REGLES GENERALES DE LECTURE ET - …¨gles... · Increased nasal resistance ... COMPLIANCE...
84
REGLES GENERALES DE LECTURE ET D’UTILISATION DES TRACES POLYGRAPHIQUES SOUS VNI Christophe Perrin Service de Pneumologie Pôle Spécialités Médicales Centre Hospitalier de Cannes Cannes, France
Transcript of REGLES GENERALES DE LECTURE ET - …¨gles... · Increased nasal resistance ... COMPLIANCE...

REGLES GENERALES DE LECTURE ET D’UTILISATION DES TRACES POLYGRAPHIQUES SOUS VNI
Christophe Perrin Service de Pneumologie Pôle Spécialités Médicales Centre Hospitalier de Cannes Cannes, France

Simonds AK, Elliott MW. Thorax 1995; 50 : 604
Simonds AK et al. Thorax 1998; 53 : 949
SURVIVAL
Main goal of long-term mechanical ventilation
NMD: progress in airway clearance management
Link with therapeutic efficiency
Importance of monitoring

Janssens JP et al. Thorax 2011;66:438
± TcPCO2 if available, although expensive and technical problems (bias, errant values) or FiO2 > 21%
Consequences
of non intentional leaks
Fall in VT (> 50%)
Increased nasal resistance
Poor triggering
Poor I/E cycling (flow threshold)
Sleep fragmentation
Eye irritation
Skin sores
Detection of non intentional leaks (clinically and/or by NIV sofware)
90%
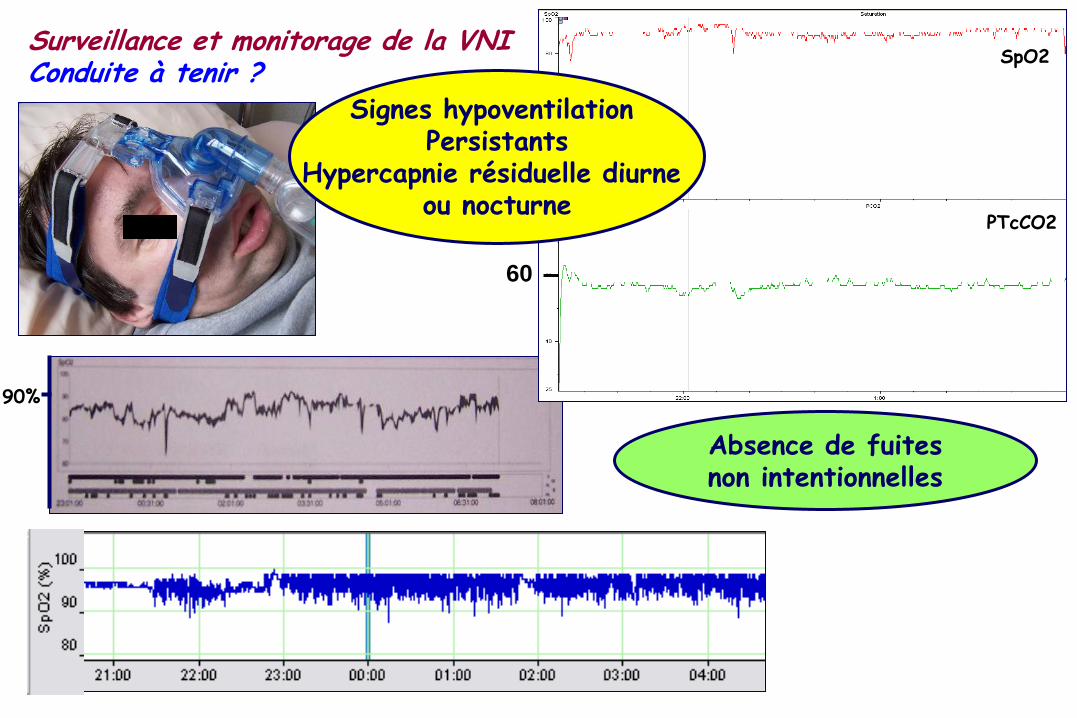
Surveillance et monitorage de la VNI Conduite à tenir ?
60
SpO2
PTcCO2
Signes hypoventilation Persistants
Hypercapnie résiduelle diurne ou nocturne
Absence de fuites non intentionnelles

Janssens JP, Borel JC, Pépin JL et al. Thorax 2011;66:438

Polygraphie respiratoire
± PTcCO2 (si disponible ou FiO2 > 21%)
± PTcCO2 si disponible ou FiO2 > 21%

RESPIRATORY EVENTS (others than leaks) PARTIAL OR TOTAL UPPER AIRWAY OBSTRUCTION
. with reduction of ventilatory drive
. without reduction of ventilatory drive
PATIENT – VENTILATOR ASYNCHRONY
. Ineffective inspiratory efforts
. Auto and double triggering
. Late cycling
. Premature cycling
OTHER UNDADEQUATE VENTILATOR SETTING
. Rise time > minimal inspiratory time

Pression au masque
Débit insufflé et expiré mesuré dans le circuit à proximité du masque (pneumotachographe)
Sangle thoracique
Sangle abdominale
POLYGRAPHIE VENTILATOIRE « CONVENTIONNELLE »
SOUS VNI Oxymétrie
Au minimum !
± PTcCO2 Si disponible ou FiO2 > 21%

But,
“CONVENTIONAL” POLYGRAPHY UNDER NIV
- Needs hospitalization
- Time consuming for the staff

Janssens JP et al. Thorax 2011; 66 : 438
Polygraphie respiratoire « intégrée » à domicile
Ventilateur Oxymètre ± PTcCO2
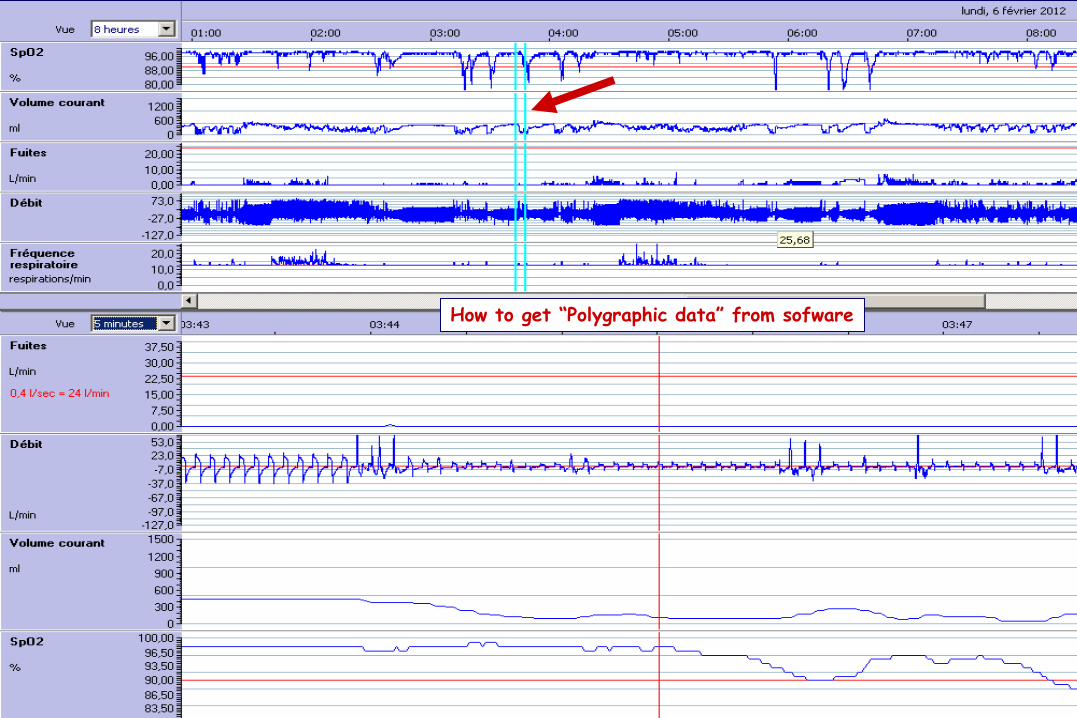
How to get “Polygraphic data” from sofware

Flow
Pressure
VT
Total leaks
SpO2
How to get “Polygraphic data” from sofware

Neuromuscular disease NIV FiO2 21% Nasal mask
Non intentional leaks through the mouth

Apprentissage
de la polygraphie respiratoire
« conventionnelle »
est indispensable pour comprendre
la polygraphie « intégrée »

Pression
Débit
Th
ABD
SpO2 95%

Le diagnostic n’est pas toujours facile ! « couple patient – machine »

Effet du sommeil sur la respiration
Chémosensibilité ( PaO2, PaCO2)
Résistance des VAS
REM : Hypotonie MR accessoires
Capacité Résiduelle Fonctionnelle
VENTILATION NON INVASIVE Couple patient – machine IMPACT DU PATIENT

VENTILATION NON INVASIVE Couple patient – machine IMPACT DE LA TECHNIQUE
Interface . Fuites non intentionnelles . Douleurs Ventilateur . Capture de la commande ventilatoire . Fermeture des VAS . Déclenchement, cyclage : inappropriés
Jounieaux V et al. J Appl Physiol 1995; 79 : 186
Leung et al. AJRCCM 1997; 155 : 1940

VENTILATION NON INVASIVE Couple patient – machine MESENTENTE PATIENT – VENTILATEUR
Asynchronisme !

Pression au masque
Débit insufflé et expiré mesuré dans le circuit à proximité du masque (pneumotachographe)
Sangle thoracique
Sangle abdominale
MONITORAGE PATIENT ET MACHINE
POLYGRAPHIE VENTILATOIRE SOUS VNI Oxymétrie
Au minimum !

EVENEMENT RESPIRATOIRE
Survenue d’une rupture ventilatoire (caractérisée par la diminution de
l’amplitude des sangles thoracique et abdominale ou leur instabilité)
qui retentit sur la qualité des échanges gazeux et/ou du sommeil.
Que rechercher ? ANALYSE : pression et débit
Abdomen
Thorax
SpO2
Onde de pouls

La sémiologie des courbes de pression et débit dépend : du type ou mode de fonctionnement du ventilateur

Ventilateur à régulation de volume Volume
Volume C
Pression
Débit
R Pression
« Quid » en cas d’ obstacle, ou de fuite ?

Ventilateur à régulation de pression Pression
Volume
R
C
Pression
Débit
« Quid » en cas d’ obstacle, ou de fuite ?


Ventilation à régulation de pression avec volume cible
Rabec C et al. Thorax. 2011; 66:170-178.

Pression
Débit
Thorax
Abdomen
SpO2
Barométrique, mode PAC + volume cible

La sémiologie des courbes de pression et débit dépend : du mode de ventilation

Rabec C et al. Thorax. 2011; 66:170-178.
Ici, dans le cas d’un ventilateur à régulation de pression
Déclenchement patient, durée insufflation variable
Déclenchement patient, durée insufflation constante

Rabec C et al. Thorax. 2011; 66:170-178.
Ici, dans le cas d’un ventilateur à régulation de pression
Déclenchement « machine », durée insufflation constante

Type de ventilateur ?, Mode ?

Barométrique, Mode ST

La sémiologie des courbes de pression et débit dépend : . position pneumotachographe / système expiratoire
. type de masque

Position du pneumotachographe par rapport au système expiratoire
Perrin C et al. Rev Mal Respir 2004; 21:556 Rabec C et al. Thorax. 2011; 66:170

pneumotachographe
EXPIRATION
Position du pneumotachographe par rapport au système expiratoire

Pression
Débit
Ventilateur volumétrique – masque nasal Fuites buccales
Type de masque

La sémiologie des courbes de pression et débit dépend : de réglages particuliers du ventilateur

Temps de montée en pression
Pente
EPAP
IPAP

TMPI 200 ms / Ti min 100 ms
Ventilateur à régulation de pression Réglage aberrant TMPI / Ti min
Pression
Débit

La sémiologie des courbes de pression et débit dépend : du comportement du patient

EFFORTS
INSPIRATOIRES
Pression VTi/débit
VENTILATEUR
BAROMETRIQUE constante
VENTILATEUR
VOLUMETRIQUE Constant

Pressure
Flow
Thoracic belt
Abdominal belt
SpO2
Ventilateur à régulation de pression

La sémiologie des tracés dépend : de différents problèmes !!!!

FUITES NON
INTENTIONNELLES
Pression VTi/débit VTe
VENTILATEUR
BAROMETRIQUE peut
VENTILATEUR
VOLUMETRIQUE Constant

Pression
Débit
Thorax
Abdomen
SpO2
Ventilateur à régulation de pression

Pression
Débit
Thorax
Abdomen
SpO2
Pression
Débit
Ventilateur à régulation de pression

Pressure
Flow
Thoracic belt
Abdominal belt
SpO2

OBSTACLE
Pression VTi/débit VTe
VENTILATEUR
BAROMETRIQUE constante
VENTILATEUR
VOLUMETRIQUE Constant

Obstruction Quelques ORIENTATIONS DIAGNOSTIQUES
COMPLIANCE THORACIQUE (lutte du patient)
RESISTANCES BRONCHIQUES
FERMETURE PARTIELLE OU COMPLETE DES VAS
. avec diminution de la commande ventilatoire
. sans diminution de la commande ventilatoire (instabilité des VAS)
EFFORTS INSPIRATOIRES NON RECOMPENSES
REGLAGES INADEQUATS DU VENTILATEUR
. Cyclage prématuré (Ti min trop court)
. Pente (temps de montée en pression) > Ti min

Pression
Débit
Thorax
Abdomen
SpO2

Pression
Débit
Thorax
Abdomen
SpO2
Obstruction AVEC diminution de la commande ventilatoire Fermeture partielle des VAS

Pression
Débit
Thorax
Abdomen
SpO2
Barométrique, mode PAC + volume cible

Pression
Débit
Thorax
Abdomen
SpO2
Barométrique, mode PAC + volume cible
Fermeture complète des VAS avec commande ventilatoire

Sankri-Tarbichi AG et al. AJRCCM 2009; 179:313
Obstruction AVEC diminution de la commande Fermeture des VAS

Pression
Débit
Thorax
Abdomen
SpO2
Onde de pouls

Fermeture partielle des VAS sans commande ventilatoire
et cyclage précoce
Pression
Débit
Thorax
Abdomen
SpO2
Onde de pouls


Obstruction SANS diminution de la commande ventilatoire Fermeture par instabilité des VAS


1
Inspiration / Insufflation

1 1
Fermeture complète des
VAS
Diaphragme efficace Parésie Diaphragmatique

Obstruction SANS diminution de la commande ventilatoire Fermeture par instabilité des VAS
Ventilation abdominale physiologique
Fatigue diaphragme – muscles accessoires

Pressure
Flow
Th
ABD
SpO2 94%

Pressure
Flow
Th
ABD
SpO2 94%
Ineffective inspiratory efforts

Vignault L et al. Intensive Care Med 2009; 35 : 840

Vignault L et al. Intensive Care Med 2009; 35 : 840

Pressure
Flow
Th
Abd
SpO2

Pressure
Flow
Th
Abd
SpO2
Premature cycling


Rise time > minimal inspiratory time

Problèmes intriqués …..

Acromégalie, tétraplégie (C3), paralysie phrénique, SAOS (IAH 75/h)
IMC 29 kg/m2
Masque nasal moulé, Elisée 150 (mode VPAC)
Montage : MN - flow - valve
Pression
Débit
ABD
SpO2
Th

Pressure
Flow
Th
ABD
SpO2 94%
Flow
VT
SpO2 %
Ineffective inspiratory efforts
“Conventional” polygraphy
“Polygraphic data” from sofware

“Polygraphic data” from sofware
“Conventional” polygraphy
Flow
Leaks
VT
SpO2
Pressure
Vignault L et al. Intensive Care Med 2009; 35 : 840
Double triggering

Pressure
Flow
Th
Abd
SpO2
VT
Leaks
Flow
SpO2
Pressure
“Polygraphic data” from sofware
“Conventional” polygraphy
Premature cycling

“Polygraphic data” from sofware
“Conventional” polygraphy
Rise time > minimal inspiratory time

Pressure
Flow
Th
Abd
SpO2
Flow
Pressure
VT
Total leaks
SpO2
Regarding to the decrease of flow, this event could be upper airway obstruction with reduction of ventilatory drive
“Polygraphic data” from sofware
“Conventional” polygraphy

“Polygraphic data” from sofware
“Conventional” polygraphy
Regarding to the decrease of flow, this event could be upper airway obstruction without reduction of ventilatory drive (upper airway instability)
Flow
Pressure
VT
Total leaks
SpO2

“Polygraphic data” from sofware
Flow
Leaks
SpO2
Periodic ventilation & non intentional leaks

Y a t-il encore un avenir pour la
Polygraphie conventionnelle ?

Pédagogique
Commande ventilatoire et VAS (sangles)
Obtention d’un réglage optimal
Analyse d’événements complexes

Upper airway obstruction with of ventilatory drive ?
Polygraphy under NIV recorded by Claudio Rabec, MD; CHU Dijon, France

Reliability of thoracic and abdominal belts ?
Polygraphy under NIV recorded by Claudio Rabec, MD; CHU Dijon, France

Monitoring of inspiratory efforts
Respiratory muscles
Pes
Indispensable !
CONVETIONAL POLYGRAPHY
PTT