The Accuracy of Diagnostic Colposcopy using IFCPC 2011 Terminology
20
The Accuracy of Diagnostic Colposcopy Using ISCCP 2011 Classification SUJOY DASGUPTA, Senior Resident, Department of Gynecological Oncology, Chittaranjan National Cancer Institute(CNCI), Kolkata
-
Upload
sujoy-dasgupta -
Category
Health & Medicine
-
view
633 -
download
1
Transcript of The Accuracy of Diagnostic Colposcopy using IFCPC 2011 Terminology

The Accuracy of Diagnostic Colposcopy
Using ISCCP 2011 Classification
SUJOY DASGUPTA, Senior Resident,
Department of Gynecological Oncology,Chittaranjan National Cancer Institute(CNCI), Kolkata
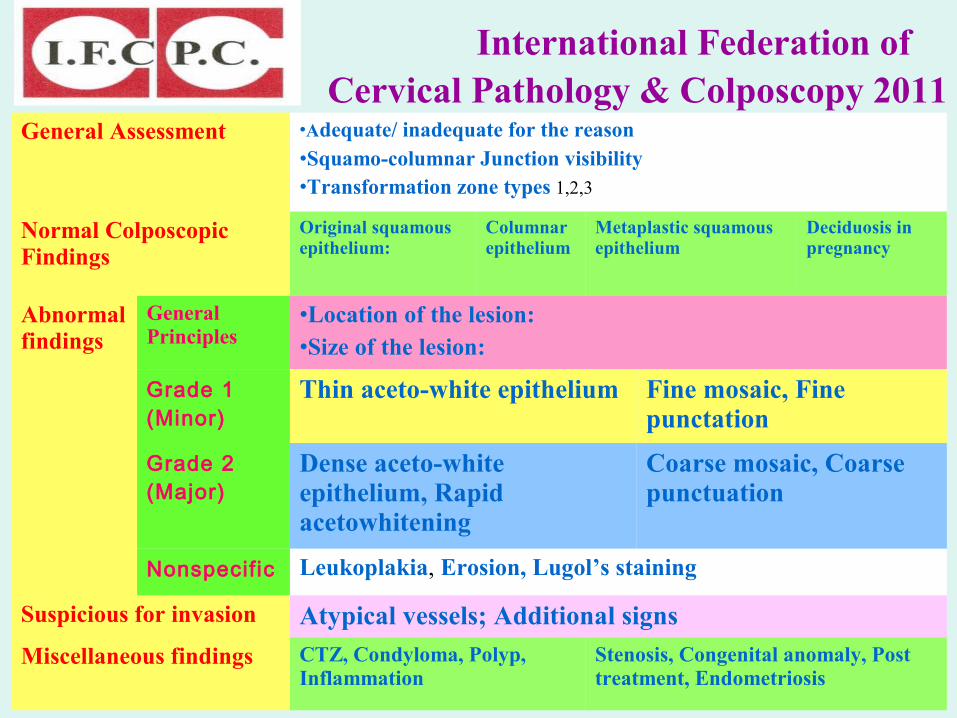
General Assessment •Adequate/ inadequate for the reason•Squamo-columnar Junction visibility•Transformation zone types 1,2,3
Normal Colposcopic Findings
Original squamous epithelium:
Columnar epithelium
Metaplastic squamous epithelium
Deciduosis in pregnancy
Abnormal findings
General Principles
•Location of the lesion:
•Size of the lesion:
Grade 1 (Minor)
Thin aceto-white epithelium Fine mosaic, Fine punctation
Grade 2 (Major)
Dense aceto-white epithelium, Rapid acetowhitening
Coarse mosaic, Coarse punctuation
Nonspecific Leukoplakia, Erosion, Lugol’s staining
Suspicious for invasion Atypical vessels; Additional signs
Miscellaneous findings CTZ, Condyloma, Polyp, Inflammation
Stenosis, Congenital anomaly, Post treatment, Endometriosis
International Federation of Cervical Pathology & Colposcopy 2011

To determine the ability of the colposcopists to correctly identify the various categories of cervical neoplasia using IFCPC, 2011 terminology
To determine the accurarcy of coposcopy in non-cytology based screening programme

STUDY DESIGN
Prospective Study
STUDY POPULATION
Subjects participating in a community-based cervical cancer screening demonstration project
Approved by CNCI Human Research Ethics Committee

Inclusion Criteria
• Non-pregnant women
• Age 30-60 years
• Intact uterus
• Without past history of cervical precancer/ cancer

STUDY METHODOLOGY
Written Informed Consent from all the participants
Examination by trained health workers
Cervical specimen collection for Hybrid Capture 2 (HC2)
(HPV DNA of 13 high-risk types)
VIA (Visual Inspection with Acetic Acid)
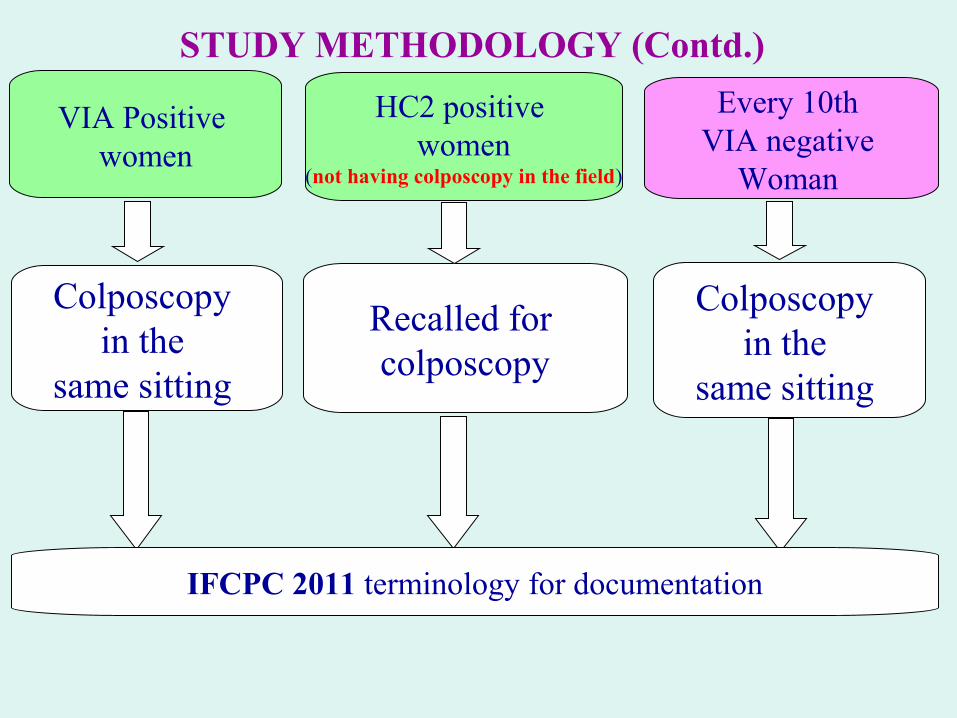
STUDY METHODOLOGY (Contd.)
VIA Positive women
Colposcopy in the
same sitting
Every 10th VIA negative
Woman
HC2 positive women
(not having colposcopy in the field)
Recalled for colposcopy
IFCPC 2011 terminology for documentation
Colposcopy in the
same sitting
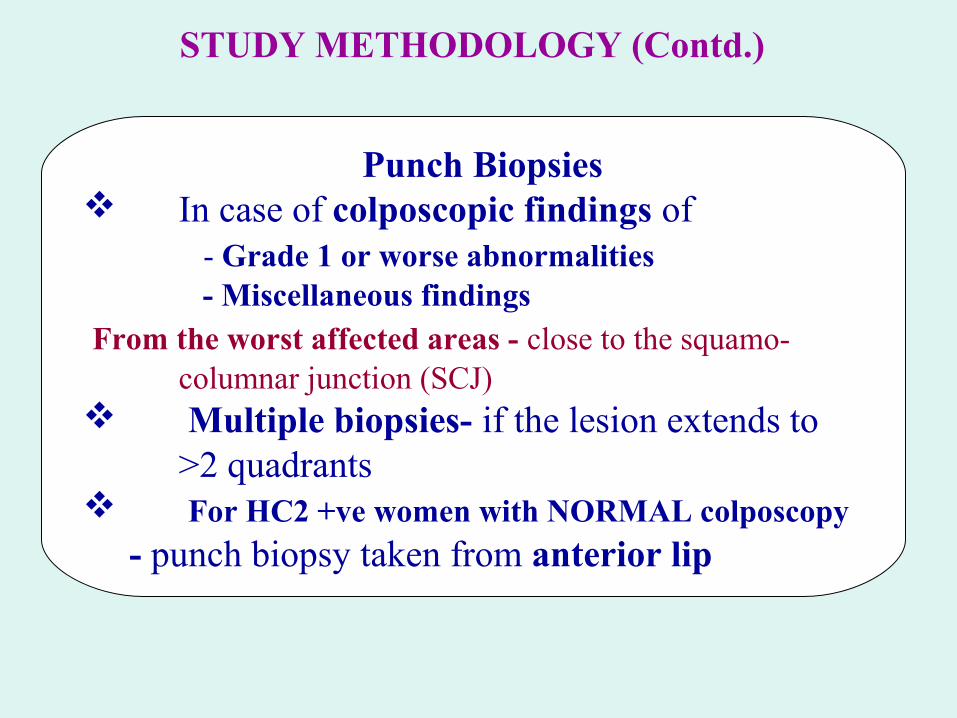
STUDY METHODOLOGY (Contd.)
Punch Biopsies In case of colposcopic findings of - Grade 1 or worse abnormalities - Miscellaneous findings From the worst affected areas - close to the squamo-
columnar junction (SCJ) Multiple biopsies- if the lesion extends to
>2 quadrants For HC2 +ve women with NORMAL colposcopy
- punch biopsy taken from anterior lip

STUDY METHODOLOGY (Contd.)
Colposcopic impressions were compared with the histological diagnosis as gold standard
Strength of agreement was measured using the weighted kappa statistics
Histology Colposcopy
Grade 1 Grade 2 Invasive
L-SIL Perfect agreement
H-SIL Perfect agreement
Invasive Perfect agreement

DEMOGRAPHIC VARIABLESof Screened Women
(n = 30773)
• Mean age (years) 38.7 + 8.1
• Mean age at marriage (years) 17.6 + 3.4
• Median number of pregnancies 3• Menopausal status Pre-menopausal 79.8% Post-menopausal 20.2%

SELECTION OF STUDY CASES
Total women screened 30773
Colposcopy done
Screen positive 3178
5556
Screen negative2378
Biopsy done2511
Inconclusive biopsy 45
Both colposcopy and satisfactory biopsy report
FINAL ANALYSIS
2466

AGREEMENT • Exact agreement between colposcopy and histology-
40.3% (993/2466)
* Weighted kappa <0.6 - poor agreement
>0.6 - good agreement
1.0 - excellent agreement
Weighted kappa* Impression
Overall (n= 2466) 0.17 Poor
VIA +ve (n = 1763) 0.12 Poor
HC2 +ve (n = 620) 0.35 'Fair'
Agreement in classifying cervical biopsy sample

AGRREEMENT (Contd.)
Colpo Diag
Histo Diagnosis
Normal Misc L-SIL H-SIL Inv Total
Normal175 (35.8%)
130 157 25 1 488
Misc 2225 (32.4%)
24 5 1 77
Grade 1 420 403688 (43.3%)
72 4 1587
Grade 2 35 41 10875 (28%)
8 267
Inv 2 3 5 730 (63.8%) 47
Total 654 602 982 184 44 2466
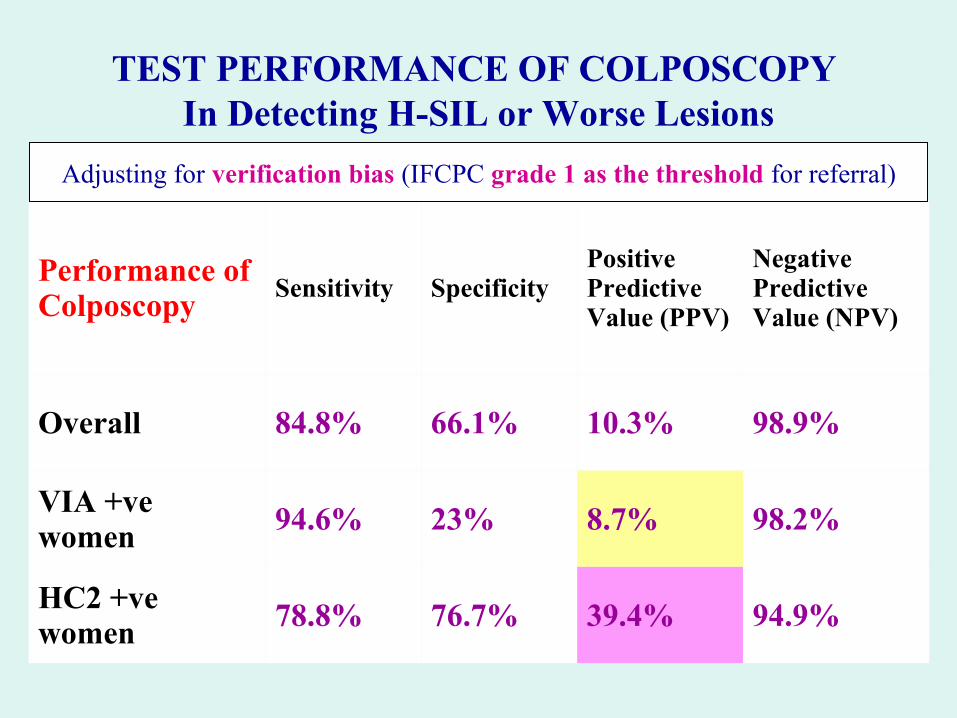
TEST PERFORMANCE OF COLPOSCOPY In Detecting H-SIL or Worse Lesions
Performance of Colposcopy
Sensitivity SpecificityPositive Predictive Value (PPV)
Negative Predictive Value (NPV)
Overall 84.8% 66.1% 10.3% 98.9%
VIA +ve women
94.6% 23% 8.7% 98.2%
HC2 +ve women 78.8% 76.7% 39.4% 94.9%
Adjusting for verification bias (IFCPC grade 1 as the threshold for referral)

DISCUSSION

Almost all the earlier studies - conducted in colposcopy clinics where women were referred for abnormal cytology (Pap smear)
Advantages of those studies-• Prior knowledge of cytological abnormalities can
influence colposcopic diagnosis
• Cytology is more specific than VIA and HC2, so less chance of False Positive Colposcopy & Histology

SALIENT FINDINGS
• Observed sensitivity to detect H-SIL+ is ≈90%, comparable to the that found in a meta-analysis of 8 longitudinal studies (60-97%)
• Colposcopy overestimates the severity of premalignant lesions, as seen in other studies
• Performs better in differentiating high grade from low grade lesions, rather than in differentiating low grade lesions from normal
• 25 HSIL cases did not have any colposcopic abnormality – suggesting ‘THIN CIN’

Accuracy of colposcopy is acceptable in non-cytology based screening using the IFCPC 2011 terminology

THANK YOU

ACKNOWLEDGEMENT
Dr Partha Basu
Dr Ranajit Mandal
Dr Pradip Das
Dr Dipanwita Banerjee
Dr Priyanka Singh
All the health workers of CPCI Project, CNCI