
Treatment Goals, Assessment, and Evaluation Practices in ...
25
1 Treatment Goals, Assessment, and Evaluation Practices in Rape Crisis Centers Rachael Voth Schrag; Tonya Edmond Abstract Counselors in Rape Crisis Centers (RCCs) provide crucial services to survivors of sexual violence. However, little is known about RCCs, including the treatment goals and assessment strategies of counselors. Counselors in all Texas RCCs (N=83) were invited to participate in a web-based survey. Participants were asked to indicate which treatment goals they frequently identified and assessed, as well as their usual assessment techniques. Counselors endorsed treatment goals around self-esteem, empowerment, and relational functioning, along with trauma and mental health. Fewer counselors endorsed goals around drugs/alcohol, or school/work/sexual functioning. Counselors in urban settings were more likely to endorse goals related to mental health. Gaps were noted between counselors’ goals and how often outcomes are assessed. Increasing the use of assessments in practice could promote the provision of effective services and increase access to funding. Key Words: Sexual Assault, Victim Services, Counseling, Clinical Measurement
Transcript of Treatment Goals, Assessment, and Evaluation Practices in ...

1
Treatment Goals, Assessment, and Evaluation Practices in Rape Crisis Centers
Rachael Voth Schrag; Tonya Edmond
Abstract
Counselors in Rape Crisis Centers (RCCs) provide crucial services to survivors of sexual
violence. However, little is known about RCCs, including the treatment goals and assessment
strategies of counselors. Counselors in all Texas RCCs (N=83) were invited to participate in a
web-based survey. Participants were asked to indicate which treatment goals they frequently
identified and assessed, as well as their usual assessment techniques. Counselors endorsed
treatment goals around self-esteem, empowerment, and relational functioning, along with trauma
and mental health. Fewer counselors endorsed goals around drugs/alcohol, or school/work/sexual
functioning. Counselors in urban settings were more likely to endorse goals related to mental
health. Gaps were noted between counselors’ goals and how often outcomes are assessed.
Increasing the use of assessments in practice could promote the provision of effective services
and increase access to funding.
Key Words: Sexual Assault, Victim Services, Counseling, Clinical Measurement
2
Background
Practitioners in Rape Crisis Centers (RCCs) provide crucial services to survivors of
sexual violence, including crisis intervention, advocacy, and individual and group counseling
(Macy, Rizo, Johns, & Ermentrout, 2013; Ullman & Townsend, 2007). Assistance provided by
RCCs is unique, in that it includes “safety, protection, and trauma services that…are not offered
by most other health, human, and legal service providers” (Macy et al., 2013, p. 1041). Survivors
frequently suffer secondary victimization during interactions with judicial, medical and law
enforcement personnel, inhibiting them from seeking services (Maier, 2008). In the face of these
risks, survivors of sexual violence rate RCCs as the most helpful in the aftermath of an assault,
with those accessing RCC services reporting significantly less distress than others (Campbell,
Wasco, Ahrens, Sefl, & Barnes, 2001). RCCs help survivors cope with and heal from sexual
violence and its resultant trauma (Macy et al., 2013).
Strong evidence supports that utilizing standardized assessments of outcomes can
enhance treatment planning, implementation, and evaluation of counseling services (Mazefsky &
White, 2013). Benefits include better targeting of interventions, improved service delivery,
improved outcomes, and increased funding (Dennison, 2002). However, the treatment goals or
accompanying assessment techniques of RCC practitioners are unknown. This study seeks to
identify counselors’ treatment goals and assessment approaches. It also examines any differences
by agency location or counselor educational attainment.
The Rape Crisis Center Service Sector
Nearly 1,100 RCCs operate within the United States, but the RCC service sector has been
described as a “black box,” as there is a general understanding of the goals, aims, and values of
RCCs, but little knowledge of the inner workings of agencies (Macy, Giattina, Sangster, Crosby,
3
& Montijo, 2009). RCCs serve adult and child survivors who have experienced a wide range of
types of sexual violence, including rape, sexual assault, incest, child sexual abuse, and sexual
harassment perpetrated by strangers, acquaintances, and intimate partners (Shaw & Campbell,
2011). Typical RCC services include crisis intervention, hospital & legal advocacy and support,
individual and group counseling, and case management services (Shaw & Campbell, 2011).
The de-centralized, grassroots nature of the service sector has led to considerable
variation in the structure, delivery, and services from agency to agency (Macy et al., 2013; Shaw
& Campbell, 2011). The work of Macy and colleagues (2013) highlights differences in service
delivery practices between RCC providers in urban and rural areas. They find that rural
practitioners emphasize flexibility and the provision of holistic services and the need to break
down as many barriers to access as possible (Macy et al., 2013).
Trauma Treatment for Sexual Assault Survivors
The consequences of sexual violence for adult and child survivors are well documented.
Survivors experience a range from minimal symptomology to serious and life-long mental and
physical health consequences (Olafson, 2011; Putnam, 2003). Negative long-term impacts
include increased rates of depression, posttraumatic stress disorder, and anxiety disorders
(Regehr, Alaggia, Dennis, Pitts, & Saini, 2013). Survivors also face higher rates of substance
use disorders, physical health challenges, self-blame, and difficulties with functioning (Regehr et
al., 2013). For children, the consequences of sexual violence include psychological
symptomology, impaired daily functioning in childhood and adulthood, and changes in self
image and perceptions of the world (Olafson, 2011). Survivors of sexual violence are also at an
increased risk of revictimization, emphasizing the need for intervention to address the negative
impacts of sexual violence and disrupt abusive cycles (Olafson, 2011). The serious impacts of

4
sexual violence are clear. However, the ways in which counselors in RCCs conceptualize their
goals when working with survivors, their processes for assessing survivors’ needs, and for
evaluating the effectiveness of their work, is unknown.
Impact of Setting on Service Delivery
There is strong evidence that geographic setting plays a major role in the delivery of effective
social services. Previous work demonstrates that the majority of services for victims of all kinds
are situated in an urban context, and few studies have been published that take rurality into
account when examining sexual assault programs (Logan, Evans, Stevenson, & Jordan, 2005;
Van Hightower & Gorton, 2002). Yet rural survivors of sexual assault face many challenges that
their urban counterparts do not, partly stemming from challenges in accessing services (Lewis,
2003; Macy, et al., 2013). Areas with smaller populations have a lower tax base to publicly fund
such services, and a lack of transportation and isolation also complicate service delivery
(Stommes & Brown, 2002). Further, mental health services are rare in rural areas (Randall &
Vance, 2005). Survivors of sexual assault who are at risk for developing PTSD may not receive
the treatment they need from traditional mental health centers, making any services provided by
rape crisis centers that much more critical. RCCs in rural areas also employ fewer practitioners
who possess the advanced degrees that are often associated with counseling tasks, even as they
seek to provide such services, potentially creating additional barriers to service delivery
(Edmond, Lawrence, & Voth Schrag, 2016; Edmond & Voth Schrag, 2017). Despite the unique
characteristics and challenges associated with service delivery in rural areas, few studies to date
have specifically examined any potential service differences between rural and urban RCCs or
among RCC providers with different levels of education (Lewis, 2003).
Treatment Planning and Assessment

5
Accurate assessment is a key step in the provision of effective services, and is critical in
treatment planning. It informs the practitioner and service recipient’s case conceptualization,
understanding of specific needs, and decision making around intervention and treatment choices
(Mazefsky & White, 2013). It can identify potential roadblocks before they arise, and serve as a
basis for making choices regarding the use of resources (Sellborn, Marion, & Bagby, 2013).
Assessment can also inform treatment planning by challenging a practitioner’s clinical
impressions and encouraging attention in areas of need (Sellborn, et al., 2013). The use of
assessments can help counselors make evidence-based treatment recommendations and identify
key areas for work, which is especially critical when treatment may be time-limited due to
financial or other constraints (Mazefsky & White, 2013). Further, evidence suggests that mental
health service recipients feel positively about participating in assessment, and find the
assessment process helpful (Lyon et al., 2016).
The use of standardized assessments, which are developed based on research and
evidence and made publically available, support treatment through providing evidence for
needed adjustments to enhance the efficacy of services (McLeod, Jensen-Doss, & Ollendick,
2013). Assessment is critical to monitoring client outcomes and program effectiveness. Using
standardized assessments can document successes and point to areas for improvement across
clinicians and program areas, as well as provide information for planning (Sellborn, et al., 2013).
Assessment techniques vary across settings and disciplines, from clinical impressions and
single case evaluations to agency wide efforts in collaboration with researchers. While important
in developing a holistic understanding of the client, ‘clinical impressions’ (i.e. the providers
sense of the clients’ needs and diagnoses based on conversation or unstructured interviews) have
been documented to result in less accurate diagnosis and provision of less relevant treatment

6
(Wilson, Sherritt, Gates, & Knight, 2004). Comparatively, the use of standardized measures to
assess specific domains has been identified as an important method for enhancing the quality of
treatment (Berkman & Marimaldi, 2001). Berkman & Maramaldi (2001) identified a number of
important criteria to consider when evaluating standardized measures for treatment outcomes for
use in practice: (1) conceptual link: the extent to which there is a logical connection between the
assessment, intervention, and outcome to be measured, (2) potential for change: extent to which
the intervention is likely to create change in the outcome being assessed over the chosen time
period, (3) reliability and validity: evidence for minimal measurement error and efficacy in
detecting change, (4) cultural competence: extent to which the assessment strategy is appropriate
for the cultural context of the survivors served by the agency, (5) practicality: the extent to which
the strategy is relatively easy to implement in a busy practice environment.
While the literature provides guidance on best practices for assessment, little is known
regarding the treatment goals and assessment approaches of RCCs. This inhibits our ability to
evaluate services provided, and could be a barrier in the effective implementation of
interventions. Expanding our knowledge can help practitioners as they seek to improve services
and demonstrate effectiveness to funders. Thus, this study sought to identify the treatment goals,
assessment and evaluation strategies of practitioners providing counseling services in RCCs, by
answering these questions: (1) What do practitioners working in RCCs see as the commonly
desired outcomes (treatment goals) of counseling services? (2) What outcomes are routinely
assessed for prior to providing services? (3) What outcomes do practitioners routinely assess for
using standardized measures? (4) What methods do the agencies use to assess the effectiveness
of their counseling programs? (5) Are there differences in these assessment practices based on
provider education level or agency setting (urban/rural location)?

7
Methods
Participants
A quantitative, cross-sectional, web-based survey of counselors from RCCs in Texas was
conducted over the summer of 2013. Practitioners were asked to participate if their job
descriptions included on-going individual or group counseling tasks. Responding counselors (n
= 76) were predominately female (95%), on average 39 years old with three years of experience
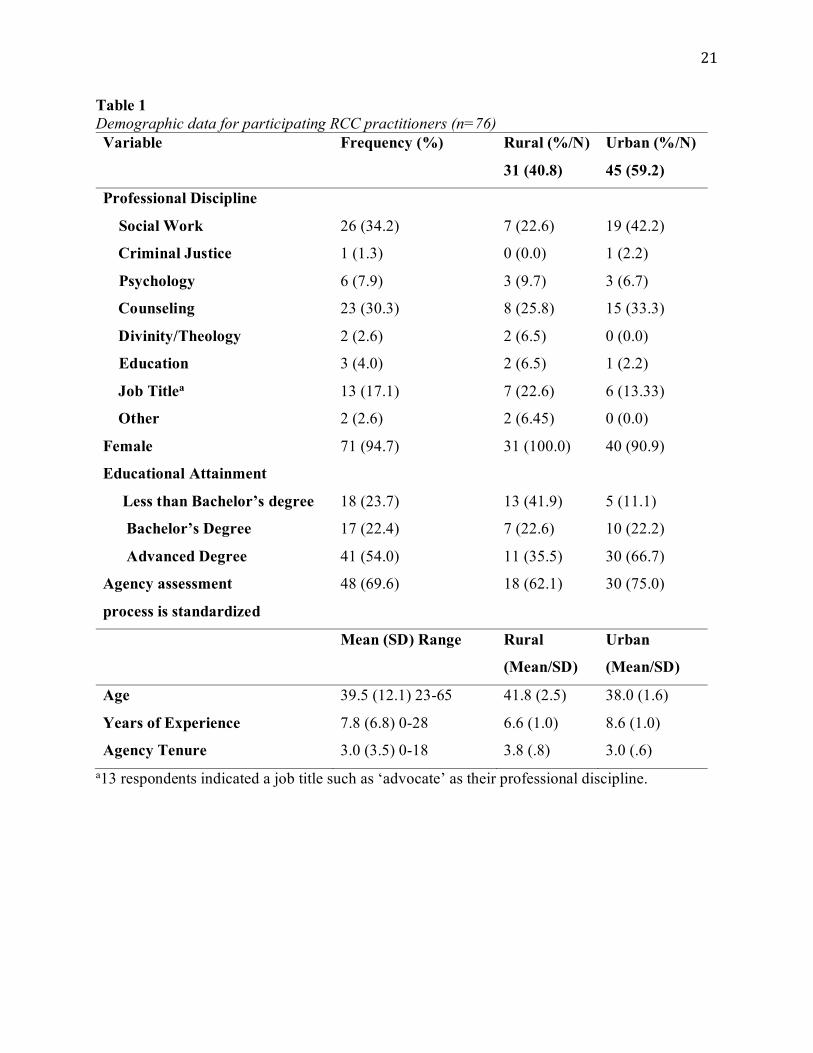
at their current agency and 8 years of experience in this field of practice (see table 1). The
majority identified as social workers and counselors, although many of those without an
advanced degree identified more with their job title (‘advocate,’ ‘counselor,’ etc.) than a
profession (n = 13, 17%). Slightly over half of the counselors (54%) had a Masters or PhD
degree, 22% had a Bachelor’s Degree, and 24% had less than a Bachelor’s Degree. Nearly 60%
worked at agencies in urban or suburban settings, while 40% worked in rural areas.
Approximately 70% of respondents reported that the assessment process used in their agency is
standard across all staff that provide individual or group counseling. <insert table 1>
Materials
Based on the available literature and in consultation with experts in the field, a set of
potential treatment goals and evaluation strategies were identified. These measures were
developed for the current study based on feedback gathered from agency leaders, RCC
counselors, Texas Association Against Sexual Assault (TAASA) staff, and a review of previous
studies of RCCs and domestic violence service agencies (e.g., Edmond, 2004; Macy et al., 2009).
The final checklist of thirteen potential treatment goals (see table 2) spanned three primary
domains- mental health (addressing trauma, PTSD, depression, anxiety, substance use, and
stigma/shame), daily functioning (general, relational, work/school, and sexual functioning), and

8
self-esteem/ empowerment (assertiveness, self-esteem/confidence, and empowerment). From this
list, practitioners were asked to identify which treatment goals they commonly pursue with
survivors in counseling. They were then asked to identify which of these areas they routinely
include in their pre-treatment assessment, and which are routinely assessed using standardized
measures. Finally, 10 potential forms of assessment were identified. These were: clinical
impressions, client satisfaction survey, assessment only before treatment with agency scales,
assessment before and after treatment with agency scales, assessment after treatment with agency
scales, assessment before treatment with standardized scales, assessment before and after with
standardized scales, assessment after treatment with standardized scales, and collaboration with a
university researcher (see table 3). Respondents were asked to indicate which of these forms of
assessment were used in their agencies. Because the study seeks to capture the perceptions of
counselors, no definition of what constitutes a ‘standardized measure’ was provided. As such,
providers may have interpreted the meaning of standardized to indicate ‘consistent.’
Procedure
In close collaboration with the Texas Association Against Sexual Assault (TAASA), the
state coalition of RCCs, a comprehensive list of all Texas RCCs was developed (N = 83). With
TAASA’s endorsement, direct practitioners from all 83 agencies were invited to participate
through postal and e-mail. Agency directors were asked forward the web-survey link to staff
members. Participants were given a $20 gift card as an incentive. Pre-approval for study
procedures was obtained from the Institutional Review Board of the sponsoring university.
Analysis included descriptive statistics and chi-square analysis for differences between
groups. Some missing data occurred due to question non-response. These missing data were
treated in an available-case analysis fashion. The number of included cases is provided for each

9
item in Tables 1-3. The final sample for analysis included 76 counselors from 47 of the 83
agencies, with 57% of all Texas RCCs represented. Forty-seven percent of rural RCCs had at
least one counselor responding, while 61% of urban agencies had a participating counselor.
Results
Commonly Desired Service Outcomes
The most frequently endorsed treatment goals were enhancing self-esteem, confidence
(99%), and a sense of empowerment (94%); improving relational functioning (93%); decreasing
general trauma symptoms (91%); and symptoms of anxiety (90%), depression (87%), and PTSD
(86%). <insert table 2>
Routinely Assessed Service Outcomes
Practitioners most frequently endorsed assessing for mental health, with 85.5% assessing
survivors’ general trauma symptoms, followed by depression (81%), anxiety (78%) and PTSD
(68%). Self-esteem (73.9%) and empowerment (63.8%) were assessed at rates that were similar
to the mental health concerns. Even though less than half of the respondents identified reducing
drug/alcohol abuse as a treatment goal, it was assessed by 56.5%of them. Respondents reported
lower rates of assessment for feelings of stigma/shame (53.6%) and assertiveness (44.9%) even
though these were highly endorsed treatment goals. Seventy-eight percent of respondents
reported assessing general functioning, with fewer assessing specific areas of functioning:
relational (65%), school/work (49%) and sexual (42%).
Use of Standardized Measures
Use of standardized measures for assessment was low across all domains, ranging from
10% for sexual functioning to a high of 38.6% for depression (see Table 2). Practitioners most
frequently used standardized measures to assess mental health: Depression (38.6%), general

10
trauma symptoms (37.1%), anxiety (35.7%), PTSD (34.3%), and drugs/alcohol abuse (21.3%).
Use of standardized measures for functioning or empowerment outcomes was uncommon.
Methods for Evaluating Effectiveness
Practitioners reported using a variety of methods to evaluate the effectiveness of their
work (see Table 3). The highest level of endorsement was for client satisfaction surveys
(84.3%), followed by clinical impressions (41.4%) and assessment before and after treatment
with agency developed scales (38.6%). Fewer than one in four use standardized scales before
and after treatment (24.3%). Client focus groups are employed by 15.7% of these agencies, and a
small number of agencies (n = 6; 8.6%) collaborate with university researchers to evaluate
program effectiveness. <insert table 3>
Differences by Rurality and Education
There were a few statistically significant differences in treatment goals or assessment
strategies between urban and rural practitioners. Practitioners in urban settings were significantly
more likely to endorse reduction of anxiety as a treatment goal, χ2 (1, N = 69) = 6.1, p < .05.
Urban practitioners were also more likely to endorse reduction of PTSD (92.5% vs 75.9%) and
enhancement of sexual functioning (65% vs 44.8%) as treatment goals. These may reflect
clinically significant differences, however neither were statistically significant. Practitioners in
rural settings indicated a higher use of “standardized measures only before treatment,” χ2 (1, N =
70) = 4.4, p < .05), and for assessment “before and after treatment,” χ2 (1, N = 70) = 5.01, p <
.05. Several differences between practitioners were observed based on level of education.
Practitioners with an advanced degree and those without any degree were significantly more
likely to select “reduce general trauma,” χ2 (2, N = 69) = 9.1, p < .05, and “reduce PTSD,” χ2 (2,
N = 69) = 6.6, p < .05 as treatment goals. Non-degreed practitioners were also more likely to

11
identify reducing abuse of alcohol and drugs as a goal than those with more education, χ2 (2, N =
69) = 6.7, p < .05. In terms of pretreatment assessment, non-degreed practitioners were more
likely to assess for self-esteem/confidence (93.8%), χ2 (2, N = 69) = 7.37, p < .05. In addition,
they were more likely than their peers with college degrees to assess general functioning in their
clients using a standardized measure (47.1% vs 14.3% and 12.8%), χ2 (1, N = 70) = 8.8, p < .05.
Differences were also found in treatment outcome assessment strategies. Practitioners with
advanced degrees were more likely to use clinical impressions as an assessment strategy (59%)
than those with less education, χ2 (1, N = 70) = 11.2, p<.01, but less likely to assess only after
treatment with scales developed ‘in house’ at the agency, χ2 (2, N = 69) = 6.9, p<.05.
Discussion
RCCs are dedicated to meeting the needs of survivors of violence, and counselors in
these agencies report substantial agreement regarding their goals and aims. They are engaged in
work to empower survivors, improve mental health, and enhance daily functioning. These
common aims, which are clearly aligned with the empirically documented needs of survivors,
can be a primary point for organizing and continuing to develop and expand this vital but often
under resourced sector. Based on this observed alignment, in order to support RCCs in doing
their important work in often under resourced settings, the authors of the current study used
Berkman & Marimaldi’s (2001) criteria to identify a number of assessment measures that could
fit within RCC system constraints and help meet the needs of survivors, practitioners, and
funders. These measures meet Berkman & Marimaldi’s (2001) criteria for acceptable
standardized assessment tools in that they are (1) logically connected to the treatment domains
most frequently endorsed by counselors in RCCs (2) capable of capturing change over time (3)
psychometrically validated (4) Previously used in a range of populations (although individual
12
agencies should always review measures to ensure cultural competence with their specific
setting) and (5) practical, in that they are generally low-cost or free, short, and easy to
administer. Administrators and practitioners in this sector should consider incorporating such
assessments to promote positive client outcomes and meet the expectations of a wide variety of
groups providing funding and oversight. <insert table 4>
Importantly, few differences in treatment goals were seen by agency setting. Given
considerable health disparities in access to treatment between urban and rural settings, the fact
that agencies reported similar goals and strategies should be seen as a positive sign for the RCC
sector in Texas (Singh & Siahpush, 2014). Despite organizational, philosophical or service
differences observed in other studies (Lewis, 2003), the treatment goals, and assessment
strategies of urban and rural providers in Texas seem to be very similar. This could be due to the
leadership of a robust state collation (TAASA), which puts considerable emphasis on and
resources into supporting the wide diversity of agencies in Texas. Indeed a major strength of the
current study was the support and assistance of TAASA leadership and staff in the development
and implementation, demonstrating their on-going commitment to supporting and building the
service sector in the state.
A number of significant differences in treatment goals and assessment strategies were
observed between providers with differing levels of education. An unexpected finding was the
way in which goals, as well as assessment practices were most aligned between practitioners
with advanced degrees and those without any degrees. These two groups of practitioners were
more likely to endorse mental health related treatment goals than practitioners with bachelor’s
degrees. Comparatively, providers with advanced degrees were less likely to assess for self-
confidence and less likely to assess general functioning with standardized measures. This may

13
be related to the fact that undergraduate programs tend to train practitioners for generalist
practice skills such as case management and advocacy, which involves more of a focus on
ameliorating problems with daily functioning and building self-confidence and personal self-
efficacy. Comparatively, graduate social work and psychology programs train practitioners to be
specialists in assessing and treating mental health related problems. Neither of these possible
explanations though accounts for the similarities in assessment practices between those
counselors without any college degrees and those with advanced degrees. Perhaps in the absence
of having a degree those counselors are compensating by more proactively seeking resources to
support their work rather than relying solely on their educational training. Given the number of
non-degreed counselors observed, and their wide range of treatment goals for survivors, state
coalitions and others providing on-going technical assistance to RCCs should consider ways to
resource this important group of practitioners. Interestingly, fewer counselors endorsed
addressing substance abuse issues as a goal than endorsed screening for them. It could be that
agencies are more likely to refer out for substance treatment, so counselors may screen and refer
rather than feel capable of treating substance issues themselves.
Although practitioners’ goals are clearly in line with the needs of survivors as explicated
in the literature, standardized assessment of treatment outcomes is uncommon. There are
substantial gaps between identified treatment goals and the use of standardized assessment tools,
which may hinder the assessment of both the specific treatment needs of a client and the
effectiveness of their treatment. In addition, it limits the ability of agencies to evaluate the
effectiveness of their client services. This creates a potential funding vulnerability for RCCs in a
competitive nonprofit environment where funders are increasingly expecting agencies to
demonstrate impact through positive service outcomes (Bliss, 2007). The adoption of

14
standardized assessment tools, such as those outlined in Table 4, could help practitioners more
accurately identify the constellation of symptoms for each survivor. This would in turn inform
the treatment plan and help guide the selection of the interventions most needed. The use of the
same standardized assessments after treatment would help the client and the practitioner see the
impact of their work, which could be an empowering experience for survivors. If each counselor
in the agency employed standardized measures with all of their clients, the agency would be able
to more accurately evaluate the effectiveness of their counseling services and demonstrate to
funders the importance of their services.
RCC practitioners operate in challenging environments with many constraints.
Consequently, it may not be feasible, even with free or low cost instruments, to use standardized
measures for each identified treatment goal. Practitioners are most often using standardized
measures is in the assessment of mental health symptoms, which are often debilitating for
survivors, and where treatment approaches such as CBT and EMDR already incorporate
standardized assessments (Foa, Keane, Friedmna, & Cohen, 2005). This should be viewed
positively, as RCC counselors are prioritizing the formal assessment of critically important
symptoms. However, service to survivors could be improved with such assessments occurring
with greater frequency, across all education levels, and in all RCCs.
Limitations
The study has a number of limitations. Data are from a small sample of providers in a single
state, and all work at agencies that are members of the state coalition against sexual assault.
There are smaller numbers of practitioner’s with no degree (24%) and Bachelors’ degrees (22%)
than advanced degrees, which may influence the findings. Given the moderate response rate,
there may be systematic differences between responding and non-responding agencies (such as

15
shared computer use or other electronic access issues) that jeopardize the generalizability of
findings. Additionally, “Standardized” was not defined, so it is possible that practitioners have
different interpretations of standardization and that some of the variation in use of standardized
measures by educational attainment is an artifact of these differences. There is a risk of social
desirability, which could lead to respondents over-endorsing goals and assessment techniques.
Similarly, as agency contracts are often tied to working towards certain treatment goals or using
certain techniques for evaluation, some items may have been over-endorsed by counselors
concerned about agency funding.
Implications
Sexual violence creates range of consequences, and counselors in RCCs are striving to reduce
symptoms and enhance empowerment and functioning of survivors. RCC practitioners need
access to free or low cost standardized measures that are easy to administer and score in order to
assess the broad constellation of trauma symptoms that survivors have and to enhance the
accuracy of assessments, treatment planning, intervention selection and monitoring of treatment
outcomes. Where measures are lacking, work should focus on development of tools to assess
key domains identified by counselors as central to their work. For example, a clinically useful
tool for assessing change in survivors’ perceptions of stigma and shame related to sexual
violence could be an important contribution for RCCs. Expanding the use of such tools in RCCs
could improve the effectiveness of assessment and treatment for survivors of sexual violence and
provide stronger data to assess effectiveness. This could help the field address funding needs by
better meeting the reporting expectations of a wide array of potential funders, including
foundations, private donors, and federal and state agencies. <insert table 4>

16
References
Berkman, B., & Maramaldi, P., (2001). Use of standardized measures in agency based research
and practice. Social Work Health & Mental Health, 34(1/2), 115-129. DOI:
10.1080/00981380109517021
Birmaher, B., Brent, D. A., Chiappetta, L., Bridge, J., Monga, S., & Baugher, M. (1999).
Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders.
Journal of the American Academy of Child & Adolescent Psychiatry, 38, 1230-1236.
DOI: 10.1097/00004583-199910000-00011
Bliss, D. L. (2007). Implementing an outcomes measurement system in substance treatment
programs. Administration In Social Work, 31(4), 83-101. DOI: 10.1300/J147v31n04_07
Briere, J. (1996), Psychometric review of the Trauma Symptom Checklist-40, in B.H. Stamm
(Ed.). Measurement of stress, trauma, and adaptation. Lutherville, MD: Sidran Press.
Bryant, R. A., Harvey, A. G., Dang, S. T., & Sackville, T. (1998). Assessing acute stress
disorder: Psychometric properties of a structured clinical interview. Psychological
Assessment, 10, 215-220. DOI: 10.1037/1040-3590.10.3.215
Campbell, R., Wasco, S., Ahrens, C., Sefl, T., & Barnes, H. (2001). Preventing the second rape:
Rape survivors’ experiences with community service providers. Journal of Interpersonal
Violence, 16 (1), 1239–1259. DOI: 10.1177/088626001016012002
Dennison, S. (2002). Integrating standardized measures into social work practice. Professional
Development. 5(2), 1097-4911.
Edmond, T. (2004, September). Theoretical and intervention preferences of service providers addressing
violence against women: A national survey. Paper presented at the 9th International Conference
on Family Violence, San Diego, CA.
17
Edmond, T., Lawrence, K., & Voth Schrag, R. J., (2016). Perceptions and Use of EMDR
Therapy in Rape Crisis Centers. The Journal of EMDR Practice and Research, 10(1),
23-32. DOI: 10.1891/1933-3196.10.11
Edmond, T., & Voth Schrag, R. J., (2017). Assessing receptivity to empirically supported
treatments in rape crisis centers. Advances in Social Work, 18(2), 611-629. DOI:
10.18060/21338
Foa, E., Keene, T., Friedmna, M., & Cohen, J., (2005). Practice Guidelines from the
International Society for Traumatic Stress Studies, 2nd Ed. New York: Guilford Press.
Goodman, L., Cattaneo, L B., Thomas, K., Woulfe, J., Chong, S., & Fels Smyth, K., (2015).
Advancing domestic violence program evaluation. Psychology of Violence. 5(4), 355-
366. DOI: 10.1037/a0038318
Kaplan, R., Ganiats, T., and Sieber, W.,(1996). The Quality of Well-Being Self-Administered.
Accessed from https://hoap.ucsd.edu/qwb-info/QWB-Manual.pdf
Kroenke, K., & Spitzer, R., (2002). The PHQ-9 a new depression diagnostic and severity
measure. Psychiatric Annals, 32(9) 1-7. DOI: 10.3928/0048-5713-20020901-06
Lewis, S. H. (2003). Unspoken Crimes: Sexual Assault in Rural America. National Sexual
Violence Resource Center. Accessed from
http://www.nsvrc.org/sites/default/files/Publications_NSVRC_Booklets_Unspoken-
Crimes-Sexual-Assault-in-Rural-America%20.pdf
Logan, T., Evans, L., Stevenson, E., & Jordan, C., (2005). Barriers to services for rural and urban
survivors of rape. Journal of Interpersonal Violence, 20(5), 591-616. DOI:
10.1177/0886260504272899
18
Lyon, A., Ludwig, K., Wassse, J., Bergstrom, A., Hendrix, E., & McCauley, E., (2016).
Determinants and functions of standardized assessment use among school mental health
clinicians: A Mixed methods evaluation. Administration and Policy in Mental Health and
Mental Health Services Research, 43(1) 122-134. DOI: 10.1007/s10488-015-0626-0
Macy, R., Giattina, M., Sangster, T., Crosby, C., & Montijo, N. J. (2009). Domestic violence and
sexual assault services. Aggression and Violent Behavior, 14(5), 359-373. DOI:
10.1177/0886260508329128
Macy, R., Rizo, C., Johns, N., & Ermentrout, D. (2013). Directors’ opinions about domestic
violence and sexual assault service strategies that help survivors. Journal of Interpersonal
Violence, 28(5), 1040-1066. 10.1177/0886260512459375
Maier, S. (2008). I have heard horrible stories: Rape victim advocates’ perceptions of the
revictimization of rape victims by the police and medical system. Violence Against
Women, 14(7), 786–808. DOI: 10.1177/1077801208320245
Mazefsky, C. A., & White, S. (2013). The role of assessment in guiding treatment
planning for youth with ASD. In A. Scarpa, S. Williams White, T. Attwood (Eds.) , CBT
for children and adolescents with high-functioning autism spectrum disorders (pp. 45-
69). New York, NY, US: Guilford Press.
McLeod, B. D., Jensen-Doss, A., & Ollendick, T. H., (2013.) Diagnostic and behavioral
assessment in children and adolescents: A clinical guide. New York, NY, US: Guilford.
Muris, P. (2001). A brief questionnaire for measuring self-efficacy in youths. Journal of
Psychopathology and Behavioral Assessment, 23, 145-149. DOI:
10.1023/A:1010961119608

19
Nader, K., Kriegler, J.A., Blake, D., Pynoos, R., Newman, E., & Weathers, F. (1996).
Clinician-Administered PTSD Scale, Child and Adolescent Version. White River
Junction, VT: National Center for PTSD
Olafson, E., (2011). Child sexual abuse: Demography, impacts, and interventions. Journal of
Child & Adolescent Trauma, (4)1, 8-21. DOI: 10.1080/19361521.2011.545811
Randall, E., & Vance, D., (2005). Directions in rural mental health practice. In R. Lohmann and
N. Lohmann (Eds.), Rural Social Work Practice (pp. 171-186). New York: Columbia
University Press.
Ravens-Sieberer, U., & Bullinger, M., (1998). Assessing health-related quality of life in
chronically ill children with the German KINDL. Quality of Life Research, 7(5), 399-407.
DOI: 10.1023/A:1008853819715
Regehr C, Alaggia R, Dennis J, Pitts A, Saini, M. (2013). Interventions to reduce distress in adult
victims of sexual violence and rape. Campbell Systematic Reviews, 2013(3), 1-133.
Accessed from https://www.campbellcollaboration.org/
Rogers, S., Chamberlin, J., Ellison, M., & Crean, T., (1997). A consumer-constructed scale to
measure empowerment among users of mental health services. Psychiatric Services.
48(8), 1042-1047. DOI: 10.1176/ps.48.8.1042
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton.
Sellbom, M., Marion, B. E., & Bagby, R. (2013). Psychological assessment in adult mental
health. In J. R. Graham, J. A. Naglieri, I. B. Weiner (Eds.) , Handbook of psychology,
Vol. 10: Assessment psychology (2nd ed.) (pp. 241-260). Hoboken, NJ: Wiley.
20
Shaw, J., & Campbell, R. (2011). Rape crisis centers: Serving survivors and their communities.
In T. Bryant-Davis (Ed.) , Surviving sexual violence: A guide to recovery and
empowerment (pp. 112-128). Lanham, MD, US: Rowman & Littlefield.
Singh, G., & Siahpush, M., (2014). Widening rural-urban disparities in life expectancy, U.S.,
1969-2009. American Journal of Preventive Medicine, 46(2), 19-29. DOI:
10.1016/j.amepre.2013.10.017.
Stommes, E., & Brown, D., (2002). Transportation in rural America: Issues for the 21st century.
Rural America, 16(1), 2-10. Accessed from http://frontierus.org/transportation-in-rural-
america-issues-for-the-21st-century/
Ullman. S., & Townsend, S., (2007). Barriers to working with sexual assault survivors: A
qualitative study of rape crisis center workers. Violence Against Women, 13(4) 412-443.
DOI: 10.1177/1077801207299191
Van Hightower, N., & Gorton, J., (2002). A case study of community-based responses to rural
woman battering. Violence Against Women, (8)7, 845-872. DOI:
10.1177/107780102400388506
Weathers, F.W., Litz, B.T., Keane, T.M., Palmieri, P.A., Marx, B.P., & Schnurr, P.P. (2013).
The PTSD Checklist for DSM-5. National Center for PTSD Accessed from
www.ptsd.va.gov.
Weissman MM, Orvaschel H, Padian N. (1980). Children’s symptom and social functioning self-
report scales. Journal of Nervous Mental Disorders, 168(12):736–740.
Wilson, C., Sherrit, L., Gates, E., & Knight, J., (2004). Are clinical impressions of adolescent
substance use accurate? Pediatrics, 114(5), 536-540. DOI: 10.1542/peds.2004-0098
21
Table 1 Demographic data for participating RCC practitioners (n=76) Variable Frequency (%) Rural (%/N)
31 (40.8)
Urban (%/N)
45 (59.2)
Professional Discipline
Social Work 26 (34.2) 7 (22.6) 19 (42.2)
Criminal Justice 1 (1.3) 0 (0.0) 1 (2.2)
Psychology 6 (7.9) 3 (9.7) 3 (6.7)
Counseling 23 (30.3) 8 (25.8) 15 (33.3)
Divinity/Theology 2 (2.6) 2 (6.5) 0 (0.0)
Education 3 (4.0) 2 (6.5) 1 (2.2)
Job Titlea 13 (17.1) 7 (22.6) 6 (13.33)
Other 2 (2.6) 2 (6.45) 0 (0.0)
Female 71 (94.7) 31 (100.0) 40 (90.9)
Educational Attainment
Less than Bachelor’s degree 18 (23.7) 13 (41.9) 5 (11.1)
Bachelor’s Degree 17 (22.4) 7 (22.6) 10 (22.2)
Advanced Degree 41 (54.0) 11 (35.5) 30 (66.7)
Agency assessment
process is standardized
48 (69.6) 18 (62.1) 30 (75.0)
Mean (SD) Range Rural
(Mean/SD)
Urban
(Mean/SD)
Age 39.5 (12.1) 23-65 41.8 (2.5) 38.0 (1.6)
Years of Experience 7.8 (6.8) 0-28 6.6 (1.0) 8.6 (1.0)
Agency Tenure 3.0 (3.5) 0-18 3.8 (.8) 3.0 (.6) a13 respondents indicated a job title such as ‘advocate’ as their professional discipline.

22
Table 2 Frequency of practitioner reported treatment goals, assessment of domains pre-treatment, and assessment of domains with standardized measure (n=69)
Treatment Goals Total Sample
No BA Degree
BA Degree
Advanced Degree
Rural Urban Assessed Pre-Treatment
Assessed: Stand. Measure
N % N % N % N % N % N % N % N %
Trauma Symptoms 63 91.3 16 100 10 71.4 37 94.9* 25 86.2 38 95.0 59 85.5 26 37.1
PTSD Symptoms 59 85.5 15 93.8 9 64.3 35 89.7* 22 75.9 37 92.5 47 68.1 24 34.3
Depression Symptoms 60 87.0 16 100 10 71.4 34 87.2 25 86.2 35 87.5 56 81.2 27 38.6
Anxiety Symptoms 62 90.0 14 87.5 12 85.7 36 92.3 23 79.3 39 97.5* 54 78.3 25 35.7
Abuse of Drugs/Alcohol 33 47.8 11 68.8 3 21.4 19 48.7* 14 48.3 19 47.5 39 56.5 15 21.3
Stigma/Shame 62 90.0 15 93.8 12 85.7 35 89.7 26 89.7 36 90.0 37 53.6 10 14.3
General Functioning 59 85.5 14 87.5 11 78.6 34 87.2 27 93.1 32 80.0 54 78.3 15 21.4
Relational Functioning 64 92.8 15 93.8 13 92.9 36 92.3 26 89.7 38 95.0 45 65.2 10 14.3
Work/School Functioning 53 76.8 15 93.8 10 71.4 28 71.8 24 82.8 29 72.5 34 49.3 9 12.9
Sexual Functioning 39 56.5 9 56.3 6 42.9 24 61.5 13 44.8 26 65.0 29 42.0 7 10.0
Assertiveness 56 81.2 14 87.5 11 78.6 31 79.5 22 75.9 34 85.0 31 44.9 8 11.4
Self-Esteem/Confidence 68 98.6 16 100 14 100 38 97.4 29 100 39 97.5 51 73.9 15 21.4
Empowerment 65 94.2 15 93.8 13 92.9 37 94.9 27 93.1 38 95.0 44 63.8 14 20.3 *p<.05 Chi-Square tests for difference in frequency of endorsing specific treatment goals between urban/rural agencies, or education level of providers (no BA/BA/Advanced)

23
Table 3 Differences in frequency of use for assessment techniques (n=70)
Assessment Technique
Total Sample
No BA Degree
BA Degree
Advanced Degree
Rural Urban
N % N % N % N % N % N % Clinical Impressions 29 41.4 3 17.7 3 21.4 23 59.0** 10 34.5 19 46.3
Client Satisfaction Survey 59 84.3 13 76.5 12 85.7 34 87.2 24 82.8 35 85.4
Client Focus Groups 11 15.7 4 23.5 2 14.3 5 12.8 5 17.2 6 14.6
Assessment only before tx with agency developed scales 3 4.3 1 5.9 1 7.1 1 2.6 2 6.9 1 2.4
Assessment before and after tx with agency scales 27 38.6 8 47.1 4 28.6 15 38.5 10 34.5 17 41.5
Assessment only after tx with agency developed scales 4 5.7 3 17.7 1 7.1 0 0.0* 3 10.3 1 2.4
Assessment only before tx with standardized scales 3 4.3 2 11.8 1 7.1 0 0.0 3 10.3 0 0.0*
Assessment before and after tx with standardized scales 17 24.3 5 29.4 2 14.3 10 25.6 11 37.9 6 14.6*
Assessment only after tx with standardized scales 4 5.7 2 11.8 2 14.3 0 0.0 3 10.3 1 2.4
Collaboration with university researcher 6 8.6 1 5.9 2 14.3 3 7.7 3 10.3 3 7.3
*p<.05 **p<.01 Chi-Square tests for difference in use of assessment methods between urban/rural agencies, or education level of providers (no BA/BA/Advanced)

24
Table 4 Measurement tools that could be used to assess frequently endorsed treatment goals
Measurement Instruments for Adult Survivors
Domain Instrument Purpose Cost
Time to
Administer Available:
Empower-
ment
Empowerment Scale (Rogers,
Chamberlin, Ellison, & Crean,
1997)
Scale to measure empowerment as defined by
consumers of mental health services
Contact the
author
28 items, 10-15
minutes
Contact the author for
rights
Empower-
ment
Measure of Victim
Empowerment Related to Safety
(Goodman et al., 2015)
Self-report scale aimed at assessing
empowerment related to safety from abuse
(Intimate Partner Violence specific)
Published in
Psychology
of Violence 13 items
Published in Psychology
of Violence
Self-Esteem Rosenburg Self-Esteem Scale
(Rosenburg, 1965) A self-report measure of feelings of self-worth. Free
10 items
completed in 5-
10 minutes
http://www.socy.umd.edu/q
uick-links/rosenberg-self-
esteem-scale
Functioning
Quality of Well-Being Scale
(Kaplan, Ganiats, and Sieber,
1996)
A self-report measure of functioning. While
some domains may be inappropriate to an RCC,
subscales from the QWB-SA could be useful.
Free to
nonprofits 10-15 minutes
https://hoap.ucsd.edu/qw
b-info/#
PTSD PTSD Checklist for DSM-V
(Weathers et al., 2013)
Self report measure for PTSD screening and
making provisional diagnosis Free
20 items, 5-10
minutes www.ptsd.va.gov
Anxiety
Acute Stress Disorder Structured
Interview (ASDI) (Bryant et al,
1998)
A clinician administered interview based on
DSM-IV criteria for Acute Stress Disorder,
including dissociative symptoms
Free for
members of
ISTSS
19 items
completed in 5-
10 minutes
http://www.istss.
org

25
Depression Patient Health Questioner (PHQ)
(Kreonke & Spitzer, 2002)
Self-report measure of severity of depression
symptoms. Can also be used for diagnosis using
DSM-IV criteria. Free
9 items
completed in 5-
10 minutes. Phqscreeners.com
Measurement Instruments for Children/Adolescents
Domain Instrument Purpose Cost
Time to
Administer Available At:
Empowerm
ent
Self-Efficacy Questionnaire
for Children (SEQ-C) (Muris,
2001)
Self report measure of three domains of self-
efficacy (academic, emtoinoal, social)
Designed for youth 14-18 years of age Free
24 items, 10-
15 minutes
http://drjenna.net/wp-
content/uploads/2013/0
7/self-
efficacy_questionnaire.
Self-Esteem
&
Functioning
KINDL (Ravens-Sieberer &
Bullinger, 1998)
Self and parent report, including wellbeing,
self-esteem, and functioning. Versions exist
for children aged 4-17.
Free to
non-profits
24 items in 10-
15 minutes
http://www.kindl.org/e
nglish/information/
PTSD
Clinician-Administered PTSD
Scale for Children (Nader et
al., 1996)
Clinician administered scale for youths aged
8-18 assessing the frequency and intensity of
DSM-IV PTSD symptoms Free
33 items in 10-
30 minutes
http://www.ptsd.va.gov
/professional/assessme
nt/child/caps-ca.asp
Anxiety
Screen for Childhood Anxiety
Related Emotional Disorders
(Birmaher et al., 1999)
Child and parent self-report instrument for
anxiety disorders, including GAD, separation
anxiety, panic disorder, and social phobias. Free
41 items
completed in
10 minutes
http://www.psychiatry.
pitt.edu/research/tools-
research/
Depression
CESD/Children (Weissman et
al., 1980)
Self-report inventory for depression
symptomology. Children ages 6-17. Free
20 items/5
minutes
http://www.brightfuture
s.org/mentalhealth/


















