Rx15 tpp tues_330_1_gavin_2nader_3jeter
56
Third-Party Payer Track Rx Drugs and Urine Testing: Knowing What’s Too Much, Too Little and Just Right Presenters: • Michael Gavin, President, PRIUM • Jo-Ellen Abou Nader, CFE, CIA, CRMA, Senior Director, Drug Waste Solutions, Express Scripts, Inc. • Elaine Jeter, MD, MolDX Medical Director, Palmetto GBA Moderator: Daniel Blaney-Koen, JD, Senior Legislative Attorney, American Medical Association Advocacy Resource Center, and Member, Rx Summit National Advisory Board
-
Upload
opunite -
Category
Healthcare
-
view
85 -
download
0
Transcript of Rx15 tpp tues_330_1_gavin_2nader_3jeter

Third-Party Payer Track
Rx Drugs and Urine Testing:Knowing What’s Too Much, Too Little and Just
Right
Presenters:• Michael Gavin, President, PRIUM• Jo-Ellen Abou Nader, CFE, CIA, CRMA, Senior Director,
Drug Waste Solutions, Express Scripts, Inc.• Elaine Jeter, MD, MolDX Medical Director, Palmetto GBA
Moderator: Daniel Blaney-Koen, JD, Senior Legislative Attorney, American Medical Association Advocacy Resource Center, and Member, Rx Summit National Advisory Board

Disclosures• Michael Gavin has disclosed no relevant, real or apparent personal
or professional financial relationships with proprietary entities that produce health care goods and services.
• Jo-Ellen Abou Nader, CFE, CIA, CRMA, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
• Elaine Jeter, MD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
• Daniel Blaney-Koen, JD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.

Learning Objectives
1. Describe how the PBM identifies, investigates and resolves Rx fraud, waste and abuse.
2. Compare appropriate with fraudulent and wasteful usage of UDT.
3. Advocate strategies that optimize usage of UDT.

Urine Drug Monitoring
Too Much or Too Little

Michael Gavin wishes to disclose he is the President of PRIUM, a wholly-owned subsidiary of Ameritox. He will present this content in a fair and balanced manner.
Disclosure 5

6
This presentation:1. Outlines the care settings and technologies used for urine
drug monitoring2. Illustrates the clinical rationale for urine drug monitoring 3. Examines why appropriate testing does not always occur
Learning Objectives

7
• Industry Context• Data and Observations• Best Practices
Agenda

8
Societal BurdenMisuse and abuse of prescription drugs is hugely expensive from a financial and socioeconomic perspective
• In the United States, prescription opioid abuse costs were about $55.7 billion in 2007.1 Of this amount, 46% was attributable to workplace costs, 45% to healthcare costs, and 9% to criminal justice costs.
• Drug overdose was the leading cause of injury death in 2012. Among people 25 to 64 years old, drug overdose caused more deaths than motor vehicle traffic crashes.2
• The drug overdose death rate has more than doubled from 1999 through 2013.3
1. Birnbaum HG, White AG, Schiller M, Waldman T, Cleveland JM, and Roland CL. Societal costs of prescription opioid abuse, dependence, and misuse in the United States. Pain Medicine 2011; 12: 657-667
2. Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]. (2014) Available from URL: http://www.cdc.gov/injury/wisqars/fatal.html.
3. Centers for Disease Control and Prevention. National Vital Statistics System mortality data. (2015) Available from URL: http://www.cdc.gov/nchs/deaths.htm.

Review of Test Settings & Technologies
Point of Care Cups / Dipsticks(Presumptive)
Desktop Analyzers(Presumptive)
Commercial Analyzers(Presumptive)
Mass Spectrometry(Definitive)
Setting Physician Offices Commercial Labs Mostly Commercial Labs
Technology Enzyme Immunoassay Enzyme Immunoassay Liquid/Gas Chromatography with Mass Spectrometry
Est. Device Cost <$10 <$30,000 ~$295,000-$690,000 ~$200,000 - $400,000
Results & Reliability
Qualitative result Detects drug class Low to moderate degree
of reliability(1)
Qualitative result Typically detects drug
class(2)
Moderate to high degree of reliability
Quality highly variable
Qualitative results Detects drug class High degree of reliability FDA approve Reagent
kits 95% confidence level
Quantitative (ng / mL) result
Detects specific compound
High degree of reliability
Lab Certification CLIA-waiver CLIA certificate – Moderate complexity lab
CLIA certificate – Moderate complexity lab
Rigorous lab audits Requires moderate to
highly trained personnel
CLIA certificate – High complexity lab
Rigorous lab audits Requires highly trained
personnel1. In a recent comparison of POCT and confirmation results performed by Ameritox POCT devices produced an incorrect result over 50% of the time.2. Assays exist for some specific compounds.
Not Created EqualNot all testing technologies and settings are created equal; the quality and quantity of data differs by setting.
6

10
Why Monitor?Urine drug monitoring informs clinical decision making by prompting new conversations between doctors and patients.
What Drug Monitoring Tells Us
• Presence of prescribed substances• Identification of non-prescribed
substances• Identification of illicits• Uncover possible misuse/abuse and
cross-reactivity risk
What Drug Monitoring Doesn’t Tell Us
• The amount of drug ingested or taken
• When last dose was taken• Source of the medication.• Proof of misuse/abuse

11Longitudinal AnalysisThe availability of information to assist with assessing likely adherence over time is of critical importance in light of chronic opioid therapy.

12
MEDs1 Rx Spend2
1 2 3 4 5 6400
800
1,200
1,600 191%
Quarters Since Injury
Avg.
Qua
rter
ly M
ED p
er C
laim
2003 2004 2005 2006 2007 2008 2009 2010 2011 $150
$200
$250
$300
58%
Service Year
Dolla
rs P
aid
per M
edica
l Cla
im
Increasing Rx SpendThe need for UDM has become more critical as prescription drug spend for chronic pain (and related conditions) has skyrocketed.
1. NCCI Research Brief, 20122. NCCI Research Brief, 2013

13
Observations
Illicits Found Rx Not Found Found, No Rx0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
Overall Testing Results Over Time
2006 2007 2008 2009 2010 2011 2012 2013 2014
Many samples show multiple issues; just 33.9% of samples show no abnormalities.
1. Data collected from Ameritox drug monitoring accessions.
14
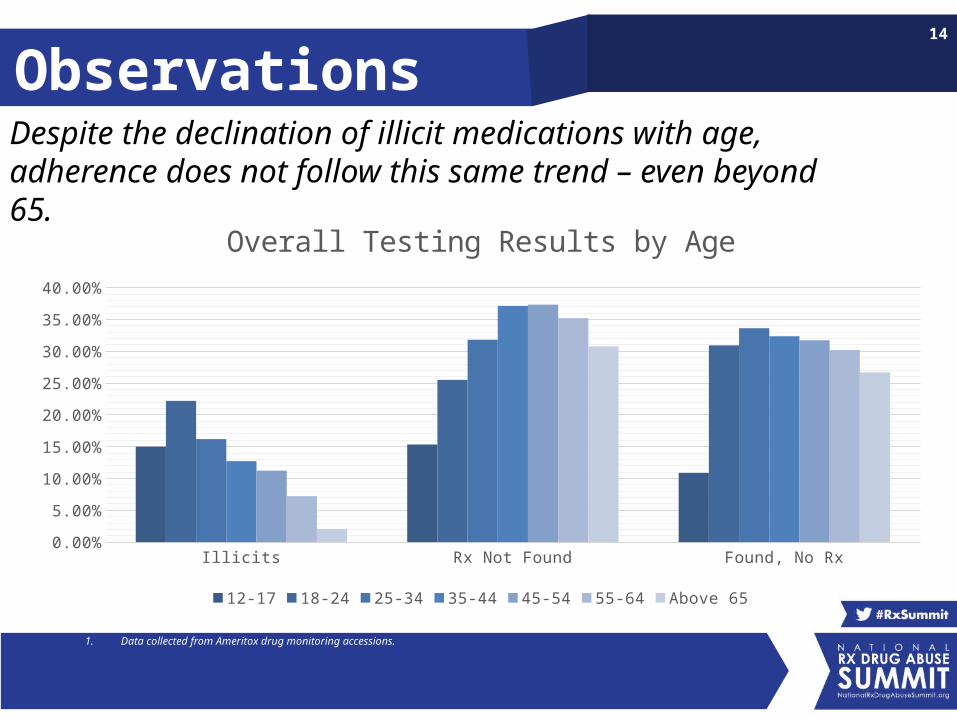
Observations
Illicits Rx Not Found Found, No Rx0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
Overall Testing Results by Age
12-17 18-24 25-34 35-44 45-54 55-64 Above 65
Despite the declination of illicit medications with age, adherence does not follow this same trend – even beyond 65.
1. Data collected from Ameritox drug monitoring accessions.

15
ObservationsThe uptick in illicit use may potentially be driven by multiples factors including payer mix, adverse selection, or a rise in use of illicits.
12-17 18-24 25-34 35-44 45-54 55-64 65-70 Above 710%
5%
10%
15%
20%
25%
IllicitsBy Age By Year
2006 2007 2008 2009 2010 2011 2012 2013 2014
1. Data collected from Ameritox drug monitoring accessions.

16
Observations
Commercial Medicaid Medicare Workers Comp5%
7%
9%
11%
13%
15%
17%
19%
21%
Illicits
2010 2011 2012 2013 2014
The use of illicits among Medicaid patients significantly greater than other payer categories.
1. Data collected from Ameritox drug monitoring accessions.

17
ObservationsPotential non-adherence among older Americans is much more pronounced.
12-17 18-24 25-34 35-44 45-54 55-64 65-70 Above 710%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Rx Not FoundBy Age By Year
2006 2007 2008 2009 2010 2011 2012 2013 2014
1. Data collected from Ameritox drug monitoring accessions.

18
Observations
Commercial Medicaid Medicare Workers Comp25%
27%
29%
31%
33%
35%
37%
39%
41%
Rx Not Found
2010 2011 2012 2013 2014
In fact Medicare population shows the highest incidence of prescriptions not found.
1. Data collected from Ameritox drug monitoring accessions.
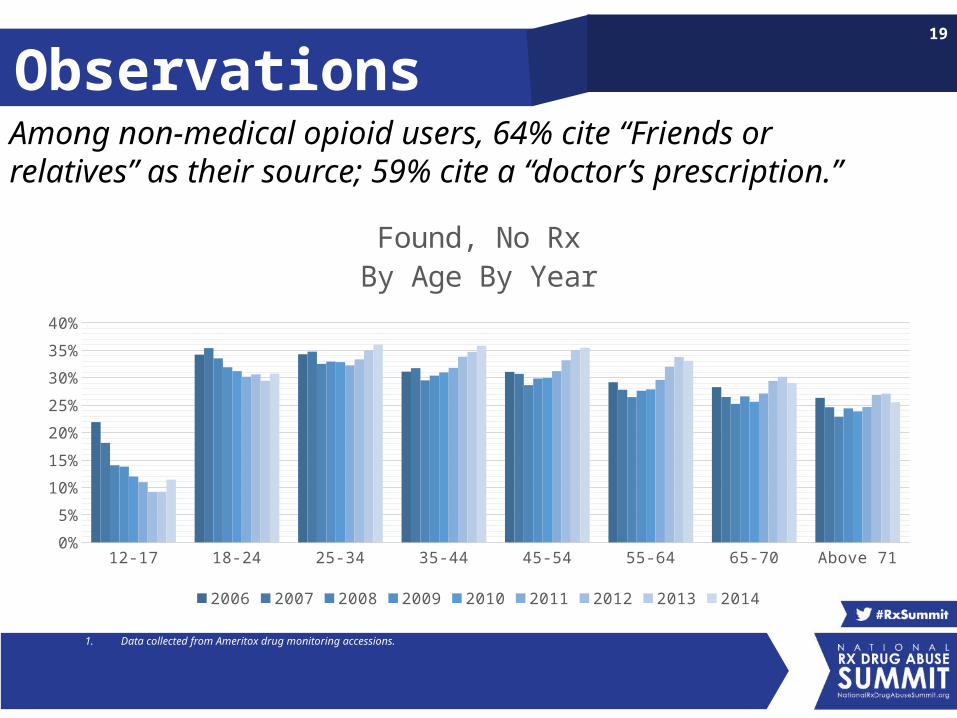
19
ObservationsAmong non-medical opioid users, 64% cite “Friends or relatives” as their source; 59% cite a “doctor’s prescription.”
12-17 18-24 25-34 35-44 45-54 55-64 65-70 Above 710%
5%
10%
15%
20%
25%
30%
35%
40%
Found, No RxBy Age By Year
2006 2007 2008 2009 2010 2011 2012 2013 2014
1. Data collected from Ameritox drug monitoring accessions.

20
Observations
Commercial Medicaid Medicare Workers Comp20%
22%
24%
26%
28%
30%
32%
34%
36%
38%
Found, No Rx
2010 2011 2012 2013 2014
The growth of this particular inconsistency is more pronounced in the Medicaid, Medicare, and Workers’ Comp populations.
1. Data collected from Ameritox drug monitoring accessions.
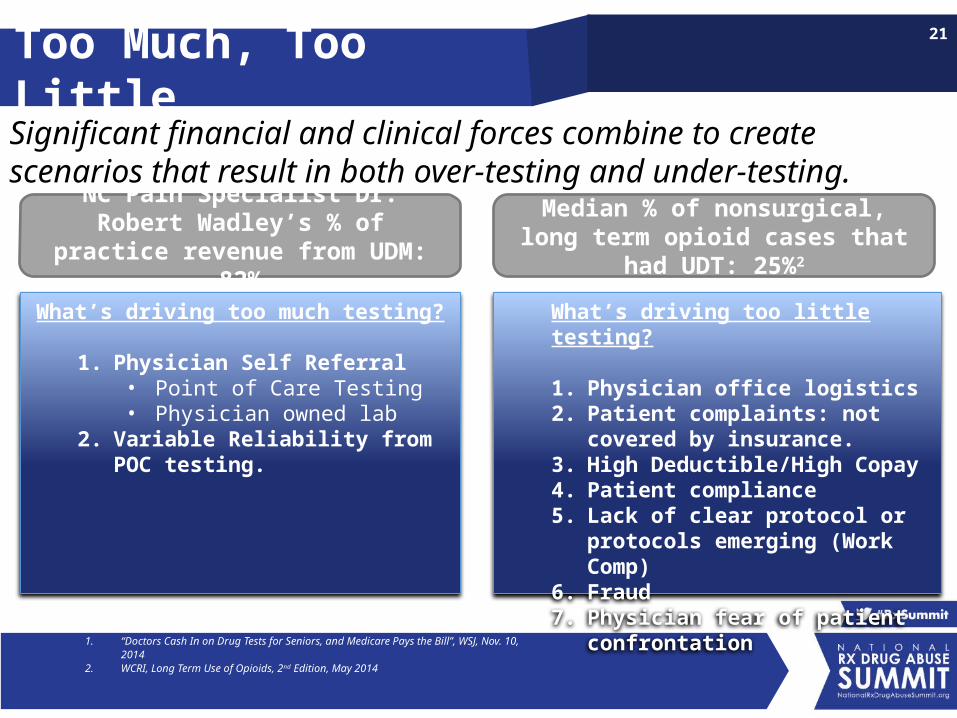
21Too Much, Too Little
What’s driving too much testing?
1. Physician Self Referral• Point of Care Testing • Physician owned lab
2. Variable Reliability from POC testing.
What’s driving too little testing?
1. Physician office logistics2. Patient complaints: not covered by
insurance.3. High Deductible/High Copay4. Patient compliance5. Lack of clear protocol or protocols
emerging (Work Comp)6. Fraud7. Physician fear of patient confrontation
Significant financial and clinical forces combine to create scenarios that result in both over-testing and under-testing.
NC Pain Specialist Dr. Robert Wadley’s % of practice revenue from UDM: 82%
Median % of nonsurgical, long term opioid cases that had UDT: 25%2
1. “Doctors Cash In on Drug Tests for Seniors, and Medicare Pays the Bill”, WSJ, Nov. 10, 20142. WCRI, Long Term Use of Opioids, 2nd Edition, May 2014
22
Best PracticesThe effective deployment of drug monitoring by payors requires planning and coordination with managed care resources.
I. Guidelines driven testing
II. Patient centered care
III. Proactive patient identification
IV. Partners and providers compliant with all regulations
V. Utilization Review for UDT
VI. Coordinated clinical interventions

23
GuidelinesEvidence-based guidelines call for monitoring medication compliance with testing protocols that align with the risk level of the patient.
1. Work Loss Data Institute. Official Disability Guidelines “Evidenced-Based Decision Support.
Risk of Addiction/Aberrant
BehaviorMonitoring Recommendation
Low • Tested within 6 months of therapy initiation• Yearly testing thereafter
Medium• Point-of-contact screening 2 to 3 times yearly• Confirmatory testing for inappropriate/unexplained
results
High• Testing as frequently as once per month.• Confirmatory testing for inappropriate/unexplained
results
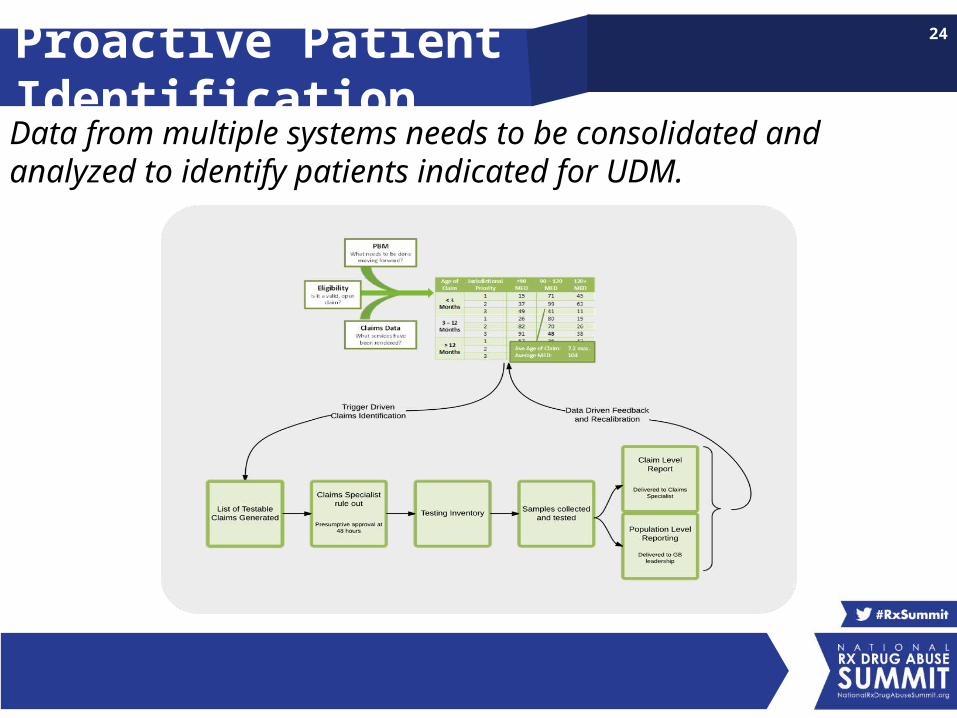
24Proactive Patient IdentificationData from multiple systems needs to be consolidated and analyzed to identify patients indicated for UDM.

25Compliant Providers
What’s driving too much testing?
1. Overuse of Point-of-Care testing and in-office analyzers (physician self-referral)
2. Too many tests per patient3. Free goods (e.g., testing cups)4. Profit sharing models (e.g., physician owns % of lab)5. Education on billing6. Free legal advice
Some doctors and/or labs engage in inappropriate business practices for which payers should be vigilant
26Utilization Review
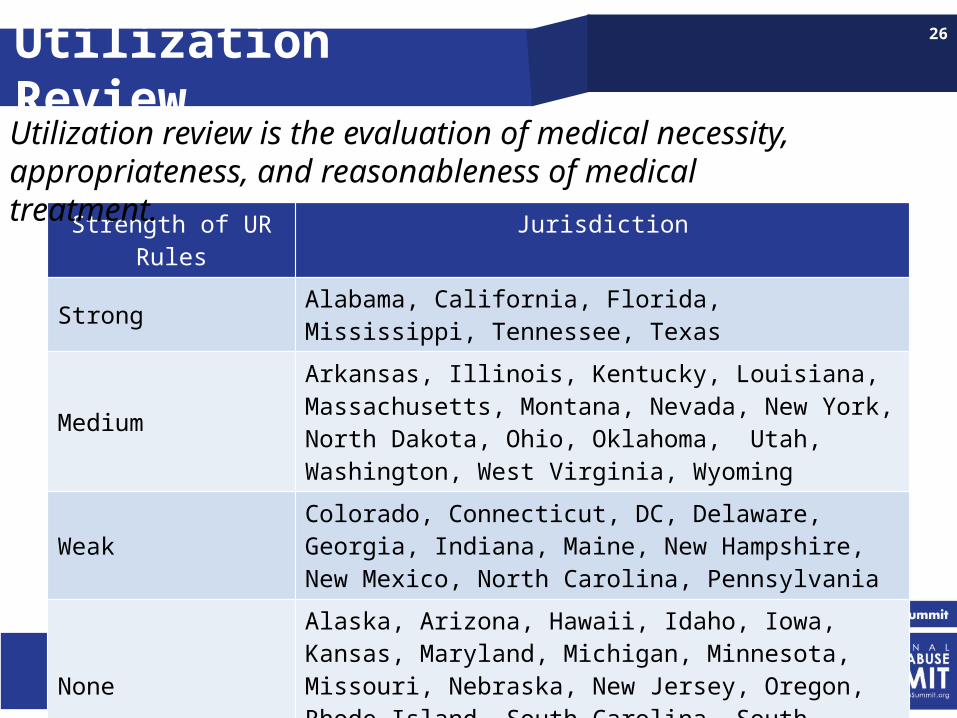
Strength of UR Rules Jurisdiction
Strong Alabama, California, Florida, Mississippi, Tennessee, Texas
MediumArkansas, Illinois, Kentucky, Louisiana, Massachusetts, Montana, Nevada, New York, North Dakota, Ohio, Oklahoma, Utah, Washington, West Virginia, Wyoming
WeakColorado, Connecticut, DC, Delaware, Georgia, Indiana, Maine, New Hampshire, New Mexico, North Carolina, Pennsylvania
NoneAlaska, Arizona, Hawaii, Idaho, Iowa, Kansas, Maryland, Michigan, Minnesota, Missouri, Nebraska, New Jersey, Oregon, Rhode Island, South Carolina, South Dakota, Vermont, Virginia, Wisconsin
Utilization review is the evaluation of medical necessity, appropriateness, and reasonableness of medical treatment.

27Coordinated InterventionsManaged care tools are all essential components to ensuring compliance with medication regimens.
What was dispensed?
What’s the patient taking?
What should they be taking?
Pharmacy Benefit Manager
Urine Drug Monitoring
Peer ReviewUtilization ReviewCase Management
Misuse, Abuse & CompoundingJo-Ellen Abou Nader, CFE, CIA, CRMA
Senior Director, Drug Waste Solutions

Jo-Ellen Abou Nader, CFE, CIA, CRMA, has disclosed no relevant, real or apparent personal or professional
financial relationships with proprietary entities that produce health care goods and services
Agenda
• Fraud, Waste & Abuse Issues: Opioids and compounds
• Express Scripts Research: Emerging challenges
• Solutions: PBM tools to safeguard members and payers
50 AMERICANS DIE EVERY DAY FROM RX POISONING
Opioid Misuse Puts Patients at Risk

Compounds Drive Wasteful Spending
MORE THAN $3 BILLION COST TO U.S. IN 2014

Pharmacy Network
POS Edits
Pharmacy Claims
Network Audit
Medical Claims
Fraud Case Work
Physician &
Member Network
ClientMedical Vendor
Best Practices: Fraud, Waste & Abuse

Data & Analytics Dig Deeper

CHRONIC USE
Troubling Findings About Opioid Use
• Fewer Americans are using opioids, but total amounts taken continue to increase
• Of patients taking an opioid pain medication for at least 30 days, nearly half will still be taking opioids 3 years later
• Nearly half of long-term users are taking short-acting formulations only, increasing risk of addiction
• Women are 30% more likely to use opioids than men
• Only 3% prescribed by pain specialists
PRESCRIBING PATTERNS

Intervene Early
Mine Pharmacy and Medical Data
Follow Evidence-Based Protocol
Communicate Clearly and Often
Increase Collaboration
Opioid Insights and Best Practices
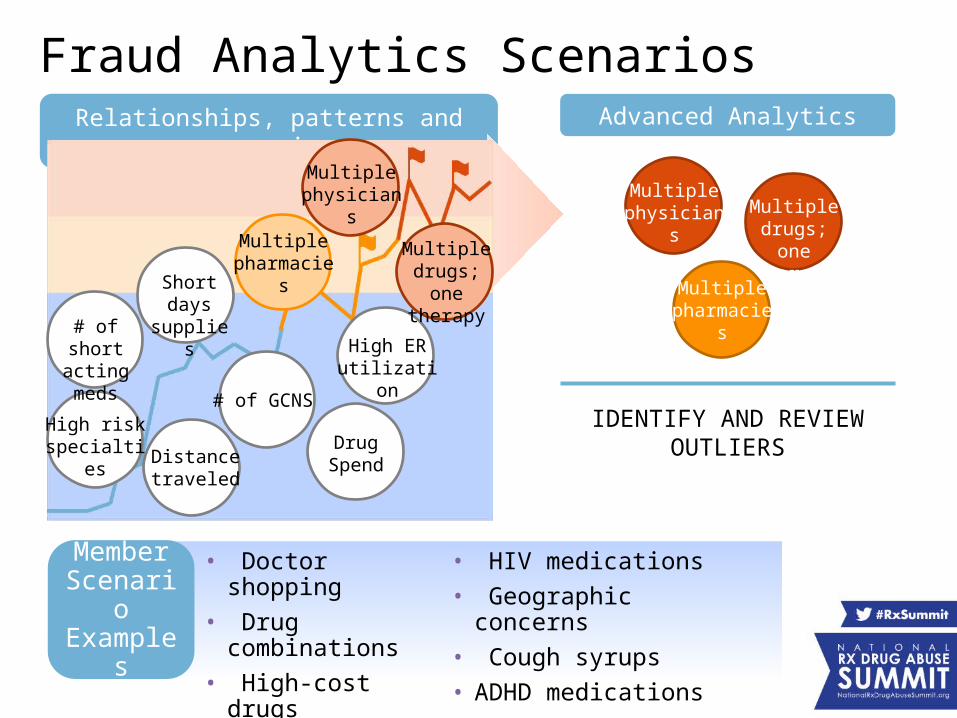
Member Scenari
o Exampl
es
Relationships, patterns and scenarios
Advanced Analytics
IDENTIFY AND REVIEW OUTLIERS
Multiple physicians Multiple
drugs; one therapy
Multiple pharmacie
s
High risk specialties
# of GCNS
Distance traveled
Short days
supplies# of short acting meds High ER
utilization
Drug Spend
Multiple pharmacie
s
Multiple physicians
Multiple drugs; one
therapy
Fraud Analytics Scenarios
• Doctor shopping• Drug combinations• High-cost drugs
• HIV medications• Geographic concerns• Cough syrups• ADHD medications

43 prescriptions 1 patient
17 prescribers 5 pharmacies
Case Study: Abuse Intervention

• Member restricted to 1 pharmacy and/or 1 physician for all controlled substances and muscle relaxers
• Efficiently manages and reduces risk within membership
• Completed through a series of letters to member
Solution: Lock-In Pharmacy, Provider
CLIENTS WITH AUTO LOCK-IN EXPERIENCE 4X MORE SAVINGS
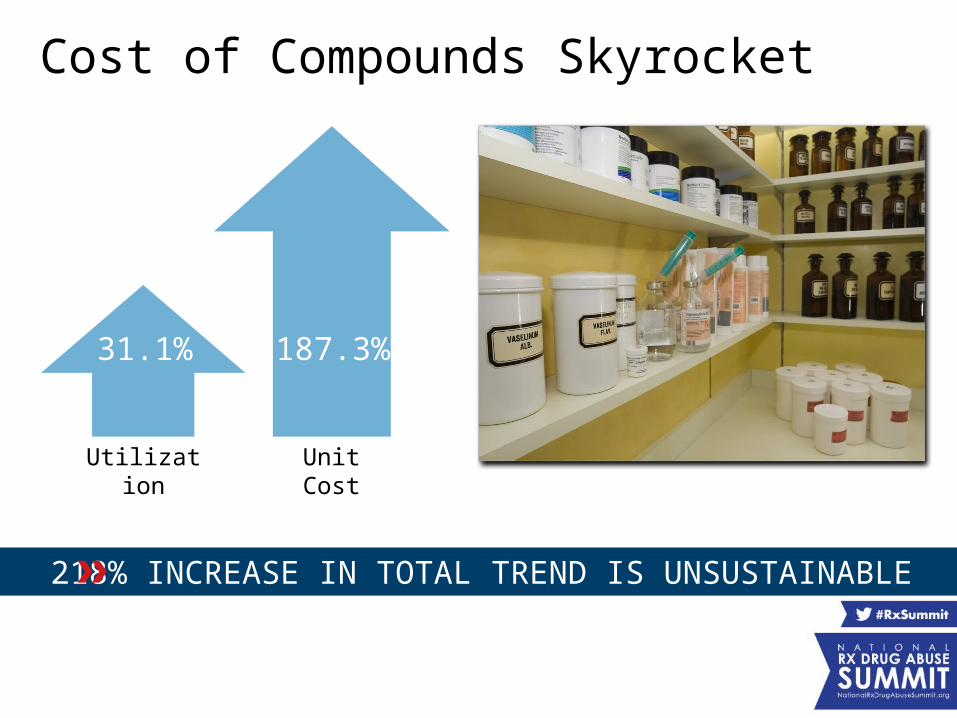
Cost of Compounds Skyrocket
Utilization
Unit Cost
187.3%
31.1%
218% INCREASE IN TOTAL TREND IS UNSUSTAINABLE

OLD
• Only most expensive ingredient submitted
• Coverage based on only most expensive ingredient
• ‘Blind’ summation of all ingredients submitted and paid
COMPOUND CLAIMS PROCESS
NEW
• All ingredients submitted
• Coverage based on all ingredients
• Each ingredient cost must be submitted for reimbursement
• Expanded reject oversight
2011(through 12/31/11)
2012(1/1/12 and
beyond)
A Tale of Unintended Consequences
INCREASING TRANSPARENCY CREATED A DISTURBING TREND

2010 AWP 2011 AWP 2012 AWP 2013 AWP 2014 AWP$0
$10
$20
$30
$40
$50
$60
AWP (Average Wholesale
Price)
1
Two options for pharmacy prescription submission:
Gabapentin
FlurbiprofenKetamine
U&C (Usual and Customary)
2
BULK POWDER MAKERS DRASTICALLY BOOSTED AWP PRICES
Taking Advantage of a Loophole
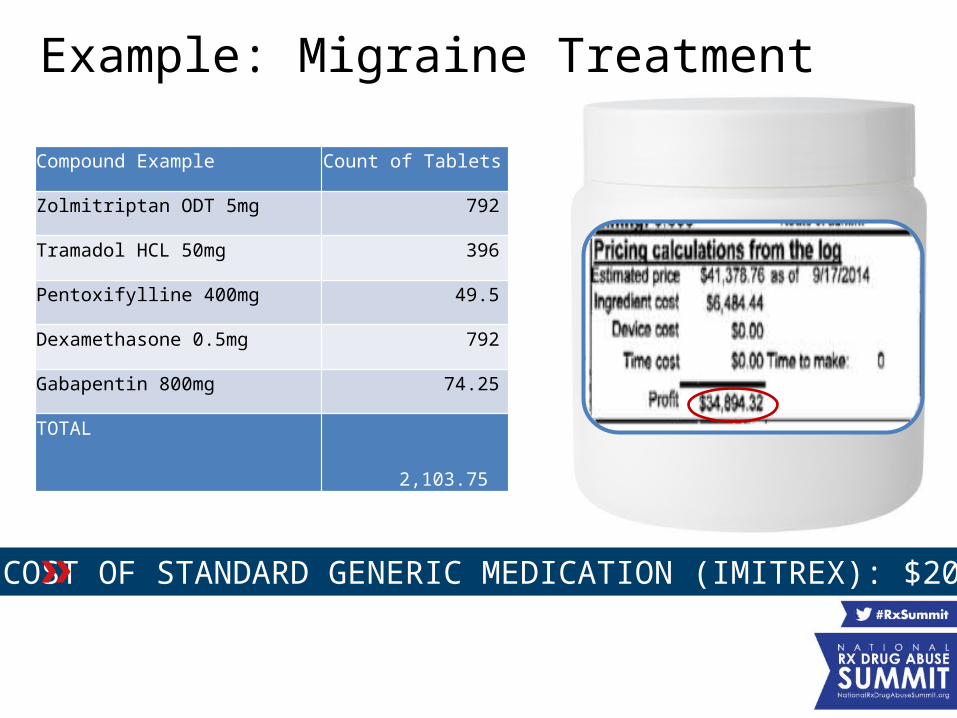
Compound Example Count of Tablets
Zolmitriptan ODT 5mg 792
Tramadol HCL 50mg 396
Pentoxifylline 400mg 49.5
Dexamethasone 0.5mg 792
Gabapentin 800mg 74.25
TOTAL 2,103.75
Example: Migraine Treatment
COST OF STANDARD GENERIC MEDICATION (IMITREX): $20

Using PBM Tools to Eliminate Waste
REDUCING SPEND BY 95% SAVES CLIENTS $2 BILLION THIS YEAR
• Formulary Exclusions: >1,000 bulk powders
• Prior Authorization: Ensuring access for patients who need it
• Dollar Thresholds
• Compound Prescription Limits

New Areas of Focus Emerge
• Sales Force
• Doctor Collusion / Kickbacks
• Tele-Docs
• Co-Pay Waiving
• Coupons
• Tablets vs. Bulk Powders
OUR SOLUTIONS EVOLVE IN RESPONSE TO CHANGING SCHEMES

Takeaways
The right data analytics can spot costly and dangerous issues 1
New threats are constantly emerging2
PBMs are uniquely positioned to identify and prevent fraud, waste and abuse
3

Optimizing Utilization and Outcomes of Urine Drug Testing
Elaine K Jeter, MDPalmetto GBA

Disclosures
Elaine Jeter, MD, has disclosed no relevant, real
or apparent personal or professional financial
relationships with proprietary entities that
produce health care goods and services.

Medicare Administrative Contractors (MACs)
• 10 Jurisdictions – multiple states• 8 Contractors
• Palmetto • Noridian • Novitas • NGS - • WPS• First Coast• CGS• Cahaba

Problems
• Blanket UDT orders • Absent medical record documentation of tests
ordered, results of cup or IA, clinical history• Self-referral testing to maximize reimbursement• Semi-quant IA billed with specific quant codes• Cup testing, followed by IA, referral to partnered
lab arrangement with change of DOS repeat IA and definitive testing
Elizabeth Jeter

UDT Policy
• L35105 – Controlled Substances Monitoring and Drugs of Abuse Testing
• Provides covered indications and testing frequency for:– Symptomatic patients, multiple drug ingestions
and/or patients with unreliable history– Patients with substance abuse or dependence– Patients on chronic opioid therapy


“G” Code Proposal
• HCPCS – quarterly update• Gxxxx – Definitive drug testing by mass
spectroscopy, with confirmation when indicated, >40 drugs, metabolites and illicits; per encounter; includes specimen validity testing (pH, specific gravity, oxidants, creatinine)
• Asked CMS not to recognize existing 21 quant codes and 58 new codes

What Happened to Comprehensive “G” code?
• 2015 CPT drug codes – not adopted by CMS• Palmetto’s G code proposal – not adopted by
CMS• CMS cross-walked 2014 CPT codes to “G” codes• Palmetto issued Coding/Billing Guidelines• Requires short text string in SV101-7 claim field• Created CSPAN text string with # of drugs > 8• Tiered reimbursement: 8-14; 15-34; >35
Third-Party Payer Track
Rx Drugs and Urine Testing:Knowing What’s Too Much, Too Little and Just
Right
Presenters:• Michael Gavin, President, PRIUM• Jo-Ellen Abou Nader, CFE, CIA, CRMA, Senior Director,
Drug Waste Solutions, Express Scripts, Inc.• Elaine Jeter, MD, MolDX Medical Director, Palmetto GBA
Moderator: Daniel Blaney-Koen, JD, Senior Legislative Attorney, American Medical Association Advocacy Resource Center, and Member, Rx Summit National Advisory Board