Screening Adults for Trauma Wendy Standifer, MA LPC, NCC.
25
Screening Adults for Trauma Wendy Standifer, MA LPC, NCC
-
Upload
dora-thomas -
Category
Documents
-
view
222 -
download
2
Transcript of Screening Adults for Trauma Wendy Standifer, MA LPC, NCC.

Screening Adults for Trauma
Wendy Standifer, MA LPC, NCC

The Purpose of This Training:
• Provide a brief overview of trauma
• Identifying various screening tools including self-assessments, symptoms checklists and questionnaires.
• Integrating screening questions into assessments and having trauma informed practices built into assessments.
• Addressing Secondary Trauma for staff

Trauma
• National community-based surveys find that between 55 and 90% of us have experienced at least one traumatic event over the course of a lifetime – and individuals report that, on average, they have experienced nearly five traumatic events!
• The experience of trauma is simply not the rare exception we once considered it to be (Fallot & Harris, 2009). It is the expectation, rather than the exception.
• Most individuals seeking public behavioral health services and many other public services, such as homeless and domestic violence services, have histories of physical and sexual abuse and other types of trauma-inducing experiences.

Traumatic Experiences
The impact of trauma is broad and touches multiple life domains. It is often deep and life-altering. These experiences can lead to:
• Mental Health Disorders (PTSD, Depression, Anxiety, etc.)
• Chronic health conditions
• Substance abuse
• Eating disorders
• HIV/AIDS

PTSD
• Re-experiencing the traumatic event: Intrusive, upsetting memories of the event; Flashbacks; Nightmares; Feelings of intense distress when reminded of trauma; Intense physical reactions of reminds of the event
• Avoidance and emotional numbing: Avoiding activities, places, thoughts, or feelings that remind you of the trauma; Inability to remember important aspects of the trauma; Loss of interest in activities and life in general; Feeling detached and emotionally numb; Sense of limited future
• Increased arousal: Difficulty falling or staying asleep; Irritability or outbursts of anger; Difficulty concentrating; Hyper-vigilance; Feeling jumpy and easily startled

Trauma Intervention
Trauma-specific interventions are designed specifically to address the consequences of trauma in the individual and to facilitate healing. Treatment programs generally recognize the following:
• The survivor's needs
• The interrelation between trauma and symptoms
• Collaboration with family and friends of the survivor as well as human
services agencies

How Do we Address Individuals with a History of Trauma?
We need to presume the individuals we serve have a history of traumatic stress and exercise
“UNIVERSAL PRECAUTIONS”
(Hodas, 2004)

Trauma Informed Screening & Assessments• Trauma-informed care means that regardless of
the reasons an individual comes to an organization, clinical staff asks them about their trauma history.
• Not what they did – But what happened to them.• We must ask respectfully.• And be prepared to listen.• Many times individuals don’t understand a trauma
has occurred and will not be able to identify it as a trauma
• May need to ask in may ways and in many places.• It may take time for them to be ready to talk.
SCREENING TOOLS

ACE•The Adverse Childhood Experiences Study (ACE Study) conducted by the Centers for Disease Control and Prevention and Kaiser Permanente. Is one of the largest investigation ever conducted to assess associations between childhood maltreatment and later-life health and wellbeing.
•Almost 2/3 of the study participants reported at least oneadverse childhood experience of physical or sexual abuse,neglect or family dysfunction and more than 1 of 5 reportedthree or more such experiences.
•The greater the number of adverse experiences = the risk for negative outcome.

ACE cont:
• These include:Alcoholism and Alcohol UseDepressionIllicit Drug UseRisk for intimate partner violenceSexually transmitted diseasesSuicide attemptsUnintended pregnancies
• A trauma survivor with an ACE score of 4 has a increase chance of 1350% of using or abusing substances.• A trauma survivor with an ACE score of 6 has a increase chance of 4600% of using or abusing substances.

ACE Finding Your ACE ScoreWhile you were growing up, during your first 18 years of life:
1. Did a parent or other adult in the household often or very often… Swear at you, insult you, put you down, or humiliate you? Or Act in a way that made you afraid that you might be physically hurt? Yes No If yes enter 1 ________2. Did a parent or other adult in the household often or very often…Push, grab, slap, or throw something at you? Or Ever hit you so hard that you had marks or were injured?
Yes No If yes enter 1 ________3. Did an adult or person at least 5 years older than you ever… Touch or fondle you or have you touch their body in a sexual way? Or Attempt or actually have oral, anal, or vaginal intercourse with you?
Yes No If yes enter 1 ________4. Did you often or very often feel that …No one in your family loved you or thought you were important or special? Or Your family didn’t look out for each other, feel close to each other, or support each other?
Yes No If yes enter 1 ________
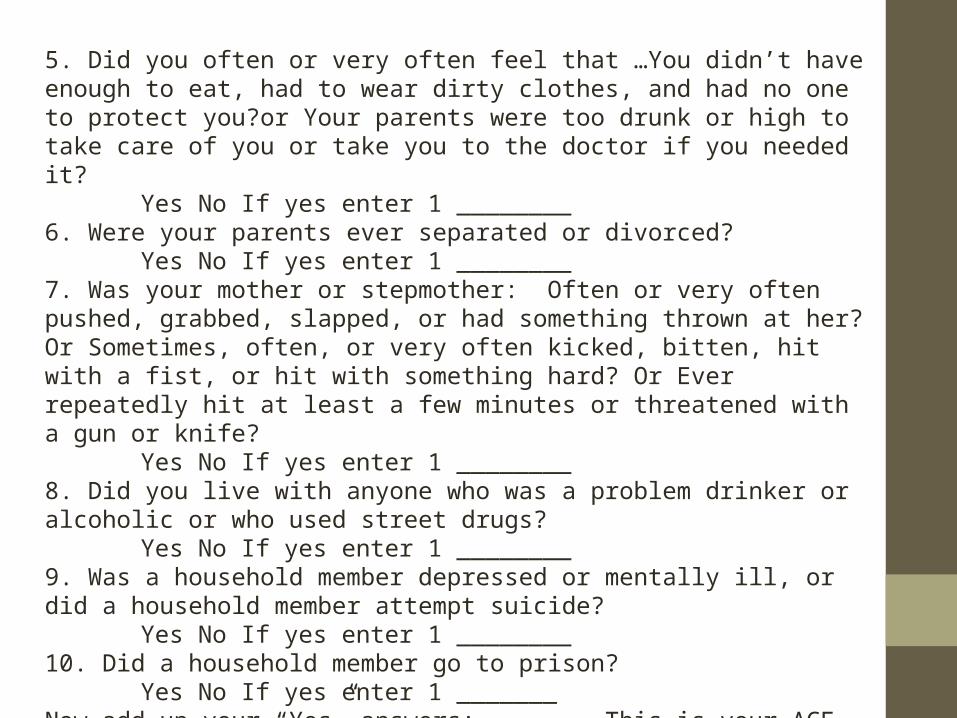
5. Did you often or very often feel that …You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you?or Your parents were too drunk or high to take care of you or take you to the doctor if you needed it?
Yes No If yes enter 1 ________6. Were your parents ever separated or divorced?
Yes No If yes enter 1 ________7. Was your mother or stepmother: Often or very often pushed, grabbed, slapped, or had something thrown at her? Or Sometimes, often, or very often kicked, bitten, hit with a fist, or hit with something hard? Or Ever repeatedly hit at least a few minutes or threatened with a gun or knife?
Yes No If yes enter 1 ________8. Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
Yes No If yes enter 1 ________9. Was a household member depressed or mentally ill, or did a household member attempt suicide?
Yes No If yes enter 1 ________10. Did a household member go to prison?
Yes No If yes enter 1 _______Now add up your “Yes” answers: _______ This is your ACE Score

PTSD Checklist• The PCL is a standardized self-report rating scale for PTSD
comprising 17 items that correspond to the key symptoms of PTSD. Two versions of the PCL exist: Handout A
1)PCL-M is specific to PTSD caused by military experiences2)PCL-C is applied generally to any traumatic event.• The PCL can be easily modified to fit specific time frames
or events. For example, instead of asking about “the past month,” questions may ask about “the past week” or be modified to focus on events specific to a deployment.
• The PCL is self-administered. Respondents indicate how much they have been bothered by a symptom over the past month using a 5-point (1–5) scale, circling their responses. Responses range from 1 Not at All – 5 Extremely

Checklist cont:
• How is the PCL Scored?• 1) Add up all items for a total severity score• or• 2) Treat response categories 3–5 (Moderately or
above) as symptomatic and responses• 1–2 (below Moderately) as non-symptomatic, then
use the following DSM criteria for a diagnosis:• Symptomatic response to at least 1 “B” item
(Questions 1–5),• Symptomatic response to at least 3 “C” items
(Questions 6–12), and• Symptomatic response to at least 2 “D” items
(Questions 13–17)

Trauma Checklists
Trauma Measures from National Center for PTSD:
•Trauma Symptom Inventory (TSI)
•Trauma Symptom Checklist- 40 (TSC-40)- Handout B
•Screen for Post Traumatic Stress Symptoms (SPTSS)
•Post Traumatic Diagnostic Scale (PDS)
•Distressing Events Questionnaire (DEQ)

Trauma Assessment for Adults - Self-Report Version• When conducting a comprehensive assessment, often it
can be helpful to let the individual guide how much information he or she tells you.
• Some clinicians might say….”I’m going to ask you some questions about current or past trauma you may have experienced. If you have questions or are unsure about anything I’m asking you, please let me know. If you don’t wish to answer the questions at this time, you can let me know that too.”
• Important to Remember: This does not mean that you would never ask the questions again, but you could ask them in different ways or return to them later.
• The point is to make it clear that the information is important to their overall assessment and treatment and you are open to hearing the information in the most respectful way possible.
• For some individuals you may take each question one at a time, or you may read them all so the person knows what’s coming and then go back to each one to get an answer.
• For some individuals, they may feel more comfortable checking off the response themselves.
• While it’s important that the clinician knows the definitions of what is being asked, e.g., what physical assault/abuse is and able to provide some psycho education if asked or when helpful, many individuals may not use the same terms that are there and may not think that their experience “fits” the definition, so it’s okay to have the clinician ask the individual if it would be okay if we put what the person is describing, e.g., that they were pushed or shoved rather than physically abused. This would also be something that could be returned to later and worked on over time through therapy and psycho education.
• In some situations, individuals may just start pouring out information, and you may need to set some parameters around this for them. Although it may be important to get it out, vomiting the information can lead some individuals to feel overwhelmed, ashamed and vulnerable later.
• So letting them know that you want to hear what is important for them to share, and at the same time want them to feel comfortable later with what they have shared, so it might be important to pace what they are sharing and check in with them how they are thinking and feeling about it with a plan to make working through the trauma a part of the treatment plan.

• It is recommended that you review the screen and ask the individual about experiences they may have identified particularly in conducting a thorough assessment and in setting goals.
• It is also very possible that responses on the screen may differ from responses that are obtained in the History during the assessment. Sometimes this occurs because someone is ready to talk about their experiences, may have just recalled them or may feel safe enough to talk more openly. Sometimes it may also reflect a shutting down or not wanting to bring up information.
• If there is a different response noted, this may just be reflecting the ambivalence, anxiety or other feelings the person is experiencing and may be explored, in a gentle manner within the therapeutic relationship rather than in a confrontational manner as to why the responses differ.
• Handout C

Assessments/ Trauma InformedSensitive Responses to Disclosure of Traumatic
Experiences• I’m sorry you were hurt in that way.• You are not alone. Unfortunately, (childhood abuse,
domestic violence, sexual assault) is more common than people recognize• It takes a lot of courage to tell your story.• You have been through a lot and survived.• You must be very strong.• What happened was not your fault.• You are not to blame for what happened to you.• Let me know how I can make you more comfortable
as we continue with this meeting.• You deserve help in dealing with something so
difficult.

Assessments cont:
Suggestions for Avoiding Re-traumatization
• Avoid positioning yourself between the individual and the door. • Ask what you can do to make the interview
process more comfortable• Use grounding techniques if the person seems to
be disconnected or in distress.• Restore a sense of control to the person by
providing them with as much choice as possible.• Instill hope.

• These are meant to serve as general guidelines. • Every individual is different, as are their
experiences and that is very important to remember.
• For some individuals who have experienced trauma, the healing process, may begin with the question, for others, it may be started in a trusting therapeutic relationship, for others it may begin with psycho education.
• Being open and asking about trauma allows the person to hear that you want to know what happened to them rather than what is wrong with them.

Addressing Secondary Trauma• Secondary trauma is commonly referred to as "the stress
resulting from helping or wanting to help a traumatized or suffering person.
• It is crucial that those in the healing profession address their past traumas in their education and on an on-going basis to prevent transference to consumers and to ensure staying healthy for themselves.
• All professionals, paraprofessionals or family members who work with and/or assist traumatized or distressed children, adults or families are at risk for secondary trauma
• Secondary trauma is a contributing factor to turnover. Turnover brings down staff morale, increases the workload for remaining staff, results in poor continuity of care for children and families, and prevents organizations from forming a high functioning and cohesive workforce.
Things to for secondary trauma
•Complete Professional Quality of Life Scale (PROQOL)- Handout D•Develop Trauma Informed Supervisor Guidelines •Definitions of Burnout and Compassion Fatigue•Provide Specific Resources for Staff :-Transforming Compassion Fatigue Into Compassion Satisfaction: -Top 12 Self-Care Tips for Helpers
-Provider Self-Care. National Center for Child Traumatic Stress ----How to heal, grow and prosper in challenging times
-What I wish I had known: Burnout & Self-care in our Social Work Profession•Refer to EAP programs

THANK YOU
QUESTIONS