Threat Level Urgent: Multidrug resistant Pseudomonas ...
32
9/30/2021 1 Brad Taranto, PharmD PGY1 Pharmacy Resident The Christ Hospital 1 2
Transcript of Threat Level Urgent: Multidrug resistant Pseudomonas ...

9/30/2021
1
Brad Taranto, PharmD
PGY1 Pharmacy Resident
The Christ Hospital
1
2

9/30/2021
2
0
2
4
6
8
10
12
14
16
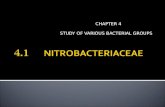
MDR Acinetobacter and Pseudomonas isolates*
(September 2019 - September 2021)
* Data from The Christ Hospital Cincinnati, Ohio, 2021
COVID-19
3
4

9/30/2021
3
5
6

9/30/2021
4
United States Centers for Disease Control (CDC) (2013)
Magiorakos, et al Clin Microbiol Inf (2012)
Multidrug-Resistant (MDR)
Resistant to ≥1 agent in 3
different antimicrobial categories
Extensively drug resistant (XDR)
Resistance to agents in
all but 2 antimicrobial categories
Pandrug-Resistant (PDR)
Resistant to all antimicrobial agents
7
8

9/30/2021
5
Enzymatic inactivation
Decreased permeability
Increased efflux Alteration of
drug target site
Overproduction of drug target
site
Britannica. Antibiotic resistance. 2009
Breijyeh, et al. Molecules (2020)
9
10

9/30/2021
6
Class A
• Penicillinases
• Carbapenemases
Class B
• Metallo-β-lactamases
Class C
• ampCβ-lactamases
Class D
• Oxacillinases
Ambler Classification of β-lactamases
Toussaint, et al. Ann Pharmacother (2015)
NSBLs
ESBLs
KPC
Hall, et al. J Antimicrob Chemo (2005)
11
12

9/30/2021
7
Mojica, et al. Curr Drug Targets (2016)
erratiaS
seudomonas/ ProteusP
cinetobacterA
itrobacterC
nterobacterEMoy, et al. Clin Ther (2017)
13
14

9/30/2021
8
Nordmann, et al. Emerg Inf Dis (2011)
Mo, et al. Diagn Microbiol Infect Dis (2019)
15
16

9/30/2021
9
17
18

9/30/2021
10
Enzymatic inactivation
Decreased permeability
Increased efflux Alteration of
drug target site
Overproduction of drug target
site
Mo, et al. Diagn Microbiol Infect Dis (2019)
19
20

9/30/2021
11
Enzymatic inactivation
Decreased permeability
Increased efflux Alteration of
drug target site
Overproduction of drug target
site
Mo, et al. Diagn Microbiol Infect Dis (2019)
Resistant39%
Intermediate2%
Susceptible59%
Acinetobacter spp. (Sep. ‘19 – Sep. ‘21)
Meropenem susceptibility
Viehman, et al. Drugs (2014)
21
22

9/30/2021
12
0 0 0
1
3
0
4
3
6
2
3
2
1
2
0
1 1
2 2
3
1
0
1
2
3
4
5
6
7
# o
f c
as
es
Month
CARBAPENEM-RESISTANT ACINETOBACTER SPP.
23
24

9/30/2021
13
Antimicrobial
classProposed agents Notes
Carbapenems Meropenem, imipenem • Increasing resistance
Polymyxins Polymyxin B, Polymyxin E (Colistin)
• Most reliable susceptibility
• Limited by toxicities (nephro- and
neuro-)
Tetracyclines Tigecycline, eravacycline, omadacycline • Limited use in bacteremia, UTI
Aminoglycosides Amikacin, tobramycin, gentamicin • Increasing resistance
β-lactam/β-lactamase
inhibitorsAmpicillin/sulbactam
• Sulbactam has intrinsic activity vs.
Acinetobacter spp.
Cephalosporins Cefiderocol • Novel mechanism
Susceptibility (%)
53
25
26

9/30/2021
14
Susceptibility (%)
74
Susceptibility (%)
~90
27
28

9/30/2021
15
Reference Patients Intervention Outcomes Conclusion
Makris (2018)RCT including
39 patients with
VAP
IV ColistinClinical response: 16%
Mortality: 63%↑Microbiological
response with
combination
therapy, but no
mortality benefit
IV Colistin +
ampicillin/sulbactam
Clinical response: 70%
Mortality: 50%
Yilmaz (2015)
Retrospective
observational
study including
70 patients with
VAP
IV ColistinClinical response: 76%
28-day mortality: 41%
No difference in
terms of
microbiological
response or
mortality
IV Colistin + extended
infusion meropenem
Clinical response: 64%
28-day mortality: 48.5%
Balkan (2015)
Retrospective
cohort study
including 107
patients with
bacteremia
IV ColistinEradication: 69%
14-day mortality: 53%No difference in
terms of
microbiological
eradication or
mortality
Non-colistin-based
combination therapy
Eradication: 83%
14-day mortality: 47%
Drug name (Brand) Formulary status
Minocycline (Minocin) Formulary
Tigecycline (Tygacil) Criteria for use*
Eravacycline (Xerava) Non-formulary
Omadacycline (Nuzyra) Non-formulary
*MDR gram-negative organism with known tigecycline susceptibility
(amongst other criteria)
Susceptibility (%)
~60
29
30

9/30/2021
16
Reference Patients Intervention Outcomes Conclusions
Shin (2012)
Retrospective
cohort study
including 27
patients with
various infections
(mainly VAP)
Tigecycline
monotherapyClinical success: 58.5%
14-day mortality: 5.9%No difference in
clinical success
(p=0.56) or 14-day
mortality (p=0.26)Tigecycline-based
combination therapyClinical success: 70%
14-day mortality: 0%
Kim (2016)
Retrospective
cohort study
including 70
patients with
PNA
Tigecycline-based
therapy
Clinical success: 47%
30-day mortality: 33% No difference in
clinical success
(p=0.95) or 30-day
mortality (p=0.77)Colistin-based therapyClinical success: 48%
30-day mortality: 33%
Ampicillin-sulbactam doses up to 12 g (2:1) described
High doses of ampicillin can cause seizures, electrolyte
derangements
Susceptibility (%)
~30
31
32

9/30/2021
17
Reference Patients Intervention Outcomes Conclusions
Ye (2016)
Retrospective
cohort study
including 168
patients with
PNA
Sulbactam-based
therapy
Eradication: 63.5%
30-day mortality: 33.3%↑Microbiologic
eradication with
sulbactam-based
therapy (p<0.001)
No difference in 30-day
mortality (p=0.618)
Tigecycline-based
therapy
Eradication: 33.3%
30-day mortality: 29.8%
Yilmaz
(2015)
Retrospective
cohort study
including 70
patients with
VAP
IV Colistin +
carbapenem
Clinical response: 64%
28-day mortality: 48.5% No difference in clinical
response rate (p=0.53)
or 30-day mortality
(p=0.21)IV Colistin +
sulbactam
Clinical response: 55%
28-day mortality: 70%
Susceptibility (%)
>90
33
34

9/30/2021
18
• Prospective, randomized, open-label phase III study
• 118 patients with carbapenem-resistant nosocomial PNA, BSI, cUTIDesign
• Cefiderocol vs. ‘Best available therapy’ (BAT)
• Most commonly colistin + tigecycline/amp-sulbactam/fosfomycinIntervention
• Clinical cure: Cefiderocol 66% vs. BAT 58% (not significant)
• Cefiderocol > BAT in BSI and cUTI, but not in PNA
Primary Outcomes
• 28-day mortality (A. baumannii only): Cefiderocol 50% vs. BAT 18%
• Cefiderocol associated with higher mortality overall in PNA/BSI, but had mortality benefit in cUTI
Safety Outcomes
Bassetti, et al. Lancet Inf Dis (2021)
Reference Patients Intervention Outcomes
Rattanaumpawan (2010)N=50 patients with
VAP
Nebulized colistin 2 MU q12h +IV
antibiotics↑ favorable
microbiological
outcome
No difference in
overall mortality
Nebulized NS +IV antibiotics
Betrosian (2008)N=28 patients with
VAP
IV colistin 3 MU q8h No difference in
microbiological
response or
overall mortalityIV amp/sulbactam 9 g q8h
35
36

9/30/2021
19
• Bayesian meta-analysis of 15 unique treatment regimensfrom 23 studies vs. MDR A. baumanii infections incritically ill patients
Design
• IV colistin monotherapy vs. alternative therapies
• Pairwise comparisons within studies
• Common-comparator comparisons across studiesIntervention
• 4 therapies improved survival compared to IV colistin
• (1) Sulbactam (2) IV colistin + IV fosfomycin(3) IV colistin + inhaled colistin (4) high-dose tigecycline
Outcomes
Jung, et al. Crit Care (2020)
Agents with potential activity include carbapenems, polymyxins, aminoglycosides, tigecycline, ampicillin-sulbactam, and cefiderocol
No single agent has emerged as the clear drug-of-choice
Regimen should be selected based on available susceptibility data
Combination therapy may be considered → Risk vs. benefit
37
38

9/30/2021
20
39
40

9/30/2021
21
41
42

9/30/2021
22
Aminoglycosides
Fluoroquinolones (except moxifloxacin)
4th generation cephalosporins (i.e. cefepime/ceftazidime)
Antipseudomonal penicillins (i.e. piperacillin, ticarcillin)
Carbapenems (except ertapenem)
Polymyxins
Monobactams
Enzymatic inactivation
Decreased permeability
Increased efflux Alteration of
drug target site
Overproduction of drug target
site
Eichenberger, et al. Antibiotics (2019)
43
44

9/30/2021
23
Enzymatic inactivation
Decreased permeability
Increased efflux Alteration of
drug target site
Overproduction of drug target
site
Eichenberger, et al. Antibiotics (2019)
45
46

9/30/2021
24
Tamma, et al. IDSA (2020)
47
48

9/30/2021
25
What is DTR and where does it fit?
Multidrug-Resistant (MDR)
Resistant to ≥1 agent in 3
different antimicrobial categories
Extensively drug resistant (XDR)
Resistance to agents in
all but 2 antimicrobial categories
Pandrug-Resistant (PDR)
Resistant to all antimicrobial agents
Resistance to all…
•β-lactams (including carbapenems)
•Fluoroquinolones
•Monobactams
Kadri, et al. Clin Infect Dis (2019)
49
50

9/30/2021
26
2014
2015
2017
2019
Ceftolozane-tazobactam(Zerbaxa®)
Ceftazidime-avibactam(Avycaz®)
Meropenem-vaborbactam(Vabomere®)
Imipenem-cilastatin-relebactam(Recarbrio®)
KPC OXA-48 NDM VIM IMP P. aeruginosa A. baumannii
Ceftolozane-
tazobactamZerbaxa® ⁺ Yes
Ceftazidime-
avibactamAvycaz® ⁺ ⁺ ⁺ Yes*
Meropenem-
vaborbactamVabomere® ⁺ No
Imipenem-
cilastatin-
relebactam
Recarbrio® ⁺ ⁺ No
Formulary?
Activity against B-lactam-
resistant isolates of:
*Ordering restricted to ID only
Drug Brand NameActivity against carbapenemases
51
52

9/30/2021
27
Infection source Preferred treatment Alternative treatment
Cystitis
Ceftolozane-tazobactam
Ceftazidime-avibactam
Imipenem-cilastatin-relebactam
Cefiderocol
Single-dose of an aminoglycoside
Colistin
Pyelonephritis or cUTI
Ceftolozane-tazobactam
Ceftazidime-avibactam
Imipenem-cilastatin-relebactam
Cefiderocol
Once-daily aminoglycosides
All other infections
Ceftolozane-tazobactam
Ceftazidime-avibactam
Imipenem-cilastatin-relebactam
Cefiderocol
Aminoglycosides (if bloodstream
infection and adequate source control)
IDSA MDR Guidance (2020)
Ceftolozane-tazobactam(Zerbaxa®)
Ceftazidime-avibactam(Avycaz®)
53
54

9/30/2021
28
Reference Patients Intervention Outcomes Conclusions
Humphries
(2017)
309 P. aeruginosa
isolates resistant to
≥1 of the following:
cefepime, Pip/tazo,
meropenem
In vitro susceptibility
testing of isolates to
ceftolozane-
tazobactam (COT)
and ceftazidime-
avibactam (CZA)
COT
%Susceptible: 73%
CZA
%Susceptible: 62%
Ceftolozane-tazobactam
(COT, Zerbaxa®)
appears to have superior
activity against MDR P.
aeruginosa compared to
ceftazidime-avibactam
(CZA, Avycaz®)COT
%Susceptible: 52%
CZA
%Susceptible: 27%
105 P. aeruginosa
isolates resistant to
all 3 above ABX
Humphries, et al. Antimicrob Agents Chemother (2017)
55
56

9/30/2021
29
• Prospective, randomized, open-label phase III study
• 118 patients with carbapenem-resistant nosocomial PNA, BSI, cUTIDesign
• Cefiderocol vs. ‘Best available therapy’ (BAT)
• Most commonly colistin + tigecycline/amp-sulbactam/fosfomycinIntervention
• Clinical cure: Cefiderocol 66% vs. BAT 58% (not significant)
• Cefiderocol > BAT in BSI and cUTI, but not in PNA
Primary Outcomes
• 28-day mortality (A. baumannii only): Cefiderocol 50% vs. BAT 18%
• Cefiderocol associated with higher mortality overall in PNA/BSI, but had mortality benefit in cUTI
Safety Outcomes
Uncomplicated cystitis
• Ceftolozane-tazobactam, ceftazidime-avibactam, cefiderocol, or single-dose aminoglycoside
Complicated UTI or pyelonephritis
• Ceftolozane-tazobactam, ceftazidime-avibactam, cefiderocol
All other infections
• Ceftolozane-tazobactam, ceftazidime-avibactam
57
58

9/30/2021
30
Combination therapy is not routinely necessary
Anti-pseudomonal β-lactams and FQs have reliable activity
BL/BLIs and cefiderocol should be reserved for DTR isolates
Drug Indication DosingDose
adjustments
MeropenemUTI, BSI, HAP/VAP caused by
MDR GNRIV: 1 g q8h (extended infusion over 3 hr) Renal
Colistin (polymyxin E)BSI, HAP/VAP caused by MDR
GNR
Inhalation: 4.5 MU q8hRenal
IV: 9 MU x1, then 4.5 MU q12h
TigecyclineIAI, HAP/VAP, SSTI caused by
MDR GNR
Standard dose IV: 100 mg x1, then 50 mg
q12h
HepaticHigh dose (complicated infections caused
by MDR A. baumannii, P. aeruginosa) IV:
200 mg x1, then 100 mg q12h
Ampicillin-sulbactamBSI, HAP/VAP caused by MDR
GNRIV: 3 g q8h (extended infusion over 4 hr) Renal
CefiderocolUTI, HAP/VAP caused by MDR
GNRIV: 2 g q8h Renal
Ceftolozane-tazobactam
HAP/VAP caused by MDR GNR IV: 3 g q8h
RenalIAI, UTI, SSTI, BSI caused by
MDR GNRIV: 1.5 g q8h
Ceftazidime-avibactamIAI, UTI, HAP/VAP caused by
MDR GNRIV: 2.5 g q8h Renal
Abbreviations: Urinary tract infection (UTI), bloodstream infection (BSI), hospital-acquired pneumonia (HAP), ventilator-associated pneumonia (VAP), skin
and soft tissue infection (SSTI), multidrug resistant (MDR), gram-negative rods (GNR)
59
60

9/30/2021
31
61
62

9/30/2021
32
63