The Importance of Sternal Approximation and Mechanical ...
4
eliminating the need for additional remodeling. 2, 12 Because it is rare to have an environment where the gap is completely reduced, another type of primary repair is gap repair. In this environment, a slight gap may be visible, but not enough for cartilage or woven bone formation; therefore repair is initiated by marrow cells of the bone and lamellar bone is laid down. However, the new bone is laid down perpendicular to the old bone, and therefore must be remodeled to match the old bone. 2, 12 Introduction Approximation and rigid fixation are key factors in supporting good bony union. 7 These principles apply to the fixation of the sternum following a sternotomy. In 1957, Julian immediately recognized “The solidity of the closure is important because it completely immobilizes the chest from abnormal movements and renders the postoperative period more comfortable. The security of wire sutures is essential. 6 ” Wire is effective at approximating sternal halves, but does not provide rigid fixation. The use of plates is one method that provides the rigid fixation needed to support healing following approximation. 7, 11 Bone Healing Requires Approximation and Rigid Fixation When bones fracture, depending on the amount of environmental stability surrounding the fracture, different mechanisms of bone repair are utilized 2, 12 . • Primary bone formation (Intramembranous ossification): Little to no separation due to a very stable environment; bone heals by direct contact without callous formation • Secondary bone formation (Endochondral ossification): Greater separation and mobility between the bony fragments due to unstable environment; bone heals by deposition of intermediate cartilage layer. While the two mechanisms of bone healing may be different, both require approximation and stability for bone remodeling to occur. 12 In both primary and secondary healing, approximation and stability allows for the formation of blood vessels which bring nutrients and initiates the repair process to the injured site. During primary healing, because the gap is reduced by the use of internal rigid fixation, good vascularization is possible, therefore allowing repair via direct contact without the formation of cartilage. Bone repair is then initiated by the Haversian system of the lamellar bone. When bone fractures, blood vessels in the bone are also broken, depriving the area of any nutrients; therefore causing bone tissue to become necrotic. Before new bone can be laid down, the necrotic tissue must be removed. 1,2 Bone cells (osteoclasts) with cutting cones at the front resorb the necrotic bone and new lamellar bone is then synthesized and laid down parallel to the old, therefore The Importance of Sternal Approximation and Mechanical Stability in Bone Healing 1 Figure 2b. Axial CT scan illustrating callous formation observed during secondary sternal healing. Figure 2a. Histological image of secondary bone formation also known as endochondral ossification. Figure 1b. Axial CT scan illustrating direct, primary healing of the sternal halves using rigid plate fixation. Figure 1a. Histological image of primary bone formation also known as intramembra- nous ossification. INTRAMEMBRANOUS OSSIFICATION During secondary healing, the inflammation surrounding the fracture stimulates the periosteum (membranous tissue surrounding bone) to develop cells which replicate and eventually transform into cartilage and woven bone. The periosteal cells closest to the fracture gap develop into cartilage ENDOCHONDRAL OSSIFICATION Callous formation WP-BoneHealing-sp.indd 2 9/9/11 1:24 PM
Transcript of The Importance of Sternal Approximation and Mechanical ...

eliminating the need for additional remodeling.2, 12 Because it is rare to have an environment where the gap is completely reduced, another type of primary repair is gap repair. In this environment, a slight gap may be visible, but not enough for cartilage or woven bone formation; therefore repair is initiatedby marrow cells of the bone and lamellar bone is laid down. However, the new bone is laid down perpendicular to the old bone, and therefore must be remodeled to match the old bone.2, 12
IntroductionApproximation and rigid fixation are key factors in supporting good bony union.7 These principles apply to the fixation of the sternum following a sternotomy. In 1957, Julian immediately recognized “The solidity of the closure is important because it completely immobilizes the chest from abnormal movements and renders the postoperative period more comfortable. The security of wire sutures is essential.6” Wire is effective at approximating sternal halves, but does not provide rigid fixation. The use of plates is one method that provides the rigid fixation needed to support healing following approximation.7, 11
Bone Healing Requires Approximation and Rigid Fixation
When bones fracture, depending on the amount of environmentalstability surrounding the fracture, different mechanisms of bone repair are utilized2, 12.
• Primary bone formation (Intramembranous ossification): Little to no separation due to a very stable environment; bone heals by direct contact without callous formation
• Secondary bone formation (Endochondral ossification): Greater separation and mobility between the bony fragments due to unstable environment; bone heals by deposition of intermediate cartilage layer.
While the two mechanisms of bone healing may be different, both require approximation and stability for bone remodelingto occur.12 In both primary and secondary healing,approximation and stability allows for the formation of blood vessels which bring nutrients and initiates the repair process to the injured site.
During primary healing, because the gap is reduced by the use of internal rigid fixation, good vascularization is possible,therefore allowing repair via direct contact without theformation of cartilage. Bone repair is then initiated by theHaversian system of the lamellar bone. When bone fractures, blood vessels in the bone are also broken, depriving the area of any nutrients; therefore causing bone tissue to become necrotic. Before new bone can be laid down, the necrotic tissue must be removed.1,2 Bone cells (osteoclasts) with cutting cones at thefront resorb the necrotic bone and new lamellar bone is thensynthesized and laid down parallel to the old, therefore
The Importance of Sternal Approximation andMechanical Stability in Bone Healing
1
Figure 2b. Axial CT scan illustrating callous formation observed during secondary sternal healing.
Figure 2a. Histological image of secondary bone formation also known as endochondral ossification.
Figure 1b. Axial CT scan illustrating direct, primary healing of the sternal halves using rigid plate fixation.
Figure 1a. Histological image of primary bone formation also known as intramembra-nous ossification.
INTRAMEMBRANOUS OSSIFICATION
During secondary healing, the inflammation surroundingthe fracture stimulates the periosteum (membranous tissuesurrounding bone) to develop cells which replicate and eventually transform into cartilage and woven bone. The periosteal cells closest to the fracture gap develop into cartilage
ENDOCHONDRAL OSSIFICATION
Callous formation
WP-BoneHealing-sp.indd 2 9/9/11 1:24 PM

2
while those distal to the gap form into woven bone. The new tissue grows until they bridge together and form what is known as a fracture callous.2, 12 Once the area is stabilized with the callous, blood vessels are then able to infiltrate and assist with the mineralization into hardened lamellar bone. If movementand separation continues in secondary healing, the softcallous may either fail to mineralize (therefore fail to harden) or lengthen the time in which complete bone healing occurs.2, 12
Animal studies have demonstrated the amount of interfrag-mentary movement between the fractured ends and size of osseous gaps, specifically those larger than 2mm may affect the quality of bone healing.13 Distraction studies using canines have shown that the ideal distraction length is 1 mm per day and 2 mm a day has proven to be detrimental in bonelengthening.14 Thus, a gap that is of sufficient size may prevent bridging by callous formation, and potential non-union ormalunion may be observed.13 Mobility of the fracture site could also have adverse results such as dehiscence, osteomyelitis and mediastinitis.7
In a primate study comparing rigid fixation to wires in sternal healing, Sargent showed that at four weeks, stability and union was seen across the fractured site after removing the plates and manipulating the sternum. In comparison, wires showed unstable sternums and mobility upon manipulation at the fractured site. “Rigid fixation of the sternum resulted in earlier union with primary osseous healing, suggesting greater inherent stability.5” By eight weeks, both groups were healed andno difference was seen between the two treatment methods. This study illustrated primary healing with plates and secondary healing with wires. Sternal Wires Support Approximation but Do Not Prevent Sternal Separation
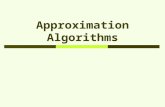
Studies have shown that using re-enforced or various wiringtechniques do not limit sternal separation.3, 9, 10 In a humancadaveric study comparing median sternotomy closures with common wire techniques, Losanoff demonstrated that using the Robicsek weave or pericostal figure of eight did not increase the mechanical stability of sternal fixation, or reduce the amount of sternal separation, relative to simple peri-sternal wires. Instead, mechanical stability was shown to be considerably weaker in the Robicsek weave and sternal separation was highest in pericostal figure of eight.9 A second study in cadavers also revealed that the amount of sternal separation and displacement seen in doublewires was comparable to single wires.3 The forces used in both studies (0-800N) were based on forces considered average to maximum (400-1200N) for coughing.3 These forces resulted in 4.8mm to 16.0mm of sternal separation after just 1 cycle of loading. Minimum permanent separation of the sternal halves after only 10 cycles was 1.3mm.3, 9 This study recognizes that the number of wires and configurations affects the closure’s integrity, stating, “Improved stability during the early healing stages is associated with more rigid sternal fixation, confirming that a stable sternotomy is essential to complete and durable healing.9”
Figure 3. PSS (Peri-sternal single wires), PSD (Peri-sternal double), TSS (Trans-sternal single), F8P (Figure of eight pericostal); note all wires failed for F8P for Maximum Displacement, thereforeno value noted.3,9 No matter the configuration of wires used, movement and separation were still permissible.
18
15
12
9
6
3
0
Dis
tanc
e (m
m)
PSS PSD TSS Robicsek F8P
Displacement after 1 cycle
Maximum Displacement
Oss
eous
gap
s >2
mm
hav
e be
en s
how
nto
hav
e a
nega
tive
impa
ct o
n bo
ne h
ealin
g
2mm Gap
Figure 4b. 8.0mm separation after maximum displacement.
Figure 4a. 4.9mm separation after 1 cycle ofdisplacement.
Peri-sternal Single Wires
Figure 5b. 11.8mm separation after maximumdisplacement.
Figure 5a. 7.5mm separation after 1 cycle of displacement.
Robicsek Weave
WP-BoneHealing-sp.indd 3 9/9/11 1:24 PM

3
Significant differences (p<0.05) were seen between plates and wires in resisting forces. Sternal separation with wires was 8-10 times more than with plates.7 When tests were completed to show how much force could be withstood before failure, in bothcadaveric and polyurethane models, the plated modelsdemonstrated the ability to withstand twice the force (400N) in contrast to the wired models (200N). In addition, the failures seen by the plates were due to rib fractures and tearing of intercostal muscles near the clamps gripping the cadaveric sternum. Where as for the wired sternums, failure occurred due to wire pulling through at the midline.6, 7
Mechanical Properties Impact Sternal Union
Overall, studies with wires have shown poor bone healing4 (with similar outcomes and complication rates for simple and modified wiring technique).10,11 In a CT scan study on sternal healing using wires completed by Bitkover, wire cerclage showed 0% healing at
Figure 7b. Although tight approximation was possible at thetime of operation, 6 months later, a coronal view of a 3D CTscan reconstruction of the same subject shows separation ofthe sternal halves.
Figure 7a. Operative photo of peri-sternal closure with standard wires.
Figure 6a. Operative photo of closure with sternal plates and screws.
Figure 6b. Continuous tight approximation and mechanical stability is observed in a coronal view of a 3D CT scan recon-struction of the same subject at 6 months with sternal plates.
Figure 6c. A close-up of an axial CT scan at 6 months of the same subject illustrating direct sternal union with plates and screws.
Figure 7c. A close-up of an axial CT scan at 6 months of thesame subject illustrating the separation of sternal halves causedby the loosening of wires.
Sternal Plating Results in Rigid Fixation and Reduced Sternal Separation
Mechanical studies with sternal plating have shown reduced sternalseparation and increased mechanical strength with sternal plates compared with wire cerclage. In a cadaveric biomechanical study by Wong, sternal closure with rigid plate fixation and wires were tested by simulating natural forces applied on the sternum in vivo. The study demonstrated 400% and 1600% increase in stiffness (lateral distraction and longitudinal shear; p<0.05) and a 40% and 45% increase in strength (lateral distraction and longitudinal shear; p<0.05, p>0.05) in plated sterna in contrast to wired sterna.6 Sternal plate fixation showed significantimprovements in resisting forces not only of lateral distraction, but also longitudinal shear when compared to wire cerclage. In another study that utilized polyurethane foam models to remove the variability of cadaveric sterna specimens, wires and plates were tested using forces similar to coughing (120N and 180N).7
WP-BoneHealing-sp.indd 4 9/9/11 1:24 PM

Biomet Microfixation does not practice medicine. The surgeon who performs any implant procedure must determine the appropriate device and surgical procedure of each individual patient. Information contained in this paper is intended for surgeon or distributor information only and is not intended for patient distribution. All surgeries carry risks. For additional information on these risks and warnings, please see appropriate package insert for each device or visit our web site at www.biometmicrofixation.com or call 1-800-874-7711.
4
References
1520 Tradeport Drive • Jacksonville, FL 32218-2480Tel (904) 741-4400 • Toll-Free (800) 874-7711 • www.biometmicrofixation.com
Form No. BMF00-3255 • Rev 03k1109
1. Doll B., Aleef M. & Hollinger J.O. (2008). Overview of Fracture Repair. In Y.H. An & A.U. Daniels (Eds.) Musculoskeletal Tissue Regeneration (pp. 39- 46). Charleston, SC: Humana Press.
2. Shapiro F. Bone Development and its relation to fracture repair. The role of mesenchymal osteoblasts and surface osteoblasts. European Cells and Materials 2008; 15: 53-76.
3. Losanoff JE, Basson MD, Gruber SA, Huff H and Hsieh F. Single Wire versusDouble Wire Loops for Median Sternotomy Closure: Experimental biomechan-ical study using a human cadveric model. Ann Thorac Surg 2007;84:1288-93.
4. Bitkover CY, Cederlund K, Aberge B, and Vaage J. Computed tomographyof the sternum and mediastinum after median sternotomy. Ann Thorac Surg 1999;68:858-63.
5. Sargent LA, Seyfer AE, Hollinger J, Hinson RM and Graeber GM. The healing sternum: a comparison of osseous healing with wire versus rigid fixation. Ann Thorac Surg 1991;52:490-4.
6. Wong MS.2010. Biomechanical comparison of wire cerclage and rigid plate fixation for median sternotomy closure in human cadaver specimens. Masters Thesis, California Polytechnic State University, San Luis Obispo. 140p.
7. Pai S, Gunja NJ, Dupak EL, McMahon NL, Roth TP, Lalikos JF, Dunn RM, Francalancia N, Pings GD, Billiar KL. In vitro comparison of wire andplate fixation for midline sternotomies. Ann Thorac Surg 2005; 80:962-8.
8. Neaman KC, Blount AL, Kim JA, Renucci JD and Hooker RL. Prophy-lactic sternal plating with pectoralis advancement flaps after sternotomy in patients with a history of chest irradiation. Inter Cardio and Thorac Surg 2011; 12:355-59.
9. Losanoff JE, Collier AD, Wagner-Mann CC, et al. BiomechanicalComparison of Median Sternotomy Closures. Ann Thorac Surg 2004;77:203-9.
10. Schimmer C, Reents W, Berneder S, Eigel P, et al. Prevention of ster-nal dehiscence and infection in high risk patients: a prospective, random-ized multicenter trial. Ann Thorac Surg 2008;86:1897-904.
11. Voss B, Bauernschmitt R, Will A, et al. Sternal reconstruction with titanium plates in complicated sternal dehiscence. Eur J Cardiothoracic Surg 2008;34:139-45.
12. Magee DJ, Zachazowski JE, Quillen WS- Scientific Foundation and Principles of Practice in Muskuloskeletal Rehabilitation.
13. Claes L, Augat P, Suger G, Wilke HJ. Influence of size and stability of the osteotomy gap on the success of fracture healing. J Orthopaed Research 1997;15:577-84.
14. Ilizarova, G. The Tension-Stress Effect on the Genesis and growth of tissues: Part II The Influence of the Rate and Frequency of Distraction. Clinical Orthopaedics and Related Research 1989; 239:263-85.
This white paper is coauthored by Brian Hatcher, Ph.D. who is the Director of Research and Minya Holdeman, Research Assistant for Biomet Microfixation.Parts of this research were funded by Biomet Microfixation.
3 months and only 50% healing at 6 months. Callous was notvisible on the radiographs three months after median sternotomywas performed even for patients without suspected infection.4
A randomized prospective study completed by Schimmer comparing simple wire cerclage to Robicsek weave after a midline sternotomy did not result in lower wound complicationrates. Rather no significant difference in sternal dehiscencerates was seen between the Robicsek weave and simple wires. “The key factor in preventing sternal dehiscence and sternalwound infection is a stable sternal approximation.10” Rigidfixation with sternal plates may provide additional mechanical stability needed to support bone healing. After failing tostabilize the sternum using standard wire to close the sternum on a small population, Voss conducted a study using plates torigidly fixate the sternum and was able to demonstrate effective stabilization of the sternum.11 Another study utilizing rigidfixation was conducted by Neaman. He showed that patients that had undergone a history of chest radiation (a known cause for inhibiting tissue wound healing) had none of the problems
often associated with poor sternal healing including non-union,sternal infection or mediastinitis after undergoing a median sternotomy for cardiothoracic procedure using plates.8
CT scans and operative images support the principle that good bony healing necessitates approximation and rigidfixation (Fig. 6-7). Wires were used to approximate thesternum in plated and wired patients. Operative photographs illustrate how well the sternal halves were approximatedduring the surgery in both groups and CT scans document bone healing. Combined with the operative photographs, this data supports that approximation alone does not lead to bone healing, but approximation plus rigid fixation support bone healing.
Conclusion
Sternal reduction along with rigid fixation may supportimproved clinical outcomes by providing the opportunity forimproved bone healing and union.
WP-BoneHealing-sp.indd 1 9/9/11 1:23 PM