Diagnosis of Hypokalemia Mahmoud Barazi, M.D. Nephrology Fellow TTUHSC.

Central Annals of Otolaryngology and Rhinology
Cite this article: Sabri A, Taher A, Homsi MT, Al Barazi R, Khalil M (2016) Submental Mass: An Unusual Presentation of Acute Myelogenous Leukemia. Ann Otolar-yngol Rhinol 3(3): 1093.
*Corresponding author
Randa Al Barazi, Division of Otolaryngology, Head and Neck Surgery, American University of Beirut Medical Center, P.O.Box:11-0236, Riad El-Solh 110 72020, Beirut, Lebanon, Tel: 961-1-350-000 ext: 5477; Fax: 961-1-370-
Submitted: 06 January 2016
Accepted: 10 February 2016
Published: 12 February 2016
ISSN: 2379-948X
Copyright© 2016 Al Barazi et al.
OPEN ACCESS
Keywords•Submental mass•Acute myelogenous leukemia•Granulocytic sarcoma
Case Report
Submental Mass: An Unusual Presentation of Acute Myelogenous LeukemiaAlain Sabri1, Ali Taher2, Marie-Therese Homsi3, Randa Al Barazi3* and Mazen Khalil4
1Otolaryngology Head and Neck Surgery, Cleveland Clinic Abu Dhabi, UAE2Department of Internal Medicine, Hematology- Oncology, American University of Beirut, Lebanon3Department of Otolaryngology Head and Neck Surgery, American University of Beirut, Lebanon4Department of Internal Medicine, Cardiology, St Rita’s Medical Center, Ohio
Abstract
Granulocytic Sarcoma is reported in the literature to occur either as an isolated finding or to be associated with Acute Myelogenous Leukemia (AML). We report a case of granulocytic sarcoma in the submental area occurring concomitantly with AML. It has been previously reported in the literature to occur in soft tissues of the head and neck; however, this is the first report of granulocytic sarcoma involving the submental area.
INTRODUCTIONGranulocytic sarcoma is an extramedullary tumor resulting
from abnormal proliferation of immature myeloid precursor cells. These extramedullary tumors can present as isolated finding preceding the leukemia, or present simultaneously with AML, and in other cases they can be a sign of blastic transformation of chronic myeloproliferative disease or of relapse [1]. Granulocytic sarcoma can develop in several tissues such as skin, CNS, lymphoid organs. Most commonly involved sites in head and neck include the orbit and the skull. This report describes a rare case of granulocytic sarcoma in the submental area presenting concomitantly with acute myelogenous leukemia.
CASE REPORTA 43 year old male patient previously healthy presented to
our medical center with the chief complaint of one week history of a midline anterior neck mass which appeared suddenly. The mass grew progressively in size from the time of onset until he presented to our medical center. The patient reported generalized weakness and 3 kg weight loss over the preceding 2 months. He also reported petechial like lesions over his shoulders under the straps of his backpack 2 days prior to presentation.
On presentation to our emergency unit, the patient was found to be pale in appearance; he was febrile 39.7 C. On exam, the mass was firm in consistency, non fluctuant, 7x7 cm in size, slightly tender to palpation with erythematous overlying skin change. Oral exam showed no oral mucosal changes, the floor of mouth was soft, no palpable cervical adenopathy. Mild trismus was present. CBC revealed a white blood cell count of 33800 with 78%
blasts and Auer rods. The patient underwent a contrast enhanced CT scan of the neck which revealed a midline mass surrounded by bilateral reactive cervical lymph nodes. The findings were consistent with cellulitis/inflammation. Panoramic x-ray of the mandible did not reveal any dental disease.
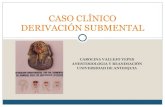
Intravenous antibiotics were started after blood cultures were taken to treat what seemed to be a cellulitis clinically. After starting the antibiotics, there was decrease in erythema, tenderness, and mass size, however a residual firm mass persisted. CT scan (Figure 1) was done revealing a 6x5 cm mass. Given the persistence of the mass, further investigations were done. FNA of the mass was performed and culture of the aspirate
Figure 1 A 6*5 cm mass in the submental area with abscess formation in the middle.

Central
Al Barazi et al. (2016)Email:
Ann Otolaryngol Rhinol 3(3): 1093 (2016) 2/3
was negative for microorganisms while the cytology revealed findings consistent with granulocytic sarcoma (Figure 2). This was followed by bone marrow aspirate and biopsy to rule out hematologic malignancy. Results revealed a hyper cellular bone marrow almost totally replaced with blasts and frequent Auer rods were seen. The results were consistent with AML-M2. Immunohistochemistry revealed blast cells positive for CD13, CD 33, CD 34, CD 117; HLA DR. Cytogenetics/karyotype testing was negative for t (8; 21), t (15; 17) translocations or any other chromosomal abnormalities. A leukemic infiltrate was in the differential diagnosis. The patient was started on idarubicin and cytarabine and the mass resolved completely.
DISCUSSIONGranulocytic granuloma is an extramedullary tumor of
myeloid cells. It is also kown as chloroma because of the greenish coloration of the tissues secondary to the high content of myeloperoxidase enzyme but 30% of the tumors might have whitish, grayish or brownish coloration [2]. This neoplastic disease is associated with acute myeloid leukemia, chronic myeloid leukemia, myeloproliferative disorders or myelodyspalstic syndrome therefore early and accurate diagnosis is very important. Granulocytic granuloma can occur concurrently with leukemia, or precede it and in some cases it is the first sign of relapse or indicative of transformation into the blastic phase [1]. In cases where GS occurs along with AML, the prognosis is usually poor [3,4]. The tumor, starting in the bone marrow would migrate to other areas via the haversian system canals to penetrate periosteum and form a soft-tissue mass [5,6].
The incidence of granulocytic sarcoma was reported to be 0.7 per million in children and 2 per million in adults [7]. Granulocytic sarcoma in adults occurs more commonly in the paraspinal areas while in children it is known to occur more in the orbital area [8]. Nearly half of the cases occur in the subcutaneous tissues or the orbit [6,9]. It was reported to occur in 2.9-9.1% of the cases of AML [10]. Granulocytic sarcoma might affect various areas of the body including bone, skin, CNS, liver, spleen and brain, other areas affected are soft tissues of the head and neck [9,11,12]. The orbit, skull and paranasal sinuses are the most commonly involved areas in head and neck. It was not previously reported to happen in the submental area although various reports of skin (chest wall, thigh muscles) and soft tissue involvement are present in the literature [2,13].
Granulocytic sarcoma is a rare disease and is often misdiagnosed; given its association with leukemia. Correct
diagnosis of this disease is very important in order not to delay adequate treatment especially that it can be misdiagnosed as malignant lymphoma mainly in patients who are not diagnosed with AML [14]. In addition, early diagnosis improves the prognosis.
The differential diagnosis includes small blue cell tumors, malignant lymphoma, blastic plasmacytoid dendritic cell neoplasm; solid tumors. There is a similarity radiographically and histologically between these malignancies which may delay correct diagnosis [15,16].
Clinical and Immunohistochemical findings are important for adequate evaluation of this disease. As per Bakst et al. tissue biopsy is preferable over fine needle aspiration in the diagnosis of myeloid sarcoma. Infiltration by myeloblasts is seen on H&E. Further tests include immunohistochemistry, flow cytometry, fluorescence in situ hybridization, and molecular analysis [17,18]. Hematoxilin and eosin, napthol ASD-chloracetate and stains for monoclonal antibodies (antimyeloperoxidase, CD43, CD 68, CD 20) are used for detection of GS [10,19,20]. After diagnosis of myeloid sarcoma, it is essential to check for bone marrow involvement and perform bone marrow biopsy and aspiration [17,18].
As for imaging, CT scan is the preferred imaging modality for assessing soft tissues. As for PET scan it is useful to assess involvement of other sites and for treatment planning [15].
Different treatment regimens of granulocytic sarcoma were reported in the literature including surgical excision, radiotherapy and chemotherapy [11]. There is no specific protocol in treatment of GS but several studies have showed better results with chemotherapy with longer periods of progression to acute leukemia and high remission [18,21]. Local approaches do not offer optimal treatment, radiation therapy or surgery without systemic treatment result in progression to AML and relapse [18]. Pancreatic granulocytic sarcoma in a patient with AML-M2 which was treated with chemotherapy and stem cell transplantation was reported; the patient remained in remission for 49 months following transplantation [3]. Dikbas et al reported a case of granulocytic sarcoma of the head and neck which antedated AML-M2 and which was treated with radiotherapy along with chemotherapy with complete remission after a first relapse. Another report described a woman with MDS and refractory anemia with a granulocytic sarcoma of the tongue which was treated with radiotherapy with complete response [3].
In our patient, granulocytic sarcoma manifested as a midline neck soft tissue mass that was erythematous, tender, progressively increasing in size. The patient had a temperature of 39.7 C and had a white blood cell count of 33000; it was suggestive of a Ludwig angina like infection in the submental area. The patient responded partially to the antibiotics treatment and the mass decreased in size and became softer. The white count normalized and the patient became afebrile. In view of the partial response to the antibiotics treatment, an FNA was done and it revealed leukemic infiltration of the soft tissue of the neck.
The patient was started on a chemotherapeutic regimen of cytarabine and idarubicin as an induction regimen to AML-M2. During the induction cycle, the mass was noticed to be decreasing in size; this was followed by complete resolution of the mass.
A BFigure 2 Section of the submental mass shows myeloblasts infiltrating the soft tissue.

Central
Al Barazi et al. (2016)Email:
Ann Otolaryngol Rhinol 3(3): 1093 (2016) 3/3
Sabri A, Taher A, Homsi MT, Al Barazi R, Khalil M (2016) Submental Mass: An Unusual Presentation of Acute Myelogenous Leukemia. Ann Otolaryngol Rhinol 3(3): 1093.
Cite this article
CONCLUSIONGranulocytic sarcoma in the submental area was not reported
previously in the literature although reports about soft tissue granulocytic sarcoma as well as head and neck granulocytic sarcomas have been reported. The patient responded very well to systemic chemotherapy which offers a good option for patients presenting with the granulocytic sarcoma concomitantly with leukemia.
REFERENCES1. Audouin J, Comperat E, Le Tourneau A, Camilleri-Broet S, Adida C,
Molina T, et al. Myeloid sarcoma: clinical and morphologic criteria useful for diagnosis. Int J Surg Pathol. 2003; 11: 271-282.
2. Ooi GC, Chim CS, Khong PL, Au WY, Lie AK, Tsang KW, et al. Radiologic manifestations of granulocytic sarcoma in adult leukemia. AJR Am J Roentgenol. 2001; 176: 1427-1431.
3. Breccia M, D’Andrea M, Mengarelli A, Morano SG, D’Elia GM, Alimena G. Granulocytic sarcoma of the pancreas successfully treated with intensive chemotherapy and stem cell transplantation. Eur J Haematol. 2003; 70: 190-192.
4. Dikbas O, Isik M, Purnak T, Karadag O, Uner A, Altundag K. Isolated granulocytic sarcoma of the head and neck preceding acute myeloid leukemia. Am J Hematol. 2004; 76: 95-96.
5. Novick SL, Nicol TL, Fishman EK. Granulocytic sarcoma (chloroma) of the sacrum: initial manifestation of leukemia. Skeletal Radiol. 1998; 27: 112-114.
6. Stein-Wexler R, Wootton-Gorges SL, West DC. Orbital granulocytic sarcoma: an unusual presentation of acute myelocytic leukemia. Pediatr Radiol 2003; 33: 136-139.
7. Lee JW, Kim YT, Min YH, Kim JW, Kim SH, Park KH, et al. Granulocytic sarcoma of the uterine cervix. Int J Gynecol Cancer. 2004; 14: 553-557.
8. Sugimoto Y, Nishii K, Sakakura M, Araki H, Usui E, Lorenzo VF, et al. Acute myeloid leukemia with t(8;21)(q22;q22) manifesting as granulocytic sarcomas in the rhinopharynx and external acoustic meatus at relapse after high-dose cytarabine: case report and review of the literature. Hematol J. 2004; 5(1):84-89.
9. Lee DA, Harris CP, Gresik VM, Rao P, Lau CC. Granulocytic sarcoma
presenting as pneumonia in a child with t(8;21) acute myelogenous leukemia: diagnosis by fluorescent in situ hybridization. J Pediatr Hematol Oncol 2004; 26: 431-434.
10. Roby BB, Drehner D, Sidman JD. Granulocytic sarcoma of pediatric head and neck: an institutional experience. Int J Pediatr Otorhinolaryngol. 2013; 77: 1364-1366.
11. Dutta Roy S, Stafford JS, Scally J, Selvachandran SN. Granulocytic sarcoma of the breast antedating acute myelogenous leukemia. Breast. 2004; 13: 242-246.
12. Best-Aguilera CR, Vazquez-Del Mercado M, Munoz-Valle JF, Herrera-Zarate L, Navarro-Hernandez RE, Martin-Marquez BT, et al. Massive myeloid sarcoma affecting the central nervous system, mediastinum, retroperitoneum, liver, and rectum associated with acute myeloblastic leukaemia: a case report. J Clin Pathol 2005; 58: 325-327.
13. Raja V, Bryant B, Bessman DJ, Alperin JB. Soft tissue sarcomas. Case 1. Granulocytic sarcoma: presentation with nodal and skin involvement. J Clin Oncol. 2004; 22: 2026-2027.
14. Lee YH, Lee NJ, Choi EJ, Kim JH. Granulocytic sarcoma (chloroma) presenting as a lateral neck mass: initial manifestation of leukemia: a case report. Eur Arch Otorhinolaryngol. 2006; 263: 16-18.
15. Vishnu P, Chuda RR, Hwang DG, Aboulafia DM. Isolated granulocytic sarcoma of the nasopharynx: a case report and review of the literature. Int Med Case Rep J. 2014; 7: 1-6.
16. Zhou J, Bell D, Medeiros LJ. Myeloid sarcoma of the head and neck region. Arch Pathol Lab Med. 2013; 137: 1560-1568.
17. Bakst RL, Tallman MS, Douer D, Yahalom J. How I treat extramedullary acute myeloid leukemia. Blood. 2011; 118: 3785-3793.
18. Yilmaz AF, Saydam G, Sahin F, Baran Y. Granulocytic sarcoma: a systematic review. Am J Blood Res. 2013; 3: 265-270.
19. Nayak DR, Balakrishnan R, Raj G, Pillai S, Rao L, Manohar C. Granulocytic sarcoma of the head and neck: a case report. Am J Otolaryngol. 2001; 22: 80-83.
20. Kieliszak CR, Cosenza MJ. Granulocytic Sarcoma of the Frontal Sinuses. Otolaryngol Head Neck Surg. 2015; 153: 691-692.
21. Paydas S, Zorludemir S, Ergin M. Granulocytic sarcoma: 32 cases and review of the literature. Leuk Lymphoma. 2006; 47: 2527-2541.