Studying Psychotherapy III (Chapter 10) PSYC 4500: Introduction to Clinical Psychology Brett Deacon,...
36
Studying Psychotherapy III (Chapter 10) PSYC 4500: Introduction to Clinical Psychology Brett Deacon, Ph.D. October 29, 2013
-
Upload
julian-freeman -
Category
Documents
-
view
215 -
download
0
Transcript of Studying Psychotherapy III (Chapter 10) PSYC 4500: Introduction to Clinical Psychology Brett Deacon,...

Studying Psychotherapy III
(Chapter 10)
PSYC 4500: Introduction to Clinical Psychology
Brett Deacon, Ph.D.
October 29, 2013

Announcements
• Response paper due today
• Next response paper due Tuesday, 11/5 (NOT this Thursday, 10/31)

Questions for Deacon (2013) article; Response paper due next Tuesday 11/5
• Describe what you believe to be the three most
significant effects (good or bad) of clinical
psychology’s adoption of the biomedical model
of psychotherapy research.

What We’ve Discussed
• Science-practice gap = split between romantics and empiricists
• Romantics endorse clinical intuition, empiricists endorse science as ways of knowing
• According to Lilienfeld, why is science a valuable way of knowing?
• What is the proper role of romanticism and empiricism in science?

Questions for Lilienfeld et al. (2013) article; Response paper due this Thursday 10/24
• Questions
• List and describe what you believe to be the three most important sources of practitioner resistance toward science-based practice in psychology.

Important Points
• Misconceptions about science-based therapies
• Confirmation bias
• Naïve realism
• Scientific thinking is unnatural
• Scientists should be humble
• Scientific training – thinking like a scientist vs. learning scientific technologies

Causes of Spurious Therapy Effectiveness
• Naïve realism – “my therapy works because my clients improve”

Prof. Dr. Hans-Jürgen MöllerChairmanDepartment of Psychiatry University of MunichGermany
Antidepressants have clinically relevant efficacy
Disclosure
• Member of the speaker bureau: AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Eisai, GlaxoSmithKline, Janssen Cilag, Lundbeck, Organon, Pfizer, Sanofi Aventis, Sepracor
• Serves as a consultant or on the advisory board: AstraZeneca, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen Cilag, Lundbeck, Organon, Pfizer, Sepracor, Servier, Wyeth
• Has received grant/research support from: AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Eisai, GlaxoSmithKline, Janssen Cilag, Lundbeck, Merck, Novartis, Organon, Pfizer, Sanofi Aventis, Sepracor, Servier, Wyeth

Patients’ experience vs. metaanalytical evidence: my patients believe in the
efficacy of antidepressants
Doctors’ experience vs. metaanalytical evidence: my doctors believe in the
efficacy of antidepressants

Causes of Spurious Therapy Effectiveness
• Name reasons why a client might appear to improve during therapy – other than the direct effects of the therapy itself.

Causes of Spurious Therapy Effectiveness
• Placebo (expectancy) effects
• Spontaneous remission
• Regression to the mean
• Effort justification
• Multiple treatment interference
• Demand characteristics
• Maturation
• Retrospective rewriting of pretreatment functioning
• Absence of knowledge of the hypothetical counterfactual
Psychotherapy Research
• Why should you care about psychotherapy
research? Why is this topic important?

Lilienfeld Harmful Treatments (2007)
• Critical Incident Stress Debriefing http://www.youtube.com/watch?v=VF3eJ0CU9w8


Lilienfeld Harmful Treatments (2007)
• Lilienfeld on the Dodo Bird verdict: “When we examine therapies that all appear to be reasonably well accepted or that are based on plausible theoretical premises, the differences among therapies tends to be minimal. Although this conclusion is not itself trivial, it overlooks the crucial point that some widely administered therapies are neither widely accepted in the scientific community nor derived from especially plausible theoretical principles.”
Lilienfeld Harmful Treatments (2007)
• Example: Thought Field Therapy
• Used by 25% of Wyoming psychotherapists,
and 50% of those who advertise themselves to
clients as anxiety specialists

Lilienfeld Harmful Treatments (2007)
• Some treatments have an overall harmful
effect on clients
• Some treatments benefit some clients but
harm others
• Some effective treatments may harm clients if
not implemented properly

Reporting Full Range of Outcomes: My Own Anxiety Treatment Research
• Comparison of brief vs. intensive exposure
• Study hypotheses and design
• Ratings obtained between exposure trials of
anxiety, catastrophic cognitions, and self-
efficacy
• Outcome: Greater improvement during
exposure in the intensive vs. standard group

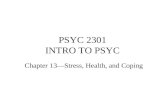
Brief vs. Intensive Exposure: Outcomes (Group Means)
1 2 3 4 5 6 7 80
5
10
15
20
25
30
35
40
45
50
Inten-sive Expo-sureBrief Ex-po-sureP
eak
Fea
r (0
-100
)
Exposure Trial

Reporting Full Range of Outcomes: My Own Anxiety Treatment Research
• In the brief exposure condition:
• Significant mean improvement from Trial 1 to
Trial 3 in anxiety, catastrophic cognitions, and
self-efficacy.
• However, 11 participants (36.7%) had worse
anxiety, catastrophic cognitions, and self-
efficacy from Trial 1 to Trial 3.

Popularity of PHTs?
• Why do many people believe in the value of
PHTs despite lack of evidence for their
effectiveness (or evidence that they cause
harm)?
• Examples: CISD and DARE

Empirically Supported Treatments (ESTs)
• Origins of the EST movement
• Health care coverage for psychotherapy
• Managed care pressures
• Increased competition from medications and pharmaceutical marketing
• Treatment guidelines for specific disorders in related professions
• Very well accepted in medicine, including psychiatry

Clinical Practice Guidelines in Psychiatry
• American Psychiatric Association has clinical
practice guidelines for (among others):
• Acute stress disorder and PTSD, bipolar
disorder, major depression, borderline
personality disorder, eating disorders,
OCD, panic disorder, schizophrenia,
substance use disorders, suicidal
behaviors http://www.psych.org/MainMenu/PsychiatricPractice/PracticeGuidelines_1.aspx

Clinical Practice Guidelines by NICE
• UK’s National Institute for Health and Clinical
Excellence has clinical practice guidelines for:
• Alcohol use disorders, antisocial
personality disorder, anxiety, ADHD,
autism, bipolar disorder, borderline PD,
adult depression, child depression, eating
disorders, enuresis, OCD, PTSD, social
phobia, schizophrenia, etc. http://guidance.nice.org.uk/Topic/MentalHealthBehavioural
Clinical Practice Guidelines in Psychology
• The American Psychological Association has
clinical practice guidelines for:
• Record keeping, child custody evaluations,
practice with older adults, multicultural
education and training, psychotherapy with
lesbian, gay, and bisexual clients, etc. http://www.apa.org/practice/guidelines/index.aspx
Empirically Supported Treatments (ESTs)
• APA Division 12 Task Force on Promotion and
Dissemination of Psychological Procedures
• Guidelines first published in 1995 task force
report
• Two types of “Empirically supported
treatments” (EST) (p. 315 in your text)
• “Well-established” and “probably efficacious”
Empirically Supported Treatments (ESTs)
• Reaction to the task force’s report• Empirically “supported, not “validated”• Guidelines use DSM-based medical model• EST list ignores relationship variables• Emphasizes differences between
treatments and ignores similarities (common factors)
• RCTs don’t generalize to real world• From scientists: EST criteria are too weak• Is psychotherapy an art or a science?

The American Psychological Association Task Force on Evidence-Based Practice in Psychology (2006)
• “Evidence-based practice in psychology (EBPP)
is the integration of the best available research
with clinical expertise in the context of patient
characteristics, culture, and preferences.”
• How commonly do mental health professionals
provide EBP?
• How do they integrate the components of EBP?

See EBP across Different Mental Health Professions Slides
State of the Field Today
• From Baker, McFall, & Shoham article (p. 61):• “(a) By clinicians’ own admission, much of what they do is little
informed by scientific evidence,• (b) many leading proponents of psychotherapy doubt whether much
of the extant scientific evidence is valid or relevant,• (c) although there are specific interventions that have relatively
strong research support, these are seldom used, and • (d) the factors that many practitioners point to as constituting the
core of their therapeutic armamentarium (i.e., nonspecific factors) are poorly understood, may not be teachable, and almost certainly do not require extensive science-based training or highly privileged status for their delivery.”
• “In summary, we are now in a situation in which many or most clinical psychologists appear strikingly unreceptive to science, incapable of taking advantage of scientific research (Tavris, 2003), and unprepared to adapt to the changing health care system.”

Questions for Baker et al. (2009) article
• 1. Beyond symptom reduction, what patient outcomes are particularly important to “decision makers” (e.g., insurance companies, government agencies) in evaluating a psychotherapy?
• 2. Describe two key factors in medicine’s development from an art to a science in the early 1900s.
• 3. What is your opinion of the new accreditation system proposed by the authors?

Baker et al. (2009) article
• Key metrics for evaluating a treatment
• Efficacy
• Effectiveness
• Dissemination potential
• Cost effectiveness
• Scientific plausibility
• How well do our best psychological treatments do on these metrics?

Baker et al. (2009) article
• What are some similarities between modern
clinical psychology and pre-scientific medicine?
• What key events contributed to medicine’s
transformation from an art to an applied science
in the early 1900s?
• What lessons can clinical psychologists take
from the history of medicine?

Baker et al. (2009) article
• The current APA accreditation system
• Broad, accommodating, problematic (?)
• Problems with the Psy.D for the field
• What is your opinion of the new accreditation
system proposed by the authors?
• Where do you see the field going from here?