Pressure Ulcer Prevention And Management Policy 2015 · 2014,NPUAP/EPUAP 2014).In...
39
Pressure Ulcer Prevention And Management Policy 2015
Transcript of Pressure Ulcer Prevention And Management Policy 2015 · 2014,NPUAP/EPUAP 2014).In...

Pressure Ulcer PreventionAnd
Management Policy
2015

Policy Amendments
Version No. Amendments
Copy of this form to be given to Information Governance Officer
Typei.e. Strategy, Policy,
Education Package etc.Policy
Name Pressure Ulcer Prevention and Management Policy
Categoryi.e. organisational, clinical,
Corporate, Finance etcOrganisational
Version 6
Author Jane Le Ruez Lane
Approved byi.e. Operational
Governance Group
Chief Executive Officer – Julie Gafoor
Date Approved29/06/15
Review Date 29/06/18
Person responsible for
review
Approved by i.e.Sub
Committee, H&SS
FAMILY NURSING & HOME CARE RATIFICATION FORM

1.0 Statement of Intent
1.1 Rationale
New pressure ulcers affect an unknown proportion of people in the community as reliable data is not available, but it is estimated that up to 30% of patients may suffer and up to 20% of patients in nursing & residential homes may be affected (NHS Institute of Innovation & Improvement 2013)
The effective management of pressure ulcers and pressure ulcer prevention is dependent upon initial nursing, allied health professionals and physician assessment to identify those patients at risk. Pressure ulcers are a huge financial burden, estimated to cost the NHS up to four billion pounds per year with the most severe cases ranging from £11,000 to £40,000 per person (National Patient Safety Agency (NPSA) 2010).
The Patient Safety Group has identified that the Prevention & Management of Pressure Trauma is high on their agenda of priorities. The community environment can be a challenging one and it requires collaboration from all health care providers to ensure all staff and patients are working towards one shared goal. (Collaborate Working in the Community Setting to reduce Pressure Ulcers; Wound Essentials 2014, Vol 9 No 1). This is important to remember when aiming to prevent and manage pressure trauma in the community.
1.2 Scope/Responsibility
The prevention and management of pressure ulcers is an organisational priority and a Family Nursing & Home Care responsibility, therefore this policy applies to all clinicians and their managers employed within Family Nursing & Home Care.
2.0 DEFINITION
Pressure ulcers are areas of damaged skin and tissue. They develop when pressure cuts off local blood supply, usually through a combination of patient factors including impaired mobility, impaired circulation, obesity, emaciation, skin integrity and care factors such as positional changes, support surfaces or skin care. A pressure ulcer is a localised injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear (National Pressure Ulcer Advisory Panel / European Pressure Ulcer Advisory Panel (NPUAP/ EPUAP) 2014).
3.0 POLICY
The aims of this policy are;
To ensure a cultural shift towards the prevention rather than the management of pressure ulcers throughout Family Nursing & Home Care and commits the organisation to ensuring that there are effective arrangements for pressure ulcer prevention and management whilst patient’s are on a Family Nursing & Home Care caseload and following discharge from the caseload.

To ensure that all patients at risk of developing pressure ulcers and any adult patients who have developed pressure ulcers are appropriately assessed and have a plan of care to include a post discharge plan to promote healing & minimise further risk to healthy tissue
To minimise the physical, psychological and financial cost of pressure ulcers to the patient and to Family Nursing & Home Care
To ensure that Family Nursing & Home Care complies with national guidance and evidence based high quality care
4. ROLES AND RESPONSIBILITES
4.1 Individual Clinical staff
Will be aware of and adhere to the Family Nursing & Home Care Pressure Ulcer Prevention and Management Policy
Will ensure pressure ulcer prevention strategies are utilised for all patients Will identify and manage any training needs and ensure they are trained in
pressure ulcer prevention and management principles Will observe, evaluate and plan the care necessary for the prevention and
management of the patient’s pressure ulcer using the ‘SSKIN’ approach(Surface. Skin, Keep Moving, Incontinence and Nutrition) see Appendix 4
Will adhere to the “reporting process for all patients identified with pressure trauma” Appendix 9
Will ensure that any pressure redistribution equipment is used in concordance with manufacturer’s instructions
Will ensure pressure ulcer prevention and management strategies and treatment options/decisions are communicated effectively to patients and their relatives/families (where appropriate) and that this is documented in the patient’s nursing records.
Will ensure that the patient & relatives understand the cost implications and the importance of concordance and that this is documented in the patient’s nursing records.
Will ensure that the patients and relatives have been given documented advice and a Patient Information Leaflet “Preventing Pressure Trauma” on discharge from the caseload which has been explained & is understood by the patient & carer
Will be responsible for the timely and accurate documentation of all prevention and management strategies employed and ensuringcommunication between patients/families and carers has been conducted.
4.2 Line Managers
Will be aware of and adhere to the Family Nursing & Home Care Pressure Ulcer Prevention and Management Policy.
Will actively promote pressure ulcer prevention care strategies for all patients.
Will ensure the Pressure Ulcer Prevention and Management Policy is distributed and promoted within all clinical areas and to all health care professionals.
Will identify and manage any training needs and ensure they are trained in pressure ulcer prevention and management principles.

Will ensure that any pressure ulcer warranting reporting is done so as outlined in this policy.
Will observe, evaluate and plan the care necessary for the management of the patient’s pressure ulcer. This management plan will be communicated to the primary nurse or the Nurse in Charge (and all plans of care will be documented in the patient’s nursing records.
4.3 Senior Management Team
Will ensure that the policy is updated and that there are processes in place to ensure that all relevant staff are aware of it and have ease of access to it.
Will continue to work with commissioners regarding the promotion of pressure redistribution equipment for all patients as required and will take into account its clinical effectiveness, educational requirements of staff and financial factors.
Will investigate any failure to comply with this policy. Will take action to prevent recurrence of reported incidences. Will ensure the provision and management of a Tissue Viability Nurse
Specialist for all clinical areas.
4.4 Tissue Viability Nurse Specialist / Patient Safety Facilitator/Education
Will lead on the implementation of the Policy throughout Family Nursing & Home Care
Will ensure that the Pressure Ulcer Care documentation and associated policy is reviewed as regularly as necessitated by the contemporary evidence base
Will support all clinical areas in the dissemination of this policy and supporting care documentation
Will liaise with other members of the organisation to ensure that practice is developed in light of contemporary evidence and best practice guidance
Will lead on pressure ulcer training in liaison with and through collaborative working with allied health care professionals and the education department
Monitoring the progress/outcomes of all pressure ulcers using the Assure system
Will write an annual report in relation to pressure ulcer incidence
5. PREVENTION OF PRESSURE ULCERS
5.1 Pressure Ulcer Risk Assessment All adult patients should have their risk of pressure trauma assessed on the first visit by a Registered nurse. (Best Practice Statement, (BPS), 2013)
All infants, children and young people should have an assessment of pressure trauma risk, carried out by a Register Nurse on admission to the Children’s Community Nursing Team if they have a risk factor e.g.;
Significantly limited mobility
Significant loss of sensation
A previous or current pressure ulcer
Nutritional deficiency
The inability to reposition themselves
Significant cognitive impairment

(National Institute of Clinical Excellence 2014 p.15)
A validated pressure ulcer risk assessment tool should be used. In adult care the Waterlow Pressure Ulcer Risk Assessment Tool is the one of choice and for paediatric care the Braden Q scale should be used for predicting paediatric pressure ulcer risk.
When it is not possible to assess risk on the first visit, a clear rationale must be documented with a plan to undertake the risk assessment on the next visit.
The outcome of any informal risk assessment should be documented in the patient’s nursing records alongside any management strategies implemented.
The Pressure Ulcer Risk Assessment tools of choice are evidence based to aid decision making and standardise care delivery. The outcome of the Waterlow score& Braden Q should not be considered in isolation but should facilitate clinical decision making enabling appropriate cost effective preventative aids and nursing resources to be allocated (Waterlow 2005). It is important that those at risk of pressure ulcers are identified early and appropriate prevention measures are implemented without delay.
As a minimum requirement, individual risk assessment should be repeated at regular intervals thereafter depending on clinical need and as a minimum of every 3 months in the community (Best Practice Statement, (BPS), 2013) (see appendix 11). If there is a change in the clinical status of the individual or worsening of an underlying condition or a change in mobility, then a reassessment of risk will need to be undertaken (National Institute for Clinical Excellence (NICE) 2014,NPUAP/EPUAP 2014).In addition, reassessment of risk should be undertaken following discharge from a respite setting or any hospital discharge.
All patients identified as being at risk of developing pressure ulcers will be offered a patient information leaflet relating to the prevention of pressure trauma (Appendix 9) Any patient with an ‘at risk’ status must be communicated during the teamhandover process, as well as being clearly documented in any base & community held nursing records. It is the responsibility of the individual nurse to ensure that records are maintained, are legible, clear and are entered in a timely manner (Nursing and Midwifery Council 2015)
Any identified tissue damage must be documented on the Pressure Ulcer Risk Assessment and any Grade 2 pressure ulcers (or above) must be communicated in writing to the patients General Practitioner G.P, and a copy of the letter kept in thepatient’s nursing records. All grades of pressure trauma must be reported on the “Assure” reporting system within 24hrs.
5.2 Pressure Ulcer Grade Recording Chart
The Pressure Ulcer Recording Chart (Appendix 1, Front) utilises a body mapping concept, which ensures that all adult patients are fully assessed in terms of skin integrity and allows for the early identification of tissue compromise. Documentation of skin damage must be identified, dated and signed on the patient diagram to include any bruising, abrasions, lacerations, rashes, moisture lesions, pressure ulcers or free text descriptions of additional damage. This will be communicated to the patient’s General Practitioner (G.P) as part of the holistic assessment and care provision for patients.
All patients should have a skin assessment undertaken by a registered nurse. Health Care Assistants (HCA’s) are permitted to undertake skin assessments if

they are deemed competent to do so, however, the registered nurse, responsible for the care of the patient, will remain professionally accountable.
Prior to undertaking any skin inspection, the registered nurse must ensure that the rationale for skin inspection is communicated to the individual and consent is obtained as dictated by professional and organisational guidelines and policy. For those patients who decline a skin assessment or are deemed to be low risk, a verbal confirmation that they have no sore, painful or broken areas may be recorded. This must be documented as self reported on the Pressure Ulcer Risk Assessment (Waterlow) in the comments section.
5.3 Clinical Photography
Any photographic records made for clinical purposes form part of a patients record and must adhere to FNHC guidelines for clinical photography.Photographs, which are taken, must not be used for any other purpose other than the patient’s care or the audit of that care, without the express consent of the patient.
5.4 Classification of Pressure Ulcers
Grading of the pressure damage will be conducted in concordance with the European Pressure Ulcer Advisory Panel (EPUAP 2014) Grading Guide. Pressure ulcer grading dictates that pressure ulcers should not be reverse graded, i.e. a grade 3 ulcer that is healing should be described as a “grade 3 healing ulcer” and not as a grade 2 (NPUAP/EPUAP 2014). A deteriorating pressure ulcer, i.e. from a grade 2 to a grade 3, will require the completion of an additional incident report.
For those patients who have been assessed as having non-blanching erythema (Grade 1 pressure damage) (Appendix 2) appropriate prevention actions should be implemented with subsequent skin assessment considered at least daily.“In the community it is rare occurrence that carers are available 24hrs a day. Therefore there need to be collaboration between the patient, informal carers and the community nurse with each person working to one plan of care to meet the needs of the individual “(ref; Collaborative Working in the Community Settings to reduce pressure ulcers Wound Essential 2014 Vol 9 No1)
Any pressure ulcer identified, as a Grade 3 or Grade 4 or multiple Grade 2, should have the grading confirmed by a senior nurse (grade 6 or 5) & a referral completed for the Tissue Viability Nurse and communicated to the patient’s G.P. The senior nurse, will be responsible for devising and communicating a management plan to the relevant practitioners responsible for delivering care.
5.5 Moisture Lesions
There is often confusion in recognising a superficial pressure ulcer and a lesion caused by moisture, which is usually associated with incontinence (Voegeli 2011). The differentiation is important (Appendix 3) as patient outcomes may be adversely affected since prevention and treatment strategies may differ.
5.6 Patient information leaflet
All at risk patients should be given timely, tailored information about managing the risks of pressure damage from practitioners delivering their care (NICE 2014). A Preventing Pressure Trauma patient information leaflet (Appendix 9) should be given to all patients and/or relatives (where appropriate) identified as being at risk.

6. MANAGEMENT OF PRESSURE ULCER RISK
6.1 SSKIN Bundle
The SSKIN Bundle is a bundle of care that involves fundamental components of pressure ulcer preventative interventions. It is crucial to remember that if only one of those components was to be omitted in the delivery of healthcare for patients at risk, the consequence is likely to be the development of a pressure ulcer.
The SSKIN Bundle will be completed for all patients identified to be at risk of developing a pressure ulcer, i.e. with a Waterlow above 10 or deemed to be at risk by the registered nurse’s clinical judgment. For paediatric care the Braden Q scale is the risk assessment of choice
The patient will have a full skin assessment in conjunction with the Waterlow/Braden Q and this will be recorded on the Pressure Ulcer Risk Assessment (Waterlow)/Braden Q Risk Assessment.
A registered nurse will initiate the SSKIN Bundle and complete all sectionsThis includes;
Patients name, URN Number and case load and Waterlow score The specific mattress and cushion required, agreement with patient to
purchase the date of the order, delivery and fitting The frequency of skin assessment based on the registered nurse clinical
judgement of the patient’s need; daily / twice weekly / weekly / monthly / 3 monthly
The patient’s current regime of movement in relation to when they get up or go back to bed or mobilise to the toilet
The advise given to the patient and/or carer regarding repositioning The MUST score and date to review this
Page 2 of the SSKIN bundle must be completed as identified by the frequency of assessment on page 1
Any member of the healthcare / social team can complete the 2nd page of the SSKIN Bundle
If the patient is known to the District Nursing Services for 3 / 6/ 12 monthly interventions (including continence assessment) and is at risk of developing a pressure ulcer, the registered nurse will offer advice to the patient and/or carer and provide Patient Information Leaflet “Preventing Pressure Trauma”.The advice will be recorded in the patient’s records.
If pressure relieving support surfaces are ordered at this point, a follow up visit will be arranged to evaluate the effectiveness of the support surfaces
If the patient is receiving healthcare from, Rapid Response and Reablement Team,

The pressure ulcer risk assessment (Waterlow) will be carried out on the first visit.
If this visit is not undertaken by a registered nurse, the assessment will be carried out by a competent health care worker.
If the patient is found to be at risk of developing pressure ulcers, the Healthcare worker will inform the registered nurse within the team of this risk.
The registered nurse within the team will implement the SSKIN Bundle
If the patient is having additional support from care agencies, the registered nursewill perform the Waterlow assessment and initiate the SSKIN Bundle on first visit.
If other agencies are involved the registered nurse should encourage them with support to complete the second page of the SSKIN bundle'.
If a patient decides not to accept the registered nurses advice or declines to purchase the recommended dressings/equipment, then this must be clearly documented in the patients nursing records on the back of the SSKIN bundle and base card & a risk assessment of the concerns carried out. (refer to the what to do if the patient refuses treatment page appendix 12)
If a patient with an at risk status is discharged from a FNHC caseload, evidence that advice on the prevention of pressure trauma has been discussed with the patient and carers and that the patient and carers have a copy of the FNHC Patient Information Leaflet “Preventing Pressure Trauma” . This must be clearly documented within the patients nursing records.
6.2 Surface
It is important to use a suitable support surface as deemed appropriate such as high specification foam mattresses/cushion or alternating air mattresses replacement system to assist in the prevention of pressure ulcers (NICE.2014)“However community nurses face different challenges with equipment installation and patients will make decisions based on the aesthetics of the equipment rather than functionality“(ref Collaborative working in the community settings to reduce pressure ulcers Wound Essential 2014 Vol 9 No1)In Jersey at Family Nursing & Home Care community staff face further challenges of equipment provision where the costs are borne by the patients. This causes further dilemma in relation to cost versus best practice advice and guidance.To overcome this, FNHC are working closely with service providers to ensure a good quality range of pressure relieving equipment at competitive prices & the organisation is also working with the Commissioners of our services regarding equipment provision.
6.3 Skin Inspection
Observation and management of an individual’s skin integrity will reduce the incidence of skin deterioration and breakdown. Therefore a regular skin inspection regimen must be undertaken and documented for those who are at risk of pressure ulcers, have had a previous pressure ulcer or have an existing pressure ulcer. Particular attention should be paid to high-risk areas and include inspection for localised heat, oedema or induration (hardness) (NPUAP/EPUAP 2014).
6.4 Keep Moving
All at risk individuals and their carers should be advised regarding the importance of repositioning as frequently as clinically indicated. Individuals should be encouraged to actively participate in mobilising and repositioning as their condition

dictates and referral to the physiotherapist and occupational therapist should be considered where there is a need for assessment and support.
6.5 Incontinence/Moisture
Moisture next to the skin puts the skin at greater risk from maceration, friction and shearing forces (NPUAP / EPUAP 2014, Waterlow 2005), therefore effective management of incontinence is an essential part of skin care and fundamental to maintaining a person’s dignity and comfort. Continence aids must be utilised as appropriate for the patient and practitioners should use opportunities during the turning schedule to cleanse and dry the skin of individuals who have been incontinent.
Skin cleansing regimes must be selected that optimise skin integrity ensuring gentle cleansing and the application of a suitable skin barrier product if indicated (Beeckman et al 2009) (NPUAP/EPUAP 2014)
6.6 Nutrition
Nutrition and hydration are extremely important contributory factors in a patient’s ability to avoid pressure ulcers (Waterlow 2005), therefore all patients at risk must have nutritional screening undertaken (NPUAP/EPUAP 2014) and documented utilising the organisationally approved nutritional assessment tool. The use of food intake diaries and fluid balance charts may be utilised as a means of monitoring dietary and fluid intake.If indicated, following the assessment outcomes, a referral to the dietician must be instigated and documented.
It remains the professional responsibility of the qualified practitioner to utilise clinical judgement as to whether nutritional screening is undertaken in patients whose episode of care is <24 hours. The qualified practitioner must ensure that any screening and outcomes are documented in the patient’s notes.
7. REPOSITIONING
7.1 Repositioning Chart
The use of repositioning could be considered in specific situations for at risk patients to reduce the duration and magnitude of pressure over vulnerable areas of the body with consideration given to the individual’s comfort, dignity, functional ability and the properties of the support surfaces they are being nursed on (NPUAP/EPUAP2014).
The Repositioning Chart (Appendix 5) allows for the documentation of a schedule of care including repositioning, pain (NPUAP/EPUAP2014), tissue tolerance and turning schedule, skin observations and other personal care interventions appropriate to the individual patient, e.g. mouth care, and eye care etc.
“In the community it is rare occurrence that carers are available 24hrs a day. Therefore there need to be collaboration between the patient, informal carers and the community nurse with each person working to one plan of care to meet the needs of the individual “(ref Collaborative working in the community settings to reduce pressure ulcers Wound Essential 2014 Vol 9 No1)
8. WOUND MANAGEMENT

8.1 Wound Assessment Chart
A Wound Assessment Chart (Appendix 6) must be completed for any patient with an identified pressure ulcer (Grade 2 and above within 24 hrs of referral into FNHC. This should be updated regularly and communicated to the patient’s G.P. The effectiveness of a wound management plan must be evaluated at each dressing change. Advice should be sought from the TVN in the event of complex pressure ulcer management or if dressing advice is needed.
The dimensions of all pressure ulcers should be documented and if possible, a validated measurement technique should be used e.g. transparency tracing or a photograph (NICE 2014). The use of photography must comply with organisational guidelines and will form part of the patient’s nursing records. Organisational consent and confidentiality policies must be adhered to.
8.2 Formulary
Pressure ulcers will be treated and dressed in concordance with the FNHC & Health & Social Services (HSSD) Dressing and Wound Formulary. All Grade 3, 4 and multiple Grade 2 pressure ulcers requiring dressing/treatment advice should be discussed, in the first instance, with the TVNS. An individual plan of care will then be formulated which should be communicated to all healthcare professionalsinvolved in the care of the patients pressure ulcer.
The FNHC & HSSD Dressing Formulary will be managed by the TVNS (in collaboration with HSSD) so as to ensure dressing usage is based on contemporary evidence and best practice guidance and is standardised across the community & HSSD.
8.3 Dressings
The type of dressing selected to promote healing of a pressure ulcer should be discussed with the individual and their family or carers if appropriate. In particular, dressings that promote a warm and moist wound healing environment to treat grade 2, 3 and 4 pressure ulcers should be considered (NICE 2014).
8.4 Debridement
Sharp Debridement should only be undertaken by a qualified practitioner or medical professional competent to undertake the procedure. As autolytic debridement is likely to take longer and prolong healing time, the utilisation of sharp debridement may need to be considered (NICE 2014).
9. Transferred Care
All incidences of damage to skin integrity must be communicated to receiving providers of care on discharge and supported with documentation to ensure continuity between care settings and agencies. When possible communication should take place prior to discharge and include any need for specialist services, equipment or dressings. It is recommended that a copy of the SSKIN bundle and assessment accompany the patient and the new providers of care are instructed on how to complete Page 2 at the recommended frequency.

10. EQUIPMENT
10.1 Repositioning equipment
All staff must undertake the mandatory organisational training for Safe Handling prior to using any of the moving and handling hoists or any other repositioning equipment. It is the responsibility of the individual practitioner to ensure that they are familiar and competent to undertake any safe handling procedure.
11. INCIDENT REPORTING
11.1 Assure/Datix
ALL identified pressure ulcers, including Grade1, that occur whilst the patient is on a FNHC caseload will be reported utilising the Assure incident reporting system. Identification of the area, size and grade should be detailed on the Assure report (Appendix 14).
Additional information, such as whether the pressure ulcer existed prior to admission, was identified following transfer between clinical areas, or occurred whilst in care must be recorded. Other mitigating factors such as patient acuity or issues with compliance must also be documented.
A Datix form must also be completed for patients who are discharged from an HSSD premises with unreported pressure trauma or for those patients that acquire a Grade 3 or 4 pressure ulcer within 72hrs post discharge. (Appendix 13)
11.2 Safeguarding
A Reporting Process for Pressure Ulcers (Appendix 10) must be adhered to when concerns have been raised regarding an incidence of significant pressure damage. Incidences of significant pressure damage are indicated by multiple pressure ulcers of grade 2 or a grade 3 or 4 classified in accordance with the NPUAP classification system (Appendix 2) (The Royal Borough of Kensington and Chelsea NHS Trust 2014).
In the event that multiple grade 2 pressure ulcers are identified or a grade 3 or 4 the senior nurse in the team must be notified & consult with the Tissue Viability Nurse to confirm classification and assist in the development of a management plan. Photographic evidence to support classification and reporting should be provided and consent for clinical photography should be sought in line with organisational consent and clinical photography guidelines. The patient’s GP must be informed.
The Safeguarding Lead for Family Nursing & Home Care / Patient Safety Facilitator and Tissue Viability Nurse will have collective responsibility for gathering the information required and will utilise the Adult Safeguarding Trigger Tool (Appendix 7) to establish if any further action is required.
The Adult Safeguarding Trigger Tool provides a focus on the thresholds for referral through the Adult Safeguarding Process however this does not negate the need to consider a safeguarding concern outside the thresholds.
The appropriate safeguarding process should be followed where a child is involved.

11.3 Root Cause Analysis (RCA)
All incidences of significant pressure damage that occur whilst a patient is on a Family Nursing & Home Care caseload will be investigated to establish the root cause. This will be conducted by the nominated investigators (Senior Sister (Grade 6)/ Patient Safety Facilitator/Tissue Viability Nurse) as outlined in the ReportingProcess for Pressure Ulcers (Appendix 10). All investigations pertaining to the reporting of multiple grade 2 pressure ulcers or a grade 3 or 4 pressure ulcer will be investigated utilising the Family Nursing & Home Care Concise Root Cause Analysis Investigation Report (Appendix 8).Following the completion of the root cause analysis a Senior Sister /Tissue Viability Nurse/Patient Safety Facilitator/ or the Operational Lead will be responsible for disseminating the outcomes and ensuring that any recommendations are implemented.
11.4 Auditing
Audits will be conducted as part of the FNHC annual audit plan and reviewed to ascertain compliance with the recommendations of this policy as well as establishing the prevalence rates of pressure trauma. The Tissue Viability Nurse Specialist will be responsible for undertaking and disseminating the results of the audits conducted across the organisation.
12. TRAINING
12.1 Educational Strategy for Pressure Ulcer Prevention and Management
The education of staff in the prevention and management of pressure ulcers is anorganisational priority. This will be led by the Tissue Viability Nurse Specialist in collaboration with the Patient Safety Facilitator and the Education & Development Coordinator.
It is the responsibility of each individual health professional to identify any deficits in their knowledge and take action to ensure their practice complies with local policy and procedures.
13. CONSULTATION
Name and Title of Individual
Tia Hall Operational Lead Adult ServicesJean Hinks Operational Lead Home CareMichelle Cumming Operational Lead Child & FamilyElspeth SnowieClinical Effectiveness FacilitatorAnne Marie WilkieDistrict Nursing SisterGilly GlendewarTissue Viability Community SisterTerena BiddulphDistrict Nursing Team Leader

14. REFERENCE DOCUMENTS
States of Jersey Health & Social Services Pressure Ulcer Prevention & Management Policy (Adults) 2014
Collaborative working in the community setting to reduce pressure ulcers.82 wound essentials 2014, Vol 9,No1
Beeckman D, Schoonhoven L, Verhaeghe S, Heyneman A and Defloor T (2009) Prevention and Treatment of incontinence-associated dermatitis: literature review. Journal of Advanced Nursing. Vol 65. No 6. Pg 1141-1154.
Defloor et al (2005). Differentiation between pressure ulcers and moisture lesions. European Pressure Ulcer Advisory Panel Reviews. Vol 6. Issue 3.
Essence of Care (2010) Benchmarks for Prevention and Management of Pressure Ulcers. Department of Health. The Stationary Office.
European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel (2014) Prevention and treatment of pressure ulcers: quick reference guide. Washington DC. Available online at www.epuap.org/guidelines/Final_Quick_Prevention.pdf
McIntyre, L., May, R. and Marks-Maran, D. (2012) A strategy to reduce avoidable pressure ulcers. Nursing Times, 108 (29), pp 14-17.
National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel. (NPUAP/EPUAP) (2009) Prevention and treatment of pressure ulcers: Clinical Practice Guideline. Washington DC.
National Patient Safety Agency (2010) NHS to adopt zero tolerance approach to pressure ulcers. Available online at www.npsa.nhs.uk/corporate/news/nhs-to-adopt-zero-tolerance-approach-to-pressure-ulcers
National Institute for Health and Clinical Excellence (2014) Pressure ulcers: prevention and management of pressure ulcers. NICE, London.
Nottingham City Care Partnership “Policy for the Prevention of Pressure Ulcers” A Reference Guide for Community Health Care Teams
Nursing and Midwifery Council (2015) The Code, Standards of Conduct, Performance and Ethics for Nurses and Midwives. London.
Pennine Care NHS Trust. Safeguarding Adults Policy. Available online at www.penninecare.nhs.uk/media/1055/cI18-safeguarding-adults-policy-v4.pdf
Reporting and Learning System (NHS) (2009) Pressure Ulcers: an analysis of RLS data. Quarterly Data Summary Issue (11). NPSA. Available online at http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=60222&type=full&servicetype=Attachment
Root Cause Analysis Templates Available online at www.npsa.nhs.uk/rca
The Royal Borough of Kensington and Chelsea NHS Trust (2014) Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures.

United Lincolnshire Hospitals NHS Trust (Date Unknown) Inpatient Risk Assessment Booklet, Booklet V2.
Voegeli, D (2011) Pressure Ulcer or Moisture Lesion- what’s the difference? Nursing and Residential Care. Vol 13. No 5. Pg 222-227.
Waterlow, J (2005) Pressure Ulcer Prevention Manual. Wound Care Society. Taunton.
www.nhs.stopthepressure.co.uk
15. GLOSSARY OF KEYWORDS
Adult For the purpose of this policy an adult is defined as an individual aged 18 and over.
Autolytic debridementThe removal of devitalised tissue using moisture-retentive dressings.
Dynamic support surfaceDynamic devices usually use electricity or a battery pack to alter the level of support provided in the different chambers within the support devices. The types of support surface devices include overlays, replacement mattresses and speciality beds. The purpose of dynamic devices is to constantly change the pressure of the support surface against the skin, particularly at the body’s pressure points.
ErythemaRedness that persists following the application of fingertip pressure, usually over a bony prominence. Darkly pigmented skin may not have visible blanching. This is a symptom of a Grade 1 pressure ulcer.
Sharp debridementThe removal of devitalised tissue by a sharp instrument e.g. scalpel or scissors.

Appendix 1 (Front) Pressure Ulcer Risk Assessment
Date/Time:N.B. several scores per category can be usedBuild/weight for height 0 Average
1 Above average2 Obese3 Below average
Skin type and visual risk area(see wound classification –EPUAP overleaf)
0 Healthy1 Tissue paper1 Dry1 oedematous1 Clammy, pyrexia2 Discoloured (grade 1)3 Broken spots (grade 2-4)
Sex/age 1 Male2 Female1 14-492 50-643 65-744 75-805 80+
Continence 0 Complete/catheterised1 Urinary incontinence2 Faecal incontinence3 Doubly incontinent
Mobility 0 Fully1 Restless/fidgety2 Apathetic3 Restricted4 Bed bound e.g. traction5 Chair bound e.g. wheelchair
Nutrition Score 0See MST tool overleaf1
2Tissue Malnutrition 8 Terminal cachexia
8 Multiple organ failure5 Single organ failure (resp, renal, cardiac)
5 Peripheral vascular disease2 Anaemia (Hb <8)1 Smoking
Neurological deficit 4-6 Diabetes, MS, CVA4-6 Motor/sensory4-6 Paraplegia (maximum of 6)
Major surgery or trauma*scores can be discounted after 48 hours if patient is recovering normally
5 Orthopaedic/spinal5 On table > 2 hours*8 On table > 6 hours*
Medication 4 Cytotoxics, long term/high dose steroids, anti inflammatory
Total Score
Signature
Score 10+ - at risk 15+ - high risk 20+ very high risk
Name:………………………………………………………………
D.O.B:………………………………………………………………
HSS No: …………………………………………………………..Or Affix Patient Label
Sheet Number:

Date Time Total Score
Waterlow Review Schedule0 to10 = 3monthly10-15 = monthly15-20 = weekly20+ = weekly or each visit
Care Plan NumberSIGNATURE
NB. A care plan must be written where there is clinical concern.
Wound Classification - EPUAPGrade 1 Discolouration of intact skin not affected by light finger pressure (non–blanching erythema).
This may be difficult to identify in darkly pigmented skin.Grade 2 Partial thickness skin loss or damage involving epidermis and/or dermis. The pressure ulcer is
superficial and presents clinically as an abrasion, blister or shallow crater.Grade 3 Full thickness skin loss involving damage of subcutaneous tissue but not extending to the
underlying fascia. The pressure ulcer presents clinically as a deep crater with or without undermining of adjacent tissue.
Grade 4 Full thickness skin loss with extensive destruction and necrosis extending to underlying tissue.
Unstageable: Depth Unknown
Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar (tan, brown or black) in the wound bed. Until enough slough and/or eschar is removed to expose the base of the wound, the true depth, and therefore Category/Stage, cannot be determined. Stable (dry, adherent, intact without erythema or fluctuance) eschar on the heels serves as ‘the body’s natural (biological) cover’ and should not be removed.
Suspected Deep Tissue Injury: Depth Unknown
Purple or maroon localized area of discoloured intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue. Deep tissue injury may be difficult to detect in individuals with dark skin tones. Evolution may include a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Evolution may be rapid exposing additional layers of tissue even with optimal treatment.
Malnutrition Screening Tool (MST)(Nutrition Vol. 15, No.6, 1999 – Australia)
A – has patient lost weight recently?Yes – go to BNo - go to CUnsure – go to C and score 2
B – weight loss score0.5 – 5kg = 1 5 – 10kg = 2 10 – 15kg = 3 > 15kg = 4unsure = 2
C – patient eating poorly or lack of appetiteNo = 0Yes = 1
Nutrition ScoreIf > 2 refer for nutrition assessment /intervention

Appendix 1A Pressure Ulcer Risk Assessment
Pressure Ulcer Grade Recording Chart Indicate by circling and numbering all pressure damage on diagrams, then complete box below.Initiate care plan/wound assessment chart
Right Foot Left Foot Anterior View Posterior View
Date Ulcer Number Ulcer Location Grade(see toolkit)
Signature
Adapted from Healthcare Improvement Scotland our work/patient safety/tissue viability
Name:
URN:
D.O.B:

Appendix 2
Classification of Pressure Ulcers
The European Pressure Ulcer Advisory Panel (2009)
Adapted from the United Lincolnshire Hospitals NHS Trust

Appendix 3

Appendix 4 (Front)
Community SSKIN BundlePressure Ulcer Prevention SSKIN BundleThe SSKIN Care Bundle is to be implemented for all patients; Please tick- at risk of pressure damage (Waterlow>10) or as a result of clinical judgement □- with existing pressure damage □- who have had pressure damage previously □
WATERLOW SCORE DATE SIGNATURE PRINT NAME DESIGNATION
Patient Information Leaflet “Preventing Pressure Trauma” given to patient Yes □ No □State all disciplines involved in the care provision:
SSKIN INTERVENTIONS
SSurface
An appropriate support surface has been selected based on assessment of patient risk and patient agrees to purchase or hireMattress type (state) Date Ordered Date Delivered +fittedCushion type (state) Date Ordered Date Delivered +fittedOther (state) Date Ordered Date Delivered +fittedWheelchair user Yes □ No□ If yes is a pressure reducing cushion in use Yes □ No□
SSkin
Assess and record skin state on each visit (but no more than once a day)Carry Out the skin tolerance test and observe for red patches of skin (erythema)Record the skin evaluation using the grading as follows and ensure location is recordedNo evidence of new pressure damage/blanching erythema/grade1/grade2/Grade3/ Grade4
Record frequency of skin assessment-circle one; daily / twice weekly / weekly / monthly / 3monthlyIf frequency changes complete new first page
KKeep Moving
Mobility will be encouraged as patient condition allows. Record current regime of movementMORNING AFTERNOONEVENING NIGHTREPOSITIONING REGIME ADVISEDMETHOD OF TRANSFER
IIncontinence
Is the patient incontinent of Urine Y □ N □ Faeces Y □ N □ Double Y □ N □
Assess continence state and complete continence assessment Assess if the patients skin is prone to moisture Y □ N □
NNutrition
A nutritional assessment and MUST score has been completedMUST Score: Review date of MUSTA referral made to the (circle): Dietician /Speech and Language Therapist Y □ N □ Nutritional intake is monitored (dietary intake chart) Y □ N □ Fluid intake is monitored (fluid balance chart) Y □ N □
Additional Referrals Other (specify)Safeguarding Assure Reporting for ALL pressure trauma
USE CODES For Additional Information Section on second pageRA Patient has capacity but has refused assessment and /or will not comply with agreed plan of care including
repositioning or maintaining position.MC Patient does not have capacity to complyCI Critical illness/with hemodynamic or end of life final days precludes turning or repositioning and may lead to
unavoidable pressure ulcerCE Patient known to a health care professional but an acute or critical event occurs, which affects the patient’s
mobility or ability to reposition. This may include the patient being undiscovered following a fall or loss of consciousness or cardiac arrest
SC Carers not implementing planSE See evaluation in nursing records
Name:
URN:
D.O.B:

Appendix 4 (Back)SSKIN Bundle
Patient Name: URN:
Date DD/MM/YYTime (use 24hr clock)S. SURFACEIs the mattress in use? Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □Is the cushion in use? Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □Is other state…………in use? Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □Is above equipment in good working order?
Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □
Is the patient comfortable? Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □* If NO to any of the above please add additional informationS. SKIN Is there evidence of pressure damage to?B Buttocks (ischial bones) Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □E Elbows Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □S Sacrum Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □T Trochanter (hips) Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □S Spine Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □H Heels Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □O Occiput Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □T Toes Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □Other please state Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □* If YES to any of the above please add additional informationIf the patient declines skin inspection record reason and action in box belowK. KEEP MOVINGIs the current regime of movement being adhered to according to the patient /carer
Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □
Is the current regime effective Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □* If no to any of the above please add additional information
I. INCONTINENCE/MOISTUREIs the skin moist? Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □Has the patient had a continence assessment?
Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □
* If YES or NO to any of the above please add additional informationN. Nutrition Is the patient eating & drinking adequately?
Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □ Y □ N □
Additional Information-Add any additional information required from you evaluation above use code as previous sheetS Support Surface
S Skin Inspection
K Keep Moving
I Incontinence/Moisture
N Nutrition
SIGNATURE

A Guide for Completion of the Community SSKIN Bundle (adapted from Nottingham City Care Partnership)
The SSKIN Bundle is a bundle of care that involves fundamental components of pressure ulcer preventative interventions. It is crucial to remember that if only one of those components was to be omitted in the delivery of healthcare for patients at risk, the consequence is likely to be the development of a pressure ulcer.
The SSKIN Bundle will be completed for all patients identified to be at risk of developing a pressure ulcer, i.e. with a Waterlow above 10 or deemed to be at risk by the registered nurse’s clinical judgment
The patient will have a full skin assessment in conjunction with the Waterlow and this will be recorded on the Pressure Ulcer Risk Assessment Tool (Waterlow)
A registered practitioner will initiate the SSKIN Bundle and complete the first sheet (appendix 4)
This includes;
Patients name, URN Number and case load and Waterlow score The specific mattress and cushion required, agreement with patient to
purchase the date of the order, delivery and fitting The frequency of skin assessment based on the registered nurse clinical
judgement of the patient’s need; daily / twice weekly / weekly / monthly / 3 monthly . If level of frequency of skin assessment changes please complete new page one
The patient’s current regime of movement in relation to when they get up or go back to bed or mobilise to the toilet
The advise given to the patient and/or carer regarding repositioning The MUST score and date to review this
Any member of the healthcare / social team can complete the 2nd page of the SSKIN Bundle
If the patient is known to the District Nursing Services for 3 / 6/ 12 monthly interventions (including continence assessment) and is at risk of developing a pressure ulcer, the registered nurse will offer advice to the patient and/or carer and provide the FNHC Patient Information Leaflet “Preventing Pressure Trauma”. The advice will be recorded in the patient’s records.
If pressure relieving support surfaces are ordered at this point, a follow up visit will be arranged to evaluate the effectiveness of the support surfaces
If the patient is receiving healthcare from, Rapid Response and Reablement Team,
• A Pressure Ulcer Risk Assessment Tool (Waterlow) will be carried out on the first visit.
If this visit is not undertaken by a registered nurse, the assessment will be carried out by a competent health care worker.
If the patient is found to be at risk of developing pressure ulcers, the Healthcare worker will inform the registered nurse within the team of this risk.
If the patient is having additional support from care agencies, the registered nurse will perform the Pressure Ulcer Risk Assessment Tool (Waterlow) and initiate the SSKIN Bundle on first visit.

If other agencies are involved the registered nurse should encourage them with support to complete the second page of the SSKIN bundle'.
If a patient decides not to accept the registered nurses advice or the registered nurse’s request of the patient to purchase the recommended dressings/equipment then this must be clearly documented in the patients nursing records on the back of the SSKIN bundle and base card & a risk assessment of the concerns carried out. (refer to the what to do if the patient refuses treatment page )
If a patient with an at risk status is discharged from a FNHC caseload evidence that advice on the prevention of pressure trauma has been discussed with patient and carers and that the patient and carers have a copy of the FNHC information leaflet “preventing pressure trauma” .

Repositioning Chart
Inspect the patient’s skin regularly. Patients on pressure redistribution equipment still require skin inspection and regular repositioning
Repositioning (using legend below) Skin Inspection Comments
Identified repositioningschedule (hrs)
Other comments –e.g. pain mouth care given, eye care etc ,
Signature/DesignationDate Time From To
Name:………………………………………………………………
D.O.B:………………………………………………………………
URN: ……………………………………………………………….
Or Affix Patient Label
Repositioning chart for all those identified at risk of pressure damage, with existing pressure damage or recently had pressure damage
Encourage all those identified as being at risk of pressure damage to change their position frequently and at least six hourly.
Encourage all those identified as being at high risk of pressure damage to change their position frequently and at least four hourly.
Individual tissue tolerance time should be taken into consideration when determining repositioning schedules.
The above are available as a guide only.
Appendix 5
Legend – left (L), Right (R), Back (B), Prone (P), Sitting up (SU), Chair (C), Mobilising (M)

Appendix 6 (Front) Wound Assessment Chart
Factor Date
Wound Aetiology1. Location 2. Type
Wound Bed1.Epithelialising (pink) 4. Sloughy (yellow)2.Granulating (red) 5. Necrotic (black)3.Over-granulating (friable/red)
Surrounding Skin 1. Healthy/ Normal 5.Macerated2. Scaly/Dry 6. Eczema 3. Cellulitis 7. Fragile4. Oedematous 8.Callus
Exudate (Amount) 1. None 2. Light - on primary dressing 3. Moderate - on to secondary4. High - saturated secondary dressing
Exudate (Colour) 1. Clear /serous 5. Yellow 2. Opaque 6. Green 3. Blood 4. Brown
Odour PresentClinician’s opinion Yes / No None / Slight / Offensive
Clinical Infection Evident If Yes: Swab taken Yes / No Started antibiotics } Tick
Finished antibiotics } Date
Objective of Dressing Product1. Debridement 4. Medicated2. Absorption 5. Closure3. Hydration 6. Protection
Name:………………………………………………………………
D.O.B:………………………………………………………………
HSS No: …………………………………………………………..
Or Affix Patient Label
Allergies& Alerts:
Example Only – printed copy available from Tissue Viability Nurse

Date
Wound sizeMeasure monthlyLength x width x (depth) cmPhotographed/Traced yes/noInitials
.TREATMENT
A) Cleansing
B) Primary Dressing Date started Date Stopped Reason Signature
C) Secondary Dressing
D) Secured by
Name:…………………………………………………………
D.O.B:…………………………………………………………
HSS No: ……………………………………………………..
Or Affix Patient Label

Appendix 7 Safeguarding Trigger Tool

Appendix 8 Root Cause Analysis Template
FNHC ROOT CAUSE ANALYSIS FOR PRESSURE ULCERSPlease complete all sections fully.Please attach Waterlow Pressure Ulcer Risk Assessment for discussion
PATIENT NAME
PATIENT ADDRESS
DOB
URN
GP
MAIN CARER
Individual completing RCA Team
Date of referral to FNHC Patient admitting diagnosis
Date pressure(s) ulcer identified
Patient secondary diagnosis
Date GP/Physician notified Patients family notified & documented date
Place of onsetResidential Home, Hospital, Home other (please state)
Date of 1st Waterlow Risk Assessment 1st Waterlow Score
Where was it carried out?
Date last Waterlow Risk Assessment Last Waterlow Score
Where was it carried out?
How often was a Waterlow score carried out?Comments – to include whether risk assessment was carried out according to FNHC policy.Were staff trained in how to properly score for a risk level
Where was patient from?Own Home Residential Home Nursing Home H&SS Other
MUST/MST score recorded
Previous Pressure damage Previous pressure damage (healed)?DescribePast/Relevant Medical History circle & give detailsNeurological conditions? Chronic disease, Trauma Recent surgery. Rapid Deterioration of conditionFalls, immunosuppressant, loss of consciousness, infection, circulatory, anaemia, malignancy, advanced
age, acute & terminal care.
Mental Health Issues?Is there a Mental Capacity Act (MCA) concern? Yes No
DescribeWas this formally assessed? Yes No
Describe

Was there evidence of a safe guarding concern? Yes No
If Yes Had a safe guarding referral been submitted? Yes No
MedicationWhat Medication was the patient on?
Was it documented? Yes No
Steroids Type/dose
Sedation Type
Pain Was pain assessment completed? Yes No
Pain Score
Analgesia , please list
Has appropriate care plans been completed? Yes No
SSKIN Bundle Implemented Yes No Second page of the SSKIN Bundle fully completed Yes No
Last Reviews Date S.S.K.I.N (Skin condition/Surface/Keep Moving/Incontinence/Nutrition)SURFACE (an appropriate support surface has been selected based on assessment of patient risk)
Individual is bedbound /wheelchair bound Yes No
Was the patient sitting /lying on the correct piece of equipment Yes No
Pressure relieving equipment in place? Was the type of mattress insitu is clinically appropriate for patient status
State type of Mattress in situ (e.g Autologic, Nimbus/Softair mattresses. Type of seating /cushion)
Date mattress ordered: Date delivered: Delay? Please give reason:
Was the patient referred to an Occupational Therapist? Yes No
Was there a Profiling bed in situ and was it being used appropriately i.e profiled to keep heels off bed surface? Yes No
Had Seating position been assessed? Yes No
Was the Chair support surface clinically appropriate for patient status? Yes No
Was Chair pressure reduction cushion utilised? Yes No

Date ordered: Date delivered: Delay? Please give reason:
Was the patient compliant using equipment? Yes No
Skin ConditionWas a skin inspection carried out on admission and at each visit? Yes No if No is there a rationale as to why not
How frequency was the inspection?
Were vulnerable areas documented? Yes No if No is there a rationale as to why
What did the care plan read?
Was a referral to Tissue Viability made? Yes No if No is there a rationale as to why
Has sacrum been protected from shear with topical products/dressing? Yes No If No is there a rationale as to why
Use of slide sheets to prevent friction Yes No If No is there a rationale as to why
KEEP MOVING
Level of Mobility: Independent Assistance of : 1 2 Bedbound Chair bound
Length of time in bed? Length of time in chair?
Was patient mobility assessed? Yes No
Was mobility encouraged? Yes No
Was moving & handling risk assessment completed? Yes No
Was there a moving & handling care plan? Yes No
Advice given ?(e.g., Repositioning chart, pressure relief care) Yes No
Referral to physiotherapist? Yes No
Referral to Occupational Therapist? Yes No
Patient’s compliance to advice: Yes No NCONTINENCE
Continence: Please circle Continent, Catheter, Incontinent of: Urine Faeces, Both
Continence Assessment evident in records Yes No
Type of incontinent pads?

Number of pads layers?
Moisture damage? Yes No
Continence aids used? – Describe
Skin cleansing regime? (including barrier) identified as………
A referral to the continence nurse? Yes No
NUTRITION
A nutritional assessment Took place? Yes No
Was a MUST completed Yes No
Did a referral to the Dietician take place? Yes No
Were diet recommendations documented & implemented? Yes No
Did food & fluid monitoring take place? Yes No
Were supplements prescribed? Yes No
Was there documentation re supplement intake? Yes No
Was the patient receiving Peg Feeding? Yes No
Was their sufficient Fluid intake describe? Yes No
Comments……………………….
ReportingHas Wound Been Mapped? Yes No Has Wound Been Photographed? Yes No
Consent for photograph? Yes No
Was the pressure trauma flow chart adhered to ? Yes No
Was the patient visited by a Grade 6/5? ? Yes No
Has a (TVN) referral been completed? If Yes, Date form completed
, If No is there a rationale as to why
Was Grade 2 and multiple grade 2 & above Pressure Damage reported as a clinical incident on the Assure System Yes No Date of Assure

If unreported pressure trauma was identified on hospital discharge or patient develops grade 3 or 4 pressure ulcer within 72hrs of discharge;
Was a datix carried out ? Yes No Date of datix
Carer / other agency involvement : Yes No Give details:
Was there any refusal of care? Yes No
Is yes is there evidence of a risk assessment Yes Yes
Is there evidence of education provided to patient /family for best practice pressure ulcer prevention? Yes No
Care & Service Delivery Problems
Was Staffing levels appropriate. Yes No
Is there a standard DN first assessment procedure? Yes No
Was there a breakdown in communication with respect to the patients risk for pressure ulcer development?Yes No Explain
Were staff involved trained in pressure trauma prevention & management? Yes No
Is there evidence based moisture skin care protocol? Yes No
Is there evidence based incontinence protocol? Yes No
Is there a process for education & documentation for family/patient refusal to comply with evidence based protocol for skin and pressure ulcer prevention & management? Yes No
Is equipment readily available for implementation? Yes No
Is there a process for support surfaces determination based on clinical need? Yes No
Is there a process to monitor surface lifespan effectiveness according to manufacturers instructions? Yes No
Is there a 24hr equipment delivery/ repair/replacement service available? Yes No
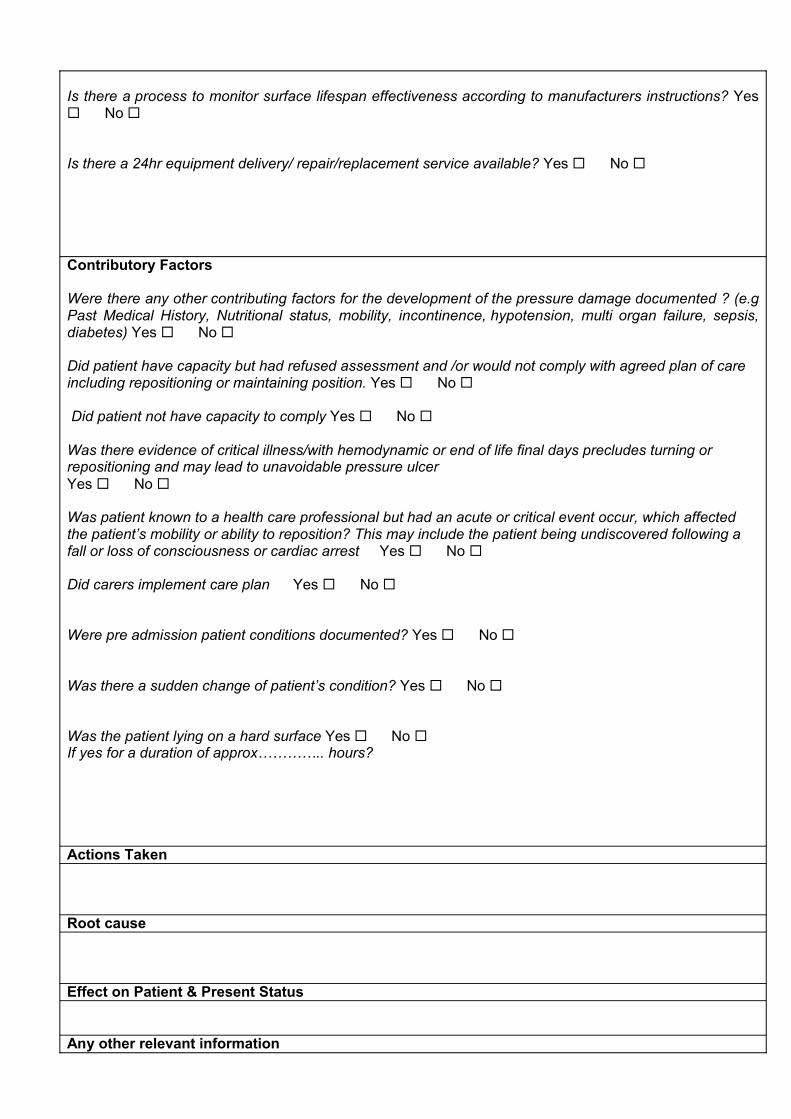
Contributory Factors
Were there any other contributing factors for the development of the pressure damage documented ? (e.g Past Medical History, Nutritional status, mobility, incontinence, hypotension, multi organ failure, sepsis, diabetes) Yes No
Did patient have capacity but had refused assessment and /or would not comply with agreed plan of care including repositioning or maintaining position. Yes No
Did patient not have capacity to comply Yes No
Was there evidence of critical illness/with hemodynamic or end of life final days precludes turning or repositioning and may lead to unavoidable pressure ulcerYes No
Was patient known to a health care professional but had an acute or critical event occur, which affectedthe patient’s mobility or ability to reposition? This may include the patient being undiscovered following a fall or loss of consciousness or cardiac arrest Yes No
Did carers implement care plan Yes No
Were pre admission patient conditions documented? Yes No
Was there a sudden change of patient’s condition? Yes No
Was the patient lying on a hard surface Yes No If yes for a duration of approx………….. hours?
Actions Taken
Root cause
Effect on Patient & Present Status
Any other relevant information

Lessons Learnt
Mitigating CircumstancesWas there an obvious omission in care which resulted in the pressure damage? Yes No
If yes, complete SV1 form - Date Completed Date Sent
Signature: Print Name:
Designation: Date:
TVN TO COMPLETE THIS SECTION, Completed from RCA tool Completed from patient assessment Has patient been seen by TVN? Include Date ……………………
Assessments: Was the Assessment timely?
Is the Assessment accurate?
Was expert advice sought and documented DetailsInterventions: Are interventions timely Are interventions undertaken Give details …………………………………………………………………………………………………………………..…………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………….Appropriately adjusted to patient’s needs and condition DetailsWas expert advice sought and documented DetailsMonitoring: Is monitoring undertaken Give details:- .............................................................……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………Is monitoring timely Appropriately adjusted to patient’s needs and condition Details……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………Was expert advice sought and documented Details………………………………………………………………………………………………………………………………………………………………………………..Conclusions
Recommendations
Arrangements For Shared LearningSignature: Print Name:
Chronology (timeline) of eventsDate & Time Event

See also ‘Types of Preventative Actions Planned’- tool at www.npsa.nhs.uk/rca
Action Plan Action 1 Action 2 Action 3
Root CAUSE
EFFECT on Patient
Recommendation
Action to Address Root CauseLevel for Action (Org, Direct, Team)
Implementation by:
Target Date for ImplementationAdditional Resources Required (Time, money, other)
Evidence of Progress and CompletionMonitoring & Evaluation Arrangements Sign off - action completed date:Sign off by:

WHAT CAN YOU DO TO PREVENT PRESSURE TRAUMA?
Keep skin dry and clean.
Utilise any specialised pressure relieving equipment that has been advised.
Change your position regularly – if you are unable to move yourself you will be given advice and support on re-positioning.
Drink plenty of fluids.
Have a varied and balanced diet
Report any areas of soreness, or if you notice any reddening over a bony areas to your nurse or carers.
PLEASE REMEMBER
This leaflet gives you some information about pressure trauma.The nurse caring for you will ask to examine you and ask you some questions to see if you are at risk of developing pressure trauma. This is part of a risk assessment. It helps to identify if you need any special equipment such as a pressure redistributing cushion or mattress to help prevent you developing pressure trauma.
With your consent a plan of care will be initiated, taking into account your personal needs and circumstances.
If you need any further advice about any aspect of pressure trauma prevention or management, the nurses are there to help.
(Adapted from National Institute for Clinical Excellence guideline; Pressure ulcer prevention, treatment and care: information for the public, 2014).
PREVENTING PRESSURE TRAUMA
An information leaflet explaining pressure trauma (bedsores) to patients
and carers
Appendix 9 - Patient Information Leaflet

WHAT IS PRESSURE TRAUMA?A pressure ulcer (bed sore) is an area of skin and underlying tissue which is damaged. This happens when pressure is applied to the same area for a period of time reducing or cutting off the blood supply.
Pressure trauma usually happens when you lie or sit in the same position for too long. It can be very painful and can have serious complications. They can take a long time to heal.
Most pressure trauma can be prevented with support and special pressure redistributing aids. If trauma occurs they need to be managed carefully to stop them getting worse.
WHAT TO LOOK FOR: Red patches on skin (purple or blue or
dark pigmented skins) Swelling over a bony area Blisters or broken skin
The skin may feel unusually: Hard, swollen, warm/hot, tender/painful
or very dry.
COMMON AREAS WHERE PRESSURE TRAUMA OCCURS.
Pressure trauma tends to occur over bony areas as shown in image below:
ARE YOU AT RISK?
Any of the following increase your risk of developing pressure trauma:
If you have problems with movementwhich means you are sitting or lying in one position for long periods of time
If you have poor circulation Moist skin caused by problems
controlling your bladder or bowels If you have had pressure trauma
before Poor diet and fluids If you do not drink
enough or have a poor diet Lack of sensitivity to pain or discomfort
Conditions such as diabetes, stroke and disorders which affect the nerve supplies, and muscle movement reduce the normal sensation or of discomfort that prompt you to move.
If you have problems with you memory and understanding things feelings, such as dementia
If you are having an operation

Reporting process for all patients identified with pressure trauma
INTERVENTIONS TO BE IMPLEMENTED BY RELEVANT MEMBER OF STAFF:-
Patient identified with suspected Pressure Trauma
Holistic assessment to be carried out by a qualified nurse within 24hr of referral
Pressure trauma to be reported on Assure reporting system within 24hrs
Qualified Nurse Complete full assessment within
24hrs of referral Complete Waterlow assessment Complete moving and handling
assessment. Identify if any moving and handling
risks & risk assess. Complete wound assessment
chart/consent for photograph/take photo/complete SSKIN Bundle & other relevant care plans/referrals etc
Report on Assure system within 24hrs
Inform 5/6 of situation by end of shift: discuss and decide course of action discuss any safeguarding triggers.
Maintain ongoing monthly reporting on Assure system until pressure trauma is healed or other outcomeoccurs, (CSN to email grade 5/6 monthly with update of pressure trauma on workload)
Grade 5 or 6 if not Identifying Nurse: Follow up discussion with Identifying
Nurse Determine if urgent joint visit with
community staff nurse to reassess situation within 24hrs.
Complete all necessary risk assessments
Retrieve CACHR records for patient with multiple grade 2 at different sites or Grade 3/4 or any other trauma (that gives concern)
Complete Root Cause Analysis Report to Tissue Viability Nurse/Op
Lead Initiate Safeguarding Alert (follow
local policy) if appropriate Monitor Pressure trauma register on
Assure Obtain ongoing update of progress
at least monthly from members of the team and update Assure system
Patient Safety Facilitator (P.S.F) &Tissue Viability Nurse (T.V.N): Monitor Assure system for all
… reported pressure trauma Trigger immediate RCA if
multiple Grade 2’s or grade 3 /4 , if not completed, as per policy
Add details to patient safety agenda
Monitor Assure data Monitor Pressure Trauma
Register Follow up completed RCA Feedback actions /outcome Report on pressure trauma
prevalence
Appendix 10