Chiropractic treatment for whiplash injuries in charlotte nc
10/7/2017
1
1
Treatment Plan Goals for Chiropractic
Presented by Evan M. Gwilliam, DC MBA BS
CPC CCPC QCC CPC-I MCS-P CPMA CMHP
Vice President
Dr. Evan Gwilliam• Education
• Bachelor’s of Science, Accounting - Brigham Young University
• Master’s of Business Administration - Broadview University
• Doctor of Chiropractic, Valedictorian - Palmer College of Chiropractic
• Certifications• Certified Professional Coder (CPC) - AAPC
• Certified Chiropractic Professional Coder (CCPC) - AAPC
• Qualified Chiropractic Coder (QCC) - ChiroCode
• Certified Professional Coder – Instructor (CPC-I) - AAPC
• Medical Compliance Specialist – Physician (MCS-P) - MCS
• Certified Professional Medical Auditor (CPMA) – AAPC, NAMAS
• Certified ICD-10 Trainer – AAPC
• Certified MIPS Healthcare Professional (CMHP)– 4Med2

10/7/2017
2
• Learn to create initial care plans that establish the need for careo Understand how to use OATs
o Create effective and relevant patient-centered goals in your own care plans
• Learn how payers use treatment plan goals to determine if care is payable
• Define prognosis, supportive care, MTB, and complicating factors
Take away
What is a Care Plan?
“A care plan is an ordered assembly of expected or planned activities, including observation goals, services, appointments and procedures, usually organized in phases or sessions, which have an objective of organizing and managing health care activity for the patient.” -CMS
4

10/7/2017
3
What is a Care Plan?
1. A list of the complaint, with its relevant diagnoses*
2. Treatments and modalities selected*
3. Duration and frequency of care*
4. Specific treatment goals*
5. Objective measures to show progress*
*for each specific problem
Put another way…
1. Why are you treating the patient?
2. What are you going to do with the patient?
3. How long and how often are you going to see the patient?
4. What are you and the patient trying to accomplish?
5. How do you know when you have accomplished the goals?

10/7/2017
4
7
For example…
1. Nerve related disorders (e.g. radiculopathy)
2. Acute injuries (e.g. sprains and strains)
3. Structural diagnoses (e.g. degenerative disc disease)
4. Functional diagnoses (e.g. difficulty with walking)
5. Soft tissue problems (e.g. myalgia)
6. Symptoms (e.g. neck pain)
7. Complicating factors/comorbidities (e.g. diabetes)
8. External causes (e.g. place and activity)
1. Diagnosis

10/7/2017
5
9
• Follow ICD-10 guidelines (Excludes1, NOS)
• When coding for symptoms, add the phrase “due to” for better specificity.
• Complicating factors may also be coded, if relevant.
• Learn to document a “Diagnostic Statement” or “Clinical Impression” that matches the code requirements.
1. Diagnosis
ICD-10 Guidelines

10/7/2017
6
12
• Do not provide services only because they are routine or part of a philosophical preferenceo If every patient receives 97012 mechanical traction regardless
of injury or patient characteristics, it may appear cookie cutter.
• Explain purpose for a service as it relates to a specific patiento “Therapeutic exercises for the neck will be used to improve
strength to the weakened areas and improve flexibility to areas with documented loss of ROM.”
• Obtain informed consent
2. Treatments and Modalities

10/7/2017
7
13
• Tie the treatments to the diagnoses
• For example, the purpose of 97110 Therapeutic exercise is to develop/improve strength, endurance, range of motion, and/or flexibilityo Diagnoses like M54.2 cervicalgia may not support this service
o But diagnoses like M62.81 muscle weakness might
• 98943 Extraspinal manipulation should not be linked to spinal diagnoseso Such as M50.3- Other cervical disc degeneration
2. Treatments and Modalities
• Plan of care should include recommendations for ongoing amelioration of musculoskeletal complaints, such as:o Home exercise program, injury prevention, lifestyle
modifications, etc
• Introduce as soon as possible, reinforce, and document in the medical record.
• Also consider wellness instructionso Lose weight, increase fluids, improve nutrition, fitness, etc.
14
2. Treatments and Modalities

10/7/2017
8
15
• Set up a “trial” that is adaptable based on evaluations rather than a long term cook book plan for all patients. Move through phases.
• CMS recognizes that:o Acute treatment is shorter duration, higher frequency
o Chronic treatment is longer duration, but lower frequency
• Use a combination of 1. clinical expertise
2. patient expectations
3. evidence-based guidelines
to determine the recommended level of care
3. Duration and frequency
Patient’s Values and Expectations Best Research
Evidence
Individual Clinical Expertise
Best Practices
‘Best’ Best Practices
BP
BP
BPBBP
BP
BBP
Also: customersconsumerspolicymakers

10/7/2017
9
17
1. What is the activity (sleep, walk) the patient will be able to perform?
2. Under what conditions (how far or for how long) will they be able to do it?
3. How well will they be able to do it (without assistance, without increased pain)?
4. When will this be accomplished (2 weeks, 2 months)?
Keep them patient-centered!
4. Goals
18
• Only address frequency and duration of visits
• Neglect goals entirely
• Include goals, but
o They are only subjective
o They do not address function
o They are not measurable
Weak Care Plans
10/7/2017
10
19
Short term goals restated:1. Reduce pain2. Increase pain-free ROM3. Restore normal vertebral segmental motion4. Increase ability to move affected area
Short term goals improved:1. Reduce VNRS from 8/10 to 5/10 within 2 weeks2. Increase pain-free ROM by 50% within 2 weeks3. If you restore normal vertebral segmental motion, you can’t
adjust anymore, right?4. Same as number 2?
20
Two weeks later
Assessment should discuss progress towards goals • Were goals achieved?• If not, why?
• Patient went on vacation• Patient fell down the stairs
• How will the care plan change to adapt to goals that were not met?• Easier or harder exercises?• More or fewer visits? • Referral or new diagnostic test?
10/7/2017
11
21
Short term goals restated:1. Reduce pain by 10% 2. Increase strength (Is there documented loss of strength?)3. Increase endurance (How do you measure this?)4. Increase ability to move affected area (Measurable?)5. Increase ability to exert force to affected area
AND (these are better)
1. Get 5-6 hours of quality sleep (within what time frame?)2. Stand for more than 20 minutes (Is this from Oswestry?)3. Sit for more than 20 minutes pain free4. Walk for more than 1 block pain free5. Lift more than 20 pounds from off the floor
22
5. Progress

10/7/2017
12
23
5. Progress
Outcome Assessment Tools
Patient
Provider
Payer
Public
“Outcomes in clinical practice provide the
mechanism by which the health care provider, the
patient, the public, and the payer are able to assess the end results of care and its effect upon the health of the patient and society.”
• Support medical necessity by quantifying patient functional loss.
• They “objectify the subjective”
• They measure a change in health status after exposure to a health care delivery system.
24
5. Progress
Outcome Assessment Tools
10/7/2017
13
• Neck Disability Index (NDI)
• Oswestry Low Back Questionnaire
• Keele STarT Back Screening tool
• Depression screens (PHQ-2)
25
5. Progress
Outcome Assessment Tools
Neck Disability Index (NDI)
Modified Oswestry Low Back Disability Index
o Ten questions, six responses scored on an ascending scale (0, 1, 2, 3, 4, 5), total is divided by # of points possible
o Higher percentage = worse disability
26
OATs
10/7/2017
14
27
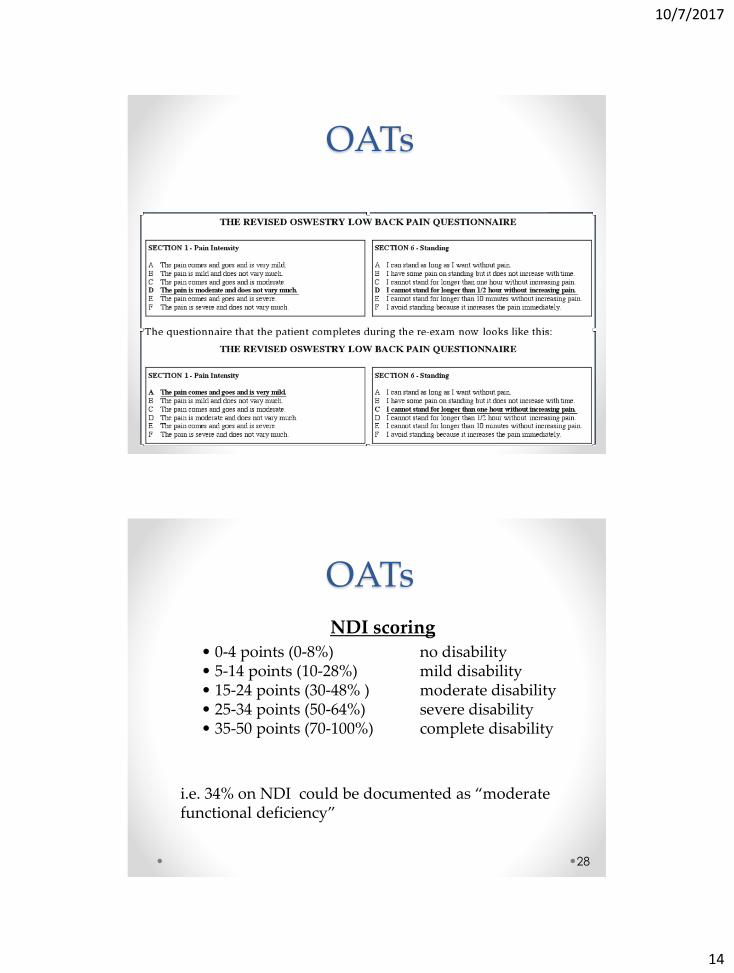
OATs
NDI scoring• 0-4 points (0-8%) no disability• 5-14 points (10-28%) mild disability• 15-24 points (30-48% ) moderate disability• 25-34 points (50-64%) severe disability• 35-50 points (70-100%) complete disability
i.e. 34% on NDI could be documented as “moderate functional deficiency”
28
OATs
10/7/2017
15
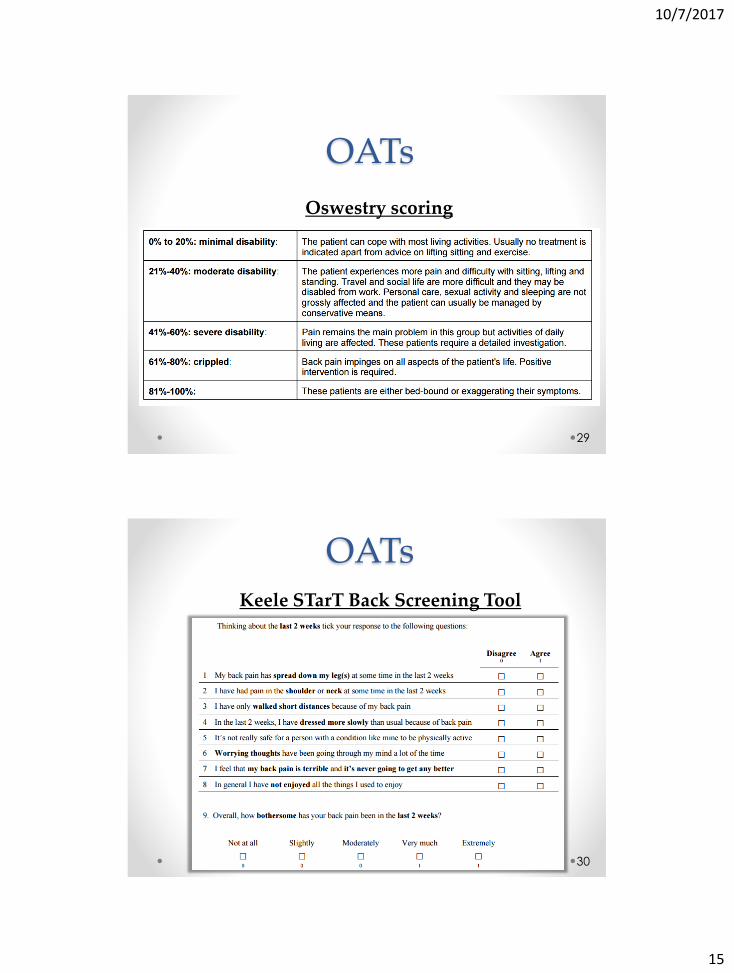
Oswestry scoring
29
OATs
30
OATsKeele STarT Back Screening Tool

10/7/2017
16
31
OATsPatient Health Questionnaire-2 (PHQ-2)
32
OATs
• 10% improvement = minimum detectable change• 30% improvement = meaningful change• 50% improvement = substantial change
Consider re-administering questionnaire at a minimum of every 30 days and also at midpoint of initial trial of care (i.e. 2 weeks)

10/7/2017
17
OATs Inspired Goals
• Goals need to be measurable and specific
• Change ADL by this much by this date
“Improve NDI from 60% to 30% by re-evaluation scheduled for 6/1/18”
“Enable patient to lift heavy weights without pain by 5/1/2018.” - from NDI, section 3
“Improve ability to stand without pain from 30 minutes to one hour by 5/20/2018.” - from Oswestry, section 6
33
OATs
34
OATs
Scenario 1: Score improves as expected• Proof that the treatment plan worked. Care
should continue until MTB is reached.Scenario 2: Score worsens or falls short of goal
• Look for a new treatment and/or refer or discharge.
Scenario 3: Score improves more than expected• Decrease frequency of care, create new
optimistic goals, or release from care.
10/7/2017
18
Are these questions answered?
1. Why are you treating the patient?
2. What are you going to do with the patient?
3. How long and how often are you going to see the patient?
4. What are you and the patient trying to accomplish?
5. How do you know when you have accomplished the goals?
Prognosis is used to forecast the probable result of treatment for a patient’s condition.
Short term – symptomatic
Long term – functional
1. Excellent
2. Good
3. Fair
4. Poor
5. Guarded
6. Unstable
Prognosis

10/7/2017
19
1. Excellent – full symptomatic and functional recovery expected within 2-4 weeks
2. Good - Symptomatic and functional recovery is expected in approximately 4- 8 weeks but the patient may experience intermittent mild pain and some restriction of motion
Prognosis
3. Fair - The patient can expect to have a reduction of their symptom although some persistent pain and stiffness from the injury is expected and may require ongoing rehabilitation.
4. Poor - The nature of the patient’s injury and preexisting conditions bring into doubt the likelihood of full recovery. It is expected that patient will continue to experience intermittent to occasional paresthesias along with occasional to frequent pain and stiffness, necessitating palliative care.
Prognosis
10/7/2017
20
5. Guarded - The patient’s condition is not expected to improve in the near future. They may expect to have continued muscle weakness and sensory deficit. Palliative and/or supportive care will be warranted for symptomatic relief and some improvement of function.
6. Unstable - Patient has not responded to the treatment trial and demonstrates evidence of deterioration. The likelihood of recovery with conservative care does not appear promising at this time. Surgical consult would be advisable.
Prognosis
Maximum Therapeutic BenefitMTB is determined following a sufficient course of care, where demonstrable improvement would be expected in a patient’s health status and one or more of the following are present:
• the patient has returned to pre-clinical/pre-onset health status
• meaningful improvement has occurred; however, there is no basis for further meaningful improvement
• meaningful improvement has occurred and there is no basis for further supervised in-office treatment
• the patient no longer demonstrates meaningful clinical improvement, as measured by standardized outcome assessment tools
• meaningful improvement, as measured by standardized outcome assessment tools, has not been achieved
• there is insufficient information documented in the submitted patient healthcare record to reliably validate the response to treatment 40

10/7/2017
21
Supportive CareMercy Conference Guidelines: Treatment for patients who have reached maximum therapeutic benefit, but who fail to sustain previous therapeutic gains through periodic withdrawals from care.
Private payer: Treatment for patients who demonstrated clinically meaningful improvement, and have reached MTB, and there remain significant residual deficits in the performance of daily activities e.g., usually >20% on a Neck/Back Index, and alternative treatments have been applied or given consideration, and self-care measures alone are likely not to sustain previously achieved therapeutic gains i.e., progressively deteriorate when treatment is withdrawn, and care is rendered PRN i.e., not prescheduled. 41
Complicating FactorsMercy Conference Guidelines:
• Symptoms present for more than 8 days can increase recovery time by a factor of 1.5
• Presence of severe pain can increase recovery time by a factor of 2
• 4 to 7 previous episodes can increase recovery time by a factor of 2
• Presence of skeletal anomaly or structural pathology can increase recovery time by a factor of 2
42

10/7/2017
22
The ChiroCode DeskBook is available at ChiroCode.com
This presentation is covered Chapter 4.4
• Learn to create initial care plans that establish the need for careo Understand how to use OATs
o Create effective and relevant patient-centered goals in your own care plans
• Learn how payers use treatment plan goals to determine if care is payable
• Define prognosis, supportive care, MTB, and complicating factors
Take away