Ethics in Addictions Counseling Leigh Falls, Ed.S., LPC, NCC.

Rutgers, The State University of New Jersey Liberty Plaza, 335 George Street, New Brunswick, NJ 08901
http://rwjms.rutgers.edu/boggscenter p. 732-235-9300 f. 732-235-9330
Robin VanEerden, MS, NCC, LPC, NADD-CC Vice President of Clinical Operations and Services
Integrative Counseling Services, PC Harrisburg, PA
Building Statewide Capacity and Implementing Best Practices for People with Dual Diagnosis
Living in the Community
October 9, 2015 The Hotel Woodbridge at Metropark, Iselin, NJ
The attached handouts are provided as part of The Boggs Center’s continuing education and dissemination activities. Please note that these items are reprinted by permission from the author. If you desire to reproduce them, please obtain permission from the originator.


10/5/2015
1
Building Statewide Capacity and Implementing Best Practices for People Living with Dual Diagnosis Living in the
Community
Objectives
• Participants will be able to describe effective strategies to build statewide capacity to best support individuals with IDD/MI living in the community.
• Participants will be able to identify specific best practices.
• Participants will be able to identify needs and gaps in training and service delivery.
Historical Structure
• 1990 State Centers and State Hospitals housed people with both developmental disabilities and mental health disorders
• 1991 The first bulletin was presented about Positive Approaches
• 1991 De‐institutionalization became a reality
Infrastructure and System Design1991 ‐ 2004
• County based Administrative Entities became the oversight of waiver services
• The PA Office of Developmental Programs was supportive and a licensing entity that assisted with overall compliance to community and facility based regulations
• 2004 the Positive Practices Bulletin was released to enhance person centered services
2001 – Present Risk and Quality Management Systems
• Incident Management System
• Risk Management Activities
• Data Analysis
• Core Indicators for Quality Management were identified.
• Both State and County Systems
• Identified Clinical expertise was needed
The Journey’s Beginning
• Increasing struggle to support people with complex needs
–Increased State Center and State Hospital admissions
–People on inpatient psychiatric units for extended periods
–Provider/County/Community Mental Health frustration
–Arenas for learning had decreased
10/5/2015
2
The Journey of Dual Diagnosis2011‐2015
• Utilized both clinical skills and global system change methodology
• Identified what was already in place and how to use these resources effectively
• Identified a common “risk factor” to begin to put processes in place
Enter Stage Right ‐ Interdependence
State Level and Contracted Entities
• The Health Care Quality Units
• Clinical Directors• Risk Managers
• Positive Practices Groups
County Organizations
• Administrative Entities
• Supports Coordination Units
• Rapid Response Teams
Journey Across Multiple Activities
A Comprehensive
Approach
A Comprehensive
Approach
StatewideStatewide
RegionalRegional
LocalLocal
A Multi‐tiered Approach to Evaluation
CollaborationCollaboration
ReviewReview
AnalysisAnalysisDevelopmentDevelopment
EvaluationEvaluation

10/5/2015
3
Efforts
Psychiatric Discharge Planning
Bi‐Weekly Incident Reviews
Technical Assistance Follow‐up takes place
Recommendations may be made as part of the Incident Management Reporting Process, OR
Immediate steps for intervention are taken when the IM process has been exhausted or is not
appropriate or timely enough
Additional information is reviewed (To answer questions on next page)
Other psychiatric hospitalizations SC notes, ISP, Behavior plan etc...
Report of psychiatric admissions is pulled from HCSIS
AE Incident Manager pulls report on a regular basis
AE DD Coordinator review and include MH DD Coordinator
Results 3 Year Evaluation
Positive Practices
Statewide
Western
Steering Committee
Resources and Development
Training and Collaboration
Central
Central
Northeast
Southeast
Rapid Response Teams
Resources
DDTT
Peer Support
CSRU
WRAP

10/5/2015
4
Training
Intensive Systems Therapy
Person Directed
Framework
Dual Diagnosis Curriculum
FASD
Identifying Additional Gaps
• Continued to be gaps in the system for some people
• “At Risk” people continued to be identified
• Typical behavioral support therapies/interventions were not working
• Trends were beginning to come to the surface (FASD)
• Transitional age coming from children services into adult services
Risk Screening for Best Practice
Developed from all best practices that were embraced and accepted by the Office of Developmental Programs over the past 35 years
Established best practices were across the state were not being used consistently
The knowledge of person centered planning, positive approaches, and positive behavioral supports were no longer evident due to high staff turn over rates and decreased opportunities for learning.
Restrictive procedure plans were becoming more frequently used and if not used people were losing their placements
National Standards for treatment (i.e.NADD) were not being taught/implemented consistently
Bio‐Psycho‐Social Model
• The biopsychosocial model (abbreviated "BPS") is a general model or approach stating that biological, psychological (which entails thoughts, emotions, and behaviors), and social (socio‐economical, socio‐environmental, and cultural) factors, all play a significant role in human functioning in the context of disease or illness. It posits that, health is best understood in terms of a combination of biological, psychological, and social factors rather than purely in biological terms
NOTHING STANDS ALONE
Bio‐Psycho‐Social Influences
Biosocial influences
Psycho‐Biologicalinfluences
Biological
Social Psychological
Bio‐psycho‐social influences
interplay and overlap!
Psychosocial influences
Everything is InterrelatedThe bio‐psycho‐social concept
24
10/5/2015
5
Bio-Psycho-Social
• Physical Health must be addressed first• Eating Patterns• 24 Hours Sleep Data (data from a month cycle)• Genetic data (if known)• Environmental Changes• Social and Developmental History• Family Medical/ Mental Health History
Bio-Psycho-Social
• Medication Changes• History of Presenting Problem and Past
Psychiatric History• Mood Charting• Strengths and Vulnerabilities• Symptoms and Behavioral Manifestations
• AKA: symptom driven behavior
Holistic Philosophy
• What do we consider when we think of a person
• Consider the whole person: past and present
• “The whole is greater than the sum of its parts”, Aristotle
• CWhat do we consider when we think of a person
Risk Screening for Best PracticeBenefits
• Bio‐psycho‐social format and structure
• Addresses neurodevelopmental disorders
• One size does not fit all – individualized
• Framework for accountability
• Provides an effective journey toward effective treatment
• Strength based
Benefits
• Identifies gaps and needs
• Learning tool (can be helpful for certification in Dual Diagnosis)
• Screening tool so it does not have to be done by a clinician
• Opens discussion and communication between all entities
Risk Screening for Best Practice Challenges
• Clinicians overall are not plentiful in the field
• Certification in Dual Diagnosis (specialists, direct care professionals, clinicians, organizations) while now available are not plentiful
• Arenas to study, network and learn are not abundant
10/5/2015
6
Risk Screening for Best Practice
• Reviewed by all Offices of Developmental Disabilities
• Reviewed by Mental Health and Substance Abuse
• Reviewed by the Bureau of Autism Services
• Reviewed by the Center of Excellence for FASD
• Supplement to Psychiatric Discharge Planning Process
Risk Screening for Best Practice
• Meet with the entire team
• Fill out the checklist
• Identify the gaps
• Write a consult report that includes all aspects of best practices for people with Dual Diagnosis (individualized depending on etiology)
• Assist in finding resources/research/tools etc.
Statistics
• The central region where the risk screening was approved for use had the lowest rate of admissions to state centers and state hospitals
• The central region had the lowest rate of people at risk of losing a placement (or being diverted from a state facility)
• It helped identify the future trending of what needs to be done in services for Dual Diagnosis
Statistics
• A 2013‐2014 and 2014‐2015 fiscal year analysis was completed on people who were admitted those years to state centers and state hospitals the results were as follows:
Statistics
• 100% had co‐occurring disorders (MH/ID/Neurodevelopmental)
• 100% had PTSD and/or complex trauma histories
• 71% had an FASD
• 64% had a Personality Disorder
• 36% had Autism
• The average age: 22.33 years and are still currently admitted
Summary
• Begin to look at the resources that are already established and how they can be retooled or utilized more effectively
• Look at the structure from top down and hold all entities accountable to the rolls and responsibilities within the structure
• Identify gaps in clinical leadership, programs, risk management activities and community services

10/5/2015
7
Summary
• Create what works, leave behind what does not
• Network and partner with National Associations
• Build bench strength (capacity) statewide with all stakeholders
• A culture of support/learning/ so competency can be achieved
References
• Psychiatric Discharge Planning Process/Adminstrative Entity Process to Decrease Inpatient Psychiatric Readmissions: Cheryl Parker, M.Ed, 2012
• Risk Screening for Best Practice and Glossary Revised: Robin VanEerden, MS, NCC, LPC, NADD‐CC, 2015
• Statistical report for future planning: Robin VanEerden, MS, NCC, LPC, NADD‐CC, 2015
• Bio‐psycho‐social slides, NADD Specialists Presentation, 2015, www.thenadd.org
Contact Information
Robin VanEerden
Vice President of Clinical Operations and Services
Integrative Counseling Services, PC
www.integrativecounselingpc.com
717.412.4908

Implementing Psych Review Process PROCESS CHART
DD Coordinator/PPRT lead/Risk Manager pulls bi-
weekly psych hospitalizations from HCSIS
Review via incident management process
(attached)
Alert Program rep of hsopitalizations of concern (if
person has been hospitalizaed more than once in last year, requires review)
Program rep and DD coordinator/PPRT lead/risk manager determine course
of action-program rep converys to AE
AE DD coordinator pulls weekly psych reports
Reviews incidents per process with MH DD
coordinator as necessary Intervenes as necessary
Not approve incidents if corrective action
is not likely to prevent incidents in future
Direct contact with team, or continued review once the
incident has been submitted
Request assistacne if needed from HCQU/ODP DD
Coordinator etc... Track data for evaluation
In order to do this-HCSIS-Tools-Reports-Reports request-Incidents by consumer detail, select date range-ODP Primary Incident Category: Psychiatric Hospitalization-select region-Exclude state centers-select report format

Questions/ criteria for review on next page
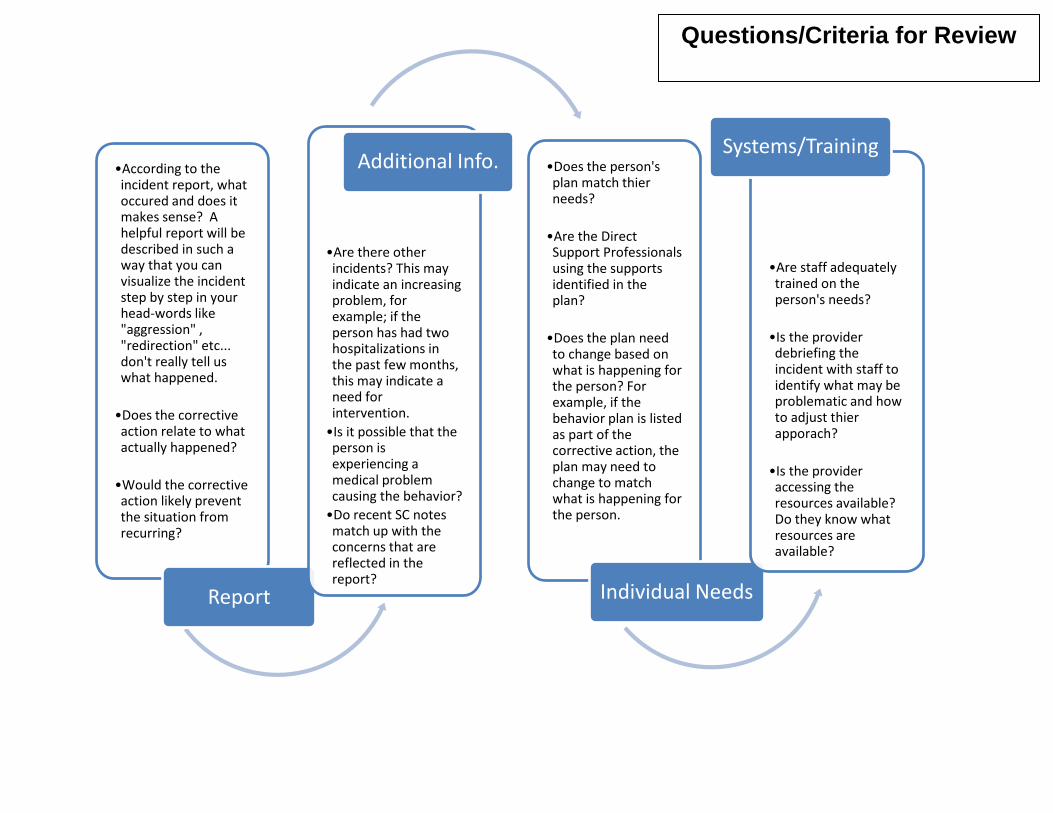
•According to the incident report, what occured and does it makes sense? A helpful report will be described in such a way that you can visualize the incident step by step in your head-words like "aggression" , "redirection" etc... don't really tell us what happened.
•Does the corrective action relate to what actually happened?
•Would the corrective action likely prevent the situation from recurring?
Report
•Are there other incidents? This may indicate an increasing problem, for example; if the person has had two hospitalizations in the past few months, this may indicate a need for intervention. •Is it possible that the person is experiencing a medical problem causing the behavior? •Do recent SC notes match up with the concerns that are reflected in the report?
Additional Info. •Does the person's plan match thier needs?
•Are the Direct Support Professionals using the supports identified in the plan?
•Does the plan need to change based on what is happening for the person? For example, if the behavior plan is listed as part of the corrective action, the plan may need to change to match what is happening for the person.
Individual Needs
•Are staff adequately trained on the person's needs?
•Is the provider debriefing the incident with staff to identify what may be problematic and how to adjust thier apporach?
•Is the provider accessing the resources available? Do they know what resources are available?
Systems/Training
Questions/Criteria for Review

Resources/Tools Challenges/ Concerns
Med
ical
eva
luat
ion
Cris
is P
lan
Func
tiona
l Beh
avio
r As
sess
men
t
Safe
ty P
lan
Beha
vior
Pla
n
Biog
raph
ical
tim
elin
e
Disc
harg
e Pl
anni
ng
Med
icat
ion
revi
ew/m
ed
trac
king
Sexu
ality
/ris
k as
sess
men
t/ed
ucat
ion
Debr
iefin
g to
ols
Occ
upat
iona
l the
rapy
as
sess
men
t/se
nsor
y as
sess
men
t Co
mm
unic
atio
n as
sess
men
t/to
ols
Fade
pla
n
Tran
sitio
n Pl
an
Behavior Changes X x x x x Self injury x x x x x x x x x Sexualized comments/behavior
x x x x x x
Frequent hospitalization
x x x x x x x x x x x
Frequent Criminal justice involvement
x x x x x x x x x x x x
Change in placement
x x x x x x x
Restraint use X X X X X X X X X X X Abuse x X X History of trauma X X X X X X X X X X x Known psychiatric diagnoses
X X X X X X X X X X
Autism spectrum disorder
X X X X X
Sex offending behavior
X X X X X X X X X X X X
Communicates using non-traditional means
X X X X X X
Aggression (physical/verbal)
X X X X X X X X X X X
Transition from child to adult services
X
X
X
X
X
X
X
High staff turnover X X X X X X X X X X X

Psychiatric Hospitalization Discharge Planning
Administrative Entities, Supports Coordination, Provider Organizations, Families and Individuals
should be aware that Discharge Planning for a patient with an Intellectual Disability and a Mental
Health Disorder should begin immediately following admission to the hospital.
Following are action steps and a checklist to serve as a guideline to aid in assuring the most appropriate
support is available for a person following a psychiatric hospitalization. Discharge planning is a critical
part of the person’s treatment and is typically handled by a designated staff at the hospital; this could be
a social worker, nurse, case manager etc… To offer the most appropriate support upon discharge there
are critical pieces of information we must ensure we have. A member of the person’s team should be
responsible for communicating with the hospital on a regular basis and the team should ensure that this
information is captured throughout the course of the hospital stay.
Name: Date of Admission:
Date of Discharge:
Debriefing-to be completed within 24 hours of admission Date Completed:
What were the circumstances surrounding this person’s hospitalization? (What happened to cause the
person to be hospitalized?)
Has the team debriefed the incident/occurrences that led to hospitalization as soon as possible
following admission?
What support will be offered to staff based on debriefing?
Based on debriefing, what went well?
Based on debriefing, what can we do differently to support this person in the future?

Disposition Date Completed:
Has the residential provider determined that they can no longer support the person’s needs?
(All attempts should be made to address this within 24 hours of admission)
If the provider does discharge, attempts to locate a new provider should begin immediately
Has a residential living arrangement been identified upon discharge?
Residential contact:____________________________ Phone #/e-mail address
Medical Considerations Date Completed:
Have potential medical causes for behavioral symptoms been ruled out? (75% of people with ID who
present at psychiatric hospitals may actually be experiencing a medical problem):
How can we verify the cause is not medical? Who is responsible for following up with medical testing?
Hospital contact-established with 24 hours of admission Date Completed:
Name of designated person responsible to contact the hospital:
Name of designated hospital contact:
Clinical Information-To be obtained from the hospital during the course of stay
Date Completed:
Current treatment goals and progress:
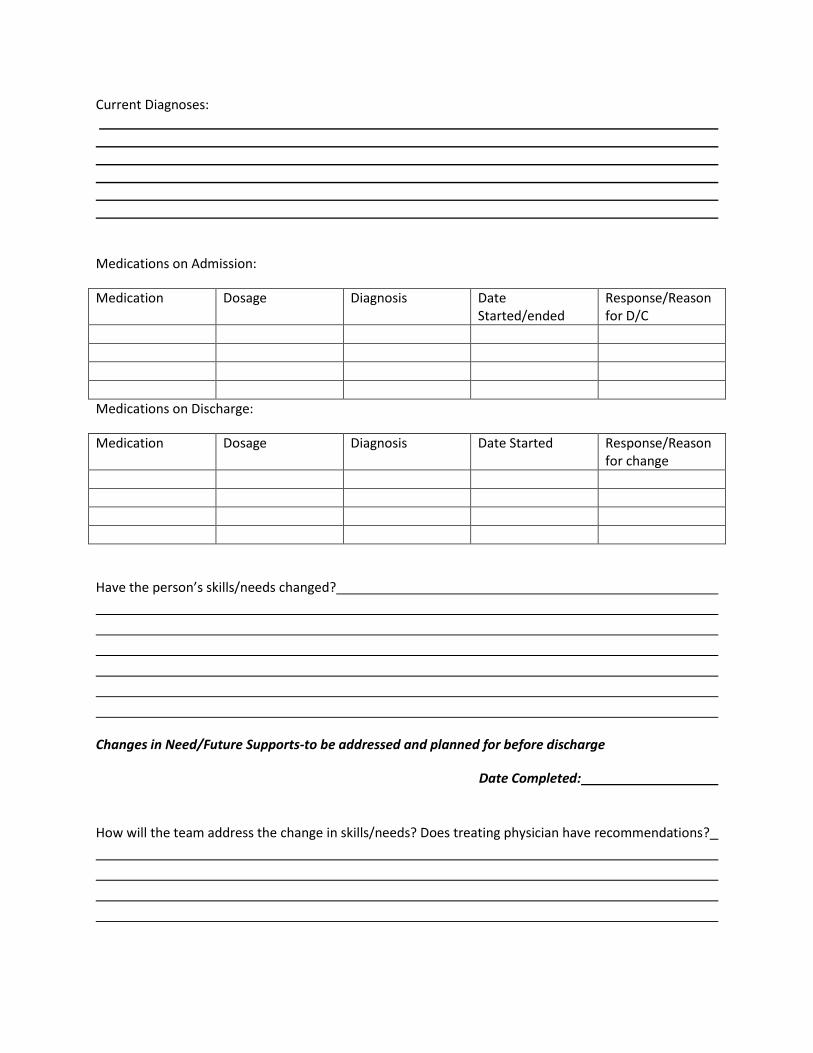
Current Diagnoses:
Medications on Admission:
Medication Dosage Diagnosis Date Started/ended
Response/Reason for D/C
Medications on Discharge:
Medication Dosage Diagnosis Date Started Response/Reason for change
Have the person’s skills/needs changed?
Changes in Need/Future Supports-to be addressed and planned for before discharge
Date Completed:
How will the team address the change in skills/needs? Does treating physician have recommendations?

What seems to be working well in the hospital setting? (i.e. group therapy, structure, behavior planning
etc…)
Can this be translated into the community setting for the person? How, and who will be responsible?
Recommended supports and outpatient services to help the person be successful in the community:
How was the person supported prior to hospitalization?
Does it make sense for the person’s supports to continue as they were prior to hospitalization? Is there
a plan in place to transition the person back to the same level of support?
Are the person’s supports changing? (Is the person moving to a new setting/provider?) How will
transitioning occur and what supports will be put in place to help?
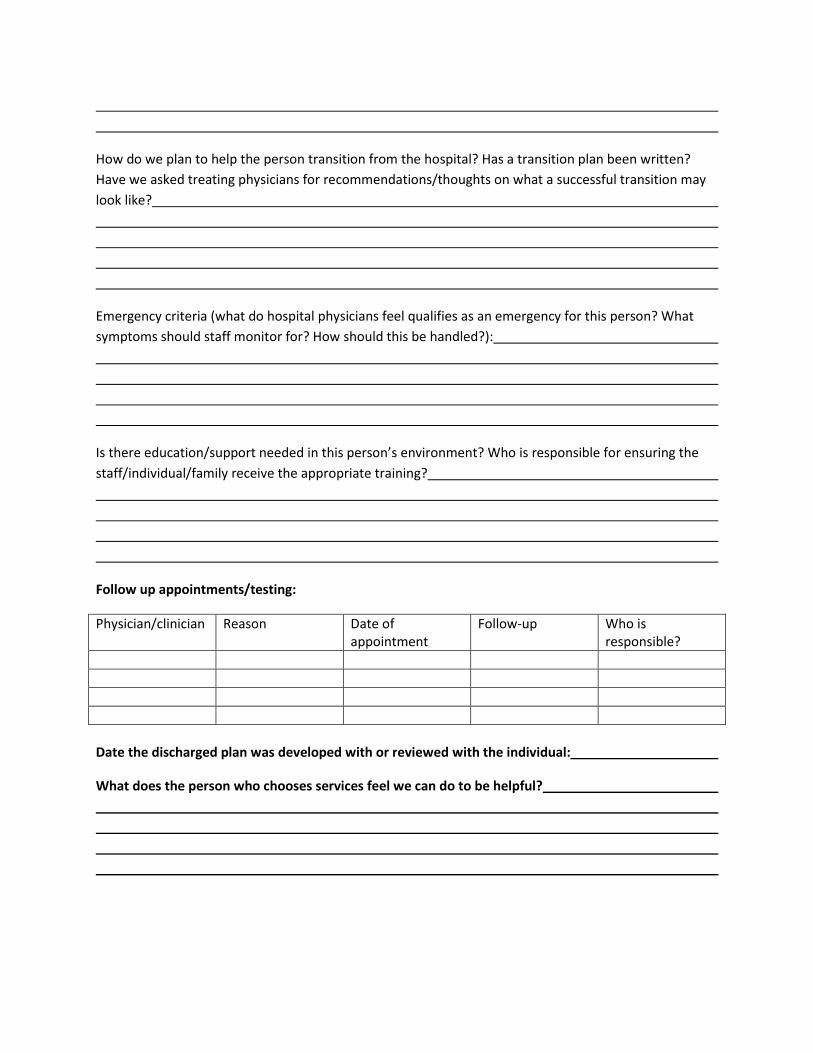
How do we plan to help the person transition from the hospital? Has a transition plan been written?
Have we asked treating physicians for recommendations/thoughts on what a successful transition may
look like?
Emergency criteria (what do hospital physicians feel qualifies as an emergency for this person? What
symptoms should staff monitor for? How should this be handled?):
Is there education/support needed in this person’s environment? Who is responsible for ensuring the
staff/individual/family receive the appropriate training?
Follow up appointments/testing:
Physician/clinician Reason Date of appointment
Follow-up Who is responsible?
Date the discharged plan was developed with or reviewed with the individual:
What does the person who chooses services feel we can do to be helpful?
PA Department of Public Welfare, Office of Developmental Programs
AE Psychiatric Hospitalization Intervention Process Incorporating Best Practices Through Incident Management
Objective: To improve supports to people with Intellectual Disabilities and Mental Illness by ensuring quality supports and appropriate intervention in a community setting to avoid
destabilization and repeated inpatient hospitalization.

Office of Developmental Programs
9/17/13 Page 2
Psychiatric Hospitalization
Psychiatric hospitalizations offer the capability for emergency implementation of life-saving medical and psychiatric interventions. Services are typically provided in a physically secured setting, and admission into this level of care is the result of a serious or dangerous condition requiring rapid stabilization of psychiatric symptoms. This service is generally used when 24-hour medical and nursing supervision are required to provide intensive evaluation, medication titration, symptom stabilization, and intensive brief treatment.
Acute psychiatric hospitalization can be life saving, and there are times when those with an intellectual disability and co-occurring mental health disorder require such hospitalization. The need for such hospitalization tells us that something isn’t working to address the person’s needs or symptoms. Once hospital personnel determine that the person no longer requires an acute level of care, he/she is typically released with recommendations for outpatient treatment and continued support needs. Repeat hospitalizations indicate that the ongoing treatment and support outside of the hospital setting require adjustment.
Responding to Hospitalizations
To most effectively support those who choose ID services and are “dually diagnosed,” it becomes our role to understand what is and isn’t working for the person and to make changes as needed. This also requires work through multi-disciplinary teams and connection to what the person wants in his/her life as well as the supports that service providers, family members, direct support professionals and supports coordinators may need in order to effectively address each person in a holistic way.
The Administrative Entity Role
The AE role in the psychiatric hospitalization and other processes is to ensure the health and welfare of those who choose our services. When needed, according to the AE Operating Agreement, “The AE shall implement immediate corrective action if a Participant’s Health and Welfare is at risk.” Routine review of individual psychiatric hospitalization process and outpatient planning process should be implemented at the AE through the incident management reporting process, and intervention should occur as timely as possible when needed. ODP Regional offices will offer support, follow-up and technical assistance as needed. The following process for review and intervention is the basic expectation of the Office, and is a proactive approach to the Individual At-Risk List Procedure. Each AE may develop a more specific process if necessary.

Office of Developmental Programs
9/17/13 Page 3
Follow-up takes place
Recommendations may be made as part of the Incident Management Reporting Process, OR
Immediate steps for intervention are taken when the IM process has been exhausted or is not
appropriate or timely enough
Additional information is reviewed (To answer questions on next page)
Other psychiatric hospitalizations SC notes, ISP, Behavior plan etc...
Report of psychiatric admissions is pulled from HCSIS
AE Incident Manager pulls report on a regular basis
AE DD Coordinator review and include MH DD Coordinator
Questions/ criteria for review on next page
Office of Developmental Programs
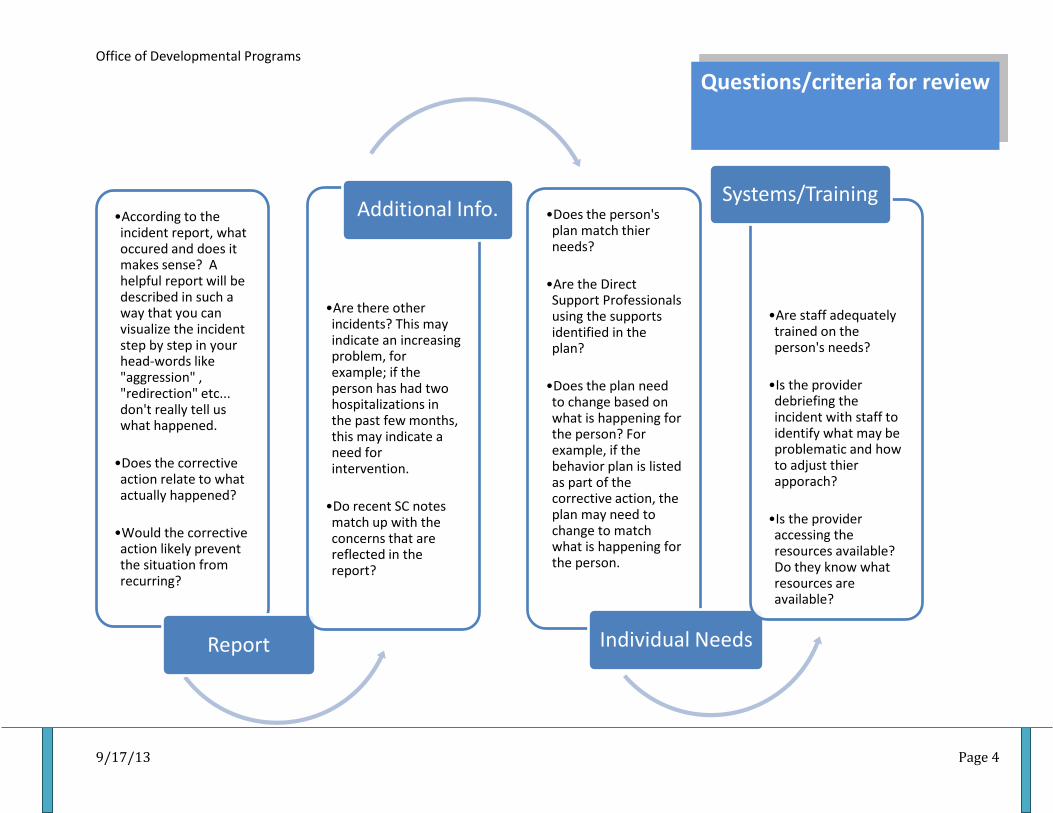
9/17/13 Page 4
•According to the incident report, what occured and does it makes sense? A helpful report will be described in such a way that you can visualize the incident step by step in your head-words like "aggression" , "redirection" etc... don't really tell us what happened.
•Does the corrective action relate to what actually happened?
•Would the corrective action likely prevent the situation from recurring?
Report
•Are there other incidents? This may indicate an increasing problem, for example; if the person has had two hospitalizations in the past few months, this may indicate a need for intervention.
•Do recent SC notes match up with the concerns that are reflected in the report?
Additional Info. •Does the person's plan match thier needs?
•Are the Direct Support Professionals using the supports identified in the plan?
•Does the plan need to change based on what is happening for the person? For example, if the behavior plan is listed as part of the corrective action, the plan may need to change to match what is happening for the person.
Individual Needs
•Are staff adequately trained on the person's needs?
•Is the provider debriefing the incident with staff to identify what may be problematic and how to adjust thier apporach?
•Is the provider accessing the resources available? Do they know what resources are available?
Systems/Training
Questions/criteria for review

Office of Developmental Programs
9/17/13 Page 5
Areas requiring correcton or action should be addressed with the provider/SC, documented and shared with the team
Instruct provider/SC that Psychiatric Discharge Planning should take place at each hospitalization, and changes should be implemented based on that process
Dual Diagnosis Tools Matrix, Risk Screening for Best Practice, HCQU can be referenced. If additional assistance is needed, contact ( Clincial Director)

Office of Developmental Programs
9/17/13 Page 6
Oversight
ODP Regional office will monitor progress through the Incident Management Reporting Process. When concerns arise on individual cases, recommendations will typically be made as part of the Incident Management Reporting Process. In some cases, when it is deemed that immediate action needs to occur, the regional office will contact the AE directly.
Oversight will also take place through the Individual At-Risk List Procedure. All documentation and intervention taken through the Psychiatric Hospitalization Intervention Process will provide documentation necessary as part of the At-Risk procedure.
ODP will offer technical assistance and support as requested. To request technical assistance, contact the Regional Clinical Director.
Improvement and Suggestions
As we partner together in improving the quality of services to those with intellectual disabilities and co-occurring mental illness, suggestions for improvement are welcome. AE staff can contact the Regional office to give feedback on the AE Psychiatric Hospitalization Intervention Process by e-mailing the regional clinical directors.

Consult for Date of Visit: August 4, 2014
Date of Report: August 21, 2014
Purpose of Visit: To review Xxxxxxxxx case, meet with the team and make recommendations for Xxxxxxxxx support and care.
Agency:
On August 4, 2014 I met with Xxxxxxxxx team and later in the day met with Xxxxxxxxx. Xxxxxxxxx has an Autism Spectrum Disorder. He has been currently struggling with physical aggression toward others. He also has pulled his own teeth out as well as his toenails. Xxxxxxxxx can also engage in self injurious behavior, property destruction, and is a possible elopement risk. Due to these safety issues, is interested in reviewing his case to insure Xxxxxxxxx quality of life improves. The outcomes from this visit are as follows:
Medical Components
Xxxxxxxxx struggles with both food and liquid intake. Specifically, Xxxxxxxxx is excessively driven for drink, but will over eat and focus on food frequently. All current and past medical needs have not been identified at this time. There is no etiology in regard to the drive for fluids. Xxxxxxxxx appears to be quiet healthy, however people with Autism Spectrum Disorder may have underlying sensitivities and allergies that are not known. Recommendations in regard to medical concerns are:
1. Request that the Health Care Quality Unit do a complete review of Xxxxxxxxx health records, past and present. It would be very important to gain records from Deveraux that may reveal more about his overall development and health history.
2. Xxxxxxxxx has experienced trauma and it is stated by the team that he was hit by his father (who is now incarcerated) quite frequently. Any blows to the head should be investigated. This is important to Xxxxxxxxx treatment, medications etc. If head trauma exists Xxxxxxxxx may need strategies and accommodations that will help him to better process information.
3. Xxxxxxxxx very much likes to move about. Health Promotion Activity Plans can be incorporated into his day to insure he gets to engage in gross motor movement throughout the day. This will add to Xxxxxxxxx overall health, distracting him from food and drink for periods of time. Xxxxxxxxx has a room downstairs that activities can be explored.
4. Genetic Syndromes are now a very prevalent issue. Considering that Xxxxxxxxx continues to struggle despite a sound behavior support plan, being referred for genetic testing may rule in or out genetic syndromes such as Fragile X. Genetic syndromes carry both medical and behavioral presentations that would guide effective treatment in regard to health and wellness.
5. All recommendations made by the Health Care Quality Unit should also be considered when completed.
6. Information in regard to allergy testing was unknown. It is recommended that allergy testing be completed in order to rule out any behavioral challenges due to such things as allergies to gluten etc.

Consult for Everyday Lives Components
Xxxxxxxxx has only paid supports in his life at this time. It is reported that relationships with women are challenging for him, yet there is a woman named Paula who works very well with him. Paula is being paired with other staff members to help others understand what strategies best work with Xxxxxxxxx.
1. An Essential Lifestyle Plan should be completed for Xxxxxxxxx since so little is known about him. The template for the ELP accompanies this document. If assistance is needed in completing the ELP. ODP can be contacted and Robin VanEerden can facilitate with an agency appointed person to observe and be trained.
2. Xxxxxxxxx team is not certain about his wants and needs or what motivates him. An Adult Positive Reinforcement Assessment can be completed to create a tool box for positive reinforcerment that all support staff would be able to use. This reinforcement listing accompanies this document and can be completed over time and experiences with Xxxxxxxxx.
3. Xxxxxxxxx would benefit from a communication evaluation. While Xxxxxxxxx expressive skills are limited, his receptive skills are not. A communication evaluation can be very helpful in discovering how Xxxxxxxxx can communicate best. Developing a system whether sign, pictures etc. would be helpful in meeting Xxxxxxxxx daily wants and needs.
4. An Occupational Therapy Sensory Integration Evaluation should be completed to understand further Xxxxxxxxx oversensitivities and undersensitivities. All sensory information must be processed and if Xxxxxxxxx may have processing problems, this can cause frustration and stress. An OT trained in Sensory Integration can be very helpful with making recommendations in regard to activities that would help Xxxxxxxxx to have improved processing of information. It is usually standard as a best practice when someone has an Autism Spectrum Disorder that their sensory needs are understood. He also has suffered trauma. The overarousal of the brain that has been caused by traumatic experiences can also be improved by the use of Sensory Integration activities.
5. It may be in Xxxxxxxxx best interest to have a sensory room located in his home, to do recommended activities scheduled throughout the day that are designed to be helpful. This should be made known to the OT so that he/she can make recommendations. Results of the evaluation should include what types of items would best meet Xxxxxxxxx needs within the sensory room.
Trauma Informed Care Components
Xxxxxxxxx has experienced trauma in the form of physical altercations with his father. This type of abuse can promote guarded responses from Xxxxxxxxx. It may be harder for him to trust others and environmental changes over which he is not in control could cause him to become overaroused and trigger dangerous behavior.
1. Xxxxxxxxx may need a “Safe Environment Plan”. This has to do with emotional safety as well as environmental safety. Feelings of abandonment can trigger people who have been abused. Staff moving from room to room without explanation can cause someone to feel unsafe. Many

Consult for
people around can be a trigger for others. Observations over time will assist in formulation this plan. It will include noticing when and where Xxxxxxxxx is at his best and when he may be feeling unsafe (i.e. new staff, unpredictable situations, changes in routine). A sample of a safety plan will accompany this document.
2. While Xxxxxxxxx has limited speech. He may benefit from the softer therapies such as art and music. These therapies assist people in processing their moments of distress and make overall improvements with people who have experienced grief and loss, abandonment, and abuse.
Psychiatric Components
1. People who support Xxxxxxxxx should be very familiar with his psychiatric symptom presentation. Anxiety is his working diagnosis as well as Intermittent Explosive Disorder which may have a mood component. Training may be needed on a way to track Xxxxxxxxx moods and distinguish any mood changes that may be significant and/or be indicative of a cyclical mood disorder. These types of tools are available from the Clinical Director at ODP. It is not convincing that the team thoroughly understands Xxxxxxxxx psychiatric issues. This would indicate training is needed in this area to insure Xxxxxxxxx psychiatric treatment results in positive progress and improved quality of life.
2. A full review of past and current medications is indicated at this time. Xxxxxxxxx continues to have struggles in his home and community. Psychiatric medications must be monitored closely to document any improvements or non-improvement in presentation. Some tools will accompany this document for review by the team.
3. Reporting symptoms accurately to the psychiatrist is paramount to Xxxxxxxxx care. Reporting behavioral presentations only would not be helpful to Xxxxxxxxx psychiatric stabilization.
4. A pharmacological review can be requested through the Positive Practices Resource Team if desired. The lead for that would be Marlinda Smith, Dual Diagnosis lead. She can be reached at
Behavioral Support Components
1. Xxxxxxxxx enjoys having a very well written behavior support plan and has behavioral supports in place.
2. Considering Xxxxxxxxx has an Autism Spectrum Disorder, he may benefit from scripted social stories that will make his environment additionally predictable. Social stories were created by Carol Gray for children with Autism. The books written on the subject are very adaptable to adults. “Revealing the Hidden Social Code” is an excellent guide that assists in correctly and effectively structuring social stories for many different occurrences and events. It is available on www.amazon.com. Structure, predictability and understanding will be very beneficial to Xxxxxxxxx. Social stories can provide this in his environment.
3. The behavior support plan must be implemented consistently across all staff. Xxxxxxxxx will be able to respond more predictably when those who interact with him follow a consistent framework.
4. Crisis plans should be written, fully understood and in a place to be accessed quickly if the need arises.

Consult for Areas of Training Suggested
Once the areas of need are agreed upon and evaluations are completed. Training may be needed. Suggested trainings in relation to these recommendations are:
1. Autism Spectrum Disorder, Anxiety and how Trauma affects the brain. 2. Medical needs that would be pertinent from the results of evaluations 3. Sensory Integration what it is and how it can be helpful 4. Identifying, tracking symptoms of mental illness/mood disorders 5. Emotional Safety Plans 6. Trauma Informed Care 7. Essential Lifestyle Planning
Trainings are available through the Health Care Quality Unit as well as the Clinical Director at ODP.
Thank you for the opportunity to meet and interview Xxxxxxxxx and the team. If there are any questions or additional needs, please do not hesitate to contact me at. A follow-up should be conducted by the agency with the Clinical Director within three months.
Respectfully submitted,
Robin VanEerden, MS, NCC, LPC, NADD-CC
Clinical Director

1
Risk Screening for Best Practice People with intellectual disabilities (ID) may have physical and mental health (MH) diagnoses. In order to support wellness and recovery, a check list was developed with items comprising the most important components of effective supports for people with dual diagnosis (ID and MH). If effective supports are put in place, as reflected by the items on this checklist, risk can be minimized and people’s lives can be enhanced. The items below are broken down into component categories, in order to identify and organize possible need for additional support. Not all items will apply to every person. The topics measured by these items represent a compilation from the document “Redefining Commitment in Pennsylvania, “and the Positive Approaches/Everyday Lives/Recovery/Positive Behavioral Supports philosophies. It is also used to support the Psychiatric Hospital Discharge Planning process. For additional information, training and/or technical assistance with any of the items on this checklist, please contact Robin VanEerden at [email protected] Directions: Please place a check in the appropriate column for each item: Yes, No, or N/A (not applicable). Any additional explanation can be listed in Comments column. If an item is not applicable, please indicate the reason in the Comments column. If there are any items for which you require clarification or resources, please utilize the Glossary attached to this tool. Again, if any of the items are not addressed, this should indicate a place to start to increase the supports for wellness and recovery for the person, and increase the knowledge and skills of the entire team. Name of Person: ____________________________________ Date:___________________________ Name and Title of Person Completing:___________________________________________________ Medical Components
Components Yes No N/A Comments All current and past medical needs identified
All current and past medical needs documented
All current and past medical needs addressed
Current neurological status has been evaluated and the record updated
Environment assessed to address needed physical adaptations
Lifetime Medical History completed and current
Health Promotion Activity Plans utilized
2
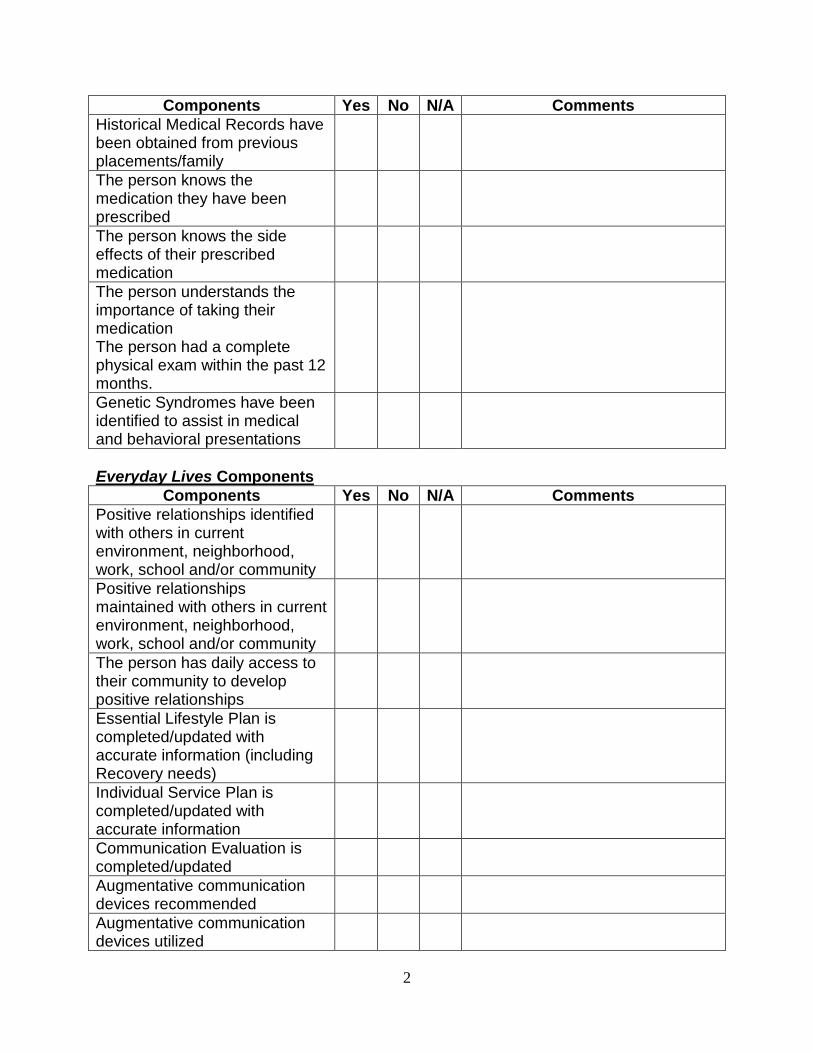
Components Yes No N/A Comments Historical Medical Records have been obtained from previous placements/family
The person knows the medication they have been prescribed
The person knows the side effects of their prescribed medication
The person understands the importance of taking their medication The person had a complete physical exam within the past 12 months.
Genetic Syndromes have been identified to assist in medical and behavioral presentations
Everyday Lives Components
Components Yes No N/A Comments Positive relationships identified with others in current environment, neighborhood, work, school and/or community
Positive relationships maintained with others in current environment, neighborhood, work, school and/or community
The person has daily access to their community to develop positive relationships
Essential Lifestyle Plan is completed/updated with accurate information (including Recovery needs)
Individual Service Plan is completed/updated with accurate information
Communication Evaluation is completed/updated
Augmentative communication devices recommended
Augmentative communication devices utilized

3
Augmentative communication devices in good repair/condition
Biographical Timeline completed/updated
Person’s sexuality is identified and supported
Transition plan for change of caregiver/change in provider completed
Transition plan for change of living arrangement, work or school completed
Sensory profile developed Sensory issues identified Sensory issues addressed Autism Spectrum Disorder (ASD) Components
Components Yes No N/A Comments Autism Spectrum Disorder is diagnosis is in the record
Supporters recognize indicators of ASD (ex: communication problems; social interaction problems; sensory sensitivities; repetitive/ritualistic behavior)
Communication/Speech evaluation completed
Alternative communication strategies have been identified
Alternative communication strategies have been implemented
Sensory evaluation (Occupational Therapy) has been completed
Environmental adaptations for sensory issues have been identified
Environmental adaptations have been implemented
The person’s routines, rituals, schedules and preferences are recognized and respected
Person’s interests, passions, preferred activities are

4
Components Yes No N/A Comments recognized and supported (if appropriate) Trauma-Informed Care Components
Components Yes No N/A Comments Trauma history, either ongoing or resolved, is documented
Person has been referred for clinical treatment of trauma
Person currently receives clinical treatment for trauma
A trauma-informed safe environment plan has been considered and implemented
A trauma-informed safety plan has been considered and implemented
People supporting the person demonstrate understanding regarding a person’s history of trauma and how it impacts the person’s thoughts and feelings
Grief and losses have been identified and person has been given appropriate support
Person has been offered assistance to help locate resources and supports regarding trauma
Person has been given education on what abuse and neglect is and how to report it, by an appropriate and trained clinician
Psychiatric Components
Components Yes No N/A Comments The person acknowledges that they have a need for behavioral health treatment.
The person receives education regarding their mental illness
The person knows the psychotropic medication they

5
Components Yes No N/A Comments have been prescribed The person knows the side effects of the psychotropic medication they have been prescribed
The person understands the importance of their prescribed psychotropic medications
Clinical Assessment/Comprehensive Review/Intake for MH services completed or updated
Psychiatric evaluation completed or updated
Target symptoms that support the identified diagnosis have been provided by the psychiatrist at the time of psychiatric evaluation
Target symptoms related to the diagnosed mental illness are included in all documentation including the Behavior Support Plan, ISP, Lifetime Medical History, Psychiatric Evaluation and Team Review of Psychotropic Medications
Target symptoms related to the individual’s risk of relapse, including agitation, mood cycles, are being tracked (This does not include data tracked for a behavior support plan).
Social/emotional/Behavior Plan as required by regs for individuals taking psychotropic medications has been completed and/or updated
Substance abuse/dependence history is documented and supports are provided
Person has been referred for out- patient community based treatment services including Psy Rehab, Certified Peer Support,

6
Components Yes No N/A Comments individual/group therapy, Assertive Community Treatment (ACT) or other services. Person receives community based treatment services.
Person has available access to mental health professionals
Clinical supervision for direct support professionals (or staff?) is in place
Alternative therapeutic treatment modalities considered in addition to more traditional talk therapy.
Other or List the therapeutic treatment modalities currently being utilized
Behavioral Support Components
Components Yes No N/A Comments Functional Behavior Assessment (FBA) or other standardize tools appropriate for the behaviors presented is completed
Behavior Support Plan completed based upon the results of a formal assessment as well as through the identification of strengths and skills that can be utilized by the person to reduce or replace challenging behavior(s)
Replacement behaviors are identified and described in the Behavior Support Plan
Behavior Support Plan incorporates the tools and philosophy of Everyday Lives, Mental Health Recovery and Positive Behavioral Supports
Staff and/or family have been trained on the implementation of the Behavior Support Plan
Behavior Support Plan is implemented correctly and

7
Components Yes No N/A Comments consistently by all team members and supporters Alternatives to restrictive procedures have been considered and implemented prior to the use of restrictive procedures
Restrictive procedures are voluntary, appropriate and approved
No more than 3 Target Behaviors listed on the Behavior Support Plan are being tracked at the same time
Data on target behaviors is being tracked correctly
The team understands that challenging behaviors might not be associated to the person’s mental illness
The person’s Behavior Support Plan includes a Crisis Plan
Crisis Support Components
Components Yes No N/A Comments Crisis plan completed by the person with support from team members
Crisis prevention techniques completed by the person with support from team members
De-escalation techniques completed by the person with support from team members
Debriefing processes identified and completed for person and support persons
Conflict management and resolution process is in place for person and support persons
The person and their staff recognize crisis triggers (ex: anniversary dates, holidays, staff changes etc.) Situational issues that provoke

8
Components Yes No N/A Comments anxiety or stress are identified and options are provided. The person and their staff recognizes crisis warning signs (ex: pacing, cursing, becoming quiet)
The person recognizes and asks for the things they need to calm down/de-escalate (ex: to call a friend or family member; to be spoken to in soft tones; to take a break from work/activity) Staff or family members ensure that the person has access to the items or process in order to de-escalate.
Partner with local crisis teams and law enforcement in regard to safety and crisis management
Mental Health Wellness and Recovery Components
Components Yes No N/A Comments Person has been given information on Wellness Recovery Action Plans®
Person has a Wellness Recovery Action Plan® that they and their staff have developed
Personal Medicine Tools™ identified by the person
Recovery Wheel used to measure progress and identify where progress is needed by the person and support people/agency
Referral to recovery oriented services such as certified peer specialist, psy rehab services, ACT etc. as well as natural supports such as spiritual groups, family etc. has been made
Recovery oriented supports and services currently being utilized by the person

9
Sexual Offending or Problematic Sexual Behavior Components
Components Yes No N/A Comments History of sexual offending and/or problematic sexual behavior is documented
Person receives clinical treatment for sexual offending and/or problematic sexual behavior
Support persons have received Safer Options training
Team communicates pertinent information to the person’s probation/parole officer and the courts as requested
Risk Assessment for Sexual Offending completed and recommendations have been followed
Safety/Supervision Plans and protocols established for person with Sexual Offending and/or Problematic Sexual Behavior
Medical reasons as the cause of Problematic Sexual Behavior have been considered (ex: hypersexuality due to side effect of medication(s)
If sexual offending or problematic sexual behavior is related to a history of sexual trauma, the environment and supports are trauma-informed (see above)
Fetal Alcohol Spectrum Disorder Components
Components Yes No N/A Comments FAS or other condition on the FASD spectrum diagnosed and/or documented; or if the person’s presentation is such that and FASD is suspected so that further diagnostic activities can be completed by a qualified clinician. (i.e. physical features

10
Components Yes No N/A Comments present, memory problems, lack of understanding of cause and effect or consequences, emotional dysregulation, impulsivity, does not learn from mistakes, person is not responding to consistently implemented behavioral supports) Has prenatal alcohol exposure been fully investigated and documented
Person receives clinical treatment that is FASD informed such as music/art therapy, (therapies that use language only have proven to be ineffective due to deficits in receptive language skills)
Support persons have received Fetal Alcohol Spectrum Disorder training by an FASD clinically informed person that includes a review of general support strategies that are helpful to people with FAS/D. (i.e. the use of visuals in the environment)
Baseline MRI is completed to rule out any undiagnosed traumatic brain injury, tissue damage or structural physical issues. MRI w/ and without contrast To assess for Fetal Alcohol Changes in the Basal ganglion, cerebellum and corpus callosum
Neuropsychological testing to understand the functions of the brain and the domain which have been affected. (this can be helpful in specifically identifying methods and modalities of strategies and treatment that will be effective for the person)
Occupational Therapy/Sensory Integration Evaluation has been
11
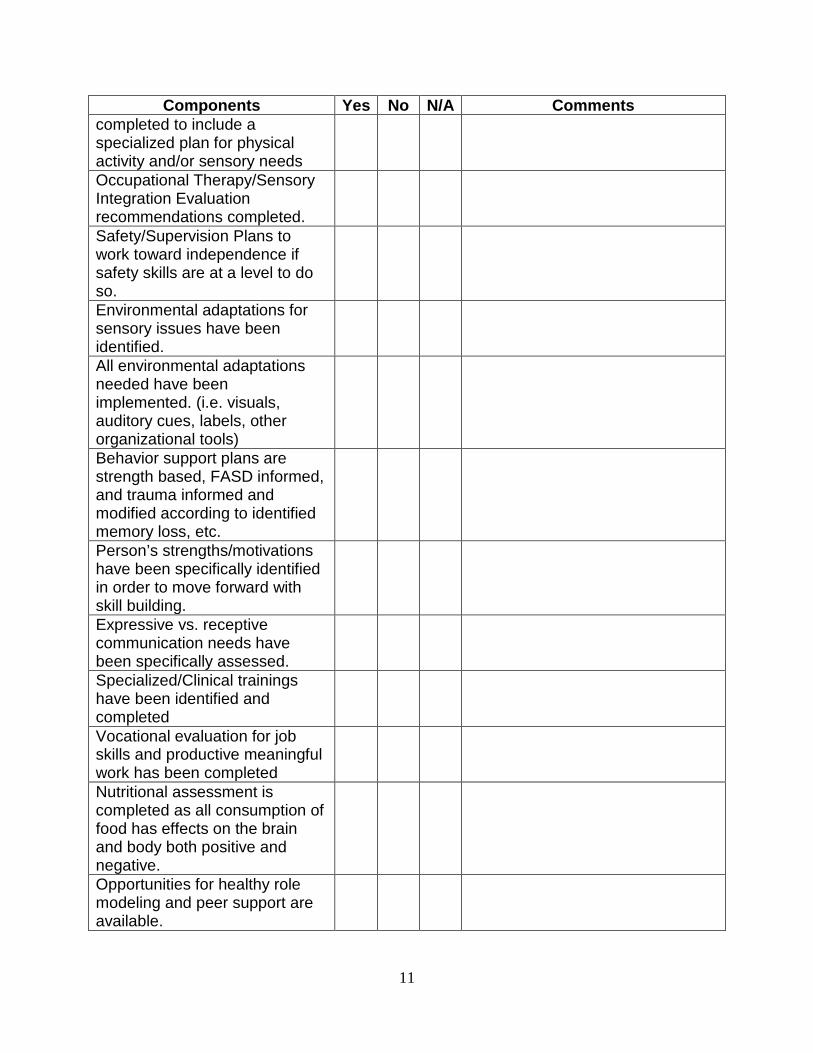
Components Yes No N/A Comments completed to include a specialized plan for physical activity and/or sensory needs Occupational Therapy/Sensory Integration Evaluation recommendations completed.
Safety/Supervision Plans to work toward independence if safety skills are at a level to do so.
Environmental adaptations for sensory issues have been identified.
All environmental adaptations needed have been implemented. (i.e. visuals, auditory cues, labels, other organizational tools)
Behavior support plans are strength based, FASD informed, and trauma informed and modified according to identified memory loss, etc.
Person’s strengths/motivations have been specifically identified in order to move forward with skill building.
Expressive vs. receptive communication needs have been specifically assessed.
Specialized/Clinical trainings have been identified and completed
Vocational evaluation for job skills and productive meaningful work has been completed
Nutritional assessment is completed as all consumption of food has effects on the brain and body both positive and negative.
Opportunities for healthy role modeling and peer support are available.

12
Trainings Needed
Training Completed Not Completed
N/A Comments
Intellectual/Developmental Disability and Psychiatric Disorders
Overview of Syndromes Psychotropic Medications Understanding Trauma-Informed Care and Stressful Life Events
Functional Behavior Assessment and Behavior Support Planning
Autism Spectrum Disorders Person Centered Planning/Positive Approaches
Safer Options for Problematic and Sexual Offending Behavior
Communicating with the Psychiatrist
Person specific training(s) Please list trainings needed
How to communicate effectively across systems
Crisis Supports and Debriefing
Mental Health Wellness Recovery and Everyday Lives
Fetal Alcohol Spectrum Disorder
Overview of Sensory Integration

13
Outcome Actions Desired Outcome:
Discussion/ Justification:
What needs to be done Who’s responsible
By when
Review of Desired Outcome: Date: Comments

14
Glossary
Augmentative Communication Devices: Devices that aid the user in communicating may include portable speech output devices as well as those that connect directly to a computer or telephone.
Behavior Support Plan – A plan that is developed from the functional behavior assessment and from various other sources that addresses methods and interventions that are proactive and positive in nature. These interventions are identified to address the social, emotional and environmental issues that may be triggering behavioral challenges. More information on Behavior Support Plans can be located at
Biographical Timeline - The biographical timeline process is sometimes called "biography," "timeline," or "life line." It is a facilitated process through which a team of people, having researched the events, passages, and interventions in a person's life, lay out those facts in a linear fashion, to enable a group to correlate information in a meaningful manner. Events and personal experiences (often thought of as "insignificant" in other contexts) that were previously stored in compartmentalized reports and files are grouped according to their occurrence along a linear life-timeline. To find out more about biographical timelines go to http://www.nasddds.org/resource-library.
Certified Peer Specialist - A certified peer specialist is an individual who is a self-identified current or former consumer of behavioral health services and who is trained to offer support to others. Certified Peer Specialists have completed training and passed a certifying test to demonstrate competency to assist others with their recovery and with the community integration process.
Conflict management – involves implementing strategies to limit the negative aspects of conflict and to increase the positive aspects of conflict at a level equal to or higher than where the conflict is taking place. Furthermore, the aim of conflict management is to enhance learning and group outcomes (effectiveness or performance in organizational setting) It is not concerned with eliminating all conflict or avoiding conflict. Conflict can be valuable to groups and organizations. It has been shown to increase group outcomes when managed properly.
Crisis Plan – A crisis plan is a plan that includes an action plan for caregivers and supporters to follow in the case the person becomes harmful to themselves or others. Crisis plans can also include suicide protocols or any other specific behavioral presentation that would be harmful to the person or others around them.
Cross Systems Communication – Communication needs to be effective and accurate between different systems (i.e. mental health, education, county, state) to assure that the needs of the person are met.
Debriefing – a process that occurs after an escalated situation has been resolved. Debriefing sessions should have a specific agenda and should be done with both caregivers/supporters and the person. This

15
can happen together or separately, but should be done so that relationships can be repaired and protocols and interventions are reviewed for safety and efficacy.
De-escalation Techniques – these techniques are very specific to the person and can be written clearly in a behavior support plan, a WRAP, or Individual Service Plan. These techniques are developed by the person and the person’s team to assist in calming a person when the person is having difficulty regulating their emotions. De-escalation techniques are proactive and vital to avoid crisis situations.
Essential Lifestyle Plan - Essential lifestyle planning is a guided process for learning how someone wants to live and for developing a plan to help make it happen. It’s also: a snapshot of how someone wants to live today, serving as a blueprint for how to support someone tomorrow; a way of organizing and communicating what is important to an individual in “user friendly”, plain language; a flexible process that can be used in combination with other person centered planning techniques; and, a way of making sure that the person is heard, regardless of the severity of his or her disability. Essential lifestyle plans are developed through a process of asking and listening. The best essential lifestyle plans reflect the balances between competing desires, needs, choice and safety.
Everyday Lives- Everyday Lives is the core philosophy and framework of the State of Pennsylvania’s Office of Developmental Programs (ODP). Originally introduced in 1991, Everyday Lives is deeply rooted in the concept of Self-Determination and Positive Approaches.
Development included the active participation of individuals and family members. Their focus was to identify what people with disabilities and families said was important to them and what kind of supports they needed.
The concept of Everyday Lives is not about disability – it applies to everyone – with or without a disability
The fundamental concept of Everyday Lives is that, with the support of family and friends, individuals with disabilities decide how to live their lives and what supports they need. It also means that they are responsible for their decisions and actions.
ODP considers and ensures that the impact of every decision, rule or regulation of its staff or those working on its behalf, continues to support and promote the ideals of Everyday Lives.
Each of the principles are assumed for most people as they go about their everyday life, but may not be recognized or assumed for the individuals who we support. Our role is to help assure the presence of these life experiences and support the individual as needed so that they can benefit and learn from these experiences.
“Our goal should be clear. We are seeking nothing less than a life surrounded by the richness and diversity of community. A collective life. An Everyday Life. A powerful life that gains joy from the creativity and connectedness that comes when we join in association as citizens and create an inclusive world.” - John McKnight

16
Functional Behavior Assessment - A Functional Behavioral Assessment (FBA) is an attempt to look beyond the obvious interpretation of behavior as "bad" and determine what function it may be serving for a person. Truly understanding why a person behaves the way he or she does is the first and best step to developing strategies to reduce or replace the behavior. The process usually involves documenting the antecedent (what comes before the behavior), behavior, and consequence (what happens after the behavior) over a number of weeks; interviewing teachers, parents, caregivers and others who work with the person; evaluating how the person's disability may affect behavior; and manipulating the environment to see if a way can be found to avoid the behavior. This is usually done by a behavioral specialist, and then becomes the basis for a behavior support plan.
Genetic Syndrome - A syndrome is a disease or disorder that has more than one identifying feature or symptom. Each particular genetic syndrome will have many typical features, depending on which aspects of development are affected by the abnormal gene chromosomes. A genotype and phenotype accompany syndromes which can shed light on medical and behavioral issues that are commonly present in the specified genetic syndrome.
Health Promotion Activity Plans - This plan serves many purposes including: easy reference for the individual diagnosed with ID/DD and any individuals providing support; provides information that can be incorporated into any annual planning documents; can be used as a training resource; and fosters optimum care for health conditions. The plan includes a definition of the diagnosis, signs and symptoms of the condition, specific signs and symptoms that the individual experiences, interventions needed, identification of health care professional responsible for monitoring condition, and frequency of follow-up. The plan can be constructed by anyone but should be reviewed by a health care professional for completeness and accuracy. http://www.pchc.org/HPAPs/HPAPs.aspx
Neurological Status- the extent to which the peripheral and central nervous systems receive, process, and respond to internal and external stimuli. This can be determined with a neurological assessment. Information regarding neurological assessment can be located at http://lane.stanford.edu/portals/cvicu/HCP_Neuro_Tab_4/Neuro_Assessment.pdf
Neuropsychology -The branch of psychology that deals with the relationship between the nervous system, especially the brain, and cerebral or mental functions such as language, memory, and perception.
Neuropsychological Status- The status of the person is needed to understand further how the person learns and retains knowledge. This includes working, short-term, long-term and procedural memory functions. If there are deficits in brain function, expectations for the person may be set too high. This, in turn, may frustrate the person, leading to challenging behaviors. How someone learns can help us

17
understand how they problem solve and make decisions. This status can be determined by a neuropsychologist and appropriate interventions can then be determined to assist the person with skill building activities.
Peer Support Services- are based on the fundamental principles of recovery and are therapeutic interactions conducted by individuals who are trained and certified to offer support and assistance in helping others in their path to wellness. Peer support services are designed to engage the consumer in choice and support the active involvement of the person in their own recovery process.
Personal Medicine® – was created by Pat Deegan and is something that a person does and has nothing to do with what the person “takes”. Pat defines Personal Medicine as "the things that give life meaning and make life worth living." Personal medicine must include an active ingredient. For example: the active ingredient of “taking a walk” is that it reduces stress and helps the person to feel better. Personal medicine forms are available on the internet and also on managed care websites. Resources are available at www.patdeegan.com
Problematic Sexual Behavior – sexual behavior that may or may not be illegal. It refers to sexual behavior that interferes with activities of daily living to the extent a person cannot interact with others in accordance with expected social norms or occurs with another person who has not consented to the sexual behavior. Sexual behavior is problematic if it interferes with the rights of others.
Recovery Principles - Recovery is a process by which a person overcomes the challenges presented by a mental illness to live a life that is meaningful to them and has purpose. Recovery is a deeply personal, individualized process of changing one’s attitudes, values, feelings, goals, skills and/or roles in order to live a satisfying, hopeful and contributing life even with limitations caused by mental illness. Ultimately, because recovery is a personal and unique process, everyone with a psychiatric illness develops his or her own definition of recovery. However, certain concepts or factors are common to recovery. Some of these are listed below.
Recovery Wheel – A Recovery Model for People with Mental Illness and Co-Occurring Disorders
Description of the Revised CSP Wheel

18
For over 20 years, the national Community Support Program (CSP) Principles have had a dramatic impact on the way systems planners conceptualize organizing services, supports and opportunities to help mental health consumers reach their full potential in our society.
The Wheel is designed to meet the needs of people with mental illness as well as those who suffer from co-occurring disorders (e.g., mental illness and substance use disorders). The central focus of community support programs is to facilitate the recovery process and personal growth of each mental health consumer.
CSP Principles remain unchanged and are portrayed in the Wheel's middle circle to support the recovery process and provide the bedrock for the way service system components are delivered. Essential community support system components include meaningful work, community mobility, psychiatric rehabilitation, leisure, recreation and education.
While the revised CSP Wheel still prioritizes mental health consumers who have the most serious psychiatric illnesses, it is acknowledged that the model is beneficial to: a) many other consumers whose psychiatric disorders continue to disrupt their lives, b) consumers who have sufficiently progressed in their recovery to the point where their psychiatric conditions can no longer be deemed serious. Non-public systems are encouraged to adopt the Model.
Description of the Revised CSP Wheel
People can and do recover from mental illness. The center circle of the Pennsylvania revised CSP Wheel portrays recovery as a multi-dimensional concept. Hope is the anchor point upon which recovery is based. Demonstrating respect for the consumer supports his or her hopefulness and nurtures the person's self-esteem. When people convey trust in the consumer, it strengthens the consumer's confidence and motivation to assume increased responsibility for taking control of one's own life. The eight factors listed on the Wheel are important antecedents for Recovery:
• Hope • Competence • Respect • Trust • Understanding • Wellness • Choice • Spirituality
Components of a Community Support System
The Recovery model incorporates the following components of a Community Support Program. These components are essential resources in recovery:
• Treatment and support • Family and friends • Peer support • Meaningful work • Income support • Community mobility • Community groups and organizations • Protection and advocacy
19
• Psychiatric rehabilitation • Leisure and recreation • Education • Housing • Health care
Replacement Behaviors- Behavioral interventions outlined in a Behavior Support Plan designed to teach the person presenting with challenging behavior a more appropriate, pro-social, and convenient way to have whatever needs or desires met without engaging in the identified challenging behavior.
Restrictive Procedures - A restrictive procedure is a practice that limits an individual’s movement, activity of function; interferes with an individual’s ability to acquire positive reinforcement; results in the loss of objects or activities that an individual values; or requires an individual to engage in a behavior that the individual would not engage in given freedom of choice.
Safe Environment Plan (trauma informed) – A safe environment plan is a plan that identifies triggers and establishes the person’s emotional needs within their environment. For example: If a person has been abandoned or has experienced loss and perceives shift changes as abandonment, a “safe” protocol should be written to consistently assist a person in feeling secure when separating from care givers.
Safer Options Manual – the manual that governs best practices in Pennsylvania in regards to people who have an intellectual disability who also have problematic or sex offending behavior. http://www.paproviders.org/Pages/MR_Archive/Safer_Options_2010.pdf
Safety Plan for Problematic Sexual Behavior – this safety plan is a therapeutic tool that requires a person with problematic sexual behavior or sex offending behavior that has deviant sexual thinking (thinking and behavior that is against the law and non-consensual) to examine where they are going, what they will be doing and who they will be with among other safety issues. This assists a person to identify and understand the risk in the environment that they will be entering. This in turn assists a safe plan to be formulated both for the person as well as the community. This tool can be found in the Safer Options Manual.
Sensory Profile – a sensory profile evaluates and assesses how a person processes sensory information. This profile is compiled by an Occupational Therapist that has been certified in sensory integration. The profile addresses over-sensitivities and under-sensitivities in the six sensory systems; proprioceptive (the awareness of posture, movement, and changes in equilibrium and the knowledge of position, weight, and resistance of objects as they relate to the body), tactile, olfactory, auditory, visual, and taste. This profile is important as processing and systems that are affected can cause people to act out and experience challenging behavior that is misunderstood.
Sexuality - the characteristic of the male and female reproductive elements as well as the constitution of a person in relation to sexual attitudes and behavior.
Supervision Plan – this plan is in accordance with Safer Options Best Practice. A written plan for supervision is formulated for people with problematic sexual or sex offending behavior to identify what levels of supervision are needed across all environments. Each environment should be examined for assessing and managing risk to the person and the community and supervision should be established accordingly. A sample of a supervision plan can be found in the Safer Options Manual.
Target Symptoms of Mental Illness – Target symptoms of Mental Illness are provided by the psychiatrist. They consist of the person’s specific presentation of psychiatric symptoms which are in

20
consistent with the person’s psychiatric diagnosis. These symptoms are found in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. These symptoms, along with special considerations for people with an Intellectual/Developmental Disability, can be found in the Diagnostic Manual-Intellectual Disability (DM-ID). More information can be located at www.apa.org and www.thenadd.org
Team Review Form of Psychotropic Medications- this tool assists with tracking of mental health symptoms on a day to day basis. This can assist caregivers and the person to visually see if mental health symptoms are increasing, decreasing or staying the same. It also assists people with mental health presentations that are cyclical in nature such as various mood disorders.
Therapeutic Treatment Modalities – any therapeutic method that is empirically studied or has been established as best practice in treatment of emotional needs of people with mental illness and an intellectual disability. Some examples are: Art therapy, Music Therapy, Behavioral Therapy and Cognitive-Behavioral Therapy.
Transition Plan – transition plans are formulated any time a person is admitted or discharged from their current placement. The plan is created to assist the person in tolerating the change as positively as possible and should include all aspects of the person’s life and how the changes will occur to. Transition plans can also be incorporated into behavior support plans for people who have difficulty with day to day changes (i.e. changes in schedules or staffing).
Trauma –an event or situation which causes great distress and disruption. Other definitions include: a serious injury or shock to the body, as from violence or an accident; an emotional wound or shock that creates substantial, lasting damage to the psychological development of a person, often leading to neurosis. Examples of trauma are: physical, sexual, psychological and emotional abuse, neglect, witnessing a traumatic incident such as a death, an accident or a murder.
WRAP® stands for Wellness Recovery Action Plan®- WRAP® is a self-management and recovery plan developed by a group of people who experienced mental health challenges. These people learned that they can identify what makes them well and then use their own Wellness Tools to relieve difficult feelings and maintain wellness. WRAP is designed to:
• Decrease and prevent intrusive or troubling feelings and behaviors • Increase personal empowerment • Improve quality of life • Assist in achieving your own life goals and dreams
WRAP consists of tools to monitor uncomfortable/distressing feelings and behaviors and through planned responses, reduces, modifies or eliminates them. It also includes plans for responses from others when the individual cannot make decisions, take care of themselves or keep themselves safe. WRAP is trademarked by Mary Ellen Copeland, PhD, an internationally acclaimed author, educator and mental health advocate. More information can be found at www.mentalhealthrecovery.com/wrap

Notes

Notes

Notes
Notes


















