202016 9unusual giomas
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
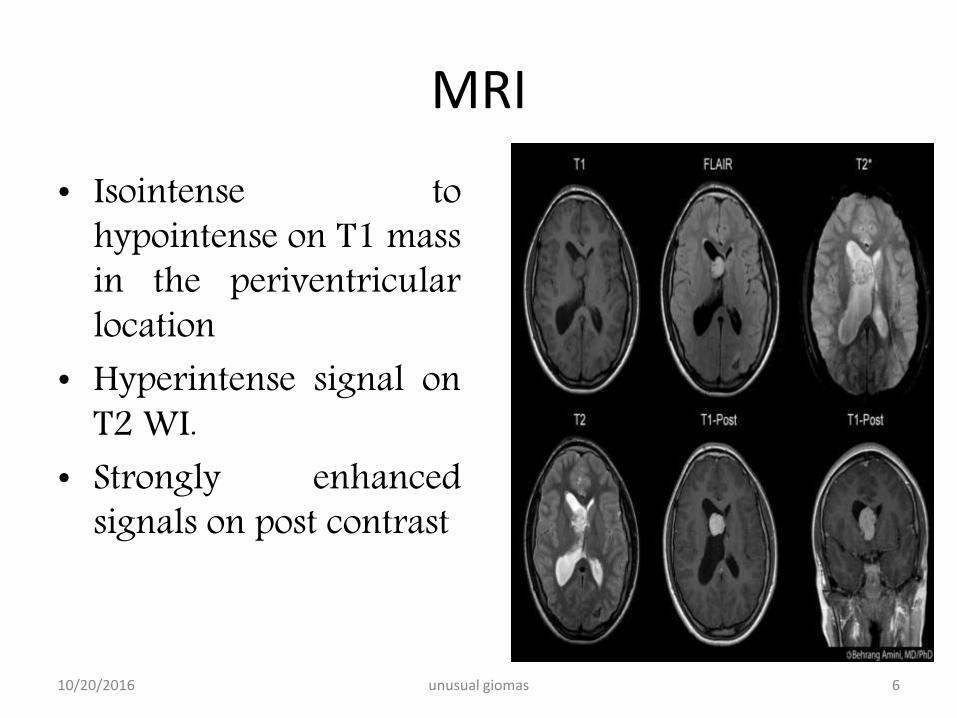
MRI
bull Isointense tohypointense on T1 massin the periventricularlocation
bull Hyperintense signal onT2 WI
bull Strongly enhancedsignals on post contrast
10202016 6unusual giomas
Management
bull Do not require interventionunless bolck the foramen ofmonroe
bull Primary treatment issurgical total resection
bull Subtotal resection may beadequate in case totalresection is hazardous
bull Tumor rarely becomesaggressive
bull Tarnscortical transcallosalapproach
bull If surgery not possible ordenied by pt thenmanagement of HCP byshunt
bull Role of chemotherapy hasshown promises
10202016 7unusual giomas
Everolimus for Subependymal Giant-Cell Astrocytomas in Tuberous SclerosisDarcy A Krueger MD PhD Marguerite M Care MD Katherine Holland MD PhD KarenAgricola FNP Cynthia Tudor PNP Prajakta Mangeshkar MS Kimberly A Wilson MSAnna Byars PhD Tarek Sahmoud MD PhD and David Neal Franz MDN Engl J Med 2010 3631801-181
bull Backgroundbull Neurosurgical resection is the standard treatment for subependymal giant-cell astrocytomas in patients with the tuberous
sclerosis complex An alternative may be the use of everolimus which inhibits the mammalian target of rapamycin a protein regulated by gene products involved in the tuberous sclerosis complex
bull Methodsbull Patients 3 years of age or older with serial growth of subependymal giant-cell astrocytomas were eligible for this open-label
study The primary efficacy end point was the change in volume of subependymal giant-cell astrocytomas between baseline and 6 months We gave everolimus orally at a dose of 30 mg per square meter of body-surface area to achieve a trough concentration of 5 to 15 ng per milliliter
bull Resultsbull We enrolled 28 patients Everolimus therapy was associated with a clinically meaningful reduction in volume of the
primary subependymal giant-cell astrocytoma as assessed on independent central review (Plt0001 for baseline vs 6 months) with a reduction of at least 30 in 21 patients (75) and at least 50 in 9 patients (32) Marked reductions were seen within 3 months and were sustained There were no new lesions worsening hydrocephalus evidence of increased intracranial pressure or necessity for surgical resection or other therapy for subependymal giant-cell astrocytoma Of the 16 patients for whom 24-hour video electroencephalography data were available seizure frequency for the 6-month study period (vs the previous 6-month period) decreased in 9 did not change in 6 and increased in 1 (median change minus1 seizure P=002) The mean (plusmnSD) score on the validated Quality-of-Life in Childhood Epilepsy questionnaire (on which scores can range from 0 to 100 with higher scores indicating a better quality of life) was improved at 3 months (634plusmn124) and 6 months (621plusmn142) over the baseline score (578plusmn140) Single cases of grade 3 treatment-related sinusitis pneumonia viral bronchitis tooth infection stomatitis and leukopenia were reported
bull Conclusionsbull Everolimus therapy was associated with marked reduction in the volume of subependymal giant-cell
astrocytomas and seizure frequency and may be a potential alternative to neurosurgical resection in some cases though long-term studies are needed
10202016 8unusual giomas
Angiocentric glioma
bull Described by WHO in2005
bull Initially included withastroblastoma andchoroid glioma
bull Mean age at diagnosis is17 years
bull Pts present with longhistory of seizures
bull Microscopically show themonomorphous bipolarcells associated withnormal vessels of thecortex and white matter
bull Tumor cells are spindleshaped
bull Mitoses are rarebull Positive for S-100 GFAP
vimentin
10202016 9unusual giomas
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Management
bull Do not require interventionunless bolck the foramen ofmonroe
bull Primary treatment issurgical total resection
bull Subtotal resection may beadequate in case totalresection is hazardous
bull Tumor rarely becomesaggressive
bull Tarnscortical transcallosalapproach
bull If surgery not possible ordenied by pt thenmanagement of HCP byshunt
bull Role of chemotherapy hasshown promises
10202016 7unusual giomas
Everolimus for Subependymal Giant-Cell Astrocytomas in Tuberous SclerosisDarcy A Krueger MD PhD Marguerite M Care MD Katherine Holland MD PhD KarenAgricola FNP Cynthia Tudor PNP Prajakta Mangeshkar MS Kimberly A Wilson MSAnna Byars PhD Tarek Sahmoud MD PhD and David Neal Franz MDN Engl J Med 2010 3631801-181
bull Backgroundbull Neurosurgical resection is the standard treatment for subependymal giant-cell astrocytomas in patients with the tuberous
sclerosis complex An alternative may be the use of everolimus which inhibits the mammalian target of rapamycin a protein regulated by gene products involved in the tuberous sclerosis complex
bull Methodsbull Patients 3 years of age or older with serial growth of subependymal giant-cell astrocytomas were eligible for this open-label
study The primary efficacy end point was the change in volume of subependymal giant-cell astrocytomas between baseline and 6 months We gave everolimus orally at a dose of 30 mg per square meter of body-surface area to achieve a trough concentration of 5 to 15 ng per milliliter
bull Resultsbull We enrolled 28 patients Everolimus therapy was associated with a clinically meaningful reduction in volume of the
primary subependymal giant-cell astrocytoma as assessed on independent central review (Plt0001 for baseline vs 6 months) with a reduction of at least 30 in 21 patients (75) and at least 50 in 9 patients (32) Marked reductions were seen within 3 months and were sustained There were no new lesions worsening hydrocephalus evidence of increased intracranial pressure or necessity for surgical resection or other therapy for subependymal giant-cell astrocytoma Of the 16 patients for whom 24-hour video electroencephalography data were available seizure frequency for the 6-month study period (vs the previous 6-month period) decreased in 9 did not change in 6 and increased in 1 (median change minus1 seizure P=002) The mean (plusmnSD) score on the validated Quality-of-Life in Childhood Epilepsy questionnaire (on which scores can range from 0 to 100 with higher scores indicating a better quality of life) was improved at 3 months (634plusmn124) and 6 months (621plusmn142) over the baseline score (578plusmn140) Single cases of grade 3 treatment-related sinusitis pneumonia viral bronchitis tooth infection stomatitis and leukopenia were reported
bull Conclusionsbull Everolimus therapy was associated with marked reduction in the volume of subependymal giant-cell
astrocytomas and seizure frequency and may be a potential alternative to neurosurgical resection in some cases though long-term studies are needed
10202016 8unusual giomas
Angiocentric glioma
bull Described by WHO in2005
bull Initially included withastroblastoma andchoroid glioma
bull Mean age at diagnosis is17 years
bull Pts present with longhistory of seizures
bull Microscopically show themonomorphous bipolarcells associated withnormal vessels of thecortex and white matter
bull Tumor cells are spindleshaped
bull Mitoses are rarebull Positive for S-100 GFAP
vimentin
10202016 9unusual giomas
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Everolimus for Subependymal Giant-Cell Astrocytomas in Tuberous SclerosisDarcy A Krueger MD PhD Marguerite M Care MD Katherine Holland MD PhD KarenAgricola FNP Cynthia Tudor PNP Prajakta Mangeshkar MS Kimberly A Wilson MSAnna Byars PhD Tarek Sahmoud MD PhD and David Neal Franz MDN Engl J Med 2010 3631801-181
bull Backgroundbull Neurosurgical resection is the standard treatment for subependymal giant-cell astrocytomas in patients with the tuberous
sclerosis complex An alternative may be the use of everolimus which inhibits the mammalian target of rapamycin a protein regulated by gene products involved in the tuberous sclerosis complex
bull Methodsbull Patients 3 years of age or older with serial growth of subependymal giant-cell astrocytomas were eligible for this open-label
study The primary efficacy end point was the change in volume of subependymal giant-cell astrocytomas between baseline and 6 months We gave everolimus orally at a dose of 30 mg per square meter of body-surface area to achieve a trough concentration of 5 to 15 ng per milliliter
bull Resultsbull We enrolled 28 patients Everolimus therapy was associated with a clinically meaningful reduction in volume of the
primary subependymal giant-cell astrocytoma as assessed on independent central review (Plt0001 for baseline vs 6 months) with a reduction of at least 30 in 21 patients (75) and at least 50 in 9 patients (32) Marked reductions were seen within 3 months and were sustained There were no new lesions worsening hydrocephalus evidence of increased intracranial pressure or necessity for surgical resection or other therapy for subependymal giant-cell astrocytoma Of the 16 patients for whom 24-hour video electroencephalography data were available seizure frequency for the 6-month study period (vs the previous 6-month period) decreased in 9 did not change in 6 and increased in 1 (median change minus1 seizure P=002) The mean (plusmnSD) score on the validated Quality-of-Life in Childhood Epilepsy questionnaire (on which scores can range from 0 to 100 with higher scores indicating a better quality of life) was improved at 3 months (634plusmn124) and 6 months (621plusmn142) over the baseline score (578plusmn140) Single cases of grade 3 treatment-related sinusitis pneumonia viral bronchitis tooth infection stomatitis and leukopenia were reported
bull Conclusionsbull Everolimus therapy was associated with marked reduction in the volume of subependymal giant-cell
astrocytomas and seizure frequency and may be a potential alternative to neurosurgical resection in some cases though long-term studies are needed
10202016 8unusual giomas
Angiocentric glioma
bull Described by WHO in2005
bull Initially included withastroblastoma andchoroid glioma
bull Mean age at diagnosis is17 years
bull Pts present with longhistory of seizures
bull Microscopically show themonomorphous bipolarcells associated withnormal vessels of thecortex and white matter
bull Tumor cells are spindleshaped
bull Mitoses are rarebull Positive for S-100 GFAP
vimentin
10202016 9unusual giomas
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Angiocentric glioma
bull Described by WHO in2005
bull Initially included withastroblastoma andchoroid glioma
bull Mean age at diagnosis is17 years
bull Pts present with longhistory of seizures
bull Microscopically show themonomorphous bipolarcells associated withnormal vessels of thecortex and white matter
bull Tumor cells are spindleshaped
bull Mitoses are rarebull Positive for S-100 GFAP
vimentin
10202016 9unusual giomas
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
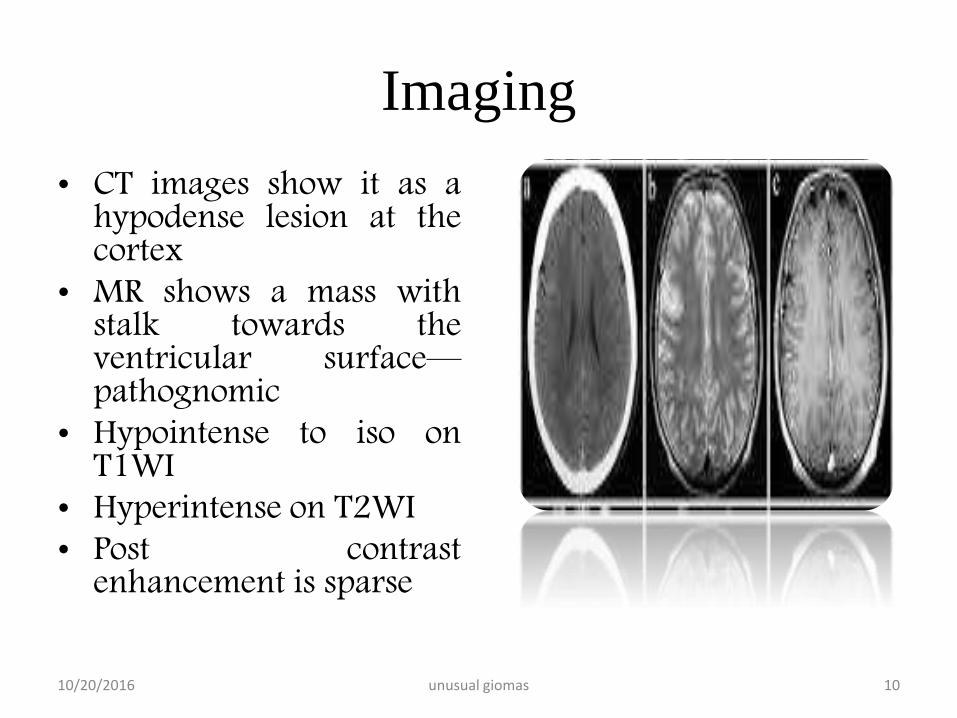
Imaging
bull CT images show it as ahypodense lesion at thecortex
bull MR shows a mass withstalk towards theventricular surfacemdashpathognomic
bull Hypointense to iso onT1WI
bull Hyperintense on T2WIbull Post contrast
enhancement is sparse
10202016 10unusual giomas
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
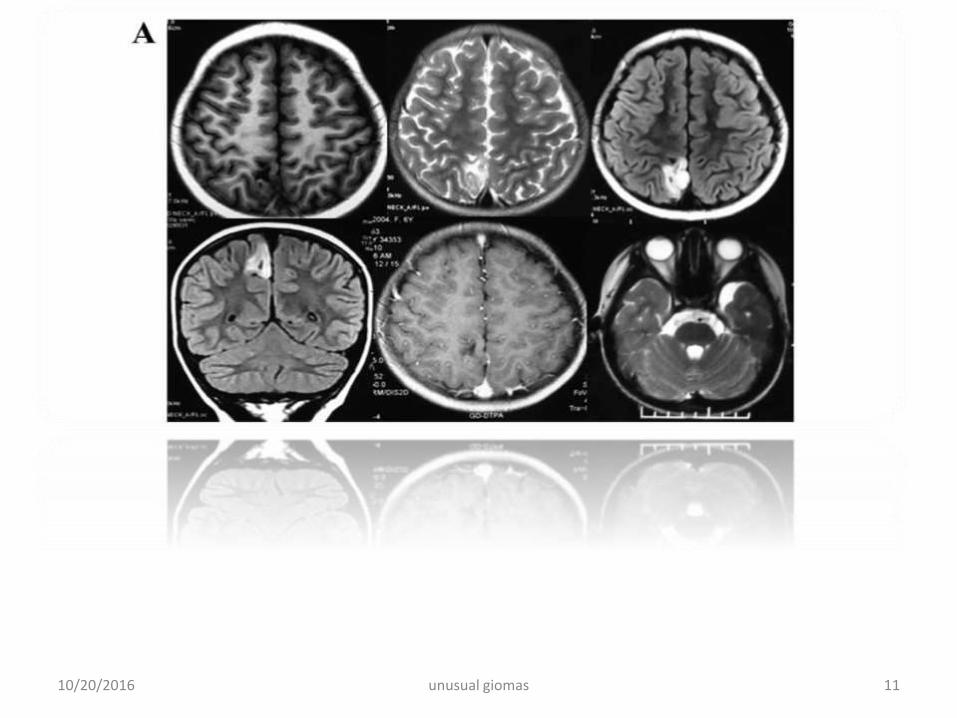
10202016 11unusual giomas
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Management and outcome
bull Follow an indolent coursebull Rare progressionbull Surgical cure obtained by total resectionbull Aggressive forms are exceedingly rare
10202016 12unusual giomas
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Perm J 2013 Winter17(1)e100-2 doi 107812TPP12-060
bull The treatment of angiocentric glioma case report and literature review
bull Alexandru D1 Haghighi B Muhonen MG
bull Abstract
bull Angiocentric glioma is a recently described tumor recognized since 2007
by the World Health Organization Classification of Tumours of the Central
Nervous System We present the only case of angiocentric glioma at our
institution in the last 15 years and review the literature in an attempt to
establish prognostic parameters Our search revealed only 27 cases of
angiocentric glioma in the literature The most common presenting
symptom of angiocentric glioma was seizures Gross total resection of
the lesion was curative without need for radiation or chemotherapy
10202016 13unusual giomas
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Astroblastoma
bull WHO grade 1bull Initially described by Bailey
and Bucy in 1930bull Has been a matter of debate
for similar features asanaplastic astrocytomaglioblastoma andgemistocytic astrocytomas
bull Commonly found in 1st
three decades of lifebull Female
preponderance(111)
bull Affects the hemispheresinvolving cortex subcortical andperiventricular regions
bull No infratentorail tumorhave been reported
bull Pts present with features ofraised ICP cortical deficitsseizures personalitychanges
10202016 14unusual giomas
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Greatly variable naturalhistory
bull Have a slow andindolent course
bull Rarely show anaggressive outcome
bull Almost always definedby their grossappearance
bull Cut surface revealhomogenous soft pinkgrey substances
bull Cystic areas arefrequently encountered
bull The clusters of cellsform pseudorossette
10202016 15unusual giomas
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Richly supplied byblood vessels
bull Nuclei of tumor cellsare away from bloodvessels and send fineprocesse to the vesselwall
bull High number of mitoticfigures can be found
bull Cellular atypia isfrequently noted
bull On IHC tumor cellsstain positive for GFAP
bull Positivity for vimentinNSE S-1OO EMA
bull These are positive foranti leu 7 antibodiesspecific for cells ofepithelial origin
bull Central necrosis can befound
10202016 16unusual giomas
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
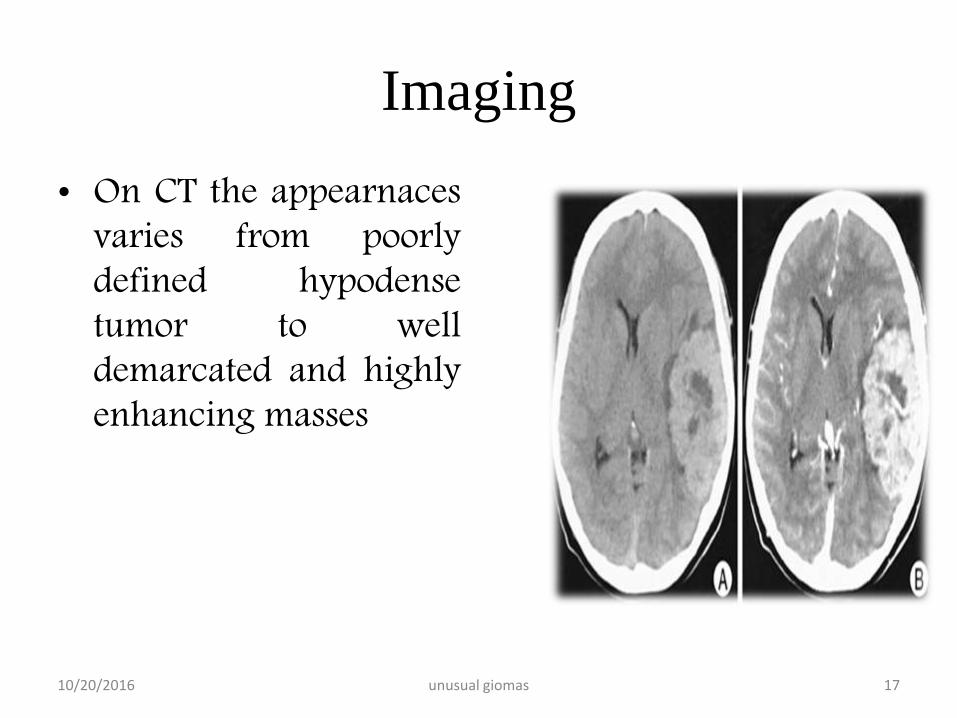
Imaging
bull On CT the appearnacesvaries from poorlydefined hypodensetumor to welldemarcated and highlyenhancing masses
10202016 17unusual giomas
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
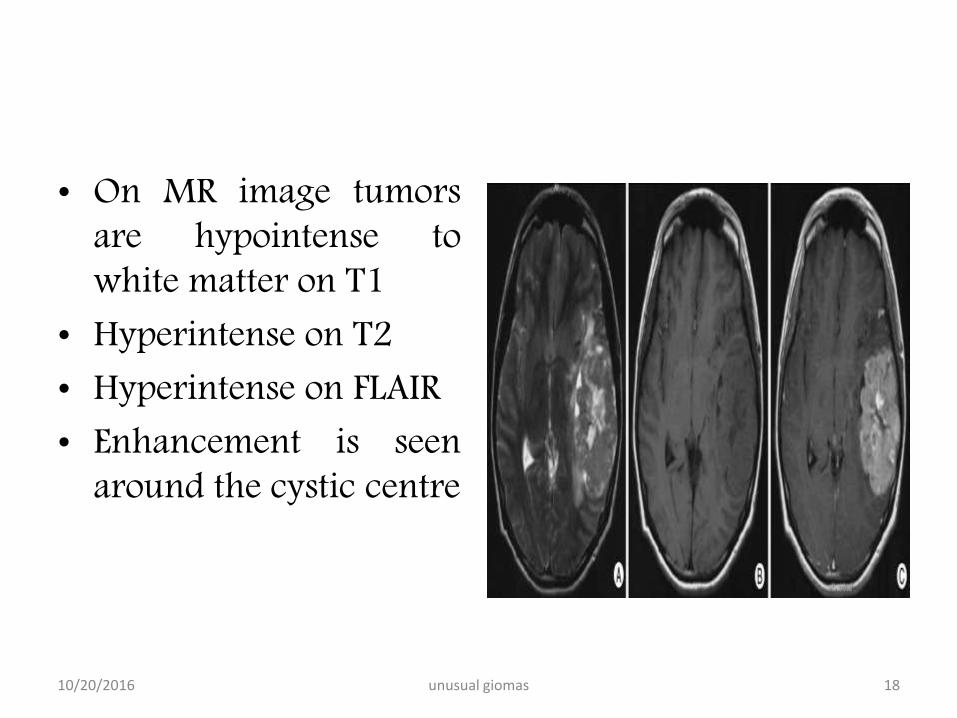
bull On MR image tumorsare hypointense towhite matter on T1
bull Hyperintense on T2bull Hyperintense on FLAIRbull Enhancement is seen
around the cystic centre
10202016 18unusual giomas
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Management And Prognosis
bull Surgical resection is main treatmentbull Gross total resection can be easily achieved as
lesions are mostly in the cortical areasbull Therapeutic value is of radiation and
chemotherapy is uncertain as these are raretumors
bull Prediction of outcome is difficult as these remainindolent for a long time and may rapidlytransform to glioblastoma resulting in fataloutcomes
10202016 19unusual giomas
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Pilomyxoid astrocytoma
bull Recently described tumorsbull Similarities with pilocytic
astrocytomasbull Until recently these were
grouped with PAbull These involve entire
neuraxisbull Mean age at preentation is
18 monthsbull Most are found in
hypothalamic ndash chiasmicregion
bull Pts present with features ofraised ICP
bull RAISED HEADCIRCUMFERENCE may beonly subtle sign in infants
bull Histologically consists ofmyxoid matrix with cells inloose fibrillary and myxoidbackground
bull Tumor cells formperivascular rosettes
10202016 20unusual giomas
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Preferred sites includebull (1) optic nerve (lsquooptic
nerve gliomarsquo)bull (2) optic
chiasmhypothalamusbull (3) thalamus and basal
gangliabull (4) cerebral hemispherebull (5) cerebellum (lsquocerebellar
astrocytomarsquo) andbull (6) brainstem (dorsal
exophytic brainstemglioma)
bull Genetically chracterized bythe presence of NF1mutations BRAFduplications and theabsence of IDH1 mutation
10202016 21unusual giomas
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
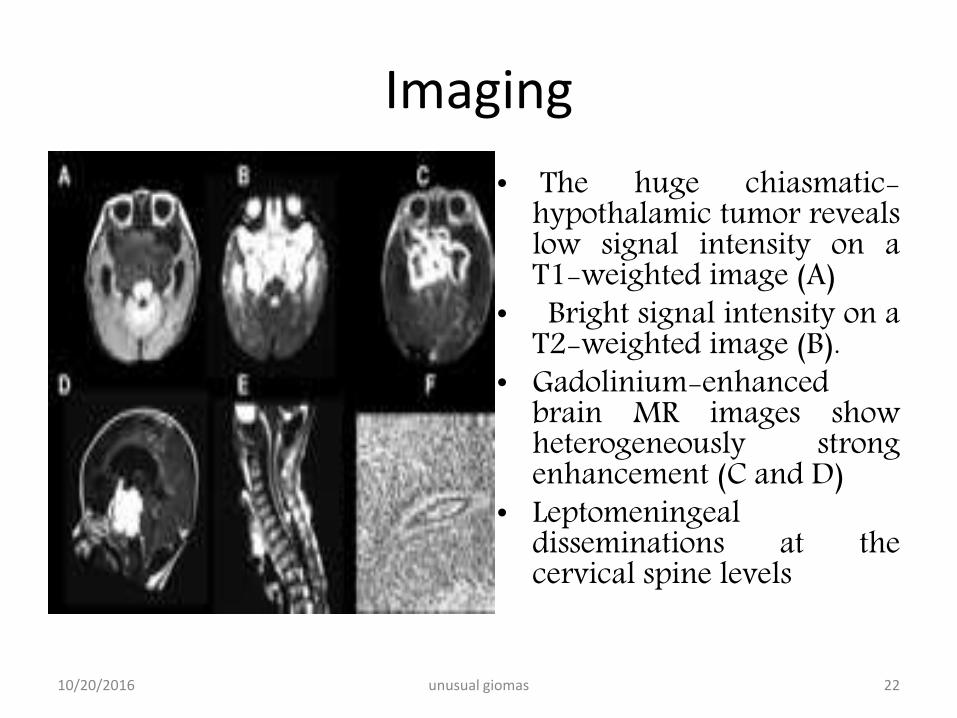
Imaging
bull The huge chiasmatic-hypothalamic tumor revealslow signal intensity on aT1-weighted image (A)
bull Bright signal intensity on aT2-weighted image (B)
bull Gadolinium-enhancedbrain MR images showheterogeneously strongenhancement (C and D)
bull Leptomeningealdisseminations at thecervical spine levels
10202016 22unusual giomas
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull NO standard careprotocols have beendefined
bull As these are newlydefined and raretumors
bull Surgical resection isfavoured if locationfavours
bull Mean progression freesurvival is 25 months
bull Mean overall survival is60 months
bull Reduced survival isbecause of inability toachieve gross resection
10202016 23unusual giomas
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull The usual indications foradjuvant treatment(chemotherapy orradiation therapy)include tumor recurrenceafter initial completeresection or symptomatictumors
bull In addition adjuvanttreatment is generallyindicated for tumors withgrowth on follow-upimaging even in theabsence of symptoms
bull The role of chemotherapyis in evolution
bull Chemotherapy may beimplemented for the treatment ofinoperable or partially resectedgliomas
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
bull The decision to use postoperativeadjuvant therapy also depends ona lesions perceived malignanttendencies as the potentialbenefits of radiation therapy andchemotherapy must be weighedagainst their morbidity
10202016 24unusual giomas
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Pleomorphic xanthoastrocytoma
bull First described by Kepsand colleuges in 1979
bull Represents lt1 of allastrocytomas
bull May be found alongentire neuraxis mostlysupratentorial( temporallobe)
bull Cerebellum and soinalcord are the other sites
bull Pts present in 2nd and 3rd
decadesbull Median age at 14 yearsbull Both sexes are affected
equallybull 70-80 pts present with
seizures and headachefocal neuro deficits
bull Rarely tumor mayhemmorrhage
10202016 25unusual giomas
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Supratentorail are mostoften cortical and meningesbased
bull Chronic seizuresbull Grossely these are firm
tumors variable in colorrelatively avascular
bull Typically invade the piaarachnoid space
bull 13 pts have involvementof all the three meninges
bull Cyst fluid is xanthochromic
bull Very specific microscpoiccriteria for diagnosis are
1 Pleomorphic andxanthomatous astrocytes
2 Perivascular lymphocytes3 Non infilterating histology4 Reticulin stainingbull Pleomorphism can be as
vast as glioblastoma orsarcomatous tumors
10202016 26unusual giomas
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull IHC Staining revealsspindle cells and roundpleomorphic cellspositive for S-100 andGFAP
bull Staining forsynaptophysin and NSEmay be also present
bull Some workers havereported them to be asubtype of ganglioglioma
bull Association between theNeurofibromatosis Sturge Weber Syndrome
bull Loss of chr 9 and gain ofchromosome 7 have beenfound
10202016 27unusual giomas
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
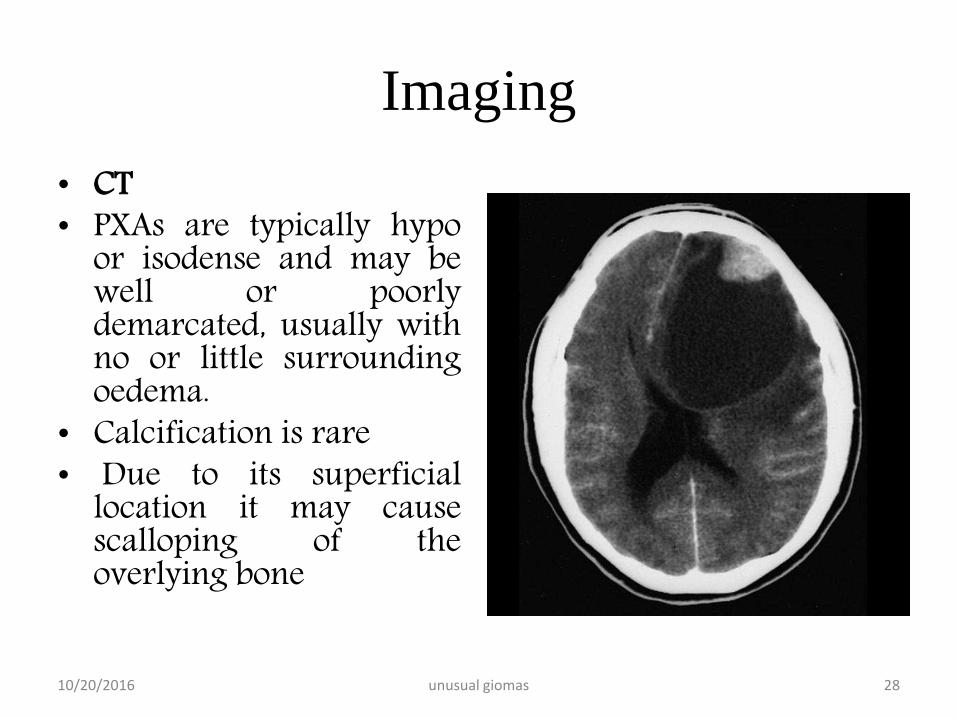
Imaging
bull CTbull PXAs are typically hypo
or isodense and may bewell or poorlydemarcated usually withno or little surroundingoedema
bull Calcification is rarebull Due to its superficial
location it may causescalloping of theoverlying bone
10202016 28unusual giomas
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
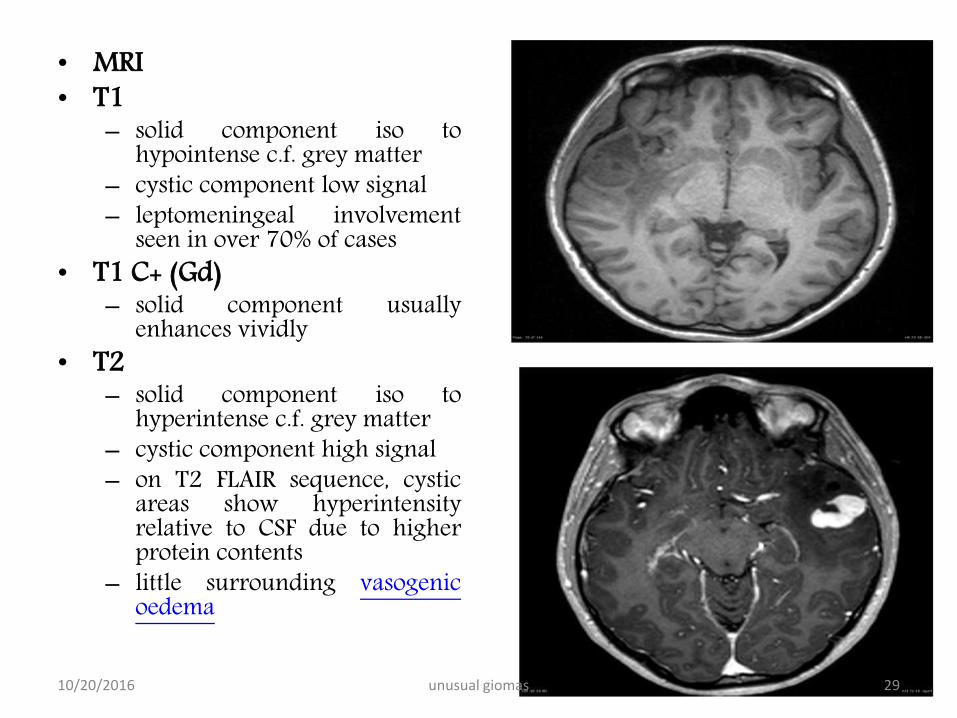
bull MRIbull T1
ndash solid component iso tohypointense cf grey matter
ndash cystic component low signalndash leptomeningeal involvement
seen in over 70 of casesbull T1 C+ (Gd)
ndash solid component usuallyenhances vividly
bull T2ndash solid component iso to
hyperintense cf grey matterndash cystic component high signalndash on T2 FLAIR sequence cystic
areas show hyperintensityrelative to CSF due to higherprotein contents
ndash little surrounding vasogenicoedema
10202016 29unusual giomas
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Management amp Outcome
bull Quite rare tumorsbull Surgical excision appears to
be best favoured modalitybull Actuarial survival trates are
91 at 5 years and 82 at10 years
bull Median survival 18 years
bull Total resection should beattempted in every case asfar as possible
bull Resection of cyst lining isnot indicated
bull Data regarding the use ofadjuvant therapy at thistime are limited to few casereports only
bull Pts who had incompleteresection high mitoticindex necrosis should bereserved for strict vigilanceand CEMRI on follow ups
10202016 30unusual giomas
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull At progression repeatresection be attempted
bull Proression should betaken as aggressivetumor type
bull Malignanttransformation maynecessitate adjuvanttherapy
10202016 31unusual giomas
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Br J Neurosurg 2013 Dec27(6)759-64 doi 103109026886972013776666 Epub 2013 Mar 20
bull Pleomorphic xanthoastrocytoma long-term results of surgical treatment and analysis of prognosticfactors
bull Gallo P1 Cecchi PC Locatelli F Rizzo P Ghimenton C Gerosa M Pinna G
bull BACKGROUND
bull Pleomorphic Xanthoastrocytoma (PXA) is a rare brain tumour most commonly affecting children andyoung adults To date only few data regarding the long-term follow-up of these patients after surgery are
available The aim of this study is to describe our single-institution experience in the surgicalmanagement of this particular glioma over a period of over 18 years
bull METHODS
bull We performed a retrospective review of all cases of PXA (40 patients) operated upon at theDepartment of Neurosurgery of Verona Italy between 1990 and 2008 The impact of clinical radiologicalsurgical and histological factors on overall survival (OS) and progression-free survival (PFS) was analysed bymeans of univariate and multivariate models
bull FINDINGS
bull We achieved a gross total resection (GTR) in 65 of patients Histological diagnosis was of grade II in 80anaplastic features were present in the remaining 20 Adjuvant treatment radiotherapy or chemo-
radiotherapy was administered in 40 of the cases Median follow-up was 74 months OS at 5- and10 years was 7632 and 6824 respectively PFS at 5- and 10 years was 71 and 58respectively In the multivariate model histological grade extent of resection and age at diagnosis (le 30years vs gt 30 years) were the only independent prognostic factors for both OS and PFS
bull CONCLUSIONS
bull Our retrospective long-term study confirms the relatively favourable prognosis associatedwith PXA Young patients with a low-grade tumour (WHO grade II) who underwent GTR carrythe longest OS and PFS
10202016 32unusual giomas
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Brain Tumor Pathol 2006 Apr23(1)55-63
bull A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination
bull Asano K1 Miyamoto S Kubo O Kikkukawa T Yagihashi A Ohkuma H
bull Pleomorphic xanthoastrocytoma (PXA) has been considered an astrocytic tumorwith a relatively favorable prognosis However PXA cases having several recurrent patterns with poor prognosis have been reported in recent years and a new concept of anaplastic PXA has been proposed The present case was a 59-year-old woman who presented with tumor bleeding onset and cerebrospinal fluid dissemination The patient had sudden-onset right hemiparesis aphasia and consciousness disturbance and was admitted to a local area hospital After emergency surgery had removed the hematoma postoperative contrast-enhanced CT scan revealed a left temporal tumor A second surgery was therefore performed for initial tumor removal 2 months later Histopathological findings showed that the tumor was typical PXA with strong pleomorphism and xanthomatous changes and contained an ependymoma-like component in the center area However endothelial proliferation and mitosis were more remarkable compared to ordinary PXA The MIB-1 labeling index was 98 high From these findings the histopathological diagnosis was anaplastic PXA The patient underwent surgery to remove recurrent tumors 5 and 16 months later The patient died 36 months after the first onset and CT revealed glioblastoma-like
findings and cerebrospinal fluid dissemination This case report is the first case in which PXA presented with tumor bleeding onset Histopathological findings suggested anaplastic PXA from the first surgical specimens and PXA recurred many times We thus believe that the patient displayed primary anaplastic PXA rather than secondary anaplastic PXA that results in malignant transformation10202016 33unusual giomas
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Ganglioglioma
bull WHO grade 1bull Initially described by
Perkins in 1926bull Benign well
differentiatedneuroepithelial tumors
bull Most commonly found intemporal lobe though canoccur anywhere in CNS
bull Commonly found inyoung patients withepilepsy
bull Most commonly notedtumor in temporal lobeepilepsy patients
bull Have been described inbrain steem spinal cordand cerebellum
bull Account for 1 ofprimary brain tumors
10202016 34unusual giomas
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Male dominencebull Most common features
are seizures headachedizziness ataxiaprogressive weakness
bull Malignanttransformation is rare
bull Histology showsimmature mixture ofabnormal neural andglial elements
bull Macroscopically appearsolid or cystic
bull Cystic are welldelineatedfromsurrounding brain
bull Calcification is common
10202016 35unusual giomas
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull IHC staing shows reactivity for GFAP S-100 andvimentin
bull Neurons show synaptophysin class III betatubulin NFP chromogranin reactivity
10202016 36unusual giomas
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
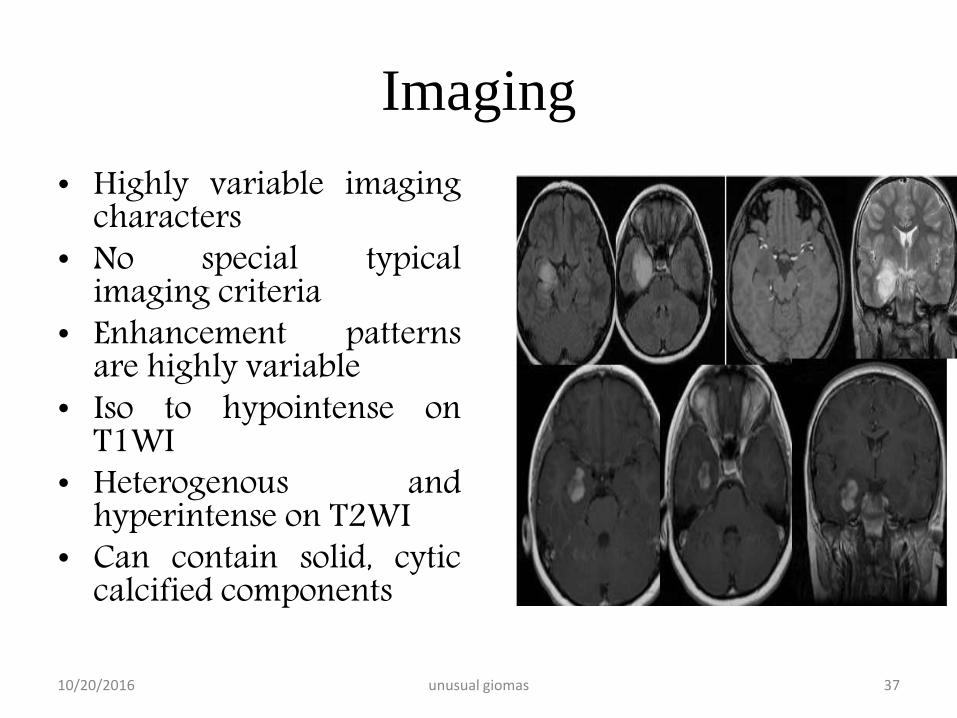
Imaging
bull Highly variable imagingcharacters
bull No special typicalimaging criteria
bull Enhancement patternsare highly variable
bull Iso to hypointense onT1WI
bull Heterogenous andhyperintense on T2WI
bull Can contain solid cyticcalcified components
10202016 37unusual giomas
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
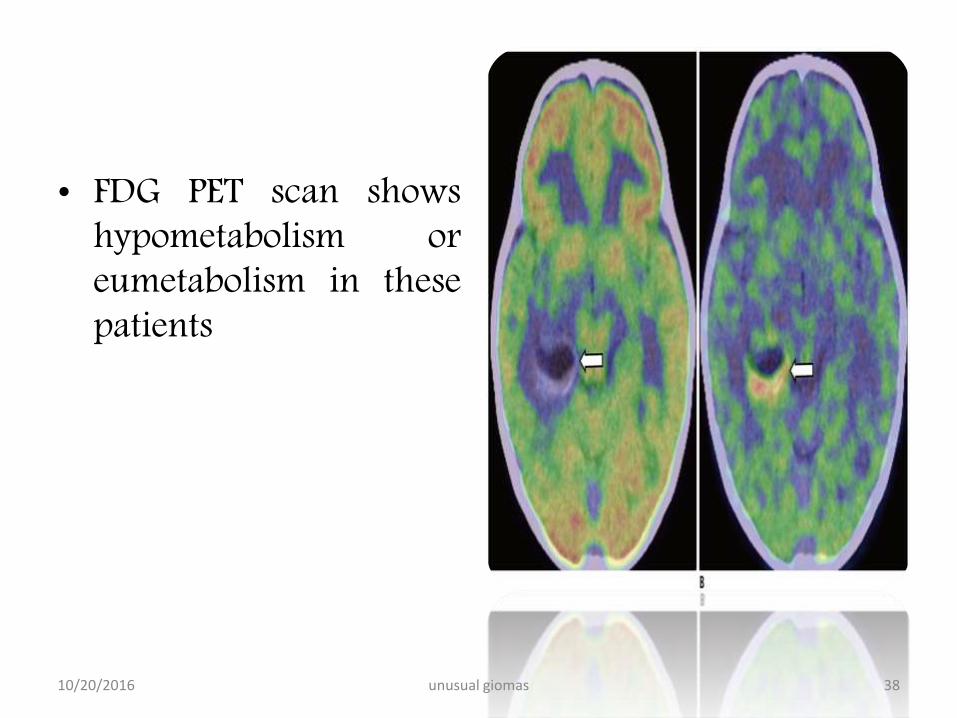
bull FDG PET scan showshypometabolism oreumetabolism in thesepatients
10202016 38unusual giomas
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Management And Outcome
bull Gold standard is grosstotal resection
bull Seizure control aftersurgery is as high as80
bull Survival rates are highbull Event free survival of
low grade and highgrade gangiogioma are57 vs 15
bull The optimal surgicalresection depends uponthe eloquent areasinvolved in the vicinityof the tumor
bull The use ofchemotherapy is notwell established
bull Typically they shouldbe allowed for chemoand radiotherapy
10202016 39unusual giomas
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull The use of adjuvant therapy is warranted in thosecases which harbour residual lesions or features ofanaplasia
bull Potential harm to nearby brain areas preclude thejudicious use of radiation
10202016 40unusual giomas
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Brain Tumor Res Treat 2014 Oct 2(2) 49ndash55
bull Treatment and Outcomes for Gangliogliomas A Single-Center Review of 16 Patients
bull Jye Young Song Jeong Hoon Kim Young Hyun Cho Chang Jin Kim and Eun Jung Lee
bull Ganglioglioma is a rare and slowly growing benign tumor We investigated the outcomes of patients who underwent different combination treatments
bull Methods
bull Between 1998 and 2012 16 patients including 11 men and 5 women with a median age of 125 years (range 25-65 years) were treated for intracranial gangliogliomas at our institution The median follow-up period was 57 years (range 48 days-156 years) Fifteen cases were included in the outcome assessment because one patient was lost to follow-up Complete resection was achieved in 8 (53) patients Six (40) patients underwent incomplete resection with or without adjuvant radiotherapy and one patient with a brainstem tumor underwent only stereotactic biopsy
bull Results
bull Gangliogliomas predominantly affected young (875) male patients and most frequently presented with seizures (64) Of eight patients who underwent complete resection seven did not show recurrence whereas only three of six with incomplete resection showed no recurrence Four patients with recurrence received salvage treatments (two repeat surgeries and two radiosurgeries) A tumor control rate of 93 (1415) was achieved at the last follow-up No recurrence or malignant changes were observed after a median follow-up of 12 and 45 years in four patients who received gamma knife (GK) radiosurgery as adjuvant and salvage treatment
bull Conclusion
bull Complete resection produced the best outcomes and incomplete resection followed by adjuvant or salvage treatments showed favorable outcomes In patients who are not eligible for complete resection because of tumor location or potential neurologic deficits following surgery GK radiosurgery should be considered for the treatment of residual or recurrent tumors
10202016 41unusual giomas
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Papillary tumours of pineal
bull WHO grade II AND IIIbull Relatively new edition to WHObull They are equal in both sexesbull Reach medical attention due to headache mental
status changes and altered visionbull Contain eosinophilic cells with distinctive
borders with large pleomorphic nucleibull Positive for cytokeratin synaptophysin stain
variably for GFAP vimentin S-100
10202016 unusual giomas 42
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Imaging
bull Generally found to be diffusely enhancinglesion of pineal region
bull Post 3rd ventricle with HCPbull Appear well demarcated from thalamus and
cerebellum
10202016 unusual giomas 43
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Mangement
bull Standard treatment is excisionbull Grow slowly and donot transform to
malignant tumorsbull Local recurrence is however possiblebull Radiotherapy appears to provide good control
in local recurrence
10202016 unusual giomas 44
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Choroid Glioma Of Third Ventricle
bull WHO Grade IIbull Ist recognised by WHO in
1998bull Arise in the anterior third
ventriclebull Commonly come to
attention after HCPbull Appera to contain in 3rd
ventricle and thought toarise from ventricularsurface
bull Composed of GFAP andvimentin positive cells inmucinous matrix
bull Nuclei are uniform insize and shape
bull Indolent growthbull May show EGF receptor
positivitybull Some suggets these tumor
arise from the lminaterminalis andventricular tanycytes
10202016 45unusual giomas
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
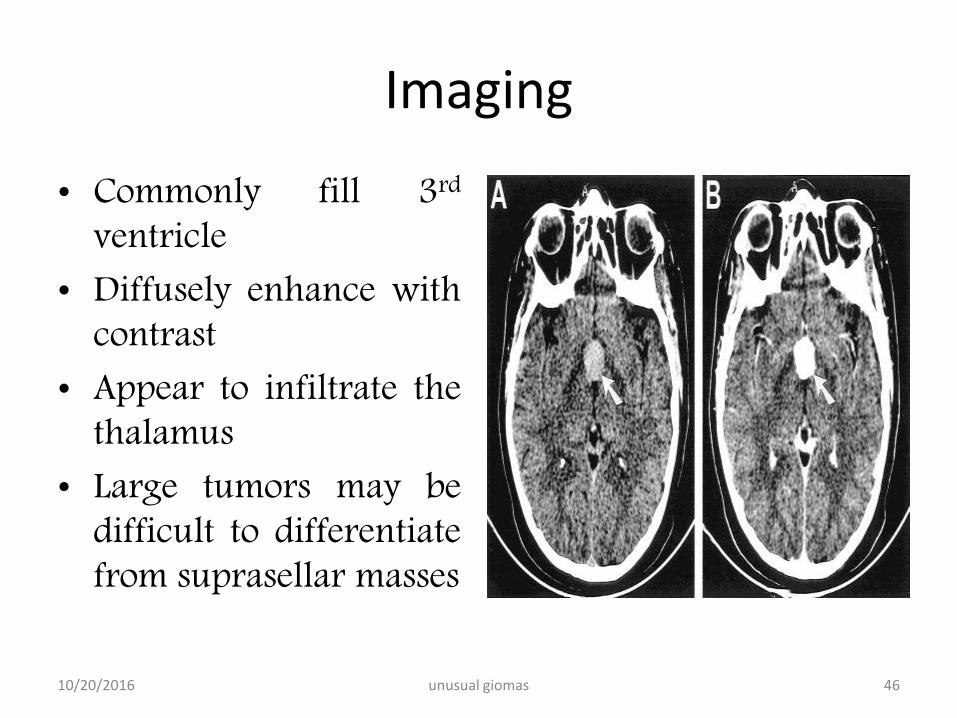
Imaging
bull Commonly fill 3rd
ventriclebull Diffusely enhance with
contrastbull Appear to infiltrate the
thalamusbull Large tumors may be
difficult to differentiatefrom suprasellar masses
10202016 46unusual giomas
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
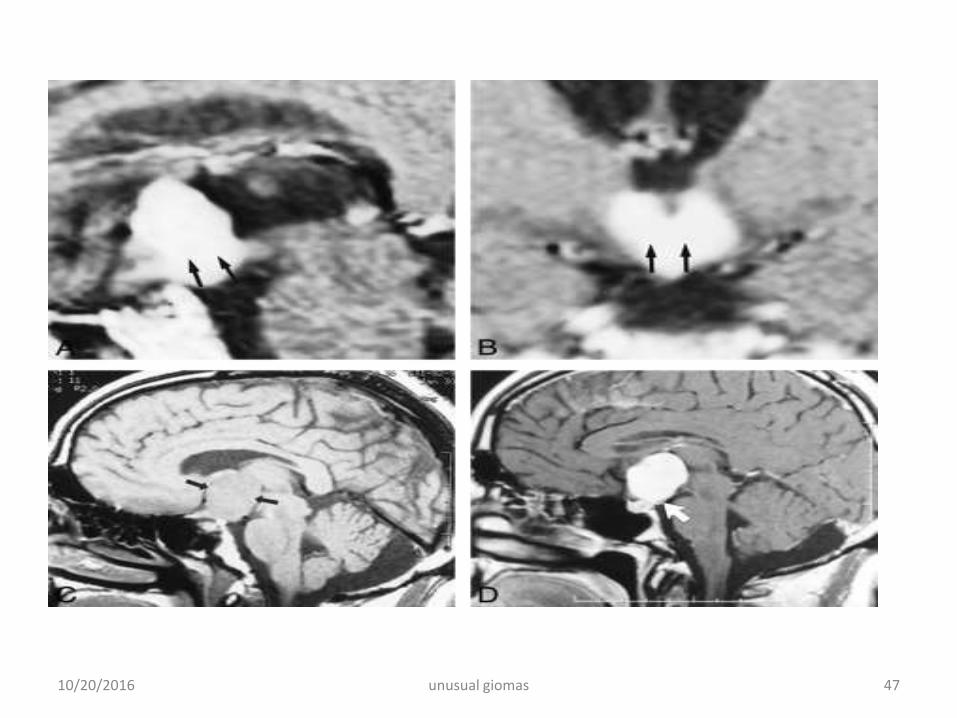
10202016 47unusual giomas
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Surgical management is limited by locationbull Access through the dialted ventricle and lamina
terminalis may be challangingbull Subtotal resection is thus commonbull Role of adjuvant radiotherapy is unknown
10202016 48unusual giomas
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Acta Neurochir (Wien) 2008 Nov150(11)1183-91 doi 101007s00701-008-0014-6 Epub
2008 Oct 21
bull Chordoid glioma of the third ventricle
bull Vanhauwaert DJ1 Clement F Van Dorpe J Deruytter MJKGROUND
bull Chordoid glioma is a rare tumour (World Health Organisation grade II) originating from the third ventricle
with both glial and chordoid features It was first described by Brat in 1998 Since there is no detailed
information available on the outcome after surgery and adjuvant treatment we reviewed the literature
bull METHODS
bull A literature search through PUBMED revealed 50 cases of chordoid glioma Most reports
were found in pathology journals Information on the postoperative course was sometimes
very limited We reviewed the available literature and studied in detail the presenting
symptoms mortality and postoperative complications in relation to the extent of resective
surgery as well as the importance of adjuvant treatment
bull CONCLUSIONS
bull Mortality in the immediate postoperative period is 32 and is higher after gross total
resection as compared to subtotal resection Non-fatal postoperative complications are
hypothalamic disorders and mental alterations Gross total resection is the treatment of
choice since no recurrence has been reported after macroscopically complete resection
but this is often difficult because of the location and adherence to the hypothalamus The
role of postoperative radiotherapy is uncertain There is some indication that radiosurgery
with or without conventional irradiation is superior to conventional radiation alone Planned
subtotal resection followed by stereotactic radiosurgery can be a safe and effective
alternative in a patient in whom gross total resection is considered to be too risky
There is no report on the use of chemotherapy in the treatment of chordoid gliomas More
information about the optimal treatment strategy is needed and more reports are also needed10202016 49unusual giomas
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
bull Neurologist 2011 Jan17(1)52bull Chordoid glioma a case report and literature reviewbull Liu WP1 Cheng JX Yi XC Zhen HN Fei Z Li Q Zhang Xbull chordoid glioma is a rare tumor (World Health Organization grade II) with both
glial and chordoid features often located in the suprasellar region and anterior third ventricle It was first described by Brat in 1998 Because there is no detailed information available from the clinical perspective we reviewed the literature
bull METHODS
bull a literature search through PUBMED and CNKI revealed 64 cases of chordoid glioma Information on the clinical course was very limited We reviewed the literature and studied the pathologic and imaging features postoperative mortality and morbidity in relation to surgical extension and approaches and the importance of adjuvant treatment
bull CONCLUSIONS bull mortality in the immediate postoperative period is 28 and postoperative
morbidity is 60 which are statistically higher after gross total resection as compared with subtotal resection Translamina terminalis approach is considered to be the best approach The current study cannot document that patients have longer survival and higher quality of life after gross total resection than subtotal resection The role of postoperative radiotherapy is uncertain and there is no report on the use of chemotherapy More information about the optimal treatment strategy is needed
10202016 50unusual giomas
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook
Conclusion
bull They are identified by their unique morphologicalfeatures
bull Many of these have indolent course and identified byepilepsy
bull Potentail diagnosis should be considered in youngpatients with seizures and cortically based lesions
bull Correct diagnosis requires experiencedneuropathologisrt
bull As more experienced is gained more knowledgetowards better understanding shall provide betteroutcomes in these patients
10202016 unusual giomas 51
10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook

10202016 52unusual giomas
Content supportndash youmann neurosurgery textbook