Prick Skin Test Proficiency - Confex · Prick Skin Test Proficiency AAAAI 2014 John Oppenheimer MD...
38
Prick Skin Test Proficiency AAAAI 2014 John Oppenheimer MD UMDNJ-Rutgers Medical School Pulmonary and Allergy Assoc
Transcript of Prick Skin Test Proficiency - Confex · Prick Skin Test Proficiency AAAAI 2014 John Oppenheimer MD...

Prick Skin Test ProficiencyAAAAI 2014
John Oppenheimer MD
UMDNJ-Rutgers Medical School
Pulmonary and Allergy Assoc

Potential COI
• Consultant: AZ, Sanofi, Celgene, Glaxo, Myelin, Teva, Sonovion
• Research: Medimmune, Genetec, BI
• Adjudication: AZ, Novartis
• DSMB: Ohio State Med School
• Annals of Allergy – Assoc Editor
• ABAI - Chair

How often have you seen a new patient with
skin tests results such as these?
• Hist /
• Control
• Cat 1
• Dog 1
• Alt 2
• Clad 2
• Pcm 2
• Asp 2
• Dust mite (f) 2
• Dust mite (p) 3
• trees 3
• timothy 2
• ragweed 3
General Rules of Success
• It is imperative that the technician performing the skin tests as well as the clinician ordering/interpreting these tests understand the characteristics of the specific tests they are administering.
• This includes:
– type of skin testing
– device used
– placement of tests (location and adjacent testing)
– the particular extracts being used
– the potential confounder of medications that may suppress skin test response.
Oppenheimer Nelson Ann Allergy 2006;96:19-23

Variables in
Allergy Skin Testing
• Uncontrollable
• Controllable

Uncontrollable Variables
• Chronobiology:- Diurnal- Seasonal
• Menstrual Cycle:
• Age:- Specific IgE- Histamine Reactivity
• Location on Body:- Variations on Back- Back vs. Forearm

Controllable Variables
• Medications:
- H1 Antihistamines
- H2 Antihistamines
- Antidepressants
- Corticosteroids
- Immunotherapy
• Relation to adjacent positive reactions.
• Extract quality
• Skin testing devices

General Rules of Success
• Clinicians must consider controllable
variables that affect results and their
interpretation
• When not considered this may be
responsible for the inaccuracies
associated with skin testing
Oppenheimer & Nelson Ann All 2006;96:19-23

Effect of Allergen
• Data were compiled from 123 sequential
skin test subjects, all of whom had skin
testing with conventional dog extract and
AP dog extract*– 59 patients were prick skin test positive to AP dog,
mean wheal 6.9 mm.
– 35 (59%) were positive to aqueous dog, mean wheal
3.4 mm (all were also A-P +).
JB Meiser, HS Nelson JACI 2001;107:744-5
*conventional dog extract contains about 5g/mL of Cand 1.
A-P dog contained about 180 g/mL.

Allergen Quality Also Impacts InVitro Testing
• Just like skin testing, the allergen used in the solid phase is of great importance– characterization
– insure that Ag epitopes are not lost in preparing the solid phase
– Ag epitopes should be in excess to maximize binding of IgE antibody
– If not in excess, can have competitive binding from antibody of other isotypes (IgG)
– Ag excess, can bind in an affinity – independent fashion
Johansson Clin Rev Allergy 1988;6:93-139
Yunginger JACI 2000;105:1077-84

The Quest for the Best
Technique/Method

Skin Testing…in the beginning:• In a 1931 report, Rapaport
described a multiple scarifier – the Mueller device .
• He noted that a significant problem with the scarification technique was a lack of uniformity in the abrasion.
• The Mueller device was designed to make six uniform abrasions 1-½ mm long and 15 mm apart. This level of uniformity was felt to be a great innovation in the attainment of reproducible skin testing and reduction in the pain associated with the skin testing procedure.
Jl of Allergy. 1931;2:379-80.

Effect of Device
• Potential causes of skin test variability include depth of penetration into the skin, (amount of antigen entering the cutis vera) as well as the angle of penetration, and skill of the investigator.
• It is for this reason that Brown and Thantrey examined optimal needle length in their 1981 report.
• To do so they developed an adjustable needle that was jabbed into the skin at a right angle through an extract of 1mg/mL histamine hydrochloride. They found that a length of 1mm resulted in the largest wheal response.
• With longer needle lengths, no greater wheal size was seen; however, bleeding did occur.
JACI 1988;82:487
Clin All 1981;11:95-8.

Studies of skin testing devices
• There have been numerous studies comparing
multiple devices simultaneously
• The devices for percutaneous testing vary in the
degree of trauma that they impart to the skin.
• Therefore they differ in the size of positive
reactions and also in the likelihood of
producing a reaction at the site of the
negative control.
• Thus, they require different criteria for what
constitutes a positive reaction.

Skin Test Survey: Results
Multitest 25.5% DermaPik (prick technique): 20.5%Other: 20%DuoTip (prick technique): 12.2%Quintest 11.8%DermaPik (twist technique): 7.2%Smallpox needle: 4.1%DuoTip (twist technique): 2.7%
A questionnaire was sent via the Internet to all US physician members and
fellows of the ACAAI. This survey explored choices regarding skin testing
(539 respondents).
There was significant variability regarding device as well as the technique
relied upon with the device
Oppenheimer & Nelson Ann All 2006;96:19-23.
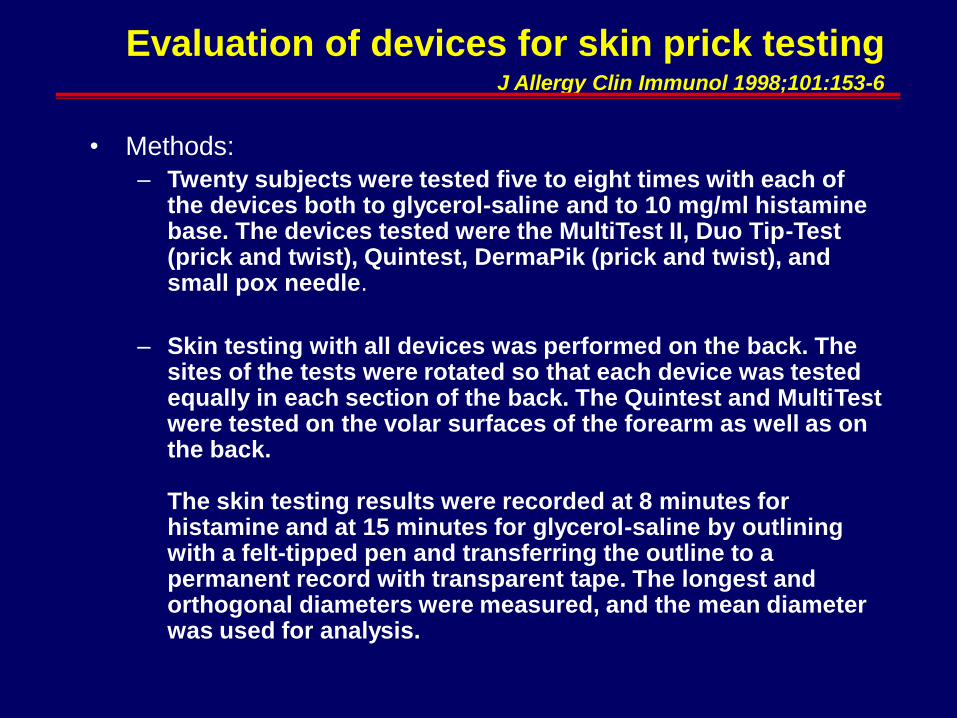
Evaluation of devices for skin prick testingJ Allergy Clin Immunol 1998;101:153-6
• Methods:
– Twenty subjects were tested five to eight times with each of the devices both to glycerol-saline and to 10 mg/ml histamine base. The devices tested were the MultiTest II, Duo Tip-Test (prick and twist), Quintest, DermaPik (prick and twist), and small pox needle.
– Skin testing with all devices was performed on the back. The sites of the tests were rotated so that each device was tested equally in each section of the back. The Quintest and MultiTest were tested on the volar surfaces of the forearm as well as on the back.
The skin testing results were recorded at 8 minutes for histamine and at 15 minutes for glycerol-saline by outlining with a felt-tipped pen and transferring the outline to a permanent record with transparent tape. The longest and orthogonal diameters were measured, and the mean diameter was used for analysis.


Size of wheals that are larger than 99 percent of the wheals with saline
using the same device by the same operator.
Devices for which a 3 mm wheal would be
significant
Devices for which a > 3 mm wheal should be
used as significant
Device .99 Quantile of
Reactions at
the negative
control sites
Device .99 Quantile of
reactions at
the negative
control sites
Quintest (HS) puncture 0 mm DermaPIK (Greer)
Prick
3.25 mm
Smallpox needle (HS) prick 0 mm DuoTip (Lincoln) twist 3.5 mm
DuoTip (Lincoln) prick 1.5 mm Bifurcated needle (ALO) prick 4.0 mm
Lancet (HS) puncture 2.0 mm MultiTest (Lincoln)
Puncture
4.0 mm
Lancet (ALK)
Puncture
3.0 mm Bifurcate needle(ALO) puncture 4.5 mm
DermaPIK (Greer) twist 5.0 mm
JACI 1993;92:750-6.
JACI 1998;101:153-6.

Inter-individual variation in SPT
Test result Nurse 1 Nurse 2 Nurse 3 Nurse 4
Negative control 0.1 mm 0.4 mm 0.2 mm 0.2 mm
Histamine 11.7 mm 9.7 mm 12.9 mm 14.5 mm
Grass 2.1 mm 2.5 mm 4.7 mm 5.2 mm
Mugwort 7.7 mm 4.8 mm 7.4 mm 9.1 mm
Dog 1.5 mm 1.1 mm 3.0 mm 2.5 mm
House dust mite 1.7 mm 2.2 mm 1.6 mm 2.8 mm
Vohlonen I et al. Allergy 1989; 44: 525-531
PP results from hypodermic needle express in geometric mean

Should We Perform Proficiency
Testing?
• Like all other laboratory tests, it is imperative that quality assurance standards be met to insure that accurate testing technique is being performed*.
• To confirm such standards, it is recommended that all technicians performing skin testing undergo evaluation of their technique.
• Such proficiency testing measures should be repeated every 12 months with written results chronicled.
*Turkeltaub Imm + All Clin NA 2001;21:324

Proficiency Testing:
• National Committee for Clinical Laboratory Standards recommend quality control procedures for daily performance of testing with minimal performance targets for IgE antibody assays. – Inter-assay coefficient of variation in IgE antibody
assays should not exceed 15%.
– Labs are also encouraged to participate in a program of inter-laboratory proficiency testing. • These are provided by both manufacturers of reagent test
systems as well as the College of American Pathologists.
Yunginger JACI 2000;105:1077-84

InVitro Proficiency In the Real World
• Even with such calibration and increased
automation, invitro assays still have flaws.
– examined 6 large commercial labs by testing
blinded samples of the same sera
• both diluted and non-diluted samples
– Only 2 of the labs demonstrated precision and
accuracy
Williams JACI 2000;105:1221-30

Suggested Proficiency Testing:
• Using desired skin test device, perform skin testing with positive and negative controls in an alternate pattern on a subjects back (H 1-10, and S 1-10)
• Record histamine results at 8 minutes by outlining wheals with a felt tip pen and transferring results with transparent tape to a blank sheet of paper
• Record saline results at 15 minutes by outlining wheal and flares with a felt tip pen and transferring results with transparent tape to a blank sheet of paper
• Calculate the mean diameter X=(D+d)/2; D=largest dia and d=perpendicular dia at midpoint of D
Oppenheimer & Nelson Ann All 2006;96:19-23

H1
S1
H2
S2
H3
S3
H4
S4
H5
S5
H6
S6
H7
S7
H8
S8
H9
S9
H10
S10
H=Histamine
S=Saline

Suggested Proficiency Testing:
• Histamine– Calculate the mean and standard deviations of each
mean wheal dia
– Determine coefficient of variation = std dev/mean
– Quality standard should be less than 30%
• Saline– All negative controls should be <3mm wheals and
<10mm flares
Protocol of CAMP Study

Suggested Proficiency Testing:
• It should be noted that this level of C.V. should be
considered conservative, as the European guidelines
suggest the C.V.% should not exceed 20% (ideally
10%).
Allergy 1989;144:S.1-57.

Recording Skin Test Response
• A record of skin testing should indicate a minimum amount of information that will allow another physician to interpret the results, avoiding the need to repeat skin testing.
• This should include: – the concentration of extract employed -consider including
manufacturer
– method of testing - ID or PST including device
– location of where testing was performed
– size of the positive and negative control reactions - preferably actual measurement, but if a score is used include the grading system.

www.AAAAI.ORG
Suggested Skin Test Documentation

Skin tests – Easy to interpret?

Semi-quantitative Reporting of Skin Test Results:
Criteria to Read Prick/Puncture Skin Tests
Negative 0 No reaction or no different from control
One plus + Erythema < a nickel in diameter
Two plus ++ Erythema > a nickel in diameter
Three plus +++ Wheal with surrounding erythema
Four plus ++++ Wheal with pseudopods and surrounding
erythema.
Criteria to Read Intracutaneous tests when control ≥ 2 mm
Negative 0 No different from control
One plus + Wheal 11/2 to 2 times control or definite
erythema > a nickel in size
Two plus ++ Wheal 2-3 times control
Three plus +++ Wheal > 3 times control
Four plus ++++ Wheal with pseudopods
Criteria to Read Intracutaneous tests when
control < 2 mm
Negative 0 No difference from control
One plus + 3-4 mm wheal with erythema or erythema > a
nickel in size.
Two plus ++ 4-8 mm wheal without pseudopods
Three plus +++ > 8 mm wheal without pseudopods
Four plus ++++ Wheal with pseudopods and erythema
A Manual of Clinical Allergy 1967

Recording Skin Test Response
• Results of both percutaneous and intracutaneous skin tests are often reported in only semi-quantitative terms. Results may be recorded only as positive or negative, or in terms of 0 to 4+ without any indication of what size reactions these numbers represent.
• At the very least, a record of skin testing should indicate a minimum of information that will allow another physician to interpret the results and alleviate the need to repeat skin testing (if an arbitrary grading system is employed, the range of reaction for each grade should be clearly indicated on the form).
Diagnostic Testing Practice Parameters 2008

Recording Skin Test Response
• Although area of the wheal and erythema is the most accurate, measurements of the product of the orthogonal diameters, the sum of the orthogonal diameters and even the longest diameter correlate very well with area, with r values greater than 0.9.
• A superior method of expressing results is to measure the reaction and enter the measurement on the form. This need not be excessively time consuming.
Ownby DR. JACI 1982;69:536 –538.

Efficacy of different skin prick testing methods in
the diagnosis of allergy to dog.
• The reliability of different means of expressing
the results of prick skin testing was compared
in patients sensitive to dogs. A determination
of sensitivity to dog was made in 202 children
based on a composite score from history,
RAST, and bronchial or conjunctival allergen
challenges
Vanto T Ann Allergy 1982;49:340-4.

Efficacy of different skin prick testing methods
in the diagnosis of allergy to dog.
Criteria
Sensitivity Specificity Overall
efficacy
≥ 3 mm wheal
diameter
0.98 0.82 0.89
≥ 5 mm wheal
diameter
0.66 0.98 0.84
3+ histamine
reference
0.92 0.93 0.93
Vanto T Ann Allergy 1982;49:340-4.

The reproducibiltiy of the allergy skin test scoring and
interpretation by board-certified/board eligible allergists
• Methods:– Series of pst were digitally photographed (22 tests with
controls) and a questionnaire regarding interpretation was sent to 70 allergists to asses (+,- or intermediate +/or whether a ID test was desired)
• Results:– 33 interpretable responses
– 24 relied on a grading scale (0-4+); 2 measured in mm, 7 provided only interpretation with no grading
– When graded std 0.26-1.35. Greatest agreement with median/mode score 4+ with least in test items with median/mode score 1-2+
– Range of requested ID test was 0-11
McCann Ann All Asthma Immun 2002;89:368-71

A1
A2
A3
A4
A5
A6
A7
A8
A9
B1
B2
B3
B4
B5
B6
B7
C1
C2
C3
C4
C5
C6
0
18
2
27
6
1
27
33
30
28
10
1
33
19
33
9
33
12
33
1
10
26
22
4
21
1
6
21
2
0
0
1
7
23
0
3
0
9
0
5
0
19
4
2
2
2
1
1
9
2
0
0
0
1
7
3
0
3
0
7
0
7
0
4
7
1
9
8
9
4
11
8
4
0
1
1
9
6
0
7
0
7
0
9
0
9
11
4
Test # Positive Negative Indeterminate ID
The reproducibiltiy of the allergy skin test scoring and
interpretation by board-certified/board eligible allergists
Ann All Asthma Immun 2002;89:368-71

“The skin test has been the most important single influence in the
development of the subject of allergy… In the early years, attention
concentrated on the improvement of the testing technics and of the
materials employed for this purpose. This led to an overemphasis
on the importance of this diagnostic procedure, so that, for a long
time, progress in the field of allergy depended almost entirely upon
development of the skin test. The failure to obtain positive
cutaneous reactions in all forms of allergy was attributed to an
inadequacy of testing materials and technics, and it was generally
anticipated that the etiologic factors in all clinical forms of
hypersensitiveness would eventually be revealed by improvements
in testing methods. After more than a quarter of a century it has
become apparent that these earlier hopes and prognostications for
the future of skin testing were too optimistic…the fact that skin
testing has not turned out to be a simple and completely reliable
technics does not detract from the fact that when it is intelligently
and skillfully performed, it remains the most effective diagnostic
procedure in reaginic allergic disorders.”
Walzer M. 1947