
Richard M. Frankel, PhD Center for Implementing Evidence Based Practice Roudebush VAMC Professor of...
35
Richard M. Frankel, PhD Center for Implementing Evidence Based Practice Roudebush VAMC Professor of Medicine and Geriatrics Senior Research Scientist Regenstrief Institute Indiana University School of Medicine VIReC Information Seminar December 19, 2006 Clinicia ns Patients Exam Room Computer s The Effect of Computers at the Point of Care: Practical Implications for Physicians and Patients
-
Upload
sabina-stevens -
Category
Documents
-
view
223 -
download
0
Transcript of Richard M. Frankel, PhD Center for Implementing Evidence Based Practice Roudebush VAMC Professor of...

Richard M. Frankel, PhD Center for Implementing Evidence Based Practice
Roudebush VAMCProfessor of Medicine and Geriatrics
Senior Research Scientist Regenstrief Institute
Indiana University School of Medicine
VIReC Information Seminar
December 19, 2006
Clinicians Patients
Exam Room
Computers
The Effect of Computers at the Point of Care: Practical Implications for Physicians
and Patients
2
Today’s Presentation:
• Background and history
• Study Overview
• Findings and Lessons
• Implications

3
Background:
• Clinician-patient relationships central to ambulatory care
• Increasing use of information technology (IT) in health care
• Increasing use of EMRs at the point of care, i.e., the exam room.
• Potential for IT to enhance clinical care• Concerns that IT could create barriers
for the relationship• Limited information on IT effects on
clinician-patient communication

4
Study Question
“How does the presence of a computer in the exam-room
impact communication between patients and
clinicians?”

5

6

7
Stakeholders in the Medical Record 1900
Patient
Recordof
care
Doctor
Doctor’s private notes
_________________________________________________
8
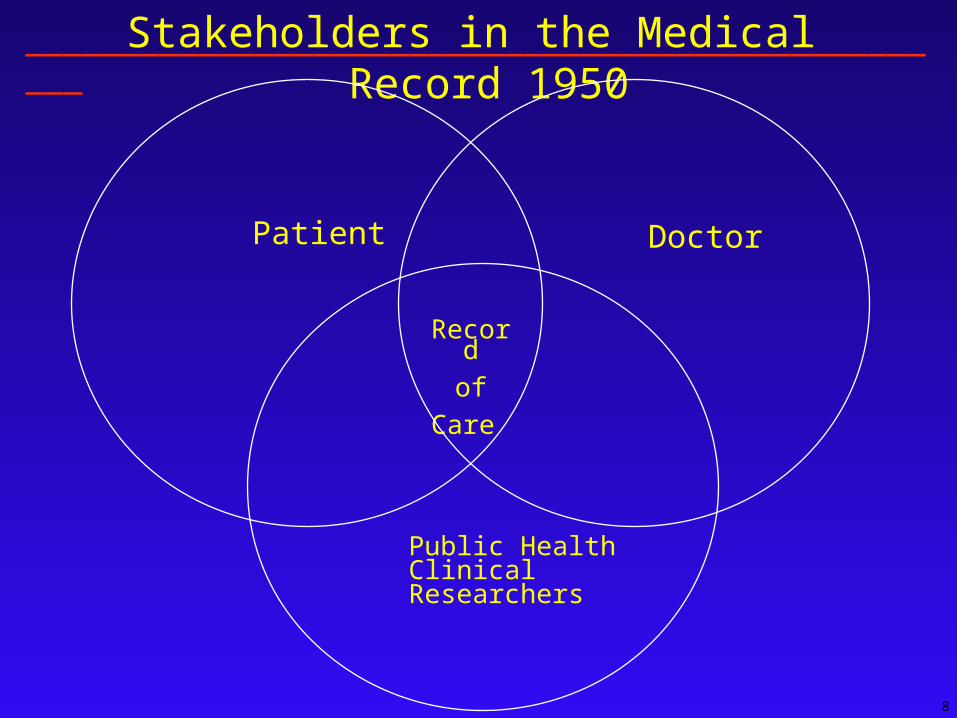
Stakeholders in the Medical Record 1950
Patient
Record
of
Care
Doctor
Public HealthClinical Researchers
__________________________________________________

9
Stakeholders in the Medical Record 2006
Patient
Recordof
care
Doctor
3rd Party Payers Medicare Pt Safety/Quality Health Services Res. Policy Analysts Regulators Hospital Epi.
_________________________________________________

10
The Interaction Study
• Setting: Single outpatient center in a prepaid, integrated delivery system
• Population: – Primary care clinicians at the
clinic– Regularly scheduled patients
• Sample: convenience sample

11
Introduction of Computers
Period 3 Post-Computer:
7 months
Period 2 Post-Computer:
Immediate
Period 1 Pre-Computer
Location: Clinicians’ regular exam-rooms
Design: Longitudinal Video-based Study Three Observation Periods
Analysis: Quantitative Analysis of questionnaires
Qualitative Review of Videotapes
Methods

12
Changes in Patient Visit Satisfaction After the Introduction of the Computer
Patients reporting Excellent or Very Good satisfaction. Differences statistically significant (p<0.05) after adjusting for age, gender, and self-reported health status, based on maximum-likelihood ordered logit model.
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
Period 1 Period 2 Period 3
Clinician's use of medicaltechnologies
Clinician's focus on prevention& health promotion
Patient's participation in themedical care decision

13
Positive Patient Overall Perceptions of the Computer: Significant Improvements Over Time
Patients reporting Strongly Agree or Agree. Differences statistically significant (P<0.05) after adjusting for age, gender, and self-reported health status, based on maximum-likelihood ordered logit model.
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
Overall, I liked the waythe provider used the
computer in today's visit
The way the providerused the computerimproved the overallquality of the visit
The computer helpedthe visit to run in a more
timely manner
Period 2
Period 3

14
Recurrent Patient Confidentiality Concerns
“The use of computers makes me concerned about my privacy”
• 41% Totally Agree or Agreed, immediately after computer introduction• 45% Totally Agree or Agreed, seven months after computer introduction
and six months after training
“Did the Clinician or the medical assistant explicitly discuss the confidentiality of
electronic medical records or data security.”
• 4% Immediately after computer introduction• 0% Seven months after computer introduction and six months after
training

15
Summary of Quantitative Findings
• Overall Patient Satisfaction was very high (88.8%) - No significant changes after the introduction of the computer
• Significant improvements in patient satisfaction with decision-making, clinician’s use of the computer, and focus on prevention after the introduction of the computer
• Patient overall perceptions of the computer were positive with some significant improvement over time
• Patient concerns about the confidentiality of information may not be adequately addressed at present
________________________________________________
16
Qualitative Analysis
• Nine clinicians and 54 visits: two visits per period per clinician
• Variations in computer use across visits in all periods
• Variations in the quality of communication across visits in all periods
• Introduction of the computer appeared to enhance the quality of communication in some visits and created barriers to communication in others

17
Quality of Communication
• Verbal Dialogue: Clinician maintains conversation, even while performing other tasks, e.g. physical exam or typing
• Visual Connection: Clinician maintains eye contact, even while performing visit tasks, e.g. Intermittently glances at the patient while entering data on the computer
• Postural Orientation: Clinician positions head and torso to align with patient and computer, e.g. positions own body and computer screen to avoid excluding the patient

18
Video Coding
• Preliminary Coding Review of tapes by entire research team to
develop initial themes • Major Coding Categories
– Visit organization – Interpersonal skills– Technical mastery skills– Spatial organization
• Coded by 2 Ph.D. qualitative researchers
________________________________________
19
Baseline Visit Organization Skills
Without a computer, not eliciting an agenda can make a visit
• Inefficient• Disorganized• Run over schedule
20
Visit Organization (Baseline/Negative)
In this baseline visit, no formal agenda is set. The patient has multiple medical concerns, including sarcoid. Problems are discussed serially as the patient brings them up and without any indication of how many concerns the patient has, how much time they will take to discuss and how they might be related. The visit appears quite inefficient and poorly organized
________________________________________________

21
Amplification Effect
Previous baseline skills may affect how exam room computers are used and the extent to which they facilitate or create additional barriers to clinician patient communication.
___________________________________________

22
Amplification of Visit Organization Skills (Post
introduction) The same clinician seems to get confused
between patient agenda items and information on the computer screen. Each time the computer is consulted current problems are deferred and are dealt with some time later, confusing the patient. The presence of the computer multiplies the sense of disorganization, and extends the length of the visit. The clinician also seems to get lost in a maze of windows while looking for a test result and at times inquires about items the MA has already checked on.
_______________________________________________

23
Interpersonal Skills
Clinicians with good interpersonal skills
• Encourage patient input• Listen to patients’ concerns • Maintain eye contact• Chart intermittently or not at all during visit

24
Amplification of Interpersonal Skills (Positive)
Increased Quality of Communication• The computer served as another tool to help
the clinician communicate or remain more familiar with the patient
• The net computer effect was a higher quality of clinician-patient communication:- More verbal dialogue about the patient’s
problems- Enhanced visual interaction - shared
review of information on the computer- Continued clinician physical alignment
with the patient, e.g. tilting the screen so both can see

25
Interpersonal Skills (Baseline/ Positive)
During this Period 1 visit, the clinician sits
on a low stool across from the patient and
maintains gaze focused on the patient when
speaking. Information is entered onto the paper chart intermittently and only when the patient has finished speaking.
________________________________________________

26
Amplification of Interpersonal Skills (Post
Introduction/Positive) The same clinician sees a patient in Period
2, who comes in after several ER visits for panic attacks. The clinician notices that the patient is on a medication known to cause similar symptoms and tells her that it may not be appropriate for her, all the while tilting the computer screen so that they can both review the notes. The clinician then reinforces and amplifies the message by pushing away the computer screen establishing eye contact and explaining the drug’s paradoxical effects to the patient.
____________________________________________

27
Technical Skills
Inability to successfully navigate program leads
to:
• Inability to access data consistently• Wastes of time• Frustration for clinicians and patients

28
Technical Skills Post Introduction/Negative
In this visit the clinician is looking for recent medical hx using the computer. The patient tries to tell the clinician, who is busy on the computer, that she has a list of meds but it is to no avail. She succeeds in her 2nd try and the clinician takes the list and starts copying the information to a paper chart that will have to be typed back into the computer at a later point. Both clinician and patient seem frustrated with the process which takes a long time to complete.
____________________________________________________

29
Spatial Organization of the Visit

30
Re-enactment: Clinician and Patient Using the Computer Together

31
Re-enactment: The Computer Creating a Barrier to Communication

32
Summary• Variations in computer use and the quality of
clinician-patient communication during visits
• Digital Amplification: Computer use could increase or decrease the quality of communication between clinicians and patients
• Key Factors Modifying the Computer Effects:– Visit Organization– Interpersonal Skills– Technical Computer Skills– Spatial Orientation

33
Limitations
• Small, convenience sample • Primary care visits only• Normative measures of communication
quality• Qualitative analyses only• Single clinic within a prepaid, integrated
delivery system• Experience during initial seven months after
the introduction of computers into the exam-room

34
Implications
• Use of computers has the potential to increase or decrease the quality of clinician-patient communication
• Four factors appear to influence the direction of this digital amplification
• More research is needed to understand the potential impact of IT innovations on the clinician-patient relationship
• Guidelines and training programs could help clinicians use the new technology more effectively

35
Thank you for your time and attention !


















