antitubercular drug susceptibility testing
77
Dr.M.Malathi Postgraduate Department of Microbiology Chengalpattu Medical College ANTITUBERCULAR DRUGS AND UG SUSCEPTIBILITY TESTI
-
Upload
drmalathi13 -
Category
Health & Medicine
-
view
82 -
download
0
Transcript of antitubercular drug susceptibility testing
Dr.M.MalathiPostgraduate
Department of MicrobiologyChengalpattu Medical College
ANTITUBERCULAR DRUGS AND
DRUG SUSCEPTIBILITY TESTING
INTRODUCTION
• Anti-tuberculosis drug resistance is a major public health problem that threatens progress made in TB care and control worldwide.
• Drug resistance arises due to improper use of antibiotics in chemotherapy of drug-susceptible TB patients.
• This improper use is a result of a number of actions including, administration of improper treatment regimens and failure to ensure that patients complete the whole course of treatment.
ANTI TUBERCULOUS DRUGS
Criteria
• Highly effective• Free from side efffects• Easy to administer• Reasonably cheap
Drugs Bactericidal and Bacteriostatic
Isoniazid
• Powerful bactericidal drug• Active against intracellular and extracellular bacilli• Action most marked on rapidly multiplying bacilli• Inhibits mycolic acid synthesis• Easily penetrate the cell membrane (BBB)• Oral, 4-5mg/kg 300mg maximum• INH should not be given in divided doses because
the peak level should be achieved in the blood to kill the bacilli.
• Adverse effects: gastritis, peripheral neuropathy, blood dyscrasias, hyperglycemia and liver damage.
• Addition of pyridoxine helps prevent the occurrence of peripheral neuropathy
Rifampicin • Bactericidal drug• Effective against intracellular and extracellular
bacilli• Permeates all the tissue membranes including BBB• Only bactericidal drug active against the persisters
or dormant bacilli• Inhibit transcription by binding with bacterial DNA
dependent RNA polymerase• Oral drug, 10 – 12mg/kg 450 – 600 mg• Food interferes with the absorption• Always given as combination therapy
• Adverse effects: hepatotoxicity, gastritis, influenza – like illness, purpura, thrombocytopenic and nephrotoxicity.
• Urine will turn red; can be used as a test of compliance
• PAS delays absorption of RMP; hence concurrent adminisitration should be avoided
Streptomycin
• Bactericidal drug• Acts entirely on rapid multiplying bacilli• No action on persisters• Binds to the 30S ribosomal subunit, which affects
polypeptide synthesis, thus inhibits translation.• Does not penetrate the biological membranes• Daily dose – 0.75 to 1 g single injection (i.m)• Side efffects: vestibular damage, nystagmus
Pyrazinamide
• Bactericidal drug• Active against the slow multiplying intracellular
bacilli• Oral drug • 30mg/kg in divided doses• Adverse effects: hepatotoxicity, hyperuricaemia• Pyrazinamide achieves high levels in CSF –
hence recommended in TB meningitis.
Ethambutol
• Bacteriostatic drug• Given in combination with other drugs• Oral drug• Inhibits the cell wall arabinan polymerization• Side effect: retrobulbar neuritis• Can be avoided at dose of 15mg/kg given in
divided doses
Thioacetazone
• Only companion drug to INH that is commonly used in India.
• 2mg/kg dose• Side effects : Gastrointesinal disturbances,
blurring of vision, hemolytic anaemia, urticaria
Fluoroquinolones
• Bactericidal antibiotics• Not FDA approved, but used as antitubercular
drug• Traps the gyrase and topoisomerase IV on
DNA as ternary complexes and blocks replication
• Moxifloxacin, gatifloxacin, levofloxacin, ofloxacin, ciprofloxacin
Macrolides
• Binds to the bacterial 50S ribosomal subunit and inhibits the RNA dependent protein synthesis
• Eg: clarithromycin
Ethionamide
• Synthetic compound related to INH• Inhibits the mycolic acid synthesis
Capreomycin
• Inhibits the protein synthesis through modification of ribosomal structures at the 16S rRNA
Bedaquiline
• First FDA approved TB drug in almost 40 years• Approved on 28th December 2012• Inhibits the proton pump of mycobacterial ATP
synthase• To treat pulmonary MDR TB• Trade name : sirturo
New TB drugs under trails
• Nitroimidazoles• PA – 824• OPC – 67683• TMC207• SQ109• Phenothiazines• Oxazolidinones• Linezolid• Benzothiazinones
When a patient is AFB- TB positive…
DOTS• DOTS remains at the heart of the Stop TB Strategy.
Five elements are:1. Political commitment with increased and sustained
financing2. Case detection through quality assured bacteriology3. Standardized treatment, with supervision and
patient support4. An effective drug supply and management system5. Monitoring and evaluation system and impact
measurement.
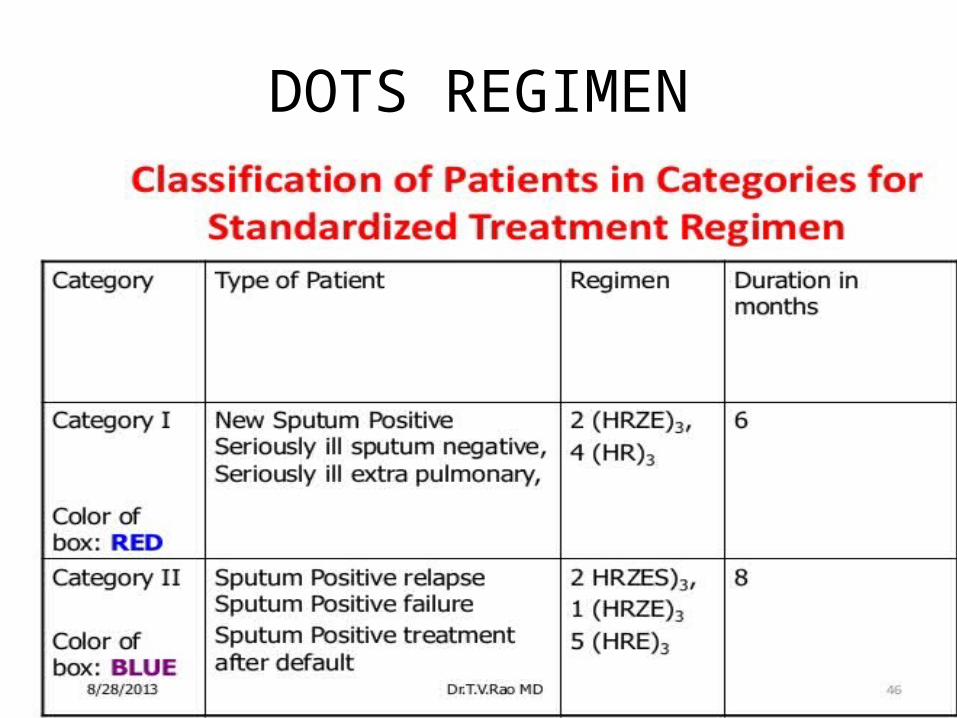
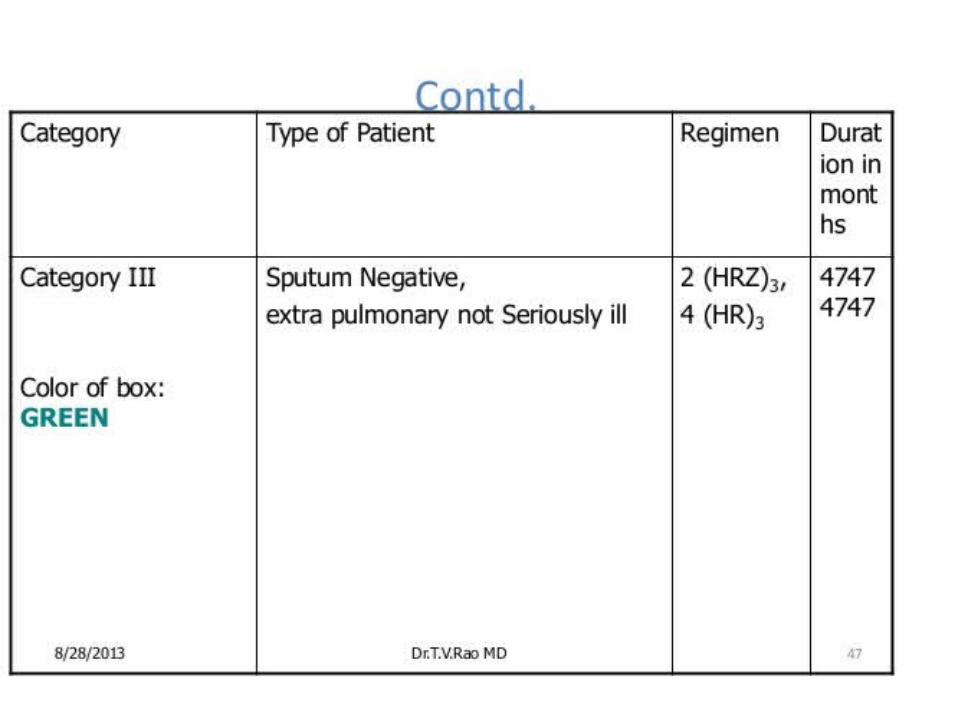
DOTS REGIMEN
Drug susceptibility testing
• Drug susceptibility testing is done to find out which drugs the tuberculous bacteria in a person are sensitive to and therefore , to rule out drug resistant TB.
• It is essential to perform testing, so that resistance can be discovered as soon as possible, in order that the patient can be provided with effective TB treatment.
Aim of susceptibility testing
• Provides data as to what drug should be used for treatment
• Screens for drug resistance• Measures the incidence and prevalence of
drug resistance within the community.
Susceptibility testing done:• Who fail to respond after 3 months of
treatment• Who do not convert to having negative smears
after 3 months of treatment• Whose smears demonstrate increasing
number of AFB after an initial decrease.• Patients on relapse• Undertaking drug resistance surveillance
studies in a region
• Routine susceptibility testing of primary TB isolates has not been generally suggested unless drug resistance in a particular community exceeds 5%.
• CDC USA Recommend that susceptibility tests should be done on all primary isolates
• Ideally, susceptibility testing should be done on all isolates.
• If Susceptibility testing not done store the culture for 6 months to 1 year
Types
• Phenotypic by observing the physical characteristics of the organisms
• Genotypic genetic characteristics of the organisms.
• Direct method :a set of drug containing and drug free media is
inoculated directly with concentrated specimen
• Indirect method:The pure culture inoculated in the drug and
drug free slopes of media
Direct methodAdvantages:• Rapid result• Can measure the sensitivity prior to cultivation
on laboratory mediaDisadvantages: uncertainty of the Mycobacterium sp.,Less control of the viable inoculum size
CONFIRMATORY – INDIRECT METHOD
Phenotypic Methods
Phenotypic methods
Absolute concentration method
Resistance ratio method
Proportion method
Absolute concentration method
• Uses a standardized inoculum grown on drug free media and media containing graded concentrations of the drug to be tested (MIC).
• Requires growth of the patient strain on drug free medium to demonstrate the viability, but does not compare the colony numbers on the drug free and drug containing media .
• This method is greatly affected by the viability of the organism.
• Hence inoculum must be carefully standardised.
Resistance ratio method
• Similar to absolute concentration method except that the patient strain is compared with the growth of a standard laboratory strain (H37Rv)
• Result MIC of the patient strain / MIC of the laboratory strain
• Greatly affected by the inoculum size as well as the viability of the strains.
Proportion method
• Enables a precise estimation of the proportion of mutants resistant to a given drug.
• Several 10 fold dilutions of inoculum are planted on to both control and test media.
• At least one dilution should yield isolated countable (50-100) colonies.
• Viable count can be calculated by counting the colonies and multiplying with the dilution of the inoculum used.
• The proportion of bacilli resistant to a given drug is then determined by expressing the resistant portion as a percentage of the total population used.
• Proportion method method of choice for estimating the drug resistance.
• Principle used in: BACTEC 460 MGIT 960 MB/BacT system ESP II System
Procedure for the proportion method of DST
BACTERIAL SUSPENSION:• With a loop, a sample of approximately 4 to 5
mg is taken from the primary culture and placed in a Mccartney bottle containing 1ml sterile distilled water and 6 glass beads of diameter 3mm.
• The bottle is vortexed for 20 to 30 seconds.• 4 to 5 ml of distilled water is added slowly
under continuous shaking.
• Allow the coarse particles to settle down.• Decant the mycobacteria carefully into
another clear, sterile McCartney bottle• The opacity is then adjusted by the addition of
DW to obtain a concentration of 1 mg/ml of tubercle bacilli by matching with McFarland Standard No.1
INOCULATION OF DST – Loop method
• Loop – nichrome wire (24SWG), internal diameter of 3mm, delivers 0.01ml
• The two bacterial dilutions required for the inoculation are 10-2 and 10-4 , prepared from the neat.
• Dilutions of 10-2 is produced by discharging two loopfuls of the bacterial suspension, standardized at 1ml/ml, into a Bijou bottle containing 2ml of DW.
• Mix the contents by shaking
• Similarly, dilutions of 10-4 is produced by discharging two loopfuls of the 10-2 dilution into a small tube containing 2ml of DW
• Mix the contents by shaking• Media used : egg based solid media – LJ medium• Two slopes of medium without drug and one
slope of medium with drug , each of the four drugs are inoculated with a loopful of each dilution
• The standard strain M.tuberculosis, H37Rv is tested with each new batch of medium.
• The recommended drug concentrations are 1. Isoniazid – 0.2mg/l2. Rifampicin – 40mg/l3. Ethambutol – 2mg/l4. Streptomycin – 4mg/l
Incubation and Reading
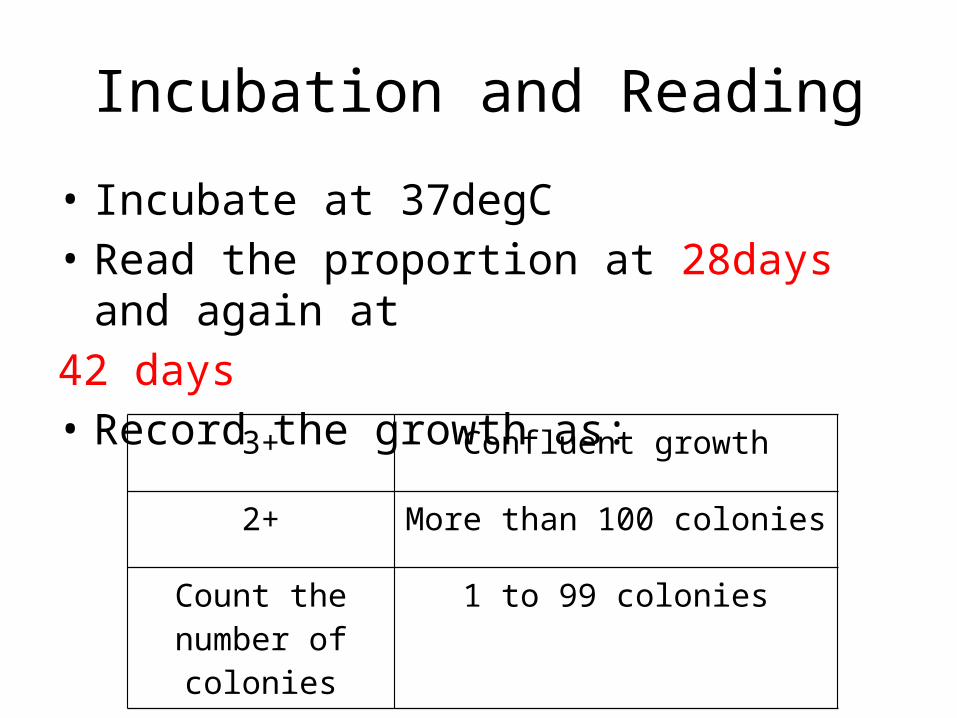
• Incubate at 37degC• Read the proportion at 28days and again at 42 days• Record the growth as:
3+ Confluent growth
2+ More than 100 colonies
Count the number of colonies
1 to 99 colonies
• The average number of colonies obtained for the drug containing slopes indicates the number of resistant bacilli contained in the inoculum
• Dividing the number of colonies in the drug containing slopes by that in drug free slopes gives the proportion of resistant bacilli existing in that strain
• On 28th day if it is resistant Declared as a resistant strain
• On 28th day if it is sensitive second reading is made on the 42nd day
• The final definitive report should be given for all the four drugs on 42nd day
Quality control
• Include a standard strain with every batch of medium as a check on drug concentration
• As an internal quality control, use a strain of M.tuberculosis with known resistance pattern to different drugs with every batch of tests as a check on procedures
• For State reference laboratories, the NRL should send strains of known susceptibility patterns
• The NRL should supply the drugs required for susceptibility tests to ensure proper standardisation
E - test
• Commercially available as AB BIODISK• Based on determination of drug susceptibility
using strips containing gradients of impregnated antibiotics
• High rate of false resistance
BACTEC 460 TB
• Detects the presence of mycobacteria based on their metabolism rather than visible growth
• The metabolism is interpreted as Growth index (GI) value
• Drug susceptibility tests can be performed for all the anti tuberculosis drugs when sufficient GI is observed
• In a study conducted at TRC, Chennai showed that the isolation of positive cultures and DST is obtained within 8 days by BACTEC
MGIT 960
• Automated system for growth detection and DST
• Rapid, accurate and cost effective method• Detection time – 8 to 15 days
Microwell alamar blue assay and micro plate tetrazolium reduction assay
• Colorimetric based on the oxidation reduction of the dye Alamar blue or MTT dimethylthiazol-2,5-dipheny tetrazolium bromide.
• Drug resistance is detected by the reduction of the dye from blue to pink due the oxidation-reduction metabolism of viable organisms.
Mycolic acid index susceptibility testing
• Modification of the original mycolic acid synthesis by HPLC where a coumarin compound is used as a fluorescent derivatizing agent of mycolic acid instead of p-bromophenacyl bromide.
• Drug sensitivity is assessed by measuring the total area under mycolic acid (TAMA) chromotographic peaks of a culture of M.tb.
Microscopic observation of broth cultures
• Microscopic observation of broth cultures with drugs
• Inexpensive• High sensitivity and specificity• Suited for endemic developing countries
Micro colony detection
• Observation of micro-colonies of M.tuberculosis with the help of a microscope, on a thin layer of 7H11 agar plate
• Less expensive• Alternative for conventional in resource poor
countries
Pha B assay
• New phenotypic culture drug susceptibility testing method
• Pha B – phage amplified biologically• Based on the ability of viable M.tuberculosis
to support the replication of an infecting mycobacteriphage;
• Non infecting exogenous phages are inactivated by chemical treatment
• In case of drug resistant M.tuberculosis, bacilli will remain viable and protect the mycobacteriophage.
• Any mycobacteriophage protected within viable bacilli replicate and ultimately lyse their host.
• For rapid detection, the released mycobacteriophages are mixed with rapidly growing M.smegmatis host in which they undergo rapid cycle of infection, replication and lysis
• Lysis is easily seen as clear areas or plaques in a lawn culture of M.smegmatis
• The number of plaques generated is directly proportional to the number of protected mycobacteriophages, which is dependent on the number of tubercle bacilli that remain viable after drug treatment (i.e., drug resistant)
Luciferase reporter phage assay
• Viable mycobacteria are infected with reporter phages expressing firefly luciferase gene.
• Easily detectable signals are seen a few minutes after the infection of M.tuberculosis with reporter phages.
• Light production requires metabolically active M.tuberculosis cells, in which reporter phages replicate and luciferase gene is expressed
• When drug susceptible M.tuberculosis strains are incubated with specific anti-tuberculosis drugs, they fail to produce light after infection with luciferase reporter phages.
• In contrast, drug resistant strains are unaffected by the drugs and produce light at levels equivalent to those documented for untreated controls after infection with reporter phages
Genotypic Methods
Genotypic methods
• Essentially required for the rapid identification of Multidrug resistant TB strains
• The drug resistance in TB bacilli is not plasmid mediated, instead it is by individual target genes.
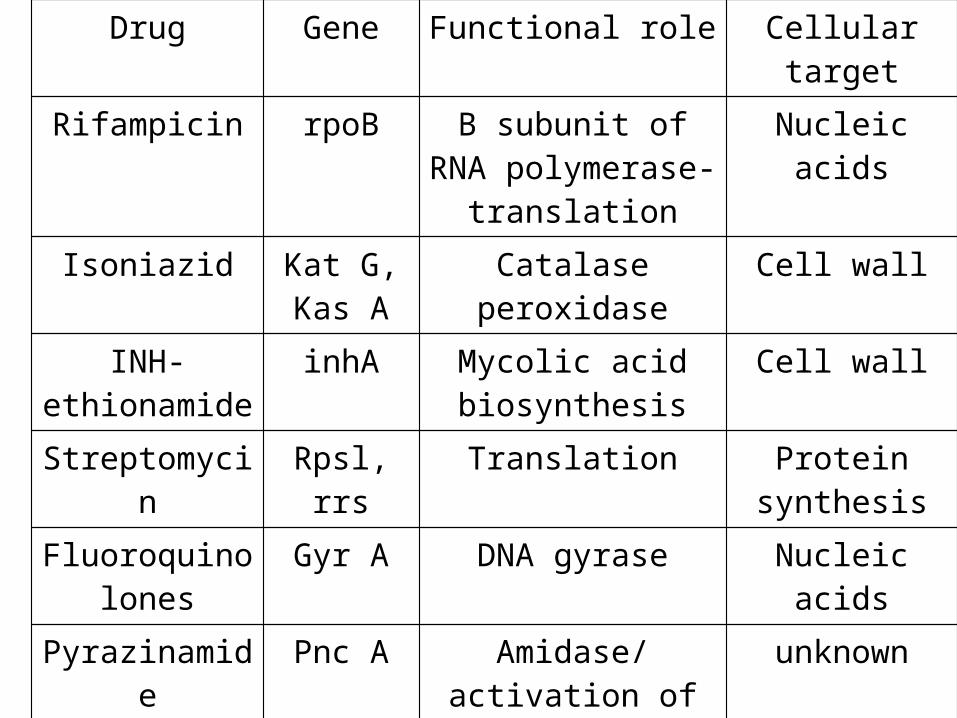
Drug Gene Functional role Cellular target
Rifampicin rpoB B subunit of RNA polymerase- translation
Nucleic acids
Isoniazid Kat G, Kas A
Catalase peroxidase Cell wall
INH- ethionamide
inhA Mycolic acid biosynthesis
Cell wall
Streptomycin Rpsl, rrs Translation Protein synthesis
Fluoroquinolones
Gyr A DNA gyrase Nucleic acids
Pyrazinamide Pnc A Amidase/activation of pro drug
unknown
Ethambutol embCAB Arabinosyl transferase-
polymerisation
Cell wall
Xpert MTB/Rif test• It is a cartridge based fully automated NAAT for TB
case detection and rifampicin resistance testing• Suitable for use in disease – endemic countries• Provides results from unprocessed sputum
samples in less than 2 hours, with minimal hand on technical time
• GeneXpert, was launched by Cepheid in 2004 • Integrated and automating the three processes
required for real time PCR based molecular testing (Sample preparation, Amplification, and detection)
Automated DNA sequencing
• DNA sequencing of PCR amplified products are most widely used
• Gold standard• DNA sequencing is used for characterizaion of
the mutation responsible for drug resistance• Mainly used for the drugs like Rifampicin,
Isoniazid, Streptomycin and Ciprofloxacin
PCR SSCP• Based on the property of single stranded DNA
to fold into a tertiary structure whose shape depends on its sequence
• Single strands of DNA differing by only one or few bases will fold into different conformations with different mobilities on a gel, producing what is called a single strand conformation polymorphism (SSCP)
• Can be done in combination with PCR• Done in large reference laboratories
PCR HDF• Performed by mixing amplified DNA from the
test organisms and susceptible control strains to obtain hybrid complementary DNA.
• If a resistant strain is present, the mutation will produce a heteroduplex which has different electrophoretic mobility compared with the homoduplex hybrid (no mutation)
• To detect all Rifampicin resistant strains having mutation in the rpo B gene.
• Cost effective, done only in reference laboratories
LiPA (Solid phase hybridization assay)
• Line probe assay is a commercial test for the rapid detection of M.tuberculosis complex and rifampicin resistance
• Based on the hybridisation of amplified DNA from the cultured strains or clinical samples to ten probes encompassing the core region of the rpo B gene of M.tuberculosis, which is immobilised on a nitrocellulose strip.
• Absence of hybridization of the amplified DNA to any of the sensitive sequence-specific probes indicates mutations that may encode resistance
• If hybridisation to the mutation specific probes occur – the mutation is present
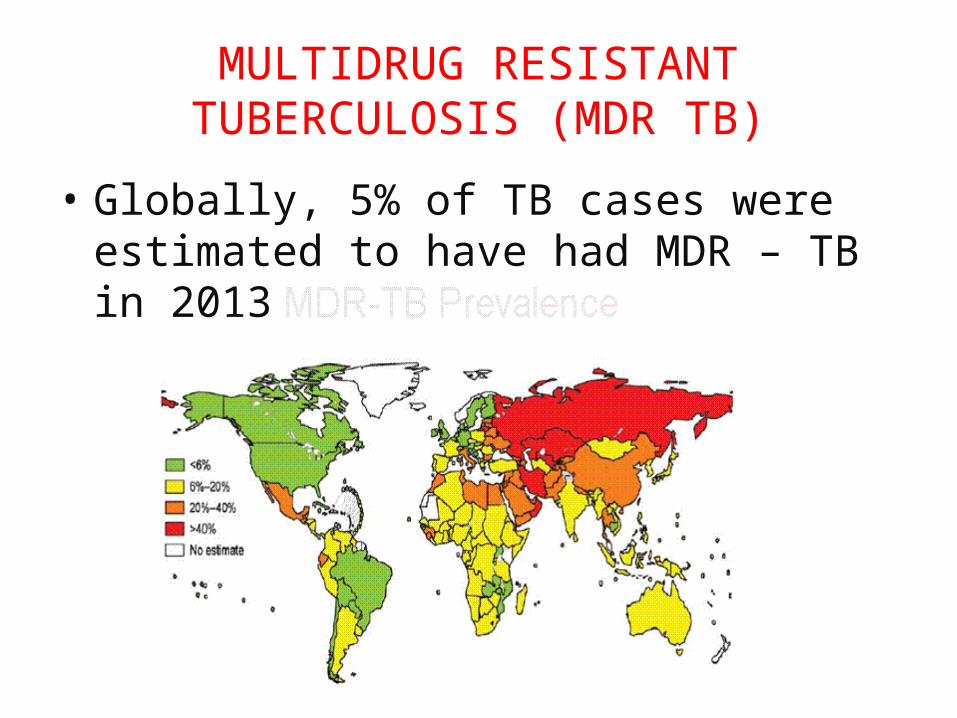
MULTIDRUG RESISTANT TUBERCULOSIS (MDR TB)
• Globally, 5% of TB cases were estimated to have had MDR – TB in 2013
MDR TB definition: • A form of TB caused by strain that is resistant
to isoniazid and rifampicin.
NEW DRUGS for MDR TB:• Bedaquiline• Delamanid
DOTS PLUS regimen
• Category IV regimen:• 6 drugs – kanamycin, ofloxacin, ethionamide,
pyrazinamide, ethambutol and cycloserine (For 6-9 months of the intensive phase)
• 4 drugs – ofloxacin, ethionamide, ethambutol and cycloserine ( 18months of continuation phase)
• PAS included in the regimen as a substitute drug if any bactericidal drug (K, Ofl, Z and Eto) or 2 bacteriostatic (E and Cs) drugs are not tolerated.
• All drug should be given in a single daily dosage under supervision except on sundays
• Sunday and daily evening dose are self administered
• The empty blister packs should be checked next morning by DOT provider
• Pyridoxine should be given to all the patients• The drug dosage is calculated according to the
weight of the patient
Extensively drug resistant TB
• XDR TB , involves resistant to the two most powerful anti TB drugs, Isoniazid and Rifampicin and also any one of the Fluoroquinolones (such as ofloxacin and moxifloxacin), and to at least one of three injectable second line drugs (amikacin, capreomycin or kanamycin).
• Coined in 2006 by CDC, USA based on the WHO guidelines for the management of drug resistant TB.
• WHO has recognized XDR- TB in 100 countries, till date including India.
• Prevalence of XDR TB??
• Confirmation of XDR TB:1. National Reference Laboratories (NRL) of
TRC/NIRT, chennai2. NTI Bangalore3. LRS institute, New Delhi
Treatment of XDR TB – category V
• Includes capreomycin, PAS, Moxifloxacin, linezolid, high dose INH, AMC, clofazimine
TDR – A fake report??
• In 2012, a letter to clinical infectious disease journal described 4 patients from Mumbai, India coined with TDR – Totally Drug Resistant tuberculosis
• A careful audit of these revealed that the term TDR TB has not yet been standardized and in any case testing for resistance beyond XDR TB is not reliable as there is no guidelines for all the drugs susceptiblity testing.
Conclusion
• Although many new techniques are available, for the diagnosis of TB, detection of AFB by direct microscopy is the only feasible method recommended by TB control programme of India.
• Wherever the facilities are available, in endemic countries, it is important to do culture and drug sensitivity by conventional or faster culture methods like BACTEC, MGIT.
References
• Revised National Tuberculosis Control Programme – DOTS guidelines
• RNTCP – technical manual• WHO – Global tuberculosis report 2014• Konemann textbook of diagnostic
microbiology • ICMR bulletin on new method of DST