SALIVARY GLANDS - med.alexu.edu.eg
18
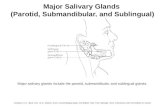
1 SALIVARY GLANDS I. PAROTID GLAND Surgical Anatomy: • It is a wedge-shaped, well-encapsulated gland on the lateral side of the face, that secretes serous secretion. • It has 2 lobes; superficial & deep, connected by an isthmus. The deep lobe (segment) is lodged between the mastoid process posteriorly, the external auditory meatus superiorly, and the ramus of the mandible anteriorly. Medially, it reaches the styloid process. Anteriorly, the parotid gland overlaps the masseter muscle, while posteriorly, it overlaps the sternomastoid muscle. • Parotid Duct (Stenson’s Duct): It runs over the masseter, pierces the buccal pad of fat & opens in the vestibule of the mouth behind the upper 2 nd molar tooth. • Structures Within the Parotid Gland: 1. ECA (it gives the posterior auricular artery just before entering the gland), with its 2 terminal branches; superficial temporal & maxillary artery. 2. Retro-mandibular Vein (Posterior facial vein with its tributaries). 3. Facial Nerve: It enters the deep surface of the gland close to the stylomastoid foramen & gives 5 branches inside the gland radiating forwards superficial to the vein & artery. 4. Parotid Lymph Nodes. • Surface Anatomy of the Parotid Gland: Upper Border: From the tragus to the mastoid process. Anterior Border: From the tragus to the posterior border of the masseter opposite the angle of the mouth. Inferior Border: From the anterior border to below & behind the angle of the mandible. Posterior Border: From the mastoid process to the inferior border. • Surface Anatomy of the Parotid Duct: The parotid ducts corresponds to the middle 1/3 of an imaginary line from the tragus of the ear to the midportion of the upper lip. • Facial nerve anatomy o Resection of the parotid tumors may be followed by recurrence due to fear of injury to the facial nerve. o The facial nerve arises from the stylomastoid foramen midway between the bases of the mastoid and styloid processes, about 1.5 cm deep from the external surface of the mastoid process, the nerve is about 1 cm in length outside the gland then pierces the gland and runs through for another 1 cm, where it divides into 2 branches which then give 5 branches: • Temprofacial: • Temporal. • Zygomatic • Buccal • Cervicofacial: • Mandibular
Transcript of SALIVARY GLANDS - med.alexu.edu.eg

1
SALIVARY GLANDS
I. PAROTID GLAND
Surgical Anatomy:
• It is a wedge-shaped, well-encapsulated gland on the lateral side of the face, that
secretes serous secretion.
• It has 2 lobes; superficial & deep, connected by an isthmus. The deep lobe
(segment) is lodged between the mastoid process posteriorly, the external
auditory meatus superiorly, and the ramus of the mandible anteriorly. Medially,
it reaches the styloid process. Anteriorly, the parotid gland overlaps the masseter
muscle, while posteriorly, it overlaps the sternomastoid muscle.
• Parotid Duct (Stenson’s Duct): It runs over the masseter, pierces the buccal pad
of fat & opens in the vestibule of the mouth behind the upper 2nd molar tooth.
• Structures Within the Parotid Gland:
1. ECA (it gives the posterior auricular artery just before entering the gland),
with its 2 terminal branches; superficial temporal & maxillary artery.
2. Retro-mandibular Vein (Posterior facial vein with its tributaries).
3. Facial Nerve: It enters the deep surface of the gland close to the
stylomastoid foramen & gives 5 branches inside the gland radiating
forwards superficial to the vein & artery.
4. Parotid Lymph Nodes.
• Surface Anatomy of the Parotid Gland:
Upper Border: From the tragus to the mastoid process.
Anterior Border: From the tragus to the posterior border of the masseter
opposite the angle of the mouth.
Inferior Border: From the anterior border to below & behind the angle of the
mandible.
Posterior Border: From the mastoid process to the inferior border.
• Surface Anatomy of the Parotid Duct: The parotid ducts corresponds to the
middle 1/3 of an imaginary line from the tragus of the ear to the midportion of
the upper lip.
• Facial nerve anatomy
o Resection of the parotid tumors may be followed by recurrence due to fear
of injury to the facial nerve.
o The facial nerve arises from the stylomastoid foramen midway between the
bases of the mastoid and styloid processes, about 1.5 cm deep from the
external surface of the mastoid process, the nerve is about 1 cm in length
outside the gland then pierces the gland and runs through for another 1 cm,
where it divides into 2 branches which then give 5 branches:
• Temprofacial:
• Temporal.
• Zygomatic
• Buccal
• Cervicofacial:
• Mandibular

2
• Cervical
o So we have 5 branches that leave the gland at its anterior border adherent to
the surface of the masseter muscle.
o The parotid is divided by an imaginary plane passing through the plane of
the facial nerve and its branches into superficial and deep lobes. This plane
is called faciovenous plane.
INFLAMMATIONS OF THE PAROTID GLAND
Acute Inflammation (Acute Parotitis = Acute Sialadenitis):
1. Mumps (Acute Epidemic Parotitis):
• Etiology: Specific acute viral infection.
• Clinical Picture: It usually affects children, incubation period is 3 weeks, it starts
unilateral but in a few days it affects the other side, preceded by a prodromal
influenza-like syndrome. It causes fever & painful swelling which is soft &
tender. There is difficulty in mastication. It never suppurates.
• It may be complicated by pancreatitis &/or orchitis.
• Treatment: It is a self-limited disease that requires rest & symptomatic R/ only
(no specific R/).

3
2. Acute Suppurative Parotitis (Parotid Abscess):
Etiology:
• The infective organism is usually staph. aureus, and the usual predisposing
factor is infected dry mouth.
• Infection spreads from the mouth through the duct into the gland i.e. retrograde,
or blood-borne.
• The parotid gland being enclosed in a dense capsule, is liable to fulminating
inflammation & necrosis due to increased tension within the tightly closed
fascial compartment. Causes include the following:
1. Following obstruction of Stenson’s duct by a stone.
2. Postoperative parotitis due to dehydration & electrolyte imbalance.
3. As a complication of debilitating diseases as typhoid, cholera and uremia due
to dehydration & reduced resistance to infection.
4. As a complication of septicemia & bad oral hygiene.
5. Idiopathic !
Clinical Picture:
1. General Manifestations: Fever, tachycardia, insomnia, anorexia & loss of
weight.
2. Local Manifestations:
• Skin Over is red & edematous, and tethered to the swelling.
• Size: The swollen gland may be 3-4 times larger than a normal gland.
• Tenderness & Temperature: The swelling is very tender and hot with
throbbing pain.
• Consistency: Brawny i.e. firm but indentable. It is not compressible.
• Fluctuation is difficult to elicit & is never waited for. Pus may exudate
from the duct orifice on palpation of the gland (diagnostic). A culture
should be done
• Relations: It can not be moved over the deep structures, and becomes more
prominent when the patient clenches his teeth by contracting the masseter
muscles.
• Lymph Drainage: The upper deep cervical L.Ns will be enlarged & tender.
• Movements of the temporo-mandibular joint are restricted.
• Facial nerve is intact. If neglected, pus tracks its way to the external
auditory meatus.
Complications:
1. Fistula formation, chronicity.
2. Local spread causing cellulitis.
3. Systemic spread of infection causing septicemia.
4. It may rupture into the external auditory meatus.
5. It may burrow its way along the carotid sheath.
Investigations: Leukocytosis - Culture & Sensitivity from the pus.
Treatment:
1. Prophylactic: Good oral hygiene + correction of fluid & electrolyte
imbalance.

4
2. Medical Treatment: In early cases; warm fomentation, antibiotics, and
analgesics.
3. Surgical Treatment: Decompression of the parotid (Hilton’s method): Do not
wait for fluctuation. Under general anesthesia, a vertical incision is done in
the skin down to the parotid capsule. The capsule in incised transversely
along the course of the branches of the facial nerve to avoid their injury. Pus
is evacuated, a drain is put in the lower part, then closure is achieved.
Complications of this procedure include parotid fistula & facial nerve injury.
Chronic Inflammation (Chronic Sialadenitis):
1. Chronic Endemic Parotitis:
• It occurs in male farmers suffering from ankylostoma.
2. Chronic Pyogenic Parotitis:
• It results from improper treatment of acute parotitis, presence of stones in
the duct, or stenosis of the Stenson’s duct.
3. Chronic Recurrent Parotitis:
• It occurs in children & young adults specially women.
• Etiology is unknown, but may be allergic or autoimmune.
• Patients present with recurrent attacks of pain & parotid swelling at meal
times & a gush of purulent saliva may come out from the orifice of the duct
on pressure.
• Sialography may show sialectasia (dilated ductules & acini) & stenosis.
• Treatment includes good oral hygiene, anti-histaminics & catheterization
of the parotid duct & injection of antiseptic solutions.
4. Mikulicz Syndrome:
• Chronic, symmetrical, bilateral enlargement of all salivary glands &
lacrimal glands.
• It is an autoimmune disease.
• It may accompany sarcoidosis, reticulosis, TB & Sjogren’s syndrome.
5. Sjogren’s Syndrome:
• Primary:
• It is similar to Mikulicz syndrome but associated with xerostomia &
xerophthalmia.
• The gland is hard & nodular.
• Massive lymphocytic infiltration with high incidence of lymphomtous
infiltration.
• Secondary:
• Similar to the primary type but in addition there are manifestations of
connective tissue disease as RA.
• It predisposes to lymphoma of the parotid gland but in a smaller % than in
primary.
6. Other rare chronic inflammatory conditions of the parotid:
A) Tuberculosis:

5
• It mostly affects the parotid or submandibular from a nearby LN.
• It may be associated with systemic manifestations of TB as fever, night
sweating & anemia.
• The gland is firm & nodular but may become cystic with sinuses.
• R: Specific therapy of TB for 1 year + SAN regimen.
B) Sarcoidosis:
• Resembles TB but with no caseation.
• Other sites of affection include mediastinum.
C) Actinomycosis:
• Characterized by sulphur granules.
D) Cat scratch disease:
• A disease caused by infection with a gram negative bacillus called
Bartonella henslae from contact with cats, thought in the past to be a fungal
infection.
Complications of Chronic Parotitis:
1. Acute exacerbations.
2. Stone formation.
3. Sialodesis (persistent infection).
4. Fistula formation: Infection causes desquamation of organic debris leading to
deposition of calcium bicarbonate & calcium phosphate resulting in stone
formation → obstruction → 2ry infection & abscess formation → rupture & fistula
formation.
Treatment:
1. Good oral hygiene & antibiotics.
2. Removal of the offending cause e.g. stone.
3. Injection of antiseptic solutions through the duct.
4. In refractory cases we can do tympanic neurectomy stopping the parasympathetic
flow to the gland which then dries up.
5. Parotidectomy.
FREY’S SYNDROME
Definition:
• It is a syndrome that may complicate incision of parotid abscess due to injury
of the auriculo-temporal nerve.
Clinical Presentation:
• When the patient eats, the cheek becomes red, hot & painful; this is followed by
beads of perispiration (sweating).
• Starch-iodine test (B&L).
Pathogenesis:
• The severed axis cylinders conveying secretory impulses grow down the sheath
of the cutaneous elements of the nerve; thus, a stimulus intended for saliva
stimulation, evokes hyperaesthesia & sweating.
Treatment:
• Nerve avulsion of auriculo-temporal nerve &/or tympanetic neurectomy.
• Injection of Botulinum toxin into the skin of the affected area.

6
TUMORS OF THE PAROTID GLAND
The parotid gland is the gland of tumors, while the submandibular gland is the
gland of stones
CLASSIFICATION (Ackermann):
A. Benign Tumors:
1. Pleomorphic Adenoma (Mixed Salivary Tumor).
2. Monomorphic Adenoma:
a) Adenolymphoma (Warthin’s Tumor = Papillary Cystadenoma
Lymphomatosum).
b) Oxyphilic Adenoma (Oncocytoma).
3. Other Tumors:
a) Connective Tissue Tumors (lipoma, fibroma, hemangioma, neurofibroma).
b) Cysts (Branchial cysts, epidermoid cysts).
c) Benign Lymphoepithelial Tumor (Godwin’s Tumor).
B. Malignant Tumors:
1. Carcinoma:
a) Malignant Mixed Salivary Tumor (carcinoma ex-pleomorphic
adenoma=Carcino-sarcoma).
b) Adenocarcinoma:
i- Adenoid cystic Carcinoma (old name = cylindroma).
ii- Oxyphilic Carcinoma (Malignant Oncocytoma).
iii- Acinar (Serous) Carcinoma.
c) Muco-epidermoid Carcinoma (Low grade, high grade).
e) Undifferentiated Carcinoma.
f) SCC.
2. Lymphoma:
3. Non- epithelial tumors:
a) Haemangioma, vascular malformation.
b) Neurofibroma, neurilemmoma.
c) Sarcomas.
4. Unclassified & allied conditions:
a) Mikulicz syndrome.
b) Sjogren's syndrome.
c) Benign epithelial lesions.
What is the rule of 80?????????????????

7
A. BENIGN TUMORS
Criteria Pleomorphic adenoma Adenolymphoma
Incidence:
- General
- Gland Affected:
- Age:
- Sex:
- Bilaterality:
75% of parotid tumors
Parotid, may be submandibular &
minor glands
30-50 years
Females > males.
Unilateral
5% of parotid tumors
Almost exclusively in the parotid gland
> 40 years
Males > females (8:1)
Bilateral in 5-10% of cases
Pathology:
Macroscopic
Picture:
- Capsule:
- Matrix:
- Cut section:
-Microscopic
Picture:
• Well defined tumor but with small
extensions into the adjacent
normal tissue (responsible for
recurrence after removal).
• No true capsule
• Pleomorphic
• Not cystic, may show islets of
cartilage.
• It is a tumor formed of a
combination of epithelial cells
intermingled with a pleomorphic
stroma (fibrous, myxomatous &
pseudo-cartilaginous).
• A reddish brown mass.
• True capsule
• Full of lymphocytes (mainly B-cells)
• Cystic spaces line with columnar
cells
• It is a tumor that arises within the
lymphoid tissue (parotid lymph
nodes) in, or superficial to the parotid
gland.
Clinical Picture:
- Complaints: • Painless mass.
• Disfigurement. • Same
- Site: • Mostly, over the angle of the
mandible & below the lobule of
the ear, but may occur anywhere.
• Same
- Size: • Variable from pea-sized nodules
to large masses, 20 cm across !
• Small, usually 1-3 cm in diameter.
- Shape: • Spherical mass. • Spherical or hemi-spherical.
- Surface: • Lobulated or bosselated. • Smooth surface, well-defined.
- Consistency: • Heterogonous consistency (cystic,
soft, firm, hard)
• Homogenous, Soft, sometimes
cystic.
- Relations: • Not attached to the skin nor to the
deep structures i.e. mobile
• Same.
- Cervical LNs: • Not enlarged • Same
- Facial nerve: • Not affected. • Same.
Investigations: • Sialogram reveals a smooth filling
defect, also: CT + MRI.
• US
• Preoperative diagnosis by Tc99 scan
is available as it is the only parotid
tumour that can give a hot spot.

8
Malignant
Transformation:
It is a potentially malignant (5-10%)
& not a locally malignant tumor.
Epithelium → duct carcinoma, CT
→ chondrosarcoma.
Exceptional but documented (epithelium
→ adeno or epidermoid carcinoma,
Lymphoid component → lymphoma).
Treatment: 1. Conservative Parotidectomy:
• Removal of the superficial
lobe &/or deep lobe with
preservation of the facial
nerve.
• The flaps are raised & the
facial nerve is exposed at the
stylomastoid foramen & all its
5 branches are followed to
avoid their injury.
2. Enucleation (removal from
within its capsule) is never done.
It has a high recurrence rate.
1. Conservative Parotidectomy.
2. Resection-Enucleation (Enucleation by
extra-capsular excision): It is usually
sufficient as it is well capsulated &
does not recur.
B. MALIGNANT TUMORS
Incidence:
• Cancer parotid represents < 1% of all body cancer, and about 20% of all parotid
tumors.
• It is either De novo or on top of pleomeorphic adenoma???!!!
Sex: males > Females. (Browse: Male = Female).
Age: Above 50 Years.
Criteria of Malignancy (Signs of Malignant Transformation):
1. Rapid growth with a short history (1-4 months) fungation.
2. Change in consistency → stony hard.
3. Fixation (infiltration of overlying or deeper structures).
4. Paralysis of the facial nerve (facial palsy - 10%): Deviation of the lip towards the
normal side.
5. Pain (30%), may be referred to the ear (auriculo-temporal nerve) tenderness.
6. Enlarged regional lymph nodes or distant metastases (lungs, bones & abdominal
organs).
7. Microscopic evidence of malignancy. Only when there is invasion beyond the
capsule that the tumor will behave clinically malignant.
8. Unequal pulsations of superficial temporal artery.
9. Trismus: due to invasion of masseter/pterygoid muscles or due to restricted
movements of TMJ.
Spread:
1. Local → nearby organs (masseter muscle, skin, ramus of the mandible).
2. Lymphatic → to the intra- and peri-glandular nodes. The next echelon of
lymphatics for the parotid is the upper jugular nodal chain.
3. Hematogenous (very late) → Mainly to lungs & bones particularly the vertebral
column.

9
4. Adenoid cystic carcinoma (cylindroma) tends to grow through peri-neural
lymphatics with 1)increased risk of nerve affection, which should be sacrificed,
2)increased rate of recurrence, 3)increased risk of intra-cranial extension.
Specific criteria of some types of Parotid Cancer:
1. Carcinoma ex-pleomorphic adenoma: Rare.
2. Adenocystic Carcinoma (cylindroma): Aggressive due to peri-neural spread.
3. Acinar Carcinoma: Low grade tumour, with very late metastases & therefore
better prognosis in comparison to others.
4. Muco-epidermoid Carcinoma: Low grade, high grade: with LNs and possibility
of distant metastases.
5. Lymphoma: Non-Hodjkin's, limited or part of generalized.
Investigations:
1. Plain X-Ray: To the mandible (to exclude bone invasion) & chest (for lung
metastases).
2. Sialogram: Irregular filling defect.
3. US: Diagnoses a stone, cyst & extension of the mass.
4. CT: Describes the character of a mass, its relation to nearby organs, the
capsule…etc.
5. MRI.
6. PET.
7. Angiography.
8. Radioactive Isotope Scanning using 99cTm.
9. Biopsy:
• Core-Needle Biopsy, or Fine Needle Aspiration Cytology: Disadvantages
include: false +ve & -ve results, it may cause seedling of tumor cells & can
not show the tumor type.
• Frozen-Section Biopsy: It is accurate in showing malignant cells & helpful in
detecting the extent of surgery needed (free margins). However, it can not
identify the tumor type !.
• Incisional Biopsy: If there is invasion of the skin. It shows the tumor type,
tumor grade & invasion.
• The least accepted surgical biopsy is superficial parotidectomy.
Differential Diagnosis:
Point of Difference Benign Tumor Malignant Tumor
1. Rate of Growth:
2. Sex:
3. Age:
4. Pain:
5. Mobility:
6. Consistency :
7. Facial Nerve:
8. Cervical Lymph Nodes:
9. Local or Distant Metastases:
10. Sialogram:
11. Biopsy:
• Slow
• Female
• Below 40 years
• Absent
• Mobile
• Firm or cystic
• Free
• Not enlarged
• Absent
• Regular filling defect
• No malignant cells
• Rapid
• Male
• Above 50 years
• Present (30%)
• Fixed
• Hard
• Affected (Facial palsy) (30%)
• May be enlarged
• May be Present
• Irregular filling defect
• Malignant cells - invasion

10
Treatment
A. Operable Cases:
a) For the Tumor:
1. Superficial Parotidectomy: For small tumors confined to superficial lobe & of
low-grade malignancy.
2. Total Parotidectomy: For tumors of the deep lobe, superficial tumors
infiltrating the deep lobe, and high-grade rapidly growing malignant tumors.
3. Radical parotidectomy: means sacrificing the facial nerve.
b) For the Lymph Nodes:
• Not felt ......................... Observe (wait & see).
• Felt & Mobile ............... Block neck dissection.
• Felt & Fixed ................. Radiotherapy.
c) Post-operative Radiotherapy is indicated in the following conditions:
1. The presence of extraglandular disease,
2. perineural invasion,
3. direct invasion of regional structures,
4. regional metastasis,
5. high-grade histology
6. If the parotidectomy was performed for a benign tumor that turned out to
be malignant !
d) Facial Nerve Replacement (if has been sacrificed):
• Nerve grafting may be used, at the time of 1ry surgery, by sural nerve or great
auricular nerve.
• Results appear after 6 months & reach their maximum by 2-3 years.
B. Inoperable Cases:
Radiotherapy is used (although there is poor response) in presence of local fixation,
fixed cervical lymph nodes, and distant metastases.
Cysts of the salivary glands
1. Mucocele:
• It is a mucous retention cyst arising either from minor salivary gland esp. in the
buccal mucosa or from a major salivary gland.
• It may be due to trauma to the salivary ducts with extravasation of the secretions
when it is called sialocele.
• R: Excision of the cyst and the gland of origin.
2. Ranula: (Vide infra).
Differential Diagnosis:
A) Bilateral parotid lesions:
1. Mumps.
2. Adenolymphoma (10-15%)
3. Autoimmune: Mikulicz Syndrome, Sjogrin’s Syndrome.
B) Cystic parotid lesions:
1. Skin Cyst: Sebaceous cyst

11
2. Subcutaneous Cyst: Dermoid cyst.
3. Parotid Cystic Swellings: Parotid cyst (probably derived from 1st branchial
cleft)- adenolymphoma.
4. Pseudo-cyst: Hematoma, Abscess.
C) Acute parotid lesions:
1. Hematoma.
2. Abscess.
3. Acute Lymphadenitis
4. Septic Parotitis.
5. Mumps.
6. Ostoemyelitis.
D) Differential Diagnosis Of A Swelling In The Parotid Region:
Tissue Of Origin Causes Of The Swelling
1. Skin 1. Benign Tumor. e.g. papilloma.
2. Cyst: e.g. Sebaceous cyst.
3. Malignant Tumor e.g. SCC, BCC, malignant melanoma,...etc.
2. SC Tissues 1. Benign Tumor: Lipoma - Fibroma - Neurofibroma - Hemangioma.
2. Cyst e.g. Dermoid Cyst.
3. Malignant Tumor: Sarcomas.
3. Parotid L.Ns 1. Acute or chronic non-specific Lymphadenitis.
2. Chronic Specific Lymphadenitis e.g. T.B.
3. Malignancy e.g. Secondaries or lymphoma.
4. Parotid Gland 1. Acute Parotitis (Mumps - Parotid Abscess).
2. Chronic Parotitis.
3. Parotid Cyst.
4. Parotid Tumor (Benign - Malignant).
5. Autoimmune Diseases (Mikulicz & Sjogrin’s Syndromes).
5. Masseter Muscle 1. Fibrosarcoma.
2. Rhabdomyosarcoma.
3. Myxoma of The Masseter.
4. Hypertrophied Muscle.
6. Mandible Ramus 1. Osteomyelitis.
2. Cysts: Adamantinoma, dental cysts.
3. Osteoclastoma.
4. Secondaries.
7. Mucosa of Cheek Squamous Cell Carcinoma.
8. Others 1. Branchial Cyst.
2. Neuroma of the facial nerve.
3. Thrombosis of the facial vein.
4. Aneurysm of the temporal artery.
5. Mastoiditis.

12
II. SUBMANDIBULAR GLAND
Surgical Anatomy:
• It is a major salivary gland that secretes seromucinous saliva.
• It lies partly under cover of the mandible, and is made of a large superficial part
& a small deep part. The superficial part lies in the digastric triangle, reaching
upward under cover of the mandible & separated posteriorly from the parotid
gland by the stylo-mandibular ligament.
• The deep part extends forward and its anterior end reaches as far as the sublingual
gland. It is related to the mucosa of the floor of the mouth, so it can be felt
bidigitally.
• The gland is covered by a capsule derived from the general investing layer of the
neck.
• Hypoglossal nerve lies deep to the gland on the hyoglossus muscle and also is the
lingual nerve which hook on the submandibular duct making the famous triple
relation.
• The marginal branch of the facial nerve runs in the sub-platysmal plane superficial
to the gland, one centimeter below the mandible.
• Its duct (Wharton’s Duct) emerges from the anterior end of the deep part of the
gland opens in the oral cavity on the summit of a small papilla, near the frenulum
of the tongue.
• The submandibular gland is supplied by branches of the facial & lingual arteries.
The veins drain into the facial & lingual veins, while the lymph vessels drain into
the submandibular & deep cervical lymph nodes.
ACUTE SUBMANDIBULAR SIALADENITIS
Etiology: It is usually accompanied with salivary stones, and is therefore, usually
recurrent.
Clinical Picture:
• Age & Sex: Young adults - Males = females.
• Complaints: Painful swelling in the submandibular region + salivary colic i.e.
pain & swelling of the gland with meals. Pain may be referred to teeth or tongue.
• Examination: Tender swelling is felt bidigitally. A stone in the duct may also be
felt. The orifice of the submandibular duct is congested & edematous. It pours
drops of purulent saliva on squeezing the duct.
Treatment:
• Antiseptic mouth wash + systemic antibiotics. Treatment of stones (if present)
after subsidence of the acute inflammation.
CHRONIC CALCULAR SUBMANDIBULAR SIALADENITIS
Etiology:
• Incidence of stone formation in submandibular gland is 30 times greater than in
the parotid gland, because:
1. The duct is directed forwards & upwards i.e. independent.
2. The secretion is more viscid than that of the parotid (increases stasis).

13
3. The end of the duct opens in the floor of the mouth & is more liable to be
obstructed by inflammation, and foreign bodies.
4. High salt content (stones consist of calcium carbonate & phosphate &
magnesium phosphate).
Clinical Picture:
1. Submandibular swelling (firm or hard simulating a tumor) which increases in size
with meals.
2. Pain associated with meal intake, smell or sight (to differentiate it from dental
pain).
3. Lemon Juice Test: Intake of lemon juice causes increase in pain & size of the
swelling.
4. Oral Examination of the Orifice of the Duct: reveals saliva pouring on the
unaffected side, whereas little or no secretion is seen ejected from the swollen
(affected) side.
5. Bidigital Examination (finger in the mouth & finger outside): The swelling or a
stone may be felt.
NB: Sites of stone impaction:
1. Meatal.
2. Intraductal.
3. Juxta-glandular.
4. Intra-glandular.
Complications:
• If the condition is not treated, it can be complicated by abscess or salivary fistula
to the skin.
Investigations:
1. Plain X-Ray:
• An intra-oral film in the occlusal or oblique view of the mandible may
show the stone. Most of the stones of the parotid are translucent, while
most of those of the submandibular are trans-opaque.
2. Sialogram: May show filling defect (if stone is translucent).
3. US: Can visualize the stone and comment of the dilatation of the duct system
if present.
Treatment:
• Meatal stone → Meatotomy & extraction of the stone + good oral hygiene.
• Intra-ductal stone → Direct incision on the stone without closure, after nerve
block or general anesthesia.
• Juxta-glandular stone → Submandibular sialadenectomy is mandatory as
extraction of the tone trans-orally is extremely hazardous for possibility of
injury of the lingual nerve which hooks around the duct at this point.
• Intra-glandular stone → Submandibular sialadenectomy.
The procedure:
The operation is done from a transverse incision 2 cms below the mandible
to safeguard the marginal branch of the VII. Ligate the facial artery and vein
twice, once when it leaves the upper border of the gland and then as it enters

14
the posterior pole of the gland. Ligate and cut the duct after freeing it from
the lingual nerve. The same operation is done for submandibular tumours.
Complications of the procedure:
1. Injury of important structures:
Hypoglossal nerve (XII) → atrophy & paralysis of half the tongue.
Lingual nerve → loss of sensation.
Mandibular nerve of facial → depression of the angle of the mouth.
Facial artery → hemorrhage.
Wall of the pharynx → fistula.
2. Salivary fistula if part is left behind.
3. Recurrence of tumor.
TUMORS OF THE SUBMANDIBUALR GLAND
Types:
The same as parotid tumors (adenolymphoma occurs almost exclusively in the
parotid), the mixed salivary tumor being also the commonest, but carcinoma is
commoner than in the parotid gland.
Incidence of Cancer of Salivary Glands:
Gland Affected B.T. M.T.
• Parotid
• Submandibular
• Sublingual
• Minor Salivary Glands
80 %
60 %
10 %
10 %
20 %
40 %
90 %
90 %
Investigations:
• Routine Investigations.
• Plain X-ray: for detection of the stone (chronic sialadenitis) or infiltration of the
mandible (cancer).
• Sialography: filling defect (stone).
• Biopsy (FNAC).
Treatment:
Benign Tumor → Submandibular sialadenectomy.
Malignant Tumor → Submandibular sialadenectomy + radical neck dissection of
lymph nodes if they were involved & partial mandibulectomy if the mandible was
involved.
DIFFERENTIAL DIAGNOSIS OF SWELLINGS IN SUBMANDIBULAR
REGION
• It should be differentiated from other swellings in the submandibular region,
especially submandibular lymph nodes. A lymph node can be rolled over the border
of the mandible, but the gland can not, due to attachment of its capsule to the lower
border of the mandible. Also, the gland is better felt than the lymph node by
bidigital examination.
• DD: refer to the section of lateral neck swellings.

15

16
III. SUBLINGUAL GLAND
• It is a major salivary gland secreting mucinous saliva.
• It is enlarged in Mikulicz’s & Sjogrins’ Syndromes (+ the major salivary glands &
lacrimal glands).
RANULA
Definition:
• It is a mucous extravasation cyst in the floor of the mouth arising from the
sublingual gland.
• It is so called because it is a bluish, translucent, cystic swelling that simulates a
frog’s belly (In Latin, ranula = a small frog).
Clinical Picture:
• Age & Sex: It affects children & young adults, of both sexes equally.
• Symptoms: A swelling in the floor of the mouth. It usually ruptures & refills
again.
• Examination:
Sites: In the angle between the tongue & the floor of the mouth, usually to one
side of the midline. If it lies in the midline, it becomes constricted by the
frenulum → hour-glass appearance.
Varies in size from 1 to 5 cm in diameter.
It is spherical (but only the top half is seen).
Smooth, covered by tortuous veins & the submandibular duct is displaced &
stretched over it.
A ranula is soft, usually fluctuant, but can not be compressed or reduced.
Characteristically translucent, with a bluish tinge.
Treatment:
• Partial Excision (Marsupilization):
Removal of the dome of the cyst
with the overlying mucous
membrane, followed by suture of the
cut edge of the mucous membrane so
that the floor of the cyst forms part
of the floor of the mouth.
NB: Plunging or
Thomson’s ranula or
deep cervical Ranula:
• This type is rare & is considered as a mucous retention cyst not extravasation one.
• Arising from sublingual or submandibular gland & extends into the
submandibular region through mylohyoid diaphragm. Patients present with a
dumb-bell shaped swelling that is soft cystic and painless.
• Treatment is through cervical approach removing the cyst, sublingual and
submandibular glands.
IV. MINOR SALIVARY GLANDS

17
• There are more than 400 minor salivary glands in the oral cavity, pharynx &
paranasal sinuses.
• Major and minor salivary glands secrete from 1-1.5 litres of saliva daily.
Clinical Picture:
• Symptomless, swelling, firm or hard, mobile or fixed, ulcerating or not, if
malignant, it invades the underlying bone.
Diagnosis:
• Biopsy is essential for diagnosis.
Treatment:
• The tumor should be widely excised with a safety margin to avoid recurrence.
• Radical neck dissection may be needed in case of lymph node involvement.

18