![[1913] #2.12 Armour's Monthly Cook Book - October 1913](https://static.fdocuments.us/doc/165x107/577d2da61a28ab4e1eae0102/1913-212-armours-monthly-cook-book-october-1913.jpg)
Stroke 2006 Tsivgoulis 1913 6
5
Common Carotid Artery Intima-Media Thickness and the Risk of Stroke Recurrence Georgios Tsivgoulis, MD; Konstantinos Vemmos, MD; Christos Papamichael, MD; Konstantinos Spengos, MD; Efstathios Manios, MD; Kimon Stamatelopoulos, MD; Demetrios Vassilopoulos, MD, PhD; Nikolaos Zakopoulos, MD Background and Purpose—Increased common carotid artery intima-media thickness (CCA-IMT) has been associated with an increased risk of myocardial infarction and stroke. We investigated the relationship between CCA-IMT and recurrent stroke in a cohort of ischemic stroke patients. Methods—High-resolution B-mode ultrasonographic measurements of the CCA-IMT were performed in a consecutive series of 238 patients hospitalized in our institution with first-ever ischemic stroke. Stroke risk factors and secondary prevention therapies were documented. Patients were followed-up prospectively and the outcome event of interest was recurrent stroke. Results—During a mean follow-up period of 28.9 months (range: 6 to 60 months), 27 recurrent strokes were documented. Patients who experienced recurrent cerebrovascular events had significantly (P0.005) higher CCA-IMT values (1.01 mm, 95% CI:0.92 to 1.11 mm) than subjects who were free of stroke recurrence (0.88 mm, 95% CI:0.85 to 0.91 mm). After adjustment for baseline characteristics, risk factors and stroke subtypes and secondary prevention therapies increasing CCA-IMT was found to be an independent predictor of stroke recurrence. For each increment of 0.1 mm in CCA-IMT the probability of experiencing recurrent stroke increased by 18.0% (95% CI:2.0% to 36.0%, P0.027). Conclusions—Increased CCA-IMT values are associated with a higher risk of long-term stroke recurrence. (Stroke. 2006; 37:1913-1916.) Key Words: atherosclerosis carotid arteries recurrence stroke A growing body of evidence supports that the intima- media thickness of the common carotid artery (CCA- IMT) can be regarded as an early marker of atherosclerosis. 1 Furthermore, increased CCA-IMT has been associated with conventional cardiovascular risk factors, 2 the presence of other localizations of atherosclerosis 3 and an increased risk of myocardial infarction 4 and stroke. 5 However, there are limited data regarding the potential significance of CCA-IMT in predicting recurrent cerebrovas- cular events. Assuming that in addition to established risk factors, increased CCA-IMT may constitute an important risk marker for recurrent stroke, the present longitudinal study aimed to evaluate the relationship between CCA-IMT and stroke recurrence in a cohort of consecutive first-ever ische- mic stroke (IS) patients. Materials and Methods Study Population A series of 324 consecutive, first-ever acute stroke patients, admitted to the acute stroke unit and the general neurology ward of our institution between January 2000 and December 2003 were screened. All patients were included in “The Athens Stroke Registry,” a computerized prospective observational data bank, gathered in 2 university teaching hospitals. 6,7 According to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria, IS was classified based on etiopathogenetic mechanisms into the following groups: large artery atherosclerotic stroke (LAA), cardioembolic stroke (CE), small artery occlusion or lacunar infarction (LAC), infarction of other determined origin and infarction of undetermined cause (IUC). 8 Height and weight were recorded and body mass index was calculated as weight to height squared. Risk factors were docu- mented as previously described. 6,7 Carotid Ultrasonography Studies The CCA-IMT of all screened patients was assessed using high resolution B-mode ultrasonography (Acuson 128XP, equipped with a 7-MHz linear-array transducer), within the first 5 days of ictus. The CCA-IMT value was defined as the mean of the IMT of the right and left IMT of the CCA, calculated from 10 measurements on each side, taken 10 mm proximal to the carotid bifurcation. The previously anatomically validated lumen/intima leading edge (I-line) to media/ adventitia leading edge (M-line) method was used. 7,9 All ultrosono- graphic measurements were performed by the same experienced sonographer (C. P.), 7,9 –13 who was blinded to any clinical informa- tion about the study population. Received March 7, 2006; accepted April 6, 2006. From the Department of Neurology (G.T., K.Spengos, D.V.), University of Athens, “Eginition” Hospital, Athens, Greece; and the Acute Stroke Unit (K.V., C.P., E.M., K.Stamatelopoulos, N.Z.), Department of Clinical Therapeutics, University of Athens, “Alexandra” Hospital, Athens, Greece. Correspondence to Georgios Tsivgoulis, MD, Iofontos 2, 11634 Athens, Greece. E-mail [email protected] © 2006 American Heart Association, Inc. Stroke is available at http://www.strokeaha.org DOI: 10.1161/01.STR.0000226399.13528.0a 1913 by MARIA BELLADONNA on January 4, 2015 http://stroke.ahajournals.org/ Downloaded from
-
Upload
isnawan-widyayanto -
Category
Documents
-
view
213 -
download
1
description
stroke
Transcript of Stroke 2006 Tsivgoulis 1913 6
-
Common Carotid Artery Intima-Media Thickness and theRisk of Stroke Recurrence
Georgios Tsivgoulis, MD; Konstantinos Vemmos, MD; Christos Papamichael, MD;Konstantinos Spengos, MD; Efstathios Manios, MD; Kimon Stamatelopoulos, MD;
Demetrios Vassilopoulos, MD, PhD; Nikolaos Zakopoulos, MD
Background and PurposeIncreased common carotid artery intima-media thickness (CCA-IMT) has been associated withan increased risk of myocardial infarction and stroke. We investigated the relationship between CCA-IMT and recurrentstroke in a cohort of ischemic stroke patients.
MethodsHigh-resolution B-mode ultrasonographic measurements of the CCA-IMT were performed in a consecutiveseries of 238 patients hospitalized in our institution with first-ever ischemic stroke. Stroke risk factors and secondaryprevention therapies were documented. Patients were followed-up prospectively and the outcome event of interest wasrecurrent stroke.
ResultsDuring a mean follow-up period of 28.9 months (range: 6 to 60 months), 27 recurrent strokes were documented.Patients who experienced recurrent cerebrovascular events had significantly (P0.005) higher CCA-IMT values(1.01 mm, 95% CI:0.92 to 1.11 mm) than subjects who were free of stroke recurrence (0.88 mm, 95% CI:0.85 to0.91 mm). After adjustment for baseline characteristics, risk factors and stroke subtypes and secondary preventiontherapies increasing CCA-IMT was found to be an independent predictor of stroke recurrence. For each increment of0.1 mm in CCA-IMT the probability of experiencing recurrent stroke increased by 18.0% (95% CI:2.0% to 36.0%,P0.027).
ConclusionsIncreased CCA-IMT values are associated with a higher risk of long-term stroke recurrence. (Stroke. 2006;37:1913-1916.)
Key Words: atherosclerosis carotid arteries recurrence stroke
A growing body of evidence supports that the intima-media thickness of the common carotid artery (CCA-IMT) can be regarded as an early marker of atherosclerosis.1Furthermore, increased CCA-IMT has been associated withconventional cardiovascular risk factors,2 the presence ofother localizations of atherosclerosis3 and an increased risk ofmyocardial infarction4 and stroke.5
However, there are limited data regarding the potentialsignificance of CCA-IMT in predicting recurrent cerebrovas-cular events. Assuming that in addition to established riskfactors, increased CCA-IMT may constitute an important riskmarker for recurrent stroke, the present longitudinal studyaimed to evaluate the relationship between CCA-IMT andstroke recurrence in a cohort of consecutive first-ever ische-mic stroke (IS) patients.
Materials and MethodsStudy PopulationA series of 324 consecutive, first-ever acute stroke patients, admittedto the acute stroke unit and the general neurology ward of ourinstitution between January 2000 and December 2003 were screened.
All patients were included in The Athens Stroke Registry, acomputerized prospective observational data bank, gathered in 2university teaching hospitals.6,7 According to the Trial of Org 10172in Acute Stroke Treatment (TOAST) criteria, IS was classified basedon etiopathogenetic mechanisms into the following groups: largeartery atherosclerotic stroke (LAA), cardioembolic stroke (CE),small artery occlusion or lacunar infarction (LAC), infarction ofother determined origin and infarction of undetermined cause(IUC).8 Height and weight were recorded and body mass index wascalculated as weight to height squared. Risk factors were docu-mented as previously described.6,7
Carotid Ultrasonography StudiesThe CCA-IMT of all screened patients was assessed using highresolution B-mode ultrasonography (Acuson 128XP, equipped witha 7-MHz linear-array transducer), within the first 5 days of ictus. TheCCA-IMT value was defined as the mean of the IMT of the right andleft IMT of the CCA, calculated from 10 measurements on each side,taken 10 mm proximal to the carotid bifurcation. The previouslyanatomically validated lumen/intima leading edge (I-line) to media/adventitia leading edge (M-line) method was used.7,9 All ultrosono-graphic measurements were performed by the same experiencedsonographer (C. P.),7,913 who was blinded to any clinical informa-tion about the study population.
Received March 7, 2006; accepted April 6, 2006.From the Department of Neurology (G.T., K.Spengos, D.V.), University of Athens, Eginition Hospital, Athens, Greece; and the Acute Stroke Unit
(K.V., C.P., E.M., K.Stamatelopoulos, N.Z.), Department of Clinical Therapeutics, University of Athens, Alexandra Hospital, Athens, Greece.Correspondence to Georgios Tsivgoulis, MD, Iofontos 2, 11634 Athens, Greece. E-mail [email protected] 2006 American Heart Association, Inc.Stroke is available at http://www.strokeaha.org DOI: 10.1161/01.STR.0000226399.13528.0a
1913 by MARIA BELLADONNA on January 4, 2015http://stroke.ahajournals.org/Downloaded from
-
Follow-UpFor the needs of the present study only cases fulfilling the followingconditions were recruited (n253): (1) first-ever IS; (2) ultrasono-graphic measurements of the CCA-IMT (patients who succumbedduring the first 1 to 2 days after admission or patients with unavailableCCA-IMT measurements because of technical reasons were excluded);(3) white origin. Secondary stroke prevention therapies (lipid-lowering,antidiabetic and antihypertensive medications, antiplatelet agents, oralanticoagulants) were administered in the entire cohort in keeping to theEuropean Stroke Initiative recommendations.14 All surviving patientswere followed-up prospectively at 1 month, 3 months, 6 months andevery 6 months thereafter by a study investigator and a trained nurse byas previously reported.15 Follow-up was routinely performed at theoutpatient clinics of our institution. When patients failed to attend theirregular follow-up assessments at the hospital, they were contacted bytelephone calls. Furthermore, we conducted a face-to-face examinationin the patients place of residence in cases with severe residual handicapand in patients who missed 2 or more scheduled consecutive follow-upevaluations. The outcome events of interest was recurrent stroke,defined as cerebrovascular events of sudden onset, lasting for24 hours, clearly resulting in an increase of an existing or in a newneurological deficit.15 They were determined after evaluation of allthe available information obtained from hospital records, physiciansnotes in private practice, necropsy findings or death certificates, andthe patients clinical presentation at the regular follow-up assess-ments. A total of 15 patients who were lost during the follow-upperiod (8 cases after having moved from their initial place ofresidence failed to attend the follow-up evaluations and to return thetelephone calls, 3 cases of immigrant workers returned to theircountry of origin in the first months following the index event, 4cases declined to continue either the clinical or the telephonefollow-up evaluations without providing any specific reasons) wereexcluded from further evaluation.
Statistical AnalysisStatistical comparisons were performed between patients with andwithout recurrent stroke in terms of demographic features, stroke riskfactors, secondary prevention therapies and carotid ultrasonographicmeasurements using the 2 test (or the Fisher exact test) and the unpairedt test (or MannWhitney U test) as indicated. We also used ANCOVA(analysis of covariance) to compare the mean CCA-IMT between the 2stroke subgroups, after adjusting for baseline characteristics.
To evaluate which factors contribute to long-term recurrence, weperformed Cox proportional hazards analyses. In the initial univariateanalyses the association of demographic characteristics, stroke riskfactors and subtypes, secondary prevention therapies and CCA-IMTwith stroke recurrence was investigated. All factors that contributed tothe outcome in the initial univariate analyses at P0.1 were included inthe multivariate model as candidate variables and then removed bybackward stepwise selection procedure. In the final multivariate analy-ses, statistical significance was achieved if P0.05. To confirm therobustness of multivariate models, we repeated all multivariate analysesusing a forward-selection procedure. Associations are presented asrelative risks (RR) with corresponding 95% CI. Kaplan-Meier curves ofgroups of stroke patients stratified by CCA-IMT tertiles are alsopresented and survival free of stroke recurrence is compared betweenthe 3 subgroups using the log-rank method. The Statistical Package forSocial Science (SPSS Inc, version 10.0 for Windows) was used forstatistical analyses.
ResultsThe final studied population fulfilling all the above-mentionedinclusion criteria consisted of 238 first-ever IS patients. Thedistribution of IS subtypes was as follows: LAA 24.8% (n59),CE 25.6% (n61), LAC 29.4% (n70) and IUC 20.2%(n48). During the follow-up period (mean: 28.9 months, range:6 to 60 months), 51 (21.4%) deaths and 27 (11.3%) recurrentcerebrovascular events (21 cases of IS [8 cases of LAA, 5 casesof IUC, 4 cases of CE and 4 cases of lacunar infarction], 2 cases
of intracerebral hemorrhage and 4 cases with unspecified type ofrecurrence because of lack of follow-up brain imaging) weredocumented. Patients who experienced recurrent stroke weresignificantly older (P0.035) and had a significantly higher
Baseline Characteristics, Stroke Subtypes, SecondaryPrevention Therapies and Carotid UltrasonographicMeasurements in Patients With and Without Recurrent Stroke
Stroke Recurrence
VariableYes
(n27)No
(n211) P
Baseline Characteristics
Age 71.2 (11.5) 66.5 (10.8) 0.035
Male sex 66.7 60.7 0.546
Body mass index(kg/m2)
26.9 (3.3) 27.0 (2.5) 0.900
Hypertension 81.5 64.5 0.078
Diabetes mellitus 29.6 28.4 0.897
Hypercholesterolemia 33.3 30.8 0.789
Smoking 25.9 37.0 0.260
Alcohol intake 11.1 8.1 0.590
CHD 29.6 15.2 0.048
Atrial fibrillation 18.5 20.4 0.821
Heart failure 3.7 2.8 0.574
TIAs 25.9 10.0 0.015
Stroke Subtypes
LAA 29.6 24.2 0.536
CE 29.6 25.1 0.613
LAC 25.9 29.9 0.673
IUC 14.8 20.9 0.462
Secondary PreventionTherapies
Antiplatelet agents 85.2 81.5 0.641
Oral anticoagulants 14.8 18.5 0.641
Lipid-loweringmedications
33.3 30.8 0.789
Blood sugarloweringmedications
29.6 28.4 0.897
Diuretics 35.7 41.9 0.532
-blocking agents 7.1 15.7 0.229
Calcium antagonists 17.9 20.5 0.746
Angiotensin-convertingenzyme inhibitors
35.7 27.6 0.373
Angiotensin II receptorblocker
3.6 11.0 0.223
Direct vasodilator 7.1 1.0 0.538
Carotid UltrasonographicMeasurements
CCA-IMT (mean, 95% CI) 1.03 (0.941.12) 0.86 (0.830.90) 0.002
Adjusted CCA-IMT(mean, 95% CI)*
1.01 (0.921.11) 0.88 (0.850.91) 0.005
Continuous variables are presented as mean (SD), unless stated. Noncon-tinuous variables are presented as percentages.
*CCA-IMT values were adjusted for baseline characteristics by means ofanalysis of covariance (ANCOVA).
1914 Stroke July 2006
by MARIA BELLADONNA on January 4, 2015http://stroke.ahajournals.org/Downloaded from
-
frequency of coronary heart disease (CHD; P0.048) and oftransient ischemic attacks (TIAs; P0.015) before the IS incomparison to subjects with no recurrent stroke during theobservation period (Table). Patients in the recurrence group hadsignificantly (P0.005) higher CCA-IMT values (1.01 mm,95% CI: 0.92 to 1.11 mm) than subjects who were free of strokerecurrence (0.88 mm, 95% CI: 0.85 to 0.91 mm) even afteradjustment for demographic characteristics and stroke riskfactors.
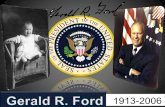
The association of baseline characteristics, stroke subtypes,secondary prevention therapies and CCA-IMT with stroke re-currence was evaluated using univariate Cox proportional haz-ards analyses. The following variables were significantly relatedto stroke recurrence and were therefore selected for entry into thefinal multiple-variable model: age (RR per 10-year in-crease:1.83, 95% CI: 1.21 to 2.75; P0.004), CHD (RR: 2.59,95% CI: 1.13 to 5.94; P0.024), hypertension (RR:2.13, 95%CI: 0.91 to 5.12; P0.098), history of TIAs (RR: 2.82, 95% CI:1.19 to 6.67; P0.018), CCA-IMT (RR per 0.1 mm increase:1.20, 95% CI: 1.08 to 1.34; P0.001). The multivariate Coxregression analyses (performed both with the backward-selection and forward-selection procedure) revealed only in-creasing age (RR per 10-year increase: 2.31, 95% CI: 1.23 to4.34; P0.009), history of TIAs (RR: 3.15, 95% CI: 1.10 to9.01; P0.033) and increasing CCA-IMT as independent out-come predictors. For each increment of 0.1 mm in CCA-IMT theprobability of experiencing recurrent stroke increased by 18.0%(95% CI: 2.0% to 36.0%; P0.027). Kaplan-Meier curves ofgroups stratified by CCA-IMT tertiles are presented in theFigure. Subjects with CCA-IMT measurements within the lowertertile had the lowest recurrence rate in comparison to thesubgroups of patients with CCA-IMT values within the medianor higher CCA-IMT tertile (log rank test: 18.83; P0.0001).
Because CCA-IMT is a marker of atherosclerosis and hasnot been associated with a cardiac source of embolism, werepeated all cox regression analyses after having excluded theCE subgroup. A more robust relationship between increasedCCA-IMT and the risk of recurrent stroke (RR per 0.1 mm
increase: 1.27, 95% CI: 1.11 to 1.46; P0.003) was docu-mented. Moreover, we included the patients who were lostduring the follow-up period in the multivariable Cox propor-tional hazards model and performed the analyses based on theworst-case scenario (assuming that all 15 patients had expe-rienced recurrent stroke). The association between CCA-IMTand stroke recurrence retained its statistical significance (RRper 0.1 mm increase: 1.15, 95% CI: 1.01 to 1.42; P0.042).Finally, the relationship between CCA-IMT and the differentrecurrent IS subgroups was investigated separately for eachsubtype of cerebral infarction. Increased CCA-IMT was anindependent predictor of recurrent LAA stroke (RR per0.1 mm increase: 1.25, 95% CI: 1.03 to 1.53; P0.020),whereas its association with recurrent LAC (P0.134), CE(P0.578) and IUC (P0.369) failed to reach the level ofstatistical significance.
DiscussionTo the best of our knowledge, no previous study has assessed theprognostic impact of CCA-IMT in predicting stroke recurrenceafter adjusting for established cardiovascular risk factors, strokesubtypes and secondary prevention therapies. Carotid IMT hasbeen associated with incident cardiovascular4 and cerebrovascu-lar disease5 in previously healthy people. Moreover, 2 studieshave identified CCA-IMT as an independent predictor of recur-rent cardiovascular disease in patients who had undergonecoronary artery bypass surgery16 or had prevalent CHD.17 Itshould be noted though that the association between CCA-IMTand stroke recurrence was not investigated in any of the formerstudies. Hence, the present analyses confirm and extend thefindings of previous investigations regarding the prognosticsignificance of CCA-IMT.
Interestingly, we also noted that increased CCA-IMT corre-lated more strongly with the risk of recurrent LAA stroke thanwith other IS subtypes. Because CCA-IMT is a marker of thetotal atherosclerotic burden of the vascular tree,1,3,12 it is con-ceivable that increased CCA-IMT values may reflect a higherrisk of recurrent IS caused by an underlying atherothrombotic
Kaplan-Meier curves of patients survivingfree from stroke recurrence according totertiles of CCA-IMT values.
Tsivgoulis et al CCA-IMT and Stroke Recurrence 1915
by MARIA BELLADONNA on January 4, 2015http://stroke.ahajournals.org/Downloaded from
-
mechanism. However, the limited number of patients in thesubgroups of recurrent IS should be taken into considerationwhen interpreting our data.
Increased CCA-IMT values have been related to a variety ofvascular risk factors such as older age, hypertension, diabetesmellitus, hyperlipidemia and cigarette smoking.2 Thus, it can beargued that if IMT reflects exposure to cardiovascular riskfactors, it can be considered as an intermediate factor in thecausal pathway between risk factors and stroke. Interestingly, inour report increasing CCA-IMT values remained an independentpredictor of stroke recurrence after adjustment for conventionalrisk factors. This suggests that besides being an intermediatephenotype between vascular risk factors and cerebrovasculardisease, CCA-IMT may be a risk factor itself. In favor of thisassumption is the strong evidence supporting a genetic compo-nent to IMT variability, with genetic factors contributing to 38%of the interindividual differences in IMT.18
Finally, certain limitations of the present report should beaddressed. First, a number of risk factors like smoking andhypertension were defined as binary variables although durationand severity are important. Second, the potential observers biasduring follow-up, affecting the documentation of recurrentcerebrovascular events, represents an additional limiting factorof our study. Of note though, the recurrent strokes were mostlydevastating or fatal (8 cases) and in most cases confirmed bymeans of hospital records, brain imaging and autopsy findings.Third, although the same experienced sonographer performedthe IMT studies, it should be acknowledged that they wereconducted by a hand-held transducer and not by semi-automatedsoftware. Fourth, association does not meet causality and ourstudy having an observational nature cannot prove a causalrelationship of CCA-IMT with stroke recurrence.
In the present study we provide evidence that increasedCCA-IMT is an adverse prognostic factor for recurrent strokein addition to established cardiovascular risk factors. Newtherapeutic approaches to carotid atherosclerosis underlinethe potential clinical implications of our work. Antihyperten-sive drugs (especially angiotensin-converting enzyme inhib-itors, and -blockers) and statin treatment have been shownto reduce the development of atherosclerosis measured asCCA-IMT.19 Thus, CCA-IMT may be a useful noninvasiveadjunctive tool in assessing the risk of recurrent stroke and indistinguishing IS patients that may benefit the most frommore aggressive secondary prevention treatment strategies.
AcknowledgmentsThe authors would like to thank Miss Mary Batsara for her valuablehelp in data collection.
DisclosuresNone.
References1. Grobbee DE, Bots ML. Carotid artery intima-media thickness as an
indicator of generalized atherosclerosis. J Intern Med. 1994;236:567573.2. Salonen R, Salonen JT. Determinants of carotid intima-media thickness:
a population-based ultrasonography study in eastern Finnish men. J InternMed. 1991;229:225231.
3. Allan PL, Mowbray PI, Lee AJ, Fowkes FG. Relationship betweencarotid intima-media thickness and symptomatic and asymptomatic pe-ripheral arterial disease. The Edinburgh Artery Study. Stroke. 1997;28:348353.
4. Chambless LE, Heiss G, Folsom AR, Rosamond W, Szklo M, SharrettAR, Clegg LX. Association of coronary heart disease incidence withcarotid arterial wall thickness and major risk factors: the AtherosclerosisRisk in Communities (ARIC) Study, 19871993. Am J Epidemiol. 1997;146:483494.
5. OLeary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, WolfsonSK Jr. Carotid-artery intima and media thickness as a risk factor formyocardial infarction and stroke in older adults. Cardiovascular HealthStudy Collaborative Research Group. N Engl J Med. 1999;340:1422.
6. Vemmos KN, Takis CE, Georgilis K, Zakopoulos NA, Lekakis JP,Papamichael CM, Zis VP, Stamatelopoulos S. The Athens stroke registry:results of a five-year hospital-based study. Cerebrovasc Dis. 2000;10:133141.
7. Tsivgoulis G, Vemmos KN, Spengos K, Papamichael CM, CimboneriuA, Zis V, Zakopoulos N, Mavrikakis M. Common carotid arteryintima-media thickness for the risk assessment of lacunar infarctionversus intracerebral haemorrhage. J Neurol. 2005;252:10931100.
8. Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL,Marsh EE 3rd. Classification of subtype of acute ischemic stroke. Defi-nitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172in Acute Stroke Treatment. Stroke. 1993;24:3541.
9. Vemmos KN, Tsivgoulis G, Spengos K, Papamichael CM, Zakopoulos N,Daffertshofer M, Lekakis JP, Mavrikakis M. Common carotid arteryintima-media thickness in patients with brain infarction and intracerebralhaemorrhage. Cerebrovasc Dis. 2004;17:280286.
10. Zakopoulos NA, Tsivgoulis G, Barlas G, Papamichael C, Spengos K,Manios E, Ikonomidis I, Kotsis V, Spiliopoulou I, Vemmos K,Mavrikakis M, Moulopoulos SD. Time rate of blood pressure variation isassociated with increased common carotid artery intima-media thickness.Hypertension. 2005;45:505512.
11. Zakopoulos N, Papamichael C, Papaconstantinou H, Dubbins PA, BurrellCJ, Lekakis J, Stamatelopoulos S, Moulopoulos S. Isolated clinic hyper-tension is not an innocent phenomenon: effect on the carotid arterystructure. Am J Hypertens. 1999;12:245250.
12. Kotsis VT, Pitiriga VCh, Stabouli SV, Papamichael CM, Toumanidis ST,Rokas SG, Zakopoulos NA. Carotid artery intima-media thickness couldpredict the presence of coronary artery lesions. Am J Hypertens. 2005;18:601606.
13. Lekakis JP, Papamichael CM, Vemmos CN, Voutsas AA, Stamatelopoulos SF,Moulopoulos SD. Peripheral vascular endothelial dysfunction in patientswith angina pectoris and normal coronary arteriograms. J Am CollCardiol. 1998;41:541546.
14. Hacke W, Kaste M, Skyhoj Olsen T, Bogousslavsky J, Orgogozo JM; forthe EUSI Executive Committee. Acute treatment of ischaemic stroke.European Stroke Initiative (EUSI): Cerebrovasc Dis. 2000;10(Suppl3):2233.
15. Tsivgoulis G, Spengos K, Zakopoulos N, Manios E, Xinos K, Vassilopoulos D,Vemmos KN. Twenty four hour pulse pressure predicts long term recur-rence in acute stroke patients. J Neurol Neurosurg Psychiatry. 2005;76:13601365.
16. Hodis HN, Mack WJ, LaBree L, Selzer RH, Liu CR, Liu CH, Azen SP.The role of carotid arterial intima-media thickness in predicting clinicalcoronary events. Ann Intern Med. 1998;128:262269.
17. Wattanakit K, Folsom AR, Chambless LE, Nieto FJ. Risk factors forcardiovascular event recurrence in the Atherosclerosis Risk in Commu-nities (ARIC) study. Am Heart J. 2005;149:606612.
18. Fox CS, Polak JF, Chazaro I, Cupples A, Wolf PA, DAgostino RA,ODonnell CJ; Framingham Heart Study. Genetic and environmentalcontributions to atherosclerosis phenotypes in men and women: herita-bility of carotid intima-media thickness in the Framingham Heart Study.Stroke. 2003;34:397401.
19. Wiklund O, Hulthe J, Wikstrand J, Schmidt C, Olofsson SO, Bondjers G.Effect of controlled release/extended release metoprolol on carotidintima-media thickness in patients with hypercholesterolemia: a 3-yearrandomized study. Stroke. 2002;33:572577.
1916 Stroke July 2006
by MARIA BELLADONNA on January 4, 2015http://stroke.ahajournals.org/Downloaded from
-
ZakopoulosEfstathios Manios, Kimon Stamatelopoulos, Demetrios Vassilopoulos and Nikolaos Georgios Tsivgoulis, Konstantinos Vemmos, Christos Papamichael, Konstantinos Spengos,Common Carotid Artery Intima-Media Thickness and the Risk of Stroke Recurrence
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright 2006 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.0000226399.13528.0a
2006;37:1913-1916; originally published online May 25, 2006;Stroke.
http://stroke.ahajournals.org/content/37/7/1913World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in theRequest Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by MARIA BELLADONNA on January 4, 2015http://stroke.ahajournals.org/Downloaded from


![Jambalaya [yearbook] 1913](https://static.fdocuments.us/doc/165x107/613ca128f046235e845cdd2c/jambalaya-yearbook-1913.jpg)