
Review article - hu-berlin.de
14
Manzke, Morbidity in breech presentation 127 Review article J.Perinat. Med. 6(1978)127 Morbidity among infants born in breech presentation H. Manzke Department of Pediatrics, University Hospital, Kiel l Causes of breech presentation Breech presentation and breech delivery are more hazardous for the fetus than cephalic ones. The failure of vertex positioning during the last 3 months of pregnancy may be due to a variety of disturbances such äs uterine anomalies, contracted pelvis, cornual-fundal Implantation of the placenta, abnormally short umbilical cord [54], oligohydram- nios and pelvic tumors [19, 39, 51], The higher incidence of breech presentation among preterm infants is caused by the lie of the fetus, which is not stabilized, until the beginning of the third trimester of pregnancy due to the relatively large volume of amniotic fluid. Correspondingly breech delivery is found more often in infants with poly- hydramnios. In twin pregnancies at term, one infant often lies in cephalic, the other one in breech presentation. This combination can be assumed to be the best form of adaptation to the uterine cavity for twins. LAW (cited by [19]) showed that the legs of the fetus were extended in 74% of primiparous breech presentations, while the figure formultiparae was only 55%. The differ- ences can be related to the affect which the unstretched abdominal and uterine walls may have on the uterine cavity in first pregnancies. For the same reason breech presentations occur more frequently with primiparae than with multiparae [14, 35]. In some cases fetal abnormalities favour breech presentation, for instance, in infants with spina bifida (paralyzed legs) or with malformations of the lower extremities. Congenital malformations have been found almost three times äs often in breech deliveries [12, 31]. Neuromuscular dys- function may limit the ability of the fetus to Curriculum vitae HERMANN MANZKE, born 1933 in Stettin. Studies of medicine at the Universities of Kiel and Freiburg 1953-1958. Doktor of Medicine 1959. Rotating Internship 1959- 1960. Assistant Resident at the University Hospital of Gynecology and Ob- stetrics in Kiel 1961- 1962. Member of the staff at the University Hospital for Children in Kiel since 1963. Qualification äs Privatdozent 1970, apl Professor 1975. Primary research interests: perinatal Medicine, respiratory physiology, purine metabolism, roentgenology. assume vertex position. In a brief communication entitled "Breech presentation äs an indicator of fetal abnormality", BRAUN et al. [11] list eleven morphologic syndromes which are associated with an increased incidence of breech presentation. Most of these are rare, but some are relatively common: e.g. embryofetal-alcohol syndrome or 21-trisomie syndrome. Therefore, when a term infant is born by breech presentation, the reasons why the fetus failed to take the vertex position should always be sought because these reasons may include morphogenetic and/or functional disturb- ances of the fetus. The important point here is that a particular pathology need not be caused by breech delivery. And in such a case it might be unwarranted to give preference to abdominal delivery in an attempt to eliminate that risk of brain damage which is associated with vaginal birth[34]. J.Perinat. Med. 6 (1978)
Transcript of Review article - hu-berlin.de

Manzke, Morbidity in breech presentation 127
Review article
J.Perinat. Med.6(1978)127
Morbidity among infants born in breech presentation
H. Manzke
Department of Pediatrics, University Hospital, Kiel
l Causes of breech presentationBreech presentation and breech delivery are morehazardous for the fetus than cephalic ones. Thefailure of vertex positioning during the last 3months of pregnancy may be due to a variety ofdisturbances such äs uterine anomalies, contractedpelvis, cornual-fundal Implantation of the placenta,abnormally short umbilical cord [54], oligohydram-nios and pelvic tumors [19, 39, 51], The higherincidence of breech presentation among preterminfants is caused by the lie of the fetus, which isnot stabilized, until the beginning of the thirdtrimester of pregnancy due to the relatively largevolume of amniotic fluid. Correspondingly breechdelivery is found more often in infants with poly-hydramnios. In twin pregnancies at term, oneinfant often lies in cephalic, the other one inbreech presentation. This combination can beassumed to be the best form of adaptation to theuterine cavity for twins. LAW (cited by [19])showed that the legs of the fetus were extended in74% of primiparous breech presentations, whilethe figure formultiparae was only 55%. The differ-ences can be related to the affect which theunstretched abdominal and uterine walls mayhave on the uterine cavity in first pregnancies. Forthe same reason breech presentations occur morefrequently with primiparae than with multiparae[14, 35]. In some cases fetal abnormalities favourbreech presentation, for instance, in infants withspina bifida (paralyzed legs) or with malformationsof the lower extremities. Congenital malformationshave been found almost three times äs often inbreech deliveries [12, 31]. Neuromuscular dys-function may limit the ability of the fetus to
Curriculum vitaeHERMANN MANZKE,born 1933 in Stettin.Studies of medicine at theUniversities of Kiel andFreiburg 1953-1958.Doktor of Medicine 1959.Rotating Internship 1959-1960. Assistant Residentat the University Hospitalof Gynecology and Ob-stetrics in Kiel 1961-1962. Member of the staffat the University Hospitalfor Children in Kiel since1963. Qualification äs Privatdozent 1970, apl Professor1975. Primary research interests: perinatal Medicine,respiratory physiology, purine metabolism, roentgenology.
assume vertex position. In a brief communicationentitled "Breech presentation äs an indicator offetal abnormality", BRAUN et al. [11] list elevenmorphologic syndromes which are associated withan increased incidence of breech presentation.Most of these are rare, but some are relativelycommon: e.g. embryofetal-alcohol syndrome or21-trisomie syndrome. Therefore, when a terminfant is born by breech presentation, the reasonswhy the fetus failed to take the vertex positionshould always be sought because these reasons mayinclude morphogenetic and/or functional disturb-ances of the fetus. The important point here isthat a particular pathology need not be caused bybreech delivery. And in such a case it might beunwarranted to give preference to abdominaldelivery in an attempt to eliminate that risk ofbrain damage which is associated with vaginalbirth[34].
J.Perinat. Med. 6 (1978)

128 Manzke, Morbidity in breech presentation
2 Perus associated with breech delivery
The causes are well known. During the beginningof the labor the umbilical cord can prolapse andbecome compressed (2.5% in [53]; 5.4% in [12]).Even without prolapse the hazard of cord com-pression is increased because the abdomen andthe cord enter the narrow confines of the birthcanal earlier than they do in cephalic deliveriesand are subject to abnormal pressures through theentire period when ehest, shoulders, and head passthe pelvic inlet. The placentamay begin to separatewhen the uterus Starts to empty. Complications ofabruptio placentae are significantly more frequentwith breech (6.0%) than with non-breech deliveries(l .8 %) [ 12]. Both situations make it more probablethat the breech infant will be born more deeply .axsphyxiated than the cephalic one.The mechanical difficulties concern the delivery ofthe shoulders and the arms äs well äs the deliveryof the aftercoming head. Among infants withbrachial plexus palsy those born by breech present-ation outnumber those born in cephalic present-ation by 3 to l [16]. When the injury includes thephrenic nerve, paralysis of the diaphragma mayproduce respiratory disorders. Besides, respirationdistress syndromes are mostly due to aspirationand meconium pneumonitis. In preterm infantsprolonged asphyxia often is followed by the idio-pathic respiratory distress syndrome (hyalinemembrane disease) and/or by massive pulmonaryhaemorrhage. According to the literature [54]approximately 30% of the breech bom infants areprematures. Nearly 20% of the stülbirths aredelivered in breech presentation [53].Cephalhematoma are equally frequent with breechborn and vertex born infants. Approximately 25%of such caseshave anunderlying linear or depressedskull fracture [7,-32, 40]. Only rarely do theycombine with subdural hematoma [1]. Claviculafracture, hematoma in the midportion of the ster-nocleidomastoid muscle (torticollis), and dysplasiaor dislocation of the hip-joint [3, 53] are consid-erably more frequent with breech born infants.FETTWEIS [23] found that congenital dislocationof the hip is ab out 9 times more frequent withinfants with breech presentation than with headpresentation. He could also show that this mal-formation involves only infants with extended legs.
BARLOW [3] reports congenital hip displasia in20% of all infants with breech/presentations.Testicular birth trauma was found in 10% of themale breech delivered infants. It is not yet possibleto state whether, or how often sterility througha permanent damage of the testes may result [18].RÄüs [44] describes severely damaged testicleswithin the inguinal canal in two cases.Traction on the hyperextended spine of the infantwith the head fixed in the maternal pelvis maylead to a long opisthotonus position, which canoften be noted with infants after breech delivery(own observations). Severe spinal cord injuries arerare and they usually cause death soon after birth[5]. Fractures of the humerus and injuries of thehumeral epiphysis in freeing the arms have becomerare. Breech extraction in footlings or breech pre-sentation with version and extraction may causecharacteristic meta-epiphyseal lesions and periostealelevation in the lower extremities [37, 51]. Theselesions take care of themselves unless they areassociated with any Separation or dislocation ofthe epiphysis. Prolonged abductiön of the hipinvolves sustained traction of the obturator nervebetween the points of flxation at the knee jointand the pubic ramus. Fortunately, the palsy of theadductor and the internal rotator muscles dis-appears within a few weeks after birth [15].Although the aetiology of the hypopituitarydwarfism is uncertain, a number of authors [6, 45,56] assume that perinatal lesions of the pituitarystalk may be a major factor. BIERICH [6] and VANDER WERFF TEN BOSCH [56] state that nearly twothirds of their patients were born in breech pre-sentation. It is easy to see how the hypophysismay get injured: the head of the breech deliveredinfant will be subjected t o extremely strongvariations of pressure. In particular, these patho-mechanical forces lead to strains between the basisof the brain and the hypophysis.Brain damage is the most common cause of deathwith breech born infants. Frequently, intracranial1
haemorrhage was found in post-mortem examin-ations, namely 50% [9], 48% [44], 35% [46]-These figures include both damage due to as-phyxia and mechanical trauma. It seems, that interm infants there is a prevalence of mechanicalfactors. But, without doubt, prematurity may
J. Perinat. Med. 6 (1978)
Manzke, Morbidity in breech presentation 129
also play an important role with preterm infantsbecause the fragility of the vessels and the immat-urity of the organs, including the brain itself,predisposes to bleeding.RÄLts [44] in his study of the birth trauma tomuscles in babies born by breech deliveiy em-phasizes the fetal combination of extensive muscledamage, crush-syndrome, haemorrhagic shock, anddisseminated intravascular coagulation.Whether adrenal haemorrhage in breech borninfants is due to trauma, anoxia, or severe stress,is unknown. X-rays showing calcified centralhaematoma of the adrenal in older infants suggestthat not all adrenal haemorrhages lead to death[40] (own observation).In summary, most injuries of the sceletal and ofthe peripheral nervous System restitute ad inte-grum. Damages to the internal organs and to thebrain are fatal. In order to answer the question ofhow often latent brain injuries may occur and towhat extent they may be reversible, follow-upstudies examining the psychomotoric developmentof high risk infants should be of particular interest.
3 Critical remarks on the validity of follow-upstudies in breech born infants
Quite a number of follow-up studies have alreadybeen done on breech born infants. However, onlya few of them hold up to critical evaluation. It isnot surprising therefore that the results of thesestudies vary considerably, for instance, someresearchers [8, 25, 27, 30, 34, 43, 48] predictfavorable developments for breech born infants,others [9, 21, 24, 42, 47, 50,55] suggest unfavor-able ones. Unfortunately, all of these follow-upstudies have serious shortcomings. The mostimportant are:I.Most of these studies proceed retrospectively.
Exceptions are BERENDES [4], NELIGAN [43],and our own work (see below), which continuesthe German prospective study "Schwanger-schaftsverlauf und Kindesentwicklung". Themain weakness of retrospective studies is thatthe researcher has to depend on records thatare neither complete nor consistent. Worst ofall, he has to depend on the memory of theparents, which increases the uncertainty [36].
Those follow-up studies which base theirevaluation solely on questionnaires have prod-uced, in general, more favorable results thanthose that also include neurological and psycho-metric examinations. Prospective investigationssufficiently broad in scope have the ad van tageof permitting the simultaneous study of manydifferent complications äs well äs the inter-relationship of each with other aetiological orassociated factors [4].
2. The number of cases is too small and the areafrom which they are drawn is too restricted.Consequently, such results are not represent-ative. But even the large follow-up studies donot provide enough cases for subdividing thechildren into those born in frank, in complete,or in incomplete breech presentation, in foot-ling and in knee presentation. Such a sub-grouping is all the more important since it iswell known that the last two varieties correlatewith a higher mortality rate than the first threenamed. No study is available in which the long-term prognosis for the vaginally breechborninfants is given separately according to the ob-stetrical type of delivery. Furthermore, thereare äs yet no reports ab out the advantages anddisadvantages of the cephalic version which isagain attracting a lot of attention.
3. Most follow-up studies do not bother to providecontrol groups. For instance, in studies onspastic children and on children with learningdisabflity one tends to find a significantly higherProportion of breech delivered infants. If suchvariables äs prematurity, twins, or anomaliesof the placenta, are not taken into accountseparately, theri the overall longterm predictionsfor breech born infants will be much more un-favorable. This, however, need not be associatedexclusively with difficulties due to the mechanicsof the delivery itself.
4. In general, the follow-up investigations arecarried out only once and almost exclusivelyduring infancy. As a rule, the methodologyhas been rather crude. However, minor disabili-ties may not become evident until the childreaches school age. On the other hand initialretardations may have been overcome before thechild enters school. In order to detect more
J.Perinat.Med.6 (1978)

130 Manzke, Morbidity in breech presentation
^
s1Cv{IH
JJ|J
(«HO
1I
Com
men
ts
GO
0 ^
Sf§0(D
^
0)
'SOIH«
P«
o 2j\0 ^h ίί
o2.Soco
s
osco
rt
3*0 '•SiT? g
II
Aut
hors
Phys
ical
ex
amin
atio
n (+
EEG
in
case
of
ne
ed)
of
176
bree
chde
liver
ed i
nfan
ts a
nd 1
10 c
ontro
ls
^5
^^00
^
04»-H
1vo
1
co
*oi
t^* f»— 1
10vo0*Ή.
13
Z1
Cat
amne
stic
rev
iew
+ E
EG. F
ocal
chan
ges
afte
r br
eech
de
liver
y6.
2%, n
on-b
reec
h de
liver
y (S
ectio
caes
.) 3.
7%
^ee
rH 'S
S
^90
£t—)
1
Q
00«o
fτί
*o1
C" ·^"a\
00vo
13'S
o
Que
stion
naire
s to
te
ache
rs.
Per-
cent
ages
re
fer
to
lear
ning
di
ffi-
culti
es.
Lorg
e-Th
ornd
ike
inte
lli-
genc
e te
st s
how
ed n
o sig
nific
ant
diffe
renc
es00
»0
r.
t
σ\
1
1
vo«oσ\
r^^|^"^
cd
MU
LLER
1106
que
stio
nnai
res
answ
ered
by
pare
nts
and
teac
hers
. Pe
rcen
tage
sre
fer t
o le
arni
ng h
andi
caps
voi-H
^»c^»o
vorHl«O
0vq^
gies ζ^
0>vo1
vo»oONT— (
iS0\
FIANU
l!
Brit
ish
Nat
iona
l Ch
ild
Dev
elop
-m
ent S
tudy
. Edu
catio
nal,
med
ical
,an
d so
cial
Inf
orm
atio
n.
/—scou
2£
0^^00
β
^
1
T-H
1 C
00«o
*o
«-H
BUTL
ER
Que
stion
naire
s an
swer
ed b
y pa
r-en
ts.
260
infa
nts
of w
hich
6 w
ere
men
tally
re
tard
ed,
1 ce
rebr
alpa
lsy.
8 in
fant
s ha
d co
ng.
hip
disl
ocat
ion
1
Q«**»rr.
>,»o|0
^O»-H
^
Γ*VO
100«o0\
etMcoH^rS0«
SINDE
R <
/**v
6
vorH
Surv
ey o
f se
vera
l sc
hool
s. Q
uota
of
bree
chbo
rn
with
in
spas
tics
15.4
%.
With
in c
olle
ctiv
e or
con-
trol
pupi
ls 4
.6%
. N
o sig
nific
ant
quot
as
amon
g th
e pu
pils
w
ithle
arni
ng
diff
icul
ties
and
with
1
1
^»H1vo
1
1
vovo1
00«oON
n-SN**]
2 S
HGQCO
men
tal d
efec
ts
J.Perinat.Med. 6(1978)
Manzke, Morbid ity in breech piesentation 131
l«O
J«O
CNl: oo
CN
vo
tΉ
ro
«s«o
· vb
?sOH
J^k.
NEL
IGA
N 1
!
TovoON
rHc*·rH
G BE
L et
al
·i
fOvo
fOOS
co2
ALEX
OPOX
J
o7irH
«βS{•< s
HO
HLW
EG4
WILL
ARD
l!
«o1
«NJT*
r*r*2•s
HO
CH
ULi
et
7CMr-ov
LA
0>
HIL
Let
aLl
7o*•**H
9O
MANZ
KE 19
I'SIδ8u1So1
i11
J,Perinat.Med.6(1978)
132 Manzke, Morbidity in breech presentation
subtile differences standardized psychometricand neurological-motoscopic tests have to beapplied. The application of such tests is easierand the results tend to be more reliable äs afunction of increasing age of the children. Itseems that this is the only way to single outthose children with minimal cerebral dysfunct-ion. Surely, such children can be expected to bemore numerous than those with clinically detect-able abnormalities.The advantage of prospective longterm invest-igations is to allow for more exact researchplanning. But, the disadvantage is that they trauad hoc statistics by at least a few years. Theresults of shortterm changes relating to newobstetric methods can be investigated onlymuch later.
4 General Statements
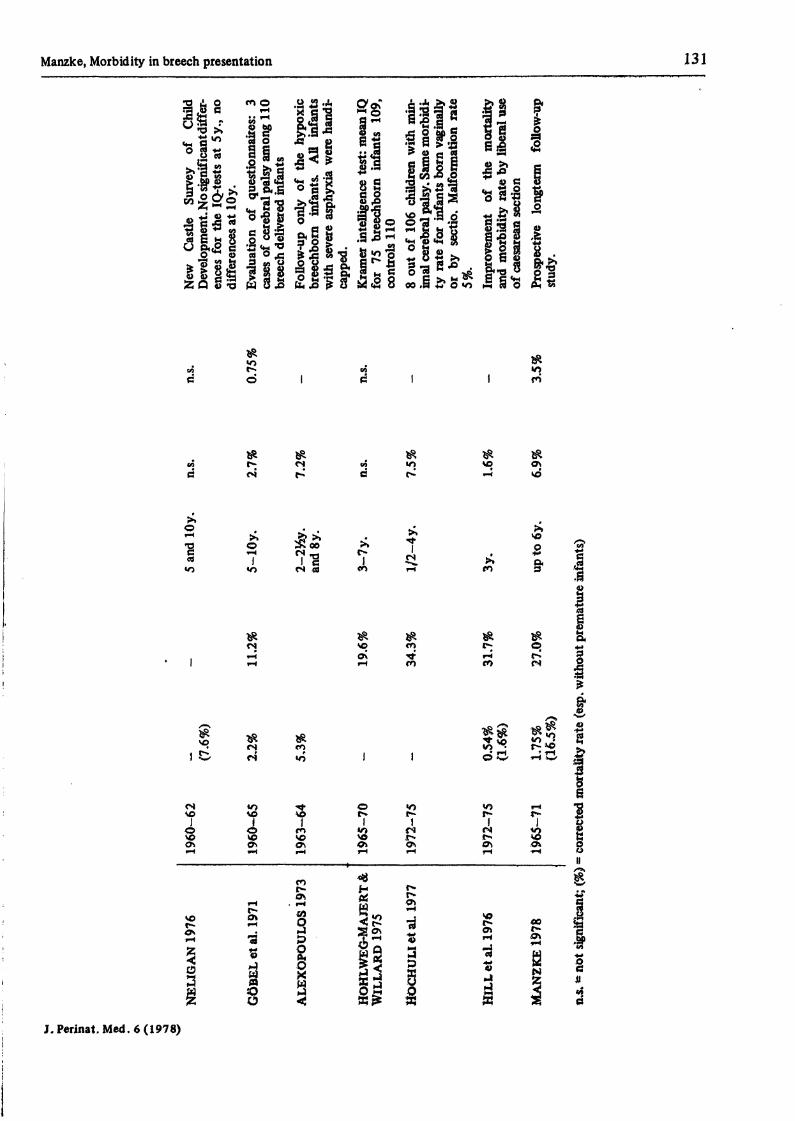
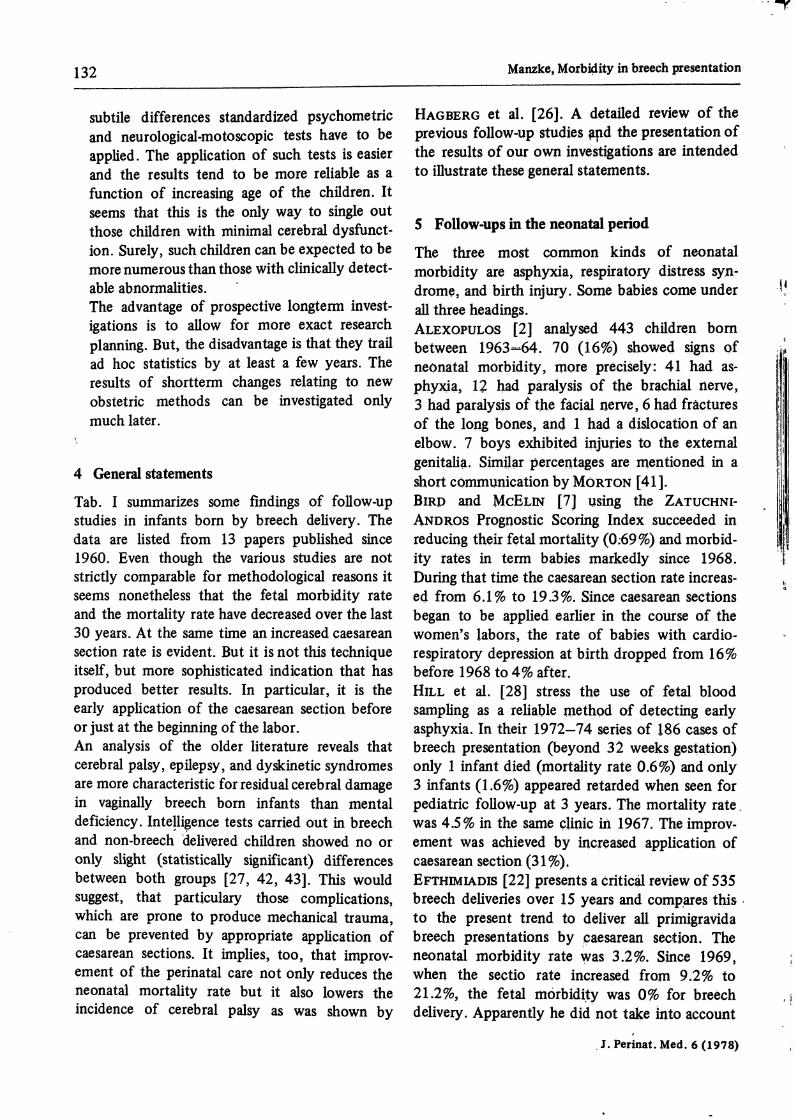
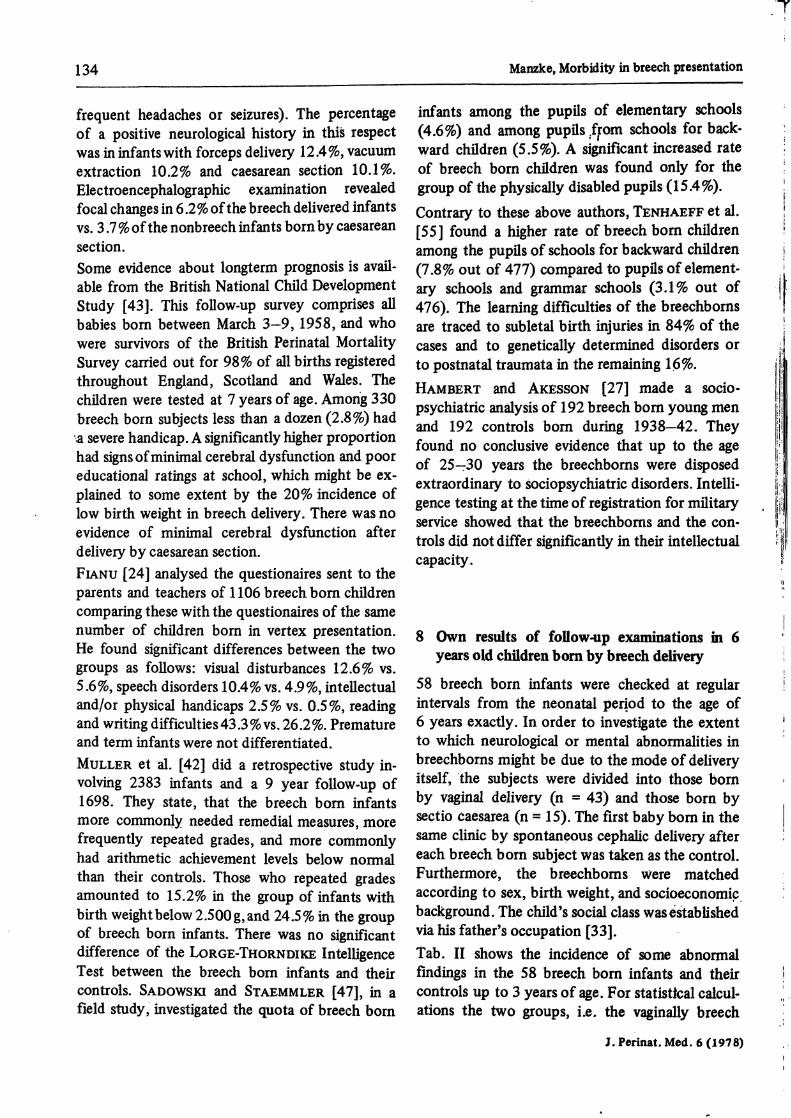
Tab. I summarizes some findings of follow-upstudies in infants born by breech delivery. Thedata are listed from 13 papers published since1960. Even though the various studies are notstrictly comparable for methodological reasons itseems nonetheless that the fetal morbidity rateand the mortality rate have decreased over the last30 years. At the same time an increased caesareansection rate is evident. But it is not this techniqueitself, but more sophisticated indication that hasproduced better results. In particular, it is theearly application of the caesarean section beforeor just at the beginning of the labor.An analysis of the older literature reveals thatcerebral palsy, epilepsy, and dyskinetic syndromesare more characteristic for residual cerebral damagein vaginally breech born infants than mentaldeficiency. Intelligence tests carried out in breechand non-breech delivered children showed no oronly slight (statistically significant) differencesbetween both groups [27, 42, 43]. This wouldsuggest, that particulary those complications,which are prone to produce mechanical trauma,can be prevented by appropriate application ofcaesarean sections. It implies, too, that improv-ement of the perinatal care not only reduces theneonatal mortality rate but it also lowers theincidence of cerebral palsy äs was shown by
HAGBERG et al. [26]. A detailed review of theprevious follow-up studies ?nd the presentation ofthe results of our own investigations are intendedto illustrate these general Statements.
5 Follow-ups in the neonatal period
The three most common kinds of neonatalmorbidity are asphyxia, respiratory distress syn-drome, and birth injury. Some babies come underall three headings.ALEXOPÜLÖS [2] analysed 443 children bornbetween 1963-64. 70 (16%) showed signs ofneonatal morbidity, more precisely: 41 had as-phyxia, 12 had päralysis of the brachial nerve,3 had päralysis of the fäciäl nerve, 6 had fräcturesof the long bönes, and l had a dislocation of anelbow. 7 boys exhibited injuries to the externalgenitalia. Similar percentages are mentiöned in ashort cömmunication by MÖRTON [41].BIRD and McELiN [7] using the ZATUCHNI-ANDROS Prognöstic Scoring Index succeeded inreducing their fetal mortality (0.69%) and morbid-ity rates in term babies markedly since 1968.During that time the caesarean section rate increas-ed from 6.1% to 19.3%. Since caesarean sectionsbegan to be applied earlier in the course of thewomen's labors, the rate of babies with cardio-respiratory depression at birth dropped from 16%before 1968 to 4% after.HILL et al. [28] stress the use of fetal bloodsampling äs a reliable method of detecting earlyasphyxia. In their 1972-74 series of 186 cases ofbreech presentation (beyond 32 weeks gestation)only l infant died (mortality rate 0.6%) and only3 infants (1.6%) appeared retarded when seen forpediatric follow-up at 3 years. The mortality rate.was 4.5% in the same clinic in 1967. The improv-ement was achieved by increased application ofcaesarean section (31%).EFTHIMIADIS [22] presents a criticäl review of 535breech deliveries over 15 years and compares thisto the present trend to deliver all primigravidabreech presentations by caesarean section. Theneonatal morbidity rate was 3.2%. Since 1969,when the sectio rate increased from 9.2% to21.2%, the fetal morbidity was 0% for breechdelivery. Apparently he did not take into account
J.Perinat.Med. 6(1978)

Manzke, Morbidity in breech presentation 133
asphyxia and respiratory distress syndrome ässometimes unavoidable complications also incaesarean section.HOCHULI et al. [29] used routine X-ray pelvimetryin breech, ultrasound fetal cephalometry andthoracometry to determine whether a caesareansection was called for. They point out that underthese circumstances there is no difference in themortality and morbidity rates in infants with breechpresentationsborn vaginally or by caesarean section.Their sectio rate was 34.3%. They note, further-more, that the delivery of an infant in breechpresentation can also be difficult and füll of risksif done by caesarean section. Among 106 breechinfants during the years 1972-75 8 infants (7.5%)were retarded or they showed signs of minimalcerebral palsy.
6 Follow-ups during infancy and preschool period
BERENDES [4] outlines the examination results ofthe children in the US Collaborative PerinatalProject. The findings are based on a comprehen-sive neurological examination at the age of l year.In children whose birth weight was less than2.501 g the abnormality rate (10%) was twice thatof the non-breech delivered children. Among thosewhose birth weight exceeded 2.500 g, however,there was no difference between the breech andnon-breech groups äs far äs the proportions ofabnormals (l .8%) were concerned.HOHLWEG-MAJERT and WILLARD [30] likewisedid not find any significant differences at the IQ-values between a group of 75 breech delivered and71 non-breech'delivered infants examined at theage of 3 to 7 years. The mean IQ was 109 and110, respectively (KRAMER-Intelligence Test).NELIGAN [43] attempted to assess the developmentof all children born to mothers in NewCastle uponTyne during the years 1960—62. He found no ex-cess of gross, but a doubtful excess of mild neuro-logical abnormalities attributableto breech delivery.In both tests at the age of 5 years (GoodenoughDraw-a-Man test and Figure Copying score, BINET)the scores for breech delivered boys were signif-icantly depressed, whereas those of the girls werenot at all depressed, äs compared with those bornspontaneously by vertex presentation. Further-
more, the depression of IQ was striking in thegroup of the heavier breech born infants whichvery likely may be the result of mechanical diff-iculties during delivery.But the differences in the mean IQ-values withinall groups compared with each other were slight.The analysis of variance revealed äs significantcontributory factors the number of previouspregnancies, the birth weight, and the occupationalsocial class. Reassessment of the children at theage of 10 years by somewhat more sophisticatedtests showed such slight differences between thebreech and non-breech delivered children, that nostatistical tests were carried out.SINDER and WENTSLER [53] evaluated questionairessent to the parents. Among 260 breech deliveredinfants 6 were mentally retarded,and l had cerebralpalsy (morbidity rate 2.7%). Sinfantshadcongenitalhip dislocations. 20.1% of the breech babies werepremature.SANO et al. [48] studied the relationship betweenthe mental development quotient (DQ) and modesof delivery in one year oldinfants born in 1971—74.But they did not find any significant differences.The average value of DQ was 111.1 in 56 infantsborn by caesarean section, 109.7 in 67 infantsborn with vacuum extraction, 117.0 in 3 infantsdelivered with forceps Operation and 110.4in 48 infants delivered with breech extraction.Likewise within the group of infants with DQ under90 there were no differences correlating with thevarious modes of delivery.TALLIAN et al. [54] re-examined 176 breech bornchildren with normal birth weight at ages 6—12years. If needed an EEG was recorded. It wasfound that the incidence of mental deficiency andneurological abnormality was twice äs high äs in acontrol group of 110 children born spontaneouslyin vertex position.
7 Follow-ups in school period and af ter
In the catamnestical histories of 339 breech borninfants reviewed at the age of 4—14 years BOLTEet al. [9] considered 20.0% of their subjects neuro-logically abnormal (for example, delay in somaticor psychic development, cerebral palsy, ataxia,
J.Perinat.Med.6(1978)
134 Manzke, Morbidity in breech presentation
frequent headaches or seizures). The percentage infants among the pupüs of elementary schoolsof a positive neurological history in this respect (4.6%) and among pupüs from schools for back-was in infants with forceps delivery 12.4%, vacuum ward chüdren (5.5%). A significant increased rateextraction 10.2% and caesarean section 10.1%. of breech born chfldren was found only for theElectroencephalographic examination revealed group of the physically disabled pupfls (15.4 %).focal changes in 6.2% of the breech delivered infants contrary to these above authors, TENHAEFF et al.vs. 3.7 %of the nonbreech infants born by caesarean j55j found a her rate of breech born childrensection. among the pupüs of schools for backward chüdrenSome evidence about longterm prognosis is avail- (7.8% out of 477) compared to pupüs of element-able from the British National Chfld Development ^y schools and grammar schools (3.1% out ofStudy [43]. This follow-up survey comprises all 475). The learning difficulties of the breechbornsbabies bom between March 3-9, 1958, and who traced to subletal birth injuries in 84% of thewere survivors of the British Perinatal Mortality cases to genetically determined disorders orSurvey carried out for 98% of all births registered to postnatal traumata in the remaining 16%.throughout England, Scotland and Wales. The HAMB£RT md AKESSQN {27] made g sodo.chüdren were tested at 7 years of age. Among; 330 ^^ is of 192 breech bom menbreech born subjects less than a dozen (2.8%) had ^ controls bom 1938_42. Theya severe handicap. A significantly higher proportion found nQ condusive evidence to thehad signsofminimal cerebral dysfunction andIpoor rf 25_3Q ^ breechboms were di d
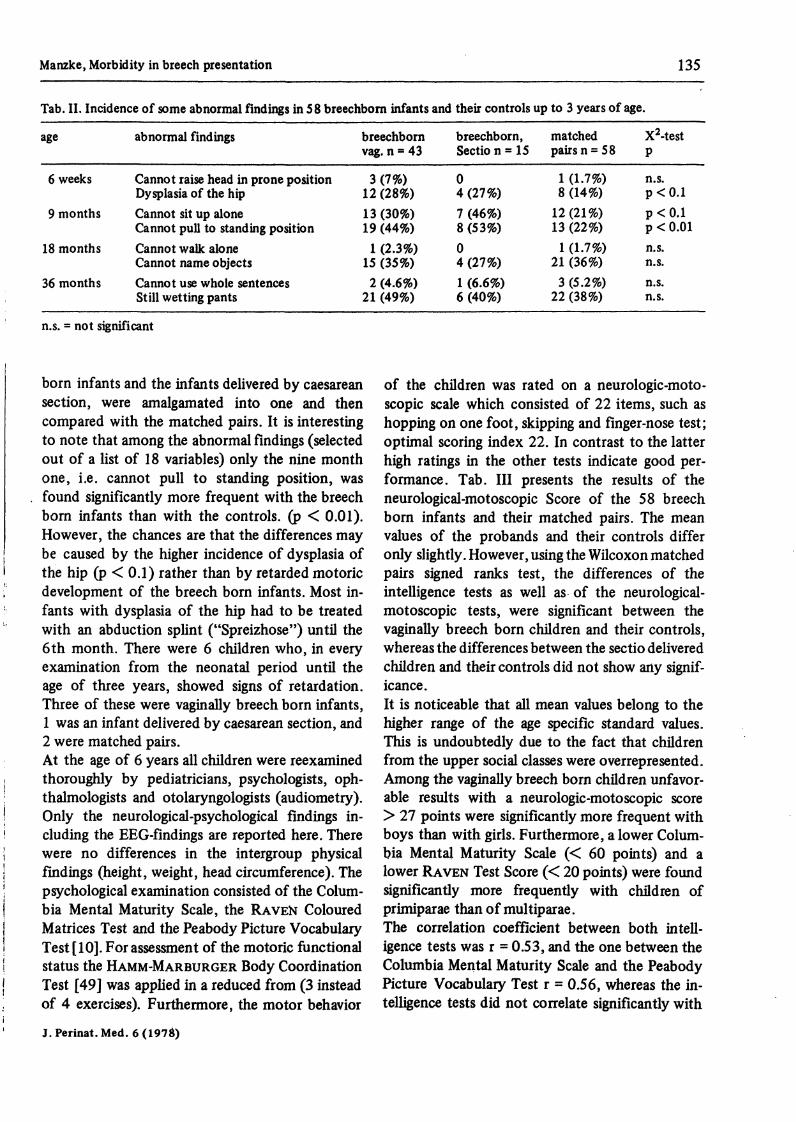
educational ratings at school which might be ex- extraordinary to ^™ disorders. Intelli- 'plained to some extent by the 20% incidence of ^ Qf Qn fof mlow birth weight in breech dehvery There was no ^^ ^ breechboms ma the con. 'evidence of minimal cerebral dysfunction arter , * . , Jvrr ...-. ,t . .* . . . „ , t, ,. f . trols did notdiffer significantly m their intellectualdelivery by caesarean section. .FIANU [24] analysed the questionaires sent to theparents and teachers of 1106 breech born childrencomparing these with the questionaires of the samenumber of chüdren born in vertex presentation. 8 ^ resuhs of follow^p examinations in 6He found significant differences between the two years old chfldren bom by breech deüverygroups äs follows: visual disturbances 12.6% vs.5.6%, speechdisorders 10.4% vs. 4.9%, intellectual 58 breech born infants were checked at regulärand/or physical handicaps 2.5% vs. 0.5%, reading intervals from the neonatal penod to the age ofand writing difficulties43.3%vs. 26.2%. Premature 6 years exactly. In Order to investigate the extentand term infants were not differentiated. to which neurological or mental abnormalities inMULLER et al. [42] did a retrospective study in- breechborns might be due to the mode of deliveryvolving 2383 infants and a 9 year follow-up of itself> the subJects were divided into those born1698. They state, that the breech born infants ^ vaSinal delivery (n = 43) and those born bymore commonly needed remedial measures, more seqtio caesarea (n = 15)· The first baby born in thefrequently repeated grades, and more commonly same clinic by spontaneous cephalic deUvery afterhad arithmetic achievement levels below normal each breech born subject was taken äs the control.than their controls. Those who repeated grades Furthermore, the breechboms were matchedamounted to 15.2% in the group of infants with a^cording to sex, birth weight, and socioeconomicbirth weight below 2.500 g, and 24.5% in the group ba<&ground. The child's social class wasestabÜshedof breech born infants. There was no significant via Ws father's occupation [33].difference of the LORGE-THORNDIKE Intelligence Tab. II shows the incidence of some abnormalTest between the breech born infants and their findings in the 58 breech born infants and theircontrols. SADOWSKI and STAEMMLER [47], in a controls up to 3 years of age. For statistteal calcul-field study, investigated the quota of breech born ations the two groups, i.e. the vaginally breech
J, Perina t. Med. 6 (1978)
Manzke, Morbidity in breech presentation 135
Tab. II. Incidence of some abnormal findings in 58 breechborn infants and their controls up to 3 years of age.
age
6 weeks
9 months
18 months
36 months
abnormal findings
Cannot raise head in prone positionDysplasia of the hipCannot sit up aloneCannot pull to Standing positionCannot walk aloneCannot name objectsCannot use whole sentencesStill wetting pants
breechbornvag. n = 43
3 (7%)12 (28%)13 (30%)19 (44%)1 (2.3%)
15 (35%)2 (4.6%)
21 (49%)
breechborn,Sectio n - 15
04 (27%)7 (46%)8 (53%)04 (27%)1 (6.6%)6 (40%)
matchedpairsn = 58
1 (1.7%)8 (14%)
12(21%)13 (22%)1 (1.7%)
21 (36%)3 (5.2%)
22 (38%)
X2-testP
n.s.p<0.1p<0.1p < 0.01n.s.n.s.n.s.n.s.
n.s. = not significant
born infants and the infants delivered by caesareansection, were amalgamated into one and thencompared with the matched pairs. It is interestingto note that among the abnormal findings (selectedout of a list of 18 variables) only the nine monthone, i.e. cannot pull to Standing position, wasfound significantly more frequent with the breechborn infants than with the controls. (p < 0.01).However, the chances are that the differences maybe caused by the higher incidence of dysplasia ofthe hip (p < 0.1) rather than by retarded motoricdevelopment of the breech born infants. Most in-fants with dysplasia of the hip had to be treatedwith an abduction Splint ("Spreizhose") until the6th month. There were 6 children who, in everyexamination from the neonatal period until theage of three years, showed signs of retardation.Three of these were vaginally breech born infants,1 was an infant delivered by caesarean section, and2 were matched pairs.At the age of 6 years all children were reexaminedthoroughly by pediatricians, psychologists, oph-thalmologists and otolaryngologists (audiometry).Only the neurological-psychological findings in-cluding the EEG-findings are reported here. Therewere no differences in the intergroup physicalfindings (height, weight, head circumference). Thepsychological examination consisted of the Colum-bia Mental Maturity Scale, the RAVEN ColouredMatrices Test and the Peabody Picture VocabularyTest [10]. For assessment of the motoric functionalStatus the HAMM-MARBURGER Body CoordinationTest [49] was applied in a reduced from (3 insteadof 4 exercises). Furthermore, the motor behavior
of the children was rated on a neurologic-moto-scopic scale which consisted of 22 items, such äshopping on one foot, skipping and finger-nose test;optimal scoring index 22. In contrast to the latterhigh ratings in the other tests indicate good per-formance. Tab. III presents the results of theneurological-motoscopic Score of the 58 breechborn infants and their matched pairs. The meanvalues of the probands and their controls differonly slightly. However, using the Wilcoxon matchedpairs signed ranks test, the differences of theintelligence tests äs well äs of the neurological-motoscopic tests, were significant between thevaginally breech born children and their controls,whereas the differences between the sectio deliveredchildren and their controls did not show ariy signif-icance.It is noticeable that all mean values belong to thehigher ränge of the age specific Standard values.This is undoubtedly due to the fact that childrenfrom the upper social classes were overrepresented.Among the vaginally breech born children unfavor-able results with a neurologic-motoscopic score> 27 points were significantly more frequent withboys than with girls. Furthermore, a lower Colum-bia Mental Maturity Scale (< 60 points) and alower RAVEN Test Score (< 20 points) were foundsignificantly more frequently with children ofprimiparae than of multiparae.The correlation coefficient between both intell-igence tests was r = 0.53, and the one between theColumbia Mental Maturity Scale and the PeabodyPicture Vocabulary Test r = 0.56, whereas the in-telligence tests did not correlate significantly with
J.Perinat.Med.6(197&)

136 Manzke, Morbidity in breech presentation
Tab. III. Resultsof psychological and neurological-motoscopic examination of 58 breechborn children and their controlsat the age of 6 years.
tests
Columbia Mental MaturityScaleRAVEN (Coloured Matrices)TestPeabody Picture VocabularyTestHAMM-MARBURGER Body-Coordination TestNeurological-Motoscopic Score
breechbornvag. n = 43
59.1 ± 11.4*
17.7 ± 4.3*
54.6 ± 5.8**
61.3 ± 22.9**
25.4 ± 4.0*
matchedpairs n = 43
62.6 ± 8.5
19.7 ± 4.8
57.2 ± 5.7
67.3 ± 23.8
24.0 ± 2.5
breechbornsectio n = 15
66.6 ± 12.7
22.2 ± 6.8
60.1 ± 5.6
60.5 ± 24.9
24.8 ± 3.3
matchedpairs n = 15
67.1 ± 11.6
23.2 ± 6.9
57.7 ± 5.4
63.7 ± 26.1
26.2 ± 5.5
**Significance at 1% and * at 5% level (WILCOXON matched pairs test)
the Neurologic-Motoscopic Score and with the-MARBURGER Body Coordination Tests
(r = 0.1-0.31).The electroencephalograms obtained from 108children showed no significant differences betweenthe findings of the probands and their matchedpairs (Tab. IV). None of the children had a clinic-ally manifested epilepsy. The relatively highincidence of theta-rhythms is age-dependent.Between the age of 2 and 5 years this sign isphysiological. In older children with unimpairedbrains abnormal thetarhythms of the backgroundactivity are found in up to 15% [17].In summary our research has been able to concludethat the prognosis for development of those chil-
Tab. IV. Abnormal EEG-findings (n = 108).
#-and/or6-rhythms
breechborns 18 (33%)(n = 54)matched 14 (26%)pairs (n = 54)
diffuseslowing
1
2
foci
4
3
foto-sensibility
2
2
dren born through the vagina and who were in apre-delivery position with the pelvis forempst, ison the whole marginally less favorable than thatfor children in the same position and who weredelivered by caesarean section.
Keywords: Breech-delivered infants, follow-up studies, morbidity rate.
Zusammenfassung
Gesundheitliche Schäden bei in Beckenendlage geborenenKindernDie Ursachen der Beckenendlage sind sehr verschieden.Sie können in seltenen Fällen Begleitphänomen primärgeschädigter Feten sein. Fehlbüdungen werden bei Becken-endlage-Kindern zwei- bis dreimal [12, 31] häufiger alsbei Schädellage-Kindern angetroffen, desgleichen be-stimmte Dysmorphie-Syndrome [11] wie zum Beispiel dasembryofetale Alkoholsyndrom oder die Trisomie-21.Daher sollte man bei der Untersuchung von Beckenendlage-Kindern besonders auf morphologische oder funktionelleStörungen achten.Typische Gefahren der Beckenendlagengeburt sind Vor-fall der Nabelschnur, Nabelschnurkompression, vor-zeitige Lösung der Plazenta [12] sowie mechanische Ver-
letzungen des Kindes: Plexuslähmung des Armes [16],Klavikulafraktur, Tortikollis, Hüftdysplasie und Genital-hämatome [18]. Eine angeborene Hüftgelenksluxationwird bei Beckenendlage-Kindern neunmal häufiger alsbei Schädellage-Kindern gefunden: sie betrifft fast aus-schließlich Feten, die in utero mit ausgestreckten Beinenliegen [23]. Als seltene Komplikationen seien genannt:Lähmung des N. obturator [15], Läsionen des Hypo-physenstiels (hypophysärer Zwergwuchs [6, 56]) undausgedehnte Muskelblutungen mit der Ausbildungeines Crush-Syndroms [44]. Atemstörungen könnendie Folge von Fruchtwasser- bzw. Mekomum-As-piration, Zwerchfelllähmung, Lungenblutung oder einesidiopathischen Atemnotsyndroms sein. , Fast 30% derBeckenendlage-Kinder sind Frühgeborene [54] [sowie
J. Perinat. Med. 6 (1978)

Manzke, Morbidity in breech presentation 137
bisher unveröffentlichte Zahlen aus dem PU-Programm„Schwangerschaftsverlauf und Kindesentwicklung" J.Als häufigste Todesursache werden intrakranielle Blu-tungen angetroffen.Die medizinische Literatur weist eine große Zahl Nach-untersuchungsstudien an Beckenendlage-Kindern auf,deren Aussagekraft jedoch aufgrund methodischerMängel begrenzt ist (Kapitel 3). Ein Vergleichskollektivfehlt häufig. Arbeiten, die sich nur auf die Auswertungvon Fragebögen stützen, zeigen zumeist günstigere Er-gebnisse als solche, die mit neurologischen und psycho-metrischen Testuntersuchungen kombiniert sind. InStudien an Kindern mit Lernstörungen oder mit körper-lichen und geistigen Behinderungen lassen sich ursäch-lich verschiedene perinatale Einflußfaktoren wie Früh-geburt, Zwillingskind und postnatale Atemstörung retro-spektiv gar nicht oder nur schwer voneinander trennen.Der Prozentsatz an Beckenendlage-Kindern ist in solchenKollektiven unverhältnismäßig hoch (8-15% [47, 551).Prospektive Studien [4, 38, 43] haben demgegenüber denVorteil, daß sie von einem unausgewählten Patientengutausgehen und sich statistisch einwandfrei bearbeitenlassen.Allgemein läßt sich feststellen, daß mit Zunahme derSektiofrequenz bzw. durch eine verfeinerte Indikations-stellung zur Schnittentbindung die Mortalitätsziffer undMorbiditätsrate der Beckenendlage-Kinder während derletzten 30 Jahre deutlich gesenkt werden konnten(s. Tab. I).Vergleichende Intelligenztestungen an Beckenendlage-Kindern [27, 42, 43] lassen nur geringe, statistisch kaumsignifikante Unterschiede erkennen. In den Kapiteln 5-7werden die wichtigsten Daten der einzelnen Nachunter-suchungsstudien entsprechend dem Zeitpunkt der Er-fassung: Neonatalperiode, Kleinkindes- sowie Schulalter,kurz referiert.Eigene Nachuntersuchungsergebnisse (Kapitel 8) basierenauf einer Nachuntersuchung von 58 Beckenendlage-Kindern im Alter von 6 Jahren. Die Probanden gehörenzur prospektiven Untersuchungsreihe „Schwangerschafts-verlauf und Kindesentwicklung" (DFG). Im Matched Pair-Verfahren wurde jedem Beckenendlage-Kind das in der-selben prospektiven Untersuchungsreihe nächstfolgendeKind gegenübergestellt, welches spontan aus Schädellagegeboren war, gleiches Geschlecht und gleiches Gewichtaufwies sowie aus gleichen sozioökonomischen Verhält-nissen stammte. Weiterhin wurden die Beckenendlage-Kinder aufgeteilt in solche, die vaginal (n = 43) und
solche, die durch Sektio geboren waren (n = 15). Beidergrob orientierenden Analyse der Entwicklungsdaten biszum Alter von 3 Jahren fiel lediglich eine größere Zahlvon Beckenendlage-Kindern auf (44% bzw. 53% gegen-über 22% bei den Kontrollkindern), die im Alter von 9Monaten noch nicht ihre Beine zum Stehen aufstellenkonnten (p < 0,01, s. Tab. II). Dieser Befund steht sichermit der größeren Anzahl von Hüftdysplasien unter denBeckenendlage-Kindern und deren Behandlung mit einerSpreizhose in Zusammenhang (28%: 14%; p < 0,1). Ins-gesamt zeigten 6 Kinder, von denen 3 vaginal aus Becken-endlage, l durch Sektio aus Beckenendlage und 2 ausSchädellage geboren waren, eine verzögerte Entwicklung.Darüberhinaus ließen sich erst bei der Analyse der psycho-metrischen und neurologisch-motoskopischen Testergeb-nisse im Alter von 6 Jahren signifikante Leistungsunter-schiede zwischen den vaginal aus Beckenendlage geborenenKindern und deren Matched pairs feststellen, währendzwischen den durch Sektio geborenen Beckenendlage-Kindern und deren Matched pairs keine Differenzen nach-weisbar waren (s. Tab. III). Die quantitativ nur geringenUnterschiede sind sowohl bei den 3 angewandten Intelli-genztests Columbia Mental Maturity Scale, RAVEN-Testund Peabody Picture Vocabulary Test als auch beimHAMM-MARBURGER-Körperkoordinationstest und beidem von uns selbst zusammengestellten neurologisch-motoskopischen Summationsscore auffällig. Bezogen aufdie Altersnormwerte [10, 49] liegen jedoch auch dieMittelwerte der vaginal aus Beckenendlage geborenenKinder in unserem Nachuntersuchungskollektiv im oberenNormbereich. Grund hierfür mag sein, daß ein überreprä-sentativ großer Anteil unserer Probanden aus sozial höhe-ren Schichten stammt.Unter den vaginal geborenen Beckenendlage-Kindernfanden sich signifikant schlechtere Testergebnisse imneurologisch-motoskopischen Summationsscore bei denKnaben als bei den Mädchen, sowie signifikant schlechtereLeistungen in der Columbia Mental Maturity Scale und imRaven-Test bei den Kindern von Primipara als von Multi-para.Die EEG-Befunde (s. Tab. IV) ergaben keine gruppensig-nifikanten Unterschiede.Zusammenfassend lassen unsere Nachuntersuchungsergeb-nisse den Schluß zu, daß im allgemeinen die Entwick-lungsprognose der vaginal aus Beckenendlage geborenenKinder geringgradig schlechter ist als die der durch Sectiocaesarea aus Beckenendlage geborenen Kinder.
Schlüsselwörter: Beckenendlage-Kinder, Nachuntersuchungsstudien, Spätmorbidität.
Resume
La morbidite chez les bebes nes avec position du siegeLes causes de la position du siege sont tres differentes.Elles peuvent dans de rares cas etre des symptömessecondaires de foetus aux lesions primaires. Les mal-formations sont de deux a trois fois [ 12,31 ] plus frequenteschez les enfants avec position du siege qu'avec position dusommet, de meme en est-il pour certains syndromes dedysmorphie [11] tels que le syndrome d'alcool embryo-foetal ou latrisomie 21. Aussi devrait-on insister davantage
sur l'examen des troubles morphologiques ou fonctionnelschez les enfants avec position du siege.Les dangers-types des accouchements par position du siegesont le prolapsus ou la compression du cordon ombilical,le detachement premature du placenta [12] ainsi que lesblessures mecaniques de l'enfant: paralysie d'un plexus dubras [16], fracture de la clavicule, torticolis, dysplasiede la hanche et hematomes genitaux [18]. Une luxationcoxale congenitale est neuf fois plus frequente chez les
J.Perinat.Med.6(1978)

138 Manzke, Morbidity in breech presentation
enfants avec positiondu siege qu'avec position du sommet:eile concerne presqu'exclusivement les foetus qui reposentles jambes etendues dans l'uterus [23 J. Des complicationsplus rares peuvent apparaitre comme la paralysie du N.Obturator [15], des lesions de la tige pituitaire (6, 56) etdes myohemorragies avec developpement d'un syndromede broiement des membres [44 J. Des troubles respiratoirespeuvent egalement resulter d'une aspiration amniotiqueou de meconium, d'une phrenoplegie, de pneumorragie oud'un syndrome de dyspnee protopathique. Pres de 30%des enfants avec position du siege sont prematures ([54],et d'apres les chiffres non encore publies du ProgrammePU de «Grossesse et Developpement embryonnaire»). Leshemorragies intracräniennes semblent constituer la causede mort la plus frequente.La litterature medicale contient un grand nombre d'etudesde reexamen d'enfants avec position du siege, niais leursmethodes defectueuses les rendent encore insuffisammentprobantes (eh. 3). Elles manquent souvent d'analysescomparatives avec un groupe de sujets normaux. Lestravaux qui reposent seulement sur Fevaluation dequestionnaires montrent des resultats en general plus
. favorables que ceux qui sont combines avec des testsneurologiques et psychometriques. Dans les observationsd'enfants souffrant de difficultes d'apprentissage oud'handicaps physiques et psychiques, il est malaise oumeme impossible de differencier retrospectivement lesdiverses causes perinatales telles que l'accouchementpremature ou gemellaire, le trouble de la respirationpostnatal. Le pourcentage des enfants avec position dusiege est eleve dans de tels groupes (8-15% [47, 55]).Des etudes prospectives [4, 38, 43] ont, a cet egard,l'avantage de partir de sujets pris au hasard et de fournirainsi des statistiques absolument süres.D'une fa£on generale, on peut constater une baissecertaine des taux de mortalite et de morbidite des enfantsavec position du siege au cours des 30 dernieres anneesgräce a l'augmentation des cesariennes et a la plus grandedifferenciation de leur indication (cf. Tab. I). Des testsd'intelligence comparatifs effectues sur des enfants nesavec position du siege [27, 42, 43] ne permettentd'obtenir que des differences minimales, d'un interetpratiquement nul pour les statistiques. Les eh. 5 et 7commentent brievement les principaux resultats desetudes suivant les divers moments oü ont ete effectuesles reexamens: periodes neonatale, de la petite enfanceet scolaire.Les propres resultats de reexamen (eh. 8) se basent surles observations a Tage de 6 ans de 58 enfants nes avecposition du siege. Les propositions relevent de la seried'examens prospectifs «Grossesse et Developpementembryonnaire» (DFG). Selon un processus de MatchedPair, chaque enfant avec position du siege a ete confronte
avec un enfant ne spontanement avec position du sommet,de meme sexe, de meme poids et de meme Statut social.De plus, les enfants avec posifiin du siege ont ete repartisen deux groupes, Tun d'accouchement vaginal (n = 43),l'autre de cesaiienne (n « 15). L'analyse sommaire desresultats de developpement jusqu'a Tage de 3 ans s'estmontree seulement interessante par le nombre superieurdes enfants avec position du siege (44% et 53% contre22% chez les enfants du groupe de contröle) qui, a Tagede 9 mois, ne parvenaient pas encore a placer leurs jambespour se mettre dans la Station debout (p < 0,01, cf Tab. II).Ce resultat depend sans aucun doute du nombre egalementsuperieur de dysplasies coxales parmi les enfants avecPosition du siege et de leur traitement par pantalond'ecartement (28%: 14%; p < 0,1).6 enfants au total, dont 3 avec accouchement vaginal deposition du siege, l avec cesarienne de position du siege et2 avec position du sommet, ont fait etat d'un developp-ement retardo.Par ailleurs, seule Tanalyse des tests psychometriques etneurologiques-motoscopiques a l'äge de 6 ans a permisde constater des differences de performance significativesentre les enfants avec position du siege nes par accouch-ement vaginal et leurs matched pairs, tandis qu'aucunedifference n'a pu etre relevee entre les enfants avec positiondu siege nes par cesarienne et leurs matched pairs (cf.Tab. III). Les differences faibles du point de vue quantitatifont pu etre etablies aussi bien par les 3 tests d'intelligenceColumbia Mental Maturity Scale, RAVEN-Test et PeabodyPicture Vocabulary Test que par le test de coordinationphysique de HAMM-MARBURG et par le Summation-score neurologique-motoscopique que nous avons elaborenousmemes. Comparees aux normes d'äge [10, 49], lesmoyennes des enfants nes en position du siege par accouch-ement vaginal et appartenant a notre groupe de reexamense situent, toutefois, dans la zone superieure des normes,ce qui est peut-etre du a ce que la majorite de nospropositions proviennent de couches sociales elevees.Parmi les enfants nes en position du siege par accouchementvaginal, le summationscore neurologique-motoscopique adonne des resultats nettement plus mauvais chez lesgargons que chez les filles et le Columbia Mental MaturityScale et le RAVEN-Test ont temoigno de performancessensiblement moins bonnes chez les enfants de primiparesque de pluripares.Les resultats d'EEG (cf. Tab. IV) n'ont revele aucunedifference significative entre les divers groupes.En resume, les donnees de nos reexamens permettent deconclure que, d'une faqon generale, le pronostic de devel-oppement des enfants nes en position du si^ge pai accouch-ement vaginal est un peu plus mauvais que chez les enfantsnes en position du siege par cesarienne.
Mots-cles: Enfants avec position du siege, etudes de reexamen, morbidite tardive
Acknowledgements: The sixyears follow-up investigationswere carried out in coUaboration with Prof. Dr. H. Genzand Dr. H. Mostowski (Institut für Sozialhygiene d. FUBerlin), Dr. M. Mensebach (Universitäts-KinderklinikMainz), Prof. Dr. R. Neth (Universitäts-KinderklinikHamburg-Eppendorf), and Prof. Dr. A. Sinios u. S. W.Worch (Kinderkrankenhaus Borgfelde, Hamburg).
Furthermore, I have to thank Dipl.-Psychol.-Dr. G. Gute-zeit and Dr. E. Völzke (EEG) (UniversitätSrKinderklinikKiel), Dr. H. Michaelis (Institut für Dokumentation u.Statistik Mainz).The own studies were supported by Deutsche Forschungs-gemeinschaft, Ma 585,1-4.
J.Perinat.Med.6(1978)

Manzke, Morbidity in breech presentation 139
Bibliography
[1] ABROMS, I. F., J. E. MCLENNAN, F. MANDELL:Acute neonatal subdural hematoma following breechdelivery. Amer. J. Dis. Child. 131 (1977) 192
[2] ALEXOPOULOS, K. A.: The importance of breechdelivery in the pathogenesis of brain damage. Clin.Pediat. 12(1973)248
[3] BARLOW, T. G.: Congenital dislocation of the hip.J. Bone J. Surg. 43 B (1961) 603
[4] BERENDES, H. W.: Obstetrical complications andmental deficiency. InternationalCopenhagenCongresson the Scientific Study of Mental Retardation, l(1964) 308
[5] BHAGWANANI, S. G., H. V. PRICE, K. M. LAU-RENCE, B. GlNZ: Risk and prevention of cervicalcord injury in the management of breech present-ation with hyperextension of the fetal head. Amer.J. Obstet. Gynecol. 115 (1973) 1159
[6] BIERICH, J. R.: On the aetiology of hypopituitarydwarfism. Growth and Growth Hormone. ExcerptaMedica International Congress Series No. 244, p. 408.Amsterdam 1972
[7] BIRD, CH. C., TH. W. MCELIN: A six-year prospec-tive study of term breech deliveries utilizing theZatuchni-Andros Prognostic Scoring Index. Amer. J.Obstet. Gynecol. 121 (1975) 551
[8] BISHOP, E. H., L. ISRAEL, C. C. BRISCOE: Ob-stetrics influences on the premature infants festyear of development. Obst. Gynec. 26 (1965) 628
[9] BOLTE, A., H. W. STEINMANN, C. H. BEUSCH,H. J. PÜTZ, G. A. SCHRAVEN: Kindliche Hirn-schäden nach operativen Geburten. Ar eh. Gynäk.205(1968)110
[10] BONDY, c., R. COHEN, D. EGGERT, G. LÜER:Testbatterie für geistig behinderte Kinder. BeltzTest Gesellschaft, Weinheim 1969
[11] BRAUN, F. H. T., L. S. JONES, D. W. SMITH:Breech presentation äs an indicator of fetal ab-normality. J. Pediat. 86 (1975) 419
[12] BRENNER, W. E., R. BRUCE, C. H. HENDRICKS:The characteristics and perils of breech presentation.Amer. J. Obstet. Gynecol. 118 (1974) 700
[13] BUTLER, M.: The short- and long-term effects ofperinatal problems. In: STEMBERA, Z. K.,K. POLACEK, V. SABATA: Perinatal Medicine.G. Thieme, Stuttgart 1975 and Avicenum, Czechos-lovak Medical Press, Prague 1975
[14] CARTER, W., J. A. WILKINSON: Genetic and en-vironmental factors in the etiology of congenitaldislocation of the hip. Clin. Orthop. Related Research33(1964)119
[15] CRAIG, W. S., J. M. P. CLARK: Obturator palsy inthe newly born. Arch. Dis. Childh. 37 (1962) 661
[16JCZURDA, R., F. MEZNIK: Zur Therapie undPrognose der Plexuslähmung beim Neugeborenen.Pädiatr. Pädol. 12 (1977) 137
[17] DOOSE, H., H. GERKEN, E. VÖLZKE: On thegenetics of EEG-anomalies in childhood. I. Abnormaltheta rhythms. Neuropädiatrie 3 (1972) 386
[18] DÜNN, P. M.: Testicular birth trauma. Arch. Dis.Childh. 50 (1975) 743
[19] DÜNN, P. M.: Maternal and fetal aetiological factors.In: ROOTH, G., L.-E. BRATTEBY: Perinatal
Medicine. Almqvist & Wiksell International, Stock-holm 1976
[20] DÜNN, P. M.: Breech delivery: perinatal morbidityand mortality. In: ROOTH, G., L.-E. BRATTEBY:Perinatal Medicine. Almqvist & Wiksell International,Stockholm 1976
[2l] EASTMAN, N. J., s. G. KOHL, J. E. MAISEL,F. KAVALIER: The obstetrical background of 753cases of cerebral palsy. Obstet. Gynec. Surv. 17(1962)459
[22] EFTHIMIADIS, J.: Steißlage und vertretbare Sektio-frequenz. Geburtsh. Frauenheilk. 36 (1976) 661
[23] FETTWEIS, E.: Das Hüftluxationsleiden bei inBeckenendlage geborenen Kindern. Z. Orthop. 111(1973)168
[24] FIANU, ST.: Fetal mortality and morbidity followingbreech delivery. Acta Obstet. Gynecol. Scand., 56(1976) Suppl.
[25] GÖBEL, D., K. W. SCHULTZE, H. WOLF: Katam-nestische Befunde bei Beckenendlagengeburten. Ge-burtsh. Frauenheilk. 31 (1971) 1249
[26] HAGBERG, B., G. HAGBERG, i. OLOW: Thechanging panorama of cerebral palsy in Sweden1954-1970. Acta Paediat. Scand. 64 (1975) 187
[27] HAMBERT, G., H. O. AKESSON: A sociopsychiatricfollow-up study of 200 breechborn children. Actapsychiat. scand. 49 (1973) 264
[28] HILL, J. G., B. W. ELIOT, A. J. CAMPBELL, A. A.PICKETT-HEAPS: Intensive care of the fetus inbreech labour. Brit. J. Obstet. Gynaecol. 83 (1976)271
[29] HOCHULI, E., o. DUBLER, E. BORNHAUSER,E. SCHOOP: Die kindliche Entwicklung nachvaginaler und abdominaler Entbindung bei Becken-endlagen. Geburtsh. Frauenheilk. 37 (1977) 4
[30] HOHLWEG-MAJERT, P., M. WILLARD: Nachunter-suchungen der aus Beckenendlage geborenen Kinderim Lebensalter von 3-7 Jahren auf ihre geistige undmotorische Entwicklung. Z. Geburtsh. Perinatol. 179(1975)441
[31] ISSEL, E. P.: Die erweiterte Sectioindikation bei derEntbindung des Fetus aus Beckenendlage. Zbl.Gynäkol. 99 (1977) 919
[32] KENDALL, N., H. WOLOSHIN: Cephalhematomaassociated with fracture of the skull. J. Pediat. 41(1952)125
[33] KLEINING,G., H. MOORE: Soziale Selbsteinstufung:Ein Instrument zur Messung sozialer Schichten.Kölner Z. Soziol. u. Soz. Psychol. 20 (1968) 3
[34] KUBLI, F., W. BOOS, H. RÜTTGERS: Caesareansection in the management of singleton breechpresentation. In: ROOTH, G., L.-E. BRATTEBY:Perinatal Medicine. Almqvist & Wiksell Stockholm1976
[35] MÄDER, H.: In: BACH, W. W.: Tagungsbericht derOberrheinischen Gesellschaft für Geburtshilfe undGynäkologie. Geburtsh. u. Frauenheilk. 33 (1973)822
[36] MANZKE, H.: Die Bedeutung prospektiver Unter-suchungen für die Erforschung pränataler und peri-nataler Schäden beim Menschen. Dtsch. med. Wschr.96(1971)1610
J.Perinat. Med. 6(1978)

140 Manzke, Morbidity in breech presentation
[37] MANZKE, H., H.-J. ROHWEDDER: Röntgenologietraumatischer Skelettveränderungen beim Säuglingund Kleinkind, pädiat. prax. 10 (1971) 73
[38] MANZKE, H., G. MAU, G. v. ONDARZA-LANDWEHR, H. GENZ, A. SINIOS, H. ALTROGGE,M. SEBACH: Prospektive Langzeituntersuchungvon Beckenendlagen-Kindern. In: SCHMIDT, E.,J. W. DUDENHAUSEN, E. SALING: PerinataleMedizin Bd. VII. Thieme, Stuttgart 1978
[39] MARTIUS, H.: Geburtshilfliche Operationen. 11.Auflage G. Thieme, Stuttgart 1971
[40] MCKAY, R. J.: The fetus and the newborn infant.In: NELSON, W. E.: Textbook of Pediatrics, 9. ed,W. B. Saunders, Philadelphia 1969
[41JMORTON, K. C.: The pediatrician and breechdelivery. Amer. J. Dis. Chüd. 105 (1963) 19
[42] MULLER, P. F., H. E. CAMPBELL, W. E. GRAHAM,H. BRITTAIN, J. A. FITZGERALD, M. A. HOGAN,V. H. MULLER, A. H. RITTENHOUSE: Perinatalfactors and their relationship to mental retardationand other parameters of development. Amer. J.Obstet. Gynec. 109 (1971) 1205
[43] NELIGAN, G. A.: The quality of the survivors ofbreech delivery in a geographicaÜy defined population.In: ROOTH, G., L.-E. BRATTEBY: PerinatalMedicine. Almqvist & Wiksell International, Stock-holm 1976
[44] R ALIS, Z. A.: Birth trauma to muscles in babiesborn by breech delivery and its possible fatal con-sequences. Arch. Dis. Childh. 50 (1975) 4
[45] RONA, R. J., J. M. TANNER: Aetiology of idio-pathic growth hormone deficiency in England andWales. Arch. Dis. Childh. 52 (1977) 197
[46]ROVINSKY, J. jr., A. MILLER, S. KAPLAN:Management of breech presentation at term. Amer.J. Obstet. Gyn. 115 (1973) 497
[47] SADOWSKI, R., H.-J. STAEMMLER: Zum Einflußder Beckenendlagengeburt auf die geistige undkörperliche Entwicklung* der Kinder. Z. Geburtsh.Perinat. 178 (1974) 104
[48] SANO, R., K. KOBAYASHI, N. FUJI: Effects ofobstetrical factors upon the mental development ofinfants. (2) Study on a relationship between modeof labor and development quotient in infants. Actaneonatal. jap. 11 (1975) 105 resp. Excerpta med.(Amst.), Sect. VII, 35 (1976) 159
[49] SCHILLING, F.: Körperkoordinationstest fürKinder. Manual. Beltz Test Gesellschaft, Weinheim1974
[50] SCHLANGE, H., B. STEIN, S. TANELI, I. ULRICH:Frühkindliche Hirnschädigung und soziale Klasse.Mschr. Kinderheilk. 123 (1975) 72
[51 ISCHRAGE, R.: Zur Ätiologie der Beckenendlage.Z. Geburtsh. Perinat. 177 (1973) 437
[52] SHULMAN, B. H., CH. B. TERHUNE: Epiphysealinjuries in breech delivery. Pediatrics 8 (1951) 693
[53] SINDER, CH., N. E. WENTSLER: Breech present-tation with follow up. Obstet. Gynecol. 25 (1965)322
[54]TALLIAN, F., E. PUSKAS, A. HERNADY, I.TOMKA: Über die Wirkung der Beckenendgeburt(Kontrolluntersuchungsergebnisse). Acta chir. hung.tomusVI(1965)375
[55] TENHAEFF, D., E. SPULAK-ESSER, H. U. FELD-MANN: Das lernbehinderte Kind nach Geburt ausBeckenendlage. Münch. Med. Wschr. 114 (1972)1565
[56] VAN DER WERFF TEN BOSCH, J. J.: Hypofysairedwerggroei. Ned. T. Geneesk. 106 (1962) 1282
Prof. Dr. med. H. ManzkeUniversitäts-KinderklinikSchwanenweg 20D-2300 Kiel
J. Perinat. Med. 6(1978)


















