REGION IX STAKEHOLDER CALL 2020 CMS PROPOSED … Proposed Rules... · 2019-09-11 · Program...
38
REGION IX STAKEHOLDER CALL – 2020 CMS PROPOSED PAYMENT RULES August 28, 2019 Neal Logue Health Insurance Specialist Division of Financial Management & Fee-for- Service Operations
Transcript of REGION IX STAKEHOLDER CALL 2020 CMS PROPOSED … Proposed Rules... · 2019-09-11 · Program...

REGION IX STAKEHOLDER CALL – 2020 CMS PROPOSED PAYMENT RULES
August 28, 2019
Neal LogueHealth Insurance SpecialistDivision of Financial Management & Fee-for-Service Operations

Agenda
• Proposed Changes to the Medicare Physician Fee Schedule for CY 2020
- General Provisions
- Payment for Evaluation and Management (E/M) Services (CY 2021)
- Quality Payment Program Year 4 (2020)
- Opioid Treatment Programs (OTPs)
• Outpatient Prospective Payment System (OPPS) & Ambulatory Surgical Center (ASC) Proposed Rule
- General Provisions
- Price Transparency
- Site Neutrality
• Proposed Changes to ESRD PPS and DMEPOS Fee Schedule (2020)
2

Physician Fee Schedule Proposed Rule
3

Proposed Changes to the Medicare Physician Fee Schedule for CY 2020
• Proposed CY 2020 PFS conversion factor of $36.09
• Additions to telehealth services for bundled episode of care for treatment of opioid use disorders
• Modifying regulation on physician supervision of physician assistants
• Modifications to documentation policy for physicians, physician assistants, nurse practitioners, clinical nurse specialists, and certified nurse-midwives
• Increase payments for Transitional Care Management (TCM)
• Bundled payments for substance use disorders
• Soliciting comments on how to align the Medicare Shared Savings Program quality performance scoring methodology more closely with MIPS
General Provisions
4

E/M Payments
5

• In the CY 2019 PFS Final Rule, CMS finalized payment, coding, and documentation changes for E/M office/outpatient visits to be implemented in CY 2021, specifically:
• Single blended rate for levels 2 through 4 (one for established and one for new patients), maintaining separate payment rates for levels 1 and 5;
• Add-on G codes for level 2 through 4 visits that describe the additional resources inherent in visits for primary care and particular kinds of non-procedural specialized medical care;
• An “extended visit” add-on G code (GPRO1) for level 2 through 4 visits to account for the additional resources required when practitioners spend additional time with these patients. Existing prolonged service codes will be used with level 5.
6
Policies for E/M Office/Outpatient Visits Finalized in the CY 2019 Final Rule for CY 2021
6

• For level 2 through 5 visits, choice to document using the current framework, medical decision making (MDM) or time:
oWhen time is used to document, practitioners will document the medical necessity of the visit and that the billing practitioner personally spent the required amount of time face-to-face with the beneficiary (typical CPT time for code reported, plus any extended/prolonged time).
o When using current framework or MDM to document, for level 2 through 4 visits CMS will only require the supporting documentation currently associated with level 2 visits (as a corollary to the blended payment).
o Current MDM guidelines will apply when using MDM to select visit level.
7
Policies for E/M Office/Outpatient Visits Finalized in the CY 2019 Final Rule for CY 2021
7

• Following the finalization of these policies, key stakeholders, including the American Medical Association (AMA) engaged CMS in ongoing dialogue.
• The AMA/CPT has developed a similar alternative approach that we are proposing to largely adopt for the PFS effective January 1, 2021 because we believe it reflects CMS’ goals of reducing documentation burden, is more in line with the current practice of medicine, and will more likely adopted by other payers. This approach is detailed in full on the AMA website at https://www.ama-assn.org/cpt-evaluation-and-management.
• CPT has redefined the office/outpatient E/M visit code set—We areproposing to adopt CPT’s revisions to the office/outpatient E/M codedescriptors (including deletion of CPT code 99201) and assign separatepayment rates to each of the codes as revised.
Proposed Policies for 2021
8

• There would be choice of time or MDM to select code level.
• MDM – We are proposing to adopt the new interpretive guidelines by CPT for levels of MDM.
• History/Exam – History and exam would no longer be used to select visit level; instead, there would be a medically appropriate history and exam.
• Time
o We would adopt the new times in the code descriptors that include all practitioner time the day of the visit
o We would adopt the new CPT code for prolonged services (CPT 99xxx) in lieu of GPRO1 (the extended service code) and CPT codes 99358, 99359 (prolonged non-face-to-face). We are seeking input on policies related to CPT codes 99358, 99359.
Proposed Policies for 2021
9

• The AMA RUC reviewed and made valuation recommendations for all codes in the office/outpatient E/M code family and an add-on code for prolonged service time, based on a robust survey of around 50 specialty societies.
• The RUC recommended values increase payment for office/outpatient E/M services.
• We are proposing to accept the RUC-recommended values for all of these codes, effective January 1, 2021.
Proposed Changes to the Office/Outpatient E/M Code Valuation for CY 2021
10

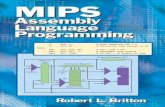
Proposed Payment for Office/Outpatient Based E/M Visits
• We are also proposing a new prolonged services code for additional time spent with patients beyond the level 5 visit.
We are proposing a payment rate of approximately $35.
• We are also proposing to consolidate the two add-on HCPCS G codes we finalized last year for primary care and
certain non-procedural specialty care into a single code describing the work associated with visits that are part of
ongoing, comprehensive primary care and/or visits that are part of ongoing care related to a patient’s single, serious,
or complex chronic condition. The proposed payment rate for this services is approximately $17.
* Current Payment for CY2019
**Proposed Payment based on the CY2020 proposed relative value units and the CY2019 payment rate
Level Current Payment*
(established patient)
Approximate Payment
Rates Finalized in 2019
for 2021
Proposed
Payment**
1 $22 $24 $24
2 $45$93
$60
3 $74 $96
4 $109 $136
5 $148 $148 $190
Level Current Payment*
(new patient)
Approximate Payment
Rates Finalized in 2019
for CY 2021
Proposed
Payment**
1 $45 $44 N/A
2 $76$135
$77
3 $110 $119
4 $167 $177
5 $211 $211 $232
11

Quality Payment Program
12

Proposed Changes to the Medicare Physician Fee Schedule for CY 2020
• Quality (40%): Remove low-bar, standard of care, process measures, focus on high-priority outcome measures, and add new specialty sets; increase sample to 70% for data completeness; introduce a benchmarking policy for 2022 payment year.
• Cost (20%): Add 10 episode-based measures and revise current global measures’ attribution methodologies (TPCC and MSPB Clinician).
• Improvement Activities (15%): Addition of 2 new Improvement Activities, modification of 7 existing Improvement Activities, removal of 15 existing Improvement Activities; new requirement for Improvement Activity credit for groups (at least 50% of MIPS eligible clinicians participate).
• Promoting Interoperability (25%): New reweighting standards for hospital-based MIPS eligible clinicians in groups; revised the Query of Prescription Drug Monitoring Program (PDMP) measure and removed the Verify Opioid Treatment Agreement measure in alignment with the Medicare PI program for eligible hospitals and CAHs.
• Performance threshold: 45 points; Exceptional performance Bonus: 80 points; payment adjustment (CY 2022): Up to 9%
• Changes to requirements for third-party intermediaries
• Introducing MIPS Value Pathways
Quality Payment Program Year 4 (2020)
13

Performance Category Weights:
Performance
Category
Performance
Category
Weights
Year 3
(2019)
Proposed Weights
Year 4 (2020)
Proposed Weights
Year 5 (2021)
Proposed Weights
Year 6 (2022)
Quality
45% 40% 35% 30%
Cost
15% 20% 35% 30%
Improvement
Activities
15% 15% 15% 15%
Promoting
Interoperability
25% 25% 25% 25%
MIPS Proposals for 2020
14

Payment Thresholds:
Performance Period Performance
Threshold
Exceptional
Performance BonusPayment
Adjustment*
Year 1 (2017) 3 points 70 points Up to +4%
Year 2 (2018) 15 points 70 points Up to +5%
Year 3 (2019) 30 points 75 points Up to +7%
Year 4 (2020)
Proposed45 points 80 points Up to +9%
Year 5 (2021)
Proposed60 points 85 points Up to +9%
*Payment adjustment (and exceptional performer bonus) is based on comparing final score to performance threshold and additional performance threshold for
exceptional performance. To ensure budget neutrality, positive MIPS payment adjustment factors are likely to be increased or decreased by an amount called a
“scaling factor.” The amount of the scaling factor depends on the distribution of final scores across all MIPS eligible clinicians.
MIPS Proposals for 2020
15

MIPS Value Pathways
CMS is proposing MIPS Value Pathways (MVPs) to create a new participation framework
beginning with the 2021 performance year. This new framework would:
• Unite and connect measures and activities across the Quality, Cost, Promoting
Interoperability, and Improvement Activities performance categories of MIPS
• Incorporate a set of administrative claims-based quality measures that focus on
population health/public health priorities
• Streamline MIPS reporting by limiting the number of required specialty or condition specific
measures
CMS encourages the health care community to review the Transforming MIPS: MIPS Value
Pathways Request for Information (RFI) and our illustrative diagram and submit formal
comments. We look forward to working with you to establish this new framework.16
MIPS Proposals for 2021 and Beyond
16

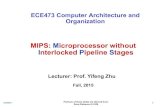
MIPS Value Pathways
17
Future State of MIPS(In Next 3-5 Years)
Current Structure ofMIPS(In 2020)
New MIPS Value PathwaysFramework(In Next 1-2 Years)
Building PathwaysFrameworkMIPS Value Pathways
Clinicians report on fewer measures and activities baseon specialty and/or outcome within a MIPS ValuePathway
Moving toValue
Fully ImplementedPathwaysContinue to increase CMS provided data and feedback to
reduce reporting burden on clinicians
• Many Choices
• Not MeaningfullyAligned
• Higher Reporting Burden
• Cohesive
• Lower Reporting Burden
• Focused Participation around Pathways that are Meaningful to Clinician’s Practice/Specialty or Public Health Priority
• Simplified
• Increased Voice of thePatient
• Increased CMS Provided Data
• Facilitates Movement to Alternative Payment Models (APMs)
2-4Activities
ImprovementActivities
Quality
6+Measures
PromotingInteroperability
6+Measures
Cost
1 or MoreMeasures
Cost
Quality and IA aligned
Foundation
Promoting Interoperability
Population Health Measures
Foundation
Promoting Interoperability
Population Health Measures
Enhanced Performance Feedback
Patient-Reported Outcomes
Value
Quality ImprovementActivities
Cost
We Need Your Feedback on:
Population Health Measures: a set of administrative claims-based quality measures that focus on public health priorities and/or cross-cutting population health issues;
CMS provides the data through administrative claims measures, for example, the All-Cause Hospital Readmissionmeasure.
Goal is for clinicians to report less burdensome data as MIPS evolves and for CMS to provide more datathrough
administrative claims and enhanced performance feedback that is meaningful to clinicians and patients.Clinician/Group Reported Data CMS Provided Data
Pathways:
What should be the structure and focus of the Pathways? What criteria
should we use to select measures and activities?
Participation:
What policies are needed for small practices and multi-specialty practices?
Should there be a choice of measures and activities within Pathways?
Public Reporting:
How should information be reported to patients?
Should we move toward reporting at the individual clinician level?

MIPS Value Pathways RFI Webinar
18
Webinar Details
Title: MIPS Value Pathways RFI webinar
Date: Wednesday, September 4, 2019
Time: 1:30 – 2:30 p.m. ET
Registration Link:
https://protect2.fireeye.com/url?k=9913072
8-c5472e03-99133617-0cc47a6d17cc-
51273c02e636e49a&u=https://engage.vev
ent.com/rt/cms/index.jsp?seid=1617

19
Technical AssistanceAvailable Resources
Learn more about technical assistance: https://qpp.cms.gov/about/help-and-support#technical-assistance

Opioid Treatment Programs
20

Proposed Changes to the Medicare Physician Fee Schedule for CY 2020
• Section 2005 of the SUPPORT Act establishes a new Medicare Part B benefit for opioid use disorder (OUD) treatment services furnished by OTPs on or after January 1, 2020
• Medicare currently covers office-based opioid treatment with buprenorphine and naltrexone but has historically not covered OTPs, which are the only entities authorized to use methadone for the treatment of OUD. Coverage of OTPs is a new benefit that we anticipate will expand access to care
• OTP proposals in the NPRM:
- Definition of opioid treatment programs
- OUD treatment service provided by OTPs
- Coding structure for OUD treatment services
- Payments (partial episodes, add-on code for intensity)
- Use of telecommunications
Opioid Treatment Programs (OTPs)
21

• We are proposing to set the copayment at zero for a time-limited duration (for example, for the duration of the national opioid crisis), as we believe this would minimize barriers to patient access to OUD treatment services.
• Setting the copayment at zero also ensures Medicare-enrolled OTP providers receive the full Medicare payment amount for Medicare beneficiaries if secondary payers are not available or do not pay the copayment, especially for those dually eligible for Medicare and Medicaid.
• We intend to continue to monitor the opioid crisis in order to determine at what point inthe future a copayment may be imposed. At such a time we deem appropriate, we wouldinstitute cost sharing through future notice and comment rulemaking.
• The Part B deductible would apply for OUD treatment services, as mandated for all Part B services by section 1833(b) of the Act.
OTP Proposals: Beneficiary Copayment
22

In order to enroll with Medicare, OTPs must be certified by SAMHSA and accredited by a SAMHSA-approved accrediting body.
For more information on the accreditation process, visit SAMHSA’s Certification of
Opioid Treatment Programs (OTPs) webpage.
OTP Enrollment
23

Outpatient Prospective Payment System (OPPS) & Ambulatory
Surgery Center (ASC) Proposed Rule
24

Outpatient Prospective Payment System (OPPS) & Ambulatory Surgical Center (ASC) Proposed Rule
• Proposed OPPS update of 2.7 percent
• Proposed ASC update of 2.7 percent
• Changes to the Inpatient Only List
• Addresses Wage Disparities to Aid Rural Health
• Changes to Hospital Outpatient Quality Reporting and ASC Quality Reporting Programs to Further Meaningful Measures Initiative
General Provisions
25

Price Transparency
26

• On June 24, the President signed an Executive Order on Improving Price and Quality Transparency in American Healthcare to Put Patients First:- Policy of the Federal Government to increase the availability of meaningful price and
quality information for patients- Directed the Secretary of HHS to propose a regulation, consistent with applicable law,
to require hospitals to publicly post standard charge information
• Proposed rule implements Section 2718(e) of the Public Health Service Act and improves upon prior agency guidance that required hospitals to make public their standard charges upon request starting in 2015 (79 FR 50146) and subsequently online in a machine-readable format starting in 2019 (83 FR 41144)
• Section 2718(e) requires each hospital operating within the United States to establish (and update) and make public a yearly list of the hospital’s standard charges for items and services provided by the hospital, including for diagnosis-related groups established under section 1886(d)(4) of the Social Security Act
Increasing Price Transparency of Hospital Standard Charges
27

• Proposing that hospitals make public their standard charges (both gross charges and payer-specific negotiated charges) for all items and services online in a single file that is machine-readable
• Propose the hospital must include the following corresponding data elements:- Description of each item or service provided by the hospital- Gross charge that applies to each individual item or service- Payer-specific negotiated charge that applies to each item or service; each list of payer-specific
charges must be clearly associated with the name of the third party payer- Any code used by the hospital for purposes of accounting or billing for the service (e.g. CPT,
HCPCS, DRG)- Revenue codes, as applicable
• Propose the following location and accessibility requirements:- Hospital may select an appropriate publicly available website for making the file public- File must be displayed in a prominent manner and clearly identified with the hospital location- Hospital must ensure the data is easily accessible and without barriers
Proposed Requirements for Making Public All Standard Charges for All Items and Services
28

• Display payer-specific negotiated charges for at least 300 shoppable services, including 70 CMS-selected shoppable services and 230 hospital-selected shoppable services. If a hospital does not provide one or more of the 70 CMS selected shoppable services, the hospital must select additional shoppable services such that the total number of shoppable services is at least 300.
• Propose to define ‘shoppable service’ as a service that can be scheduled by a health care consumer in advance.
• In their display of shoppable services, hospitals would:- Include charges for services that the hospital customarily provides in conjunction with the
primary service that is identified by a common billing code (e.g. CPT/HCPCS/DRG)- Make sure that the charge information is displayed prominently on a publicly available webpage
and clearly identifies the hospital (or hospital location)- Information must be easily accessible and without barriers, and searchable- Update the information at least annually
Proposed Requirements for Making Public Consumer-Friendly Standard Charges for a Limited Set of ‘Shoppable Services’
29

• Proposing regulations for monitoring and enforcement of hospitals’ compliance with these requirements
• CMS would have the authority to monitor hospital compliance with Section 2718(e) of the Public Health Service Act, by evaluating complaints made by individuals or entities to CMS, reviewing individuals’ or entities’ analysis of noncompliance, and auditing hospitals’ websites:- Should CMS conclude a hospital is noncompliant with one or more of the requirements to make
public standard charges, CMS may provide a warning notice to the hospital, or a corrective action plan.
- If the hospital fails to respond to CMS’ request to submit a corrective action plan or comply with the requirements of a corrective action plan, CMS may impose a civil monetary penalty on the hospital not in excess of $300 per day, and publicize these penalties on a CMS website
- Also propose to establish an appeals process for hospitals to request a hearing before an Administrative Law Judge (ALJ) of the civil monetary penalty
Proposals for Monitoring and Enforcement
30

• CMS is soliciting feedback on the best way to capture information on the quality of hospital inpatient care so that information can be provided to patients in a way that is useful for them when comparing care options
• Specifically, we are seeking comment on:- Improving availability and access to existing quality of health care information for third parties and
health care entities to use when developing price transparency tools and when communicating charges for health care services
- Improving incentives and assessing the ability of health care providers and suppliers to communicate and share charge information with patients
Request for Information
31

Site Neutrality
32

• Proposed rule includes policies that reduce payment differences between certain outpatient sites of service so that patients can:- Benefit from high-quality care at lower costs- Receive care that is provided safely and is clinically appropriate
Increasing Choices and Encouraging Site Neutrality
33

• Completing two-year phase-in by addressing payments for clinic visits furnished in the off-campus hospital outpatient setting- Clinic visits are the most common service billed under the Outpatient Prospective Payment
System (OPPS)- CMS and beneficiaries often pay more for the same type of clinic visit in the hospital
outpatient setting than in the physician office setting- Proposed change would result in lower copayments for beneficiaries and savings for the
Medicare program and taxpayers estimated to be a total of $810 million for 2020
Example: For a clinic visit furnished in an excepted off-campus provider-based department, average beneficiary cost sharing is currently $16 in CY 2019, but would be $23 absent this policy. With the completion of the two-year phase-in, that cost sharing would be reduced to $9, saving beneficiaries an average of $14 each time they visit an off-campus department for a clinic visit in CY 2020.
Method to Control for Unnecessary Increases in Utilization of Outpatient Services
34

ESRD PPS and DMEPOS Proposed Rule
35

Proposed Changes to ESRD PPS and DMEPOS Fee Schedule (2020)
• Implementing President’s Executive Order on Advancing American Kidney Health to better recognize costs for new therapies under the ESRD PPS
• Proposing a transitional add-on payment adjustment for new and innovative equipment/supplies
• Proposing refinements to eligibility for the transitional drug add-on payment adjustment (TDAPA)
• Soliciting comments on stakeholder concerns regarding wage index used to adjust labor-related portion of ESRD PPS base rate
• Proposing how Medicare pricing is determined for new DMEPOS items without a pricing history
General Provisions
36

How to Comment on the 2020 Proposed Rules
Comments due no later than Friday, September 27, 2019 at 5:00 PM
37
Rule Press Release Fact Sheet Comment at FederalRegister
Physician Fee Schedule (CMS-1715-P)
https://www.cms.gov/newsroom/press-releases/trump-administrations-patients-over-paperwork-delivers-doctors
https://www.cms.gov/newsroom/fact-sheets/proposed-policy-payment-and-quality-provisions-changes-medicare-physician-fee-schedule-calendar-year-2QPP: https://qpp-cm-prod-content.s3.amazonaws.com/uploads/594/2020%20QPP%20Proposed%20Rule%20Fact%20Sheet.pdf
https://www.federalregister.gov/documents/2019/08/14/2019-16041/medicare-program-cy-2020-revisions-to-payment-policies-under-the-physician-fee-schedule-and-other
OPPS (CMS-1717-P) https://www.cms.gov/newsroom/press-releases/cms-takes-bold-action-implement-key-elements-president-trumps-executive-order-empower-patients-price
https://www.cms.gov/newsroom/fact-sheets/cy-2020-medicare-hospital-outpatient-prospective-payment-system-and-ambulatory-surgical-center
https://www.federalregister.gov/documents/2019/08/09/2019-16107/medicare-program-proposed-changes-to-hospital-outpatient-prospective-payment-and-ambulatory-surgical
ESRD/DME (CMS-1713-P) https://www.cms.gov/newsroom/press-releases/new-cms-proposals-strengthen-medicare-unleash-innovation-and-promote-competition-provide-kidney
https://www.cms.gov/newsroom/fact-sheets/end-stage-renal-disease-esrd-and-durable-medical-equipment-prosthetics-orthotics-and-supplies-dmepos
https://www.federalregister.gov/documents/2019/08/06/2019-16369/medicare-program-end-stage-renal-disease-prospective-payment-system-payment-for-renal-dialysis
Submit via: electronically through Regulations.gov; regular mail; express/overnight mail; by hand/courier (faxes NOT accepted)