
The Chronicle of Skin & Allergy - June 2010
40
Psoriasis Evaluating best therapies for pregnant women, pediatric patients Some treatments for adults with psoriasis can also be options for children and adolescents by LYNN BRADSHAW Senior Associate Editor, The Chronicle A lthough research is lacking concerning the best treat- ment options for pediatric patients with psoriasis and women with psoriasis who would like to start a family, it’s clear that the dis- ease often negatively affects the quality of patients’ lives and clini- cians have a duty to provide them with the best possible treatment, according to Dr. Bruce Strober. Pediatric psoriasis patients “I disagree that the average onset age of psoriasis is 28 years of age, because I have found that a num- ber of people have reported their psoriasis started as a child,” said Dr. Strober, assistant professor, Department of Dermatology at NYU, Langone Medical Center in New York during a presentation at mini Dermatology Update in Toronto. “Really, I think there is a lot going on that we are not diagnosing as psoriasis under the age of 18. Maybe pediatricians called it eczema. Maybe it is mild and ignored by parents.” Dr. Strober highlighted that pso- riasis is a concern among pediatric patients and must not be ignored. During his presentation, he posed a question to the audience: Should treatment options for children be prioritized differently than those for adults? Dr. Strober admitted that there is really no right answer to the question, and that all clinicians have their treatment style and pref- Please turn to Psoriasis page 13 study of generalized vitiligo in Caucasians of European descent mainly turned up previously- described associations with immune-related genes, Dr. Richard A. Spritz of the University of Colorado in Aurora, and colleagues reported. However, the association with the TYR genetic locus (p=1.60x10 -18 ) came as a surprise, “though probably it should not have been in retro- spect,” Dr. Spritz said in an interview. P RACTICAL T HERAPEUTICS and C LINICAL N EWS from the WORLD of D ERMATOLOGY ■ J UNE 2010 by CRYSTAL PFEND Special to The Chronicle A n unexpected genetic link between the hair and skin pigmentation disorder vitiligo and malignant melanoma may have implications for treat- ment of both, researchers report- ed online in the New England Journal of Medicine. The genome-wide association Genetics Vitiligo shares roots with skin cancer, say researchers Genetic inquiry finds vitiligo associated with major alleles of melanoma of & ALLERGY SKIN SKIN The Chronicle Eczema Alitretinoin a new option for chronic hand eczema patients Condition often seen in daily practice by IAN J.S. MOORE, Correspondent, The Chronicle A new oral formulation of tretinoin—as a once-daily therapy for patients with severe, chronic hand eczema who are unresponsive to corticosteroids—is now available. Alitretinoin was approved for use in Canada earlier this year, and is expected to be available for prescription sometime this summer, after the manufacturer, Basilea Pharmaceutica, reaches an agree- ment on price with the Patented Medicine Prices Review Board (PMPRB). All rights reserved. Chronicle Information Resources Ltd. Canada Post Canadian Publications Mail Sales Product Agreement Number 40016917 TANNING ISSUES • 11 CDA working with legislators to implement age limits on tanning parlour patrons ACD • 12 Patch tests useful for Dx of eczematous disease, says the University of Ottawa’s Dr. Melanie Pratt The Chronicle INSIDE Please turn to Chronic hand eczema page 28 This gene encodes tyrosinase, the key enzyme in melanocytes that synthesizes melanin and that is the major tar- get of autoim- munity in gener- alized vitiligo. This pro- vides an impor- tant insight into the pathogenesis of vitiligo and may point to targets for treatment of the disease, which affects 0.5% to Please turn to Vitiligo page 9 Update on See page 4 Refined therapies attracting new patients Dr. Richard Spritz Cosmetic dermatology
-
Upload
pharmaweenie -
Category
Documents
-
view
1.185 -
download
3
Transcript of The Chronicle of Skin & Allergy - June 2010

P s o r i a s i s
Evaluating besttherapies forpregnant women,pediatric patients� Some treatments
for adults with
psoriasis can also be
options for children
and adolescents
by LYNN BRADSHAWSenior Associate Editor, The Chronicle
Although research is lacking
concerning the best treat-
ment options for pediatric
patients with psoriasis and women
with psoriasis who would like to
start a family, it’s clear that the dis-
ease often negatively affects the
quality of patients’ lives and clini-
cians have a duty to provide them
with the best possible treatment,
according to Dr. Bruce Strober.
Pediatric psoriasis patients
“I disagree that the average onset
age of psoriasis is 28 years of age,
because I have found that a num-
ber of people have reported their
psoriasis started as a child,” said
Dr. Strober, assistant professor,
Department of Dermatology at
NYU, Langone Medical Center in
New York during a presentation at
mini Dermatology Update in
Toronto.
“Really, I think there is a lot
going on that we are not diagnosing
as psoriasis under the age of 18.
Maybe pediatricians called it
eczema. Maybe it is mild and
ignored by parents.”
Dr. Strober highlighted that pso-
riasis is a concern among pediatric
patients and must not be ignored.
During his presentation, he posed a
question to the audience: Should
treatment options for children be
prioritized differently than those for
adults?
Dr. Strober admitted that there
is really no right answer to the
question, and that all clinicians
have their treatment style and pref-
Please turn to Psoriasis page 13�
study of generalized vitiligo in
Caucasians of European descent
mainly turned up previously-
described associations with
immune-related genes, Dr. Richard
A. Spritz of the University of Colorado
in Aurora, and colleagues reported.
However, the association with
the TYR genetic locus (p=1.60x10-18)
came as a surprise, “though probably
it should not have been in retro-
spect,” Dr. Spritz said in an interview.
PRACTICAL THERAPEUTICS and CLINICAL NEWS from the WORLD of DERMATOLOGY � JUNE 2010
by CRYSTAL PFENDSpecial to The Chronicle
An unexpected genetic link
between the hair and skin
pigmentation disorder
vitiligo and malignant melanoma
may have implications for treat-
ment of both, researchers report-
ed online in the New EnglandJournal of Medicine.
The genome-wide association
G e n e t i c s
Vitiligo shares roots withskin cancer, say researchers� Genetic inquiry finds vitiligo associated with major alleles of melanoma
o f & A L L E R G YSKINSKIN
The Chronicle
E c z e m a
Alitretinoin a new option forchronic hand eczema patients � Condition often seen in daily practice
by IAN J.S. MOORE, Correspondent, The Chronicle
Anew oral formulation of tretinoin—as a once-daily therapy
for patients with severe, chronic hand eczema who are
unresponsive to corticosteroids—is now available.
Alitretinoin was approved for use in Canada earlier this year, and is
expected to be available for prescription sometime this summer,
after the manufacturer, Basilea Pharmaceutica, reaches an agree-
ment on price with the Patented Medicine Prices Review Board
(PMPRB).
All
rig
hts
reserv
ed
. C
hro
nic
le I
nfo
rmati
on
Reso
urc
es L
td.
Can
ad
a P
ost
Can
ad
ian
Pu
bli
cati
on
s M
ail
Sale
s P
rod
uct
Ag
reem
en
t N
um
ber
40
01
69
17
TANNING ISSUES • 11CDA working withlegislators to implementage limits on tanningparlour patrons
ACD • 12Patch tests useful for Dx ofeczematous disease, saysthe University of Ottawa’sDr. Melanie Pratt
The ChronicleINSIDE
Please turn to Chronic hand eczema page 28�
This gene encodes tyrosinase,
the key enzyme in melanocytes that
s y n t h e s i z e s
melanin and that
is the major tar-
get of autoim-
munity in gener-
alized vitiligo.
This pro-
vides an impor-
tant insight into
the pathogenesis
of vitiligo and
may point to targets for treatment of
the disease, which affects 0.5% to
Please turn to Vitiligo page 9�
Update on
See page 4
RReeffiinneedd tthheerraappiieess aattttrraaccttiinngg nneeww ppaattiieennttss
Dr. Richard Spritz
CCoossmmeettiiccddeerrmmaattoollooggyy
21385A_SkinAllergy_J10:.ps 6/22/2010 9:00 AM Page 1
1.877.9ENBREL (1.877.936.2735) enbrel.ca
YOUR ENBREL SUPPORT PROGRAM
AdaptableCaters to your needs and the unique needs of each patient you treat
ComprehensiveCovers all the bases, from initial drug access and injection training to continued long-term support
Handling the details with careHandling the details with care
ReliableThe dedicated Enliven team is there for you and your patients, from the moment you prescribe ENBREL®
ENBREL is indicated for reducing signs and symptoms, inhibiting structural damage progression and improving physical function of moderately to severely active arthritis in adult patients with rheumatoid arthritis and psoriatic arthritis. ENBREL is indicated for reducing the signs and symptoms of moderately to severely active polyarticular juvenile idiopathic arthritis (JIA) in patients aged 4 to 17 years who have had an inadequate response to one or more DMARDs. ENBREL is indicated for reducing signs and symptoms of active ankylosing spondylitis. ENBREL is also indicated for the treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. Product Monograph available upon request.
ENBREL and Enliven are registered trademarks of Immunex Corporation.
21385A_SkinAllergy_J10:.ps 6/17/2010 5:56 PM Page 2

THE CHRONICLE of SKIN & ALLERGY
Vol. 16, No. 4June 2010 · 3
A Message from theMedical Editor
Canadian dermatologists contin-
ue to impress and inspire me
every time I am asked to review
cutting edge articles for THE
CHRONICLE. Within the
world's dermatology
community Canadian
dermatologists in
terms of numbers are
less than 1% (most
likely less than 0.1%)
but continue to be
over-represented in
our contribution on the world stage.
Whether it be enrolling disproportion-
ately high numbers of high quality
patients to the first head-to-head bio-
logic trial of ustekinumab versus etan-
ercept, or helping with trials working
toward novel therapeutics such as
alitretinoin for hand eczema,
Canadian dermatologists are up to
the challenge in continuing to be a
significant force within the world’s
clinical trials community. We also
make significant impact in the global
arena in many other areas including
contact dermatitis, wound care, and
cosmetic dermatology to name a few.
Our association, the CDA, is
another shining example to the world
of the leadership we display. One of
the best examples is the CDA’s Sun
Awareness Program. It is truly a
model for dermatology associations
worldwide and if we are successful in
passing the “Skin Cancer Prevention
Act” (see report on page 11), we will
UBC professor Dr. John Hill has identified high levels of the enzyme
myeloperoxidase as a important predictor of cardiovascular death.
C A D
Key predictor for CV death found
TOP of the MONTH
CDA working with legislators to
implement new age limits and
other restrictions on patrons of
tanning parlours in Canada
Meanwhile, the World Health
Organization elevates tanning
device risk to other known cancer-
causing agents, such as as ciga-
rettes and mustard gas . . . . . . . .11
Acne: Online followup for patients
with acne just as effective as
conventional consultation
Also: Laser, retinaldehyde combina-
tion shown to improve acne
rosacea, and tretinoin microsphere
gel safe and effective for the treat-
ment of acne vulgaris in eight- to 12-
year-olds .. . . . . . . . . . . . . . . . . . . 14
Burn treatment: In children, 70%
of burns are scalds, in adults, 70%
are typically flame burns
One of the biggest advances in the
care of patients with burn wounds
is the development of dressings
impregnated with silver, which do
not have to be changed as fre-
quently. . . . . . . . . . . . . . . . . . . . . 18
Chronicle Postgraduate
Educational Supplement
In this issue’s Postgraduate
Educational Supplement,
CHRONICLE guest authors from the
University of Cologne investigate
new understandings of cell matrix
interactions in dermal repair and
scarring . . . . . . . . . . . . . . . . . . . . 21
“The proposed private members’ bill for improvedwarnings and labels on tanning beds is
certainly a move in the right direction andwe definitely support this bill.”
Dr. Cheryl Rosen, chief of dermatology, Toronto Western Hospital
and national director of the CDA’s Sun Awareness Program (see page 11)
A high level of myeloperoxidase has
been found to be a key predictor of car-
diovascular death, according to a study
out of the University of British
Columbia’s department of pathology
and laboratory science and the
Providence Heart and Lung Institute,
published in the Journal of theAmerican College of Cardiology
“We hope that the discovery of new
markers of cardiovascular risk will help
identify specific patients who could
benefit from more aggressive treatment
strategies,” said associate professor Dr.
John Hill, the lead investigator who co-
wrote the article with PhD student
Claire Heslop and professor Dr. Jiri
Frohlich.
Data was collected from the med-
ical records and blood samples of con-
senting patients with coronary artery
disease (CAD). The records covered a
13-year period.
The study determined that CAD
patients with higher levels of the enzyme
myeloperoxidase experience twice the
mortality rate than those with lower rates.
The enzyme is associated with oxidative
stress, which damages arterial tissue.
CAD is the cause of over 160,000
hospitalizations in Canada each year.
One-quarter of those hospitalized die.
Bobbe Wood, president and CEO
of the Heart and Stroke Foundation of
B.C. & Yukon, said he was proud to
support these researchers.
Wood added “since almost 40,000
deaths occur in Canada each year due to
CAD, it’s crucial to focus on better meth-
ods to treat such a devastating health
problem.”
From the News Resources of The Chronicle
Published eight times per year bythe proprietor, ChronicleInformation Resources Ltd., withoffices at 555 Burnham thorpe Road,Ste 306, Toronto, Ont. M9C 2Y3Canada. Telephone: (416) 916-2476; Facs. (416) 352-6199.
E-mail: [email protected]
ISSN No. 1209-0581
Contents © ChronicleInformation Resources Ltd., 2010except where noted. All rights
reserved worldwide.
The Publisher prohibits reproduc-
tion in any form, including print,
broadcast, and electronic, without
written permissions.
Printed in Canada. The Chronicleof Skin & Allergy is a Canadianpublication. The Publisher certifiesthat advertising placed in this pub-lication meets Revenue Canadarequirements for tax deductibility.
Subscriptions: $85.60 per year inCanada, $129.95 per year in allother countries. Single copies:$10.00 per issue (plus 5% GST).
Canada Post Canadian PublicationsMail Sales Product AgreementNumber 40016917. Please forwardall correspondence on circulationmatters to: The Chronicle of Skin &Allergy, 555 Burnhamthorpe Road,Ste 306, Toronto, Ont. M9C 2Y3
Ideas in the Service of Medicinesm
Affiliated journals of
the Chronicle
Companies include
Dental Chronicle, The Chronicle of
Neurology & Psychiatry, TheChronicle of Urology & SexualMedicine, The Chronicle ofHealthcare Marketing, Drug RepChronicle, and Linacre’s Books/LesEditions Linacre
June 2010 • Vol. 16 No. 4
Medical Editor
Wayne Gulliver, MD, FRCPC
Editor, Cosmetic Dermatology
Sheldon V. Pollack, MD, FRCPC
Publisher Mitchell Shannon
Editorial Director R. Allan Ryan
Senior Associate Editor
Assistant Editor
Lynn Bradshaw
Production and Circulation
Josh Long
Cathy DusomeComptroller Rose Arciero
Founding Editor Colin A. Ramsay, MD, FRCPC (1936-2003)
John P. Arlette, MD, FRCPC
Benjamin Barankin, MD, FRCPC
Marc Bourcier, MD, FRCPC
W. Alan Dodd, MD, FRCPC
Eric Goldstein, MD, FRCPC
Peter Hull, MD, FRCPC
Rod Kunynetz, MD, FRCPC
Richard Langley, MD, FRCPC
Danielle Marcoux, MD, FRCPC
R.A.W. Miller, MD, FRCPC
H. Eileen Murray, MD, FRCPC
Kim Papp, MD, FRCPC
Yves Poulin, MD, FRCPC
Melanie D. Pratt, MD, FRCPC
Denis Sasseville, MD, FRCPC
Jerry Tan, MD, FRCPC
Ronald B. Vender, MD, FRCPC
Contacting The Chronicle
� READER SERVICE: To change your address, or
for questions about your receipt of the journal,
send an e-mail to [email protected] with
subject line “Circulation,” or call during busi-
ness hours at 416.916.CHROn (2476), or toll-
free at 866.63.CHRON (24766).
� LETTERS: We welcome your correspondence
by mail, fax (416.352.6199), or e-mail. Kindly
use the co-ordinates listed above.
� ADVERTISING: For current rates and data,
please contact the publisher.
� REPRINTS: The content of this journal is copy-
righted. Please contact Mitchell Shannon for
reprint information.
Please turn to Message page 36�
Photo
illustra
tion b
y Josh
Long
, heart d
raw
ing
courte
sy Vin
tag
e C
olle
ctive
/Flic
kr
21385A_SkinAllergy_J10:.ps 6/17/2010 6:05 PM Page 3

Cosmetic Dermatology:New botulinum therapies
coming to market
A n n u a l r e p o r t o n C o s m e t i c D e r m a t o l o g y
4 · June 2010
Lead articleTHE CHRONICLE of SKIN & ALLERGY
The imminent introduction
of alternatives to Botox will
likely provide options that
are more economical for
patients seeking cosmetic
enhancement, according to Can ad -
ian dermatologists.Whether or not an injectable like Xeomin,
Botulinum Neurotoxin Type A, will become a viable
alternative to Botox may involve factors other than the
price point, including consideratons such as the exis-
tence of evidence that supports the superiority of effica-
cy of one product over another and the longer duration
of effect of one product over another, according to Dr.
Rob Miller, a dermatologist in Halifax and associate
professor of medicine in the division of dermatology at
Dalhousie University.
Dosing will be different
“They have different molecular weights,” explained Dr.
Miller, director of the Dermatology Rejuvenation Centre
in Halifax. “The dosing will be different, and the diffu-
sion of the product may be different. That may affect
how rapidly they are accepted into the vanguard of
usage.”
Competitors such as Xeomin and Reloxin (anoth-
er botulinum toxin product also known as Dysport),
are poised to enter the Canadian cosmetic market-
place.
One of the observations made by Dr. Miller, who
has a special interest in wound healing, is that Botox,
and likely other toxins that will come to market, can
improve and accelerate wound healing.
“One of the things that has come out in the litera-
ture is that when there is muscle movement, that
movement opens up the wound,” said Dr. Miller. “If you
inject [botulinum toxin] in the muscle around a facial
wound, for example, you don’t have as much pull of
the muscles, so the wound tends to
heal better.”
The launch of Soft Lift in
Canada is being eagerly awaited,
according to Dr. Miller. Soft Lift, a
combination of Botox and Juve -
derm, purports to provide more
complete correction and increased
longevity through the synergy of
the two products. “It will be used
for adding volume in the face,”
said Dr. Miller.
Aggressive advertising and an
increasing number of manufactur-
ers of cosmetic products are
prompting greater consumer
awareness and leading consumers
to ask dermatologists about particu-
lar categories of products such as
injectables, observes Dr. Nowell
Solish, an assistant professor of
medicine in the division of derma-
tology at the University of Toronto
in Toronto.
“The fillers are the vast major-
i ty of the business,” says Dr.
Solish. “Lasers are also popular
for skin rejuvenation and hair
removal.”
Dr. Solish points to Novabel as
a unique filler that has been approved in Europe. The
manufacturer is pursuing entry of the filler to the
U.S., and it will likely hit the Canadian market after
that.
“It is different from the other fillers because most
other fillers are made of hyaluronic acid or collagen,
whereas this one uses alginate,” explains Dr. Solish.
“The studies indicate that it has longevity of up to 18
months. It looks like it will be a filler that will be good
for certain areas that have been harder to fill in the
past, such as under the eyes.”
Dr. Solish agrees that the arrival of other toxins,
� Factors such as
competitive advertis-
ing and an increasing
number of products
prompt consumer
curiousity
by LOUISE GAGNON,Correspondent, The Chronicle
Dr. Rob Miller
Dr. Nowell Solish
Dr. Mark Lupin
Please turn to Cosmetic dermatology, page 8�
21385A_SkinAllergy_J10:.ps 6/17/2010 6:06 PM Page 4
® Registered trade-markProtected by patent CA2142530STIEFEL CANADA INC.Montreal, Quebec H4R 1E1©2009SCI/D/09-08/CDXL/1187/JA-E
CLINDOXYL Gel (clindamycin phosphate and benzoyl peroxide) is indicated in the topical treatment of moderate acne vulgaris characterized by the presence of comedones, papules and pustules. CLINDOXYL Gel is not indicated for the treatment of cystic acne.
For external use only. Avoid contact with eyes and mucous membranes. If signifi cant diarrhea occurs, the drug should be discontinued. CLINDOXYL Gel should not be given to pregnant or lactating women. Safety and effectiveness in children under 12 have not been established. Use with caution in patients taking neuromuscular blocking agents. Most common side effects are peeling 16.3%, erythema 7.6%, dryness 7.0%, burning 2.3% and pruritus 1.7%.† p<0.01 vs. placebo and p<0.02 vs. clindamycin gel. Global evaluation graded by means of a scale of 0 to 4: 0 = worsening,1 = poor, 2 = fair, 3 = good and 4 = excellent. Based on combined data from 2 double-blind, randomized, parallel, vehicle-controlled trials lasting 11 weeks. Once-daily application. n = 95 (CLINDOXYL Gel), 89 (clindamycin gel) and 58 (placebo).
1. IMS Health Canada: Canadian CompuScript Audit, April 2009. 2. Lookingbill DP et al. J Am Acad Dermatol 1997;37:590-595. 3. CLINDOXYL Gel Product Monograph, Stiefel Canada Inc.
THE # 1 TOPICAL ACNE THERAPY DISPENSED IN CANADA1
3
Acne Detention is a fun and interactive program that engages patients to learn about acne, skin care and proper Clindoxyl use through the latest online technology.
See prescribing summary on page 27
21385A_SkinAllergy_J10:.ps 6/17/2010 8:04 PM Page 5

ENBREL®
*Quality of life (Dermatology Life Quality Index [DLQI]) signifi cantly improved in patients treated with ENBREL vs. placebo (p<0.0001).¶
¶ Randomized, double-blind, placebo-controlled study of adult patients with chronic, stable plaque psoriasis involving ≥10% of body surface area, a minimum PASI of 10. ENBREL 50 mg SC (n=194) or placebo (n=193), twice weekly for 3 months followed by open-label ENBREL 25 mg twice weekly. Percent mean improvement from baseline in DLQI was 70% for ENBREL vs. 6% for placebo. “Clear” or “almost clear” was equal to a score of 0 or 1 on a 0-5 scale. Measured using the static Physicians’ Global Assessment (sPGA). Placebo (sPGA) at 3 months. Baseline PASI (median): ENBREL 50 mg twice weekly 16.1 and placebo 16.0 (last observation carried forward).2
An excellent combination of safety experience and efficacy to help unlock new possibilities*
21385A_SkinAllergy_J10:.ps 6/17/2010 6:12 PM Page 8

www.enbrel.ca
Comprehensive support for patients on ENBREL Services:1-877-9ENBREL (1-877-936-2735)
Experience is Clear
References: 1. IMS, Custom Projected Prescription Data for Specialty Rx Markets (Custom PRx), January 2009. 2. Papp K, et al. A global phase III randomized controlled
trial of etanercept in psoriasis: safety, efficacy, and effect of dose reduction. Br J Dermatol 2005;152:1304-12. 3. Data on file, Amgen Canada Inc. 4. ENBREL Product
Monograph, Amgen Canada Inc. and Wyeth Canada. March 2, 2009.
Significant skin clearance
demonstrated in plaque psoriasis
patients
Established safety profile
Extensive experience
57% of patients assessed as “clear” or “almost clear” at 3 months (ENBREL 50 mg BIW [n=194] vs. 4% for placebo [n=193]; sPGA; p≤0.0001)2¶
67% mean improvement in PASI scores maintained out to 9 months
in an open-label extension (68% mean improvement at 3 months, ENBREL 50 mg BIW [n=194] vs. 0.2% for placebo [n=193]; p<0.0001; followed by 25 mg BIW for 6 months [n=190])3¶
Safety profi le similar to placebo in clinical trials4
Please see Product Monograph for important warnings regarding infections and malignancies
No need for hepatic and renal function tests4ß
Used by >500,000 patients across all indications worldwide3
Over 1 million patient-years of post-market experience4 8 years in Canadian practice, 16 years of clinical experience worldwide3
1
ENBREL is indicated for reducing signs and symptoms, inhibiting structural damage progression and improving physical function of moderately to severely active arthritis in adult patients with rheumatoid arthritis (RA) and psoriatic arthritis (PsA). ENBREL can be initiated in combination with methotrexate in adult patients or used alone in RA and PsA. ENBREL is indicated for reducing the signs and symptoms of moderately to severely active polyarticular juvenile idiopathic arthritis (JIA) in patients aged 4 to 17 years who have had an inadequate response to one or more DMARDs. ENBREL is indicated for the treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. ENBREL is also indicated for reducing signs and symptoms of active ankylosing spondylitis (AS). ENBREL is contraindicated in patients with, or at risk of, sepsis syndrome, such as immunocompromised and HIV+ patients, and in patients with a known hypersensitivity to ENBREL or any of its components. Adverse reactions reported in JIA, PsA, AS, and plaque psoriasis patients were similar to those in RA clinical trials. Adverse events, including serious adverse events occurred at a higher frequency in plaque psoriasis patients over age 65 treated with 50 mg twice weekly. In RA patients, the most common adverse events in placebo-controlled trials were injection site reactions (37%), infection (35%), headache (3%), dizziness (3%) and rash (3%). In RA patients, infections and malignancies were the most common serious adverse events observed. In plaque psoriasis trials, serious infections experienced by ENBREL-treated patients have included: cellulitis, gastroenteritis, pneumonia, abscess, osteomyelitis, viral meningitis, myositis, fascial infection and septic shock. Serious infections leading to hospitalization or death, including sepsis, tuberculosis (TB), invasive fungal and other opportunistic infections, have been observed with the use of TNF blocking agents including ENBREL. Cases of TB may be due to reactivation of latent TB infection or to new infection. Patients have frequently presented with disseminated rather than localized disease. Many of the serious infections have occurred in patients on concomitant immunosuppressive therapy that, in addition to their underlying disease, could predispose them to infections. Treatment with ENBREL should not be initiated in patients with active infections including TB, chronic or localized infections. Administration of ENBREL should be discontinued if a patient develops a serious infection or sepsis. Physicians also should exercise caution when considering the use of ENBREL in patients with a history of recurring or latent infections, including TB, or with underlying conditions, which may predispose patients to infections, such as advanced or poorly controlled diabetes. Before starting treatment with ENBREL, all patients should be evaluated for both active and inactive (‘latent’) TB. Prescribers are reminded of the risk of false negative tuberculin skin test results, especially in patients who are severely ill or immuno-compromised. If inactive (‘latent’) TB is diagnosed, treatment for latent TB should be started with anti-TB therapy before the initiation of ENBREL. Patients should be monitored for the development of signs and symptoms of infection during and after treatment with ENBREL, including the possible development of tuberculosis in patients who tested negative for latent tuberculosis infection prior to initiating therapy. Histoplasmosis and other invasive fungal infections are not consistently recognized in patients taking TNF blockers, including ENBREL. For patients who reside or travel in regions where mycoses are endemic, invasive fungal infection should be suspected if they develop a serious systemic illness. Very rare cases of hepatitis B virus (HBV) reactivation have been reported in patients treated with TNF antagonists. Patients at risk for HBV infection should be evaluated for prior evidence of HBV infection before initiating TNF antagonist therapy and exercise caution in prescribing ENBREL for patients identified as carriers of HBV. There have been rare reports of CNS demyelinating disorders, exercise caution when considering ENBREL for patients with these disorders. Rare cases of neutropenia, leukopenia, thrombocytopenia, anemia and pancytopenia (including aplastic anemia), some with fatal outcomes, have been reported in patients treated with ENBREL. Exercise caution in patients who have a previous history of significant hematologic abnormalities. Reports of malignancies affecting various sites have been received in the postmarketing period. In clinical trials of TNF antagonists, more cases of lymphoma were seen compared to control patients. Patients with RA or psoriasis may be at higher risk for the development of lymphoma. The potential role of TNF blocking therapy in the development of malignancies is not known.
Please refer to Product Monograph for complete prescribing information.ENBREL and Enliven are registered trademarks of Immunex Corporation.
ß Hepatitis B virus carriers should be closely monitored for clinical and laboratory signs of active infection throughout therapy and for several months following discontinuation of therapy.4
See prescribing summary on page 16See prescribing summary on page 34
21385A_SkinAllergy_J10:.ps 6/17/2010 8:07 PM Page 9

8 · June 2010 THE CHRONICLE of SKIN & ALLERGY
such as Xeomin and Reloxin
(Dysport), will expand the toxin mar-
ket. One of the advantages of Xeomin
is its simple formulation. “Xeomin
does not have extra proteins. The
chance of developing antibodies
against Botox would be extremely
low,” says Dr. Solish. “They would be
even lower with Xeomin.”
Other specialists, such as plastic
surgeons, are becoming more
involved in the non-invasive aspects
of cosmetic dermatology, which is a
reflection of the exponential growth
of non-invasive procedures in aes-
thetic medicine, according to Dr.
Solish. Ultrasound technology is being
used for fat removal and is also being
used to tighten skin, he says.
“There are non-surgical app -
roaches to fat removal such as
Liposonix, Zeltiq, and UltraShape,”
says Dr. Solish. “We are seeing results
in most patients. Many patients say
they would rather not have surgery. If
they can get significant improvement
without surgery, that is what they will
opt for—it’s a rapidly growing part of
my practice.”
One of the new developments in
cosmeceuticals are those that contain
peptides and can stimulate collagen
production, producing a noticeable
result in skin, says Dr. Solish.
“There are over-the-counter topi-
cal creams that contain peptides,” he
says. “I tend to use more than one
product. I typically suggest a peptide-
containing product, retinoids, and
Vitamin C. I think they work different-
ly, and the effect is cumulative.”
New products around corner
Individuals who are seeking cosmet-
ic enhancement cover a broad spec-
trum of the patient population, notes
Dr. Solish. “There are individuals
who are under the age of 30 and
they may want lip augmentation,
and there are individuals who are
older than 70 and they may want to
look better. Men now make up
about 10 per cent of my patient pop-
ulation that is seeking cosmetic
treatments.”
Dr. Mark Lupin, a dermatologist in
Victoria and director and founder of
Cosmedica in Victoria, recently
attended the annual meeting of the
American Society of Laser Medicine
and Surgery in Phoenix, and echoes
Dr. Solish’s opinion regarding the
expansion of non-invasive techniques
in cosmetic dermatology.
“There is a non-invasive facial lift
technique using ultrasound and a
non-invasive brow lift,” says Dr.
Lupin, a clinical instructor in the
department of dermatology and skin
science at the University of British
Columbia. “They both do not require
downtime.”
The arrival of Soft Lift is a
response to the emphasis on volumiz-
ing the face in addition to correcting
wrinkles, observes Dr. Lupin. “The
new fillers have more ’lift,’ and they
last longer,” says Dr. Lupin.
Like his colleagues, Dr. Lupin
says that the emergence of alterna-
tives to Botox in Canada is an exciting
phenomenon. “The molecule
[Xeomin] has less protein in it, so
there is less potential of reactions to
it,” he notes. “There is a convenience
factor in that it does not have to be
kept in the fridge.”
With the popularity of tattoos in
contemporary culture, there is an
increasing demand for the removal of
tattoos in some individuals. Q-
switched Yag Lasers now offer the
ability to remove tattoos from the
body and are able to treat more col-
ors in the tattoos, without leaving
noticeable scars or creating pigmen-
tary changes, says Dr. Lupin.
“These lasers have been around
for a number of years, but the quality
is now better,” explains Dr. Lupin.
Lasers being refined
IsoLaz, which combines vacuum with
a painless laser, represents a novel
therapeutic option for patients with
acne vulgaris. The laser helps to
destroy acne-causing bacteria, and
the vacuum helps to loosen dirt,
blackheads, and excess oil from
inside the pores.
Fractional lasers that are ablative,
such as UltraPulse and Fraxl re:pair,
can treat the effects of aging, so that
patients can look more youthful, but
the lasers can also be used to treat
scars on the face and body. “The
patients’ skin is softened with laser
therapy, and it can increase their
mobility and improve function as a
result,” says Dr. Lupin, noting the
lasers have been used to treat the
injuries and scarring experienced by
soldiers who have been injured in
combat.
Patients looking for a treatment
for hypotrichosis can look to solutions
such as Latisse. The product is not yet
available in Canada, but it has been
approved for use in the U.S.
Containing bimatoprost ophthalmic
solution 0.03%, the therapy makes
eyelashes appear longer, thicker, and
darker. RevitaLash, a cosmetic eye-
lash conditioner, is available in
Canada, and is designed to lengthen
eyelashes.
Cosmetic derm: New therapies driving patient interestContinued from page 4
Re: ABCDE mnemonic, April 2010, page 1
THE DEVELOPMENT of the ABCDE mnemonic has
been of great benefit to my practice and my
patients.
I see large number of patients for assessment
of pigmented lesions. I ask my patients to do a
monthly self exam much like doing self breast
exams. I find the ABCDE representation a practical
tool to easily explain what atypical lesions are; that
would alert the patients to seek further medical
assessment. The concept is easy and has proved
invaluable in my practice.
Kudos to the ABCDE!
Dr. Charles Lynde
M A R K H A M , O N T .
� THE ABCDE RULE is a useful screening tool, how-
ever dermoscopy continues to demonstrate supe-
rior sensitivity for detecting melanoma. The odds
ratio for diagnosing melanoma was 15.6 times
higher with dermoscopy versus the naked eye.1
Improved specificity has been demonstrated by a
42 per cent reduction in the number of benign
lesions removed.2 More recently a combination of
dermoscopy and dermoscopic digital monitoring
resulted in a dramatic 64 per cent reduction in the
need for excisions or referrals of benign pigment-
ed lesions in primary care settings.3
The limitations of the ABCDE rule and superi-
ority of dermsocopy has been formalized in the
recommendation contained in the CPG,
Management of Melanoma in Australia and New
Zealand: “Training and utilization of der-
moscopy is recommended for clinicians routinely
examining pigmented skin lesions” (Grade A
Evidence). This recognition plays a role in the
improved diagnostic abilities of family physicians
‘down under’.
Dermsocopy is not as widely practised in
North America as in other jurisdictions. Inclusion
of formalized training in dermsocopy is not the
standard in North America.
The ABCDE rule is a simple screening tool that
is an excellent public health measure. However, I
believe that dermscopy will supplement this rule
in guiding management of worrisome pigmented
lesions.
Dr. David W. Knox
O R A N G E V I L L E , O N T .
1. Vestergaard ME et al: Dermoscopy compared with
naked eye examination for the diagnosis of primary
melanoma: a meta-analysis of studies performed in
a clinical setting. Br J Dermatol 2008.
2. Carli P et al: Addition of dermoscopy to conventional
naked-eye examination in melanoma screening: a
randomized study. J Am Acad Dermatol 2004;
50:683-689.
3. Menzies S et al: Impact of dermoscopy and short-
term sequential digital dermoscopy imaging for the
management of pigmented lesions in primary care:
a sequential intervention trial. Br J Dermatol (in
press).
THE CHRONICLE OF SKIN & ALLERGY welcomes all correspondence from readers, on any matter related to the practice of
medicine. Please send correspondence via email to [email protected], via fax to 416.352.6199, or by mail to The
Chronicle of Skin & Allergy, 555 Burnhamthorpe Rd., Suite 306, Toronto, Ont. M9C 2Y3. Letters may be subject to edit-
ing for length and/or clarity.
L E T T E R S T O T H E C H R O N I C L E
A Toast to ‘Decade 10’
It’s said that in front of
every great man is a
great woman, who
probably can’t believe
her eyes. Here, Dr.
Stuart Maddin of the
University of British
Columbia Department
of Dermatology & Skin
Science celebrates his
90th birthday in
Vancouver, among col-
leagues, proteges, fami-
ly, admirers, childhood
friends, and spouse
Betty Maddin, who must
wait until this
September before she
too is allowed entry into
the Nonagenerians’
Club.
Photo by PAUL KIDSON
21385A_SkinAllergy_J10:.ps 6/17/2010 6:19 PM Page 10

THE CHRONICLE of SKIN & ALLERGY June 2010 · 9
1% of the population, Dr. Spritz said.
“One of the reasons there’s been
such interest in the genetics [of vitili-
go] is that relatively little is under-
stood about the fundamental biolo-
gy,” he told MedPage Today, “and
that has prevented the development
of very effective treatments or, of
course, even prevention.”
But the bigger, more immediate
implication for practice is in malig-
nant melanoma, he said.
In the study, vitiligo was associat-
ed with the major alleles of single
nucleotide polymorphisms (SNPs) in
the TYR region.
Alleles associated with susceptibilityThe strongest associations were with
rs1393350, which increased the odds
of vitiligo by 53% (p=1.60× 10-18 in the
combined analysis), and the nearby
nonsynonymous SNP rs1126809, with
tight linkage disequilibrium between
the two.
“The minor alleles of both these
SNPs are associated with susceptibili-
ty to malignant melanoma,” the
researchers explained in the N Engl J
Med paper.
Thus, vitiligo and malignant
melanoma “may be two sides to the
same coin from a genetic stand-
point,” Dr. Spritz said in the inter-
view.\
Susceptibility to TYR-related
cases of the two diseases might be
“mediated by different or perhaps
even inverse biologic mechanisms,”
the researchers added in the online
paper.
A link of some kind between the
two diseases was suspected because
some melanoma patients develop
vitiligo during the course of treatment
as a good prognostic sign, Dr. Spritz
noted.
The immediate usefulness could
be in helping physicians chose
among treatment options for malig-
nant melanoma patients, he said.
Genetic testing for tyrosinase and
other genes in the study could deter-
mine the best candidates for
melanoma-fighting immunotherapies,
such as interleukin 2 and various vac-
cines, he noted.
“It’s been long known that
patients with the HLA type HLA-A*02
tend to respond best to certain types
of immunotherapy for melanoma,”
he told MedPage Today. “We think
we understand why that is now.”
The study examined more than
half a million SNPs in 1,514 patients of
European-derived, white ancestry
who had generalized vitiligo and
compared them with publicly avail-
able control genotypes from 2,813
others of similar descent.
The top 50 candidates were then
tested in two replication sets in white,
European-descent populations (677
independent patients versus 1,106
controls and 183 simplex trios with
generalized vitiligo versus 332 multi-
plex families).
Among the 10 independent sus-
ceptibility loci for generalized vitiligo,
one of the two major association sig-
nals in the major histocompatibility
complex was in “near-perfect” link-
age disequilibrium with HLA-A*02,
suggesting this was the variant at this
rs12206499 locus that conferred sus-
ceptibility to vitiligo.
The other was in the class II gene
region, between HLA-DRB1 and HLA-
DQA1.
Outside of the major histocom-
patibility complex and aside from
TYR, there were independent associ-
ations of vitiligo with RERE, PTPN22,
LPP, IL2RA, GZMB, UBASH3A, and
C1QTNF6 genes, five of which have
also been associated with genetic
susceptibility to other autoimmune
diseases.
“Most of these genes encode
immune-system proteins involved in
biologic pathways that probably influ-
ence the development of autoimmu-
nity,” Dr. Spritz’ group wrote in the
paper.
Altogether these 10 associations
likely account for only 7.4% of the
total genetic risk for generalized vitili-
go, the researchers noted.
Many of these are in variants that
“basically don’t exist outside of
Caucasians,” Dr. Spritz said.
So the next step is to examine the
associations in other racial and ethnic
populations, a process he said is
already well under way, with results
expected within months.
Copyright MedPage Today, LLC. All
rights reserved. Reprinted with per-
mission. www.medpagetoday.com
See prescribing summary on page xxx
NEWXamiol® gel is indicated for the topical treatment of moderate to severe scalp psoriasis for up to 4 weeks. Xamiol® should be applied to affected areas of the scalp once daily for up to 4 weeks. After satisfactory improvement, the drug can be discontinued. If recurrence takes place, treatment may be reinstituted. The maximum daily dose, including other calcipotriol-containing products, should not exceed 15 g and the maximum weekly dose should not exceed 100 g. Patients should be instructed on correct application and hand washing.
Hypercalcaemia may occur if the maximum weekly dose is exceeded. Serum calcium is quickly normalized when treatment is discontinued. In patients at risk, serum calcium levels should be obtained before treatment and subsequently monitored.
Do not apply on large areas of broken skin or under occlusive dressings, since this increases systemic absorption of corticosteroids. Xamiol® should not be used on the face. Clinical trials with Xamiol® in children, pregnant or nursing women were not done; use is not recommended. Not for ophthalmic use.
Contraindications: viral lesions of the skin; fungal or bacterial skin infections; parasitic infection; skin manifestations in relation to tuberculosis or syphilis, perioral dermatitis, atrophic skin, striae atrophicae, fragility of skin veins, ichthyosis, acne vulgaris or rosacea, rosacea, ulcers or wounds; patients with severe renal insuffi ciency, hepatic disorders, known disorders of calcium metabolism or known hypersensitivity to its formulation; patients with guttate, erythrodermic, exfoliative or pustular psoriasis.
Adverse reactions: Xamiol®: pruritus. Calcipotriol: skin irritation, burning and stinging sensation, dry skin, erythema, rash, dermatitis, eczema, aggravated psoriasis, photosensitivity, hypersensitivity. Betamethasonedipropionate (especially during prolonged topical application): skin atrophy, telangiectasia, striae, folliculitis, hypertrichosis, perioral dermatitis, allergic contact dermatitis, depigmentation, colloid milia.
Combined use of calcipotriol with ultraviolet radiation (UVR) may enhance the skin carcinogenic effect of UVR. This potential risk is known from a pre-clinical fi nding in mice of a reduced time-to-tumour formation from long-term exposure of UVR and topically applied calcipotriol. Patients who apply Xamiol® to exposed skin (e.g. a bald scalp) should avoid both natural and artifi cial sunlight.
For the product monograph or further information, please contact Medical Information at LEO Pharma Inc, at 1-800-263-4218.
® Registered trademarkof LEO Pharma A/S used under license by LEO Pharma Inc. Thornhill, ON www.leo-pharma.com/canada
For Effective Treatment Of Scalp Psoriasis
Hats off to Xamiol®
NOW ON PROVINCIAL FORMULARY IN AB AND QC*
* Exception medication
Vitiligo study demonstrates a genetic link to melanomaContinued from page 1
See prescribing summary on page 28
21385A_SkinAllergy_J10:.ps 6/17/2010 8:08 PM Page 11
Thank you ZYCLARA™ Introducing ZYCLARA™:
1
1*1
1
2 1
1
1 1
See prescribing summary on page
* 81.8% median reduction of AK lesions from baseline was demonstrated 8 weeks post-treatment (vs. placebo 25%; p<0.001).1 In two double-blind, randomized, placebo-controlled clinical studies, 319 subjects with AK were treated with ZYCLARA™ cream or placebo cream. Studies enrolled subjects >18 years of age with 5-20 typical visible or palpable AK lesions of the face or scalp. Study cream was applied to face or balding scalp once daily for two 2-week treatment cycles separated by a 2-week no-treatment period. Subjects continued in the study for an 8-week follow-up period during which they returned for clinical observations and safety monitoring.1 Patients with an increase in AK lesions relative to the number present at baseline had a similar response to those with no increase in AK lesions.
Please see Product Monograph for warnings, precautions and adverse events.
Reference: 1. ZYCLARA™ Product Monograph, December 31, 2009. Graceway Pharmaceuticals.
A new choice in AK treatment. A new day for your AK patients.
See prescribing summary on page 30
21385A_SkinAllergy_J10:.ps 6/18/2010 12:59 AM Page 12

THE CHRONICLE of SKIN & ALLERGY June 2010 · 11
by LYNN BRADSHAWSenior Associate Editor, The Chronicle
The Canadian Dermatology
Association has teamed up
with a number of Canadian
government politicians to introduce a
Skin Cancer Prevention Act that will
prevent youth under the age of 19
years from using indoor tanning
equipment. The legislation would
also be expected to strengthen tan-
ning bed marketing and equipment
use restriction laws.
Tanning beds a risk factor
“The proposed private members bill
for improved warnings and labels on
tanning beds is certainly a move in
the right direction and we definitely
support this bill,”
said Dr. Cheryl
Rosen, chief of
d e r m a t o l o g y ,
Toronto Western
Hospital and
national director
of the CDA’s Sun
A w a r e n e s s
Program, who
spoke at a press
conference in
February.
“Tanning bed
use has been,
according to the
World Health
O r g a n i z a t i o n ,
shown to
increase substan-
tially the risk of
developing melanoma of the skin and
eyes,” said Dr. Benjamin Barankin, a
Toronto dermatologist who special-
izes in medical, surgical, and cosmet-
ic care of the skin.
“We also know it causes prema-
ture wrinkles and age spots. So, a
stronger label will result in fewer skin
cancer deaths, and a less wrinkled
population,” Dr. Barankin told THE
CHRONICLE OF SKIN & ALLERGY.
Melanoma rates on rise
Studies have shown that indoor tan-
ning before the age of 35 years raises
the risk of melanoma by 75%.
Presently in Canada, as in many other
countries, the melanoma incidence
rates are rising every year.
As a result of the danger of tan-
ning, the WHO has elevated tanning
devices to their highest risk category,
which includes other carcinogenic
agents such as mustard gas and ciga-
rettes.
“Tanning bed use under the age
of 18 should be strictly prohibited.
After that age, it is should be a free
choice issue similar to smoking, but
strict labelling and a ban on the false
benefits proclaimed by the tanning
industry should be enforced,” said Dr.
Barankin.
Dr. Barankin suggests that the
tanning industry, like the smoking
industry, should be heavily taxed,
with proceeds going to support
patient education about skin cancer,
tanning bed use, and the types of
lesions to look for.
“Physicians do and should contin-
ue to emphasize the dangers of UV
radiation, and tanning bed salon use.
The CDA and AAD [American
Academy of Dermatology] through
various programs including skin can-
cer screening are already doing a
great job getting the word out,” Dr.
Barankin said.
“Avoiding exposure to ultraviolet
radiation is the main preventable
way of avoiding this type of skin can-
cer, and for this reason we focus on
prevention from sun exposure and
other sources of UV radiation includ-
ing indoor tanning,” reported Dr.
Rosen.
“We will continue to work toward
our goal of banning the use of indoor
tanning for all those 18 years of age
and younger,” Dr. Rosen said in con-
clusion.
Dr. Cheryl Rosen
Dr. BenjaminBarankin
T a n n i n g l e g i s l a t i o n
CDA, legislators work on tanning restrictions� Tanning devices elevated to WHO’s highest cancer risk category, with cigarettes and mustard gas
21385A_SkinAllergy_J10:.ps 6/22/2010 10:02 AM Page 13

12 · June 2010 THE CHRONICLE of SKIN & ALLERGY
by IAN J.S. MOORECorrespondent, The Chronicle
Patch testing may be a stan-
dard technique in dermatol-
ogy, but the diagnostic results
it provides in cases of allergic contact
dermatitis (ACD) confirms its value in
medicine, according to a University of
Ottawa professor of dermatology.
“I would encourage you regard-
ing the value of patch testing for all
sorts of scenarios of eczematous dis-
ease and the value that it brings to
your patients, and what you’re miss-
ing if you do not patch test,” Dr.
Melanie Pratt said during a recent
presentation to attendees at the
Allergy Asthma and Immunology
Society’s Allergy
Update 2010
meeting in
Toronto.
“There is a lot
of disease out
there that goes
undiagnosed.”
Dr. Pratt, who
is also a member
of the North
America Contact Dermatitis Group
(14 dermatologists who compile and
co-publish clinical data on approxi-
mately 5,000 cases every two years),
presented a number of patient case
histories where the results of patch
testing led to successful diagnosis
and treatment.
Shoe dermatitis an example
Shoe dermatitis is a common ACD
that is often undiagnosed, Dr. Pratt
reported during the session. The
prevalence in patch test clinics
ranges between three and 12% and it
erupts in all age groups, with a
greater prevalence in warm climate
zones.
Often superimposed on atopic
dermatitis, the risk factors for this
type of ACD include heat, friction,
occlusion, and hyperhidrosis.
Freeman has reported a 43% inci-
dence of atopy and hyperhidrosis in
shoe ACD cases (Contact Dermatitis1997; 36).
“The ACD can be acute, sub-
acute, or chronic, depending on
when you see [the patients],” Dr.
Pratt added. “They often have it on
the dorsal foot, the dorsal toes, spar-
ing the insteps, and not between the
toe web, where you do see fungus,
but you don’t see that allergy.”
Dr. Pratt recently linked one
eczematous eruption to the epoxy
resin in a human dialysis catheter,
and noted there have been other
similar reactions after medical expo-
sure to the epoxy in ostomy bags,
nasal cannulae, infusion sets for
insulin pumps, and dental fil l ing
materials.
“It’s important when you see
these individuals to test not to epoxy,
but also to everything else they’re
using,” she said. “Polysporin,
chlorhexadine, all their topical
creams and ointments.”
Acrylates—synthetic plastics and
resins used in a wide variety of prod-
ucts—may also provoke occupation-
al and non-occupational allergies,
she added, especially in hearing aid
wearers and women wearing artifi-
cial nails that contain acrylic-based
glues
“This is important, because if [the
women] become sensitized they’ll go
on and have problems, possibly with
dental prostheses, which are made of
acrylates. All the dental cements
nowadays have acrylates in them and
so do those composite [dental] fill-
ings.”
One novel case described by Dr.
Pratt involved a woman with a histo-
ry of acrylic nail and temporary den-
tal crown allergic reactions who,
years later, developed a full-blown
acute contact reaction in the supra-
pubic area of her upper inner thighs
to the Poise brand of incontinence
pad.
Queries to the manufacturer con-
firmed that acrylates are used in the
pad’s super-absorbent material.
Testing in Ottawa and a European
report of a similar case revealed the
provocative agents were printing ink
acrylates.
Dr. Pratt also discussed and illus-
trated cases of ACD reactions to nick-
el (eyeglass frames, belt buckles),
beryllium (dental implants), shellac
(mascara), rubber accelerators (Fruit
of the Loom underwear) and a
lichenoid outbreak caused by a mer-
cury dental amalgam.
“I think it’s important for nickel
allergic people, if they’re strongly pos-
itive, to be encouraged to get the
nickel test kit,” she said. “Especially
those young teen-age girls who come
in with that peri-umbilical contact
dermatitis from belt buckles or pierc-
ing.
“If you just tell them to not wear
their jeans, they won’t do that.”
Polysensitization not uncommon
Polysensitization is not uncommon,
Dr. Pratt noted. In one of her cases, a
gentleman had ACD reactions on sev-
eral body sites to formaldehyde
releasers: coconut amido propyl
betaine (CAPB) and dimethyl amino-
propylamine (DMAPA) in several
shampoos the patient used; balsum
of Peru in the scented products he
favored; budesonide in desonide and
Cyclocort (group B steroids) medica-
tions and the thiorurea component in
the neoprene of the CPAP (continu-
ous positive airway pressure) strap he
used.
“With contact dermatitis you
have to figure out what the positives
are, find the sources, educate the
patient, and eliminate the source and
then treat [the patient],” Dr. Pratt
summarized.
She has added dimethylfumarate
to her list of suspect ACD antigens
after reading a report from the BritishJournal of Dermatology (2008;
159:218-221). Used mainly as biocide
sachets by furniture and shoe manu-
facturers to eliminate moulds that
may cause leather to deteriorate dur-
ing storage and transportation in
humid climates, the chemical has
also had medical applications in pso-
riasis, multiple sclerosis, therapy-
resistant alopecia areata, and other
illnesses.
“Dimethylfumarate proved to be
a very potent allergic contact sensitiz-
er,” Dr. Pratt cautioned.
“It produces severe allergic con-
tact dermatitis at very low concentra-
tions.”
A C D
Patch tests valuable for eczematous disease � Patch tests bring value in many scenarios of eczematous disease, according to Dr. Melanie Pratt
Dr. Melanie Pratt
Study data suggest that isotretinoin 0.3 mg/kg might be an effective and
well-tolerated therapy option for the treatment of rosacea subtypes II and III
and can be used successfully as an alternative to therapy with oral antibi-
otics (J Dtsch Dermatol Ges 2010; Mar 12).
In the study, 573 patients with rosacea subtypes II and III received one
of three different dosages of isotretinoin (0.1 mg, 0.3 mg, or 0.5 mg per kg
body weight), doxycycline (100 mg daily for 14 days, then 50 mg daily) or
placebo during this double-blinded, randomized study conducted over the
course of 12 week at 35 German centers.
Study findings indicate that isotretinoin 0.3 mg/kg proved to be the most
effective dose and demonstrated significant superiority versus placebo.
Isotretinoin 0.3 mg/kg also showed significant non-inferiority versus doxycy-
cline with reduction of lesions of 90% compared to 83% with doxycycline.
The investigators diagnosed complete remission in 24% of patients partici-
pating in the study, and marked improvement in a further 57% of patients
receiving isotretinoin treatment, in contrast to those treated with doxycy-
cline, which showed remission in 14% of patients and marked improvement
in 55% of patients. The authors added that isotretinoin 0.3 mg/kg had a simi-
lar safety profile to when it is used for the treatment of acne. Compared to
0.3 mg/kg, isotretinoin at a dose of 0.5 mg/kg produced more dermatitis
facialis.
“Systemic isotretinoin has been known for decades to be effective in
the treatment of severe forms of rosacea, but it must be used off-label
because of the lack of evidence-based data,” the study authors concluded.
From the News Resources of The Chronicle
R o s a c e a
Isotretinoin 0.3 mg/kg showspotential in Tx of rosacea
21385A_SkinAllergy_J10:.ps 6/22/2010 10:02 AM Page 14

THE CHRONICLE of SKIN & ALLERGY June 2010 · 13
erence.
“I do not think differently regard-
ing what treatment options I can offer
children,” he noted.
Dr. Strober added that some
viable choices for treating pediatric
patients include methotrexate,
cyclosporine, acitretin, etanercept,
adalimumab, infliximab, the IL12 and
23 inhibitor ustekinumab, and ale-
facept.
“All of these are viable choices in
my opinion even though they are not
approved for the treatment of kids
with moderate to severe psoriasis.
Really, there is no approved systemic
therapy for moderate to severe psori-
asis in children, just some topicals.”
Dr. Strober commented.
“Some treatments for adults can
be options for children and adoles-
cents, especially adolescents, but I
think for children as well. Frankly, if my
child had psoriasis, I might prefer them
not to be on methotrexate or acitretin,
but I might prefer them to be on a bio-
logic that has data substantiating safe-
ty, and there are data out there.”
Dr. Strober noted that methotrex-
ate has been used off-label for the
treatment of juvenile idiopathic arthri-
tis, and that juvenile idiopathic arthri-
tis often presents in a similar manner
as psoriatic arthritis. These can be
considered psoriatic patients without
skin problems, he said.
“Cyclosporine is very effective in
children as well and is used as a
treatment option for many pediatric
conditions,” he said.
Acitretin is effective; however,
researchers are not clear of its effect
on skeletal development.
Etanercept, he noted, has been
shown to be effective in pediatric
patients between four and 17 years of
age. “I think etanercept actually
works better in children from a raw
data standpoint than adults, probably
because there was a weight-based
dosing—8.8 mg/kg per week in little
patients up to a maximum dose of 50
mg weekly,” said Dr. Strober.
“But FDA approval will not hap-
pen so etanercept is always going to
be used off label, so to speak.”
Pregnancy and psoriasis treatment
“Vaccination and pregnancy might
seem esoteric, but vaccination should
be considered carefully,” he said.
Dr. Strober recalls a case involv-
ing a 32-year-old woman with exten-
sive psoriasis, and psoriatic arthritis
as well. She indicated that her psori-
atic arthritis was very debilitating and
it had a tremendously negative
impact on her quality of life. This
patient reported that eventually she
would like to start a family.
“This is a challenging case and in
addition [to these factors] the patient
indicated that she plans to go to
South America in three months and
wants a vaccination for yellow fever
within one month of her departure,”
Dr. Strober told the audience.
The first step is to decide what
therapy you will give her up front, Dr.
Strober noted. He added that could
be methotrexate, an anti-TNF biolog-
ic, ustekinumab, or a nonsteroidal.
“Remember, she has psoriatic
arthritis. I think that more or less nar-
rows it down to choices of one and
two.”
Dr. Strober said he has a problem
with the idea psoriatic arthritis can be
treated with nonsteroidal anti-inflam-
matory drugs.
“I think psoriatic arthritis is a seri-
ous condition and it really needs to
be addressed as aggressively as psori-
Help your patients treat their psoriasis
Available in 60 g and 120 g tubes.
For the product monograph or for further information, please contact Medical Information at LEO Pharma Inc. 1-800-263-4218.
NOW ON PROVINCIAL FORMULARY IN AB, SK,
ON AND QC*
Dovobet® (calcipotriol betametha-sone dipropionate) ointment is indicated for the topical treat-ment of psoriasis vulgaris for up to 4 weeks.Application on large areas of damaged skin, in skin folds, or under occlusive dressings should be avoided due to increased systemic absorption of corticosteroids. Dovobet® (calcipotriol betamethasone dipropionate) should not be used on the face or in children.
If long-term therapy is anticipated, it is recommended that treatment be interrupted periodically or that one area of the body be treated at a time. Prolonged use of corticosteroid-containing preparations may produce striae or atrophy of the skin or subcutaneous tissues. There may be a risk of rebound psoriasis when discontinuing corticosteroids after prolonged periods of use. Hypercalcemia can develop but is usually associated with excessive administration (maximum recommended weekly amount of 100 g). If serum calcium levels become elevated, Dovobet® should be discontinued and serum calcium levels measured once weekly until they return to normal.
The most common adverse reaction associated with Dovobet® (calcipotriol/betamethasone dipropionate) was pruritus. Calcipotriol is associated with local reactions such as transient lesional and perilesional irritation. Topical corticosteroids can cause the same spectrum of adverse effects associated with systemic steroid administration, including adrenal suppression. Adverse effects associated with topical corticosteroids are generally local and include dryness, itching, burning, local irritation, striae, atrophy of the skin or subcutaneous tissues, telangiectasia, hypertrichosis, folliculitis, skin hypopigmentation, allergic contact dermatitis, maceration of the skin, miliaria, or secondary infection. If applied to the face, acne rosacea or perioral dermatitis can occur. In addition, there are reports of the development of pustular psoriasis from chronic plaque psoriasis following reduction or discontinuation of potent topical corticosteroid products.
Due to the corticosteroid component, Dovobet® is contraindicated for the treatment of viral, fungal, or bacterial skin infections; tuberculosis of the skin; syphilitic skin infections; chicken pox; eruptions following vaccinations; and in viral diseases such as herpes simplex, varicella, and vaccinia.
Calcipotriol when used in combination with ultraviolet radiation (UVR) may enhance the known skin carcinogenic effect of UVR.
Not for ophthalmic use.
See prescribing summary on page xxx
® Registered trademarkof LEO Pharma A/S used under license by LEO Pharma Inc. Thornhill, ON www.leo-pharma.com/canada
®
Once Daily. Effective psoriasis therapy.
* Exception medication
Psoriasis: Considerations for pregnant, pediatric patientsContinued from page 1
“This is a
chal-lenging
caseand in addition [to these
factors] the patientindicated that she plans to
go to South America inthree months and wants a
vaccination for yellowfever within one month of
her departure.”—Dr. Bruce Strober
Please turn to Psoriasis, page 36�
See prescribing summary on page 29
21385A_SkinAllergy_J10:.ps 6/17/2010 8:10 PM Page 15

14 · June 2010 THE CHRONICLE of SKIN & ALLERGYAcne research
From the News Resources of The Chronicle
Data published in the May 24, 2010 issue of Pediatrics suggests the 0.04%
tretinoin microsphere gel (TMG) pump is effective and safe for the treat-
ment of acne vulgaris in this eight- to 12-year-old population.
This open-label study was conducted with 40 patients eight to 12 years of
age (mean age: 10.7 years) with mild/moderate acne, defined on the basis of
Evaluator’s Global Severity Score (EGSS) values between two and three. Over
the course of this investigation, patients were treated with the 0.04% TMG for
12 weeks and evaluated at baseline and weeks 3, 6, and 12. Authors note that
the primary end points were changes in EGSS and Alternative Evaluator’s
Global Severity Score values; the secondary efficacy end point was the
Investigator’s Global Evaluation of treatment responses at week 12.
Findings reveal that the mean EGSS value decreased significantly from
baseline to week 12 (2.6 vs 2.1; p<0.001), with 75% of cases being graded
as almost clear or mild. Additionally, the mean Alternative Evaluator’s
Global Severity Score value decreased to 2.4 from 3.1 during the 12-week
period (p<0.001). The mean Investigator’s Global Evaluation score was
3.39 at week 12, indicating moderate improvement of acne. Treatment-
associated adverse events were minimal, with mild skin irritation being
most commonly recorded, generally in the first three weeks of therapy.
The investigators recommend additional studies in this population to con-
firm their findings.
F o r m u l a t i o n s
Tretinoin gel effective� For treatment of acne vulgaris in teens
From the News Resources of The Chronicle
Scientists suggest that delivering online follow-up care to acne patients via
an e-visit platform might be beneficial and produce clinical outcomes
equivalent to those of conventional office visits (Arch Dermatol April 2010;
146(4):406-411).
During this study, 151 patients with mild to moderate facial acne were
assessed at two teaching hospitals in Boston between Sept. 2005 and May
2007. The mean age of subjects was 28 years; most were female (78%),
white (65%), and college educated (69%).
Over the course of the investigation, each of the participants was
asked to carry out four follow-up visits using either an e-visit platform or
conventional office care. At six-week intervals, subjects in the e-visit group
were prompted to send images of their skin and an update, via a secure
Web site, to their dermatologist.
Finding reveal that the decrease in total inflammatory lesion count
was similar in the e-visit and office visit groups (6.67 and 9.39, respective-
ly) (p=0.49). Both subjects and dermatologists reported comparable satis-
faction with the care provided regardless of the visit type (p=0.06 and
p=0.16, respectively). Compared with conventional office visits, online
follow-up visits were considered to be time saving for subjects and time
neutral for dermatologists (4 minutes, 8 seconds vs. 4 minutes, 42 sec-
onds) (p=0.57).
E - m e d i c i n e
Online followup for acne� E-visit as good as conventional consultation
Acne updateSTUDY SHOWS TAZAROTENE0.1% CREAM EFFECTIVEInvestigators suggest that tazarotene
0.1% cream might be more effective
and nearly as well tolerated as ada-
palene 0.3% gel in reducing acne
lesions and more effective than ada-
palene 0.3% gel in reducing postin-
flammatory hyperpigmentation
(PIH) (J Drugs Dermatol May 2010;
9(5):549-558).
This 16-week study evaluated
once-daily tazarotene 0.1% cream
and adapalene 0.3% gel in patients
with moderate-to-severe acne.
Findings revealed that patients treat-
ed with tazarotene 0.1% cream per-
formed better in many acne efficacy
measures (reduction in lesion
counts, percentage of patients
achieving a 50% lesion count reduc-
tion, overall disease severity, investi-
gator’s global assessment) than did
patients treated with adapalene 0.3%
gel. Reduction in postinflammatory
hyperpigmentation (PIH) was also
significantly greater with tazarotene
0.1% cream than with adapalene
0.3% gel (p</= 0.018). Irritation was
infrequent, generally mild, and simi-
lar between treatment groups.
LASER, RETINALDEHYDE COMBO
IMPROVES ACNE ROSACEAStudy results suggest a 532 nm laser
combined with topical retinaldehyde
improved overall redness, telangiec-
tasia, and skin texture in acne
rosacea patients (J Otolaryngol HeadNeck Surg June 2010; 39(3):292-296).
A total of 14 patients with type 1
erythematotelangiectatic acne
rosacea participated; during the inves-
tigation researchers had randomly
chosen a side of the patient face to be
treated. The opposite side of the face
served as the control. Patients under-
went six treatments with the 532 nm
laser, with four sets of photodocumen-
tation over a period of three months.
After each treatment, patients were
asked to rate their degree of improve-
ment based on a five-point improve-
ment scale, and they were assessed
by five separate blinded evaluators.
Findings reveal that 100% of
patients noted a mild to moderate
improvement in all signs of type 1
acne rosacea, including overall red-
ness of the face, telangiectasia, and
skin texture. The blinded evaluators
were able to note a difference
between the treated and untreated
sides 47% of the time.
NEW AHA CREAM FOR ACNEStudy data confirms the high tolera-
bility and efficacy of a cream formu-
lated with a new mix of alpha-
hydroxy acids (Hyseac AHA cream),
and also reasonably suggest its pos-
sible use as monotherapy (G ItalDermatol Venereol June 2010;
145(3):319-322).
In all, 248 patients with mild-
moderate acne (comedonic, inflam-
matory, or mixed) were assessed by
10 dermatologists from different
Italian areas during their routine prac-
tice for tolerability and efficacy.
Investigators indicate that the med-
ication with Hyseac AHA cream was
prescribed at first consultation for 60
days, twice a day, either as a
monotherapy (49.2% patients) or in
association with a pharmacological
treatment (50.2%). Tolerability was
good to excellent in 92.3% of patients,
without significant differences
between patients using AHA cream in
monotherapy (90%) or associated
with concomitant pharmacological
treatment (97.6%). Efficacy was high
in 64.2% patients, without significant
differences related to concomitant
pharmacological treatment and/or
the acne clinical type.
LASER NO ADDITIONAL BENEFITFindings from a report in the Apr. 15,
2010 issue of the British Journal of
Dermatology does not support the
concept that pulsed dye laser (PDL)
treatment in acne vulgaris provides
substantial benefit when combined
with a proven topical treatment.
During this study, 80 patients
(47.5% males, 52.5% females, mean
age 19.7+/-5.9 years) were random-
ized in a 1:2 ratio to receive clin-
damycin 1%/benzoyl peroxide 5%
hydrating gel (C/BPO ) alone or in
combination with PDL treatment
(wavelength: 585 nm, energy flu-
ence: 3 J/cm2, pulse duration: 0.35
msec, spot size: 7 mm). Overall,
patients were evaluated at baseline,
two, and four weeks after initial
treatment. Primary end points were
the Investigator’s Static Global
Assessment (ISGA) score and lesion
count; the secondary end point was
the Dermatology Life Quality Index
(DLQI). Both groups showed signifi-
cant improvement during observa-
tion, but there was no significant or
otherwise appreciable difference
between treatment modalities as far
as the extent of improvement was
concerned.
21385A_SkinAllergy_J10:.ps 6/22/2010 10:33 AM Page 16
ANTHELIOS XLFace and Body Cream SPF 60
Broad-spectrum UVB and UVA protection with photostablesun-filtering system featuring Mexoryl® XL.
With Mexoryl® XL, La Roche-Posay enters a new era in dermatological sun protection
La Roche-Posay - a committed partner to dermatologists — has integrated ANTHELIOS XL SPF 60 into its line of sun protection products. Containing Mexoryl® XL, a photostable sun filter that works synergistically with Mexoryl® SX, ANTHELIOS XL provides broad-spectrum protection against UVB and UVA.
The protective performance of ANTHELIOS XL has been demonstrated in 21 clinical studies carried out by world-renowned dermatologists.
Broad-spectrum UVB and UVA protection> A patented formulation of Mexoryl® XL, Mexoryl® SX and other sun filters
Soothing to the skin> Comfortable texture and easy to apply> Fragrance-free> Non-comedogenic> Tolerance-tested under dermatological control
Loyal to its education mission, La Roche-Posay has created a skin cancer awareness initiative that revolves around an interactive tool to help patients monitor their moles.
Cau
tion:
For
ext
erna
l use
onl
y. A
void
con
tact
with
eye
s.D
isco
ntin
ue u
se if
irri
tatio
n or
ras
h oc
curs
.Fo
r us
e on
chi
ldre
n un
der
6 m
onth
s of
age
con
sult
you
r do
ctor
.M
exor
yl®
is a
reg
iste
red
trad
emar
k of
L’O
réal
S.A
.
LA ROCHE-POSAY. COMMITTED TO DERMATOLOGY.
SUN INNOVATION: MEXORYL® XL
21385A_SkinAllergy_J10:.ps 6/17/2010 6:36 PM Page 17

19 Green Belt Drive, Toronto, Ontario M3C 1L9© 2010 JANSSEN-ORTHO Inc.*All trademark rights used under license STJA100048E
STELARA® (ustekinumab injection) is indicated in adult patients for the treatment of chronic moderate to severe plaque psoriasiswho are candidates for phototherapy or systemic therapy.
Contraindications for STELARA® include: patients with known hypersensitivity to STELARA® or any of its components or patientswith severe infections such as sepsis, tuberculosis and opportunistic infections.
STELARA® is a selective immunomodulator. Immunomodulating agents have the potential to increase the risk of malignancy.Some patients who received STELARA® in clinical studies developed malignancies. In the controlled and non-controlled portionsof the placebo-controlled psoriasis clinical studies, the incidence of malignancies excluding non-melanoma skin cancer was 0.36per 100 patient-years of follow-up for STELARA®-treated patients (8 patients in 2,249 patient-years of follow-up) and includedbreast, colon, head and neck, kidney, prostate, and thyroid cancers. The rate of malignancies reported in STELARA®-treatedpatients was comparable to the rate expected in the general population (standardized incidence ratio = 0.68 [95% confidenceinterval: 0.29, 1.34]). The incidence of non-melanoma skin cancer was 0.80 per 100 patient-years of follow-up for STELARA®-treated patients (18 patients in 2,245 patient-years of follow-up).
STELARA® has not been studied in patients with a history of malignancy. Caution should be exercised when considering the useof STELARA® in patients with a history of malignancy or when considering continuing treatment in patients who develop amalignancy.
STELARA® is a selective immunomodulator and may have the potential to increase the risk of infections and reactivate latentinfections. Caution should be exercised when considering the use of STELARA® in patients with a chronic infection or a historyof recurrent infection. If a patient develops a serious infection, they should be closely monitored and STELARA® should not beadministered until the infection resolves.
Prior to initiating treatment with STELARA®, patients should be evaluated for tuberculosis infection. STELARA® should not begiven to patients with active tuberculosis. Treatment of latent tuberculosis infection should be initiated prior to administeringSTELARA®. Anti-tuberculosis therapy should also be considered prior to initiation of STELARA® in patients with a past history oflatent or active tuberculosis in whom an adequate course of treatment cannot be confirmed. Patients receiving STELARA® shouldbe monitored closely for signs and symptoms of active tuberculosis during and after treatment.
The most common adverse reactions (>10%) in controlled and uncontrolled portions of the psoriasis clinical studies withSTELARA® were nasopharyngitis and upper respiratory tract infection. Most were considered to be mild and did not necessitatedrug discontinuation.1
Please see Product Monograph for full prescribing information for STELARA®. For more information, please contactJanssen-Ortho Inc. Medical Information Department at 1-800-567-3331. The Product Monograph may also be found atwww.janssen-ortho.com.
† Multicentre, randomized, active-controlled study comparing the safetyand efficacy of STELARA® and etanercept in 903 patients 18 years ofage and older with chronic (>6 months) plaque psoriasis who had aminimum body surface area (BSA) involvement of 10%, Psoriasis Areaand Severity Index (PASI) score ≥12, Physician Global Assessment(PGA) score ≥3, were candidates for phototherapy or systemic therapy,and who had had an inadequate response to, intolerance to, orcontraindication to cyclosporine, methotrexate, or PUVA therapy.Patients who were randomized to STELARA® were administered studydrug at weeks 0 and 4 (n=209 for 45 mg, n=347 for 90 mg); patientsrandomized to etanercept 50 mg (n=347) were administered study drugtwice weekly through week 12.1
‡ Initial doses of STELARA® administered at weeks 0 and 4 (induction)followed by once every 12 weeks (q12w – maintenance). For patientswho inadequately respond to dosing every 12 weeks, consideration maybe given to treating as often as every 8 weeks.1
§ IL = interleukin// Multicentre, randomized, double-blind, placebo-controlled study toassess the safety and efficacy of STELARA® in 766 patients 18 years ofage and older with chronic (>6 months) plaque psoriasis who had aminimum BSA involvement of 10%, PASI score ≥12 and who werecandidates for phototherapy or systemic therapy. Percentage of patientsachieving PASI 75 at week 12 was 67% in the STELARA® 45 mg group(n=255), 66% in the STELARA® 90 mg group (n=256) and 3% in the
placebo group (n=255); percentage of patients achieving PASI 75 at week24 were 76% for the 45 mg group and 85% for the 90 mg group.1
# Multicentre, randomized, double-blind, placebo-controlled study toassess the safety and efficacy of STELARA® in 1,230 patients 18 yearsof age and older with chronic (>6 months) plaque psoriasis who had aminimum BSA involvement of 10%, PASI score ≥12 and who werecandidates for phototherapy or systemic therapy. Percentage of patientsachieving PASI 75 at week 12 was 67% in the STELARA® 45 mg group(n=409), 76% in the STELARA® 90 mg group (n=411) and 4% in theplacebo group (n=410).1
**In PHOENIX 1 (n=766) patients randomized to STELARA® received45 mg or 90 mg at weeks 0 and 4 followed by the same dose every12 weeks. Patients randomized to receive placebo at weeks 0 and 4crossed over to receive STELARA® (either 45 mg or 90 mg) at weeks12 and 16 followed by the same dose every 12 weeks. PASI 75responders at both weeks 28 and 40 were re-randomized to eithercontinue dosing of STELARA® every 12 weeks or to placebo (i.e.,withdrawal of therapy). Patients withdrawn from STELARA® at week 40reinitiated STELARA® at their original dosing regimen when theyexperienced at least a 50% loss of their PASI improvement obtained atweek 40. Patients were followed for at least 76 weeks. The studydesign for PHOENIX 2 (n=1,230) was identical to PHOENIX 1 throughweek 28.1
References: 1. STELARA® (ustekinumab) Product Monograph, Janssen-Ortho Inc., December 12, 2008.2. Griffiths CEM, et al. Comparison of ustekinumab and etanercept for moderate-to-severe psoriasis. N Engl J Med 2010;362:118-28.
See prescribing summary on page xxxSee prescribing summary on page 36
21385A_SkinAllergy_J10:.ps 6/17/2010 8:13 PM Page 18

Head-to-head study results: NOW PUBLISHED!
STELARA®* 45 and 90 mg demonstrated superior PASI 75 andPASI 90 response rates vs. 50 mg etanercept at week 12†1,2
• PASI 75: 67 and 74% vs. 57% (p=0.012 and p<0.001)• PASI 90: 36 and 45% vs. 23% (p<0.001 for both)
Dose free... days a year
maintenancedoses/year‡1
STELARA®, a novel first-in-class treatment (IL-12 and IL-23§ selectiveimmunomodulating agent), demonstrated:
STELARA®, a treatment for chronic moderate to severe plaque psoriasis, is givensubcutaneously at weeks 0 and 4 (induction period) followed by convenient maintenancedosing once every 12 weeks.‡1
• ≥75% psoriasis improvement (PASI 75)� 67–76% of patients vs. 3–4% for placebo (p<0.001) at week 12 (after only 2 doses:weeks 0 and 4) //#**1
• Response over time� 76–85% of patients achieved PASI 75 by week 24 (after only 3 doses: weeks 0, 4 and 16) andresults were generally sustained through week 36//**1
Proven safety profile. Demonstrated excellent tolerability.1
21385A_SkinAllergy_J10:.ps 6/17/2010 6:41 PM Page 19

by LOUISE GAGNONCorrespondent, The Chronicle
One of the newest advances
in the care of burns is the
use of dressings that are
impregnated with silver and do not
require clinicians to change them fre-
quently.
“One of the products that we are
using a lot right now at Sick
Children’s Hospital is Aquacel Ag,
which absorbs a lot of fluid and is soft
and malleable to the wound,” said Dr.
Joel Fish, medical director of the
burn program at the Hospital for Sick
Children in
Toronto and chief
medical officer at
St. John’s Rehab
in Toronto.
Aquacel Ag is
made from sodi-
um carboxymeth-
lycellulose con-
taining 1.2% silver
in an ionic form,
which exerts an
a n t i m i c r o b i a l
effect. As healing
progresses and
the amount of
exudate is
reduced, the
interval between
dressing changes
may be extended
to up to 14 days in burns.
“We have been using it as almost
the standard of care for childhood
burns,” explained Dr. Fish, saying the
use of the dressing minimizes hospi-
tal visits. “We see two or three chil-
dren a week with small burns. It real-
ly has had an impact in the treatment
of small childhood burns.”
Clinicians now recognize that
pediatric patients, in particular, are
facing nutritional deficiencies from 18
months to two years after experienc-
ing a significant burn. To respond to
those deficits, clinicians are now
administering synthetic testosterone
orally to children who have experi-
enced major burns that cover at least
50% of their body surface area.
“We now have a good under-
standing that there are metabolic
deficits in children long after their
wounds have healed,” said Dr. Fish,
noting adult patients are also being
administered synthetic testosterone.
Surgery should be as early as possible
Another emerging therapy is
Debridase, an enzymatic debriding
agent that contains
bromelain, found in
pineapple and other
tropical fruit, as its active
ingredient. In clinical
studies, it was success-
ful in debriding second-
degree and third-degree
burns.
“It cleaves dead tis-
sue and leaves all the
live tissue,” said Dr. Fish.
“What is not appealing
is that it can be quite
painful. It is a non-inva-
sive form of cleaning
deep wounds. It may
catch on because it is
non-invasive.”
Integra, a tissue-
engineered product for
burn and reconstructive
surgery, is being
employed with increas-
ing frequency in managing burns, par-
ticularly in instances when surgeons
are lacking donor sites, according to
Dr. Fish.
Generally, when burns are deep,
it is imperative to have surgery sooner
rather than later, said Dr. Fish. Most
burns should heal within a window of
two weeks, and if they do not heal on
their own, then surgery should be
considered, he added.
Factors such as the degree of a
burn, whether it is a superficial burn,
partial-thickness burn, or full-thick-
ness burn, influence the manage-
ment of the burn, as does the extent
to which the burn covers the body
surface area, explained Dr. David
Keast, co-director of the International
Interprofessional Wound Care Course
sponsored by the University of
Toronto.
“You can have a full-thickness
burn that covers a minor percentage
of the body surface area, which does
not require hospitalization, or a
superficial burn, where nearly 100
per cent of the body is covered, and
that may require hospitalization,”
said Dr. Keast, clinical adjunct pro-
fessor of family medicine at the
University of Western Ontario in
London, Ont.
There are several considerations
that need to be weighed in terms of
the care of a patient who experiences
a burn.
“Someone who has a small area
of the body affected by a second-
degree burn who is 95 years old may
require hospitalization compared to
someone who is much younger,” said
Dr. Keast.
“It may be that an individual has a
bunch of co-morbid conditions [at
age 95], and one insult can tip that
person over the edge.”
In addition, if a burn is sustained
that affects a joint, mobility may be
affected and physiotherapy is war-
ranted in such instances.
Since the management of burns
and rehabilitation following burns is a
specialized area, there are not a great
deal of studies in the literature to sup-
port best practices, according to Dr.
Fish.
Given the absence of best prac-
tices, Dr. Fish and other health pro-
fessionals in Ontario, such as physio-
therapists and occupational thera-
pists, met last year to review stan-
dards for rehabilitation in burn care
in the province.
New standards to be published
“The guidelines will be published this
year,” said Dr. Fish, who chaired the
committee that reviewed the stan-
dards. “It sets some standards in
terms of the frequency of therapy and
what is required for more serious
burn injuries.”
Dr. Fish differentiated between
the presentation of burns in adult
patients and those in pediatric
patients: about 70% of burns that pre-
sent in children are scald burns, due
to exposure to hot liquids, and 30%
are flame burns; in adults, 30% of
burns are scald burns, and 70% are
flame burns that are deep and often
require surgery.
“It [the proportions] have to do
with exposure to risk in children,”
said Dr. Fish. “Children aged two to
three years of age are at highest risk
of experiencing a scald burn.”
Fortunately, prevention efforts
have produced results and have
reduced the number of major burns
that present annually to pediatric
burn units in North America, accord-
ing to Dr. Fish.
Electrical burn injuries are a new
a new focus of prevention. Dr. Fish
and colleagues have studied the
prevalence of these burn injuries
among electricians and electrical
apprentices in Ontario, and they con-
cluded that fused lead multimeters
have been effective in stemming
electrical burn injuries.
18 · June 2010 THE CHRONICLE of SKIN & ALLERGY
B u r n t h e r a p y
Burns often different in children, adults� In children, 70% of burns are scald burns; in adults, 70% of cases are typically flame burns
Dr. David Keast
Dr. Joel Fish
Abbott Laboratories LimitedHumira . . . . . . . . . . . . 39, 31-33
Amgen Canada/Wyeth Canada Enbrel . . . . . . . . . . . . . . ..6-7, 34-35Enliven. . . . . . . . . . . . . . . . . . . .2
Bayer Inc.Finacea . . . . . . . . . . . . . . . . . . .12
Daniele HenkelCorporate . . . . . . . . . . . . . . 19
Stiefel, a GSK companyClindoxyl . . . . . . . . . . . . 5, 14, 27
Graceway Canada CompanyZyclara . . . . . . . . . . . . . . 10, 30
Janssen-Ortho Inc.Stelara . . . . . . . . . . . .16-17, 36-37
La Roche-PosayAnthelios XL . . . . . . . . . . . . 15
LEO Pharma Inc.Xamiol . . . . . . . . . . . . . . . . .9, 28Dovobet . . . . . . . . . . . . . . 13, 29Fucidin . . . . . . . . . . . . . . . . . .20
L’Oreal CanadaSkinCeutical . . . . . . . . . . . . 11
Pierre Fabre Dermo-Cosmétique
Canada Inc.Tolérance . . . . . . . . . . . . . . 40
THERAPEUTIC
INDEX
Scald injury (left) in a 42-year-old male with diabetes and peripheral neuropathy,who soaked his foot in scalding water and sustained a partial thickness (2nd degree)burn injury to the forefoot. He was treated with debridement, silver-containing burndressings, oral antibiotics, and pressure off-loading for the foot. The injury resolvedcompletely with four weeks of treatment as an outpatient.
(Photos courtesy Dr. David Keast)
21385A_SkinAllergy_J10:.ps 6/17/2010 6:42 PM Page 20

Massage techniques that restore the physical properties of scar tissue, to improve the appearance of the epidermis and skin inflammation, have now been in use for more than 30 years and the benefits should not be overlooked. Since 1991 the LPG technique has been used to treat the after-effects of burns. By shifting both rollers of the device’s treatment head, the formed cutaneous fold is stimulated using a ‘roll and lift’ technique that alleviates the tangential pressure that causes the fold. A wide variety of protocols allows for a measured and adapted stimulation of the aponeurosis and skin connective tissue, which is also associated with an improvement of microcirculatory disorders. Since 1992, this technique has significantly evolved with three advancements: 1995: Development of the rhythmicity allowing for better control of the microcirculation and the inflammatory evolution. 1997: Creation of the active treatment heads in order to preserve the epithelium by an appropriate tangential mechanization. 1998: Optimization of the rhythmicity. Throughout LPG’s development and evolution, studies have shown the benefits of the treatment on skin pigmentation and vascularisation, which makes the skin appear more supple while reducing inflammation, itchiness and pain.
LPG and the cutaneous softening of burns By: Dr JP Gavroy, Dr M. Costagliola, Dr Rouge, Dr O. Griffe, Dr L. Teot, Dr F. Ster. Massage has been used for many years to improve the physical properties of scar tissue resulting from burns. Hypertrophic fibrous zones can be softened by direct and gentle movements. The tissue, whose physical properties (slide, elasticity) and look (colour, texture) have been altered, can be modified one to two years after healing through specific technique. Manual techniques are designed to lift the skin off its base using tangential pressure leading to the creation of a cutaneous fold. The LPG device is designed to achieve a skin lift through suction without too much strain on the new epidermis. Our study focused on the effects of this machine on: skin elasticity, skin lift, inflammation, the articular state, which were quantified in clinical studies. They were then paired with an echographic study. We compared the results of these different parameters obtained through: continuous LPG technique, rhythmic LPG technique, traditional manual massage. Results show that the LPG techniques are more efficient than manual massage. Indeed, this method seems more successful than manual massage at mobilizing collagen without harming the surface epithelium. Clinical Assessment: These methods of massage will be
indicated only after one precise and rigorous appreciation of quality of the skin. It will be done by tests simple, comparative and reproducible; the test of vitropression, the test of cutaneous stretching, the test of cutaneous sliding, a measurement of articular amplitudes. Equipment and method: 1. Population - We compared 606 patients. These patients benefited in all other respects from the same treatment: hydration, pressure garment therapy, active and passive mobilization of the cutaneous fold, equipment, and filiform high-pressure showers... 2. Equipment - There are two types of apparatuses of massages: one is mobile (the Cellu M6 Integral) and one has the device integrated to the massage bed (the Cellu M6 Endermolab). They have in common the same technology; a vacuum pump connected by a flexible device to a choice of several interchangeable heads, with different suction levels. These devices are adjustable in their intensity to allow essential safety. The depression of 690 millibars causes suction of the cutaneous plan, the two rollers allow a displacement of the cutaneous fold by decreasing the friction. 3. Method - Passive Fold Rolls; it is used in the beginning of the treatment. The first operations are performed on the circumference of the scar. They are centrifugal in order to drain from the periphery a maximum of the haematic collection. As soon as the skin offers a more important solidity and the test of vitropression increases, we start on the scar, longitudinal, transverse and “star shape” maneuvers... Cutaneous stretch test; the clinical test assesses, cutaneous expandability, adhesion to deep layers... Cutaneous sliding test; it is possible to assess the mobility of the skin in relation to the deep layer as well as skin thickness... Articular recovery; this is controlled by weekly assessments. Measurement machines includes: a goniometer and a tape measure. The amplitudes of the majority of the articulations are taken in degree... Cutaneous strength; cutaneous solidity is appreciated visually by a concerted examination (doctor, nurse, physical therapist): aspect, coloring, detail of scarring... Results: Vitropressure test - Two elements appear: a) After 30 days of massages, LPG rhythmic technique appears definitely less aggressive than the continuous technique; b) Earlier increase in the time of the test with LPG rhythmic technique sign a faster regression of the inflammatory state. We begin the treatment with the LPG rhythmic technique in order to avoid painful phenomena, the hyper-vascularisation and cutaneous aggravations... Skin folding test - This test is improved more quickly with the continuous LPG technique...
Stretching test - The opinion of the six physical therapists and occupational therapists is unanimous: the continuous technique is more effective and used more than the rhythmic technique, the choice is guided by the inflammatory evolution of the skin... Articular assessment - In a general way, the continuous LPG affects articular recovery in 2/3 of the cases... Conclusion: Results of LPG technique used on burns are very encouraging, especially in treating subcutaneous adhesions. In our opinion, the combination of suction, garment therapy massage is a perfect example of effective mechanical treatment of collagen scar tissue.
The four years of use currently enable us to adapt in very precise manner the intensity of the treatment as the inflammatory changes of the scar. The LPG technique is important for a wide range of mechanical proposals: frequency, suction, rhythmicity, diversity of morphology and surface of the suction heads seem perfectly adapted as the chronology of the scar changes To see the whole study, please visit the website of the International Scientific committee of research at : www.cosire-lpg.com.
LPG Technique in burns : Examining 24 years of the technique’s application in burn patients.
Completely reinvented for you ! The new generation of Cellu M6® is the outcome of 24 years of research and expertise in stimulation of the connective tissue.
Therapeutic treatments have never been so effectives.
Expect the unexpected !
For more information, please contact: Les Entreprises Danièle Henkel 9283 Thimens Pierrefonds, Québec, H8Y 0A1 1.877 585 3116 www.danielehenkel.com
Hypertrophy, retractions, adhesions, adherences…
Burns sequels
The most efficient technology for connective tissue
Advertisement
21385A_SkinAllergy_J10:.ps 6/17/2010 6:42 PM Page 21

20 · June 2010 THE CHRONICLE of SKIN & ALLERGYSkin infection research
From the News Resources of The Chronicle
Investigators indicate that a single dose and a seven day daily dose of itra-
conazole can be effective in the treatment of tinea versicolor with extensive
involvement, but single dose appears to be better for improving compliance
and decreasing cost of treatment (Mymensingh Med J 2010 Jan;19(1):72-76).
The aim of this study was to compare the efficacy, safety, tolerability and
cost effectiveness of single dose 400 mg versus seven day 200 mg daily dose
of itraconazole in the treatment of tinea versicolor. A total of 60 patients
(aged 18 to 50 years) were selected for the study during the period of June
2007 to May 2008 in the department of dermatology of three different hospi-
tals in Bangladesh. During the investigation patients were randomly allocat-
ed into two equal groups. The first group, Group A, was given single dose
400 mg itraconazole and the second group, Group B, was given seven day
200 mg daily itraconazole. Overall, 53 (88%) male and seven (12%) female
patients were included in the study. The mean age of group A was 32.37+/-9
years and in group B 33.23+/-8 years. The mean duration of the disease in
group A was 2.63+/-2 months and 2.76+/-2 months in group B. Findings in
group A reveal 22 (73.33%) clinical responders reached cure and five
(16.33%) reached improvement, and in group B 24 (79.99%) reached cure
and four (13.33%) reached improvement. The overall measure at the end
point (EP1) equaled 90% response. The researchers concluded, however,
that the EP clinical analysis showed a 91.66% response.
From the News Resources of The Chronicle
Data published in the Journal of the American Academy of Dermatologysuggest pramiconazole is a well-tolerated and effective treatment for
pityriasis versicolor (2009 Dec; 61(6):971-976).
The aim of this randomized, multicenter, double-blind, placebo-con-
trolled, 28-day, dose-finding study was to assess the efficacy and tolerability
of five doses of pramiconazole relative to placebo. Over the course of the
evaluation, 147 patients were randomized to treatment with placebo or one
of five doses of pramiconazole for three consecutive days. The overall effi-
cacy was based on mycological response, severity of clinical signs and
symptoms, and the Investigator Global Assessment of lesion clearance.
Findings suggest that the most effective treatment regimen in this
study included 200 or 400 mg of pramiconazole taken once, and 200 mg
taken once daily for two or three days. In all, when compared with place-
bo, a significant response (p<0.05) was obtained for all but the lowest
single dose of pramiconazole.
The study authors indicated that a statistically significant (p<0.001)
dose-dependent effect was observed. Additionally, the authors added that
there were no serious, treatment-related adverse events or other safety
concerns. Overall, pramiconazole is considered to be a broad-spectrum
triazole antifungal with potential for oral treatment of pityriasis versicolor,
they concluded.
T i n e a v e r s i c o l o r
Itraconazole effective� Single dose, seven day regimen effective
P i t y r i a s i s v e r s i c o l o r
Pramiconazole useful� 200 or 400 mg single dose called most effective
Skin infection updateSERTACONZOLE NITRATE CREAM2% FOR TX OF TINEA PEDIS Data suggest that sertaconazole
nitrate cream 2% is safe and effec-
tive in the treatment of tinea pedis
interdigitalis (Cutis 2010 Feb;
85(2):107-111).
The objective of this subgroup
analysis was to evaluate the safety
and efficacy of sertaconazole nitrate
cream 2% in participants with tinea
pedis interdigitalis of dermatophyte
origin. A total of 92 participants were
included. The authors indicate the
primary end points were eradication
of the pathogen (confirmed by fun-
gal culture results) and reduction in
total clinical score (TCS) of at least
two points. Secondary end points
included a reduction in signs and
symptoms and reporting of adverse
events (AEs). Findings reveal that
after four weeks of treatment, 88.8%
(79/89) of evaluable participants
achieved success on the primary
end points. Most participants also
demonstrated substantial improve-
ment in signs and symptoms after
four weeks of treatment: 63.7%
(58/91) were free of erythema, 33.0%
(30/91) were free of desquamation,
and 91.2% (83/91) were free of itch.
TREATING COMPLICATED ANDUNCOMPLICATED IMPETICOResearchers indicate that for limited
uncomplicated impetigo, either topi-
cal mupirocin or fusidic acid are as
effective, or even more effective,
than systemic antibiotics (Cutis 2010
Feb; 85(2):65-70).
For extensive or complicated
impetigo, the authors suggest that
systemic antibiotics may be warrant-
ed, but beta-lactam antibiotics
should be avoided if methicillin-
resistant S aureus (MRSA) is suspect-
ed. Investigators also summarized in
their report that Staphylococcus
aureus is the most common overall
cause of impetigo, but
Streptococcus pyogenes remains an
important cause in developing
nations. Community-acquired methi-
cillin-resistant S aureus (CA-MRSA)
poses a challenge because of its
enhanced virulence and increasing
prevalence in children.
MYSTERY TOPICAL TREATMENTFOR TINEA PEDIS SHOWSPROMISE: EUROPEAN JOURNALData appear to indicate that an
unidentified and mysterious new
topical treatment might be effective,
well tolerated, and safe in the treat-
ment of moderate and severe tinea
pedis during active and preventive
stages (J Eur Acad DermatolVenereol; Feb 2010).
During this study, 50 patients
who had tinea pedis were treated in
two stages: the active stage—single
use of the novel topical solution for
45 minutes and novel cream twice
weekly for four weeks, and the pre-
ventive stage—cream application
once weekly for 10 months.
Findings reveal that 45 patients
completed the active stage and
achieved a 76% cure rate. The med-
ication was well tolerated; one
patient dropped out of the study
because of very mild irritation. No
other topical or systemic side effects
were noted. Another five patients
were lost to follow-up during the
preventive stage. The total cure rate
after the preventive stage was deter-
mined to be 70%.
NEEDED: NOVEL METHODS TOLESSEN BACTERIAL RESISTANCEIn a report, scientists suggest that in
light of increasing bacterial drug
resistance, novel agents and/or
modes of bactericidal action are
required (Int J Antimicrob AgentsJuly 2010; 36(1):14-18).
In particular, agents that can act
at multiple sites within the bacterial
cell appear to offer less potential for
the development of resistance. The
authors indicate this effect may be
achieved using combinations of
established drugs. Similar effects
have been reported as a result of
photodynamic antimicrobial action
alone. The photoactivation require-
ment suggests the utility of such
agents in light-accessible presenta-
tions such as skin and soft-tissue
infections. This approach also offers
considerable potential in decreasing
conventional antibacterial use and
allowing the conservation of impor-
tant life-saving systemic agents, the
authors concluded.
21385A_SkinAllergy_J10:.ps 6/17/2010 7:35 PM Page 22
������
������������������ ��������� �� ��������� ��� ����������� ��� ��� ������������������ � �������������� ������ �� �� �� ������ �� �� � �� ���!
���� ���!� ���� ������������ �� � �������� � !� �� �������!� ���� � !���� ���������� �� �� ���������������������� ������� ����� ��������������� �� ������� �� � ��� ���������!������ �������������������! ����������� ����"� "��������� ����������� ���������� ��� ����� ��������� ��� ��������� ������� � �������������� ���������� ����� �������������������� ������������������������� � ������!��������������������� �������������� � �����"��������� ��� �� ��� ������������ ��#������������� ���"� �����!� �� �������� �������� �� �"� "�������"��� ������� ���� � �������� ���� ����������!� ������ ������������ ��!��������!����� ������ $�� ��� ��"��!� ��� ��"��� � ������ ����������� ��� �� � ���������������� ����� �%���� �� ��� �&��������������
��������� � �������'���������"��� ������� ()�������������������������������������� ��
���������������������������!��������������� ��������*���������� �������������������+���������������������� ��� ��� �� ���� ��"��� �� ��� ������ �� ��������������!�����"��� ���������!������� �����!��������� � �����������+� ���������������� �� ���� ��������� ������ ������� ������������� ��������$� �� ������� ������ ��� ����� ���"��� �������� ������ � ���� � ��"���!����� ��������"��������������������������&���!�������� ��������������������������������������������� ���� ��������������(!, ������������ ����� ��� ������� � ������ ����� � ������������ ������ � ��� �������������!� ���� �� ���������� �����������&������������ ����������������� � ����������� $�������!� ������"����������� ����� *��� �������� ������ ��� �� � ��� ���"��� ����� ������ �� ����� ����������� �� ������ ������������� ������ ��"���-
.������!��������!� ���� ������ ���������������� ���� ������ � ���� ���������������������� ���������������� �� ���� ��������������������� ���
������������������������������
�� ���������������������������"���������� �� ��� ��� �������� �� ���(/��������� �� ����� ����� ��� ����������� �����������-(�������,!0
+ � ��� ���� ������ �� ������������� � ������!� ������������ ��� � ���� ���� �� �� �� �� � ������� ����������� ������*��������������� ��
�� �������� ������������������������ ��� �� ��� �� �����!� ���� ��� ������ � �� ������ ��������� ��� � � �!�� �����1$������������������� � � ��� ��������!� �� ����� $1� ����1$$$ � �� ����������&�!������� �����1$$������������������� � ��������&��2������ �� ��� ��� �� ���� � � ������������� �������������������� ��� ���!��� � ����� ��� � �� �� ��� �� ��������������������������������� ����� �� ������ �+������(����� � ����� ������ � ��������� �������������������������������������� �� ��� �� �����!� �� � ��� ��� ������� ������������������ ������� ��������� ��� �� ��� �������� ��� �� �������������������������������������� ���� ���� � ���������� ����� ��� ������� ��� �� ����� ����� ��� �� �������!� ���� ��� ����� ������ �������� ����������������� ����� ������ 3��������� �� �����#��� �� �������� ����� �� ������ ����������� ������� ����������� ��� ��� ����� ���� � ����� ���� � �������� ��� ���������� ��"���� ��������� ���������� ������������� � ���� ���"���!� ��"��� � �������� ���� ��� ���������������� ���������� �!����������� �!� ������ ���������� �����4
�������!���������������� ����51$$$!� �� ������� ��� �����������*���� ��������������6 $�������� ���������������� �������� ���� ����"� ��"������������������������������������������� ��/
2������ � ��� �� �� �� ������� ��������� ��� ���� �����"���� �� �������������������� ��� ������������� �����$1!������!�������������"�� ����� �������������������� ���!� ����� ���������������7 2��� ������� ����� �� ������� �� �����51�������!� ����!� ������������ ������ ���� ��� �"� � ���) 8�� ������!�������� �!� ���������� � ������������� ����!� �� ��������� � �� ��� ������������� �� ������� ������������ �� ���� ���� � ����������������� ������ � � �� ��4 ���� ������������� ��"�� ��� �������� �� �� ������� �� ����� �� �������(��!� �� � ����� ����"��������������������.93��� �.������� ���� (���������������������!������ ���������������� ���!� ���� ���"���� �������� �������� &������ �� ����� "���� �������� � � ������ ������ �1�:2������������
���������������� ����� ����� � ����������!� ����� ��!� � � �� ���� � � �!� ���� �� �� ��������� ��� ��� � ��������� $� ��������� �� ��������������"��� � ����� ������"�� ������ ������� "���� ��� ��� .�"��� � �������� ��� �&����������������������������� � ���� ����!� �� ����� ���������� ��� ���� ���� ���������� �����������( � ���� � ���� ��������������� �� ��� ����� ���� ����� �������*��� ������ ��� �� ������� ����������� ��!� ������� ��� �� ������ ���
��������� ����� ��� � �� ���� ���#���������������� ����������,
�����������3����� ������ ���� ����������������"� �� ���������� ����������� ������������ �� �������� ��& ������������� ��"���� �������������������� �!����� ������� ���������������� �����������!�������������"���� ����������������������������������������3����� ���������� ������ �� �������� ��� �����!� ��� �� �� ���� �������� ��������������������� �� ��� 3�� ����!� ���������� �� ����������� ����!���������������� ���������� ��� �������� ���������� ������������ "�� �� �������� �� ���� �����!����� ��� �������� ��������� �������� ����� ��� � �� ��� ������ ������2:2�(!�1�:2������ �� �����"�������� �������- ���� ��������������������� ��������������������������� �������� ��������������� ������������ �� ��������������!�������� ����� �������������� ��� �������� "���� ��*������������� �������� �� ��������2:2(�������� �������������0 2�����!� �"������������������� ��������������� ����"����������� ��� �� �������������������������� �� �������"�� ���"���� ������ ������ ������������� ������� ���� ���� � *���������������������������� ���� *�������������� ����������� ������� ������������4 $������� �!� ����������������� ������ ������!������ �� � ����!� ���� ������ ��������� �������������������������������!� ������� �������� �� ������ ������ ���"���� ���6
�����������;��������� �����������*���� ������������������������ ������!�����%��������� ��� ����� � � �� ���� ������� �� ���!���������� ���������� ���� �� ��������!� �� �������� �������� � ���������� ����� *����2 ������� �� �� ����� �����"�� � ������������� ���������� ��������������� ���������8������ �� ������� �� �!� � ������� �� ������� �� � ����������� ��� �!����� ����������� �� ��� ��"���� $��������!� � ����"��� ���� ��������� � ���� �� ()� ������� "�����������������������!�������������<�+�"��������� ������� ���� ���� ��� � �� ��� ����� �� ���������������/ +����%���!�� ��������� �� �������������� ���� � ����!� ���� � ���� ����������� ����� �� �������������� �� ����� ��� ������ ������� ������&�����7 ������������ ��������"�����������������"���� ������������ �������!� ������ � �� ������� �� �������� �� �� �� ��� ��� ���%����� $�� �������� �� ��������!� �� ���� ������� � ������� �����!����� ���� �����*��� ��� �� ���������� � ��� �����&� �� �� �� ��������� ���� ��������������� �������()
������������������� ���� �����$=$$$� � ��������&�����������������
���������������������� ���� ����������������
� ����!��" #� $�������%���� $#!���� &
8������&��!�'������>���!������������?�����������<�����������<����� ���!
@�"���������� ����!��� ����!�:�������'������'��� ������� �� � ��� ������������������� � ������ �� ����� �%���� �� ���� ���������� ������������������������������ ������������������������� �� ��������������������������������"��������� ������������� ��� �������������������� ������� ������������!� ��� �������������� � ���� ���"����+����%���� �� ��� �&�!� ��������� �� � ��� �������"���� ������ ��� �� �"����� ��� �������� �� �!� �������� ����"���� �� ���� � �� ����� $�� �� ���������!� ���������������!� ��� ����� �� ��� ����� �������� ������"�� �������������� ���"����� �� ���!������������ �� ��������+ ��� �� �"� "����������������� ����������� ������������������������������������������������� ���������������"�������������������"������� ������� �������� ������������������ �����������������"��� �������������������������� � ���� ���"���� �� ������� �� � ���""� !������������������� �� ���!������������� �������"��!������������������ ���� ����� ������ ���������"�� ������ &� ���� ��������������������������!����� ������������������������������������� �������� ������ ����������������������������� ������!��������������� �����������"������� ��� � ���� �������@������������������ ������� ����������������"����� ���������������������"����������������������������������������������������������"������������������ ���� ������������
�������
'�����������������������A������������� �����������()�)B�,A-�C�()�)��&������ B� �������8���������� �D���A==�������%����� ����=�����=0=�=0
21385A_SkinAllergy_21_24:.ps 6/23/2010 8:45 AM Page 23
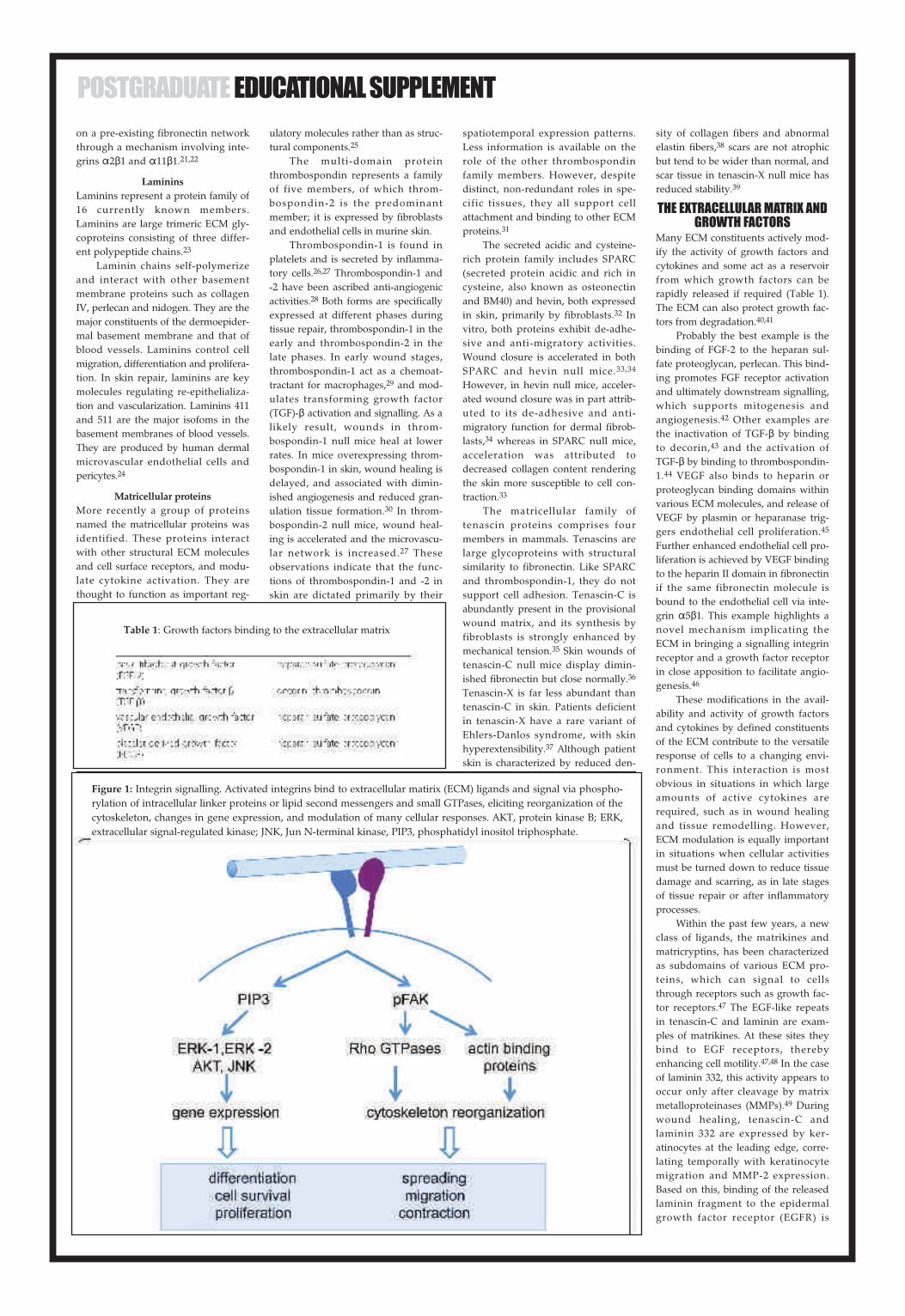
����������� ������������ ����� ���� ������������������������������� ���������������������������
������������������������� ������ �������������� � ������ ��� ������ ��������������������������� ��������!"#��������� ����� ������ ���� ��� ����� �������� �������� ������������$
�������� ������� ������������%����� �� ���� � �� �� � ���� ������� ������������ ����� �������� ��������&'������������������������(�������� ����)������� � ��� ����� ������������������������� �������������� �� ��������������������������� ��� ���� ��������� ������������� �� ����������������� ����� &�� ����� �������� ��������� ����������������� ������ ���� ����� �������%� �����������������%� ��������������*������+������� �����)��� �������� ��� ��������� ����������������������������(���������������������������������������������� ���� ������� ������ ��������� ����*
����� � ��������#���� ����� ��� �� ������������ ���������� ����� �������������� ������������ �������(�������� ����� �� ���� �� ��� ���� � ��� ����� !"#�������������������������������� ��������������� �� �� ������ �� ��� �����(���� ��� ����� � �� ���� ������� ����� �� ����
��� ���������������� ���� �������� ��� ������������� ���+
(��� ��� �������� ��� ��� �������������� �������� �� �� ��������� �������������� ��������� ��������������� ��� ��� ���������� ������,� � � ������������������������ ��������� �����������������������������
(��������������� ��� ������ ����� ��� �������������� �������������� ���� ������� ��- (��������������� �������������������������� ������������� ��� �����. /� ��������������������������������� � ��������� �������������� �������������� ������������������ �������� ���� ��������������� ��� ���� ���������� &�� ������������ � ����� ��������������� �� � ��� �� ������ ��� �� � �����������������0 ���������� ��� ���������������� �� ��� ��1(234� �� ��� ��������������������5���������� ����� �� ������� ��� ������������������������������ � � ������� ���� &������� �������������� ������������������������������������������������� ���� ������� ����� ��������������������������������������������� ���� ������ ����� ����$6 &�� ��������������������������������������������������� ������� ����������������� �� ����� ��� �����������- (����������� ����� ������ �� �� � ��� ���� ����� ��� ��������������� ���� �� ������� ������� � ������������� ��� ����
��� �� �������� ������������ ���������� ������� ���� ��� ���������� ��� ������� ��� ��� � ���� �����������������������������7�������� ����� ���� ��� �� ����������� � ������ ��� ��������� �������� ���� ���� ������ � ����� ������ ������������� ��� ����!"#��� �����$�
(��� ����� ��� ������� ���� ��� ������������ ���� ������� ��������� 895:"1����� ������ ���� ������� ���� ����� ����� ������ ����� ��������� �� ����� ������/#*64�������������� ������������� ������ ���������� ��� ��������� ��$� &��� ���� �� ����� ����� ����� � ����������� ���� �� ������ ���� �� ��� ����;����� �������� ��� �������� ��� ��� �� �895:"� ���� ������ ����� �����$$�$*
7�������� �������������������� �������� ��������������������������� �� ���� ��� �� � �� ����������� ���� �� ������ ���� ���� ���� ����������� ��������� ��$* �������� ��� 895:"������������������� ���� ���� � ���� ��� ����������� ��������� ��� �� � ��������� ��� ���������� ������ ����� �� ����� ��� ��� ����$$
(��� �� ����������� ������� �� �������� ��� ����� ���������� ������������ ������������ (��������� ����������������� ������� �� � ��� ������������ �� �� �������� ���� ����� 895:"���� ���������������� ��������� ������ � ����� ����������(�������"� ��������� ��������� � ��� ���������������������� ���� ���� � �� ��� ������ ����������� �� ��� � ������� ���������������������� �������$+ 8������������� �������"�������������������������������������� ����� ����������������$
(�������<� ��� ���� ����� ������� � ��� �������"� ��� ������ 9� ��� ���������� ��� �������<������ �� ����� ������ � ��!�����=������ ������������ �� ���������� �������� ��$- 5� �������� ��� ����� ��� ������ ���%������ �����������
�� �� ��� ��������� ������� ���� ������������ ��� �������$. ������ ������ � � �������� � ���� ����������� �������������������� ��������� �������<����������������������� ����� ��$0
������������������ ������������������
#����!"#����� � ��� ���� ������������� ��� �� ��� �� ��� ���� �� ��� ���� ����� ����������� ������� � ��� �� ������������������������ �� ��� ���� �������������� ��������� ��� ��>������ 1(����� �4�(���!"#������������� �� ����� ����� ���������������� ����*6�*�
9�������� ��� ��� � ������� ��� ������������� 323�� �� ����������� ����� ����� ��������������������(����������������� ��� 323� ����� ��� �� ��� ��������� ��� ��������� ���������������������� ������ �� �� ��������� ����������������*� ? ���� �������� ��� ��� ���� ��� �������(23� ���������� ����������*$ ���� ��� �� ��� ������(23� ����������� �� ���������������** '!23������ ������ ���������� ����� ��������������������������� �����������!"#��������������������������'!23�������������������������� �������� ���� ������� ����� ��������� ����*+
3�� ����������������� ��������������������� �������������������'!23�������� �� �����������&&������������������� ����� ��� ����� �������� ������������ �������� �� ������� ������������������ �������+����(���� ��������������� �� ����������������� ������� ���� ��!"#���������������������������� ���������� ������������� ����� �������� ����������������� ���� �������� � ���������������*
(������������� ����� ��� ��� ���������� �� ���� �� ��� �� ��� ���� �� ��� ��������� ���������������������� � ��� ���� ���!"#���� ���� �� �� �������� ��������������� ������ �� �� ��������� ���������� �� (���� �� ���� ���� ������ �������� ��� �� �� ����� ��������� ���������� �� ��� �� ���� �� ������� �����>������� ����� ��� �������������������� ������ �������������7�������!"#������� ��������>����������� �� ��� �� �� ���������� ��������� �� ��� ������ ���� ����������� ��������� ���������������������������������� ��� ������� ������ ������� ��� �� ��� �������� �������������
;� ���� ������ ����������������������� ��� ��������� ����� �������� ����� ������ ����� ���� ����� ������ ���%����� ����������� ��� ��������!"#���� ������ ������ ���� ������� �� ����� ������������ ���������������� ����� ��� ����� ����*- (���!23����� ����� ���� �������"� ���� �������� ���� ������������� ���������5 � ����� �� ��� �������� �� !23� ����� ����� ����������������������� ��� ��*-�*. &�� ������������������$$��� ������ ��� ���������� ������� ����� �� ��� �������������� ���� ������� �������� 1##9�4�*0 =����������� ��������� �������"� ����������� $$�� ���� ���������������� ����� ��� � � ��� �������� ������ ������� ���� ������������ ������ ����� ������ ���� ����##9�� ����������/�������� ���������������� ������������������� ������� � �� ��� ������������� �� ��� ��� ����� ��� 1!23:4� ��
������������ ����� �������������
��� ���@�2��� ����� ������������ �� ���� ������������� ��
���������&� ������������������5� ��� ����� ������������ ��� ������������� ����1!"#4����������������������������������� ��������� ��������������������� ������������������������������������������2(9����������� ������������%� ������� ���� ������ ����������������������������������������� ��������������������������������5A(����� �����������/,�!:A�� ����������������������� ���������,�BCA��B���C ����������������9&9$��������� ���������� ��� ��������� ��
Table 1: Growth factors binding to the extracellular matrix
Figure 1: Integrin signalling. Activated integrins bind to extracellular matirix (ECM) ligands and signal via phospho-rylation of intracellular linker proteins or lipid second messengers and small GTPases, eliciting reorganization of thecytoskeleton, changes in gene expression, and modulation of many cellular responses. AKT, protein kinase B; ERK,extracellular signal-regulated kinase; JNK, Jun N-terminal kinase, PIP3, phosphatidyl inositol triphosphate.
21385A_SkinAllergy_21_24:.ps 6/23/2010 8:46 AM Page 24

��������� ���������� �������������������������������������������������������������������������������������������� ���������������� ������ ��������������������� ���������� ���������� ���������������� ��� �� ������������ �����������������������������!"#$������������������ %������� ������� ������������!"#$� ������� ���� ������� ������!"#$����������������&
'������ ������� ����� ���������������� ����������� ��������������� ������� ��� �� (���������� ����������������������������������������� ���� ����!�)���������� ��� ����� ����� ����� ������������ �������� �������������
*�� ��������� ��� ����������������� �� ���!�)� ���� ������������ ����� ����� ����������� ����������������������������������� �� ���������� ����������������� ����� ��� ������������ ���� ������� ������ ������ ���� ��������� +���������������!�)��������������� ������� ��������� ��������� ��� �������,������� ��� ����� ��������������������������������������������� �������� ���� ����,� ������ ���� ��������������� ������ -��� ��������������������.�
������������� �����������������
/����������� �������� ��� !�)������� ����� ����� ����������� ���������� ������� �������� ��������������������� ������������� ���� ��� ����������� ���������� ���������������!�)�� *�������� ����� ����������� ���������� ����� ��� ������������ ���, ��������� �,������������������� �������� �����������0������� ����� � ��� �,����������������� �� ���������� ���� ����������������� ����� ������ ���� ���������������������������*���������������������������������������������������������������������������� ����������� �������� � ������ ����� ����������������������������%������������������������������� ������������������������������������������ �������� �������������������� �������������� ���� ��� � �������������������������1��2
*������� ������� ��� ������� �� ���������� �������� �����������
3�������� ��������� ���� �,�������� ���� ����� �������� ��� ��� �������� ����4������� �������� ���� ��� ��������-������ �� ����������.�������� ��� ����� ���������� +����� ���� �������
������������������������������������������� ����������� ��� ����������� ���������5 /������� ������� �������������������� ���!�)������������� ���������� ��� ����� ���� �����6��7 ���� ������ ������� ��� ����������������������������������� ��������� ��� ��� ���������� �������������������������+����������������� ��� ���������� ��������� �������������� ��$��"+8����������� ���� �������9���� �� �������������������� ��������� �����������������������������-#������&.��:
*������� �,�������� ���� ���������� ��� ��������������� ��� ���������������� ������� ����� ������������� �� ����� �������� �������������� ������������)�� �� �������� �,�������� ��� �� ����� ��� ��������������� ��� ��������� ������� �� ������������������������5�
/��������� ���������� ������� ���� ������������� ������ ������ ���� ���� ������ ������������ ���� ����������� ������� �� ����� ���������������������������������������� ���� ��������� �������������� ���������������� ���� ��������� /������� �+"# � ����� ��������� ��� �� ���,�����������������������%�������������+"# � ������������5���������� ���������� �,�������� ��� ��� �������� �������� ���������� ������ �������������5& �������� �� �� ����������������������������� ���,�� ��������� ��� ���������� �� �������� +"# � ������ ����������+"# � �������� �� ��;����� ���������� ����������+"# � ����������� ���������������������������������51�52
%��������������������7������������ ����� ���� ��� ��� ����� +"# ������,� ��� ����������� �� ���� ��������� ���� ������� �������� ������� �����,� ��������� ����))8�� ��� ������� ��� ������������� ��� �������� ��� ��� ����� �����8������� �������� �� ��� ���������,� ��������� ������� ����������������+"# <�������������������������5�
/����������� ���� ��� ���������� ��� �������� ����������2� ���#"#� ��� ������� ����������� �#"#� �����������5��55 ������� ��� �������������� ������� �����������&����+�� 1� ������� ������� ��������� ��������� ���������� ���������������������� &�56
+����������������������� ��� ������������ ��������� ��������� ��������������� ������������� ��� �������� ���������������������
�����,� ��������������������������� ���������� ���������� +���������������� ���� ����������������� ������ ����� ������� ��� !�)�� ����������� ���� ��������=������� ��������� ���� ��� ����� ���� ���������>������������ �,���� ������������������������������������� �������� �������� ��������������� ��� ���������� ����� ���������������� ���!�)� ��� �� �����,���� ����������� ������ ����� ��� ����������*����������������������������������������������������������� �������������������������������� ����� �������� �������� ���� ��� ����� ������������������������
���� ������������ ����������
/����������� ��� ���������������������� ��� ������� ��������9��� ����������������� ������ ���������� ��� ����������� ���������� ������ ������� ����� ������������������������������������������� ��������������������� �������� �,�������� !�)�#�������������� ����� ��� ����� ���������� ��� ��������������� ��� ������������������������� �������������������� ���������� ��� ���� ������������������� +���� ���� �������������������������������������������������������������� ����� �,���� ����� *�� ������ �������� ���� �������9����!�)���������� ��������������������(�������������������������������������#��������������������������� ����� ������ ����������� ��� ��� ������ ����� �������������������� ������ ������� ������������57�5:
/���� ������������� ���� ��� ��� ���� ����������� �������� �������������������������(�������������� ��������� ������������ ��������� ��������� ������ ������� *� �������� ���� ������� ��� ���� ������� ������������������������� ��� ���������������� ����� ����������� �������������������� ��� ����� �������� ����,��������!�)���������57 +������� ��� �������������������� �������� ��� ����(�������� ��������� ������ ���������������������������(���� ��
�������������� ��������������������������+��� �,��� ������ �� ���������� ���������� ������� ������ ������������������������������������������/����������������������������������������������������������������� ���� ����� ���������� *�� ������������ ��������������������������� ������� ���� ��� �������������������� ��� ��� ������������������������������ �������������������������������������,����������������(������ ��� ������ ���������������6�
�������� �������������� ������������ ��� ��������������� ������ �������������� ������ ������� ��� �������������� ��� ������������� ������������� ��������������� ����������������� ����� ������ ������� ���� ���������������� ��������� ��������� ���!�)�6&�61
)���� ������� ����� ������������������� ������� �� ���������� ����������� ���� ��������� /� �������������������� �� ���������� ��� ����������������������������������� ��� ��� ������ ���������� ��������������������62 +����� ��� ���� ��� ������ ��� ��������� �����������������������������������������������������������������6�
'������� �� ��� �� ��������������������������������������������� ������ ���������� ��� �������� ��� �������� ���������9������ ��������������� ���� �������� ����������������� ������������ �������������������������������� � �� ������ �������������� ���� ���� ����6��65
/������ ���� ������ ��� ������������������ ��� ��������� ������� ����������������������������������� ���� ���� �������������������� *��� ������� ��� ��� �,��� ������,�������� ���� ��������������� ���������� ��������� ��������������� ��� ����� ����������� !�)��� ������������������ ������� ���� ��������������� ������� �������������� �������������������������� ��������������������������-#�����1.�
��������� ����������)������������������������������ ��������������������������������66
+���� ���� ��������� ������������� �������� �������� ���� �������������� ��������� �,������ ������� �� ����������������������������������������-�����������������.��+����������������������������� ��� ���� ������������������������������ �����������!�)�� ���� ����������� ���������������������� �����������)������������������������������������������������������������ ��� ���� ����� ���������� ��� ���������������� ��� �,������� ��� �������� ���
8�����������������������������������9������������������������� �������������+����������� ��������������������������,���������� 4)/�������� ��� ������������������������ ����������������+��������������������9�������,������������! /� ������� ������� �� ����������������������������������������� ����� !�)� ������� ���� ����������67 *������� �� ! /����������� ��� ����� ��(����������������+"# � ��������������������������� ���������� ��� �����,���������� ������������������� ����������� ��� ��������������������������� ����������������6��67 *��������� ��������� ��������� ���� ������ ��� �������� ���������������� ������� � ����� �������� ���� �������� *�� ���� �������+"# ������������������� &����������������������������������������6:
)����������� ������������� ����� �������� ��� ��������������� ����� ���� ���� � !�)� ������ ����������� ������� +���� ������������� ���������������������� ����,������� ���������,� ����������������� ���������������� � ��� ���
������� �����������������������������������������,���������������,-!�).�����������)��������������� ������ ����������� ��������� �������+������������������ ���� ������� ��������������� ��� �����������!�)�����������������������������������������)���������������������������������������� ������������������������!�)��������� ���������������������������������������
Figure 2: Coformation of myofibroblasts and their effects on extracellular matrix(ECM) homeostasis. Myofibroblasts may arise from various cellular sources.Their differentiation and activity are modulated by the surrounding ECM,growth factor activity, and mechanical tension. Myofibroblasts affect connectivetissue homeostasis by upregulated production of ECM proteins, fibrogenicmediators, and protease inhibitors.
21385A_SkinAllergy_21_24:.ps 6/23/2010 8:46 AM Page 25

���������� ����� �������� ������������� ���������� ���� ���������������������������� �� ��!������� ��"��!����� ����� �������� ����������� ��� ���������!��� �� ��� #�$�%��������&��'���������������������!��'� ��!������������� ����"������ �� �������������� �����! ��������������������!������������������&��� ����� ����� ��� ��� �������������� ()*�+
,� ��� ����� ������ �� ���!��&���� ��"���*!������������� �������� �"�"����� �������""��� -��� ��!����������������*������������������������ �� "������� �������� ���.��������� �� ��� "������ �� �����������&�� ������� ��� ������� �� ����������� �� ���� ����� /�������������������������������!���������������� ��������� ��!������������� ��������������������"���������������������� �� � * �������� �� ���������*!������������� "������ ��� ������"������� ��� ��!� �� ��� ����������!"��!�
�������������� ������� ���������� � ��� ������������� �������� ���� �
���� ����� ���� ��"�� ������ ���������������������������������������!������ �������������!!����������������� ��������� ���������� � ��!"��� �����������������*&������"��������������� ���"��������� ������������� ������ �����!��� �� ��� �����!�!������������������""�����
,� ������� �������* �"���������!��������!�� ����������"���� �� �!"������� ���� ������������"!���* ������ !��� �������� ���� ������������������ ��� ��"������� ���������"�!����� ��������* ��� ���!"��* ��'���������"������������� ,����"������ ���&�� ������� ��� �����������������*�"��������������������������"�������� "������� ��� ���"� �!��������!��"������"� 01
���!������������ "�������� �����������"���������!�����������*���"��� �� �!"������ ���� �� ��������������������� ����� %������� ��� "������� ����������"�������� ����� ��������� ��������� ���������� �� �������2���� !������ ������ &����� ���!��������������� �) 3�������� �������
�����������"�������������"�������������������������������� ,���������������!�� ��"���* "�������� ����!����������* ���!�� ��"������ � "�����!�������!��"������������������������
���������������� ������� ��
%��������������� ��������������������� �����* ����������� ���!�������������� ����� ������� ����������� ���!����������!��� ��������������!������ ��� ������� ��������*�4 ��������� ��������2����� �� ��� �����'��������� ��� ����������� �� �"������ �����������!������� ���� ��"������� ,�!������*����* ������* �'�������������* ����������� ��!��������� ��������� ������������ �������2�� �� �������� ����� ��������� ��� ���"������������ �� ��� ���������� ��5�����!���� ,� !��������� ������� ����!����* ����� �������������������"��* ���������� ��� �!"������ ������!��������� ������� ���!����������"��"�������������������������! �6
7��������* � ���������� ���!����������������������!"�����������������*&���� �� �������� ����������� ��!��������� ������� 8���������"�����!����������������������� ���!����� ���������*&�����������������������������!���������������������"���������������� ����� ������� ��� ����� ��!"�����*����� ��������� ��� ��������� ���������� ���!�9�� ���������� ��5������� ���! ����!����� �������� ��� ����������� ����"����*&���� ��������������� ��� �� ���������� �� ���������������� �����'������ ���&��' �:
�������������!�������������������'������:�+��������������������� �����������*&������ ��������� ���"��!����� �������2�� �� ����������+�+*�)�+����++�+������������� ������ �� ����� ����"���� ���� ������ ������� ��"���� ������� "������������� ����������� �� �����������!��� ����"���� ������ )� ���������� ������ ��� �� ����� ����������* ��������� �� ������� ����������!��������� ()*�0
���� ��������* ����������� �������� ���&� �� ��������!���������� ����������* ��&���� ���� ���"�
��!������������������!���"���� % ����� ����������� �� ��� ���������������!����������!������������*�������� ���������� ��� �5����� �!"���������������������������������������&��� ��� ������������������� ���� ������� �(*�� /���� ����������� ��������!�������� ����������* �������� ����"� ������!��������� �����""�����������������!�������������� ������� ��� ������������ ��"�������������������� �1
������ �� ������� �������"������!�������!� ��&�������������������"�������!��!���������� ������� ��� ��� ����� ���������� ����!���� ������� �������������������� ��������* ������ ���������������&��� ���������� ��� ������������!"������* �� ���������� �� �!���;�3���� 1�
%��������������*!������"�������� ������������ ����� ���&��� ����������������&������������������ ,�"���������* ���������� ��!���������������������� �����$�% ��"������������������"��������!����������!��������������������; �� �+
���� �� ��������* ���������� ������������ ������!������������ ����!�����* ������� � �����"��"�����������" % ��!���� ��������� ���" �� ���������� ��� ��� ��������� �� ����������������� ���������������!���������������� ,���������*�; �� ����������� �������*&���� �� ���� ���������������������������������������"����&��� 1+ ,� ��������* ����������� ��������� �� ��� �""�������� �� �������������� ����������� ,�"�������*!���"�������� �����&����������*&������� "������� ���������� ����"���������� ��������&��'��� �������������� ����������*&���� �� ����� �� �������� &��� ���� ������� ������ 4:
<������� �������� ����� ������� ������� �����!������!��������� �������������� ��"������� �� ���������"��������� �� ��� ��������"����������� ��!��������� ������* ����������"������ ���������� ���!���� �� �������������"��!���� 1)*14
��������� ���������!������������!����������������*&����������������������&���������������*�������!����� ��� �� �������� ������* ���!������� ��� ���� ��"������� ����������������!��������������!��������������������������������!��������� ������ ���������������!����������� ��������"����* ������� �������������!�������������������!���;�3������ �������.�������� ���&�� ������ ����������*&���� ���� ���������� ���������"������ ��������� �� ������������.!������������� 8����!���������� �����!�������!�*!��������� �������� ������� �� ���������* ���������������������.!������������"������"�����������2�������������������������� ����"�������* ��&"����������������������"����������� ���������������'����
������ ���������������� ���
,�����������������&�������������������������!"������!������������� �������� ���������� � ����� 4� �����
������� �� ��5�����*"����������� ����������!�������� ����������������������"!���* ������ ��"��� ��� ���������� ����������* ��&���� ���������������������������������������&����������� ��������'&��� ��� ������������������������������������������ ��� �����* ��� �� ��� ��������������������������������"�������!���������� ��� ����������� ���!��������������
��������������������������&�������������������������� ��!���������� ������� ��������� ���� ��������������������� ��� �����!��!���������� ������ ���� ��� ���������������"����������� ���������� �������������������!���������������������������� ���'�� �� ���&�� ������ ������������������!"���!���������������������������'������ ������!"��������"��� �������� ��� �"������ ������"�������"�����!������������!� <������� ������� ���� ��� ����� ��������������"�������* ��� �������������������* �����!����������� ������*��� ����� �����"���&������&�� ��������&��� ���"�� ������������ ������������������ ������ ��������������� ���"������������������ �����������������������������
���������������=� ����' ��� !�!���� �� ���<�"���!��� ��<��!������� �� ���/����������������������� ���$ 8�)1���������������!����������������������������� 7��&��'������������� < ; ������� $ 8 �)1 �� ���/��������� ��������� ��� ��������>?::�.+6
������ ��� �����������������������������������������!"��������������
������������ ������ �������������
������ ������������ � �� ���� � �����������������������������
@ $���������"�������A���������*�������*����������*��������
@ %������������"�������A�����������*�����������*!��������*��!�����
@ 3������������A"�������*���������*��������*�������*��������*��!����
@ �������������"�������A����!���"������*���������*$3%?�.8��6�.�����������
���������� ���� �����������������
@ ���������!�������������,*,,*,,,�
@ �������������������������&����������"�����������,B*B,,*B,C*BB*BB,*BC,�
@ D�����������&��'����!�������������C,,,�
@ 8���!���!�!��������������������������,C*C,,*BC,,*BC,,,�
@ 8����������!������!�������������C,�
@�����!�!���������������B,,,*BC,,*BB,,,*BBC�
@ �����"�������BC*BC,,,�
�������A��������� � ������ �������������������������!"�#$������������������%��������!��������������������������"������������������������ ���������*"�������������������
Figure 3: Interaction of cells with the extracellular matrix (ECM) during dermal repair. This schematic illustrates different types of cell-ECM interac-tions. For details, please refer to the text.
21385A_SkinAllergy_21_24:.ps 6/23/2010 8:46 AM Page 26

21385A_SkinAllergy_J10:.ps 6/17/2010 6:46 PM Page 27

AUTHOR’SCONTRIBUTIONS
BE, RN and TK drafted the manuscript.TK was responsible for its design andcoordination. All authors read andapproved the final manuscript.
REFERENCES1. Bissell MJ, Hall HG, Parry G: How does
the extracellular matrix direct geneexpression? J Theor Biol 1982; 99:31-68.
2. Aszodi A, Legate KR, Nakchbandi I,Fassler R: What mouse mutantsteach us about extracellular matrixfunction. Annu Rev Cell Dev Biol2006; 22:591-621.
3. Myllyharju J, Kivirikko KI: Collagens,modifying enzymes and their muta-tions in humans, flies and worms.Trends Genet 2004; 20:33-43.
4. Schultz GS, Wysocki A: Interactionsbetween extracellular matrix andgrowth factors in wound healing.Wound Repair Regen 2009; 17:153-162.
5. Heino J: The collagen family membersas cell adhesion proteins. Bioessays2007;29:1001-1010.
6. Woodall BP, Nystrom A, Iozzo RA, EbleJA, Niland S, Krieg T, Eckes B, PozziA, Iozzo RV: Integrin alpha2beta1 isthe required receptor for endore-pellin angiostatic activity. J Biol Chem2008; 283:2335-2343.
7. Rehn M, Veikkola T, Kukk-Valdre E,Nakamura H, Ilmonen M, LombardoC, Pihlajaniemi T, Alitalo K, Vuori K:Interaction of endostatin with inte-grins implicated in angiogenesis. ProcNatl Acad Sci USA 2001; 98:1024-1029.
8. Sund M, Hamano Y, Sugimoto H,Sudhakar A, Soubasakos M,Yerramalla U, Benjamin LE, Lawler J,Kieran M, Shah A, Kalluri R:Function of endogenous inhibitors ofangiogenesis as endothelium-specifictumor suppressors. Proc Natl Acad SciUSA 2005; 102:2934-2939.
9. Mundel TM, Kalluri R: Type IV colla-gen-derived angiogenesis inhibitors.Microvasc Res 2007; 74:85-89.
10. Ramchandran R, Dhanabal M, Volk R,Waterman MJ, Segal M, Lu H,Knebelmann B, Sukhatme VP:Antiangiogenic activity of restin,NC10 domain of human collagenXV: comparison to endostatin.Biochem Biophys Res Commun 1999;255:735-739.
11. Nystrom A, Shaik ZP, Gullberg D,Krieg T, Eckes B, Zent R, Pozzi A,Iozzo RV: Role of tyrosine phos-phatase SHP-1 in the mechanism ofendorepellin angiostatic activity.Blood 2009; 114:4897-4906.
12. Kielty CM, Sherratt MJ, ShuttleworthCA: Elastic fibres. J Cell Sci 2002;115:2817-2828.
13. Zheng Q, Choi J, Rouleau L, Leask RL,Richardson JA, Davis EC,Yanagisawa H: Normal wound heal-ing in mice deficient for fibulin-5, anelastin binding protein essential fordermal elastic fiber assembly. J InvestDermatol 2006; 126:2707-2714.
14. Knox SM, Whitelock JM: Perlecan:how does one molecule do so manythings? Cell Mol Life Sci 2006;63:2435-2445.
15. Zhou Z, Wang J, Cao R, Morita H,Soininen R, Chan KM, Liu B, Cao Y,Tryggvason K: Impaired angiogene-sis, delayed wound healing andretarded tumor growth in perlecanheparan sulfate-deficient mice.Cancer Res 2004; 64:4699-4702.
16. Zcharia E, Zilka R, Yaar A, Yacoby-Zeevi O, Zetser A, Metzger S, SaridR, Naggi A, Casu B, Ilan N,
Vlodavsky I, Abramovitch R:Heparanase accelerates woundangiogenesis and wound healing inmouse and rat models. FASEB J 2005;19:211-221.
17. Mast BA, Frantz FW, Diegelmann RF,Krummel TM, Cohen IK: Hyaluronicacid degradation products induceneovascularization and fibroplasia infetal rabbit wounds. Wound RepairRegen 1995; 3:66-72.
18. Muro AF, Chauhan AK, Gajovic S,Iaconcig A, Porro F, Stanta G, BaralleFE: Regulated splicing of thefibronectin EDA exon is essential forproper skin wound healing and nor-mal lifespan. J Cell Biol 2003; 162:149-160.
19. Clark RA: Fibronectin matrix deposi-tion and fibronectin receptor expres-sion in healing and normal skin. JInvest Dermatol 1990; 94:128S-134S.
20. Wierzbicka-Patynowski I,Schwarzbauer JE: The ins and outs offibronectin matrix assembly. J Cell Sci2003; 116:3269-3276.
21. Sottile J, Hocking DC: Fibronectinpolymerization regulates the compo-sition and stability of extracellularmatrix fibrils and cell-matrix adhe-sions. Mol Biol Cell 2002; 13:3546-3559.
22. Velling T, Risteli J, Wennerberg K,Mosher DF, Johansson S:Polymerization of type I and III col-lagens is dependent on fibronectinand enhanced by integrins alpha11beta 1 and alpha 2beta 1. J BiolChem 2002; 277:37377-37381.
23. Aumailley M, Bruckner-Tuderman L,Carter WG, Deutzmann R, Edgar D,Ekblom P, Engel J, Engvall E,Hohenester E, Jones JC, KleinmanHK, Marinkovich MP, Martin GR,Mayer U, Meneguzzi G, Miner JH,Miyazaki K, Patarroyo M, PaulssonM, Quaranta V, Sanes JR, Sasaki T,Sekiguchi K, Sorokin LM, Talts JF,Tryggvason K, Uitto J, Virtanen I,Mark K, Wewer UM, Yamada Y,Yurchenco PD: A simplified lamininnomenclature. Matrix Biol 2005;24:326-332.
24. Hallmann R, Horn N, Selg M,Wendler O, Pausch F, Sorokin LM:Expression and function of lamininsin the embryonic and mature vascu-lature. Physiol Rev 2005; 85:979-1000.
25. Kyriakides TR, Bornstein P:Matricellular proteins as modulatorsof wound healing and the foreignbody response. Thromb Haemost 2003;90:986-992.
26. Bornstein P, Agah A, Kyriakides TR:The role of thrombospondins 1 and 2in the regulation of cell-matrix inter-actions, collagen fibril formation, andthe response to injury. Int J BiochemCell Biol 2004; 36:1115-1125.
27. Agah A, Kyriakides TR, Lawler J,Bornstein P: The lack of throm-bospondin-1 (TSP1) dictates thecourse of wound healing in double-TSP1/TSP2-null mice. Am J Pathol2002; 161:831-839.
28.Armstrong LC, Bornstein P:Thrombospondins 1 and 2 functionas inhibitors of angiogenesis. MatrixBiol 2003; 22:63-71.
29.Mansfield PJ, Suchard SJ:Thrombospondin promotes chemo-taxis and haptotaxis of humanperipheral blood monocytes. JImmunol 1994; 153:4219-4229.
30. Streit M, Velasco P, Riccardi L,Spencer L, Brown LF, Janes L,Lange-Asschenfeldt B, Yano K,Hawighorst T, Iruela-Arispe L,Detmar R: Thrombospondin-1 sup-presses wound healing and granula-
tion tissue formation in the skin oftransgenic mice. EMBO J 2000;19:3272-3282.
31. Adams JC, Lawler J: The throm-bospondins. Int J Biochem Cell Biol2004; 36:961-968.
32. Brekken RA, Sullivan MM, WorkmanG, Bradshaw AD, Carbon J, Siadak A,Murri C, Framson PE, Sage EH:Expression and characterization ofmurine hevin (SC1), a member of theSPARC family of matricellular pro-teins. J Histochem Cytochem 2004;52:735-748.
33. Bradshaw AD, Reed MJ, Sage EH:SPARC-null mice exhibit acceleratedcutaneous wound closure.J HistochemCytochem 2002; 50:1-10.
34. Sullivan MM, Puolakkainen PA,Barker TH, Funk SE, Sage EH:Altered tissue repair in hevin-nullmice: inhibition of fibroblast migra-tion by a matricellular SPARChomolog. Wound Repair Regen 2008;16:310-319.
35. Chiquet-Ehrismann R, Chiquet M:Tenascins: regulation and putativefunctions during pathological stress.JPathol 2003; 200:488-499.
36. Forsberg E, Hirsch E, Frohlich L,Meyer M, Ekblom P, Aszodi A,Werner S, Fassler R: Skin woundsand severed nerves heal normally inmice lacking tenascin-C. Proc NatlAcad Sci USA 1996; 93:6594-6599.
37. Schalkwijk J, Zweers MC, Steijlen PM,Dean WB, Taylor G, van Vlijmen IM,van Haren B, Miller WL, Bristow J: Arecessive form of the Ehlers-Danlossyndrome caused by tenascin-X defi-ciency. N Engl J Med 2001; 345:1167-1175.
38. Mao JR, Taylor G, Dean WB, WagnerDR, Afzal V, Lotz JC, Rubin EM,Bristow J: Tenascin-X deficiencymimics Ehlers-Danlos syndrome inmice through alteration of collagendeposition. Nat Genet 2002; 30:421-425.
39. KirEgging D, van Vlijmen-Willems I,van Tongeren T, Schalkwijk J,Peeters A: Wound healing intenascin-X deficient mice suggeststhat tenascin-X is involved in matrixmaturation rather than matrix depo-sition.Connect Tissue Res 2007; 48:93-98.
40. Flaumenhaft R, Rifkin DB:Extracellular matrix regulation ofgrowth factor and protease activity.Curr Opin Cell Biol 1991; 3:817-823.
41. Hynes RO: The extracellular matrix:not just pretty fibrils. Science 2009;326:1216-1219.
42. Schlessinger J, Plotnikov AN, IbrahimiOA, Eliseenkova AV, Yeh BK, YayonA, Linhardt RJ, Mohammadi M:Crystal structure of a ternary FGF-FGFR-heparin complex reveals adual role for heparin in FGFR bind-ing and dimerization. Mol Cell 2000;6:743-750.
43. Yamaguchi Y, Mann DM, Ruoslahti E:Negative regulation of transforminggrowth factor-beta by the proteogly-can decorin. Nature 1990; 346:281-284.
44. Murphy-Ullrich JE, Poczatek M:Activation of latent TGF-beta bythrombospondin-1: mechanisms andphysiology. Cytokine Growth FactorRev 2000, 11:59-69.
45. Robinson CJ, Stringer SE: The splicevariants of vascular endothelialgrowth factor (VEGF) and theirreceptors. J Cell Sci 2001; 114:853-865.
46. Wijelath ES, Rahman S, Namekata M,Murray J, Nishimura T, Mostafavi-Pour Z, Patel Y, Suda Y, HumphriesMJ, Sobel M: Heparin-II domain of
fibronectin is a vascular endothelialgrowth factor-binding domain:enhancement of VEGF biologicalactivity by a singular growth fac-tor/matrix protein synergism. CircRes 2006; 99:853-860.
47. Tran KT, Lamb P, Deng JS: Matrikinesand matricryptins: Implications forcutaneous cancers and skin repair. JDermatol Sci 2005; 40:11-20.
48. Panayotou G, End P, Aumailley M,Timpl R, Engel J: Domains of lamininwith growth-factor activity. Cell 1989;56:93-101.
49. Giannelli G, Falk-Marzillier J, SchiraldiO, Stetler-Stevenson WG, QuarantaV: Induction of cell migration bymatrix metalloprotease-2 cleavage oflaminin-5. Science 1997; 277:225-228.
50. Tran KT, Griffith L, Wells A:Extracellular matrix signalingthrough growth factor receptors dur-ing wound healing. Wound RepairRegen 2004; 12:262-268.
51. Csordas G, Santra M, Reed CC,Eichstetter I, McQuillan DJ, Gross D,Nugent MA, Hajnoczky G, Iozzo RV:Sustained down-regulation of theepidermal growth factor receptor bydecorin. A mechanism for controllingtumor growth in vivo. J Biol Chem2000; 275:32879-32887.
52. Hynes RO: Integrins: bidirectional,allosteric signaling machines. Cell2002; 110:673-687.
53. Calderwood DA: Integrin activation. JCell Sci 2004; 117(Pt 5):657-666.
54. Askari JA, Buckley PA, Mould AP,Humphries MJ: Linking integrin con-formation to function. J Cell Sci 2009;122:165-170.
55. Moser M, Nieswandt B, Ussar S,Pozgajova M, Fassler R: Kindlin-3 isessential for integrin activation andplatelet aggregation. Nat Med 2008;14:325-330.
56. Tadokoro S, Shattil SJ, Eto K, Tai V,Liddington RC, de Pereda JM,Ginsberg MH, Calderwood DA: Talinbinding to integrin beta tails: a finalcommon step in integrin activation.Science 2003; 302:103-106.
57. Eble JA: The molecular basis of inte-grin-extracellular matrix interactions.Osteoarthritis Cartilage 2001; 9(SupplA):S131-140.
58. Legate KR, Wickstrom SA, Fassler R:Genetic and cell biological analysis ofintegrin outside-in signaling. GenesDev 2009; 23:397-418.
59. Jaffe AB, Hall A: Rho GTPases: bio-chemistry and biology. Annu Rev CellDev Biol 2005; 21:247-269.
60.Watt FM: Role of integrins in regulat-ing epidermal adhesion, growth anddifferentiation. EMBO J 2002;21:3919-3926.
61. Hakkinen L, Koivisto L, Gardner H,Saarialho-Kere U, Carroll JM, LaksoM, Rauvala H, Laato M, Heino J,Larjava H: Increased expression ofbeta6- integrin in skin leads to spon-taneous development of chronicwounds. Am J Pathol 2004; 164:229-242.
62. Munger JS, Huang X, Kawakatsu H,Griffiths MJ, Dalton SL, Wu J, PittetJF, Kaminski N, Garat C, MatthayMA, Rifkin DB, Sheppard D: Theintegrin alpha v beta 6 binds andactivates latent TGF beta 1: a mecha-nism for regulating pulmonaryinflammation and fibrosis. Cell 1999;96:319-328.
63. Annes JP, Chen Y, Munger JS, RifkinDB: Integrin alphaVbeta6-mediatedactivation of latent TGF-beta requiresthe latent TGF-beta binding protein-1. J Cell Biol 2004; 165:723-734.
64. Mu D, Cambier S, Fjellbirkeland L,
POSTGRADUATE EDUCATIONAL SUPPLEMENT
21385A_SkinAllergy_J10:.ps 6/18/2010 8:12 AM Page 28
Prescribing Summary
Patient Selection Criteria
THERAPEUTIC CLASSIFICATION: Topical Acne TherapyINDICATIONS AND CLINICAL USECLINDOXYL Gel (clindamycin phosphate and benzoyl peroxide) is indicated in the topical treatment of moderate acne vulgaris characterised by the presence of comedones, papules and pustules. CLINDOXYL Gel is not indicated for the treatment of cystic acne. CONTRAINDICATIONSCLINDOXYL Gel (clindamycin phosphate and benzoyl peroxide) is contraindicated in individuals with a history of hypersensitivity to preparations containing clindamycin or lincomycin, benzoyl peroxide, or any other component of the preparation, a history of regional enteritis or ulcerative colitis, or a history of antibiotic-associated colitis.
Safety Information
WARNINGSFOR EXTERNAL USE ONLY. NOT FOR OPHTHALMIC USE. Avoid contact with eyes and mucous membranes. In the event of accidental contact with sensitive surfaces (eyes, abraded skin, mucous membranes), bathe with copious amounts of cool tap water.Orally and parenterally administered clindamycin has been associated with severe colitis which may result in patient death. Use of the topical formulation of clindamycin results in absorption of the antibiotic from the skin surface. Diarrhea, bloody diarrhea, and colitis (including pseudomembranous colitis) have been reported with the use of topical and systemic clindamycin.Studies indicate that a toxin(s) produced by clostridia is one primary cause of antibiotic-associated pseudomem-branous colitis. The colitis is usually characterized by severe persistent diarrhea and severe abdominal cramps and may be associated with the passage of blood and mucous. Endoscopic examination may reveal pseu-domembranous colitis. Stool culture for Clostridium difficile and stool assay for C. difficile toxin may be helpful diagnostically. When significant diarrhea occurs, the drug should be discontinued. Large bowel endoscopy should be considered to establish a definitive diagnosis in cases of severe diarrhea.Diarrhea, colitis, and pseudomembranous colitis have been observed to begin up to several weeks following cessation of oral and parenteral therapy with clindamycin.PRECAUTIONSGeneralConcomitant topical acne treatment are not recommended because a possible cumulative irritancy effect may occur, especially with peeling, or abrasive agents. If severe irritation develops, discontinue use and institute appropriate therapy.Use in PregnancyAnimal reproductive studies have not been performed with benzoyl peroxide. Reproductive studies have been performed in rats and mice using subcutaneous and oral doses of clindamycin ranging from 100 to 600 mg/kg/day and have revealed no evidence of impaired fertility or harm to the fetus due to clindamycin.Animal reproduction studies have not been conducted with CLINDOXYL Gel (clindamycin phosphate and benzoyl peroxide). It is not known whether CLINDOXYL Gel can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. CLINDOXYL Gel should not be given to a pregnant woman unless the potential benefits to the mother outweigh the possible risks to the fetus.Use in Nursing MothersIt is not known whether benzoyl peroxide or clindamycin are excreted in human milk following the topical use of CLINDOXYL Gel. However, orally and parenterally administered, clindamycin have been reported to appear in breast milk. Because of the potential for serious adverse reactions in nursing infants, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the potential benefits to the mother and the potential risks to the fetus. Pediatric UseSafety and effectiveness in the pediatric population under the age of 12 have not been established.Drug InteractionsClindamycin has been shown to have neuromuscular blocking properties that may enhance the action of other neuromuscular blocking agents. Therefore, it should be used with caution in patients receiving such agents. Benzoyl peroxide inactivates tretinoin when used concomitantly. ADVERSE REACTIONSIn controlled clinical trials where a total of 172 patients received CLINDOXYL Gel (clindamycin phosphate and benzoyl peroxide), the reported adverse events considered to have a relationship to CLINDOXYL Gel were comprised mainly of reactions at the site of application such as peeling (16.3%), erythema (7.6%), dryness (7.0%), burning (2.3%) and pruritus (1.7%). Mild paraesthesia and worsening of acne were noted in one patient each. Orally and parenterally administered clindamycin has been associated with severe colitis which may end fatally.Cases of diarrhea, bloody diarrhea and colitis (including, rarely, pseudomembranous colitis) have been infrequently reported as adverse reactions in patients treated with topical clindamycin (see WARNINGS). Abdominal pain and gastrointestinal disturbances as well as gram-negative folliculitis have also been reported in association with the use of topical formulations of clindamycin.
To report a serious or unexpected reaction to this drug, you may notify Health Canada by:Toll-free telephone: 866-234-2345Toll-free fax: 866-678-6789E-mail: [email protected] website:http://www.hc-sc.gc.ca/dhp-mps/medeff/index_e.htmlRegular mail: National AR CentreMarketed Health Products Safety and Effectiveness Information DivisionMarketed Health Products DirectorateTunney’s Pasture AL 0701COttawa ON K1A 0K9
Administration
CLINDOXYL Gel (clindamycin phosphate and benzoyl peroxide) should be applied to affected areas once daily before bed time, after the skin has been thoroughly washed, rinsed with warm water and gently patted dry.
Supplemental Product Information SYMPTOMS AND TREATMENT OF OVERDOSAGESymptoms Topically applied clindamycin phosphate formulations can be absorbed in sufficient amounts to produce systemic effects (see WARNINGS). If medication is applied excessively, marked redness and peeling may occur. There are no reports of human ingestion overdosage with CLINDOXYL Gel (clindamycin phosphate and benzoyl peroxide). TreatmentIf ingested orally, no specific antidote is available. Simple gastric lavage should be performed. Treatment should be symptomatic.AVAILABILITY OF DOSAGE FORMSCLINDOXYL Gel (clindamycin phosphate and benzoyl peroxide) is available in a 45 g tube, and a 5 g sample tube.
PRODUCT MONOGRAPH AVAILABLE UPON REQUEST
® Trade-markProtected by patent CA2142530Stiefel Canada Inc.6635 Henri Bourassa WestMontreal, QuebecH4R 1E1
www.stiefel.caSCI/D/09-05/CDXL/1172/PI-E Control No: 089202
clindamycin 1% and benzoyl peroxide 5%Baron JL, Munger JS, KawakatsuH, Sheppard D, Broaddus VC,Nishimura SL: The integrinalpha(v)beta8 mediates epithelialhomeostasis through MT1-MMP-dependent activation of TGF-beta1.J Cell Biol 2002; 157:493-507.
65. Mori S, Wu CY, Yamaji S, Saegusa J,Shi B, Ma Z, Kuwabara Y, Lam KS,Isseroff RR, Takada YK, Takada Y:Direct binding of integrin alphav-beta3 to FGF1 plays a role in FGF1signaling. J Biol Chem 2008;283:18066-18075.
66. Rusnati M, Tanghetti E, Dell'Era P,Gualandris A, Presta M: alphavbe-ta3 integrin mediates the cell-adhe-sive capacity and biological activityof basic fibroblast growth factor(FGF-2) in cultured endothelialcells. Mol Biol Cell 1997; 8:2449-2461.
67. Cascone I, Napione L, Maniero F,Serini G, Bussolino F: Stable inter-action between alpha5beta1 inte-grin and Tie2 tyrosine kinasereceptor regulates endothelial cellresponse to Ang-1. J Cell Biol 2005;170:993-1004.
68. Abraham DJ, Eckes B, Rajkumar V,Krieg T: New developments infibroblast and myofibroblast biolo-gy: implications for fibrosis andscleroderma. Curr Rheumatol Rep2007; 9:136-143.
69. Neilson EG: Mechanisms of disease:Fibroblasts-a new look at an oldproblem. Nat Clin Pract Nephrol2006; 2:101-108.
70. Tomasek JJ, Gabbiani G, Hinz B,Chaponnier C, Brown RA:Myofibroblasts and mechano-regu-lation of connective tissue remodel-ling. Nat Rev Mol Cell Biol 2002;3:349-363.
71. Eckes B, Krieg T: Regulation of con-nective tissue homeostasis in theskin by mechanical forces. Clin ExpRheumatol 2004; 22(3):S73-76.
72. Hinz B: Masters and servants of theforce: the role of matrix adhesionsin myofibroblast force perceptionand transmission. Eur J Cell Biol2006; 85:175-181.
73. Fathke C, Wilson L, Hutter J, KapoorV, Smith A, Hocking A, Isik F:Contribution of bone marrow-derived cells to skin: collagendeposition and wound repair. StemCells 2004; 22:812-822.
74. Hashimoto N, Jin H, Liu T, ChensueSW, Phan SH: Bone marrow-derived progenitor cells in pul-monary fibrosis. J Clin Invest2004;113:243-252.
75. Bucala R, Spiegel LA, Chesney J,Hogan M, Cerami A: Circulatingfibrocytes define a new leukocytesubpopulation that mediates tissuerepair. Mol Med 1994; 1:71-81. Eckeset al: Fibrogenesis & Tissue Repair2010; 3:4.www.fibrogenesis.com/content/3/1/4
76. Strieter RM, Gomperts BN, KeaneMP: The role of CXC chemokinesin pulmonary fibrosis. J Clin Invest2007; 117:549-556.
77. Gabbiani G: The myofibroblast inwound healing and fibrocontrac-tive diseases. J Pathol 2003; 200:500-503.
78. Serini G, Bochaton-Piallat ML,Ropraz P, Geinoz A, Borsi L, ZardiL, Gabbiani G: The fibronectindomain ED-A is crucial for myofi-broblastic phenotype induction bytransforming growth factor-beta1. JCell Biol 1998; 142:873-881.
79. Shephard P, Martin G, Smola-HessS, Brunner G, Krieg T, Smola H:Myofibroblast differentiation isinduced in keratinocyte-fibroblastcocultures and is antagonisticallyregulated by endogenous trans-forming growth factor-beta andinterleukin-1. Am J Pathol 2004;164:2055-2066.
80. Singer II, Kawka DW, Kazazis DM,Clark RA: In vivo co-distribution offibronectin and actin fibers in gran-ulation tissue: immunofluorescenceand electron microscope studies ofthe fibronexus at the myofibroblastsurface. J Cell Biol 1984; 98:2091-2106.
81. Wipff PJ, Rifkin DB, Meister JJ, HinzB: Myofibroblast contraction acti-vates latent TGF-beta1 from theextracellular matrix. J Cell Biol 2007;179:1311-1323.
82. Bondjers C, He L, Takemoto M,Norlin J, Asker N, Hellstrom M,Lindahl P, Betsholtz C: Microarrayanalysis of blood microvessels fromPDGF-B and PDGF-Rbeta mutantmice identifies novel markers forbrain pericytes. FASEB J 2006;20:1703-1705.
83. Shyy JY, Chien S: Role of integrinsin cellular responses to mechanicalstress and adhesion. Curr Opin CellBiol 1997; 9:707-713.
84. Kjaer M: Role of extracellular matrixin adaptation of tendon and skele-tal muscle to mechanical loading.Physiol Rev 2004; 84:649-698.
85. Evans EA, Calderwood DA: Forcesand bond dynamics in cell adhe-sion. Science 2007; 316:1148-1153.
86. Balaban NQ, Schwarz US, RivelineD, Goichberg P, Tzur G, Sabanay I,Mahalu D, Safran S, Bershadsky A,Addadi L, Geiger B: Force and focaladhesion assembly: a close relation-ship studied using elastic micropat-terned substrates. Nat Cell Biol2001; 3:466-472.
87. Even-Ram S, Yamada KM: Cellmigration in 3D matrix. Curr OpinCell Biol 2005; 17:524-532.
88. Ingber DE: Cellular mechanotrans-duction: putting all the piecestogether again. Faseb J 2006; 20:811-827.
89. Grinnell F: Fibroblast biology in three-dimensional collagen matrices. TrendsCell Biol 2003; 13:264-269.
90. Chiquet M, Gelman L, Lutz R, MaierS: From mechanotransduction toextracellular matrix gene expres-sion in fibroblasts. Biochim BiophysActa 2009; 1793:911-920.
91. Lindahl GE, Chambers RC,Papakrivopoulou J, Dawson SJ,Jacobsen MC, Bishop JE, LaurentGJ: Activation of fibroblast procol-lagen alpha 1(I) transcription bymechanical strain is transforminggrowth factor-betadependent andinvolves increased binding ofCCAAT-binding factor (CBF/NF-Y)at the proximal promoter. J BiolChem 2002; 277:6153-6161.
92. Chiquet-Ehrismann R, TannheimerM, Koch M, Brunner A, Spring J,Martin D, Baumgartner S, ChiquetM: Tenascin-C expression byfibroblasts is elevated in stressedcollagen gels. J Cell Biol 1994;127:2093-2101.
93. Yamamoto K, Dang QN, KennedySP, Osathanondh R, Kelly RA, LeeRT: Induction of tenascin-C in car-diac myocytes by mechanicaldeformation. Role of reactive oxy-gen species. J Biol Chem 1999;274:21840-21846.
21385A_SkinAllergy_J10:.ps 6/18/2010 8:12 AM Page 29

the face, mouth and eyes. If facial dermatitis or corticosteroid related adverse effects develop, Xamiol® should be discontinued. There may be a risk of generalised pustular psoriasis or of rebound psoriasis when discontinuing corticosteroids after prolonged periods of use. Patients who apply Xamiol® to exposed skin (e.g. a bald scalp) should avoid both natural and artificial sunlight.
SPECIAL POPULATIONSPregnant Women: Safety for use during pregnancy has not been established. The use of Xamiol® is not recommended in pregnant women.Nursing Women: The safety of calcipotriol and/or topical corticosteroids for use in nursing women has not been established. The use of Xamiol® is not recommended in nursing women. Pediatrics (<18 years of age): There is no clinical trial experience with the use of Xamiol® in children, use is therefore not recommended.
MONITORING AND LABORATORY TESTSIn patients at risk of hypercalcaemia, it is recommended that baseline serum calcium levels be obtained before starting treatment and subsequent monitoring of serum calcium levels at suitable intervals. (see OVERDOSAGE)
ADVERSE REACTIONSApproximately 8% of patients treated with Xamiol® experienced an adverse reaction. Based on data from clinical trials, the most common adverse reaction is pruritus. The following adverse reactions led to discontinuation of the treatment with Xamiol® in 0.1-0.2% of patients: pruritus, skin pain or irritation, dermatitis, eye irritation, rash, burning sensation, face oedema, folliculitis and dry skin. Other adverse reactions were observed for the individual drug substances calcipotriol and betamethasone dipropionate. Systemic effects due to topical use of corticosteroids in adults occur infrequently but can be severe. To report an adverse reaction please notify Health Canada at 1-866-234-2345 or LEO Pharma Inc. at 1-800-263-4218.
DRUG INTERACTIONSThere is no experience of concomitant therapy with other anti psoriatic drugs.
Dosing Considerations
Xamiol® (calcipotriol and betamethasone dipropionate) is not recommended for use in patients below the age of 18 years. Xamiol® is FOR TOPICAL USE ONLY and not for ophthalmic use.Xamiol® should be applied to affected areas of the scalp once daily for up to 4 weeks. After satisfactory improvement has occurred, the drug can be discontinued. If recurrence takes place after discontinuation, treatment may be reinstituted. The maximum daily dose including other calcipotriol-containing products on the body should not exceed 15 g and the maximum weekly dose should not exceed 100 g. If a dose is missed, the patient should apply Xamiol® when remembered, but only once a day and then continue on as usual.
THERAPEUTIC CLASSIFICATIONTopical Antipsoriatic Agent Vitamin D Analogue/Corticosteroid.
INDICATIONS AND CLINICAL USEXamiol® (calcipotriol and betamethasone dipropionate) gel is indicated for the topical treatment of moderate to severe scalp psoriasis for up to 4 weeks.
CONTRAINDICATIONSKnown hypersensitivity to Xamiol® (calcipotriol and betamethasone dipropionate) or any ingredient; ophthalmic use; patients with known disorders of calcium metabolism; viral lesions of the skin; fungal or bacterial skin infections; parasitic infections; skin manifestations in relation to tuberculosis or syphilis; perioral dermatitis, atrophic skin; striae atrophicae; fragility of skin veins; ichthyosis; vulgaris and rosacea acne; rosacea; ulcers and wounds; guttate, erythrodermic, exfoliative and pustular psoriasis; severe renal insufficiency or severe hepatic disorders.
WARNINGS AND PRECAUTIONS
GeneralDue to the content of calcipotriol, hypercalcaemia may occur if the maximum weekly dose (100 g) is exceeded. Serum calcium is quickly normalised when treatment is discontinued. The risk of hypercalcaemia is minimal at recommended dosing.
CarcinogenesisCalcipotriol when used in combination with ultraviolet radiation (UVR) may enhance the known skin carcinogenic effect of UVR.
Endocrine and MetabolismXamiol® contains a potent group III steroid and concurrent treatment with other steroids on the scalp must be avoided. Application on large areas of broken skin or under occlusive dressings should be avoided since it increases systemic absorption of corticosteroids; adverse effects such as adrenocortical suppression with the potential for glucocorticosteroid insufficiency after withdrawal of treatment; manifestations of Cushing’s syndrome, and effects on the metabolic control of diabetes mellitus can also be produced in some patients by systemic absorption of topical corticosteroids.
SkinFacial skin is very sensitive to corticosteroids and Xamiol® is not indicated for use in this area. The patients must wash their hands after each application to avoid accidental transfer to
50 mcg/g calcipotriol (as monohydrate) and 0.5 mg/g betamethasone (as dipropionate) gel
Safety Information
Patient Selection Criteria
Prescribing Summary
Administration
SUPPLEMENTAL PRODUCT INFORMATIONADVERSE REACTIONSTwo pivotal and 4 supporting controlled clinical studies were conducted in scalp psoriasis. The incidence of patients with at least one ADR was lowest in the Xamiol® gel group.
Table 1. Adverse Drug Reactions Occurring in ≥ 1% of Patients for the Pivotal Scalp Studies: safety analysis set
Detailed and/or summarized report
Xamiol® gel(n=1093)
Betamethasone gel
(n=1104)
Calcipotriol gel (n=548)
Gel vehicle (n=135)
Primary System Organ Class1
Preferred Term1
Number of Patients
%Number of Patients
%Number of Patients
%Number of Patients
%
Nervous system disorders
Headache 6 0.5 11 1.0 1 0.2 1 0.7
Burning sensation
2 0.2 6 0.5 10 1.8 0 0.0
Skin and subcutaneous tissue disorders
Pruritus 25 2.3 18 1.6 45 8.2 7 5.2
Skin irritation 5 0.5 5 0.5 15 2.7 3 2.2
Alopecia 4 0.4 6 0.5 3 0.5 2 1.5
Erythema 4 0.4 4 0.4 16 2.9 1 0.7
Dry skin 1 0.1 3 0.3 6 1.1 0 0.0
General disorders and administration site conditions
Pain 1 0.1 0 0.0 3 0.5 3 2.2
1Coded according to MedDRA version 6.1
OVERDOSAGE:Use of Xamiol® (calcipotriol and betamethasone dipropionate) above the recommended dose may cause elevated serum calcium which should rapidly subside when treatment is discontinued. In such cases, it is recommended to monitor serum calcium levels once weekly until they return to normal. Excessive prolonged use of topical corticosteroids may suppress the pituitary-adrenal functions, resulting in secondary adrenal insufficiency which is usually reversible. If this occurs, symptomatic treatment is indicated. In cases of chronic toxicity, treatment with Xamiol® must be discontinued gradually.
® Registered trademark of LEO Pharma A/S used under license by LEO Pharma Inc., Thornhill, ON
Full Product Monograph available on request by contacting LEO Pharma Inc. at 1-800-263-4218
LEO Pharma Inc. Thornhill, Ontario L3T 7W8 www.leo-pharma.com/canada
28 · June 2010 THE CHRONICLE of SKIN & ALLERGY
“Chronic hand eczema is a com-
mon problem and really has a very
high prevalence in daily practice,”
says Dr. Charles Lynde, assistant
clinical professor in the division of
dermatology at the University of
Toronto, and is one of several
Canadian dermatologists who partic-
ipated in the Canadian arm of the
alitretinoin studies leading to
approval of the therapy.
Hand eczema a high unmet needCurrent treatment options, Dr. Lynde
notes, include topical steroids, which
are sometimes useful, and short
courses of oral steroids in severe
cases. Rarely, cyclosporine,
methotrexate, or phototherapy may
also have been utilized.
“Chronic hand eczema is an area
with a high unmet need. Really, the
disease needs a better mouse trap,”
said Dr. Lynde.
In a critical
Phase III trial,
1,032 patients
with severe
chronic hand
eczema, who had
not benefitted
from potent topi-
cal steroids and
who had chronic
hand eczema for an average of nine
years were enrolled in a double-blind,
randomized, placebo-controlled mul-
ticenter trial in Europe and Canada
(Ruzicka, et al: Br J Derm 2008;
158:808-817).
Of the 1,292 patients screened for
enrolment in the study, 260 were not
randomized, 409
were placed in
the 30 mg group,
418 in the 10 mg
group, and 205
were randomized
to the placebo
arm. All patients
were within the
18 to 75 year age
range and all had
chronic hand
eczema refractory to standard treat-
ment for at least six months.
Patients received a daily oral
dose of 10 mg or 30 mg for 12 or 24
weeks, depending upon their
responses which were evaluated
according to the Physician’s Global
Assessment of disease severity
(severe, moderate, mild, almost
clear, and clear).
The modified Total Lesion
Symptom Score (mTLSS) was also
used to measure the intensity of indi-
vidual symptoms of pain, skin red-
ness, breaks in the skin and swelling,
and the time to relapse.
Almost half (48%) of the patients
in the 30 mg arm and more than one-
quarter (28%) were judged by their
physicians to have responded with
clear or almost clear hands; the
response rate among placebo
patients was 17%.
The median reduction in disease
signs and symptoms respectively was
Chronic hand eczema: High prevalence in daily practiceContinued from page 1
Dr. Charles Lynde Dr. Wayne Gulliver
21385A_SkinAllergy_J10:.ps 6/18/2010 8:19 AM Page 30

of the body be treated at a time. Topical corticosteroids should be used with
caution on lesions of the face, groin and axillae as these areas are more
prone to atrophic changes than other areas of the body. If skin atrophy oc-
curs, discontinue treatment. There may be a risk of rebound psoriasis when
discontinuing corticosteroids after prolonged periods of use (see ADVERSE
REACTIONS).
MONITORING AND LABORATORY TESTS
Treatment with Dovobet® in the recommended amounts (See DOSAGE AND
ADMINISTRATION) does not generally result in changes in laboratory values.
In patients using greater than the recommended weekly maximum of 100 g
of Dovobet®, patients at risk of hypercalcemia, and patients with marginally
elevated serum calcium levels, serum calcium should be monitored at suitable
intervals.
MOST COMMON ADVERSE REACTIONS
In clinical trials, the most common adverse reaction associated with Dovobet®
was pruritus. Pruritus was usually mild and no patients were withdrawn from
treatment. Calcipotriol is associated with local reactions such as transient
lesional and perilesional irritation.
Rare cases of hypersensitivity reaction have been reported.
To report an adverse reaction please notify Health Canada at
1-866-234-2345 or LEO Pharma Inc. at 1-800-263-4218.
DRUG INTERACTIONS
There is no experience of concomitant therapy with other antipsoriatic drugs.
Dosing Considerations
Dovobet® is FOR TOPICAL USE ONLY. Not for ophthalmic use. There is no
clinical trial experience with the use of Dovobet® in children.
Recommended Dose and Dosage Adjustment
Dovobet® should be applied topically to the affected areas once daily for up
to 4 weeks. After satisfactory improvement has occurred, the drug can be
discontinued. If recurrence takes place after discontinuation, treatment may
be reinstituted.
The maximum recommended adult dose of Dovobet® ointment is 100 g per
week.
SUPPLEMENTAL PRODUCT INFORMATION
OTHER POTENTIAL ADVERSE REACTIONS
Prolonged use of corticosteroid-containing preparations may produce striae or atrophy of the skin or subcuta-
neous tissues. Topical corticosteroids should be used with caution on lesions of the face, groin and axillae as
these areas are more prone to atrophic changes than other areas of the body. If skin atrophy occurs, discontinue
treatment.
Topical corticosteroids can cause the same spectrum of adverse effects associated with systemic steroid ad-
ministration, including adrenal suppression. Adverse effects associated with topical corticosteroids are generally
local and include: dryness, itching, burning, local irritation, striae, atrophy of the skin or subcutaneous tissues,
telangiectasia, hypertrichosis, folliculitis, skin hypopigmentation, allergic contact dermatitis, maceration of the
skin, miliaria, or secondary infection. If applied to the face, acne rosacea or perioral dermatitis can occur. In addi-
tion, there are reports of the development of pustular psoriasis from chronic plaque psoriasis following reduction
or discontinuation of potent topical corticosteroid products.
SUPPLEMENTAL SAFETY INFORMATION
Carcinogenesis
Calcipotriol when used in combination with ultraviolet radiation (UVR) may enhance the known skin carcinogenic
effect of UVR. (See TOXICOLOGY, Carcinogenicity, in the Product Monograph).
Endocrine and Metabolism
Application on large areas of damaged skin, under occlusive dressings, or in skin folds should be avoided since it
increases systemic absorption of corticosteroids and the risk of adverse effects such as adrenal suppression with
the potential for glucocorticosteroid insufficiency after withdrawal of treatment. Manifestations of Cushing’s syn-
drome, hyperglycaemia and glucosuria can also be produced in some patients by systemic absorption of topical
corticosteroids. Occlusive dressings should not be applied if body temperature is elevated.
All of the adverse effects associated with systemic use of corticosteroids, including adrenal suppression, may
also occur following topical administration of corticosteroid-containing products such as Dovobet®, especially in
children.
Missed Dose
If a dose is missed, the patient should apply Dovobet® as soon as he/she remembers and then continue on
as usual.
Overdosage
Due to the calcipotriol component of DOVOBET (calcipotriol and betamethasone dipropionate), excessive admin-
istration (i.e. more than the recommended weekly amount of 100 g) may cause elevated serum calcium, which
rapidly subsides when treatment is discontinued. In such cases, it is recommended to monitor serum calcium
levels once weekly until they return to normal. Excessive or prolonged use of topical corticosteroids can suppress
THERAPEUTIC CLASSIFICATION
Topical Antipsoriatic Agent Vitamin D Analogue/Corticosteroid
INDICATIONS AND CLINICAL USE
Dovobet® ointment is indicated for the topical treatment of psoriasis vulgaris
for up to 4 weeks. Dovobet® should not be used on the face.
SPECIAL POPULATIONS
Pregnant Women: The safety of calcipotriol and/or topical corticosteroids for
use during pregnancy has not been established. Although studies in experi-
mental animals have not shown teratogenic effects with calcipotriol, studies
with corticosteroids have shown teratogenic effects. The use of Dovobet® is
not recommended in pregnant women.
Nursing Women: The safety of calcipotriol and/or topical corticosteroids for
use in nursing women has not been established. It is not known whether
calcipotriol can be excreted in breast milk or if topical application of corti-
costeroids can lead to sufficient systemic absorption to produce detectable
quantities in breast milk. The use of Dovobet® is not recommended in nursing
women.
Pediatrics (<18 years of age): There is no clinical trial experience with the
use of Dovobet® in children. Children may demonstrate greater susceptibility
to systemic steroid-related adverse effects due to a larger skin surface area
to body weight ratio as compared to adults.
CONTRAINDICATIONS
Known hypersensitivity to any of the ingredients of Dovobet® ointment. NOT
FOR OPHTHALMIC USE. Not for the treatment of viral, fungal or bacterial skin
infections, tuberculosis of the skin, syphilitic skin infections, chicken pox,
eruptions following vaccinations, and in viral diseases such as herpes sim-
plex, varicella and vaccinia.
WARNINGS AND PRECAUTIONS
General
Due to the content of calcipotriol, hypercalcaemia may occur if the maximum
weekly dose (100 g) is exceeded. Serum calcium is quickly normalised when
treatment is discontinued. The risk of hypercalcaemia is minimal when the
recommendations relevant to calcipotriol are followed (see Monitoring and
Laboratory Tests).
The safety of calcipotriol and/or topical corticosteroids for use with children
or pregnant or lactating women has not been established. (See SUPPLE-
MENTAL SAFETY INFORMATION; Special Populations).
Skin
Dovobet® should not be used on the face since this may give rise to itching
and erythema of the facial skin. Patients should be instructed to wash their
hands after each application of Dovobet® in order to avoid inadvertent trans-
fer to the face. Should facial dermatitis develop in spite of these precautions,
Dovobet® therapy should be discontinued.
Prolonged use of corticosteroid-containing preparations may produce striae
or atrophy of the skin or subcutaneous tissues. Therefore, it is recommended
that corticosteroid treatment be interrupted periodically, and that one area
Safety Information
Patient Selection Criteria
Prescribing Summary
Administration
pituitary-adrenal function, resulting in secondary adrenal in-
suffi ciency and manifestations of hypercorticoidism, including
Cushing’s disease. Recovery is usually prompt and complete
upon steroid discontinuation. In cases of chronic toxicity, slow
withdrawal of corticosteroids is recommended.
AVAILABLE DOSAGE FORMS
Dosage Form: Ointment (faintly translucent white to yellow-
ish ointment).
Strength: 50 μg/g calcipotriol and 0.5 mg/g betamethasone
(as dipropionate).
Packaging: Available in 60 g and 120 g lacquered aluminium
tubes (equipped with an aluminium membrane).
Store at 5° to 25°C. For easy application: do not refrigerate
(this is to prevent rubbing and pulling of delicate skin).
Use within 12 months of fi rst opening the tube. Product
monograph available upon request.
For further information, please contact Medical Information at
LEO Pharma Inc. 1-800-263-4218.
® Registered trademark of LEO Pharma A/S used under
license and distributed by LEO Pharma Inc., Thornhill, ON.
LEO Pharma Inc. Thornhill, Ontario L3T 7W8
www.leo-pharma.com/canada
THE CHRONICLE of SKIN & ALLERGY June 2010 · 29
75% for the 30 mg arm and and 56%
for the 10 mg group. Only 32% of
those who responded to the medica-
tion relapsed during the immediate
six months following their treatment
periods, researchers reported. In the
study, relapse was defined as the
recurrence of 75% of the initial signs
and symptoms within 5.6 months to
6.2 months in the absence of anti-
eczema medication.
“Treatment was well tolerated,”
the clinicians reported, “with dose-
dependent adverse effects compris-
ing headache (more common among
the 30 mg group), mucocutaneous
events, hyperlipidemia, and
decreased free thyroxine and thyroid-
stimulating hormone.”
The 117 patients who relapsed
after initially responding to therapy
were subsequently entered into a re-
treatment study; 80% of those patients
from the 30 mg group and 48% of
those patients from the 10 mg group
were deemed by PGAs to have
responded a second time with almost
clear or clear hands (Poster 280,
European Academy of Dermatology
and Venerology, 2007).
Often becomes chronicEczema is the most common der-
matosis affecting hands, with an
annual prevalence estimated
between 7% and 12% in Northern
Europe and perhaps higher in North
America. Irritants, allergens, and
endogenous factors are intertwined
in the etiology of the condition, mak-
ing accurate identification of the true
cause(s) difficult.
Eczema in many patients devel-
ops into a chronic condition of persis-
tent and disfiguring changes in their
hands, and accompanying occupa-
tional, functional, social, and psycho-
logical sequelae.
“Treatment is quite a challenge,”
agrees Dr. Wayne Gulliver, professor
of medicine and dermatology and
chair, discipline of medicine at
Memorial University, St. John’s,
Newfoundland and Labrador, who
was also one of the Canadian
researchers who participated in the
multicenter study, “because we
haven’t had anything new recently
since steroids.
“You go through all the usual
steps, evaluating the patient to make
sure it’s not something else—psoria-
sis, fungus infection—and when
you’ve made the diagnosis the ques-
tion is ‘Is it an allergic type of
eczema?”
Moisturizers, topical steroids, and
topical calcineurin inhibitors are
among the standard agents for mild
cases, he reports, combined with
antibiotics when infections emerge.
Cyclosporine, phototherapy and, in
rare cases, azothioprine are other
treatment options in severe cases.
“[Alitretinoin] looks very promis-
ing as a new therapy,” Dr. Gulliver
says. “If you look at the results both at
12 and at 24 weeks, we’re very happy
with the outcomes.
“The nice thing is that I have
patients from the study who are still
on the drug. Some have been on it for
three years and are continuing.”
Non-proprietary and brand name oftherapy: alitretinoin (Toctino, BasileaPharmaceutica).
21385A_SkinAllergy_J10:.ps 6/18/2010 8:19 AM Page 31
PRESCRIBING SUMMARY
PATIENT SELECTION CRITERIA
INDICATIONS AND CLINICAL USEZYCLARA™ cream is indicated for the topical field (area) treatment of multiple clinically typical visible or palpable actinic keratoses (AKs), whether presenting at the start of therapy or revealed during therapy, of the face or balding scalp in adults.
CONTRAINDICATIONSZYCLARA™ cream is contraindicated in individuals with a history of sensitivity reactions to any of its components. It should be discontinued if hypersensitivity to any of its ingredients is noted.
SPECIAL POPULATIONSPregnant Women: Imiquimod was not teratogenic in rat or rabbit teratology studies. In rats at a high maternally toxic dose (28 times human dose on a mg/m2 basis), reduced pup weights and delayed ossification were observed. However, there are no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nursing Women: It is not known whether topically applied imiquimod is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when ZYCLARA™ cream is administered to nursing women.
Pediatrics (<18 years of age): Actinic keratosis is not a condition generally seen within the pediatric population. Safety and efficacy in patients below the age of 18 years have not been established.
Geriatrics (>65 years of age): Of the 160 subjects treated with ZYCLARA™ cream in the clinical studies, 78 subjects were 65 years or older. No overall differences in safety or effectiveness were observed between these subjects and younger subjects. No other clinical experience has identified differences in responses between the elderly and younger subjects, but greater sensitivity of some older individuals cannot be ruled out.
SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
GeneralThe efficacy of ZYCLARA™ in the prevention of squamous cell carcinoma (SCC) associated with AK has not been established.
Hypersensitivity reactions (urticaria) and erythema multiforme have been reported in patients receiving imiquimod cream. Causality has not been established and no other reports of similar cases have been reported in post-marketing surveillance. ZYCLARA™ cream should be discontinued immediately if these events occur.
The efficacy and safety of ZYCLARA™ cream have not been established for patients with Basal Cell Nevus Syndrome or Xeroderma Pigmentosum.
The safety and efficacy of ZYCLARA™ cream in immunosuppressed patients have not been established.
Local Skin ReactionsIntense local skin reactions including skin weeping or erosion can occur after a few applications of ZYCLARA™ cream and may require an interruption of dosing (see DOSAGE AND ADMINISTRATION and ADVERSE REACTIONS). ZYCLARA™ cream has the potential to exacerbate inflammatory conditions of the skin, including chronic graft versus host disease.
Should a severe local skin reaction occur, the cream should be removed by washing the treatment area with mild soap and water. Treatment with ZYCLARA™ can be resumed after the skin reaction has subsided.
ADVERSE REACTIONSBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adverse reactions occurring in >3% of ZYCLARA™-treated subjects and at a greater frequency than placebo in clinical trials included headache (6.3%), application site pruritus (4.4%), fatigue (4.4%), nausea (3.8%), application site reaction (3.1%), application site pain (3.1%) and pyrexia (3.1%).
The most frequently reported local skin reactions were erythema, flaking/scaling/dryness and scabbing/crusting.
To report any adverse reactions, please contact Graceway Pharma ceuticals at 1-800-328-0255.
ADMINISTRATION
DOSAGE
Recommended Dose and Dosage AdjustmentZYCLARA™ cream (up to 2 packets, 250 mg imiquimod cream per packet) should be applied once daily before bedtime to the skin of the affected treatment field (area) for two treatment cycles of 2 weeks each separated by a 2-week no-treatment period or as directed by physician.
AdministrationBefore applying the cream, the patient should wash the treatment area with mild soap and water and allow the area to dry thoroughly. ZYCLARA™ cream should be applied as a thin film to the entire treatment area and rubbed in until the cream is no longer visible. Up to 2 packets of ZYCLARA™ cream may be applied to the treatment area at each application. ZYCLARA™ cream should be left on the skin for approximately 8 hours, after which time the cream should be removed by washing the area with mild soap and water. The prescriber should demonstrate the proper application technique to maximize the benefit of ZYCLARA™ cream therapy.
Use in or near the eyes, lips and nostrils should be avoided.
Local skin reactions in the treatment area are common (see ADVERSE REACTIONS). A rest period of several days may be taken if required by the patient’s discomfort or severity of the local skin reaction. However, each treatment cycle should not be extended beyond 2 weeks due to missed doses or rest periods. Response to treatment cannot be adequately assessed until resolution of local skin reactions. Lesions that do not respond to treatment should be carefully re-evaluated and management reconsidered. ZYCLARA™ cream is packaged in single-use packets. Partially-used packets should be discarded and not reused. The application site is not to be occluded.
Missed Dose
Each treatment cycle should not be extended beyond 2 weeks due to missed doses or rest periods.
STUDY REFERENCES
1. ZYCLARA™ Product Monograph, Graceway Pharmaceuticals Canada Inc. December 31, 2009.Please refer to Product Monograph.
SUPPLEMENTAL PRODUCT INFORMATION
Therapeutic ClassificationImmune response modifier
WARNINGS AND PRECAUTIONS
GeneralThe efficacy of ZYCLARA™ in the prevention of squamous cell carcinoma (SCC) associated with AK has not been established.
Hypersensitivity reactions (urticaria) and erythema multiforme have been reported in patients receiving imiquimod cream. Causality has not been established. ZYCLARA™ cream should be discontinued immediately if these events occur.
The efficacy and safety of ZYCLARA™ cream have not been established for patients with Basal Cell Nevus Syndrome or Xeroderma Pigmentosum.
The safety and efficacy of ZYCLARA™ cream in immunosuppressed patients have not been established.
Local Skin ReactionsIntense local skin reactions including skin weeping or erosion can occur after a few applications of ZYCLARA™ cream and may require an interruption of dosing (see DOSAGE AND ADMINISTRATION and ADVERSE REACTIONS). ZYCLARA™ cream has the potential to exacerbate inflammatory conditions of the skin, including chronic graft versus host disease.
Local skin reactions such as erythema, scabbing/crusting, flaking/scaling/dryness, and edema are common.
Should a severe local skin reaction occur, the cream should be removed by washing the treatment area with mild soap and water. Treatment with ZYCLARA™ can be resumed after the skin reaction has subsided.
Provocative repeat insult patch test studies involving induction and challenge phases produced no evidence that imiquimod cream causes photoallergenicity or contact sensitization in healthy skin; however, cumulative irritancy testing revealed the potential for imiquimod cream to cause irritation, and application site reactions were reported in clinical studies (see ADVERSE REACTIONS).
Systemic ReactionsFlu-like signs and symptoms may accompany, or even precede, local skin reactions and may include fatigue, nausea, fever, myalgias, arthralgias, and chills. An interruption of dosing and an assessment of the patient should be considered (see ADVERSE REACTIONS).
Ultraviolet Light ExposureExposure to sunlight (including sunlamps) should be avoided or minimized during use of ZYCLARA™ cream because of concern for heightened sunburn susceptibility. Patients should be warned to use protective clothing (e.g., hat) when using ZYCLARA™ cream. Patients with sunburn should be advised not to use ZYCLARA™ cream until fully recovered. Patients who may have considerable sun exposure, e.g., due to their occupation, and those patients with inherent sensitivity to sunlight should exercise caution when using ZYCLARA™ cream. Phototoxicity has not been adequately assessed for ZYCLARA™ cream. The enhancement of ultraviolet carcinogenicity is not necessarily dependent on phototoxic mechanisms. Despite the absence of observed phototoxicity in humans, imiquimod cream shortened the time to skin tumour formation in an animal photoco-carcinogenicity study (see Carcinogenesis, Mutagenesis, Impairment of Fertility). Therefore, it is prudent for patients to minimize or avoid natural or artificial sunlight exposure.
Carcinogenesis and MutagenesisTwo-year bioassays in Wistar rats (up to 3 mg/kg orally per day) and CD-1 mice (up to 4.5 mg/kg applied topically 3 times per week) showed no evidence of a carcinogenic effect in male and female rats and female mice. Liver tumours were increased in male mice exposed to the highest dose concentration, compared to the unexposed controls. However, the number of tumours was within the range seen historically for male CD-1 mice. It is generally accepted that an increase in liver tumours in male mice, in the absence of other neoplastic responses in mice or rats, is not indicative of a carcinogenic risk for humans.
In a photocarcinogenicity study in hairless mice, animals received ZYCLARA™ cream 3 times per week at imiquimod concentrations of 0.03%, 0.1% and 0.3% and were irradiated with solar ultraviolet light for 5 days each week for 40 weeks and observed an additional 12 weeks. Vehicle cream enhanced UVR-induced skin tumour development. ZYCLARA™ cream had no additional effect on tumour development beyond the vehicle effect (i.e., the addition of the active ingredient, imiquimod, to the vehicle cream did not result in an additional effect beyond the vehicle effect on tumour development).
ADVERSE REACTIONSClinical Trial Adverse Drug ReactionsThe data described below reflect exposure to ZYCLARA™ cream or placebo in 319 subjects enrolled in two double-blind, placebo-controlled studies. Subjects applied ZYCLARA™ cream or placebo daily to the skin of the affected area (either the face or balding scalp) for two 2-week treatment cycles separated by a 2-week rest period.
Table 1: Adverse Reactions Occurring in >1% of ZYCLARA™-Treated Subjects and at a Greater Frequency than with Placebo in the Combined Studies
Preferred Term ZYCLARA™ cream, 3.75%(N=160)
placebo(N=159)
Headache 10 (6.3%) 5 (3.1%)
Application site pruritus 7 (4.4%) 1 (0.6%)
Fatigue 7 (4.4%) 0 (0%)
Nausea 6 (3.8%) 2 (1.3%)
Application site irritation 5 (3.1%) 0 (0%)
Application site pain 5 (3.1%) 0 (0%)
Pyrexia 5 (3.1%) 0 (0%)
Anorexia 4 (2.5%) 0 (0%)
Dizziness 4 (2.5%) 0 (0%)
Herpes simplex 4 (2.5%) 1 (0.6%)
Pain 4 (2.5%) 0 (0%)
Chest pain 3 (1.9%) 0 (0%)
Diarrhea 3 (1.9%) 0 (0%)
Lymphadenopathy 3 (1.9%) 0 (0%)
Application site swelling 2 (1.3%) 0 (0%)
Arthralgia 2 (1.3%) 0 (0%)
Blood glucose increased 2 (1.3%) 0 (0%)
Dermatitis 2 (1.3%) 0 (0%)
Food poisoning 2 (1.3%) 0 (0%)
Insomnia 2 (1.3%) 0 (0%)
Seborrhœic keratosis 2 (1.3%) 0 (0%)
Squamous cell carcinoma 2 (1.3%) 1 (0.6%)
Vomiting 2 (1.3%) 1 (0.6%)
Table 2: Application Site Reactions in ZYCLARA™-Treated Subjects as Assessed by the Investigator
Included Term ZYCLARA™ cream, 3.75%*(N=160)
placebo*(N=159)
Any application site reaction 17 (10.6%) 2 (1.3%)
Application site pruritus 7 (4.4%) 1 (0.6%)
Application site irritation 5 (3.1%) 0 (0%)
Application site pain 5 (3.1%) 0 (0%)
Application site swelling 2 (1.3%) 0 (0%)
Application site paraesthesia 1 (0.6%) 1 (0.6%)
Application site scar 1 (0.6%) 0 (0%)
* up to 2 packets daily
Local skin reactions were collected independently of the adverse event “application site reaction” in an effort to provide a better picture of the specific types of local reactions that might be seen. The most frequently reported local skin reactions were erythema, flaking/scaling/dryness, and scabbing/crusting. The prevalence and severity of local skin reactions that occurred during controlled studies are shown in the following table.
Table 3: Local Skin Reactions in the Treatment Area in ZYCLARA™-Treated Subjects as Assessed by the Investigator
Included Term ZYCLARA™ cream, 3.75%(N=160)
placebo(N=159)
All Grades Severe All Grades Severe
Erythema 154 (96.3%) 40 (25.2%) 124 (78.0%) 0 (0.0%)
Edema 120 (75.0%) 9 (5.7%) 31 (19.5%) 0 (0.0%)
Weeping/Exudate 81 (50.6%) 9 (5.7%) 6 (3.8%) 0 (0.0%)
Flaking/Scaling/Dryness 147 (91.9%) 13 (8.2%) 123 (77.4%) 2 (1.3%)
Scabbing/Crusting 149 (93.1%) 22 (13.8%) 72 (45.3%) 0 (0.0%)
Erosion/Ulceration 99 (61.9%) 17 (10.7%) 14 (8.8%) 0 (0.0%)
Other adverse events observed in subjects treated with ZYCLARA™ cream in treatment regimens other than two 2-week treatment cycles include: application site bleeding, cheilitis, chills, herpes zoster, influenza-like illness, lethargy, myalgia, pancytopenia and pruritus.
Post-Market Adverse Drug ReactionsThere is no post-marketing data available for the ZYCLARA™ cream, 3.75% product.
OVERDOSAGEOverdosage of ZYCLARA™ cream in humans is unlikely due to minimal percutaneous absorption. Animal studies reveal a rabbit dermal lethal imiquimod dose of greater than 5000 mg/kg. Persistent topical overdosing of ZYCLARA™ cream could result in an increased incidence of severe local skin reactions and may increase the risk for systemic reactions.
The most clinically serious adverse event reported following multiple oral imiquimod doses of 200 mg was hypotension which resolved following oral or intravenous fluid administration.
See Product Monograph for complete prescribing information.
Full Product Monograph is available at Graceway Pharmaceuticals 252 Pall Mall St., Suite 302 London, Ontario, Canada N6A 5P6
© 2010 Graceway Canada Company London, Ontario N6A 5P6
21385A_SkinAllergy_J10:.ps 6/17/2010 6:50 PM Page 32

THERAPEUTIC CLASSIFICATION:
BIOLOGICAL RESPONSE MODIFIER
INDICATIONS AND CLINICAL USE
HUMIRA® (adalimumab) treatment should be initiated and supervised by
specialist physicians experienced in the diagnosis and treatment of
rheumatoid arthritis (RA), psoriatic arthritis (PsA), ankylosing spondylitis
(AS), Crohn’s disease (CD), or psoriasis (Ps), and familiar with the HUMIRA®
efficacy and safety profile.
HUMIRA® is indicated for:
Rheumatoid Arthritis: reducing the signs and symptoms, inducing major
clinical response and clinical remission, inhibiting the progression of structural
damage and improving physical function in adult patients with moderately to
severely active rheumatoid arthritis. HUMIRA® can be used alone or in combination
with methotrexate (MTX) or other Disease-Modifying Anti-rheumatic Drugs
(DMARDs). When used as first-line treatment in recently diagnosed patients who
have not been previously treated with methotrexate (MTX), HUMIRA® should be
given in combination with MTX. HUMIRA® can be given as monotherapy in case
of intolerance to MTX or when treatment with MTX is contraindicated.
Psoriatic Arthritis: reducing the signs and symptoms of active arthritis and
inhibiting the progression of structural damage and improving the physical
function in adult psoriatic arthritis patients. HUMIRA® can be used in combi-
nation with methotrexate (MTX) in patients who do not respond adequately to
MTX alone.
Ankylosing Spondylitis: reducing signs and symptoms in patients with
active ankylosing spondylitis who have had an inadequate response to
conventional therapy.
Crohn’s Disease: reducing signs and symptoms and inducing and maintaining
clinical remission in adult patients with moderately to severely active Crohn’s
disease who have had an inadequate response to conventional therapy,
including corticosteroids and/or immunosuppressants. HUMIRA® is indicated for
reducing signs and symptoms and inducing clinical remission in these patients if
they have also lost response to or are intolerant to infliximab.
Psoriasis: treatment of adult patients with chronic moderate to severe psoriasis
who are candidates for systemic therapy. For patients with chronic moderate plaque
psoriasis, HUMIRA® should be used after phototherapy has been shown to be
ineffective or inappropriate.
USE IN SPECIAL POPULATIONS
For complete information on special populations, please consult the
supplemental product information section.
Geriatrics (>65 years of age): Evidence from clinical studies and experience
suggests that use of adalimumab in the geriatric population is not associated with
differences in safety or effectiveness. Because there is a higher incidence of
infections and malignancies in the elderly population in general, caution
should be used when treating the elderly. Population pharmacokinetic analyses
in patients with rheumatoid arthritis revealed that there was a trend toward
lower clearance with increasing age in patients aged 40 to >75 years. A brief
discussion can be found under WARNINGS AND PRECAUTIONS; Special
Populations: Geriatrics (>65 years of age).
Pediatrics: Safety and effectiveness in pediatric patients have not been
established.
Pregnant Women: The extent of exposure in pregnancy during clinical trials
is very limited, consisting only of individual cases. There are no adequate and
well-controlled studies in pregnant women. Because animal reproduction and
developmental studies are not always predictive of human response, HUMIRA®
should be used during pregnancy only if clearly needed.
Labor and Delivery: There are no known effects of adalimumab on labor or
delivery.
Nursing Women: It is not known whether adalimumab is excreted in human milk
or absorbed systemically after ingestion. Because many drugs and immuno-
globulins are excreted in human milk, and because of the potential for serious
adverse reactions in nursing infants from adalimumab, a decision should be
made whether to discontinue nursing or to discontinue the drug, taking into
account the importance of the drug to the mother.
Renally and Hepatically Impaired: HUMIRA® has not been studied in these
patient populations.
CONTRAINDICATIONS
•Patients with known hypersensitivity to adalimumab or any of its components.
For a complete listing, see the DOSAGE FORMS, COMPOSITION AND PACK-
AGING section.
•Patients with severe infections such as sepsis, tuberculosis and opportunis-
tic infections (see WARNINGS AND PRECAUTIONS; Serious Warnings and
Precautions: Infections).
WARNINGS AND PRECAUTIONS
For complete information on warnings and precautions, please consult
the supplemental product information section.
Serious Warnings and Precautions:
Infections: SERIOUS INFECTIONS DUE TO BACTERIAL, MYCOBACTERIAL,
INVASIVE FUNGAL (DISSEMINATED OR EXTRAPULMONARY HISTOPLAS-
MOSIS, ASPERGILLOSIS, COCCIDIOIDOMYCOSIS), VIRAL, OR OTHER
OPPORTUNISTIC INFECTIONS HAVE BEEN REPORTED IN PATIENTS
RECEIVING TNF-BLOCKING AGENTS. SEPSIS, RARE CASES OF TUBER-
CULOSIS, CANDIDIASIS, LISTERIOSIS, AND PNEUMOCYSTIS HAVE ALSO
BEEN REPORTED WITH THE USE OF TNF-BLOCKING AGENTS, INCLUDING
HUMIRA® (ADALIMUMAB). OTHER SERIOUS INFECTIONS SEEN IN
CLINICAL TRIALS INCLUDE PNEUMONIA, PYELONEPHRITIS, SEPTIC
ARTHRITIS AND SEPTICEMIA. HOSPITALIZATION OR FATAL OUTCOMES
ASSOCIATED WITH INFECTIONS HAVE BEEN REPORTED. MANY OF THE
SERIOUS INFECTIONS HAVE OCCURRED IN PATIENTS ON CONCOMITANT
IMMUNOSUPPRESSIVE THERAPY THAT, IN ADDITION TO THEIR
UNDERLYING DISEASE, COULD PREDISPOSE THEM TO INFECTIONS.
TREATMENT WITH HUMIRA® SHOULD NOT BE INITIATED IN PATIENTS
WITH ACTIVE INFECTIONS, INCLUDING CHRONIC OR LOCALIZED
INFECTIONS, UNTIL INFECTIONS ARE CONTROLLED. IN PATIENTS WHO
HAVE BEEN EXPOSED TO TUBERCULOSIS, AND PATIENTS WHO HAVE
TRAVELLED IN AREAS OF HIGH RISK OF TUBERCULOSIS OR ENDEMIC
MYCOSES, SUCH AS HISTOPLASMOSIS, COCCIDIOIDOMYCOSIS, OR
BLASTOMYCOSIS, THE RISK AND BENEFITS OF TREATMENT WITH
HUMIRA® SHOULD BE CONSIDERED PRIOR TO INITIATING THERAPY (see
Other Opportunistic Infections). AS WITH OTHER TNF ANTAGONISTS,
PATIENTS SHOULD BE MONITORED CLOSELY FOR INFECTIONS –
INCLUDING TUBERCULOSIS – BEFORE, DURING AND AFTER TREATMENT
WITH HUMIRA®. PATIENTS WHO DEVELOP A NEW INFECTION WHILE
UNDERGOING TREATMENT WITH HUMIRA® SHOULD BE MONITORED
CLOSELY AND UNDERGO A COMPLETE DIAGNOSTIC EVALUATION.
ADMINISTRATION OF HUMIRA® SHOULD BE DISCONTINUED IF A
PATIENT DEVELOPS A SERIOUS INFECTION OR SEPSIS, AND APPROPRI-
ATE ANTIMICROBIAL OR ANTIFUNGAL THERAPY SHOULD BE INITIATED.
PHYSICIANS SHOULD EXERCISE CAUTION WHEN CONSIDERING THE
USE OF HUMIRA® IN PATIENTS WITH A HISTORY OF RECURRENT INFEC-
TION OR WITH UNDERLYING CONDITIONS WHICH MAY PREDISPOSE
THEM TO INFECTIONS, OR PATIENTS WHO HAVE RESIDED IN REGIONS
WHERE TUBERCULOSIS AND HISTOPLASMOSIS ARE ENDEMIC (see
WARNINGS AND PRECAUTIONS; Infections – Tuberculosis and ADVERSE
REACTIONS; Adverse Drug Reaction Overview: Infections). THE
BENEFITS AND RISKS OF TREATMENT WITH HUMIRA® SHOULD BE
CAREFULLY CONSIDERED BEFORE INITIATING THERAPY. Hepatosplenic
T-cell lymphoma: Very rare postmarketing reports of hepatosplenic
T-cell lymphoma (HSTCL), a rare aggressive lymphoma that is often
fatal, have been identified in patients treated with adalimumab. Most
of the patients had prior infliximab therapy as well as concomitant
azathioprine or 6-mercaptopurine use for Crohn’s disease. The causal
association of HSTCL with adalimumab is not clear.
Use with Anakinra: Serious infections were seen in clinical studies with concurrent
use of anakinra (an interleukin-1 antagonist) and another TNF-blocking agent,
etanercept, with no added benefit compared to etanercept alone. Because of the
nature of the adverse events seen with the combination of etanercept and
anakinra, similar toxicities may also result from the combination of anakinra and
other TNF-blocking agents. Therefore, the combination of adalimumab and
anakinra is not recommended (see DRUG INTERACTIONS; Drug-Drug
Interactions).
Malignancies: In the controlled portions of clinical trials of some TNF-blocking
agents, including HUMIRA®, more cases of malignancies have been observed
among patients receiving those TNF blockers compared to control patients. In
the controlled and uncontrolled open-label portions of clinical trials of HUMIRA®,
the more frequently observed malignancies, other than lymphoma and non-
melanoma skin cancer, were breast, colon, prostate, lung, and melanoma. With
current knowledge in this area, a possible risk for development of lymphomas
or other malignancies in patients treated with a TNF antagonist cannot be
excluded. No studies have been conducted that include patients with a history of
malignancy or that continue treatment in patients who develop malignancy while
receiving HUMIRA®. Additional caution should be exercised when considering
HUMIRA® treatment in these patients. All patients, and in particular psoriasis
patients with a medical history of extensive immunosuppressant therapy or
psoriasis patients with a history of Psoralen Ultra Violet A (PUVA) treatment
should be examined for the presence of non-melanoma skin cancer prior to and
during treatment with HUMIRA®.
Hypersensitivity Reactions: Allergic reactions (e.g., allergic rash, anaphylactoid
reaction, fixed drug reaction, non-specified drug reaction, urticaria) have been
observed in approximately 1% of patients receiving HUMIRA® in clinical trials (see
ADVERSE REACTIONS). Serious allergic reactions, including anaphylaxis, have
been reported very rarely following post-marketing HUMIRA® administration.
If an anaphylactic reaction or other serious allergic reactions occur, administration
of adalimumab should be discontinued immediately and appropriate therapy
initiated. The needle cover of the syringe contains dry natural rubber (latex).
This may cause severe allergic reactions in patients sensitive to this substance
(see DOSAGE AND ADMINISTRATION; Administration: Pre-filled Syringe or
Pre-filled Pen).
Carcinogenesis and Mutagenesis: Long-term animal studies of adalimumab
have not been conducted to evaluate the carcinogenic potential or its effect
on fertility.
Immune
Immunosuppression: The possibility exists for TNF-blocking agents, including
HUMIRA®, to affect host defences against infections and malignancies since TNF
mediates inflammation and modulates cellular immune responses. The impact of
treatment with adalimumab on the development and course of malignancies, as
well as active and/or chronic infections, is not fully understood (see WARNINGS
AND PRECAUTIONS and ADVERSE REACTIONS; Adverse Drug Reaction
Overview: Infections and Malignancies).
Immunizations: Patients on HUMIRA® may receive concurrent vaccinations, except
for live vaccines. No data are available on the secondary transmission of infection
by live vaccines in patients receiving HUMIRA®.
Autoimmunity: Treatment with adalimumab may result in the formation of
autoantibodies, and rarely, in the development of a lupus-like syndrome. If a
patient develops symptoms suggestive of a lupus-like syndrome following treat-
ment with adalimumab, treatment should be discontinued (see ADVERSE
REACTIONS; Adverse Drug Reaction Overview: Autoantibodies).
Neurologic Events: Use of TNF-blocking agents, including HUMIRA®, has been
associated with rare cases with new onset or exacerbation of clinical symptoms
and/or radiographic evidence of demyelinating disease, including multiple
sclerosis. Prescribers should exercise caution in considering the use of
adalimumab in patients with preexisting or recent-onset central nervous system
demyelinating disorders.
Infections
Tuberculosis: As observed with other TNF-blocking agents, tuberculosis
(frequently disseminated or extrapulmonary at clinical presentation) associated
with the administration of HUMIRA® in clinical trials has been reported
(see WARNINGS AND PRECAUTIONS; Serious Warnings and Precautions:
Infections). While cases were observed at all doses, the incidence of tuberculosis
reactivations was particularly increased at doses of HUMIRA® that were higher
than the recommended dose. Before initiation of, during and after treatment with
HUMIRA®, patients should be evaluated for active or latent tuberculosis infection
with a tuberculin skin test.Treatment of latent tuberculosis infections should be ini-
tiated prior to therapy with HUMIRA®. When tuberculin skin testing is performed
for latent tuberculosis infection, an induration size of 5 mm or greater should be
considered positive, even if vaccinated previously with Bacille Calmette-Guerin
(BCG). The possibility of undetected latent tuberculosis should be considered
especially in patients who have immigrated from or traveled to countries with
a high prevalence of tuberculosis or who had close contact with a person with
active tuberculosis. If latent infection is diagnosed, appropriate prophylaxis in
accordance with the Canadian Tuberculosis Standards and Centers for
Disease Control and Prevention guidelines should be instituted. Anti-tuberculosis
therapy prior to initiating HUMIRA® should also be considered in patients who have
a negative test for latent tuberculosis but have risk factors for TB infection. The
decision to initiate anti-tuberculosis therapy in these patients should only be made
after taking into account both the risk for latent tuberculosis infection and the risks
of anti-tuberculosis therapy. If necessary, consultation should occur with a
physician with expertise in the treatment of tuberculosis. Active tuberculosis has
developed in patients receiving HUMIRA® whose screening for latent tuberculosis
infection was negative, and some patients who have previously received
treatment for latent or active tuberculosis have developed active tuberculosis
while being treated with TNF-blocking agents. Patients receiving HUMIRA should
be monitored for signs and symptoms of active tuberculosis, particularly because
tests for latent tuberculosis infection may be falsely negative. The risk of false
negative tuberculin skin test results should be considered especially in patients
who are severely ill or immunocompromised. Patients should be instructed to
seek medical advice if signs/symptoms (e.g., persistent cough,wasting/weight loss,
low grade fever) suggestive of a tuberculosis infection occur, and physicians
should monitor for signs and symptoms of active tuberculosis, including patients
who are tuberculosis skin test negative.
Other Opportunistic Infections: Opportunistic infections, including invasive fungal
infections, have been observed in patients receiving HUMIRA®. These infections
are not consistently recognized in patients taking TNF blockers and this has
resulted in delays in appropriate treatment, sometimes resulting in fatal
outcomes. Patients taking TNF blockers are more susceptible to serious
fungal infections such as histoplasmosis, coccidioidomycosis, blastomycosis,
aspergillosis, candidiasis, and other opportunistic infections. Those who develop
fever, malaise, weight loss, sweats, cough, dyspnea, and/or pulmonary infiltrates,
or other serious systemic illness with or without concomitant shock should
promptly seek medical attention for a diagnostic evaluation. For patients who
reside or travel in regions where mycoses are endemic, invasive fungal infections
should be suspected if they develop the signs and symptoms of possible sys-
temic fungal infection. Patients are at risk of histoplasmosis and other invasive
fungal infections and hence clinicians should consider empiric antifungal
treatment until the pathogen(s) are identified. Antigen and antibody testing for
histoplasmosis may be negative in some patients with active infection. When
feasible, the decision to administer empiric antifungal therapy in these patients
should be made in consultation with a physician with expertise in the diagnosis
and treatment of invasive fungal infections and should take into account both the
risk for severe fungal infection and the risks of antifungal therapy. Patients who
develop a severe fungal infection are also advised to stop the TNF blocker until
infections are controlled.
Hepatitis B Virus (HBV) Reactivation: Very rare cases of Hepatitis B virus (HBV)
reactivation have been associated with anti-TNF therapy. Clinically active HBV
infection occurred following a latency period ranging from 3 to 20 months after
initiation of therapy. In the majority of cases, patients were also taking other
immunosuppressive drugs, including methotrexate, azathioprine, and/or
corticosteroids. Hence, establishing a causal relationship to anti-TNF agents is
confounded by the presence of these other medications. Where outcome
information was provided, most patients were reported to have improved after
antiviral treatment and/or discontinuation of the anti-TNF agent. However, fatal
outcomes have also occurred in reported cases. Patients at risk of HBV infection
should be evaluated for prior evidence of HBV infection before initiating anti-TNF
therapy. Those identified as chronic carriers (i.e., surface antigen positive) should
be monitored for signs and symptoms of active HBV infection throughout the
21385A_SkinAllergy_J10:.ps 6/17/2010 6:50 PM Page 33

course of therapy and for several months following discontinuation of therapy.
Reactivation of HBV is not unique to anti-TNF-alpha agents and has been
reported with other immunosuppressive drugs.
Hematologic Events: Rare reports of pancytopenia, including aplastic anemia,
have been reported with TNF-blocking agents. Adverse events of the hematologic
system, including medically significant cytopenia (e.g., thrombocytopenia,
leukopenia) have been infrequently reported with HUMIRA®. The causal
relationship of these reports to HUMIRA® remains unclear. All patients should
be advised to seek immediate medical attention if they develop signs and
symptoms suggestive of blood dyscrasias (e.g., persistent fever, bruising,
bleeding, pallor) while on HUMIRA®. Discontinuation of HUMIRA® therapy
should be considered in patients with confirmed significant hematologic
abnormalities.
Patients with Congestive Heart Failure: Cases of worsening congestive heart
failure (CHF) and new onset CHF have been reported with TNF blockers. Cases of
worsening CHF have also been observed with HUMIRA®. HUMIRA® has not been
formally studied in patients with CHF; however, in clinical trials of another TNF
blocker, a higher rate of serious CHF-related adverse events was observed.
Physicians should exercise caution when using HUMIRA® in patients who have
heart failure and monitor them carefully.
Small Bowel Obstruction: Failure to respond to treatment for Crohn’s
disease may indicate the presence of fixed fibrotic stricture that may
require surgical treatment. Available data suggest that HUMIRA® does not
worsen or cause strictures.
ADVERSE REACTIONS
For complete information on adverse reactions, please consult the
supplemental product information section.
Adverse Drug Reaction Overview
The most serious adverse reactions were (see WARNINGS AND PRECAUTIONS):
• serious infections
•neurologic events
•malignancies
The most common adverse reaction in rheumatoid arthritis patients treated
with HUMIRA® (adalimumab) was injection site reactions. In the 15 controlled
trials for rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn’s
disease, and psoriasis, 14% of patients treated with adalimumab developed
injection site reactions (erythema and/or itching, hemorrhage, pain or swelling),
compared to 8% of patients receiving control treatment. Most injection site
reactions were described as mild and generally did not necessitate drug dis-
continuation. The proportion of rheumatoid arthritis patients who discontinued
treatment due to adverse events during the double-blind, placebo-controlled por-
tion of rheumatoid arthritis Studies RA I, RA II, RA III, and RA IV was 7.0% for
patients taking adalimumab, and 4.0% for placebo-treated patients. The most
common adverse events leading to discontinuation of HUMIRA® were clinical flare
reaction (0.7%), rash (0.3%) and pneumonia (0.3%). Among patients with
rheumatoid arthritis in placebo-controlled studies, deaths occurred in 8 of
1380 (0.58%) HUMIRA®-treated patients compared to 1 of 690 (0.14%)
placebo-treated patients. The rate of deaths in both treatment arms is less
than expected in the normal population with a Standardized Mortality Ratio
(SMR) of 0.87 (0.38, 1.72; 95% CI) in the adalimumab group and 0.25 (0.00,
1.37; 95% CI) in the placebo group. HUMIRA® has also been studied in 542
patients with early rheumatoid arthritis (disease duration less than 3 years)
who were methotrexate (MTX) naïve (Study RA V). No new safety signals
were seen in this patient population compared to the safety profile seen
in HUMIRA® Studies RA I to RA IV. In this study, deaths occurred in 5 of
542 (0.92%) HUMIRA®-treated patients compared to 1 of 257 (0.39%)
methotrexate-treated patients. The rate of deaths in both treatment arms is
less than expected in the normal population with a Standardized Mortality
Ratio of 0.57 (0.18, 1.32; 95% CI) in the adalimumab group and 0.22
(0.00, 1.23; 95% CI) in the methotrexate group. HUMIRA® has also been studied
in 395 patients with psoriatic arthritis in two placebo-controlled studies and in an
open-label extension study, in 393 patients with ankylosing spondylitis in two
placebo-controlled studies and in over 1400 patients with Crohn’s disease in four
placebo-controlled and two open-label extension studies. The safety profile for
patients with psoriatic arthritis treated with HUMIRA® 40 mg every other week was
similar to the safety profile seen in patients with rheumatoid arthritis, HUMIRA®
Studies RA I to RA V. During the controlled period of the psoriatic arthritis studies,
no deaths occurred in the HUMIRA®-treated or placebo-treated patients. During the
psoriatic arthritis open-label study 2 deaths occurred in 382 patients with 795.7
patient-years of exposure. The rate of deaths is less than expected in the normal
population with a Standardized Mortality Ratio (SMR) of 0.39 (0.04, 1.43; 95% CI).
Injection Site Reactions: In the 15 controlled trials, 14% of patients treated
with HUMIRA® developed injection site reactions (erythema and/or itching,
haemorrhage, pain or swelling), compared to 8% of patients receiving placebo
or active control. Injection site reactions generally did not necessitate discon-
tinuation of the medicinal product.
Infections: In the 15 controlled trials for rheumatoid arthritis, psoriatic arthritis,
ankylosing spondylitis, Crohn’s disease, and psoriasis, the rate of infection was 1.56
per patient-year in the adalimumab-treated patients and 1.39 per patient-year in
the control-treated patients. The infections consisted primarily of nasopharyngitis,
upper respiratory tract infection and sinusitis. Most patients continued on HUMIRA®
after the infection resolved. The incidence of serious infections was 0.03 per
patient-year in HUMIRA®-treated patients and 0.03 per patient-year in placebo-
and active control-treated patients. In controlled and open label studies with
HUMIRA®, serious infections (including fatal infections, which occurred rarely)
have been reported, which include reports of tuberculosis (including
miliary and extra-pulmonary locations) and invasive opportunistic infections (e.g.,
disseminated histoplasmosis, pneumocystis carinii pneumonia, aspergillosis and
listeriosis). Most of the cases of tuberculosis occurred within the first 8 months
after initiation of therapy and may reflect recrudescence of latent disease.
Malignancies: More cases of malignancy have been observed in HUMIRA®-treated
patients compared to control-treated patients in clinical trials (see WARNINGS
AND PRECAUTIONS; Malignancies ).
Autoantibodies: Patients had serum samples tested for autoantibodies at multiple
time points in studies RA I to RA V. In those rheumatoid arthritis controlled trials,
11.9% of patients treated with adalimumab and 8.1% of placebo- or active
control-treated patients who had negative baseline antinuclear antibody (ANA)
titers, developed positive titers at Week 24. Two patients out of 3441 treated with
adalimumab developed clinical signs suggestive of new-onset lupus-like
syndrome. The patients improved following discontinuation of therapy.
No patients developed lupus nephritis or central nervous system symptoms.
The impact of long-term treatment with adalimumab on the development
of autoimmune diseases is unknown.
Immunogenicity: Formation of anti-adalimumab antibodies is associated with
increased clearance and reduced efficacy of adalimumab. There is no apparent
correlation between the presence of anti-adalimumab antibodies and adverse
events. Rheumatoid arthritis patients in Studies RA I, RA II, and RA III were
tested at multiple time points for antibodies to adalimumab during the 6- to
12-month period. Approximately 5% (58 of 1062) of adult rheumatoid arthritis
patients receiving adalimumab developed low-titer antibodies to adalimumab
at least once during treatment, which were neutralizing in vitro. Patients treated
with concomitant methotrexate (MTX) had a lower rate of antibody development
than patients on adalimumab monotherapy (1% versus 12%). With monotherapy,
patients receiving every-other-week dosing may develop antibodies more
frequently than those receiving weekly dosing. In patients receiving the recom-
mended dosage of 40 mg every other week as monotherapy, the ACR 20
response was lower among antibody-positive patients than among antibody-
negative patients. The immunogenicity of adalimumab long term is unknown.
In patients with psoriatic arthritis, adalimumab antibodies were identified in
38/376 subjects (10%) treated with adalimumab. In patients not given con-
comitant methotrexate, the incidence was 13.5% (24/178 subjects), compared
to 7% (14 of 198 subjects) when adalimumab was used as add-on to methotrex-
ate. In patients with ankylosing spondylitis, antibodies were identified in 17/204
subjects (8.3%) treated with adalimumab. In patients not given concomitant
methotrexate, the incidence was 16/185 (8.6%), compared to 1/19 (5.3%) when
adalimumab was used as add-on to methotrexate. In patients with Crohn’s
disease, adalimumab antibodies were identified in 2.6% (7 of 269) of patients
receiving adalimumab. In patients with psoriasis, anti-adalimumab
antibodies were identified in 77/920 subjects (8.4%) treated with adalimumab
monotherapy. The data reflect the percentage of patients whose test results were
considered positive for antibodies to adalimumab in an ELISA assay, and are
highly dependent on the sensitivity and specificity of the assay. Additionally,
the observed incidence of antibody positivity in an assay may be influenced by
several factors including sample handling, timing of sample collection,
concomitant medications, and underlying disease. For these reasons, comparison
of the incidence of antibodies to adalimumab with the incidence of antibodies to
other products may be misleading.
Post-Market Adverse Drug Reactions: The following post-market adverse
drug reactions have been rarely reported:
Hematologic Events: Thrombocytopenia (see WARNINGS AND PRECAUTIONS;
Hematologic Events).
Hypersensitivity Reactions: Anaphylaxis and angioneurotic edema (see WARNINGS
AND PRECAUTIONS; Hypersensitivity Reactions).
Skin Reactions: Cutaneous vasculitis, Stevens Johnson Syndrome, erythema
multiforme, new onset or worsening of psoriasis (including palmoplantar
pustular psoriasis).
Respiratory Disorders: Interstitial lung disease, including pulmonary fibrosis.
Infections: Reactivation of hepatitis B virus (HBV).
Gastrointestinal Disorders: Intestinal perforation.
Nervous System Disorders: Guillain-Barré syndrome.
Neoplasia: Hepatosplenic T-cell lymphoma.
DRUG INTERACTIONS
For complete information on drug interactions, please consult the
supplemental product information section.
Serious Drug Interactions: SERIOUS INFECTIONS AND SEPSIS, INCLUDING
FATALITIES, HAVE BEEN REPORTED WITH THE USE OF TNF-BLOCKING
AGENTS, INCLUDING HUMIRA® (ADALIMUMAB). MANY OF THE SERIOUS
INFECTIONS HAVE OCCURRED IN PATIENTS ON CONCOMITANT IMMUNO-
SUPPRESSIVE THERAPY THAT, IN ADDITION TO THEIR RHEUMATOID
ARTHRITIS, COULD PREDISPOSE THEM TO INFECTIONS. TUBERCULOSIS
AND INVASIVE OPPORTUNISTIC FUNGAL INFECTIONS HAVE BEEN
OBSERVED IN PATIENTS TREATED WITH TNF-BLOCKING AGENTS,
INCLUDING ADALIMUMAB.
Overview: Population pharmacokinetic analyses with data from over 1200
rheumatoid arthritis (RA) patients revealed that co-administration of methotrex-
ate (MTX) had an intrinsic effect on the apparent clearance of adalimumab
(CL/F) (see DRUG INTERACTIONS; Drug-Drug Interactions). As expected,
there was a trend toward higher apparent clearance of adalimumab with
increasing body weight and in the presence of anti-adalimumab antibodies.
Other more minor factors were also identified: higher apparent clearance was
predicted in RA patients receiving doses lower than the recommended dose,
and in RA patients with high rheumatoid factor or CRP concentrations. These
factors are not likely to be clinically important. Adalimumab has been studied in
rheumatoid arthritis patients taking concomitant MTX. The data do not suggest
the need for dose adjustment of either adalimumab or methotrexate.
Drug-Drug Interactions
Methotrexate (MTX): When adalimumab was administered to 21 rheumatoid
arthritis patients on stable MTX therapy, there were no statistically significant
changes in the serum MTX concentration profiles. In contrast, after single and
multiple dosing, MTX reduced adalimumab apparent clearances by 29% and
44% respectively, in patients with rheumatoid arthritis.
Anakinra: Concurrent administration of anakinra (an interleukin-1 antagonist) and
another TNF-blocking agent has been associated with an increased risk of serious
infections, an increased risk of neutropenia and no additional benefit compared
to these medicinal products alone. Therefore, the combination of anakinra with
other TNF-blocking agents, including HUMIRA®, may also result in similar toxicities
(see WARNINGS AND PRECAUTIONS; Use with Anakinra).
Abatacept: Concurrent administration of TNF antagonists and abatacept has
been associated with an increased risk of infections including serious infections
compared to TNF antagonists alone. This combination has not demonstrated
increased clinical benefit. Thus the combined use of TNF antagonists and abata-
cept is not recommended.
Other: Interactions between HUMIRA® and drugs other than methotrexate (MTX)
have not been evaluated in formal pharmacokinetic studies. In rheumatoid arthritis
clinical trials where HUMIRA® was co-administered with commonly-used DMARDs
(sulfasalazine, hydrochloroquine, leflunomide and parenteral gold), glucocorticoids,
salicylates, nonsteroidal anti-inflammatory drugs or analgesics, no safety signals
were seen. There is no data on other DMARDs, and patients with prior treatment
with alkylating agents (e.g., cyclophosphamide) were excluded.
To report suspected side effects:
Abbott Laboratories, Limited
P.O. Box 6150, Station Centre-ville
Montréal (Québec) H3C 3K6
Tel.: 1 800 361-7852
DOSAGE AND ADMINISTRATION
Dosing Considerations
Hepatic and Renal Insufficiency: No pharmacokinetic data are available in
patients with hepatic or renal impairment. No dose recommendation can
be made.
Race: No differences in immunoglobulin clearance would be expected among
races. From limited data in non-Caucasians, no important kinetic differences
were observed for adalimumab. Dosage adjustment is not required.
Recommended Dose and Dosage
Adjustment
Rheumatoid Arthritis: The recommended dose of HUMIRA® (adalimumab) for
adult patients with rheumatoid arthritis (RA) is 40 mg administered every other
week as a subcutaneous (s.c.) injection.
Psoriatic Arthritis: The recommended dose of HUMIRA® (adalimumab) for adult
patients with psoriatic arthritis (PsA) is 40 mg administered every other week
as a subcutaneous (s.c.) injection. For the RA and PsA indications, available
data suggest that the clinical response is usually achieved within 12 weeks of
treatment. Continued therapy should be carefully reconsidered in a patient not
responding within this time period.
Ankylosing Spondylitis: The recommended dose of HUMIRA® (adalimumab) for
patients with ankylosing spondylitis (AS) is 40 mg adalimumab administered every
other week as a single dose via subcutaneous (s.c.) injection. Glucocorticoids,
salicylates, nonsteroidal anti-inflammatory drugs, analgesics or disease-modifying
anti-rheumatic drugs can be continued during treatment with HUMIRA®.
Crohn’s Disease: The recommended HUMIRA® (adalimumab) induction dose
regimen for adult patients with Crohn’s disease is 160 mg at Week 0 [dose can
be administered as four subcutaneous (s.c.) injections in one day or as two sub-
cutaneous (s.c.) injections per day for two consecutive days], followed by 80
mg at Week 2. The recommended HUMIRA® maintenance dose regimen for
adult patients with Crohn’s disease is 40 mg every other week beginning at
Week 4. During treatment with HUMIRA®, other concomitant therapies (e.g.,
corticosteroids and/or immunomodulatory agents) should be optimized. For
patients who experience a disease flare, dose escalation may be considered.
Some patients who have not responded by Week 4 (induction period) may
benefit from continued maintenance therapy through Week 12. Available data
suggest that the clinical response is usually achieved at Week 4 of treatment.
Continued therapy should be carefully reconsidered in a patient not respond-
ing within this time period. The use of HUMIRA® in Crohn’s disease beyond
one year has not been evaluated in controlled clinical studies.
Psoriasis: The recommended dose of HUMIRA® (adalimumab) for adult patients
with psoriasis (Ps) is an initial dose of 80 mg administered subcutaneously,
followed by 40 mg subcutaneously given every other week starting one week
after the initial dose. Continued therapy beyond 16 weeks should be carefully
reconsidered in a patient not responding within this time period.
Administration
Administration of HUMIRA® (adalimumab) Subcutaneous Injection: HUMIRA® is
intended for use under the guidance and supervision of a physician. Patients may
self-inject HUMIRA® if their physician determines that it is appropriate and with
medical follow-up, as necessary, after proper training in subcutaneous injection
technique. Methotrexate (MTX), glucocorticoids, salicylates, nonsteroidal anti-
inflammatory drugs (NSAIDs), analgesics or other DMARDs may be continued
during treatment with adalimumab. When treated with HUMIRA® as monotherapy,
some rheumatoid arthritis patients who experience a decrease in their response to
HUMIRA® 40 mg every other week, may benefit from an increase in dose intensity
to 40 mg HUMIRA® every week.
Pre-filled Syringe or Pre-filled Pen: The solution in the syringe or pen should be
carefully inspected visually for particulate matter and discolouration prior to
subcutaneous administration. If particulates and discolourations are noted, the
product should not be used. HUMIRA® does not contain preservatives; therefore,
unused portions of drug remaining in the syringe should be discarded.
NOTE: The needle cover of the syringe contains a dry natural rubber (latex),
which should not be handled by persons sensitive to this substance. Patients
using the pre-filled syringes should be instructed to inject the full amount in
the syringe (0.8 mL), which provides 40 mg of HUMIRA®. Injection sites should
be rotated and injections should never be given into areas where the skin is
tender, bruised, red or hard.
1. Menter A, Tyring SK, Gordon K et al. Adalimumab therapy for moderate to
severe psoriasis: A randomized, controlled phase III trial. J Am Acad
Dermatol 2008;58:106-15. [A 52-week, double-blind, placebo-controlled
study (REVEAL) in 1,212 patients with moderate to severe chronic plaque
psoriasis (≥10% BSA involvement, PASI ≥12 and a PGA of at least
moderate severity at baseline). Patients were randomized to HUMIRA
(80 mg at week 0, then 40 mg every two weeks at week 1) or placebo.
Patients were treated continuously with HUMIRA 40 mg every two weeks
from week 17 through 33. At week 33, all PASI 75 responders were
randomized to continue HUMIRA or switch to placebo.]
21385A_SkinAllergy_J10:.ps 6/17/2010 6:51 PM Page 18

2. Saurat J-H, Stingl G, Dubertret L et al. Efficacy and safety results from the
randomized controlled comparative study of adalimumab vs. methotrexate
vs. placebo in patients with psoriasis (CHAMPION). Br J Dermatol
2008;158(3):558-66. [A 16-week, randomized, double-blind, double-
dummy, multicentre, placebo- and active-controlled study in subjects with
moderate to severe plaque psoriasis (PASI ≥10, BSA ≥10%).]
3. Data on file. Abbott Laboratories, Limited.
4. Data on file. Abbott Laboratories, Limited.
5. HUMIRA Product Monograph. Abbott Laboratories, Limited,
December 16, 2009.
B. Supplemental Product InformationWARNINGS AND PRECAUTIONS
Malignancies:
Lymphoma
In the controlled portions of clinical trials of all the TNF-blocking agents, more cases of lymphoma have been observed
among patients receiving TNF blockers compared to control patients. However, for HUMIRA®, the occurrence of
lymphoma was rare, and the follow-up period of placebo patients was shorter than for patients receiving TNF-
antagonist therapy. The size of the control group and limited duration of the controlled portions of studies precludes
the ability to draw fiirm conclusions. Furthermore, there is an increased background lymphoma risk in rheumatoid
arthritis patients with long-standing, highly active, infllammatory disease, which complicates the risk estimation.
In combining the controlled and uncontrolled open-label portions of these clinical trials with a median duration of
approximately 1.7 years, including 6539 patients and over 16,000 patient-years of therapy, the observed rate of
lymphomas is approximately 0.11/100 patient-years. This is approximately 3.0-fold higher than expected in the
general population. During the long-term open-label trials with HUMIRA®, the overall standard incidence ratio (SIR) of
malignancies was 0.99 (95% CI; 0.81-1.20).
Non-lymphoma Malignancy: During the controlled portions of HUMIRA® trials in patients with rheumatoid arthritis,
psoriatic arthritis, ankylosing spondylitis, Crohn’s disease, and psoriasis, malignancies, other than lymphoma and
non-melanoma skin cancer, were observed at a rate (95% confiidence interval) of 0.6 (0.4, 1.0)/100 patient-years
among 3853 HUMIRA®-treated patients versus a rate of 0.4 (0.2, 1.0)/100 patient-years among 2183 control
patients (median duration of treatment of 5.5 months for HUMIRA®-treated patients and 3.9 months for control-treated
patients). During the controlled portions of HUMIRA® rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis,
Crohn’s disease, and psoriasis trials, the rate (95% confidence interval) of non-melanoma skin cancers was 0.9 (0.57,
1.35)/100 patient-years among HUMIRA®-treated patients and 0.3 (0.08, 0.80)/100 patient-years among control
patients. Of these skin cancers, squamous cell carcinomas occurred at rates (95% confidence interval) of 0.2 (0.1, 0.6)
per 100 patient-years among HUMIRA®-treated patients and 0 per 100 patient-years among control patients. The rate
(95% confidence interval) of lymphomas was 0.1 (0.02, 0.33) per 100 patient-years among HUMIRA®-treated patients
and 0.1 (0.01, 0.61) per 100 patient-years among control patients. In combining the controlled and uncontrolled
open-label portions of these clinical trials with a median duration of approximately 1.7 years, including 6539
patients and over 16,000 patient-years of therapy, the observed rate of malignancies, other than lymphoma and
non-melanoma skin cancers is approximately 1.0 per 100 patient-years. The observed rate of non-melanoma skin
cancers is approximately 0.9 per 100 patient-years.
Carcinogenesis and Mutagenesis: No clastogenic or mutagenic effects of adalimumab were observed in the
in vivo mouse micronucleus test or the Salmonella-Escherichia coli (Ames) assay, respectively.
Immune
Immunosuppression: In a study of 64 patients with rheumatoid arthritis who were treated with adalimumab, there
was no evidence of depression of delayed-type hypersensitivity, depression of immunoglobulin levels, or change in
enumeration of effector T- and B-cells and NK-cells, monocyte/macrophages, and neutrophils.
Immunizations: In a randomized, double-blind, placebo-controlled study in 226 adult rheumatoid arthritis
patients treated with HUMIRA®, antibody responses to concomitant pneumococcal and inflluenza vaccines were
assessed. Protective antibody levels to the pneumococcal antigens were achieved by 86% of patients in the
HUMIRA® group compared to 82% in the placebo group. A total of 37% of HUMIRA®-treated subjects and 40%
of placebo-treated subjects achieved at least a 2-fold increase in antibody titer to at least three out of fiive
pneumococcal antigens. In the same study, 98% of patients in the HUMIRA® group and 95% in the placebo
group achieved protective antibody levels to the inflluenza antigens. A total of 52% of HUMIRA®-treated subjects
and 63% of placebo-treated subjects achieved at least a 4-fold increase in antibody titer to at least two out
of three inflluenza antigens.
SPECIAL POPULATIONS
Pregnant Women: An embryo-fetal perinatal developmental toxicity study has been performed in cynomolgus
monkeys at dosages up to 100 mg/kg (266 times human AUC when given 40 mg adalimumab subcutaneously
with methotrexate every week, or 373 times when given 40 mg adalimumab subcutaneously without methotrexate)
and has revealed no evidence of harm to the fetuses due to adalimumab.
Geriatrics (>65 years of age): A total of 519 rheumatoid arthritis patients 65 years of age and older, including
107 patients 75 years and older, received adalimumab in clinical studies RA I to RA IV. No overall differences in
effectiveness were observed between these subjects and younger subjects. The frequency of serious infection and
malignancy among adalimumab-treated subjects over age 65 was higher than for those under the age of 65.
MONITORING AND LABORATORY TESTS
There is no known interference between adalimumab and laboratory tests.
ADVERSE REACTIONS
Clinical Trial Adverse Drug Reactions
General Statement: Because clinical trials are conducted under very specifiic conditions, the adverse reaction
rates observed in the clinical trials may not refllect the rates observed in practice and should not be compared
to the rates in the clinical trials of another drug. Adverse drug reaction information from clinical trials is useful
for identifying drug-related adverse events and for approximating rates.
Rheumatoid Arthritis Clinical Trials
Description of Data Sources: The data described below refllect exposure to HUMIRA® (adalimumab) in 3046
patients, including more than 2000 patients exposed for 6 months, and more than 1500 exposed for more than
one year (Studies RA I, RA II, RA III, RA IV, and RA V). Adalimumab was studied in placebo-controlled trials and in
long-term follow-up studies for up to 60 months duration in patients with moderately to severely active rheumatoid
arthritis who had failed previous DMARD therapy; the mean age was 54 years, 77% were female and 91%
Caucasian (Studies RA I, RA II, RA III, RA IV). A further study (Study RA V) was in patients with recently diagnosed
rheumatoid arthritis who had not previously been treated with methotrexate. Most patients received
40 mg adalimumab every other week.
Relative Frequency of Adverse Drug Reactions: Table 1 summarizes adverse drug reactions reported at a rate of at
least 1% in patients treated with adalimumab 40 mg every other week (EOW), as well as all doses of adalimumab
tested, compared to placebo or methotrexate (Study RA V). Adverse reaction rates in patients treated with adalimumab
40 mg weekly were similar to rates in patients treated with adalimumab every other week. In Study RA III, the types and
frequencies of adverse drug reactions in the 5-year open-label extension were similar to those observed in the one-year
double-blind portion.
TABLE 1: Number and Percentage of Subjects with ≥1% Treatment-Emergent Adverse Events at Least
Possibly Related to Study Drug During the Control Period in RA Studies (Studies RA I, RA II, RA III, RA IV, RA V)
System Organ Adalimumab All Placebo MTX
Class (SOC) 40 mg s.c. adalimumab (not DE013) (DE013)
EOW N =1247 N=1922 N =690 N=257
N (%) N (%) N (%) N (%)
Gastrointestinal Disorders
Nausea 80 (6.4) 112 (5.8) 12 (1.7) 33 (12.8)
Diarrhea 47 (3.8) 60 (3.1) 17 (2.5) 18 (7.0)
Abdominal pain 22 (1.8) 29 (1.5) 5 (0.7) 3 (1.2)
Abdominal pain upper 20 (1.6) 25 (1.3) 0 (0.0) 13 (5.1)
Mouth ulceration 17 (1.4) 24 (1.2) 5 (0.7) 12 (4.7)
Dyspepsia 14 (1.1) 21 (1.1) 4 (0.6) 7 (2.7)
Vomiting 16 (1.3) 20 (1.0) 5 (0.7) 6 (2.3)
General Disorders and Administration Site Conditions
Injection site irritation 74 (5.9) 122 (6.3) 61 (8.8) 3 (1.2)
Injection site reaction 49 (3.9) 67 (3.5) 3 (0.4) 2 (0.8)
Injection site pain 36 (2.9) 63 (3.3) 24 (3.5) 6 (2.3)
Injection site erythema 36 (2.9) 60 (3.1) 2 (0.3) 1 (0.4)
Fatigue 37 (3.0) 58 (3.0) 7 (1.0) 9 (3.5)
Injection site rash 17 (1.4) 22 (1.1) 2 (0.3) 0 (0.0)
Influenza-like illness 15 (1.2) 21 (1.1) 2 (0.3) 8 (3.1)
Pyrexia 13 (1.0) 20 (1.0) 1 (0.1) 6 (2.3)
Infections and Infestations
Nasopharyngitis 61 (4.9) 95 (4.9) 10 (1.5) 28 (10.9)
Upper respiratory
infection 72 (5.8) 93 (4.8) 15 (2.2) 17 (6.6)
Sinusitis 46 (3.7) 55 (2.9) 17 (2.5) 4 (1.6)
Herpes simplex 33 (2.6) 48 (2.5) 6 (0.9) 5 (1.9)
Urinary tract infection 31 (2.5) 44 (2.3) 6 (0.9) 7 (2.7)
Bronchitis 19 (1.5) 29 (1.5) 8 (1.2) 9 (3.5)
Herpes zoster 17 (1.4) 23 (1.2) 8 (1.2) 2 (0.8)
Influenza 16 (1.3) 21 (1.1) 7 (1.0) 5 (1.9)
Pneumonia 17 (1.4) 21 (1.1) 3 (0.4) 1 (0.4)
Investigations
Lymphocyte count
decreased 11 (0.9) 38 (2.0) 11 (1.6) 1 (0.4)
Alanine aminotrans-
ferase increased 27 (2.2) 33 (1.7) 4 (0.6) 9 (3.5)
Liver function test
abnormal 19 (1.5) 22 (1.1) 4 (0.6) 7 (2.7)
Musculoskeletal and Connective Tissue Disorders
Rheumatoid arthritis 11 (0.9) 28 (1.5) 7 (1.0) 2 (0.8)
Nervous System Disorders
Headache 75 (6.0) 124 (6.5) 14 (2.0) 14 (5.4)
Dizziness 23 (1.8) 32 (1.7) 6 (0.9) 3 (1.2)
Respiratory, Thoracic and Mediastinal Disorders
Pharyngolaryngeal
pain 33 (2.6) 44 (2.3) 9 (1.3) 7 (2.7)
Cough 31 (2.5) 42 (2.2) 4 (0.6) 9 (3.5)
Skin and Subcutaneous Tissue Disorders
Rash 44 (3.5) 66 (3.4) 9 (1.3) 8 (3.1)
Pruritus 28 (2.2) 43 (2.2) 4 (0.6) 5 (1.9)
Alopecia 22 (1.8) 28 (1.5) 2 (0.3) 6 (2.3)
Rash pruritic 14 (1.1) 22 (1.1) 0 (0.0) 3 (1.2)
Psoriatic Arthritis Clinical Trials
Table 2 summarizes adverse drug reactions reported in placebo-controlled and open-label studies at a rate of at
least 1% in psoriatic arthritis patients treated with adalimumab 40 mg every other week.
TABLE 2: Number and Percentage of Subjects with ≥1% Treatment-Emergent Adverse Events at Least
Possibly Related to Study Drug During the Control and Open-label Periods in PsA Studies (Studies
PsA I, PsA II, PsA III)
Double-blind study Open-label study
System Organ Placebo Adalimumab Adalimumab
Class (SOC) 40 mg s.c. 40 mg s.c.
N=211 EOW N=202 EOW N=382
N (%) N (%) N (%)
Gastrointestinal Disorders
Nausea 2 (0.9) 2 (1.0) 3 (0.8)
General Disorders and Administration Site Conditions
Injection site reaction 5 (2.4) 11 (5.4) 21 (5.5)
Injection site pain 8 (3.8) 8 (4.0) 2 (0.5)
Injection site erythema 0 (0.0) 4 (2.0) 2 (0.5)
Injection site burning 4 (1.9) 4 (2.0) 4 (1.0)
Fatigue 5 (2.4) 0 (0.0) 4 (1.0)
Infections and Infestations
Upper respiratory infection 7 (3.3) 8 (4.0) 17 (4.5)
Herpes simplex 3 (1.4) 6 (3.0) 7 (1.8)
Skin fungal infection NOS 0 (0.0) 3 (1.5) -
Pharyngitis 1 (0.5) 2 (1.0) 4 (1.0)
Sinusitis 4 (1.9) 2 (1.0) 12 (3.1)
Urinary tract infection 0 (0.0) 2 (1.0) 6 (1.6)
Bronchitis 1 (0.5) 1 (0.5) 5 (1.3)
Nasopharyngitis 2 (0.9) 1 (0.5) 8 (2.1)
Influenza 2 (0.9) 0 (0.0) 5 (1.3)
Investigations
Liver function tests abnormal 1 (0.5) 2 (1.0) 5 (1.3)
Nervous System Disorders
Headache 5 (2.4) 5 (2.5) 5 (1.3)
Paraesthesia 1 (0.5) 3 (1.5) 2 (0.5)
Respiratory, Thoracic, and Mediastinal Disorders
Rhinitis NOS 0 (0.0) 3 (1.5) 3 (0.8)
Skin and Subcutaneous Tissue Disorders
Erythema 0 (0.0) 3 (1.5) -
Ankylosing Spondylitis Clinical Trials
HUMIRA® has been studied in 393 patients with ankylosing spondylitis in two placebo-controlled studies.
The safety profiile for patients with ankylosing spondylitis treated with HUMIRA® 40 mg every other week (EOW)
was similar to the safety profiile seen in patients with rheumatoid arthritis, HUMIRA® Studies RA I to RA IV.
Table 3 summarizes adverse drug reactions reported at a rate of at least 1% in ankylosing spondylitis patients
treated with adalimumab 40 mg every other week compared to placebo.
TABLE 3: Number and Percentage of Subjects with ≥1% Treatment-Emergent Adverse Events at
Least Possibly Related to Study Drug During the Control Period in AS Studies (Studies AS I and AS II)
System Organ Adalimumab Placebo
Class (SOC) 40 mg s.c. EOW N =246 N=151
N (%) N (%)
General Disorders and Administration Site Conditions
Fatigue 5 (2.0) 3 (2.0)
Injection site erythema 5 (2.0) 1 (0.7)
Injection site irritation 4 (1.6) 2 (1.3)
Injection site pain 6 (2.4) 3 (2.0)
Injection site reaction 8 (3.3) 1 (0.7)
Infections and Infestations
Nasopharyngitis 8 (3.3) 0 (0.0)
Upper respiratory tract infection 5 (2.0) 2 (1.3)
Nervous System Disorders
Dizziness 3 (1.2) 3 (2.0)
Headache 11 (4.5) 4 (2.6)
Skin and Subcutaneous Tissue Disorders
Eczema 3 (1.2) 1 (0.7)
Pruritus 4 (1.6) 1 (0.7)
Pruritus generalized 3 (1.2) 0 (0.0)
Rash 4 (1.6) 1 (0.7)
Urticaria 3 (1.2) 0 (0.0)
Crohn’s Disease Clinical Studies
HUMIRA® has been studied in over 1400 patients with Crohn’s disease in four placebo-controlled and two open-label
extension studies. The safety profiile for patients with Crohn’s disease treated with HUMIRA® was similar to the safety
profiile seen in patients with rheumatoid arthritis. Table 4 and Table 5 summarize adverse drug reactions reported at a
rate of at least 1% in Crohn’s disease patients treated with HUMIRA® in Induction and Maintenance studies, respectively.
TABLE 4: Number and Percentage of Subjects with ≥1% Treatment-Emergent Adverse Events at Least
Possibly Related to Study Drug During Administration of Induction Study Medications in CD Studies
System Organ Adalimumab Adalimumab Placebo
Class (SOC) 160/80 mg N=235 80/40 mg N=75 N=240
N (%) N (%) N (%)
Eye Disorders
Corneal pigmentation 0 (0.0) 1 (1.3) 0 (0.0)
Visual disturbance 0 (0.0) 1 (1.3) 0 (0.0)
Gastrointestinal Disorders
Abdominal pain 5 (2.1) 0 (0.0) 2 (0.8)
Abdominal pain lower 3 (1.3) 0 (0.0) 0 (0.0)
Change of bowel habit 0 (0.0) 1 (1.3) 0 (0.0)
Cheilitis 0 (0.0) 1 (1.3) 1 (0.4)
Constipation 2 (0.9) 1 (1.3) 3 (1.3)
Crohn’s disease 2 (0.9) 1 (1.3) 3 (1.3)
Flatulence 3 (1.3) 0 (0.0) 0 (0.0)
Nausea 6 (2.6) 0 (0.0) 4 (1.7)
Vomiting 1 (0.4) 1 (1.3) 3 (1.3)
General Disorders and Administration Site Conditions
Asthenia 0 (0.0) 1 (1.3) 1 (0.4)
Chills 0 (0.0) 2 (2.7) 1 (0.4)
Fatigue 2 (0.9) 1 (1.3) 10 (4.2)
Influenza like illness 0 (0.0) 2 (2.7) 2 (0.8)
Injection site bruising 5 (2.1) 1 (1.3) 1 (0.4)
Injection site erythema 4 (1.7) 0 (0.0) 0 (0.0)
Injection site irritation 19 (8.1) 8 (10.7) 14 (5.8)
Injection site pain 6 (2.6) 4 (5.3) 9 (3.8)
Injection site pruritus 3 (1.3) 0 (0.0) 0 (0.0)
Injection site reaction 11 (4.7) 5 (6.7) 6 (2.5)
Pain 2 (0.9) 1 (1.3) 3 (1.3)
Pyrexia 3 (1.3) 3 (1.3) 3 (1.3)
Infections and Infestations
Staphylococcal infection 0 (0.0) 1 (1.3) 0 (0.0)
Investigations
Double stranded DNA antibody 0 (0.0) 1 (1.3) 0 (0.0)
White blood cell count increased 0 (0.0) 1 (1.3) 0 (0.0)
Metabolism and Nutrition Disorders
Hypokalaemia 0 (0.0) 1 (1.3) 0 (0.0)
Musculoskeletal and Connective Tissue Disorders
Arthralgia 3 (1.3) 1 (1.3) 2 (0.8)
Back pain 0 (0.0) 1 (1.3) 0 (0.0)
Muscle spasms 0 (0.0) 1 (1.3) 1 (0.4)
Pain in extremity 0 (0.0) 1 (1.3) 0 (0.0)
Nervous System Disorders
Dizziness 3 (1.3) 0 (0.0) 2 (0.8)
Headache 8 (3.4) 2 (2.7) 7 (2.9)
Restless legs syndrome 0 (0.0) 1 (1.3) 0 (0.0)
Reproductive System and Breast Disorders
Genital pruritus female 0 (0.0) 1 (1.3) 0 (0.0)
Skin and Subcutaneous Tissue Disorders
Eczema 1 (0.4) 1 (1.3) 0 (0.0)
Erythema 1 (0.4) 1 (1.3) 1 (0.4)
Hyperhidrosis 0 (0.0) 1 (1.3) 0 (0.0)
Onychorrhexis 0 (0.0) 1 (1.3) 0 (0.0)
Pruritus 1 (0.4) 0 (0.0) 4 (1.7)
Rash 2 (0.9) 2 (2.7) 1 (0.4)
Rash maculo-papular 1 (0.4) 1 (1.3) 0 (0.0)
Rash pruritic 0 (0.0) 1 (1.3) 1 (0.4)
TABLE 5: Number and Percentage of Subjects with ≥1% Treatment-Emergent Adverse Events at Least
Possibly Related to Study Drug During Administration of Blinded Study Maintenance Medications in CD
Studies
System Organ Adalimumab Placebo
Class (SOC) 40 mg s.c. EOW, 40 mg EW
N=554 N =279
N (%) N (%)
Gastrointestinal Disorders
Abdominal pain 7 (1.3) 4 (1.4)
Crohn’s disease 9 (1.6) 9 (3.2)
Diarrhea 7 (1.3) 1 (0.4)
Nausea 9 (1.6) 5 (1.8)
General Disorders and Administration Site Conditions
Fatigue 10 (1.8) 1 (0.4)
Injection site bruising 6 (1.1) 1 (0.4)
Injection site erythema 10 (1.8) 0 (0.0)
Injection site irritation 18 (3.2) 2 (0.7)
Injection site pain 8 (1.4) 2 (0.7)
Injection site reaction 26 (4.7) 1 (0.4)
Pyrexia 7 (1.3) 5 (1.8)
Infections and Infestations
Herpes simplex 6 (1.1) 4 (1.4)
Nasopharyngitis 8 (1.4) 2 (0.7)
Rhinitis 7 (1.3) 1 (0.4)
Musculoskeletal and Connective Tissue Disorders
Arthralgia 9 (1.6) 2 (0.7)
Nervous System Disorders
Headache 19 (3.4) 6 (2.2)
Skin and Subcutaneous Tissue Disorders
Rash 11 (2.0) 5 (1.8)
Psoriasis
HUMIRA® has been studied in 1696 patients with psoriasis in placebo-controlled and open-label extension
studies. The safety profiile for patients with psoriasis treated with HUMIRA® was similar to the safety profiile
seen in patients with rheumatoid arthritis. Table 6 summarizes adverse drug reactions reported at a rate of
at least 1% in psoriasis patients treated with an initial dose of adalimumab 80 mg followed by adalimumab
40 mg every other week compared to placebo or methotrexate.
TABLE 6: Number and Percentage of Subjects ≥ 1% Reporting Treatment-Emergent Adverse Events
Possibly or Probably Related to Study Drug in Controlled Psoriasis Studies (Studies I, II and III)
System Organ Adalimumab Placebo + MTX
Class (SOC) 80 mg x 1, then
40 mg s.c. EOW
N=966 N=613
N (%) N (%)
Gastrointestinal Disorders
Nausea 10 (1.0) 11 (1.8)
General Disorders and Administration Site Conditions
Injection site reaction 29 (3.0) 9 (1.5)
Injection site irritation 16 (1.7) 6 (1.0)
Injection site pain 14 (1.5) 9 (1.5)
Fatigue 10 (1.0) 5 (0.8)
Infections and Infestations
Upper respiratory infection 12 (1.2) 3 (0.5)
Musculoskeletal and Connective Tissue Disorders
Arthralgia 10 (1.0) 3 (0.5)
Nervous System Disorders
Headache 19 (2.0) 14 (2.3)
Less Common Clinical Trial Adverse Drug Reactions: Infrequent serious adverse drug reactions occurring
at an incidence of less than 1% in patients treated with HUMIRA® in Studies RA I to RA V, Studies PsA I and
PsA II, Studies AS I and AS II, CD Maintenance Studies, and Ps Studies I to III:Blood and Lymphatic System Disorders: lymphadenopathy, pancytopenia, agranulocytosis, eosinophilia,
leukopenia, lymphocytosis, neutropenia, anemia;
Cardiac Disorders: arrhythmia superventricular, cardiac arrest, palpitations;
Gastrointestinal Disorders: abdominal pain, Crohn’s disease, anal fiistula, frequent bowel movements, hemorrhoidal
hemorrhage, rectal hemorrhage, small intestine obstruction, pancreatitis;
General Disorders and Administration Site Conditions: chest pain, death, non-cardiac chest pain, pyrexia;
Hepatobiliary Disorders: hepatic necrosis;
Immune System Disorders: hypersensitivity;
Infections and Infestations: pneumonia, arthritis bacterial, cellulitis, escherichia sepsis, perianal abscess, urinary
tract infection, wound infection, sinusitis, bronchitis, cystitis, device-related infection, diverticulitis, erysipelas,
gastroenteritis, herpes virus infection, herpes zoster, histoplasmosis, infected skin ulcer, infection, lobar pneumonia,
lower respiratory tract infection, meningitis viral, mycobacterium avium complex infection, necrotizing fasciitis,
pneumonia pneumococcal, pyelonephritis, respiratory tract infection, sepsis, septic shock, tuberculosis,
urosepsis, abscess, abscess limb;
Injury, Poisoning and Procedural Complications: postoperative wound complication;
Investigations: double stranded DNA antibody, hepatic enzyme increased;
Musculoskeletal and Connective Tissue Disorders: rheumatoid arthritis, arthritis, arthropathy, back pain, muscular
weakness, musculoskeletal chest pain, osteitis, systemic lupus erythematosus;
Neoplasms Benign, Malignant and Unspecifiied (Including Cysts and Polyps): B-cell lymphoma, breast
cancer, malignant melanoma in situ, metastases to liver, ovarian cancer, basal cell carcinoma, squamous cell
carcinoma, testicular seminoma (pure);
Nervous System Disorders: hyperrefllexia, clonus, hypertensive encephalopathy, intention tremor, multiple sclerosis,
paresthesia, tremor;
Psychiatric Disorders: confusional state;
Reproductive System Disorders: cervical dysplasia, endometrial hyperplasia;
Respiratory, Thoracic and Mediastinal Disorders: pleural effusion, pneumonitis, bronchospasm, lung infiiltration,
pleurisy, respiratory failure;
Skin and Subcutaneous Tissue Disorders: psoriasis, pustular psoriasis, rash;
Surgical and Medical Procedures: arthrodesis;
Vascular Disorders: circulatory collapse, rheumatoid vasculitis.
Abnormal Hematologic and Clinical Chemistry Findings: There are no known laboratory tests that may be
helpful in following the patient’s response or in identifying possible adverse reactions.
Rheumatoid arthritis clinical trials: in controlled rheumatoid arthritis clinical trials (RA Studies I-IV), elevations
of ALT were similar in patients receiving adalimumab or placebo. In patients with early rheumatoid arthritis (dis-
ease duration of less than 3 years) (RA Study V), elevations of ALT were more common in the combination arm
(HUMIRA® /methotrexate) compared to the methotrexate monotherapy arm or the HUMIRA® monotherapy arm.
Psoriatic arthritis clinical trials: elevations in ALT were more common in psoriatic arthritis patients compared
with patients in rheumatoid arthritis clinical studies. Crohn’s disease clinical trials: in controlled clinical trials,
elevations of ALT were similar in patients receiving adalimumab or placebo. In all indications, patients with
raised ALT were asymptomatic and in most cases, elevations were transient and resolved on continued treatment.
DRUG INTERACTIONS
Drug-Food Interactions: Adalimumab is administered as a subcutaneous injection. Interactions with food are
therefore not applicable.
Drug-Herb Interactions: Interactions with herbal products have not been established.
Drug-Laboratory Interactions: There are no known laboratory tests that may be helpful in following the
patient’s response or in identifying possible adverse reactions.
MISSED DOSE:
Patients who miss a dose of HUMIRA® should be advised to inject this missed dose as soon as they become
aware of it, and then follow with their next scheduled dose.
OVERDOSAGE
The maximum tolerated dose of HUMIRA® has not been established in humans. Multiple doses up to 10 mg/kg
have been administered to patients in clinical trials without evidence of dose-limiting toxicities. In case of
overdosage, it is recommended that the patient be monitored for any signs or symptoms of adverse reactions
or effects and appropriate symptomatic treatment instituted immediately.
STORAGE AND STABILITY
HUMIRA® (adalimumab) must be refrigerated between 2 and 8°C. Store in original carton until time of
administration. DO NOT FREEZE. Protect from light. Do not use beyond the expiration date.
DOSAGE FORMS, COMPOSITION AND PACKAGING
HUMIRA® (adalimumab) is supplied as a sterile solution for subcutaneous administration in the following
packaging confiigurations:
Pre-fiilled Syringe: HUMIRA® is available in a carton containing two dose trays. In addition to one alcohol pad, each
dose tray consists of a single-dose, 1 mL pre-fiilled glass syringe with a fiixed 27 gauge 1/2 inch needle, providing
40 mg adalimumab dissolved in 0.8 mL sterile solution (50 mg/mL).
Pre-fiilled Pen: HUMIRA® pen is available in a carton containing two dose trays and two alcohol pads. Each dose
tray consists of a single-use pen, containing a 1 mL pre-fiilled glass syringe with a fiixed 27 gauge 1/2 inch needle,
providing 40 mg adalimumab dissolved in 0.8 mL sterile solution (50 mg/mL).
Listing of Non-medicinal Ingredients: In addition to the active ingredient adalimumab, each HUMIRA®
50 mg/mL pre-fiilled syringe or pre-fiilled pen contains the following non-medicinal ingredients: citric acid
monohydrate, dibasic sodium phosphate dihydrate, mannitol, monobasic sodium phosphate dihydrate, polysorbate
80, sodium citrate, sodium chloride, sodium hydroxide (added as necessary to adjust pH), and water for injection.
Abbott Laboratories, LimitedP.O. Box 6150, Station Centre-ville, Montréal (Québec) H3C 3K6
Based on product monograph dated December 16, 2009.Product monograph available upon request.©Abbott Laboratories, LimitedHUM/553A01-February 2010
21385A_SkinAllergy_J10:.ps 6/17/2010 6:51 PM Page 19
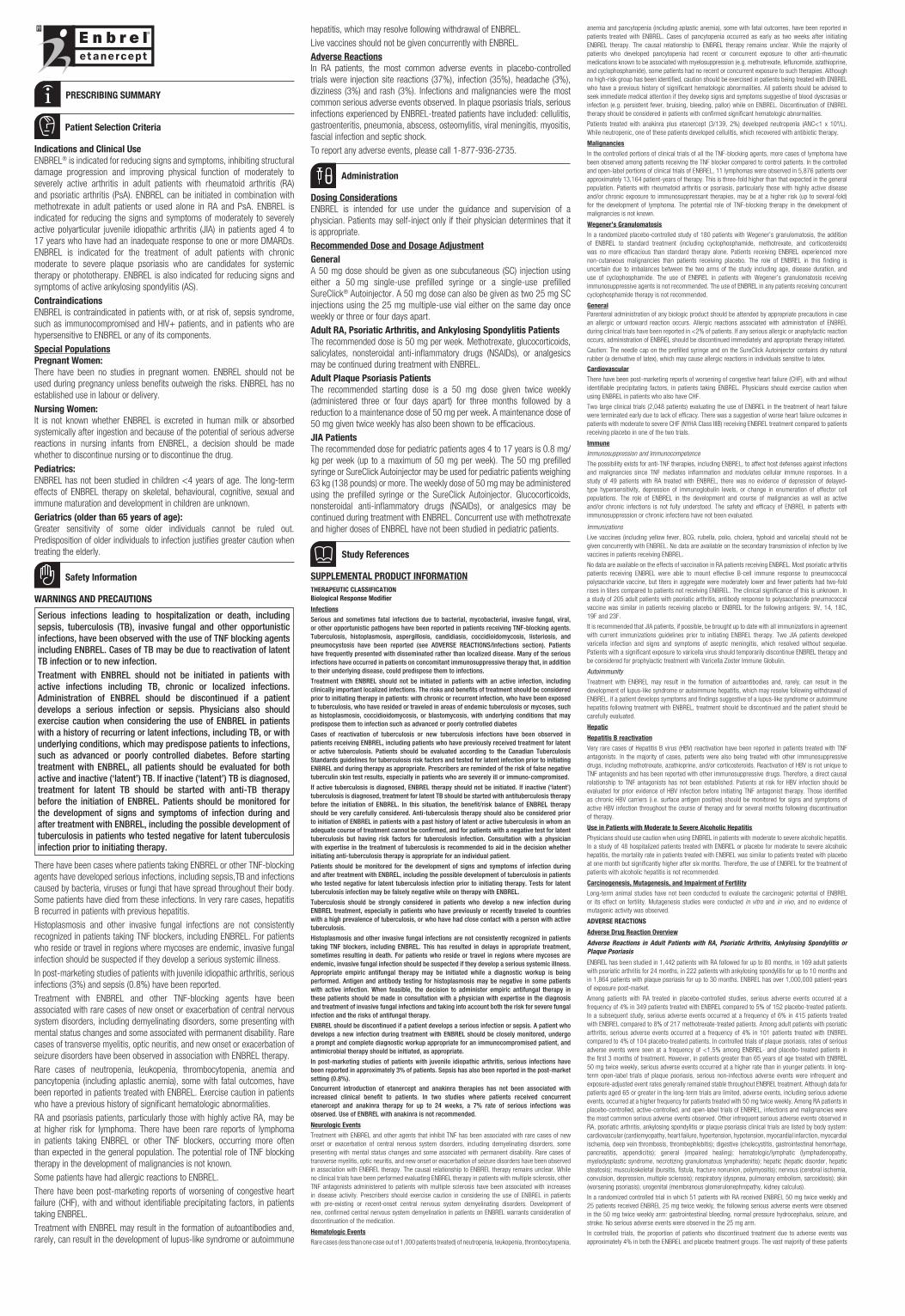
PRESCRIBING SUMMARY
Patient Selection Criteria
Indications and Clinical Use
ENBREL® is indicated for reducing signs and symptoms, inhibiting structural
damage progression and improving physical function of moderately to
severely active arthritis in adult patients with rheumatoid arthritis (RA)
and psoriatic arthritis (PsA). ENBREL can be initiated in combination with
methotrexate in adult patients or used alone in RA and PsA. ENBREL is
indicated for reducing the signs and symptoms of moderately to severely
active polyarticular juvenile idiopathic arthritis (JIA) in patients aged 4 to
17 years who have had an inadequate response to one or more DMARDs.
ENBREL is indicated for the treatment of adult patients with chronic
moderate to severe plaque psoriasis who are candidates for systemic
therapy or phototherapy. ENBREL is also indicated for reducing signs and
symptoms of active ankylosing spondylitis (AS).
Contraindications
ENBREL is contraindicated in patients with, or at risk of, sepsis syndrome,
such as immunocompromised and HIV+ patients, and in patients who are
hypersensitive to ENBREL or any of its components.
Special Populations
Pregnant Women:
There have been no studies in pregnant women. ENBREL should not be
used during pregnancy unless benefits outweigh the risks. ENBREL has no
established use in labour or delivery.
Nursing Women:
It is not known whether ENBREL is excreted in human milk or absorbed
systemically after ingestion and because of the potential of serious adverse
reactions in nursing infants from ENBREL, a decision should be made
whether to discontinue nursing or to discontinue the drug.
Pediatrics:
ENBREL has not been studied in children <4 years of age. The long-term
effects of ENBREL therapy on skeletal, behavioural, cognitive, sexual and
immune maturation and development in children are unknown.
Geriatrics (older than 65 years of age):
Greater sensitivity of some older individuals cannot be ruled out.
Predisposition of older individuals to infection justifies greater caution when
treating the elderly.
Safety Information
WARNINGS AND PRECAUTIONS
Serious infections leading to hospitalization or death, including
sepsis, tuberculosis (TB), invasive fungal and other opportunistic
infections, have been observed with the use of TNF blocking agents
including ENBREL. Cases of TB may be due to reactivation of latent
TB infection or to new infection.
Treatment with ENBREL should not be initiated in patients with
active infections including TB, chronic or localized infections.
Administration of ENBREL should be discontinued if a patient
develops a serious infection or sepsis. Physicians also should
exercise caution when considering the use of ENBREL in patients
with a history of recurring or latent infections, including TB, or with
underlying conditions, which may predispose patients to infections,
such as advanced or poorly controlled diabetes. Before starting
treatment with ENBREL, all patients should be evaluated for both
active and inactive (‘latent’) TB. If inactive (‘latent’) TB is diagnosed,
treatment for latent TB should be started with anti-TB therapy
before the initiation of ENBREL. Patients should be monitored for
the development of signs and symptoms of infection during and
after treatment with ENBREL, including the possible development of
tuberculosis in patients who tested negative for latent tuberculosis
infection prior to initiating therapy.
There have been cases where patients taking ENBREL or other TNF-blocking
agents have developed serious infections, including sepsis,TB and infections
caused by bacteria, viruses or fungi that have spread throughout their body.
Some patients have died from these infections. In very rare cases, hepatitis
B recurred in patients with previous hepatitis.
Histoplasmosis and other invasive fungal infections are not consistently
recognized in patients taking TNF blockers, including ENBREL. For patients
who reside or travel in regions where mycoses are endemic, invasive fungal
infection should be suspected if they develop a serious systemic illness.
In post-marketing studies of patients with juvenile idiopathic arthritis, serious
infections (3%) and sepsis (0.8%) have been reported.
Treatment with ENBREL and other TNF-blocking agents have been
associated with rare cases of new onset or exacerbation of central nervous
system disorders, including demyelinating disorders, some presenting with
mental status changes and some associated with permanent disability. Rare
cases of transverse myelitis, optic neuritis, and new onset or exacerbation of
seizure disorders have been observed in association with ENBREL therapy.
Rare cases of neutropenia, leukopenia, thrombocytopenia, anemia and
pancyto penia (including aplastic anemia), some with fatal outcomes, have
been reported in patients treated with ENBREL. Exercise caution in patients
who have a previous history of significant hematologic abnormalities.
RA and psoriasis patients, particularly those with highly active RA, may be
at higher risk for lymphoma. There have been rare reports of lymphoma
in patients taking ENBREL or other TNF blockers, occurring more often
than expected in the general population. The potential role of TNF blocking
therapy in the development of malignancies is not known.
Some patients have had allergic reactions to ENBREL.
There have been post-marketing reports of worsening of congestive heart
failure (CHF), with and without identifiable precipitating factors, in patients
taking ENBREL.
Treatment with ENBREL may result in the formation of autoantibodies and,
rarely, can result in the development of lupus-like syndrome or autoimmune
hepatitis, which may resolve following withdrawal of ENBREL.
Live vaccines should not be given concurrently with ENBREL.
Adverse Reactions
In RA patients, the most common adverse events in placebo-controlled
trials were injection site reactions (37%), infection (35%), headache (3%),
dizziness (3%) and rash (3%). Infections and malignancies were the most
common serious adverse events observed. In plaque psoriasis trials, serious
infections experienced by ENBREL-treated patients have included: cellulitis,
gastroenteritis, pneumonia, abscess, osteomylitis, viral meningitis, myositis,
fascial infection and septic shock.
To report any adverse events, please call 1-877-936-2735.
Administration
Dosing Considerations
ENBREL is intended for use under the guidance and supervision of a
physician. Patients may self-inject only if their physician determines that it
is appropriate.
Recommended Dose and Dosage Adjustment
General
A 50 mg dose should be given as one subcutaneous (SC) injection using
either a 50 mg single-use prefilled syringe or a single-use prefilled
SureClick® Autoinjector. A 50 mg dose can also be given as two 25 mg SC
injections using the 25 mg multiple-use vial either on the same day once
weekly or three or four days apart.
Adult RA, Psoriatic Arthritis, and Ankylosing Spondylitis Patients
The recommended dose is 50 mg per week. Methotrexate, glucocorticoids,
salicylates, nonsteroidal anti-inflammatory drugs (NSAIDs), or analgesics
may be continued during treatment with ENBREL.
Adult Plaque Psoriasis Patients
The recommended starting dose is a 50 mg dose given twice weekly
(administered three or four days apart) for three months followed by a
reduction to a maintenance dose of 50 mg per week. A maintenance dose of
50 mg given twice weekly has also been shown to be efficacious.
JIA Patients
The recommended dose for pediatric patients ages 4 to 17 years is 0.8 mg/
kg per week (up to a maximum of 50 mg per week). The 50 mg prefilled
syringe or SureClick Autoinjector may be used for pediatric patients weighing
63 kg (138 pounds) or more. The weekly dose of 50 mg may be administered
using the prefilled syringe or the SureClick Autoinjector. Glucocorticoids,
nonsteroidal anti-inflammatory drugs (NSAIDs), or analgesics may be
continued during treatment with ENBREL. Concurrent use with methotrexate
and higher doses of ENBREL have not been studied in pediatric patients.
Study References
SUPPLEMENTAL PRODUCT INFORMATION
THERAPEUTIC CLASSIFICATION
Biological Response Modifier
Infections
Serious and sometimes fatal infections due to bacterial, mycobacterial, invasive fungal, viral,
or other opportunistic pathogens have been reported in patients receiving TNF-blocking agents.
Tuberculosis, histoplasmosis, aspergillosis, candidiasis, coccidioidomycosis, listeriosis, and
pneumocystosis have been reported (see ADVERSE REACTIONS/Infections section). Patients
have frequently presented with disseminated rather than localized disease. Many of the serious
infections have occurred in patients on concomitant immunosuppressive therapy that, in addition
to their underlying disease, could predispose them to infections.
Treatment with ENBREL should not be initiated in patients with an active infection, including
clinically important localized infections. The risks and benefits of treatment should be considered
prior to initiating therapy in patients: with chronic or recurrent infection, who have been exposed
to tuberculosis, who have resided or traveled in areas of endemic tuberculosis or mycoses, such
as histoplasmosis, coccidioidomycosis, or blastomycosis, with underlying conditions that may
predispose them to infection such as advanced or poorly controlled diabetes
Cases of reactivation of tuberculosis or new tuberculosis infections have been observed in
patients receiving ENBREL, including patients who have previously received treatment for latent
or active tuberculosis. Patients should be evaluated according to the Canadian Tuberculosis
Standards guidelines for tuberculosis risk factors and tested for latent infection prior to initiating
ENBREL and during therapy as appropriate. Prescribers are reminded of the risk of false negative
tuberculin skin test results, especially in patients who are severely ill or immuno-compromised.
If active tuberculosis is diagnosed, ENBREL therapy should not be initiated. If inactive (‘latent’)
tuberculosis is diagnosed, treatment for latent TB should be started with antituberculosis therapy
before the initiation of ENBREL. In this situation, the benefit/risk balance of ENBREL therapy
should be very carefully considered. Anti-tuberculosis therapy should also be considered prior
to initiation of ENBREL in patients with a past history of latent or active tuberculosis in whom an
adequate course of treatment cannot be confirmed, and for patients with a negative test for latent
tuberculosis but having risk factors for tuberculosis infection. Consultation with a physician
with expertise in the treatment of tuberculosis is recommended to aid in the decision whether
initiating anti-tuberculosis therapy is appropriate for an individual patient.
Patients should be monitored for the development of signs and symptoms of infection during
and after treatment with ENBREL, including the possible development of tuberculosis in patients
who tested negative for latent tuberculosis infection prior to initiating therapy. Tests for latent
tuberculosis infection may be falsely negative while on therapy with ENBREL.
Tuberculosis should be strongly considered in patients who develop a new infection during
ENBREL treatment, especially in patients who have previously or recently traveled to countries
with a high prevalence of tuberculosis, or who have had close contact with a person with active
tuberculosis.
Histoplasmosis and other invasive fungal infections are not consistently recognized in patients
taking TNF blockers, including ENBREL. This has resulted in delays in appropriate treatment,
sometimes resulting in death. For patients who reside or travel in regions where mycoses are
endemic, invasive fungal infection should be suspected if they develop a serious systemic illness.
Appropriate empiric antifungal therapy may be initiated while a diagnostic workup is being
performed. Antigen and antibody testing for histoplasmosis may be negative in some patients
with active infection. When feasible, the decision to administer empiric antifungal therapy in
these patients should be made in consultation with a physician with expertise in the diagnosis
and treatment of invasive fungal infections and taking into account both the risk for severe fungal
infection and the risks of antifungal therapy.
ENBREL should be discontinued if a patient develops a serious infection or sepsis. A patient who
develops a new infection during treatment with ENBREL should be closely monitored, undergo
a prompt and complete diagnostic workup appropriate for an immunocompromised patient, and
antimicrobial therapy should be initiated, as appropriate.
In post-marketing studies of patients with juvenile idiopathic arthritis, serious infections have
been reported in approximately 3% of patients. Sepsis has also been reported in the post-market
setting (0.8%).
Concurrent introduction of etanercept and anakinra therapies has not been associated with
increased clinical benefit to patients. In two studies where patients received concurrent
etanercept and anakinra therapy for up to 24 weeks, a 7% rate of serious infections was
observed. Use of ENBREL with anakinra is not recommended.
Neurologic Events
Treatment with ENBREL and other agents that inhibit TNF has been associated with rare cases of new
onset or exacerbation of central nervous system disorders, including demyelinating disorders, some
presenting with mental status changes and some associated with permanent disability. Rare cases of
transverse myelitis, optic neuritis, and new onset or exacerbation of seizure disorders have been observed
in association with ENBREL therapy. The causal relationship to ENBREL therapy remains unclear. While
no clinical trials have been performed evaluating ENBREL therapy in patients with multiple sclerosis, other
TNF antagonists administered to patients with multiple sclerosis have been associated with increases
in disease activity. Prescribers should exercise caution in considering the use of ENBREL in patients
with pre-existing or recent-onset central nervous system demyelinating disorders. Development of
new, confirmed central nervous system demyelination in patients on ENBREL warrants consideration of
discontinuation of the medication.
Hematologic Events
Rare cases (less than one case out of 1,000 patients treated) of neutropenia, leukopenia, thrombocytopenia,
anemia and pancytopenia (including aplastic anemia), some with fatal outcomes, have been reported in
patients treated with ENBREL. Cases of pancytopenia occurred as early as two weeks after initiating
ENBREL therapy. The causal relationship to ENBREL therapy remains unclear. While the majority of
patients who developed pancytopenia had recent or concurrent exposure to other anti-rheumatic
medications known to be associated with myelosuppression (e.g. methotrexate, leflunomide, azathioprine,
and cyclophosphamide), some patients had no recent or concurrent exposure to such therapies. Although
no high-risk group has been identified, caution should be exercised in patients being treated with ENBREL
who have a previous history of significant hematologic abnormalities. All patients should be advised to
seek immediate medical attention if they develop signs and symptoms suggestive of blood dyscrasias or
infection (e.g. persistent fever, bruising, bleeding, pallor) while on ENBREL. Discontinuation of ENBREL
therapy should be considered in patients with confirmed significant hematologic abnormalities.
Patients treated with anakinra plus etanercept (3/139, 2%) developed neutropenia (ANC<1 x 109/L).
While neutropenic, one of these patients developed cellulitis, which recovered with antibiotic therapy.
Malignancies
In the controlled portions of clinical trials of all the TNF-blocking agents, more cases of lymphoma have
been observed among patients receiving the TNF blocker compared to control patients. In the controlled
and open-label portions of clinical trials of ENBREL, 11 lymphomas were observed in 5,876 patients over
approximately 13,164 patient-years of therapy. This is three-fold higher than that expected in the general
population. Patients with rheumatoid arthritis or psoriasis, particularly those with highly active disease
and/or chronic exposure to immunosuppressant therapies, may be at a higher risk (up to several-fold)
for the development of lymphoma. The potential role of TNF-blocking therapy in the development of
malignancies is not known.
Wegener’s Granulomatosis
In a randomized placebo-controlled study of 180 patients with Wegener’s granulomatosis, the addition
of ENBREL to standard treatment (including cyclophosphamide, methotrexate, and corticosteroids)
was no more efficacious than standard therapy alone. Patients receiving ENBREL experienced more
non-cutaneous malignancies than patients receiving placebo. The role of ENBREL in this finding is
uncertain due to imbalances between the two arms of the study including age, disease duration, and
use of cyclophosphamide. The use of ENBREL in patients with Wegener’s granulomatosis receiving
immunosuppressive agents is not recommended. The use of ENBREL in any patients receiving concurrent
cyclophosphamide therapy is not recommended.
General
Parenteral administration of any biologic product should be attended by appropriate precautions in case
an allergic or untoward reaction occurs. Allergic reactions associated with administration of ENBREL
during clinical trials have been reported in <2% of patients. If any serious allergic or anaphylactic reaction
occurs, administration of ENBREL should be discontinued immediately and appropriate therapy initiated.
Caution: The needle cap on the prefilled syringe and on the SureClick Autoinjector contains dry natural
rubber (a derivative of latex), which may cause allergic reactions in individuals sensitive to latex.
Cardiovascular
There have been post-marketing reports of worsening of congestive heart failure (CHF), with and without
identifiable precipitating factors, in patients taking ENBREL. Physicians should exercise caution when
using ENBREL in patients who also have CHF.
Two large clinical trials (2,048 patients) evaluating the use of ENBREL in the treatment of heart failure
were terminated early due to lack of efficacy. There was a suggestion of worse heart failure outcomes in
patients with moderate to severe CHF (NYHA Class IIIB) receiving ENBREL treatment compared to patients
receiving placebo in one of the two trials.
Immune
Immunosuppression and Immunocompetence
The possibility exists for anti-TNF therapies, including ENBREL, to affect host defenses against infections
and malignancies since TNF mediates inflammation and modulates cellular immune responses. In a
study of 49 patients with RA treated with ENBREL, there was no evidence of depression of delayed-
type hypersensitivity, depression of immunoglobulin levels, or change in enumeration of effector cell
populations. The role of ENBREL in the development and course of malignancies as well as active
and/or chronic infections is not fully understood. The safety and efficacy of ENBREL in patients with
immunosuppression or chronic infections have not been evaluated.
Immunizations
Live vaccines (including yellow fever, BCG, rubella, polio, cholera, typhoid and varicella) should not be
given concurrently with ENBREL. No data are available on the secondary transmission of infection by live
vaccines in patients receiving ENBREL.
No data are available on the effects of vaccination in RA patients receiving ENBREL. Most psoriatic arthritis
patients receiving ENBREL were able to mount effective B-cell immune response to pneumococcal
polysaccharide vaccine, but titers in aggregate were moderately lower and fewer patients had two-fold
rises in titers compared to patients not receiving ENBREL. The clinical significance of this is unknown. In
a study of 205 adult patients with psoriatic arthritis, antibody response to polysaccharide pneumococcal
vaccine was similar in patients receiving placebo or ENBREL for the following antigens: 9V, 14, 18C,
19F and 23F.
It is recommended that JIA patients, if possible, be brought up to date with all immunizations in agreement
with current immunizations guidelines prior to initiating ENBREL therapy. Two JIA patients developed
varicella infection and signs and symptoms of aseptic meningitis, which resolved without sequelae.
Patients with a significant exposure to varicella virus should temporarily discontinue ENBREL therapy and
be considered for prophylactic treatment with Varicella Zoster Immune Globulin.
Autoimmunity
Treatment with ENBREL may result in the formation of autoantibodies and, rarely, can result in the
development of lupus-like syndrome or autoimmune hepatitis, which may resolve following withdrawal of
ENBREL. If a patient develops symptoms and findings suggestive of a lupus-like syndrome or autoimmune
hepatitis following treatment with ENBREL, treatment should be discontinued and the patient should be
carefully evaluated.
Hepatic
Hepatitis B reactivation
Very rare cases of Hepatitis B virus (HBV) reactivation have been reported in patients treated with TNF
antagonists. In the majority of cases, patients were also being treated with other immunosuppressive
drugs, including methotrexate, azathioprine, and/or corticosteroids. Reactivation of HBV is not unique to
TNF antagonists and has been reported with other immunosuppressive drugs. Therefore, a direct causal
relationship to TNF antagonists has not been established. Patients at risk for HBV infection should be
evaluated for prior evidence of HBV infection before initiating TNF antagonist therapy. Those identified
as chronic HBV carriers (i.e. surface antigen positive) should be monitored for signs and symptoms of
active HBV infection throughout the course of therapy and for several months following discontinuation
of therapy.
Use in Patients with Moderate to Severe Alcoholic Hepatitis
Physicians should use caution when using ENBREL in patients with moderate to severe alcoholic hepatitis.
In a study of 48 hospitalized patients treated with ENBREL or placebo for moderate to severe alcoholic
hepatitis, the mortality rate in patients treated with ENBREL was similar to patients treated with placebo
at one month but significantly higher after six months. Therefore, the use of ENBREL for the treatment of
patients with alcoholic hepatitis is not recommended.
Carcinogenesis, Mutagenesis, and Impairment of Fertility
Long-term animal studies have not been conducted to evaluate the carcinogenic potential of ENBREL
or its effect on fertility. Mutagenesis studies were conducted in vitro and in vivo, and no evidence of
mutagenic activity was observed.
ADVERSE REACTIONS
Adverse Drug Reaction Overview
Adverse Reactions in Adult Patients with RA, Psoriatic Arthritis, Ankylosing Spondylitis or
Plaque Psoriasis
ENBREL has been studied in 1,442 patients with RA followed for up to 80 months, in 169 adult patients
with psoriatic arthritis for 24 months, in 222 patients with ankylosing spondylitis for up to 10 months and
in 1,864 patients with plaque psoriasis for up to 30 months. ENBREL has over 1,000,000 patient-years
of exposure post-market.
Among patients with RA treated in placebo-controlled studies, serious adverse events occurred at a
frequency of 4% in 349 patients treated with ENBREL compared to 5% of 152 placebo-treated patients.
In a subsequent study, serious adverse events occurred at a frequency of 6% in 415 patients treated
with ENBREL compared to 8% of 217 methotrexate-treated patients. Among adult patients with psoriatic
arthritis, serious adverse events occurred at a frequency of 4% in 101 patients treated with ENBREL
compared to 4% of 104 placebo-treated patients. In controlled trials of plaque psoriasis, rates of serious
adverse events were seen at a frequency of <1.5% among ENBREL- and placebo-treated patients in
the first 3 months of treatment. However, in patients greater than 65 years of age treated with ENBREL
50 mg twice weekly, serious adverse events occurred at a higher rate than in younger patients. In long-
term open-label trials of plaque psoriasis, serious non-infectious adverse events were infrequent and
exposure-adjusted event rates generally remained stable throughout ENBREL treatment. Although data for
patients aged 65 or greater in the long-term trials are limited, adverse events, including serious adverse
events, occurred at a higher frequency for patients treated with 50 mg twice weekly. Among RA patients in
placebo-controlled, active-controlled, and open-label trials of ENBREL, infections and malignancies were
the most common serious adverse events observed. Other infrequent serious adverse events observed in
RA, psoriatic arthritis, ankylosing spondylitis or plaque psoriasis clinical trials are listed by body system:
cardiovascular (cardiomyopathy, heart failure, hypertension, hypotension, myocardial infarction, myocardial
ischemia, deep vein thrombosis, thrombophlebitis); digestive (cholecystitis, gastrointestinal hemorrhage,
pancreatitis, appendicitis); general (impaired healing); hematologic/lymphatic (lymphadenopathy,
myelodysplastic syndrome, necrotizing granulomatous lymphadenitis); hepatic (hepatic disorder, hepatic
steatosis); musculoskeletal (bursitis, fistula, fracture nonunion, polymyositis); nervous (cerebral ischemia,
convulsion, depression, multiple sclerosis); respiratory (dyspnea, pulmonary embolism, sarcoidosis); skin
(worsening psoriasis); urogenital (membranous glomerulonephropathy, kidney calculus).
In a randomized controlled trial in which 51 patients with RA received ENBREL 50 mg twice weekly and
25 patients received ENBREL 25 mg twice weekly, the following serious adverse events were observed
in the 50 mg twice weekly arm: gastrointestinal bleeding, normal pressure hydrocephalus, seizure, and
stroke. No serious adverse events were observed in the 25 mg arm.
In controlled trials, the proportion of patients who discontinued treatment due to adverse events was
approximately 4% in both the ENBREL and placebo treatment groups. The vast majority of these patients
21385A_SkinAllergy_J10:.ps 6/17/2010 6:52 PM Page 20
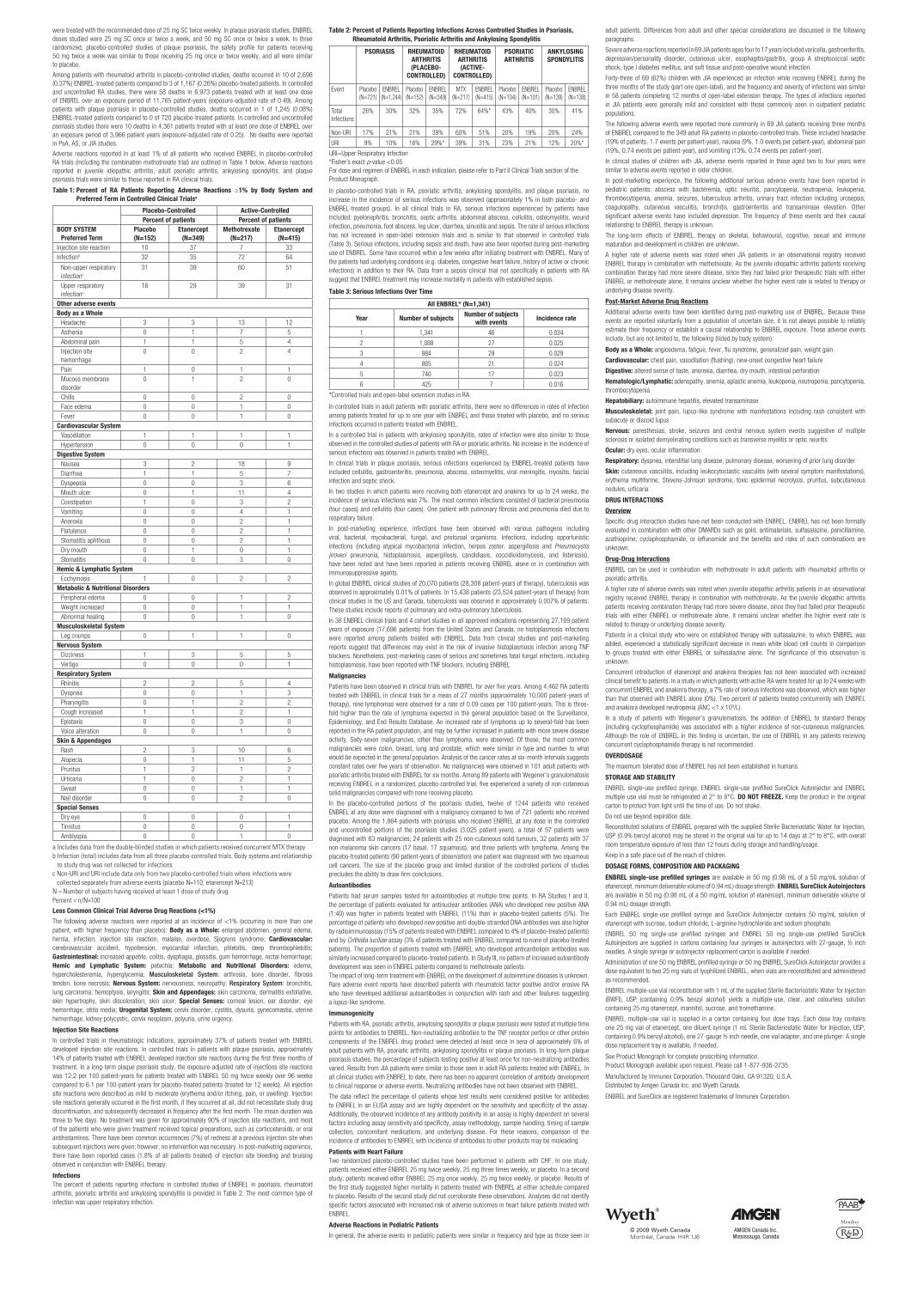
were treated with the recommended dose of 25 mg SC twice weekly. In plaque psoriasis studies, ENBREL
doses studied were 25 mg SC once or twice a week, and 50 mg SC once or twice a week. In three
randomized, placebo-controlled studies of plaque psoriasis, the safety profile for patients receiving
50 mg twice a week was similar to those receiving 25 mg once or twice weekly, and all were similar
to placebo.
Among patients with rheumatoid arthritis in placebo-controlled studies, deaths occurred in 10 of 2,696
(0.37%) ENBREL-treated patients compared to 3 of 1,167 (0.26%) placebo-treated patients. In controlled
and uncontrolled RA studies, there were 58 deaths in 6,973 patients treated with at least one dose
of ENBREL over an exposure period of 11,765 patient-years (exposure-adjusted rate of 0.49). Among
patients with plaque psoriasis in placebo-controlled studies, deaths occurred in 1 of 1,245 (0.08%)
ENBREL-treated patients compared to 0 of 720 placebo-treated patients. In controlled and uncontrolled
psoriasis studies there were 10 deaths in 4,361 patients treated with at least one dose of ENBREL over
an exposure period of 3,966 patient-years (exposure-adjusted rate of 0.25). No deaths were reported
in PsA, AS, or JIA studies.
Adverse reactions reported in at least 1% of all patients who received ENBREL in placebo-controlled
RA trials (including the combination methotrexate trial) are outlined in Table 1 below. Adverse reactions
reported in juvenile idiopathic arthritis, adult psoriatic arthritis, ankylosing spondylitis, and plaque
psoriasis trials were similar to those reported in RA clinical trials.
Table 1: Percent of RA Patients Reporting Adverse Reactions ≥1% by Body System and
Preferred Term in Controlled Clinical Trialsa
Placebo-Controlled Active-Controlled
Percent of patients Percent of patients
BODY SYSTEM
Preferred Term
Placebo
(N=152)
Etanercept
(N=349)
Methotrexate
(N=217)
Etanercept
(N=415)
Injection site reaction 10 37 7 33
Infectionb 32 35 72 64
Non-upper respiratory
infectionc
31 39 60 51
Upper respiratory
infectionc
16 29 39 31
Other adverse events
Body as a Whole
Headache 3 3 13 12
Asthenia 0 1 7 5
Abdominal pain 1 1 5 4
Injection site
hemorrhage
0 0 2 4
Pain 1 0 1 1
Mucous membrane
disorder
0 1 2 0
Chills 0 0 2 0
Face edema 0 0 1 0
Fever 0 0 1 0
Cardiovascular System
Vasodilation 1 1 1 1
Hypertension 0 0 0 1
Digestive System
Nausea 3 2 18 9
Diarrhea 1 1 5 7
Dyspepsia 0 0 3 6
Mouth ulcer 0 1 11 4
Constipation 1 0 3 2
Vomiting 0 0 4 1
Anorexia 0 0 2 1
Flatulence 0 0 2 1
Stomatitis aphthous 0 0 2 1
Dry mouth 0 1 0 1
Stomatitis 0 0 3 0
Hemic & Lymphatic System
Ecchymosis 1 0 2 2
Metabolic & Nutritional Disorders
Peripheral edema 0 0 1 2
Weight increased 0 0 1 1
Abnormal healing 0 0 1 0
Musculoskeletal System
Leg cramps 0 1 1 0
Nervous System
Dizziness 1 3 5 5
Vertigo 0 0 0 1
Respiratory System
Rhinitis 2 2 5 4
Dyspnea 0 0 1 3
Pharyngitis 0 1 2 2
Cough increased 1 1 2 1
Epistaxis 0 0 3 0
Voice alteration 0 0 1 0
Skin & Appendages
Rash 2 3 10 6
Alopecia 0 1 11 5
Pruritus 1 2 1 2
Urticaria 1 0 2 1
Sweat 0 0 1 1
Nail disorder 0 0 2 0
Special Senses
Dry eye 0 0 0 1
Tinnitus 0 0 0 1
Amblyopia 0 0 1 0
a Includes data from the double-blinded studies in which patients received concurrent MTX therapy
b Infection (total) includes data from all three placebo-controlled trials. Body systems and relationship
to study drug was not collected for infections
c Non-URI and URI include data only from two placebo-controlled trials where infections were
collected separately from adverse events (placebo N=110, etanercept N=213)
N = Number of subjects having received at least 1 dose of study drug
Percent = n/N×100
Less Common Clinical Trial Adverse Drug Reactions (<1%)
The following adverse reactions were reported at an incidence of <1% (occurring in more than one
patient, with higher frequency than placebo): Body as a Whole: enlarged abdomen, general edema,
hernia, infection, injection site reaction, malaise, overdose, Sjogrens syndrome; Cardiovascular:
cerebrovascular accident, hypotension, myocardial infarction, phlebitis, deep thrombophlebitis;
Gastrointestinal: increased appetite, colitis, dysphagia, glossitis, gum hemorrhage, rectal hemorrhage;
Hemic and Lymphatic System: petechia; Metabolic and Nutritional Disorders: edema,
hypercholesteremia, hyperglycemia; Musculoskeletal System: arthrosis, bone disorder, fibrosis
tendon, bone necrosis; Nervous System: nervousness, neuropathy; Respiratory System: bronchitis,
lung carcinoma, hemoptysis, laryngitis; Skin and Appendages: skin carcinoma, dermatitis exfoliative,
skin hypertrophy, skin discoloration, skin ulcer; Special Senses: corneal lesion, ear disorder, eye
hemorrhage, otitis media; Urogenital System: cervix disorder, cystitis, dysuria, gynecomastia, uterine
hemorrhage, kidney polycystic, cervix neoplasm, polyuria, urine urgency.
Injection Site Reactions
In controlled trials in rheumatologic indications, approximately 37% of patients treated with ENBREL
developed injection site reactions. In controlled trials in patients with plaque psoriasis, approximately
14% of patients treated with ENBREL developed injection site reactions during the first three months of
treatment. In a long-term plaque psoriasis study, the exposure-adjusted rate of injections site reactions
was 12.2 per 100 patient-years for patients treated with ENBREL 50 mg twice weekly over 96 weeks
compared to 6.1 per 100-patient-years for placebo-treated patients (treated for 12 weeks). All injection
site reactions were described as mild to moderate (erythema and/or itching, pain, or swelling). Injection
site reactions generally occurred in the first month, if they occurred at all, did not necessitate study drug
discontinuation, and subsequently decreased in frequency after the first month. The mean duration was
three to five days. No treatment was given for approximately 90% of injection site reactions, and most
of the patients who were given treatment received topical preparations, such as corticosteroids, or oral
antihistamines. There have been common occurrences (7%) of redness at a previous injection site when
subsequent injections were given; however, no intervention was necessary. In post-marketing experience,
there have been reported cases (1.8% of all patients treated) of injection site bleeding and bruising
observed in conjunction with ENBREL therapy.
Infections
The percent of patients reporting infections in controlled studies of ENBREL in psoriasis, rheumatoid
arthritis, psoriatic arthritis and ankylosing spondylitis is provided in Table 2. The most common type of
infection was upper respiratory infection.
Table 2: Percent of Patients Reporting Infections Across Controlled Studies in Psoriasis,
Rheumatoid Arthritis, Psoriatic Arthritis and Ankylosing Spondylitis
PSORIASIS RHEUMATOID
ARTHRITIS
(PLACEBO-
CONTROLLED)
RHEUMATOID
ARTHRITIS
(ACTIVE-
CONTROLLED)
PSORIATIC
ARTHRITIS
ANKYLOSING
SPONDYLITIS
Event Placebo
(N=721)
ENBREL
(N=1,244)
Placebo
(N=152)
ENBREL
(N=349)
MTX
(N=217)
ENBREL
(N=415)
Placebo
(N=104)
ENBREL
(N=101)
Placebo
(N=139)
ENBREL
(N=138)
Total
Infections
26% 30% 32% 35% 72% 64%* 43% 40% 30% 41%
Non-URI 17% 21% 31% 39% 60% 51% 20% 19% 20% 24%
URI 9% 10% 16% 29%* 39% 31% 23% 21% 12% 20%*
URI=Upper Respiratory Infection
*Fisher’s exact p-value <0.05
For dose and regimen of ENBREL in each indication, please refer to Part II Clinical Trials section of the
Product Monograph.
In placebo-controlled trials in RA, psoriatic arthritis, ankylosing spondylitis, and plaque psoriasis, no
increase in the incidence of serious infections was observed (approximately 1% in both placebo- and
ENBREL-treated groups). In all clinical trials in RA, serious infections experienced by patients have
included: pyelonephritis, bronchitis, septic arthritis, abdominal abscess, cellulitis, osteomyelitis, wound
infection, pneumonia, foot abscess, leg ulcer, diarrhea, sinusitis and sepsis. The rate of serious infections
has not increased in open-label extension trials and is similar to that observed in controlled trials
(Table 3). Serious infections, including sepsis and death, have also been reported during post-marketing
use of ENBREL. Some have occurred within a few weeks after initiating treatment with ENBREL. Many of
the patients had underlying conditions (e.g. diabetes, congestive heart failure, history of active or chronic
infections) in addition to their RA. Data from a sepsis clinical trial not specifically in patients with RA
suggest that ENBREL treatment may increase mortality in patients with established sepsis.
Table 3: Serious Infections Over Time
All ENBREL* (N=1,341)
Year Number of subjectsNumber of subjects
with eventsIncidence rate
1 1,341 46 0.034
2 1,088 27 0.025
3 984 29 0.029
4 865 21 0.024
5 740 17 0.023
6 425 7 0.016
*Controlled trials and open-label extension studies in RA.
In controlled trials in adult patients with psoriatic arthritis, there were no differences in rates of infection
among patients treated for up to one year with ENBREL and those treated with placebo, and no serious
infections occurred in patients treated with ENBREL.
In a controlled trial in patients with ankylosing spondylitis, rates of infection were also similar to those
observed in the controlled studies of patients with RA or psoriatic arthritis. No increase in the incidence of
serious infections was observed in patients treated with ENBREL.
In clinical trials in plaque psoriasis, serious infections experienced by ENBREL-treated patients have
included cellulitis, gastroenteritis, pneumonia, abscess, osteomyelitis, viral meningitis, myositis, fascial
infection and septic shock.
In two studies in which patients were receiving both etanercept and anakinra for up to 24 weeks, the
incidence of serious infections was 7%. The most common infections consisted of bacterial pneumonia
(four cases) and cellulitis (four cases). One patient with pulmonary fibrosis and pneumonia died due to
respiratory failure.
In post-marketing experience, infections have been observed with various pathogens including
viral, bacterial, mycobacterial, fungal, and protozoal organisms. Infections, including opportunistic
infections (including atypical mycobacterial infection, herpes zoster, aspergillosis and Pneumocystis
jiroveci pneumonia, histoplasmosis, aspergillosis, candidiasis, coccidioidomycosis, and listeriosis),
have been noted and have been reported in patients receiving ENBREL alone or in combination with
immunosuppressive agents.
In global ENBREL clinical studies of 20,070 patients (28,308 patient-years of therapy), tuberculosis was
observed in approximately 0.01% of patients. In 15,438 patients (23,524 patient-years of therapy) from
clinical studies in the US and Canada, tuberculosis was observed in approximately 0.007% of patients.
These studies include reports of pulmonary and extra-pulmonary tuberculosis.
In 38 ENBREL clinical trials and 4 cohort studies in all approved indications representing 27,169 patient
years of exposure (17,696 patients) from the United States and Canada, no histoplasmosis infections
were reported among patients treated with ENBREL. Data from clinical studies and post-marketing
reports suggest that differences may exist in the risk of invasive histoplasmosis infection among TNF
blockers. Nonetheless, post-marketing cases of serious and sometimes fatal fungal infections, including
histoplasmosis, have been reported with TNF blockers, including ENBREL
Malignancies
Patients have been observed in clinical trials with ENBREL for over five years. Among 4,462 RA patients
treated with ENBREL in clinical trials for a mean of 27 months (approximately 10,000 patient-years of
therapy), nine lymphomas were observed for a rate of 0.09 cases per 100 patient-years. This is three-
fold higher than the rate of lymphoma expected in the general population based on the Surveillance,
Epidemiology, and End Results Database. An increased rate of lymphoma up to several-fold has been
reported in the RA patient population, and may be further increased in patients with more severe disease
activity. Sixty-seven malignancies, other than lymphoma, were observed. Of these, the most common
malignancies were colon, breast, lung and prostate, which were similar in type and number to what
would be expected in the general population. Analysis of the cancer rates at six-month intervals suggests
constant rates over five years of observation. No malignancies were observed in 101 adult patients with
psoriatic arthritis treated with ENBREL for six months. Among 89 patients with Wegener’s granulomatosis
receiving ENBREL in a randomized, placebo-controlled trial, five experienced a variety of non-cutaneous
solid malignancies compared with none receiving placebo.
In the placebo-controlled portions of the psoriasis studies, twelve of 1244 patients who received
ENBREL at any dose were diagnosed with a malignancy compared to two of 721 patients who received
placebo. Among the 1,864 patients with psoriasis who received ENBREL at any dose in the controlled
and uncontrolled portions of the psoriasis studies (3,025 patient-years), a total of 57 patients were
diagnosed with 63 malignancies; 24 patients with 25 non-cutaneous solid tumours, 32 patients with 37
non-melanoma skin cancers (17 basal, 17 squamous), and three patients with lymphoma. Among the
placebo-treated patients (90 patient-years of observation) one patient was diagnosed with two squamous
cell cancers. The size of the placebo group and limited duration of the controlled portions of studies
precludes the ability to draw firm conclusions.
Autoantibodies
Patients had serum samples tested for autoantibodies at multiple time points. In RA Studies I and II,
the percentage of patients evaluated for antinuclear antibodies (ANA) who developed new positive ANA
(1:40) was higher in patients treated with ENBREL (11%) than in placebo-treated patients (5%). The
percentage of patients who developed new positive anti-double-stranded DNA antibodies was also higher
by radioimmunoassay (15% of patients treated with ENBREL compared to 4% of placebo-treated patients)
and by Crithidia luciliae assay (3% of patients treated with ENBREL compared to none of placebo-treated
patients). The proportion of patients treated with ENBREL who developed anticardiolipin antibodies was
similarly increased compared to placebo-treated patients. In Study III, no pattern of increased autoantibody
development was seen in ENBREL patients compared to methotrexate patients.
The impact of long-term treatment with ENBREL on the development of autoimmune diseases is unknown.
Rare adverse event reports have described patients with rheumatoid factor positive and/or erosive RA
who have developed additional autoantibodies in conjunction with rash and other features suggesting
a lupus-like syndrome.
Immunogenicity
Patients with RA, psoriatic arthritis, ankylosing spondylitis or plaque psoriasis were tested at multiple time
points for antibodies to ENBREL. Non-neutralizing antibodies to the TNF receptor portion or other protein
components of the ENBREL drug product were detected at least once in sera of approximately 6% of
adult patients with RA, psoriatic arthritis, ankylosing spondylitis or plaque psoriasis. In long-term plaque
psoriasis studies, the percentage of subjects testing positive at least once for non-neutralizing antibodies
varied. Results from JIA patients were similar to those seen in adult RA patients treated with ENBREL. In
all clinical studies with ENBREL to date, there has been no apparent correlation of antibody development
to clinical response or adverse events. Neutralizing antibodies have not been observed with ENBREL.
The data reflect the percentage of patients whose test results were considered positive for antibodies
to ENBREL in an ELISA assay and are highly dependent on the sensitivity and specificity of the assay.
Additionally, the observed incidence of any antibody positivity in an assay is highly dependent on several
factors including assay sensitivity and specificity, assay methodology, sample handling, timing of sample
collection, concomitant medications, and underlying disease. For these reasons, comparison of the
incidence of antibodies to ENBREL with incidence of antibodies to other products may be misleading.
Patients with Heart Failure
Two randomized placebo-controlled studies have been performed in patients with CHF. In one study,
patients received either ENBREL 25 mg twice weekly, 25 mg three times weekly, or placebo. In a second
study, patients received either ENBREL 25 mg once weekly, 25 mg twice weekly, or placebo. Results of
the first study suggested higher mortality in patients treated with ENBREL at either schedule compared
to placebo. Results of the second study did not corroborate these observations. Analyses did not identify
specific factors associated with increased risk of adverse outcomes in heart failure patients treated with
ENBREL.
Adverse Reactions in Pediatric Patients
In general, the adverse events in pediatric patients were similar in frequency and type as those seen in
adult patients. Differences from adult and other special considerations are discussed in the following
paragraphs.
Severe adverse reactions reported in 69 JIA patients ages four to 17 years included varicella, gastroenteritis,
depression/personality disorder, cutaneous ulcer, esophagitis/gastritis, group A streptococcal septic
shock, type I diabetes mellitus, and soft tissue and post-operative wound infection.
Forty-three of 69 (62%) children with JIA experienced an infection while receiving ENBREL during the
three months of the study (part one open-label), and the frequency and severity of infections was similar
in 58 patients completing 12 months of open-label extension therapy. The types of infections reported
in JIA patients were generally mild and consistent with those commonly seen in outpatient pediatric
populations.
The following adverse events were reported more commonly in 69 JIA patients receiving three months
of ENBREL compared to the 349 adult RA patients in placebo-controlled trials. These included headache
(19% of patients, 1.7 events per patient-year), nausea (9%, 1.0 events per patient-year), abdominal pain
(19%, 0.74 events per patient-year), and vomiting (13%, 0.74 events per patient-year).
In clinical studies of children with JIA, adverse events reported in those aged two to four years were
similar to adverse events reported in older children.
In post-marketing experience, the following additional serious adverse events have been reported in
pediatric patients: abscess with bacteremia, optic neuritis, pancytopenia, neutropenia, leukopenia,
thrombocytopenia, anemia, seizures, tuberculous arthritis, urinary tract infection including urosepsis,
coagulopathy, cutaneous vasculitis, bronchitis, gastroenteritis and transaminase elevation. Other
significant adverse events have included depression. The frequency of these events and their causal
relationship to ENBREL therapy is unknown.
The long-term effects of ENBREL therapy on skeletal, behavioural, cognitive, sexual and immune
maturation and development in children are unknown.
A higher rate of adverse events was noted when JIA patients in an observational registry received
ENBREL therapy in combination with methotrexate. As the juvenile idiopathic arthritis patients receiving
combination therapy had more severe disease, since they had failed prior therapeutic trials with either
ENBREL or methotrexate alone, it remains unclear whether the higher event rate is related to therapy or
underlying disease severity.
Post-Market Adverse Drug Reactions
Additional adverse events have been identified during post-marketing use of ENBREL. Because these
events are reported voluntarily from a population of uncertain size, it is not always possible to reliably
estimate their frequency or establish a causal relationship to ENBREL exposure. These adverse events
include, but are not limited to, the following (listed by body system):
Body as a Whole: angioedema, fatigue, fever, flu syndrome, generalized pain, weight gain
Cardiovascular: chest pain, vasodilation (flushing), new-onset congestive heart failure
Digestive: altered sense of taste, anorexia, diarrhea, dry mouth, intestinal perforation
Hematologic/Lymphatic: adenopathy, anemia, aplastic anemia, leukopenia, neutropenia, pancytopenia,
thrombocytopenia
Hepatobiliary: autoimmune hepatitis, elevated transaminase
Musculoskeletal: joint pain, lupus-like syndrome with manifestations including rash consistent with
subacute or discoid lupus
Nervous: paresthesias, stroke, seizures and central nervous system events suggestive of multiple
sclerosis or isolated demyelinating conditions such as transverse myelitis or optic neuritis
Ocular: dry eyes, ocular inflammation
Respiratory: dyspnea, interstitial lung disease, pulmonary disease, worsening of prior lung disorder
Skin: cutaneous vasculitis, including leukocytoclastic vasculitis (with several symptom manifestations),
erythema multiforme, Stevens-Johnson syndrome, toxic epidermal necrolysis, pruritus, subcutaneous
nodules, urticaria
DRUG INTERACTIONS
Overview
Specific drug interaction studies have not been conducted with ENBREL. ENBREL has not been formally
evaluated in combination with other DMARDs such as gold, antimalarials, sulfasalazine, penicillamine,
azathioprine, cyclophosphamide, or leflunomide and the benefits and risks of such combinations are
unknown.
Drug-Drug Interactions
ENBREL can be used in combination with methotrexate in adult patients with rheumatoid arthritis or
psoriatic arthritis.
A higher rate of adverse events was noted when juvenile idiopathic arthritis patients in an observational
registry received ENBREL therapy in combination with methotrexate. As the juvenile idiopathic arthritis
patients receiving combination therapy had more severe disease, since they had failed prior therapeutic
trials with either ENBREL or methotrexate alone, it remains unclear whether the higher event rate is
related to therapy or underlying disease severity.
Patients in a clinical study who were on established therapy with sulfasalazine, to which ENBREL was
added, experienced a statistically significant decrease in mean white blood cell counts in comparison
to groups treated with either ENBREL or sulfasalazine alone. The significance of this observation is
unknown.
Concurrent introduction of etanercept and anakinra therapies has not been associated with increased
clinical benefit to patients. In a study in which patients with active RA were treated for up to 24 weeks with
concurrent ENBREL and anakinra therapy, a 7% rate of serious infections was observed, which was higher
than that observed with ENBREL alone (0%). Two percent of patients treated concurrently with ENBREL
and anakinra developed neutropenia (ANC <1 x 109/L).
In a study of patients with Wegener’s granulomatosis, the addition of ENBREL to standard therapy
(including cyclophosphamide) was associated with a higher incidence of non-cutaneous malignancies.
Although the role of ENBREL in this finding is uncertain, the use of ENBREL in any patients receiving
concurrent cyclophosphamide therapy is not recommended.
OVERDOSAGE
The maximum tolerated dose of ENBREL has not been established in humans.
STORAGE AND STABILITY
ENBREL single-use prefilled syringe, ENBREL single-use prefilled SureClick Autoinjector and ENBREL
multiple-use vial must be refrigerated at 2° to 8°C. DO NOT FREEZE. Keep the product in the original
carton to protect from light until the time of use. Do not shake.
Do not use beyond expiration date.
Reconstituted solutions of ENBREL prepared with the supplied Sterile Bacteriostatic Water for Injection,
USP (0.9% benzyl alcohol) may be stored in the original vial for up to 14 days at 2° to 8°C, with overall
room temperature exposure of less than 12 hours during storage and handling/usage.
Keep in a safe place out of the reach of children.
DOSAGE FORMS, COMPOSITION AND PACKAGING
ENBREL single-use prefilled syringes are available in 50 mg (0.98 mL of a 50 mg/mL solution of
etanercept, minimum deliverable volume of 0.94 mL) dosage strength. ENBREL SureClick Autoinjectors
are available in 50 mg (0.98 mL of a 50 mg/mL solution of etanercept, minimum deliverable volume of
0.94 mL) dosage strength.
Each ENBREL single-use prefilled syringe and SureClick Autoinjector contains 50 mg/mL solution of
etanercept with sucrose, sodium chloride, L-arginine hydrochloride and sodium phosphate.
ENBREL 50 mg single-use prefilled syringes and ENBREL 50 mg single-use prefilled SureClick
Autoinjectors are supplied in cartons containing four syringes or autoinjectors with 27-gauge, ½ inch
needles. A single syringe or autoinjector replacement carton is available if needed.
Administration of one 50 mg ENBREL prefilled syringe or 50 mg ENBREL SureClick Autoinjector provides a
dose equivalent to two 25 mg vials of lyophilized ENBREL, when vials are reconstituted and administered
as recommended.
ENBREL multiple-use vial reconstitution with 1 mL of the supplied Sterile Bacteriostatic Water for Injection
(BWFI), USP (containing 0.9% benzyl alcohol) yields a multiple-use, clear, and colourless solution
containing 25 mg etanercept, mannitol, sucrose, and tromethamine.
ENBREL multiple-use vial is supplied in a carton containing four dose trays. Each dose tray contains
one 25 mg vial of etanercept, one diluent syringe (1 mL Sterile Bacteriostatic Water for Injection, USP,
containing 0.9% benzyl alcohol), one 27-gauge ½ inch needle, one vial adapter, and one plunger. A single
dose replacement tray is available, if needed.
See Product Monograph for complete prescribing information.
Product Monograph available upon request. Please call 1-877-936-2735
Manufactured by Immunex Corporation, Thousand Oaks, CA 91320, U.S.A.
Distributed by Amgen Canada Inc. and Wyeth Canada.
ENBREL and SureClick are registered trademarks of Immunex Corporation.
21385A_SkinAllergy_J10:.ps 6/17/2010 6:52 PM Page 21

asis,” he said.
“Even if you do not want
to be the primary person who
is treating this patient, you still
have to think about it and
question whether there
should be therapy for that
aspect of the disease as well.”
Rapid response to etanercept
In this particular patient, Dr.
Strober indicated that they
decided to use etanercept as
a treatment option and after
six weeks of therapy she
showed a pretty rapid
response, her 18% body sur-
face area affected by psoria-
sis was reduced to 3%, and
her psoriatic arthritis, liga-
ment, and tendon symptoms
and signs abated.
At a follow-up appoint-
ment, the patient reminded
him about the yellow fever
vaccine, which she plans on
receiving in three weeks.
In this patient’s case, he
said that he stopped the etan-
ercept so the patient could
have the yellow fever vaccine
and then resumed the etaner-
cept treatment two weeks
later.
“Two weeks off the etaner-
cept gets it out of your body; it
is a simple rule. And if you stop
the etanercept two weeks
before, she can safely receive
the vaccination and then
resume [the etanercept] two
weeks after to make sure the
vaccine takes,” said Dr. Strober.
He added that the same
32-year-old woman—10
weeks later—indicated that
she was trying to get pregnant.
Should Tx be discontinued?
Dr. Strober wondered what
the audience would think
when a female patient, on
etanercept and doing well,
told their physician they were
trying to get pregnant?
He wondered if clinicians
in the audience would con-
tinue the etanercept, discon-
tinue treatment, or change
the treatment approach to
cyclosporine, or perhaps topi-
cal therapy?
“There are a lot of
options and really no right
answer,” he said. “In this
case we continued the etan-
ercept even with the woman
indicating that she is present-
ly attempting to start a family.
I told her to talk to me when
she’s pregnant and then we
will decide what treatment
will happen from that point
onward,” Dr. Strober noted.
“I just think this is a safe
drug and almost all the data
says I am right. Really, I am
not one to create risk for
unborn children. But I just
think the data are good.”
In this patient’s case, Dr.
Strober reported that they
continued treatment with
etanercept and the patient did
well, and the baby was born.
“I will tell you right now,
the moment she is pregnant,
you know she is still on etan-
ercept, she is having first
trimester exposure, there is
no doubt. The half-life of the
drug keeps it around another
two weeks. So, you are not
going to avoid exposure to
the unborn child,” he said.
“I believe that if you are
going to commit to using the
drug while she is trying to
conceive, then you are going
to have exposure in the first
trimester. There is just no way
around it, which might be the
most critical time period of
exposure for anything that is
potentially teratogenic.”
Non-proprietary and brand
names of therapies: cyclo-sporine (no branded prod-ucts); methotrexate (nobranded products); alefacept(Amevive, Astellas); etaner-cept (Enbrel, Amgen/Wyeth);infliximab (Remicade,Schering); adalimumab(Humira, Abbott); ustekinum-ab (Stelara, Janssen-Ortho).
45 mg/0.5 mL
Selective Immunomodulating Agent
(standardized incidence ratio = 0.68 [95% confidence interval: 0.29, 1.34]. Theincidence of nonmelanoma skin cancer was 0.80 per 100 patient-years offollow-up for ustekinumab-treated patients (18 patients in 2245 patient-years offollow-up). STELARA (ustekinumab) has not been studied in patients with ahistory of malignancy. Caution should be exercised when considering the use ofSTELARA in patients with a history of malignancy or when considering continuingtreatment in patients who develop a malignancy. Hepatic/Biliary/Pancreas Specificstudies have not been conducted in patients with hepatic insufficiency.Hypersensitivity Reactions If an anaphylactic or other serious allergic reactionoccurs, administration of STELARA (ustekinumab) should be discontinuedimmediately and appropriate therapy instituted (see ADVERSE REACTIONS).Immune Immunization It is recommended that live viral or bacterial vaccines notbe given concurrently with STELARA (ustekinumab). Patients receiving STELARAmay receive concurrent inactivated or non-live vaccinations (see DRUGINTERACTIONS). Immunosuppression The safety and efficacy of STELARA(ustekinumab) in combination with immunosuppressive agents or phototherapyhave not been evaluated. Caution should be exercised when consideringconcomitant use of immunosuppressive agents and STELARA. InfectionsSTELARA (ustekinumab) is a selective immunomodulator and may have thepotential to increase the risk of infections and reactivate latent infections. Inclinical studies, serious bacterial, fungal, and viral infections have been observedinfrequently in patients receiving ustekinumab. STELARA (ustekinumab) shouldnot be given to patients with an existing clinically important, active infection.Caution should be exercised when considering the use of STELARA in patientswith a chronic infection or a history of recurrent infection. Prior to initiatingtreatment with STELARA (ustekinumab), patients should be evaluated fortuberculosis infection. STELARA should not be given to patients with activetuberculosis. Treatment of latent tuberculosis infection should be initiated prior toadministering STELARA. Anti-tuberculosis therapy should also be consideredprior to initiation of STELARA in patients with a past history of latent or activetuberculosis in whom an adequate course of treatment cannot be confirmed. Inclinical studies, patients with latent tuberculosis who were concurrently treatedwith isoniazid did not develop tuberculosis. Patients receiving STELARA should bemonitored closely for signs and symptoms of active tuberculosis during and aftertreatment. Patients should be instructed to seek medical advice if signs orsymptoms suggestive of an infection occur. If a patient develops a seriousinfection, they should be closely monitored and STELARA (ustekinumab) shouldnot be administered until the infection resolves (see ADVERSE REACTIONS). RenalSpecific studies have not been conducted in patients with renal insufficiency.
ADVERSE REACTIONS
The following is a summary of the ADVERSE REACTIONS section. For additionalinformation, including tables and sections where only headings appear, seeSupplemental Product Information. Adverse Drug Reaction Overview The followingserious adverse reactions were reported: • Serious Infections • Malignancies.The most common adverse reactions (>10%) in controlled and uncontrolledportions of the psoriasis clinical studies with STELARA (ustekinumab) werenasopharyngitis and upper respiratory tract infection. Most were considered to bemild and did not necessitate drug discontinuation. Clinical Trial Adverse DrugReactions The safety data described below reflect exposure to STELARA(ustekinumab) in 3 placebo-controlled studies of 2266 patients, including 1970exposed for at least 6 months, 1285 exposed for at least 1 year and 373 for atleast 18 months. Table 1.1 summarizes the adverse drug reactions that occurredat a rate of at least 1% and at a higher rate by preferred term in the STELARA(ustekinumab) group during the placebo-controlled period of the Phase 3 studies(PHOENIX 1 and PHOENIX 2).
Table 1.1 Adverse drug reactions reported by �1% of patients through Week 12 in
PHOENIX 1 and II
Placebo STELARA (ustekinumab)
45 mg 90 mg
Patients treated 665 664 666
Nasopharyngitis 51 (7.7%) 56 (8.4%) 49 (7.4%)
Upper respiratory tract infection 30 (4.5%) 36 (5.4%) 28 (4.2%)
Headache 23 (3.5%) 33 (5.0%) 32 (4.8%)
Fatigue 14 (2.1%) 18 (2.7%) 17 (2.6%)
Diarrhea 12 (1.8%) 13 (2.0%) 13 (2.0%)
Back pain 8 (1.2%) 9 (1.4%) 14 (2.1%)
Dizziness 8 (1.2%) 8 (1.2%) 14 (2.1%)
Pharyngolaryngeal pain 7 (1.1%) 9 (1.4%) 12 (1.8%)
Pruritus 9 (1.4%) 10 (1.5%) 9 (1.4%)
Injection site erythema 3 (0.5%) 6 (0.9%) 13 (2.0%)
Myalgia 4 (0.6%) 7 (1.1%) 8 (1.2%)
Depression 3 (0.5%) 8 (1.2%) 4 (0.6%)
PRESCRIBING SUMMARY
IMPORTANT: Before making prescribing decisions, please refer to complete ProductMonograph at www.janssen-ortho.com or request a hard copy from Janssen-OrthoInc. Medical Information Services (800) 567-3331.
Patient Selection Criteria
INDICATIONS AND CLINICAL USE
STELARA (ustekinumab) is indicated in adult patients for the treatment of chronicmoderate to severe plaque psoriasis who are candidates for phototherapy orsystemic therapy.
Special Populations Pregnant Women: There is no evidence from animal studies ofteratogenicity, birth defects or developmental delays at dose levels up toapproximately 45-fold higher than the highest equivalent dose intended to beadministered to psoriasis patients. However, animal reproductive anddevelopmental studies are not always predictive of human response. It is notknown whether STELARA (ustekinumab) can cause fetal harm when administeredto a pregnant woman or whether it can affect reproductive capacity. While it isknown that human IgG antibodies, like ustekinumab, cross the placenta, noadequate and well-controlled studies have been conducted to evaluate ifustekinumab can cross the human placenta in pregnant women. In developmentaltoxicity studies in monkeys, ustekinumab was detected in fetal serum followingrepeated dosing of pregnant monkeys during the period of organogenesis.Although ustekinumab crossed the monkey placenta there was not evidence ofteratogenicity in these studies. STELARA should be given to a pregnant womanonly if the benefit clearly outweighs the risk. Nursing Women: Ustekinumab isexcreted in the milk of lactating monkeys administered ustekinumab. It is notknown if ustekinumab is absorbed systemically after ingestion. Because manydrugs and immunoglobulins are excreted in human milk, and because of thepotential for adverse reactions in nursing infants from ustekinumab, a decisionshould be made whether to discontinue nursing or to discontinue the drug.Pediatrics (<18 years of age): Specific studies of STELARA (ustekinumab) inpediatric patients have not been conducted. Geriatrics (>65 years of age): No majorage-related differences in clearance or volume of distribution were observed inclinical studies. While the experience in the elderly is limited, no overall differencesin efficacy or safety in patients age 65 and older [N=131] who receivedustekinumab were observed compared with younger patients.
CONTRAINDICATIONS
• Patients with known hypersensitivity to STELARA or any of its components. • Patientswith severe infections such as sepsis, tuberculosis and opportunistic infections (seeWARNINGS AND PRECAUTIONS, Infections).
Safety Information
WARNINGS AND PRECAUTIONS
Carcinogenesis and Mutagenesis STELARA (ustekinumab) is a selectiveimmunomodulator. Immunomodulating agents have the potential to increase therisk of malignancy. Some patients who received ustekinumab in clinical studiesdeveloped malignancies (see ADVERSE REACTIONS). In the controlled and non-controlled portions of psoriasis clinical studies, the incidence of malignanciesexcluding nonmelanoma skin cancers was 0.36 per 100 patient-years offollow-up for ustekinumab-treated patients (8 patients in 2249 patient-years offollow-up) and included breast, colon, head and neck, kidney, prostate, andthyroid cancers. The rate of malignancies reported in ustekinumab-treatedpatients was comparable to the rate expected in the general population
36 · June 2010 THE CHRONICLE of SKIN & ALLERGY
Psoriasis: Considerations for pregnant, pediatric patientsContinued from page 13
Message from theMedical Editor
Continued from page 3empower other associations
to work with their govern-
ments to implement pro-
grams that will be life saving.
Well done Canadian der-
matology. Let’s continue the
great work in maintaining
our leadership role on the
world stage in so many areas
as it will only result in
enhanced care and better
outcomes for our patients.
—Wayne P. Gulliver,MD, FRCPC
Medical Editor
21385A_SkinAllergy_J10:.ps 6/17/2010 6:53 PM Page 22

THE CHRONICLE of SKIN & ALLERGY June 2010 · 37
JULY 201015-18 36th Annual
Meeting of the Society forPediatric Dermatology
Portland, Ore.Contact: Meeting organizer ¶ Tel:317-202-0224 ¶ Fax:317-205-9481 ¶Email:[email protected]
AUGUST 201004-08 2010 Summer
(Academy) Meeting of theAmerican Academy of
Dermatology
ChicagoContact: Meeting organizer ¶ Tel:
866-503-SKIN (7546) / 847-240-1280 ¶
Fax: 847-240-1859 ¶ Email:
06-07 InternationalCongress of Therapeutic
Dermatological Bahia de Caraquez, Ecuador
Contact: Luis Palacios ¶Email:[email protected]
06-16 Dermatology &Aesthetics: Mediterranean
CME Cruise Conference Rome
Contact: Martin Gerretsen MD ¶Tel:1-888-647-7327 ¶ Fax:1-888-547-7337 ¶ Email:[email protected]
SEPTEMBER 2010
09-11 40th Annual Meetingof the European Society forDermatological Research
(ESDR) Helsinki, Finland
Contact: ESDR Secretariat ¶ Tel:41-22-321-4890 ¶ Fax:41-22-321-4892
17-18 Perspectives inMelanoma XIV
Amsterdam
Contact: Latasha Milner ¶ Phone: 1-
678-242-0906 ¶ Fax: 1-678-242-0920 ¶
Email: [email protected]
23-25 25th IUSTI EuropeConference Tbilisi, Georgia
Contact: Tamuna Guniava or OlegKvlividze ¶ Tel:995-90-809-015 or 995-90-809-025 ¶ Fax:995-32-957-330 ¶Email:[email protected]
25 The Management ofWomen with Chronic
Immune Disorders in theEra of Biologics
New York CityContact: Tel: 678-242-0906 ¶ Fax: 678-
242-0920 ¶ Email: meet-
25-26 6th National Laserand Cosmetic Medicine
Conference Surfers Paradise,
Queensland, AustraliaContact: Conference Secretariat: DCConferences ¶ Tel:612-9954-4400 ¶Fax:612-9954-0666 ¶ Email:[email protected]
30 Pan American Societyfor Pigment Cell Research2010 Annual Conference
VancouverContact: Meeting Organizer ¶ Tel: 1(604) 875-5101 ¶ Fax: 1 (604) 875-5078¶ Email: [email protected]
OCTOBER 2010
6-10 19th Congress of theEuropean Academy of
Dermatology andVenereology (EADV)
Gothenburg, Sweden Contact: EADV Office ¶ Tel: 322-650-0090 ¶ Fax:322-650-0098 ¶Email:[email protected]
13-15 4th Congress onRegenerative Biology and
Medicine Stuttgart, Baden-Wuerttemberg,
Germany Contact: Dr. Thomas Grieshammer ¶Tel: 49-711-8703-54-28 ¶ Fax: 49-711-8703-54-44 ¶ Email: [email protected]
10-14 EMAA 2010 -European Masters in
Aesthetic & Anti-AgingMedicine
ParisContact: Christophe Luino ¶ Tel: 01-56-837-800 ¶ Fax:01-56-837-805 ¶Email: [email protected]
21-24 2010 ASDS (AmericanSociety for DermatologicSurgery) Annual Meeting
ChicagoContact: ASDS ¶ Tel: 847-956-0900
NOVEMBER 2010
04-07 The 1st WorldCongress on Controversies
in Plastic Surgery &Dermatology (CoPLASDy)
BarcelonaContact: Congress Secretariat ¶ Tel:97-235-666-166 ¶ Email: [email protected]
04-07 CanadianAssociation of Wound Care
Annual ProfessionalConference
CalgaryContact: Tel: 416-485-2292/toll free: 1-
866-474-0125 ¶ Fax: 416-485-2291 ¶
Email: [email protected]
07-10 The 8th Asia PacificCongress of Allergy,Asthma and Clinical
Immunology Singapore
Contact: Stella Chee ¶ Tel: 65-63-795-259 ¶ Fax:65-64-752-077 ¶ Email:[email protected]
Infections: In placebo-controlled studies of psoriasis patients, the rates ofinfection or serious infection were similar between ustekinumab-treated patientsand those treated with placebo. In the placebo-controlled period of clinical studiesof psoriasis patients, the rate of infection was 1.39 per patient-year of follow-upin ustekinumab-treated patients, and 1.21 per patient-year of follow-up inplacebo-treated patients. Serious infections occurred in 0.01 per patient-year offollow-up in ustekinumab-treated patients (5 serious infections in 407 patient-years of follow-up) and 0.02 per patient-year of follow-up in placebo-treatedpatients (3 serious infections in 177 patient-years of follow-up) (see WARNINGSAND PRECAUTIONS). In the controlled and non-controlled portions of placebo-controlled psoriasis clinical studies, the rate of infection was 1.24 per patient-year of follow-up in ustekinumab-treated patients. The incidence of seriousinfections was 0.01 per patient-year of follow-up in ustekinumab-treated patients(24 serious infections in 2251 patient-years of follow-up) and included cellulitis,diverticulitis, osteomyelitis, viral infections, gastroenteritis, pneumonia, andurinary tract infections. Malignancies: In the placebo-controlled period of thepsoriasis clinical studies, the incidence of non-melanoma skin cancer was 0.74per 100 patient-years of follow-up for ustekinumab-treated patients (3 patients in406 patient-years of follow-up) compared with 1.13 per 100 patient-years offollow-up for placebo-treated patients (2 patient in 176 patient-years of follow-up) during the placebo-controlled periods. In a Phase 3 clinical trial (ACCEPT)comparing ustekinumab and etanercept for the treatment of moderate to severeplaque psoriasis, 209 patients received ustekinumab 45 mg, 347 patientsreceived ustekinumab 90 mg, and 347 patients received etanercept. ThroughWeek 12, three (0.5%) subjects in the ustekinumab groups had a non-melanomaskin cancer detected in areas of psoriasis that had cleared with treatment. Noskin cancers were observed in the etanercept group but due to the shorttreatment period, the possible pre-existing malignancies and the differences inefficacy, the clinical relevance has not been established. The incidence ofmalignancies excluding non-melanoma skin cancer was 0.25 per 100 patient-years of follow-up for ustekinumab-treated patients (1 patient in 406 patient-years of follow-up) compared with 0.57 per 100 patient-years of follow-up forplacebo-treated patients (1 patient in 177 patient-years of follow-up) during theplacebo-controlled periods. In the ACCEPT trial, through Week 12, one subject(0.2%) with a familial history of breast cancer was diagnosed with breast cancerversus no malignancies in the etanercept group. In the controlled and non-controlled portions of the placebo-controlled psoriasis clinical trials, the incidenceof malignancies excluding non-melanoma skin cancers was 0.36 per 100patient-years of follow-up for ustekinumab-treated patients (8 patients in 2249patient-years of follow-up) and included breast, colon, head and neck, kidney,prostate, and thyroid cancers. The rate of malignancies reported in ustekinumab-treated patients was comparable to the rate expected in the general population(standardized incidence ratio = 0.68 [95% confidence interval: 0.29, 1.34]. Theincidence of non-melanoma skin cancer was 0.80 per 100 patient-years offollow-up for ustekinumab-treated patients (18 patients in 2245 patient-years offollow-up). Hypersensitivity Reactions: In clinical studies of ustekinumab, rash andurticaria have each been observed in <2% of patients. Immunogenicity:Approximately 5% of patients treated with ustekinumab developed antibodies toustekinumab, which were generally low-titer. No apparent correlation of antibodydevelopment to injection site reactions was seen. Patients positive for antibodiesto ustekinumab exhibited median serum levels of ustekinumab that wereconsistently lower that those in patients negative or undetectable for antibodiesto ustekinumab and tended to have lower efficacy; however, antibody positivitydoes not preclude a clinical response. Less Common Clinical Trial Adverse DrugReactions (<1%) The following adverse drug reactions occurred at rates less than1% during the psoriasis clinical trials: Infections and infestations: cellulitis Generaldisorders and administration site conditions: injection site reactions (includingpain, swelling, pruritus, induration, hemorrhage, bruising and irritation) AbnormalHematologic and Clinical Chemistry Findings During the placebo-controlled periodof the Phase 2 and Phase 3 studies (through week 12), an increase in non-fastingblood glucose levels was observed, as follows: Subjects with any abnormal value:49 (6.7%) placebo vs. 83 (5.3%) in the combined ustekinumab group; Subjectswith >1 abnormal value: 9 (1.2%) placebo vs 35 (2.2%) in the combinedustekinumab group. The clinical significance of these changes in glucose isunknown. No such increase in fasting blood glucose levels was observed in thesame subjects.
Post-Market Adverse Drug Reactions
To report an adverse event or a side effect, contact Janssen Ortho Drug Safety:
Tel: (416) 382-5105 or 1-800-567-3331Fax: (416) 382-5982 or 1-866-767-5865
DRUG INTERACTIONS
Overview Specific drug interaction studies have not been conducted withSTELARA (ustekinumab). In population pharmacokinetic analysis, the effect of themost frequently used concomitant medications in patients with psoriasis
(including paracetamol/acetaminophen, ibuprofen, acetylsalicylic acid,metformin, atorvastatin, naproxen, levothyroxine, hydrochlorothiazide, andinfluenza vaccine) on pharmacokinetics of ustekinumab was explored and noneof the concomitant medications exerted significant impact. The pharmacokineticsof ustekinumab was not impacted by the prior use of methotrexate, cyclosporine,or other biological therapeutics for the treatment of psoriasis. Drug-DrugInteractions Live Vaccines Live vaccines should not be given concurrently withSTELARA (ustekinumab) (see WARNINGS AND PRECAUTIONS). Immuno-suppressants The safety and efficacy of STELARA (ustekinumab) in combinationwith immunosuppressive agents or phototherapy have not been evaluated (seeWARNINGS AND PRECAUTIONS). Drug-Food Interactions Interactions with foodhave not been established. Drug-Herb Interactions Interactions with herbalproducts have not been established. Drug-Laboratory Interactions Interactionswith laboratory tests have not been established. Drug-Lifestyle Interactions Thepharmacokinetics of ustekinumab were not impacted by the use of tobacco oralcohol.
Administration
DOSAGE AND ADMINISTRATION
STELARA (ustekinumab) is administered by subcutaneous injection. DosingConsiderations STELARA (ustekinumab) is intended for use under the guidanceand supervision of a physician. A patient may self-inject with STELARA(ustekinumab) if a physician determines that it is appropriate after proper trainingin subcutaneous injection technique. Prior to subcutaneous administration,visually inspect the solution in the STELARA (ustekinumab) vial for particulatematter and discoloration. The product is colourless to light yellow and maycontain a few small translucent or white particles of protein. This appearance isnot unusual for proteinaceous solutions. The product should not be used ifsolution is discolored or cloudy, or if other particulate matter is present. STELARA(ustekinumab) does not contain preservatives; therefore, any unused productremaining in the vial and syringe should not be used. Patients should beinstructed to inject the full amount of STELARA (ustekinumab) according to thedirections provided in the CONSUMER INFORMATION Section (see ProductMonograph, Part III: CONSUMER INFORMATION Section). Recommended Dose andDosage Adjustment The recommended dose of STELARA (ustekinumab) is 45 mgadministered at Weeks 0 and 4, then every 12 weeks thereafter. Alternatively,90 mg may be used in patients with a body weight greater than 100 kg. Inpatients weighing >100 kg, both 45 mg and 90 mg were shown to beefficacious. However, 90 mg was efficacious in a higher percentage of thesepatients than the 45 mg dose. For patients who inadequately respond to dosingevery 12 weeks, consideration may be given to treating as often as every 8weeks. Consideration should be given to discontinuing treatment in patients whohave shown no response up to 12 weeks of treatment. Re-treatment Re-treatment with a dosing regimen of Weeks 0 and 4 followed by 12 week dosingafter interruption of therapy has been shown to be safe and effective.
Study References
Supplemental Product Information
OVERDOSAGE Single doses up to 4.5 mg/kg intravenously have been administered in clinical studies without dose
limiting toxicity. In case of overdosage, it is recommended that the patient be monitored for any signs or symptoms
of adverse reactions or effects and appropriate symptomatic treatment be instituted immediately.
Product Monograph available at www.janssen-ortho.com or from Janssen-Ortho Inc. Medical Information Services
(800) 567-3331.
Janssen-Ortho Inc., Toronto, Ontario M3C 1L9
Date of Issuance: December 2008 STPI080871E
© 2008 JANSSEN-ORTHO Inc.
* All trademark rights used under license
Agenda
21385A_SkinAllergy_J10:.ps 6/22/2010 8:49 AM Page 23

38 ·June 2010
Journal ClubTHE CHRONICLE of SKIN & ALLERGY
WHEN BRACELET CHANGES
COLOR, IT’S TIME TO REAPPLY
THE SUNSCREEN
Consumers can now purchase a plastic
bracelet that changes color to remind
the wearer when it is time to re-apply
sunscreen, reports the Chicago Sun-
Times (April 14, 2010).
The bracelet called UVSunSense is
orange when it is taken out of its pack-
age, then turns purple when it encoun-
ters sunlight. The manufacturer indi-
cates that in order for the bracelet to
work users must apply sunscreen onto
the band, which eventually turns brown
to remind people that it is time to re-
apply sunscreen. The UVSunSense
costs $6.95 U.S. for a pack of seven
bands.
BREASTFEEDING FOR LONGER
PERIODS APPEARS TO INCREASE
RISK OF DEVELOPING ECZEMA
Data published in the Journal of Allergy
and Clinical Immunology reveals that
infants who breastfeed for longer peri-
ods of time are more likely to contract
eczema, reports Reuters Health
(March 26, 2010). During the study
researchers from Denmark conducted
an analysis of more than 320 infants.
Findings indicated that 55% of babies
who were breastfed exclusively for
more than six months developed
eczema by age two. Only 37% of the
babies, however, who were breastfed
for less than six months developed
eczema. Researchers conclude that
while in the past breastfeeding has
been recommended as a way to pre-
vent allergic conditions in infants, sci-
entists are now suggesting that breast-
feeding should not be viewed as a way
to prevent eczema in high-risk infants.
COULD MOTHER’S MILK PROVIDE
AN ACNE CURE?
University of California scientists sug-
gest they have developed a face cream
that is derived from breast milk and
that might be beneficial in the treat-
ment of acne, reports the U.K. Daily
Mail (April 17, 2010).
The component ingredient of
mother’s milk used in the cream is lau-
ric acid which, according to
researchers, can help reduce irritation
and spots caused by acne. The cream
incorporates tiny gold particles to carry
lauric acid into pores where it can fight
bacteria.
According to the scientists, the
cream is currently being assessed in
clinical trials.
AND TONIGHT THE SUSHI
RESTAURANT IS OFFERING . . .
A beauty regimen that uses toothless
fish to help exfoliate feet and treat
other skin conditions has been
launched in Dubai, reports Business
Standard (April 3, 2010). The treatment
is available to patrons at Dubai’s Wild
Wadi Waterpark.
The new treatment, FISHO, provid-
ed by Dubai-based Jumeirah Group,
employs Garra Ruffa fish to help
remove the dead skin cells of their
clients, which aids in the improvement
of circulation and other conditions.
The cost of the treatment?
Approximately $15 for adults and $11
for children.
Research of Note
PIMECROLIMUS MOST EFFECTIVE ON THE FACE IN LOCALIZED VITILIGO
Arecent comparison study suggests that mometasone cream is effective in the treatment
of vitiligo on any part of the body, while in childhood localized vitiligo pimecrolimus is
just effective on the face, not the body.
Overall, 40 patients with childhood vitiligo were included in this study. Each of the partici-
pants were treated for three months either with mometasone cream (0.1%) once daily or with
pimecrolimus cream (1%) twice daily. Findings show the two drugs were found to be statistical-
ly significantly effective for diminishing lesion size (Z=3.070, p=0.002 and Z=3.845, p<0.001,
respectively). There were no statistical differences between the two drugs: Z=1.427, p=0.154
(mometasone non-inferiority to pimecrolimus). The mean repigmentation rate was 65% in the
mometasone group and 42% in the pimecrolimus group at the end of therapy. Atrophy, telang-
iectasia, and erythema were observed in two patients (10%) in the mometasone cream group
and a burning sensation and pruritus were observed in two patients (10%) in the pimecrolimus
cream group; drop-out was not related to the observed adverse effects.
Köse O, Arca E, Kurumlu Z: Mometasone cream versus pimecrolimus cream for the treatment ofchildhood localized vitiligo, in Journal of Dermatology Treatment May 2010; 21(3):133-139.
PSORIASIS: BENEFIT OF ANTI-TNF THERAPY OUTWEIGHS RISK
Data show that a psoriasis patient is more likely to achieve benefit through anti-TNF
therapy than to be at risk for serious toxicity. During this integrated analysis of pub-
lished literature, investigators calculated the number needed to treat (NNT) for various
efficacy measures and the number needed to harm (NNH) for various adverse events for
approved dosing regimens of adalimumab, etanercept, and infliximab. The authors indicate that
integrated analyses that included open-label safety data from tumor necrosis factor (TNF)-
antagonist clinical trials were also conducted.
Overall, the PASI 75 treatment effect data from the literature show NNT values to be 1.6
(95% confidence interval, CI 1.5 to 1.7) for adalimumab 40 mg every other week; 3.2 (95% CI 2.8
to 3.7) for etanercept 50 mg weekly or 25 mg twice weekly, and 2.3 (95% CI 2.1-2.5) for etaner-
cept 50 mg twice weekly; and 1.4 (95% CI 1.3-1.5) for infliximab 5 mg kg(-1) dosing. In all, for
serious noninfectious, serious infectious, and malignant adverse events, point estimates of the
NNHs were generally at least two orders of magnitude larger than the NNTs, and the 95% CIs for
the NNHs for adalimumab, etanercept, and infliximab overlap.
The authors concluded that increased exposure to study agents resulted in a low risk of
adverse events during observed placebo-controlled trial periods suggesting that the likelihood of
success with anti-TNF therapy for psoriasis was several orders of magnitude greater than the
likelihood of serious toxicity.
Langley RG, Strober BE, Gu Y, Rozzo SJ, Okun MM: Benefit-risk assessment of tumour necrosisfactor antagonists in the treatment of psoriasis, in the April online edition
of the British Journal of Dermatology..
What THE LAY PRESS is saying about . . .
Department Editor: Lynn Bradshaw
Coming in the
next issue of
The Chronicle
Watch for Chronicle’sannual Special Report
on the diagnosis and treatmentof the herpetic syndrome
Diagnostic Quiz
A. Polymorphous light eruptionB. Erythropoietic protoporphyria
C. Urticaria, solar
THE EDITORS invite your participation in this regular
feature of the journal. Please send all images and
correspondence to: Medical Editor,
The Chronicle of Skin & Allergy
555 Burnhamthorpe Road, Suite 306,
Toronto, Ont. M9C 2Y3. Telephone: (416) 916-2476
Correct answer: Erythropoietic protoporphyria
21385A_SkinAllergy_J10:.ps 6/22/2010 8:23 AM Page 30

TARGET: PASI 100
and after. . .
Aiming with the confi dence of experience• During fi ve years in Canadian practice and 12 years
clinical experience worldwide, over 340,000 patients have been treated with HUMIRA for RA, PsA, AS,
CD and psoriasis3,4
• Approximately one in four HUMIRA psoriasis patients achieved full skin clearance at week 24(HUMIRA PASI 100: 22%; PGA clear: 24%, n = 580)1
• As early as week 16, 80% of patients achieved PASI 75(PASI 75 at week 16: HUMIRA 79.6%, n =108; MTX 35.5%,
n =110; placebo 18.9%, n = 53; p < 0.001 vs. MTX and placebo)2
• HUMIRA has demonstrated sustained skin clearance to one year(PASI 75 responders: week 16: 71% [n = 814] vs. 7% for placebo
[n = 398], p < 0.001; week 24: 70% for HUMIRA patients;‡
week 52: only 5% of patients lost adequate response§ vs. 28%
for placebo, p < 0.001)1
and after. . .
After†. . .Before
What sustained skinclearance could look like.
See prescribing summary and study parameters on page
HUMIRA is indicated for the treatment of adult patients with chronic moderate to severe psoriasis who are candidates for systemic therapy. For patients with chronic moderate plaque psoriasis, HUMIRA should be used after phototherapy has been shown to be ineffective or inappropriate. HUMIRA is also indicated in:
Psoriatic arthritis (PsA): for reducing the signs and symptoms of active arthritis and inhibiting the progression of structural damage and improving the physical function in adult PsA patients. HUMIRA can be used in combination with methotrexate (MTX) in patients who do not respond adequately to MTX alone.
Rheumatoid arthritis (RA): for reducing the signs and symptoms, inducing major clinical response and clinical remission, inhibiting the progression of structural damage and improving physical function in adult patients with moderately to severely active RA. HUMIRA can be used alone or in combination with MTX or other disease-modifying anti-rheumatic drugs (DMARDs). When used as fi rst-line treatment in recently diagnosed patients who have not been previously treated with MTX, HUMIRA should be given in combination with MTX. HUMIRA can be given as monotherapy in case of intolerance to MTX or when treatment with MTX is contraindicated.
Ankylosing spondylitis (AS): for reducing signs and symptoms in patients with active AS who have had an inadequate response to conventional therapy.
Crohn’s disease (CD): for reducing signs and symptoms and inducing and maintaining clinical remission in adult patients with moderately to severely active CD who have had an inadequate response to conventional therapy, including corticosteroids and/or immunosuppressants. HUMIRA is indicated for reducing signs and symptoms and inducing clinical remission in these patients if they have also lost response to or are intolerant to infl iximab.
The most frequently reported adverse events in psoriasis clinical trials were: injection site reaction (3.0%), headache (2.0%) and injection site irritation (1.7%).
HUMIRA is contraindicated in patients with severe infections such as sepsis, tuberculosis and opportunistic infections.
Serious infections due to bacterial, mycobacterial, invasive fungal (disseminated or extrapulmonary histoplasmosis, aspergillosis, coccidioidomycosis), viral, or other opportunistic infections have been reported in patients receiving TNF-blocking agents. Sepsis, rare cases of tuberculosis, candidiasis, listeriosis, and pneumocystis have also been reported with the use of TNF-blocking agents, including HUMIRA (adalimumab). Other serious infections seen in clinical trials include pneumonia, pyelonephritis, septic arthritis and septicemia. Hospitalization or fatal outcomes associated with infections have been reported. Many of the serious infections have occurred in patients on concomitant immunosuppressive therapy that, in addition to their underlying disease, could predispose them to infections. Treatment with HUMIRA should not be initiated in patients with active infections, including chronic or localized infections, until infections are controlled. In patients who have been exposed to tuberculosis, and patients who have travelled in areas of high risk of tuberculosis or endemic mycoses, such as histoplasmosis, coccidioidomycosis, or blastomycosis, the risk and benefi ts of treatment with HUMIRA should be considered prior to initiating therapy. As with other TNF antagonists, patients should be monitored closely for infections – including tuberculosis – before, during, and after treatment with HUMIRA. Patients who develop a new infection while undergoing treatment with HUMIRA should be monitored closely and undergo a complete diagnostic evaluation. Administration of HUMIRA should be discontinued if a patient develops a serious infection or sepsis, and appropriate antimicrobial or antifungal therapy should be initiated. Physicians should exercise caution when considering the use of HUMIRA in patients with a history of recurrent infection or with underlying conditions which may predispose them to infections, or patients who have resided in regions where tuberculosis and histoplasmosis are endemic. The benefi ts and risks of treatment with HUMIRA should be carefully considered before initiating therapy. Very rare post-marketing reports of hepatosplenic T-cell lymphoma (HSTCL), a rare aggressive lymphoma that is often fatal, have been identifi ed in patients treated with adalimumab. Most of the patients had prior infl iximab therapy as well as concomitant azathioprine or 6-mercaptopurine use for Crohn’s disease. The causal association of HSTCL with adalimumab is not clear.
Product Monograph available on request.
‡ Pooled effi cacy outcomes from the 17-week open-label period and the open-label extension.§ Defi ned as < 50% improvement in the PASI response relative to baseline and at least
a 6-point increase in PASI score relative to week 33.
† Fictitious case. Individual case may not be representative of the general population. HUMIRA has demonstrated skin clearance up to 52 weeks.1
© Abbott Laboratories, Limited www.abbott.ca
1-800-361-7852
See prescribing summary on page 31
21385A_SkinAllergy_J10:.ps 6/22/2010 8:25 AM Page 31
Tolérance extrêmeA dermo-cosmetics breakthrough
Innovation in Dermatology
INNOVATION
For hypersensitive and allergic skin
Preservative Fragrance Emulsifier
For the first time, it is possible to keepa formula totally sterile in a large tube (50 ml),
shielded from bacteria during the entire time it is used.
An innovative and unique combination of two patentedprocesses*:
ETS concept (Extreme
manufacturing and conditioning in a sterile environment, with no potential irritants.
D.E.F.I pure and safe product thanks to its exclusive patented closure device. It
intact and germ free throughout the product’s life span.
*Patents pending.
D E F IE I F D
21385A_SkinAllergy_J10:.ps 6/17/2010 6:58 PM Page 32


















