2013 Link et al Bromus Tectorum cover mapping and fire risk.pdf
�����
�
World Health Organization, Western Pacific Regional Office World Health Organization, Western Pacific Regional Office
Tuberculosis control among high risk and vulnerable populations
CPD Seminar, Ministry of Health, Fiji
10 July 2012
“The best way to predict the future is to create it”! ! !! ! ! !! ! ! !– Peter F Drucker
Nobu Nishikiori, MD, PhD, MSc Medical Officer, Stop TB WHO Western Pacific Regional Office [email protected]
World Health Organization, Western Pacific Regional Office
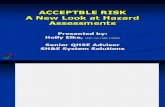
Tuberculosis – a social disease�
�����
��
World Health Organization, Western Pacific Regional Office
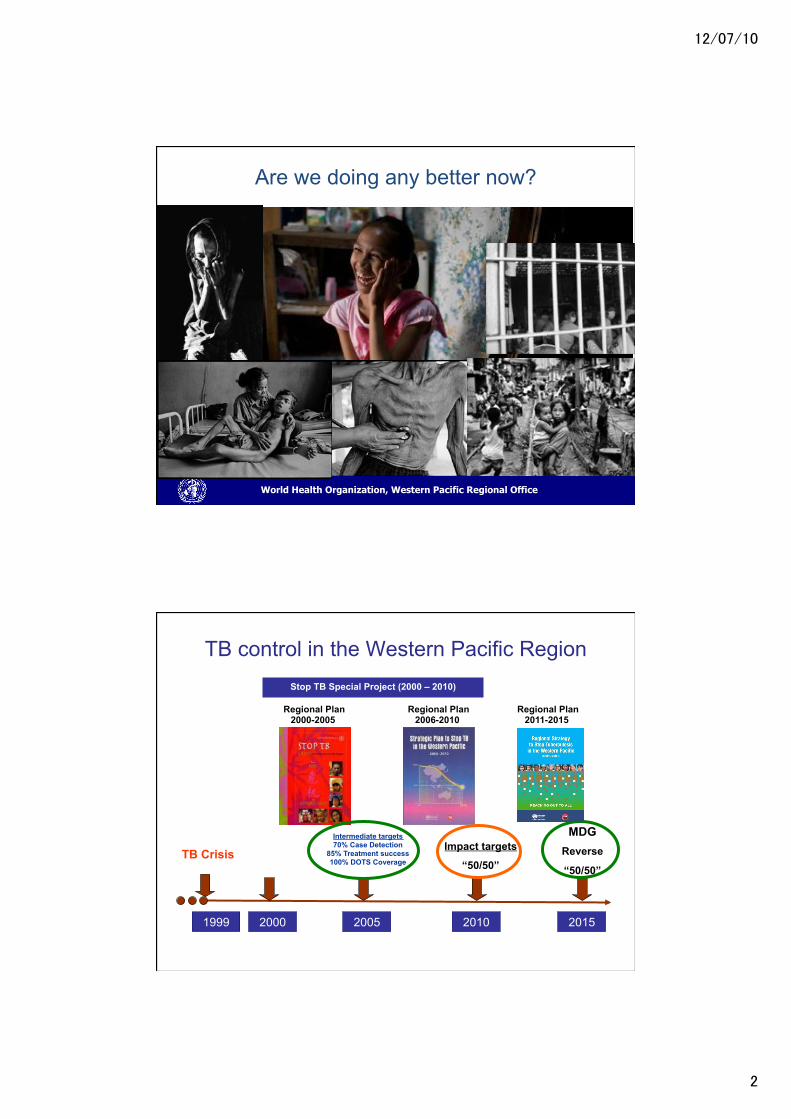
Are we doing any better now?�
TB control in the Western Pacific Region Stop TB Special Project (2000 – 2010)
2000 2005 1999 2010
Impact targets
“50/50”
Intermediate targets 70% Case Detection
85% Treatment success 100% DOTS Coverage
TB Crisis
2015
MDG Reverse
“50/50”
Regional Plan 2000-2005
Regional Plan 2006-2010
Regional Plan 2011-2015
�����
��
World Health Organization, Western Pacific Regional Office
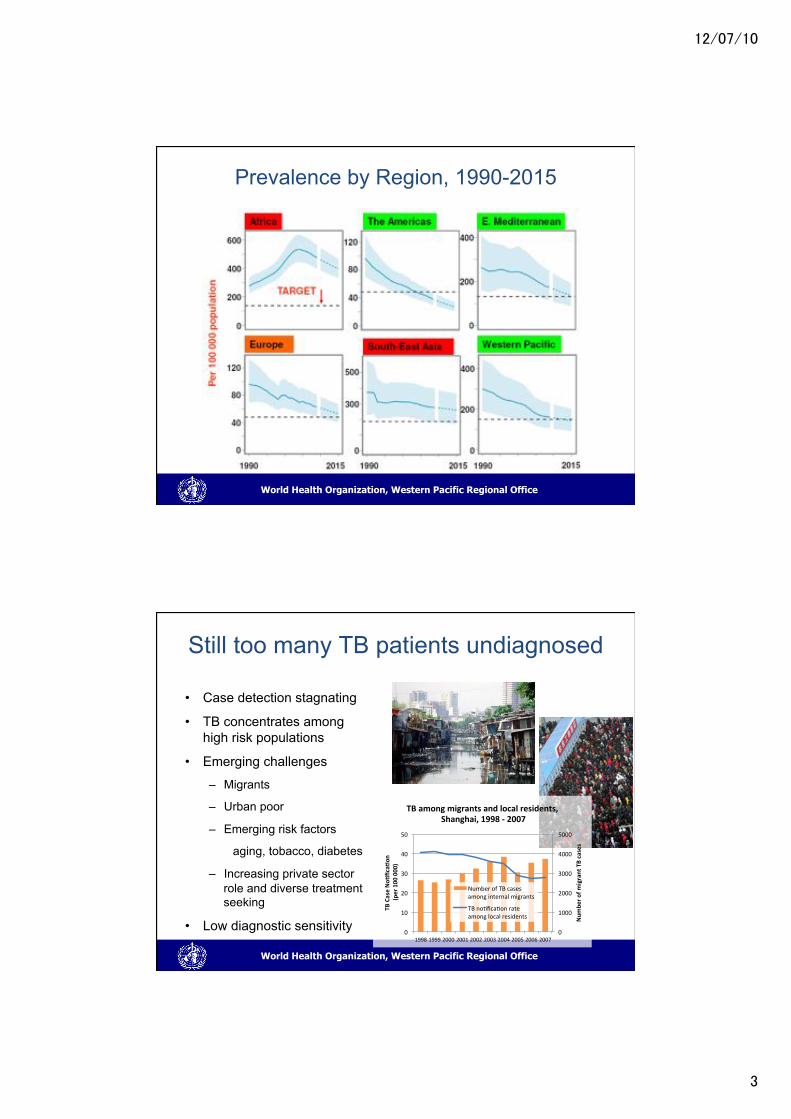
Prevalence by Region, 1990-2015
World Health Organization, Western Pacific Regional Office
Still too many TB patients undiagnosed
• Case detection stagnating
• TB concentrates among high risk populations
• Emerging challenges
– Migrants
– Urban poor
– Emerging risk factors
aging, tobacco, diabetes
– Increasing private sector role and diverse treatment seeking
• Low diagnostic sensitivity
0"
1000"
2000"
3000"
4000"
5000"
0"
10"
20"
30"
40"
50"
1998"1999"2000"2001"2002"2003"2004"2005"2006"2007"
Num
ber'of'm
igrant'TB'cases'
TB'Case'No4
fica4on
''(p
er'100
'000
)'
TB'among'migrants'and'local'residents,''Shanghai,'1998'B'2007'
Number"of"TB"cases"among"internal"migrants"
TB"no>fica>on"rate"among"local"residents"
�����
�
World Health Organization, Western Pacific Regional Office
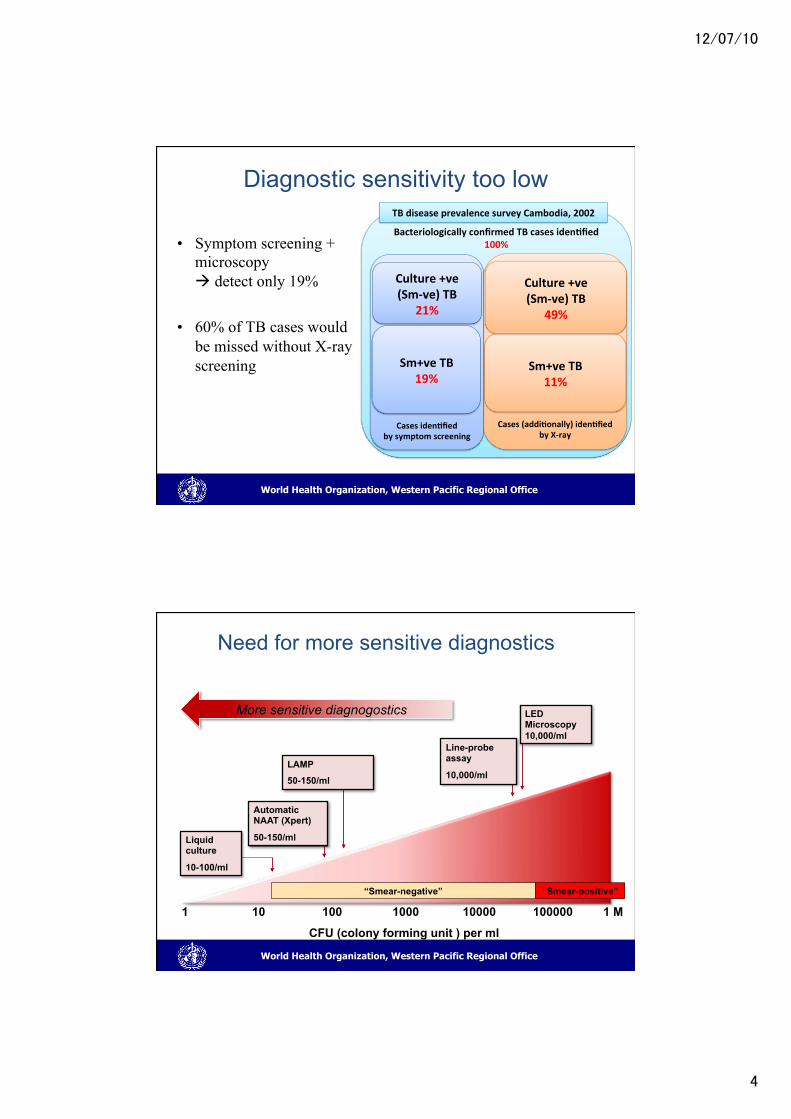
Bacteriologically'confirmed'TB'cases'iden4fied'100%''
Cases'(addi4onally)'iden4fied''by'XBray"
Sm+ve'TB'11%"
Culture'+ve''(SmBve)'TB'
49%"
Diagnostic sensitivity too low
• Symptom screening + microscopy ! detect only 19%
• 60% of TB cases would be missed without X-ray screening
Cases'iden4fied''by'symptom'screening"
Sm+ve'TB'19%"
Culture'+ve''(SmBve)'TB'
21%"
TB'disease'prevalence'survey'Cambodia,'2002''
(Data from Draft Report National Prevalence Survey in Viet Nam 2006-7)
World Health Organization, Western Pacific Regional Office
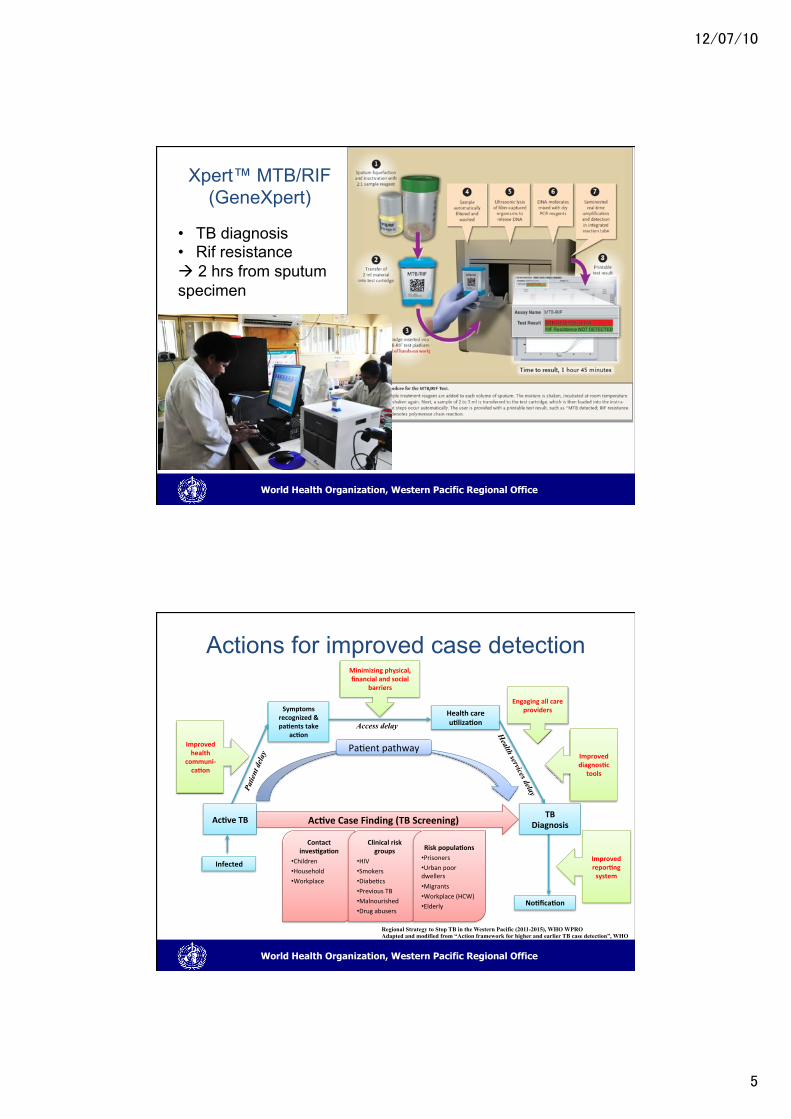
Need for more sensitive diagnostics
1 10 100 1000 10000 100000 1 M
CFU (colony forming unit ) per ml
More sensitive diagnogostics LED Microscopy 10,000/ml
LAMP
50-150/ml
Automatic NAAT (Xpert)�
50-150/ml
Line-probe assay
10,000/ml
Liquid culture
10-100/ml
“Smear-positive” “Smear-negative”
�����
��
World Health Organization, Western Pacific Regional Office
Xpert™ MTB/RIF (GeneXpert)
• TB diagnosis • Rif resistance ! 2 hrs from sputum specimen
World Health Organization, Western Pacific Regional Office
Actions for improved case detection
Contact'inves4ga4on'
• Children"• Household"• Workplace"
Clinical'risk'groups'
• HIV"• Smokers"
• Diabe>cs"• Previous"TB"• Malnourished"
• Drug"abusers"
Risk'popula4ons'• Prisoners"• Urban"poor"dwellers"
• Migrants"
• Workplace"(HCW)"
• Elderly"
Ac4ve'Case'Finding'(TB'Screening)'
Minimizing'physical,'financial'and'social'
barriers'
Improved'health'
communiBca4on'
Engaging'all'care'providers'
Improved'diagnos4c'
tools'
Pa>ent"pathway"
Symptoms'recognized'&'pa4ents'take'
ac4on'
Health'care'u4liza4on'
No4fica4on'
Infected'
Health services delay
Access delay
Patie
nt d
elay
Ac4ve'TB'TB'
Diagnosis'
Improved'repor4ng'system'
Regional Strategy to Stop TB in the Western Pacific (2011-2015), WHO WPRO Adapted and modified from “Action framework for higher and earlier TB case detection”, WHO
�����
��
World Health Organization, Western Pacific Regional Office
TB high groups
World Health Organization, Western Pacific Regional Office
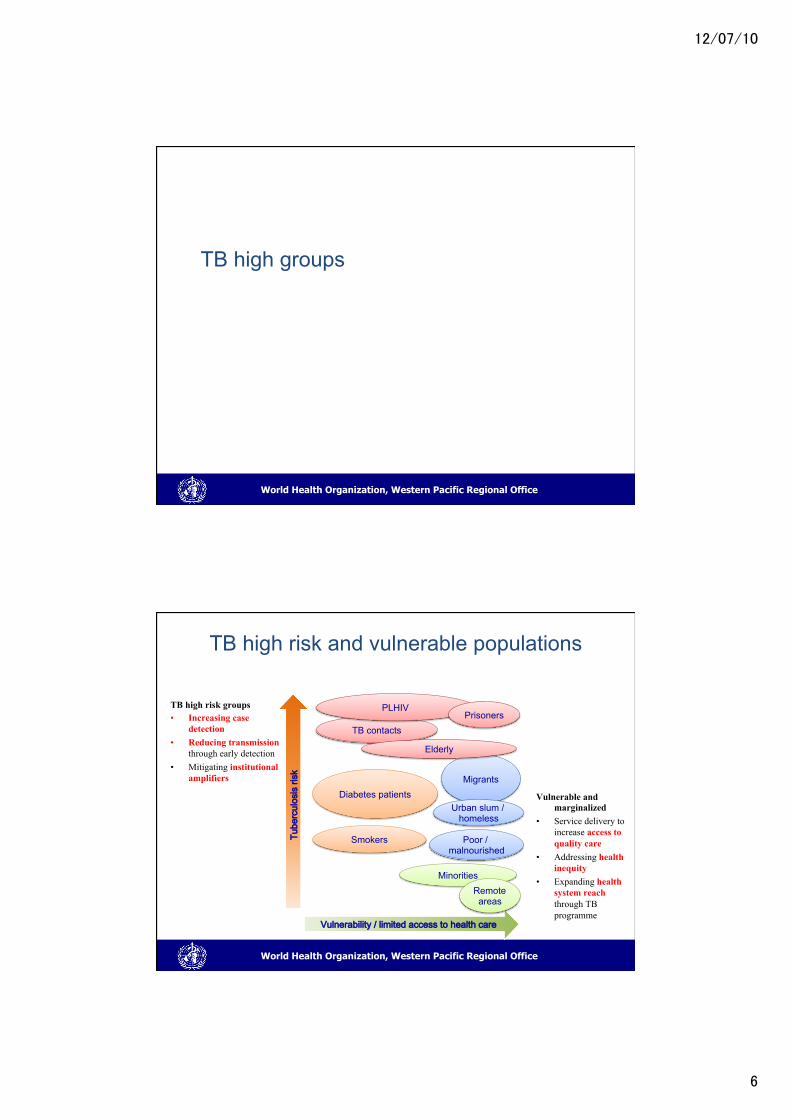
TB high risk and vulnerable populations
TB high risk groups • Increasing case
detection • Reducing transmission
through early detection • Mitigating institutional
amplifiers
Vulnerable and marginalized
• Service delivery to increase access to quality care
• Addressing health inequity
• Expanding health system reach through TB programme
�����������������
������������������������������������������
Diabetes patients
Smokers
Migrants
Urban slum / homeless
Poor / malnourished
TB contacts
PLHIV Prisoners
Elderly
Minorities Remote areas
�����
��
World Health Organization, Western Pacific Regional Office
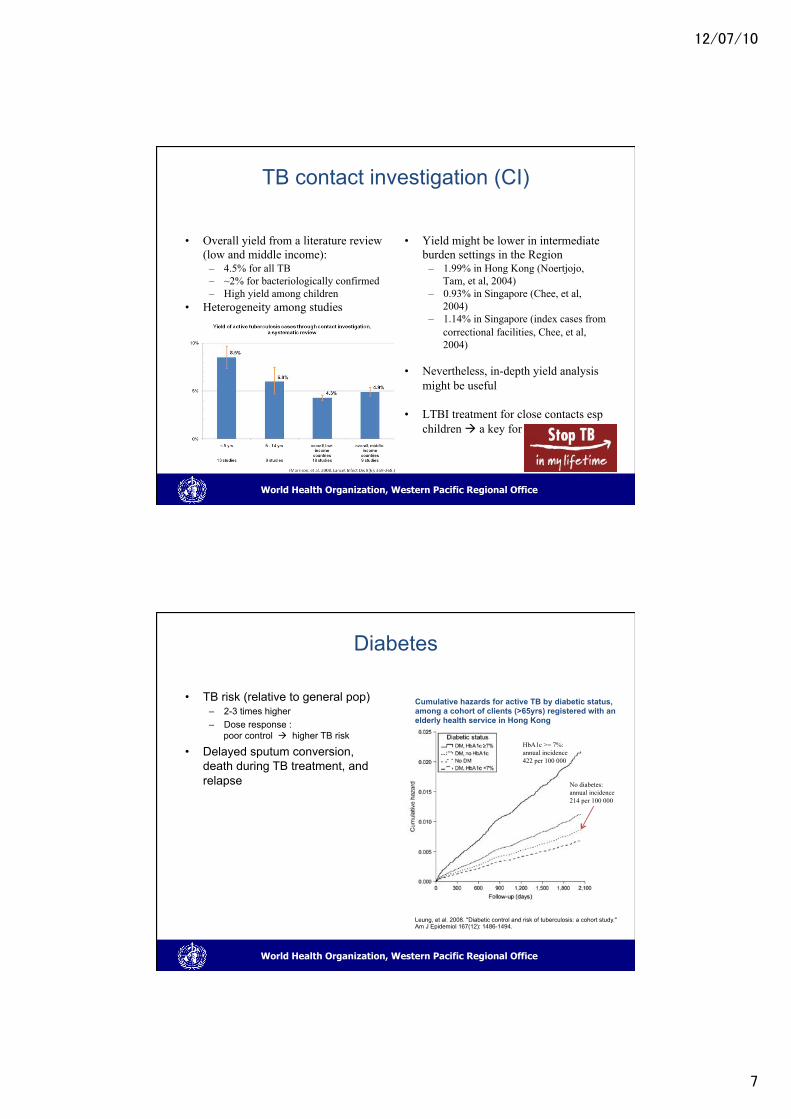
TB contact investigation (CI)
• Overall yield from a literature review (low and middle income):
– 4.5% for all TB – ~2% for bacteriologically confirmed – High yield among children
• Heterogeneity among studies
• Yield might be lower in intermediate burden settings in the Region
– 1.99% in Hong Kong (Noertjojo, Tam, et al, 2004)
– 0.93% in Singapore (Chee, et al, 2004)
– 1.14% in Singapore (index cases from correctional facilities, Chee, et al, 2004)
• Nevertheless, in-depth yield analysis might be useful
• LTBI treatment for close contacts esp children ! a key for
World Health Organization, Western Pacific Regional Office
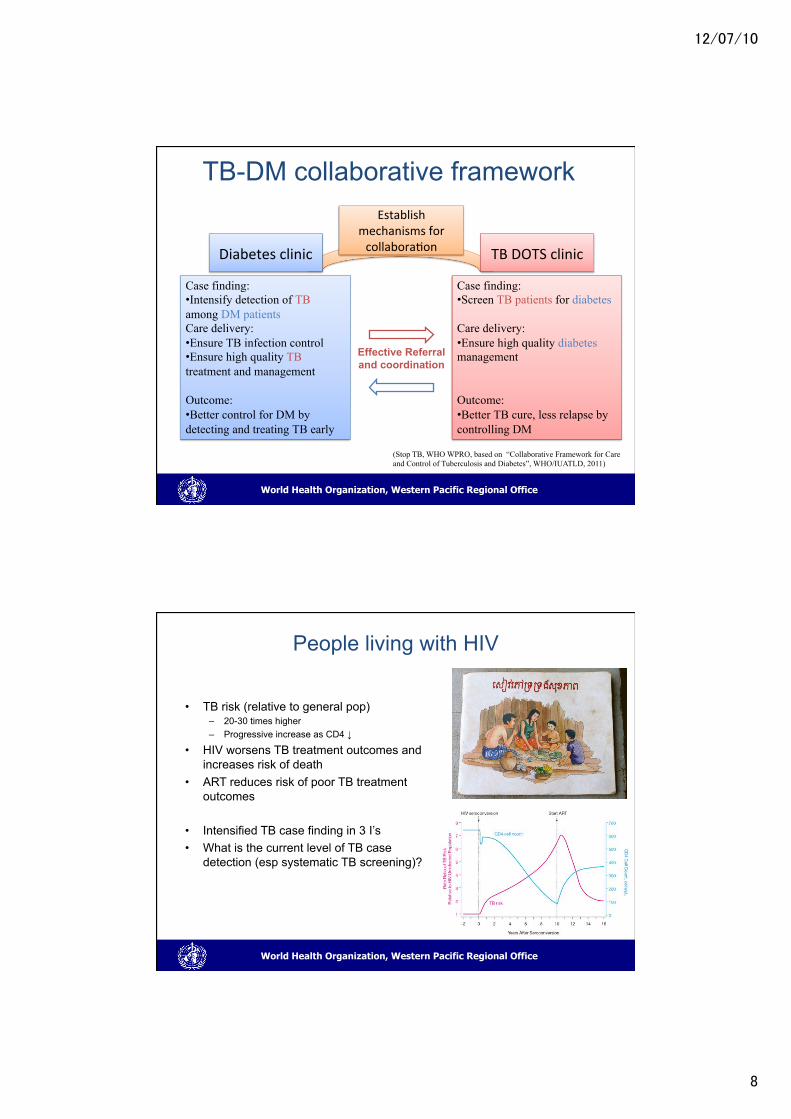
Diabetes
• TB risk (relative to general pop) – 2-3 times higher – Dose response :
poor control ! higher TB risk
• Delayed sputum conversion, death during TB treatment, and relapse
Cumulative hazards for active TB by diabetic status, among a cohort of clients (>65yrs) registered with an elderly health service in Hong Kong
Leung, et al. 2008. "Diabetic control and risk of tuberculosis: a cohort study." Am J Epidemiol 167(12): 1486-1494.
HbA1c >= 7%: annual incidence 422 per 100 000
No diabetes: annual incidence 214 per 100 000
�����
��
World Health Organization, Western Pacific Regional Office
TB-DM collaborative framework
Diabetes"clinic� TB"DOTS"clinic�
Case finding: • Intensify detection of TB among DM patients Care delivery:�• Ensure TB infection control • Ensure high quality TB treatment and management Outcome:�• Better control for DM by detecting and treating TB early
Case finding: • Screen TB patients for diabetes Care delivery: • Ensure high quality diabetes management Outcome: • Better TB cure, less relapse by controlling DM
Effective Referral and coordination
Establish"mechanisms"for"collabora>on�
(Stop TB, WHO WPRO, based on “Collaborative Framework for Care and Control of Tuberculosis and Diabetes”, WHO/IUATLD, 2011)
World Health Organization, Western Pacific Regional Office
People living with HIV
• TB risk (relative to general pop) – 20-30 times higher – Progressive increase as CD4 ↓
• HIV worsens TB treatment outcomes and increases risk of death
• ART reduces risk of poor TB treatment outcomes
• Intensified TB case finding in 3 I’s • What is the current level of TB case
detection (esp systematic TB screening)?
�����
��
World Health Organization, Western Pacific Regional Office
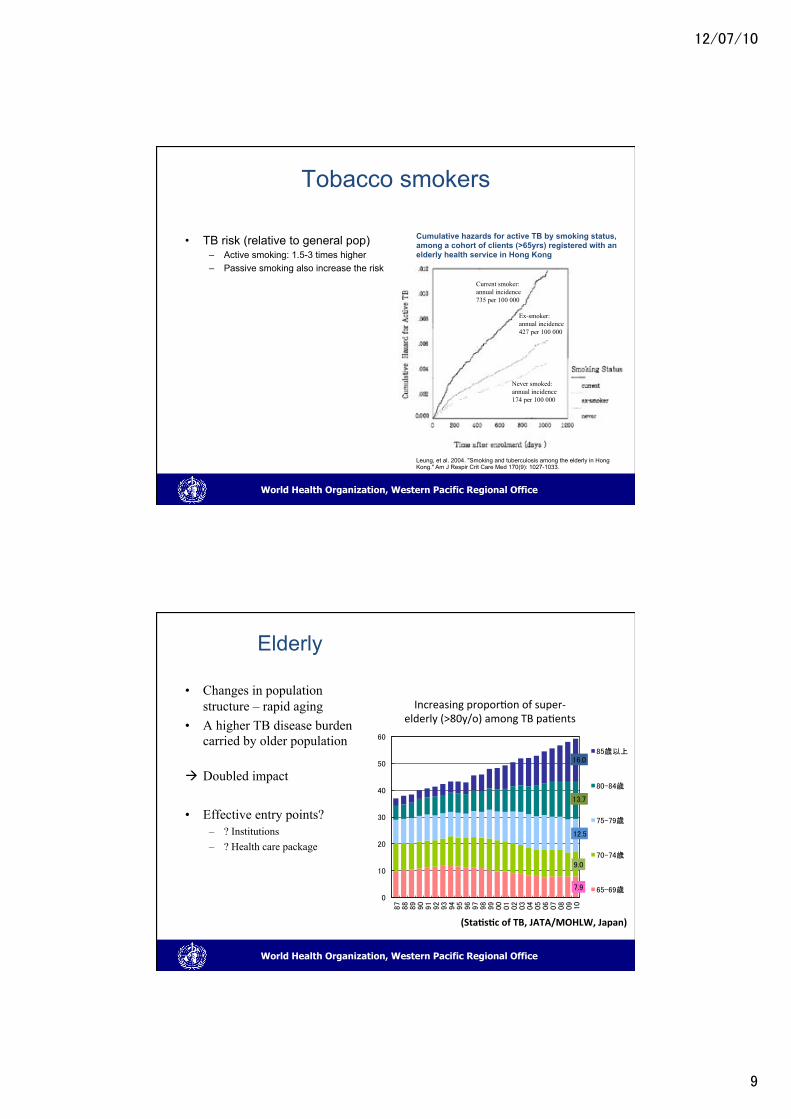
Tobacco smokers
• TB risk (relative to general pop) – Active smoking: 1.5-3 times higher – Passive smoking also increase the risk
Current smoker: annual incidence 735 per 100 000
Ex-smoker: annual incidence 427 per 100 000
Never smoked: annual incidence 174 per 100 000
Cumulative hazards for active TB by smoking status, among a cohort of clients (>65yrs) registered with an elderly health service in Hong Kong
Leung, et al. 2004. "Smoking and tuberculosis among the elderly in Hong Kong." Am J Respir Crit Care Med 170(9): 1027-1033.
World Health Organization, Western Pacific Regional Office
Elderly
• Changes in population structure – rapid aging
• A higher TB disease burden carried by older population
! Doubled impact
• Effective entry points? – ? Institutions – ? Health care package
�����
����
�����
�����
����
�
�
��
��
�
��
��
�������������������� ���������������������� ������������
������
��� ��
�������
��� ��
�������
(Sta4s4c'of'TB,'JATA/MOHLW,'Japan)�
Increasing"propor>on"of"superUelderly"(>80y/o)"among"TB"pa>ents"
�����
�
World Health Organization, Western Pacific Regional Office
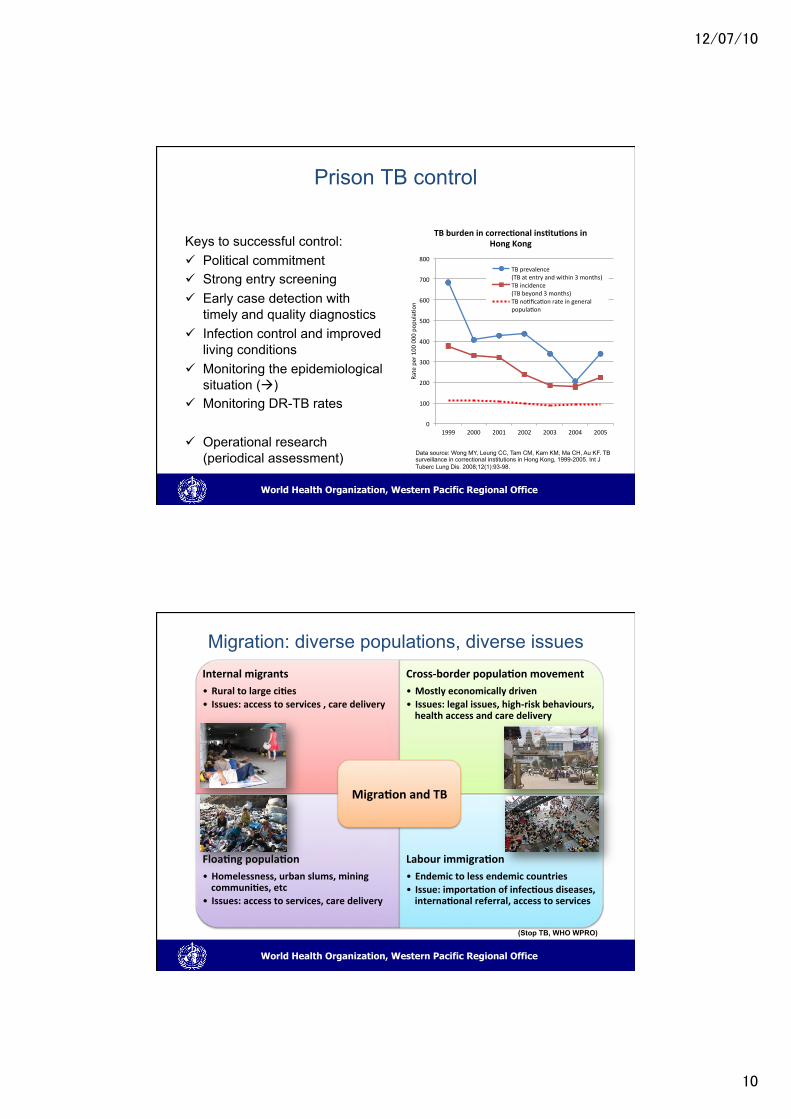
Prison TB control
Keys to successful control: " Political commitment " Strong entry screening " Early case detection with
timely and quality diagnostics " Infection control and improved
living conditions " Monitoring the epidemiological
situation (!) " Monitoring DR-TB rates
" Operational research (periodical assessment)
0"
100"
200"
300"
400"
500"
600"
700"
800"
1999" 2000" 2001" 2002" 2003" 2004" 2005"
Rate"per"100
"000"pop
ula>
on"
TB'burden'in'correc4onal'ins4tu4ons'in'Hong'Kong'
TB"prevalence""(TB"at"entry"and"within"3"months)"TB"incidence""(TB"beyond"3"months)"TB"no>fica>on"rate"in"general"popula>on"
Data source: Wong MY, Leung CC, Tam CM, Kam KM, Ma CH, Au KF. TB surveillance in correctional institutions in Hong Kong, 1999-2005. Int J Tuberc Lung Dis. 2008;12(1):93-98.
World Health Organization, Western Pacific Regional Office
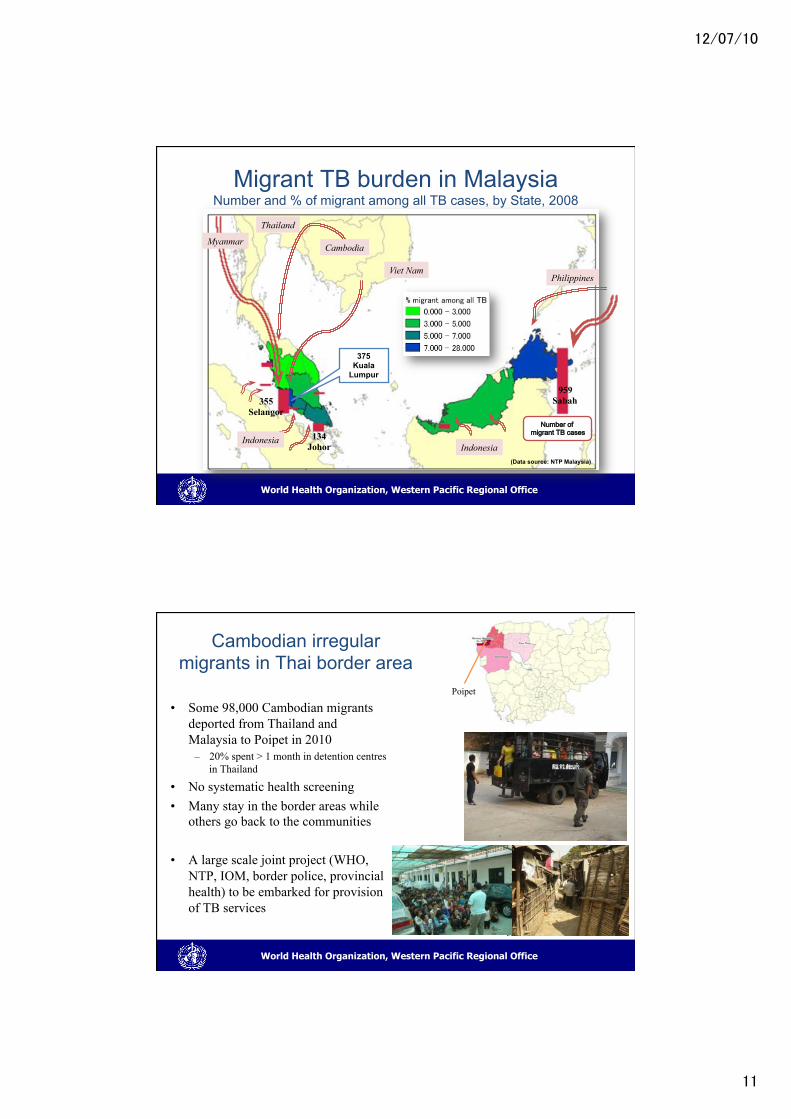
Migration: diverse populations, diverse issues Internal'migrants'
• Rural'to'large'ci4es'• Issues:'access'to'services','care'delivery'
CrossBborder'popula4on'movement'
• Mostly'economically'driven'• Issues:'legal'issues,'highBrisk'behaviours,'health'access'and'care'delivery'
'
Floa4ng'popula4on'
• Homelessness,'urban'slums,'mining'communi4es,'etc'
• Issues:'access'to'services,'care'delivery'
"
Labour'immigra4on'
• Endemic'to'less'endemic'countries'• Issue:'importa4on'of'infec4ous'diseases,'interna4onal'referral,'access'to'services'
Migra4on'and'TB'
(Stop TB, WHO WPRO)
�����
�
World Health Organization, Western Pacific Regional Office
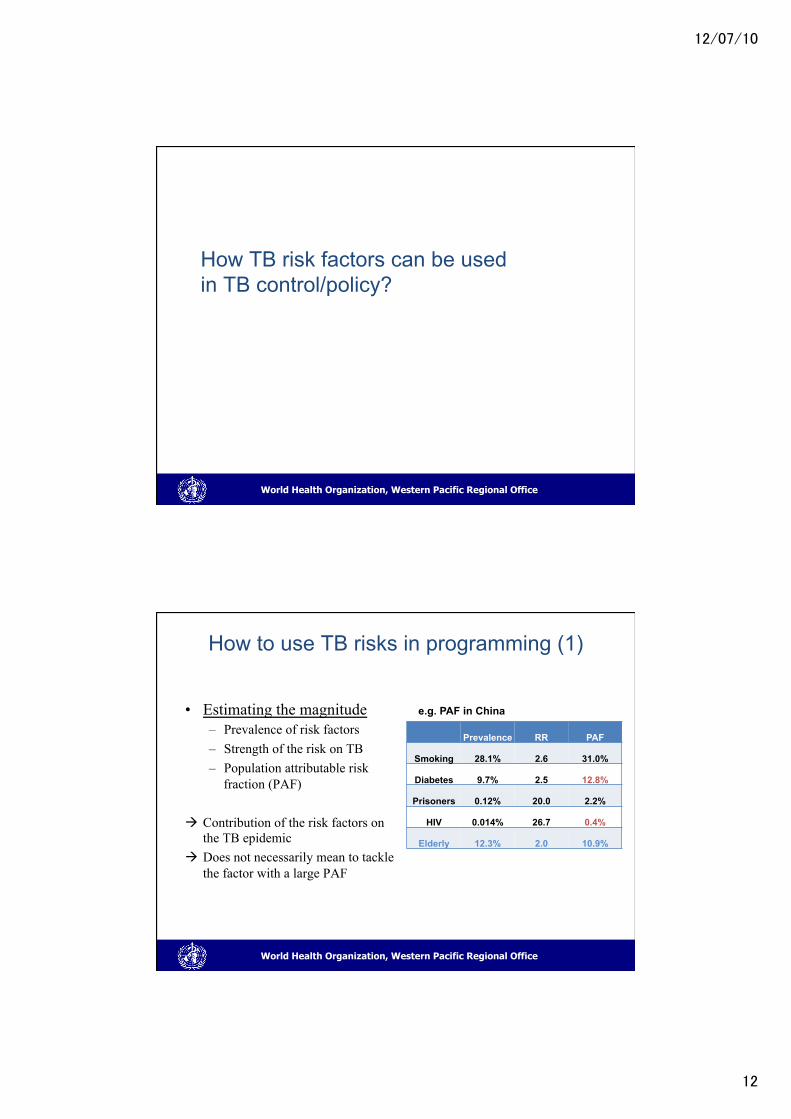
Migrant TB burden in Malaysia Number and % of migrant among all TB cases, by State, 2008
�
������������ �������������
959 Sabah 355
Selangor
134 Johor
375 Kuala
Lumpur �
Myanmar�
Thailand�
Cambodia�
Viet Nam�Philippines�
Indonesia�Indonesia�
(Data source: NTP Malaysia)
World Health Organization, Western Pacific Regional Office
Cambodian irregular migrants in Thai border area
• Some 98,000 Cambodian migrants deported from Thailand and Malaysia to Poipet in 2010
– 20% spent > 1 month in detention centres in Thailand
• No systematic health screening • Many stay in the border areas while
others go back to the communities
• A large scale joint project (WHO, NTP, IOM, border police, provincial health) to be embarked for provision of TB services
Poipet
�����
��
World Health Organization, Western Pacific Regional Office
How TB risk factors can be used in TB control/policy?
World Health Organization, Western Pacific Regional Office
How to use TB risks in programming (1) • Estimating the magnitude
– Prevalence of risk factors – Strength of the risk on TB – Population attributable risk
fraction (PAF)
! Contribution of the risk factors on the TB epidemic
! Does not necessarily mean to tackle the factor with a large PAF
Prevalence RR PAF
Smoking 28.1% 2.6 31.0%
Diabetes 9.7% 2.5 12.8%
Prisoners 0.12% 20.0 2.2%
HIV 0.014% 26.7 0.4%
Elderly 12.3% 2.0 10.9%
e.g. PAF in China
�����
��
World Health Organization, Western Pacific Regional Office
How to use TB risks in programming (2)
• Upstream determinants vs downstream risk factors – e.g. addressing poverty vs targeted
service delivery for homeless – e.g. advocate for smoking reduction vs
smoking cessation among TB patients
• Use of risk markers for targeted service delivery – e.g. ACF in urban slum – e.g. ACF among homeless
• Potential impact on TB epidemics – e.g. targeted population likely produce
more secondary cases (urban slums, prisons, etc)
Increased risk of TB
Poverty
Homeless Urban slum
Mal-nutrition
[0,0)[0,0.5429298)[0.5429298,1.032532)[1.032532,1.637538)[1.637538,221.7128]
Standardized Incidence (all forms)
[0,0)[0,0.5429298)[0.5429298,1.032532)[1.032532,1.637538)[1.637538,221.7128]
Standardized Incidence (all forms)
[0,0)[0,0.5429298)[0.5429298,1.032532)[1.032532,1.637538)[1.637538,221.7128]
Standardized Incidence (all forms)
[0,0)[0,0.5429298)[0.5429298,1.032532)[1.032532,1.637538)[1.637538,221.7128]
Standardized Incidence (all forms)
Neighbourhood"factor"analysis"and""targeted"interven>ons"
�����
�
World Health Organization, Western Pacific Regional Office
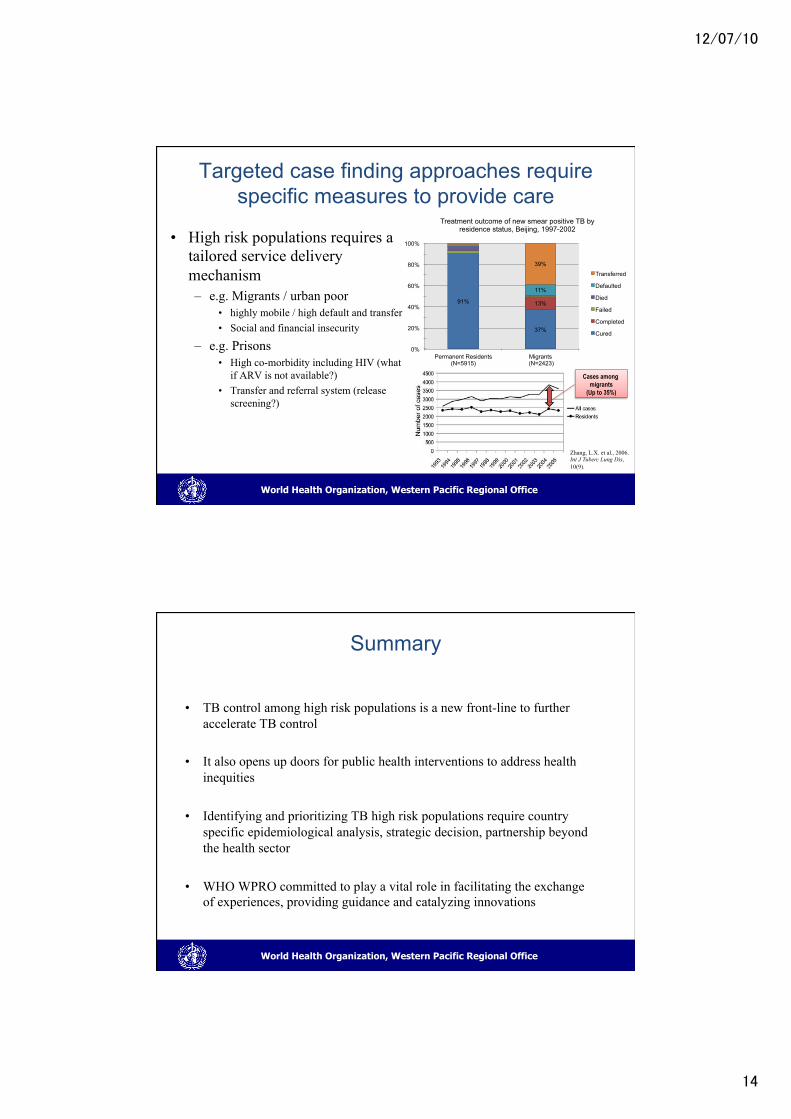
Targeted case finding approaches require specific measures to provide care
• High risk populations requires a tailored service delivery mechanism – e.g. Migrants / urban poor
• highly mobile / high default and transfer • Social and financial insecurity
– e.g. Prisons • High co-morbidity including HIV (what
if ARV is not available?) • Transfer and referral system (release
screening?)
91%
37%
13%
11%
39%
0%
20%
40%
60%
80%
100%
Permanent Residents (N=5915)
Migrants (N=2423)
Treatment outcome of new smear positive TB by residence status, Beijing, 1997-2002
Transferred
Defaulted
Died
Failed
Completed
Cured
Cases among migrants
(Up to 35%)
Zhang, L.X. et al., 2006. Int J Tuberc Lung Dis, 10(9).�
World Health Organization, Western Pacific Regional Office
Summary
• TB control among high risk populations is a new front-line to further accelerate TB control
• It also opens up doors for public health interventions to address health inequities
• Identifying and prioritizing TB high risk populations require country specific epidemiological analysis, strategic decision, partnership beyond the health sector
• WHO WPRO committed to play a vital role in facilitating the exchange
of experiences, providing guidance and catalyzing innovations