Susceptibility Testing Systems
21
Susceptibility Testing Systems CLSI versus EUCAST
Transcript of Susceptibility Testing Systems

Susceptibility Testing Systems
CLSI versus EUCAST
50008757
Highlight
50008757
Typewritten Text
50008757
Typewritten Text
John Turnidge 2014 ASA Meeting
50008757
Typewritten Text

The ISO Reference Standard

Desirable Features of a Susceptibility Testing System
• Methods – Reliability
• Reproducibility, intra- and inter-laboratory
• Accuracy
• Precision
• International reference standard – To which it has been calibrated
• High predictive value – patient outcome – Driven by breakpoint selection

Broth or Disc Method?
• Broth methods – Basis of semi-automated systems which are
calibrated to ISO standard
– More readily comparable to the reference method
– Can generate MIC values (if on scale) which can be directly plugged into PK-PD parameters
• Disk methods – Much more flexible
– Requires good correlation with MIC breakpoints.

So what choices are there?
System Calibrated to
ISO reference
Breakpoint Setting
CLSI: Clinical and Laboratory Standards
Institute [www.clsi.org] Yes
Micro + PK/PD + Clinical
Outcome
EUCAST: European Committee on AST
[www.eucast.org] Yes
Micro + PK/PD + Clinical
Outcome
BSAC: British Society for Antimicrobial
Chemotherapy [bsac.org.uk/susceptibility] No Micro + PK/PD
CDS: Calibrated Dichomotous System
[web.med.unsw.edu.au/cdstest/] No Wild-type cutoffs

So what choices are there?
System Calibrated to
ISO reference
Breakpoint Setting
CLSI: Clinical and Laboratory Standards
Institute [www.clsi.org] Yes
Micro + PK/PD + Clinical
Outcome
EUCAST: European Committee on AST
[www.eucast.org] Yes
Micro + PK/PD + Clinical
Outcome
BSAC: British Society for Antimicrobial
Chemotherapy [bsac.org.uk/susceptibility] No Micro + PK/PD
CDS: Calibrated Dichomotous System
[web.med.unsw.edu.au/cdstest/] No Wild-type cutoffs

Most media the same except… Species/Group EUCAST CLSI
Streptococcus spp. Mueller-Hinton F MH + 5% sheep (disk)
MH + 2.5-5% LH (BMD) = ISO
Haemophilus influenzae(+para) Mueller-Hinton F Haemophilus Test Medium
Listeria monocytogenes Mueller-Hinton F MH + 2.5-5% LH (BMD) = ISO
M. catarrhalis Mueller-Hinton F MHB and MHA
Pasteurella multocida (spp.) Mueller-Hinton F MH + 5% sheep (disk)
MH + 2.5-5% LH (BMD) = ISO
Campylobacter jejuni/coli Mueller-Hinton F MH + 5% sheep (disk)
MH + 2.5-5% LH (BMD) = ISO

Most media the same except… Species/Group EUCAST CLSI
Corynebacterium spp. Mueller-Hinton F MH + 2.5-5% LH (BMD) = ISO
N. gonorrhoeae (MIC method) GC Agar + suppl.
N. meningitidis (MIC method) MH + 5% sheep (disk)
MH + 2.5-5% LH (BMD) = ISO
Helicobacter pylori (MIC method) MH + 5% sheep aged (disk)
Anaerobes (MIC method) Brucella + haemin + Vit K
(agar dilution, add LHB for BMD)

Difference in tests available for…
Species EUCAST v5 CLSI M100-S25 CLSI M45-A2
Pseudomonas spp.
Other Non-Enterobacteriaceae
S. maltophilia only 1 agent
H. parainfluenzae ()
N. gonorrhoeae disk
N. meningitidis disk
Gram-positive anaerobes
Gram-negative anaerobes
C. difficile specific
M. catarrhalis
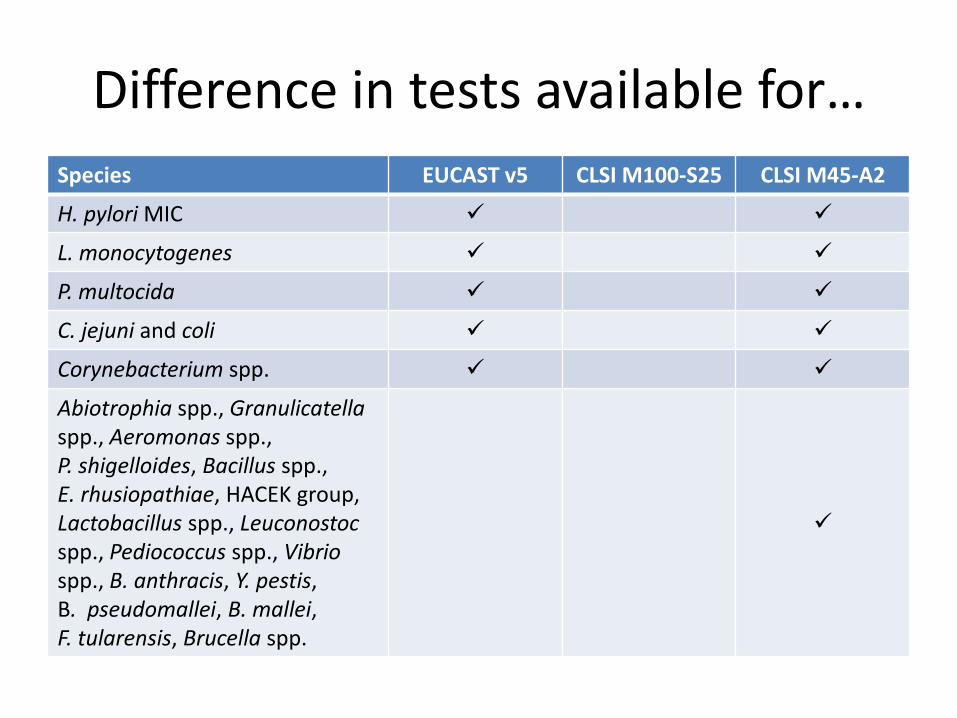
Difference in tests available for…
Species EUCAST v5 CLSI M100-S25 CLSI M45-A2
H. pylori MIC
L. monocytogenes
P. multocida
C. jejuni and coli
Corynebacterium spp.
Abiotrophia spp., Granulicatella spp., Aeromonas spp., P. shigelloides, Bacillus spp., E. rhusiopathiae, HACEK group, Lactobacillus spp., Leuconostoc spp., Pediococcus spp., Vibrio spp., B. anthracis, Y. pestis, B. pseudomallei, B. mallei, F. tularensis, Brucella spp.

Difference in tests available for…
Species EUCAST v5 CLSI M100-S25
Cefazolin No
Cefoperazone-sulbactam No No
Cephalexin ( CZL - UTI)
Fosfomycin IV No
Fusidic acid Maybe soon?
Teicoplanin
Telavancin January 2016
Tigecycline FDA only
Tetracyclines unrevised
Older (uncommon) cephalosporins ( unrevised)
Older (uncommon) fluoroquinolones ( unrevised)
Older (uncommon) aminoglycosides ( unrevised)

Difference in Use of “Intermediate”
• CLSI uses “I” liberally, EUCAST sparingly – Buffer zone to prevent “S” “R“ (main reason) – Implies “S” where drug is concentrated
• EUCAST applies when only dose escalation is possible and widely used
• Questions that have vexed many over the years include – Should it be reported as such? – What will the clinician do with it? – Are our tests reproducible enough to rarely require its
use?

Differences in Disk Strengths Agent Species CLSI EUCAST
Ampicillin Enterococcus spp. H. influenzae P. multocida
10µg 2µg
Amoxycillin-clavulanate
H. influenzae M. catarrhalis P. multocida
20-10µg 2-1µg
Piperacillin Enterobacteriaceae Pseudomonas spp.
100µg 30µg
Piperacillin-tazobactam
Enterobacteriaceae Pseudomonas spp.
100-10µg 30-6µg
Cefotaxime Enterobacteriaceae Viridans Streptococcus spp. H. influenzae
30µg 5µg
Ceftazidime Enterobacteriaceae Pseudomonas spp.
30µg 10µg

Differences in Disk Strengths Agent Species CLSI EUCAST
Ceftaroline Enterobacteriaceae S. aureus
30µg 5µg
Netilmicin Enterobacteriaceae Staphylococcus spp.
30µg 10µg
Benzylpenicillin Staphylococcus spp. β-haem & viridans Streptococcus spp.
10 units 1 unit
Linezolid Staphylococcus spp. Enterococcus spp. β-haem Streptococcus spp.
30µg 10µg
Nitrofurantoin Enterobacteriaceae Staphylococcus spp. Enterococcus spp.
300µg 100µg
Vancomycin Enterococcus spp. β-haem Streptococcus spp. S. pneumoniae
30µg 5µg
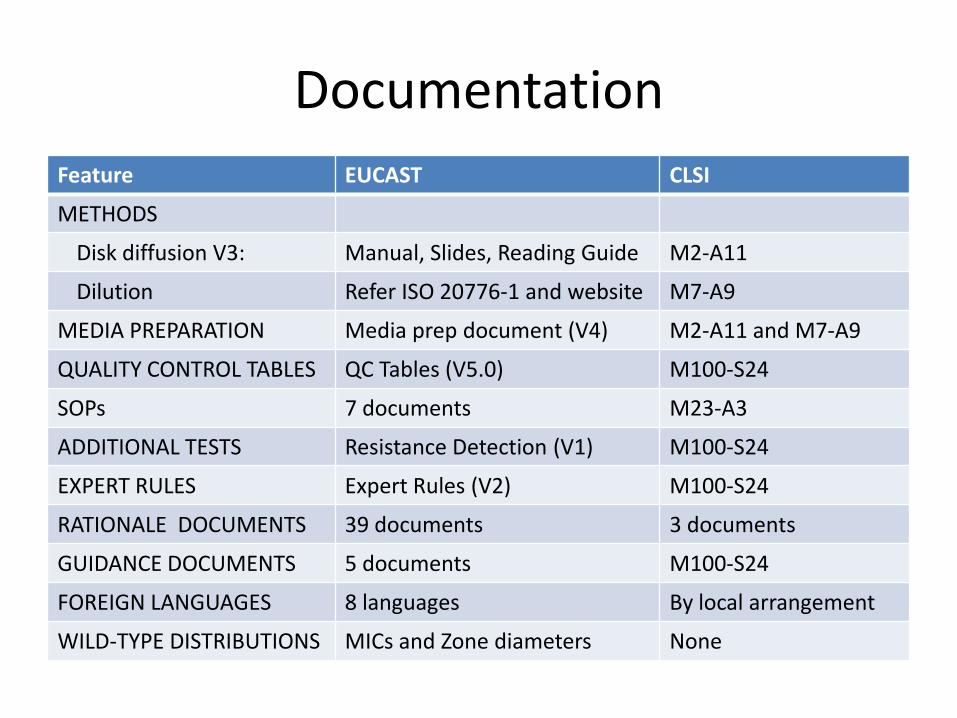
Documentation
Feature EUCAST CLSI
METHODS
Disk diffusion V3: Manual, Slides, Reading Guide M2-A11
Dilution Refer ISO 20776-1 and website M7-A9
MEDIA PREPARATION Media prep document (V4) M2-A11 and M7-A9
QUALITY CONTROL TABLES QC Tables (V5.0) M100-S24
SOPs 7 documents M23-A3
ADDITIONAL TESTS Resistance Detection (V1) M100-S24
EXPERT RULES Expert Rules (V2) M100-S24
RATIONALE DOCUMENTS 39 documents 3 documents
GUIDANCE DOCUMENTS 5 documents M100-S24
FOREIGN LANGUAGES 8 languages By local arrangement
WILD-TYPE DISTRIBUTIONS MICs and Zone diameters None
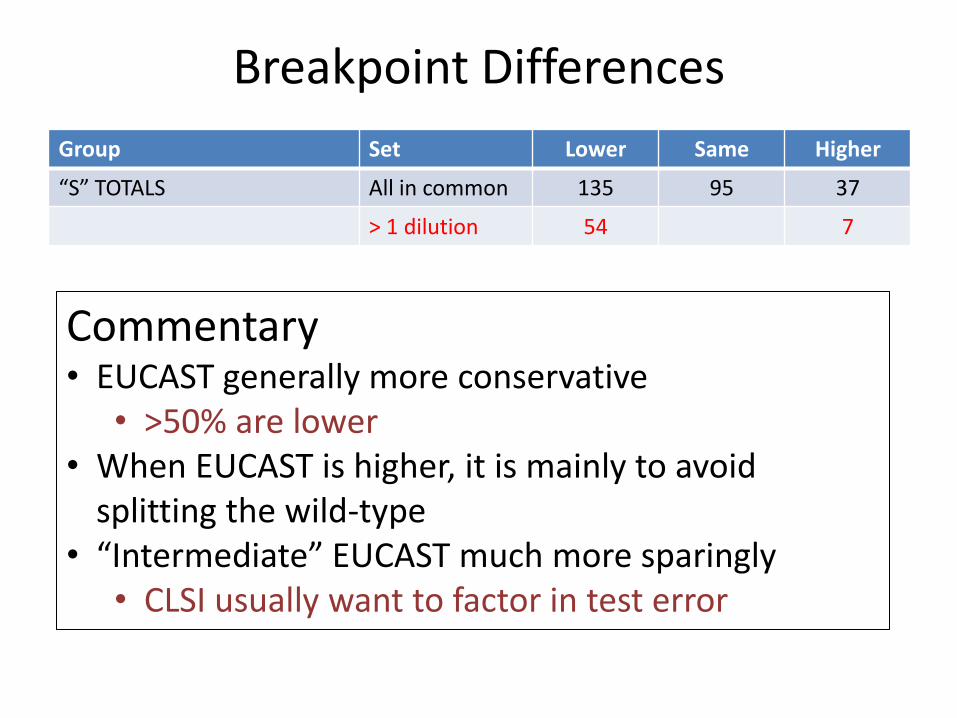
Breakpoint Differences
Group Set Lower Same Higher
“S” TOTALS All in common 135 95 37
> 1 dilution 54 7
Commentary • EUCAST generally more conservative
• >50% are lower • When EUCAST is higher, it is mainly to avoid
splitting the wild-type • “Intermediate” EUCAST much more sparingly
• CLSI usually want to factor in test error
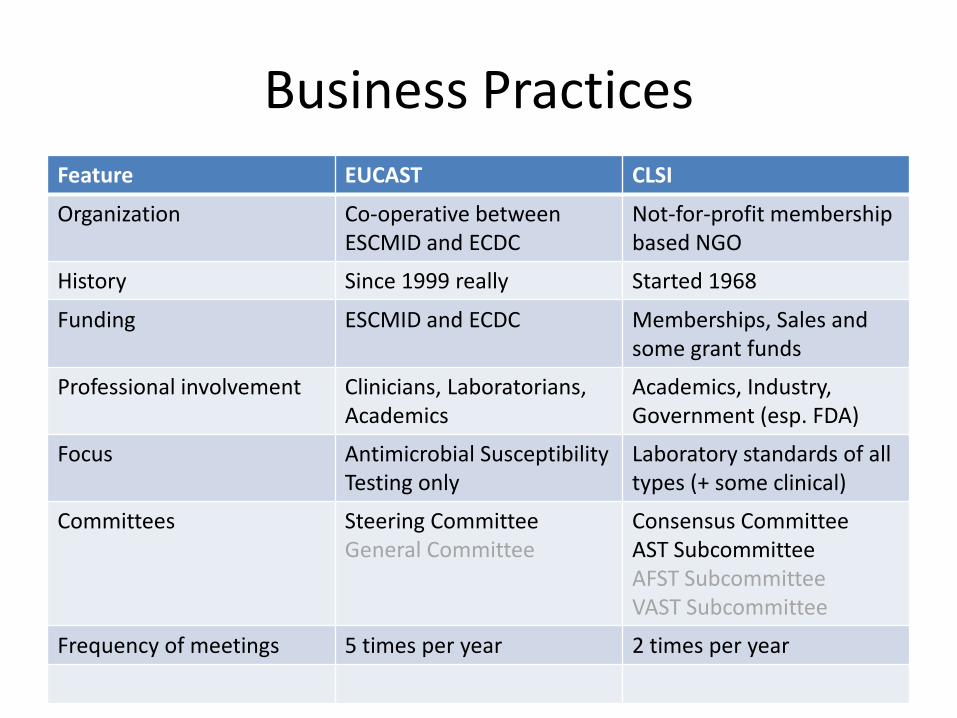
Business Practices
Feature EUCAST CLSI
Organization Co-operative between ESCMID and ECDC
Not-for-profit membership based NGO
History Since 1999 really Started 1968
Funding ESCMID and ECDC Memberships, Sales and some grant funds
Professional involvement Clinicians, Laboratorians, Academics
Academics, Industry, Government (esp. FDA)
Focus Antimicrobial Susceptibility Testing only
Laboratory standards of all types (+ some clinical)
Committees Steering Committee General Committee
Consensus Committee AST Subcommittee AFST Subcommittee VAST Subcommittee
Frequency of meetings 5 times per year 2 times per year
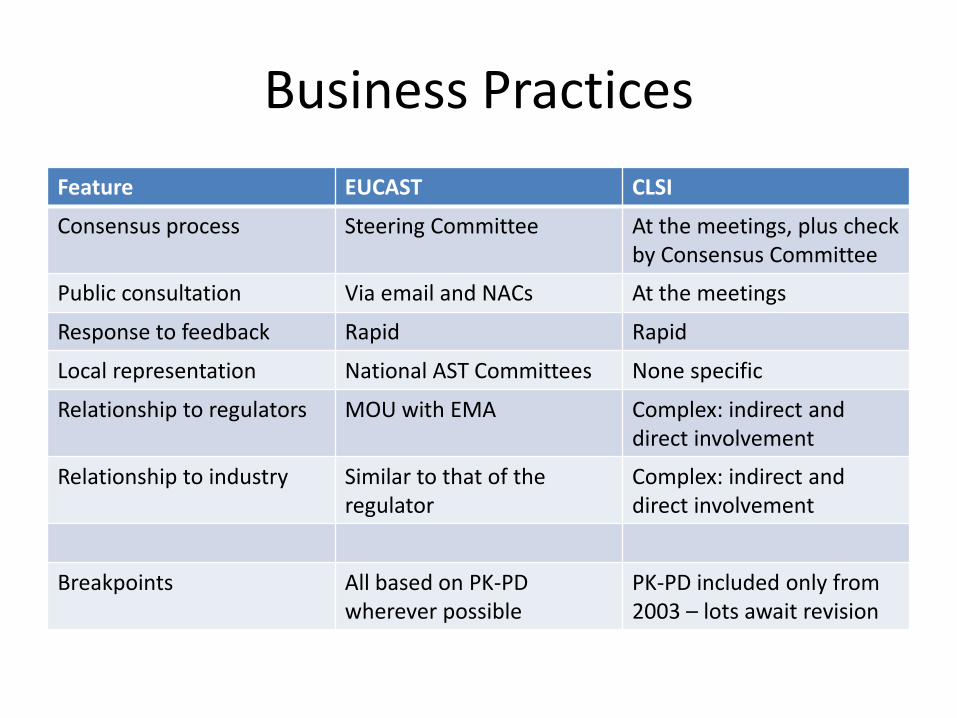
Business Practices
Feature EUCAST CLSI
Consensus process Steering Committee At the meetings, plus check by Consensus Committee
Public consultation Via email and NACs At the meetings
Response to feedback Rapid Rapid
Local representation National AST Committees None specific
Relationship to regulators MOU with EMA Complex: indirect and direct involvement
Relationship to industry Similar to that of the regulator
Complex: indirect and direct involvement
Breakpoints All based on PK-PD wherever possible
PK-PD included only from 2003 – lots await revision

The most notable difference
EUCAST CLSI
$=€=£=0 Minimum $170 USD
per year (For M100)