Prenatal diagnosis of congenital anomalies 3
217
-
Upload
drahmed-badr -
Category
Health & Medicine
-
view
390 -
download
0
Transcript of Prenatal diagnosis of congenital anomalies 3


Prenatal Diagnosis of Congenital Anomalies
F.E.B.O.G.

Background Ultrasound allows the detection of not
only major defects but also of soft markers of chromosomal abnormalities .
The vast majority of fetal abnormalities occur in the low-risk group. Consequently, ultrasound examination should be offered routinely to all pregnant women.

Background
The Society of Obstetricians and Gynaecologists of Canada (SOGC) recommends a single “routine” ultrasound evaluation at 16 to 20 weeks in all pregnancies.
Patients need to be counselled about the positive and negative findings that ultrasound may reveal.

What is fetal
anomaly?

What is fetal anomaly?
Definition: "a marked deviation from the normal
standard, especially as a result of congenital defects").
An anomaly scan will not detect every case of abnormality

The objective of the fetal anomaly scan is to reassure the woman that her baby appears to have no obvious structural abnormalities, and if this is not the case, to identify anomalies:
1. not compatible with life 2. associated with high morbidity and long term disability 3. fetal conditions with the potential for intrauterine
therapy 4. fetal conditions that will require postnatal
investigations or treatments

Definition a soft marker is defined
as” ultrasound finding at 16-20 weeks gestation which increases the risk of the fetus having a chromosomal anomaly”

The screening ultrasound at 16 to 20 weeks should evaluate 8 markers, 5 of which:-
1. Thickened nuchal fold
2. Echogenic bowel
3. Mild ventriculomegaly
4. Echogenic focus in the heart
5. Choroid plexus cyst
are associated with an increased risk of fetal aneuploidy, and in some cases with nonchromosomal problems
while 3 (single umbilical artery, enlarged cisterna magna, and pyelectasis) are only associated with an increased risk of nonchromosomal abnormalities when seen in isolation . (II-2 B).

The minimum standard for a "20 week" anomaly scan
measurement of:- Bi-parietal diameter, head circumference femur length. abdominal circumference.
RCOG GUIDELINES

The minimum standard for a "20 week" anomaly scan
Head shape + internal structures cavum pellucidum cerebellum ventricular size at atrium (<10 mm)
Spine: longitudinal and transverse Abdominal shape and content at level of stomach Abdominal shape and content at level of kidneys and umbilicus Renal pelvis (<5 mm AP measurement) Longitudinal axis - abdominal-thoracic appearance
(diaphragm/bladder) Thorax at level of 4 chamber cardiac view Arms - three bones and hand (not counting fingers) Legs - three bones and foot (not counting toes)
RCOG GUIDELINES

The optimal standard for the "20 week" anomaly scan
The fol lowing could be added to the features above
Cardiac outflow tracts Face and l ips
RCOG GUIDELINES

Fetal Nuchal Translucency

Fetal Nuchal Translucency
Nuchal translucency refers to the normal subcutaneous fluid-filled space between the back of the fetal neck and the overlying skin.
Sonographic criteria to maximize quality of nuchal translucency sonography are:
1. Transabdominal or transvaginal approach should be left to the sonographer's discretion, based on maternal body habitus, gestational age, and fetal position.
2. Gestation should be limited to between 11 weeks 14 weeks.

3-Fetus should be examined in a midsagittal plane.
4-Fetal neck should be in a neutral position. 5-Fetal image should occupy at least 75% of
the viewable screen. 6-Fetal movement should be awaited to
distinguish between amnion and overlying fetal skin.
Fetal Nuchal Translucency

7-Calipers should be placed on the inner borders of the nuchal fold.
8-Calipers should be placed perpendicular to the long axis of the fetal body.
9-At least three nuchal translucency measurements should be obtained.
10-At least 20 minutes might need to be dedicated to the nuchal translucency measurement before abandoning the effort
Correct
Incorrect
Fetal Nuchal Translucency

Abnormal nuchal translucency .Normal nuchal translucency

THICKENED NUCHAL FOLD

THICKENED NUCHAL FOLD
Definition and Imaging Criteria
The nuchal fold is the skin thickness in the posterior aspect of the fetal neck.
A nuchal fold measurement is obtained in a transverse section of the fetal head at the level of the cavum septum pellucidum and thalami, angled posteriorly to include the cerebellum. The measurement is taken from the outer edge of the occiput bone to the outer skin limit
* measurement of 6 mm is considered abnormal between 18 and 24 weeks

A thickened nuchal fold should be distinguished from cystic hygroma, in which the skin in this area has fluid-filled loculations.
A thickened nuchal fold should not be confused with nuchal translucency.
THICKENED NUCHAL FOLD

Increased nuchal fold

Increased nuchal fold

THICKENED NUCHAL FOLD
Recommendations1. A thickened nuchal fold significantly increases
the risk of fetal aneuploidy. by 17-fold, So karyotyping should be offered . (II-1 A).
2. A thickened nuchal fold is associated with congenital heart disease and may be an early sign of hydrops. (II-2 B).
SOGC guidelines June 2005





The integrity of the abdominal wall should always be demonstrated; this can be achieved by transverse scans demonstrating the insertion of the umbilical cord. It is also important to visualize the urinary bladder within the fetal pelvis, because this rules out exstrophy of the bladder and of the cloaca.
Anterior abdominal wall

Anterior abdominal wall Prevalence Exomphalos is found in about 1 per
4000 births. The majority of cases are sporadic
and the recurrence risk is 1%. However, there may be an associated
genetic syndrome. (mainly tr isomy 18 or 13) in about 30% of cases.

Exomphalos

Diagnosis The diagnosis of exomphalos is based
on the demonstration of the mid-line anterior abdominal wall defect, the herniated sac with its visceral contents and the umbilical cord insertion at the apex of the sac.
Exomphalos






GASTROSCHISIS
In gastroschisis, evisceration of the intestine occurs through a small abdominal wall defect located just lateral and usually to the right of an intact umbilical cord. The loops of intestine lie uncovered in the amniotic fluid.
Prevalence Gastroschisis is found in about 1 per 4000
births.


GASTROSCHISIS

BLADDER EXSTROPHY AND CLOACAL EXSTROPHY
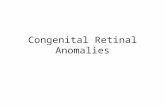
Bladder exstrophy is a defect of the caudal fold of the anterior abdominal wall; leads to exposure of the posterior bladder wall.
In cloacal exstrophy, both the urinary and gastrointestinal tracts are involved.
Cloacal exstrophy is the association of an omphalocele, exstrophy of the bladder, imperforated anus, and spinal defects such as meningomyelocele.

green arrows: everted bladder;
blue arrows the scrotum;
yellow arrows: umbilcal cord

HYDROPS FETALIS

HYDROPS FETALIS Definit ion: Hydrops is defined by abnormal
accumulation of serous fluid in skin (edema) and body cavities (pericardial, pleural, or ascitic effusions).
Prevalence: Hydrops fetalis is found in about 1 per
2,000 births.

HYDROPS FETALIS

HYDROPS FETALIS



CARDIOVASCULAR SYSTEM

CARDIOVASCULAR SYSTEM
Prevalence:Cardiovascular abnormalities are found in 5-10 per 1,000 live births and in about 30 per 1,000 stillbirthsASSESSMENT OF THE FETAL heart
The heart can be observed in the four-chamber, left and right chambers and
great vessel views.

CARDIOVASCULAR SYSTEM
The four chambers view The heart occupies one third of the thorax. The heart is
shifted to the left side of the chest, with the apex pointing to the left. The axis of the interventricular septum is about 45º to 20º to the left of the anteroposterior axis of the fetus.
. The right ventricle is located behind the sternum and is characterized by the presence of the moderator band. Normally, both ventricles are approximately the same size. The mitral valve insertion is slightly cephalad to the insertion of the tricuspid valve). These features help distinguish the right ventricle from the left ventricle).






Evaluation of the cardiac outflow tracts can be difficult, and at present it is not considered a part of the standard examination of fetal anatomy.
The outflow tracts and great arteries can be demonstrated by slight angulations of the transducer from the four-chamber view.
By turning the transducer while keeping the left ventricle and the aorta in the same plane, one can obtain the left heart views,
while the right heart views are obtained by moving the transducer cranially and tilting slightly in the direction of the left shoulder.
The left heart views demonstrate the left ventricle and aortic outflow tract.

VENTRICULAR SEPTAL DEFECTS
Are either isolated (about 50%) or they are part of a complex heart defect
Prevalence: Ventricular septal defects, which
represent 30% of all congenital heart defects, are found in about 2 per 1,000 births.

VENTRICULAR SEPTAL DEFECTS


VENTRICULAR SEPTAL DEFECTS
Diagnosis: depends on the
demonstration of a dropout of echoes in the ventricular septum., multiple views should be used.

SINGLE UMBILICAL ARTERY
Single umbilical artery (SUA) is the absence of one of the arteries surrounding the fetal bladder and in the fetal umbilical cord.
Assessment of the umbilical arteries can be made from the cord itself and on either side of the fetal bladder.
The assessment can be enhanced with colour f low Doppler.

SINGLE UMBILICAL ARTERY


SINGLE UMBILICAL ARTERY

SINGLE UMBILICAL ARTERY
Recommendations1. The finding of a single umbilical artery
requires a more detailed review of fetal anatomy, including kidneys and heart Because it may be associated with both underlying renal and cardiac abnormalit ies . (II-2 B).
2. An isolated single umbilical artery does not warrant invasive testing for fetal aneuploidy. (II-2)
SOGC guidelines June 2005


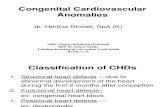
ECHOGENIC INTRACARDIAC FOCUS Definition
Echogenic intracardiac focus (EICF) is defined as a focus of echogenicity comparable to bone, in the region of the papillary muscle in either or both ventricles.
88% are only in the left ventricle, 5% are only in the right, and 7% are biventricular.
Grade 2 suggests that echogenicity is equal to bone, and grade 3 suggests it is greater

Prevalence: EIF are found in about 1.5% to 5.5% of
pregnancies Imaging Criteria An EICF can be diagnosed on the standard 4-
chamber view of the fetal heart and should be located within the ventricle where papillary muscles are situated and should move with valve leaflets (golf balls); EIF should seen from more than one angle .
ECHOGENIC INTRACARDIAC FOCUS

ECHOGENIC INTRACARDIAC FOCUS standard 4-chamber view



Recommendations1. Isolated EICF require no further investigation when maternal age or the serum screen equivalent is less than
the risk of a 31-year-old. (III-D). 2. Women with an isolated EICF and at increased risk for fetal aneuploidy owing to maternal age
(31 years or more) or maternal serum screen results should be offered counselling regarding fetal karyotyping . (II-2 B).
3. Women with right-sided, biventricular, multiple, or nonisolated EICF should be offered referral for expert review and possible karyotyping . (II-2 A).
ECHOGENIC INTRACARDIAC FOCUS

Face

Face A series of transverse scans from the top of
the head moving caudally allows examination of the forehead, nasal bridge, orbits, nose, upper lip and anterior palate, the tongue within the oral cavity, lower lip and mandible.
Each orbital diameter is equal in size to the interorbital diameter.


Hypertelorism
Hypertelorism is an increased interorbital distance and this can be either an isolated finding or associated with many cl inical syndromes or malformations.


Hypotelorism (stenopia(:
Hypotelorism (decreased interorbital distance) is almost always found in association with other severe anomalies, such as holoprosencephaly, trigonocephaly, microcephaly, Meckel syndrome, and chromosomal abnormalities.

Hypotelorism (stenopia(:

FACIAL CLEFTThis term refers to a wide spectrum of clefting
defects (unilateral, bilateral and less commonly midline) usually involving the upper lip, the palate, or both
Prevalence:1 per 800 births. In about 50% of cases in both
the lip and palate are defective, in 25% only the lip and in 25% only the palate involved.



FACIAL CLEFT


Gastrointestinal
tract

Gastrointestinal tract Sonographically, the fetal stomach is visible from 9
weeks of gestation as a sonolucent cystic structure in the upper left quadrant of the abdomen.
The bowel is normally uniformly echogenic until the third trimester of pregnancy,.
The liver comprises most of the upper abdomen

Duodenal atresia Prevalence Duodenal atresia is found in about 1 per
5000 birth Diagnosis Prenatal diagnosis is based on the
demonstration of the characteristic ‘double bubble’ appearance of the dilated stomach and proximal duodenum, commonly associated with polyhydramnios.

Duodenal atresia

Although the characteristic ‘double bubble’ can be seen as early as 20 weeks, it is usually not diagnosed until after 25 weeks, suggesting that the fetus is unable to swallow a sufficient volume of amniotic fluid for bowel dilatation to occur before the end of the second trimester of pregnancy.
Duodenal atresia

Intestinal obstruction Prevalence Intestinal obstruction is found in about 1
per 2000 births; in about half of the cases, there is small bowel obstruction and in the other half anorectal atresia.
Diagnosis Diagnosis of obstruction is usually made
quite late in pregnancy (after 25 weeks),. as multiple fluid-f i l led loops of bowel in the abdomen.
Polyhydramnios (usually after 25 weeks) is common, especially with proximal obstructions

Intestinal obstruction


Once an echogenic bowel is suspected, the gain of the ultrasound unit is lowered gradually unti l only bone or bowel is visible
Definit ion Bowel echogenicity equal to or greater than
bone is signif icant (grade 2 or 3) . (II-2 A).
No further investigations are required for grade 1 echogenic bowel . (I I-2 D).
Echogenic bowel

Echogenic bowel


Fetal bowel that is as echogenic as surrounding bone

Echogenic bowel

Echogenic bowelEchogenic bowel is diagnosed in 0.2%
to 1.4% of all second-trimester ultrasounds.
It is associated with normal fetuses, fetuses with aneuploidy, intrauterine growth restrict ion (IUGR), intra-amniotic bleeding owing to placental abruptions, cystic f ibrosis (CF), congenital viral infections (cytomegalovirus , herpes, parvovirus, rubella, varicella, and toxoplasmosis), and thalassemia.

Echogenic bowelSO Expert review is recommended to initiate the following:
a. Detailed ultrasound evaluation looking for additional structural anomalies or other soft markers of aneuploidy . (II-2 A)
b. Detailed evaluation looking for signs of bowel obstruction and placental characteristics . (II-2 B).
c.Genetic counselling (II-2 A).
d. Laboratory investigations that should be offered, including maternal serum screening, and testing for congenital infection . (II-2 A)SOGC guidelines June 2005

ABDOMINAL CYSTS Abdominal cystic masses are frequent
findings. Renal tract anomalies or dilated bowel are the most common explanations,
Although cystic structures may arise from the biliary tree, ovaries, mesentery or uterus. the most likely diagnosis is usually suggested by the position of the cyst, its relationship with other structures and the normality of other organs.

kidneys

kidneys Longitudinal and transverse sections of
the abdomen can be used to study the kidneys.
The fetal bladder can be visualized from the first trimester changes in volume over time help to differentiate it from other cystic pelvic structures.

Renal agenesis Prevalence Bilateral renal agenesis is found in 1 per 5000
births, while unilateral disease is found in 1 per 2000 births.
Diagnosis Antenatally, the condition is suspected by the
combination of anhydramnios (from 17 weeks) and empty fetal bladder (from as early as 14 weeks).

Failure to visualize the renal arteries with color Doppler is another important clue to the diagnosis in dubious cases,
Prenatal diagnosis of unilateral renal agenesis is difficult because there are no major features, such as anhydramnios and empty bladder.
Renal agenesis


INFANTILE POLYCYSTIC KIDNEY DISEASE (POTTER TYPE I)
Diagnosis is based on the
demonstration of bilaterally enlarged and homogeneously hyperechogenic kidneys. There is often associated oligohydramnios, but this is not invariably so.




MULTICYSTIC DYSPLASTIC KIDNEY DISEASE (POTTER TYPE II)
Prevalence Multicystic dysplastic kidney disease is found in
about 1 per 1000 births. Diagnosis the kidneys are replaced by multiple irregular
cysts of variable size with intervening hyperechogenic stroma. The disorder can be bilateral or unilateral if bilateral, there is associated anhydramnios and the bladder is ‘absent’.



obstructive uropathy The term ‘obstructive uropathy’ characterized by
dilatation of part or all of the urinary tract. When the obstruction is complete and occurs early in fetal life can lead to renal hypoplasia.
On the other hand, where intermittent obstruction allows for normal renal development, or when it occurs in the second half of pregnancy, hydronephrosis will result

Hydronephrosis
Varying degrees of pelvicalyceal dilatation are found in about 1% of fetuses.
Mild pyelectasia. In about 20% of cases, there may be an underlying ureteropelvic junction obstruction or vesicoureteric reflux that requires postnatal follow-up and possible surgery.
hydronephrosis, characterized by an anteroposterior pelvic diameter of more than 10 mm and pelvicalyceal dilatation, is usually progressive and in more than 50% of cases surgery is necessary during the first 2 years of life.

Hydronephrosis


MILD PYELECTASIS
Definit ion and Imaging CriteriaMild pyelectasis is defined as a
hypoechoic spherical or ell iptical space within the renal pelvis that measures 5mm to 10 mm. The measurement is taken on a transverse section.


MILD PYELECTASIS1. All fetuses with renal pelvic measurements 5 mm should have a neonatal ultrasound, Renal pelvis
measurements > 10 mm should be considered equivalent to congenital hydronephrosis and should be considered for a third tr imester scan . (II-2 A).
2. Isolated mild pyelectasis does not require fetal karyotyping (I I-2 E).
3. Referral for pyelectasis should be considered with addit ional ultrasound f indings and (or) in women at increased risk for fetal aneuploidy owing to maternal age or maternal serum screen results . (I I-2 A).SOGC guidelines June 2005


Pulmonary abnormalit ies
At 18-23 weeks, the central third of the thoracic area at the level of the four chamber view is occupied by the heart, and the remaining two thirds by the lungs, that are normally uniformely echogenic.


PLEURAL EFFUSIONS
Fetal pleural effusions, which may be unilateral or bilateral, may be an isolated finding or they occur in association with generalized edema and ascites.




DIAPHRAGMATIC HERNIA Prevalence Diaphragmatic hernia is found in about 1 per
4000 births. Diagnosis Diaphragmatic hernia can be diagnosed by
the demonstrat ion of stomach and intestines (90% of the cases) or l iver in the thorax and the associated mediastinal shif t to the opposite side.
A left-sided diaphragmatic hernia, are easy to demonstrate because the echo-free f luid-f i l led stomach and small bowel. In contrast, a r ight-sided hernia is more dif f icult to identify

DIAPHRAGMATIC HERNIA

Cystic adenomatoid malformation Prevalence Cystic adenomatoid malformation of the lung
is found in about 1 in 4000 births. Diagnosis Prenatal diagnosis is based on the
demonstration of a hyperechogenic pulmonary tumor which is cystic (CAM type 1), mixed (CAM type 2), or solid – microcystic (CAM type 3)..
In macrocystic disease, single or multiple cystic spaces may be seen within the thorax.

Cystic adenomatoid malformation

Foot and hand

Clubfoot The relat ionship of leg and foot should also be
assessed to rule out clubfoot







Examination of the fetal brain can essentially be carried out by two transverse planes, the transventricular and the transcerebellar plane.
The transventricular plane, obtained by a transverse scan at the level of the cavum septum pellucidum will demonstrate the lateral borders of the anterior (or frontal) horns, the medial and lateral borders of the posterior horns (or atria) of the lateral ventricles and the choroid plexuses.The transventricular view is used for measurement of the biparietal diameter (BPD), head circumference (HC), and width of the ventricles.
The transcerebellar (or suboccipitobregmatic) view allows examination of the mid-brain and posterior fossa; this view is used for measurement of the transverse cerebellar diameter (TCD) and cisterna magna (CM).
CENTRAL NERVOUS SYSTEM

CENTRAL NERVOUS SYSTEM

CENTRAL NERVOUS SYSTEM

CENTRAL NERVOUS SYSTEM

A sagittal and/or coronal view of the entire fetal spine should be obtained in each case. In the sagittal plane the normal spine has a 'double railway' appearance and it is possible to appreciate the intact soft tissues above it.
In the coronal plane, the three ossification centers of the vertebra form three regular lines that tether down into the sacrum.
CENTRAL NERVOUS SYSTEM


NEURAL TUBE DEFECTS These include anencephaly, spina bif ida and
cephalocele. In anencephaly there is absence of the cranial
vault (acrania) with secondary degeneration of the brain.
Encephaloceles are cranial defects, usually occipital, with herniated f luid-f i l led or brain-f i l led cysts.
In spina bif ida the neural arch, usually in the lumbosacral region, is incomplete with secondary damage to the exposed nerves.
Prevalence: the prevalence is about 5 per 1,000 births.
Anencephaly and spina bif ida, with an approximately equal prevalence, account for 95% of the cases and cephalocele for the remaining 5%.

Anencephaly Diagnosis: The diagnosis of
anencephaly during the second trimester of pregnancy is based on the demonstration of absent cranial vault and cerebral hemispheres. Associated spinal lesions are found in up to 50% of cases.






Spina bifidaDiagnosis of spina bif ida
requires the systematic examination of each neural arch from the cervical to the sacral region both transversely and longitudinally.
In the transverse scan the normal neural arch appears as a closed circle with an intact skin covering, whereas in spina bif ida the arch is "U" shaped and there is an associated bulging meningocele (thin-walled cyst) or myelomeningocoele.

Spina bif ida

Spina bif ida The diagnosis of spina bifida has
been greatly enhanced by the recognition of associated abnormalities in the skull and brain.
These include frontal bone scalloping (lemon sign), and obliteration of the cisterna magna with either an "absent" cerebellum or abnormal anterior curvature of the cerebellar hemispheres (banana sign).










Diagnosis: Fetal hydrocephalus is diagnosed sonographically,
by the demonstration of abnormally dilated lateral cerebral ventricles10 mm or more. The choroid plexuses, which normally fill the lateral ventricles are surrounded by fluid.
A distinction is usually made between mild ventriculomegaly (diameter of the posterior horn 10-15 mm) and hydrocephalus (diameter greater than 15 mm )
Certainly before 24 weeks and particularly in cases
of associated spina bifida, the head circumference may be small rather than large for gestation.,
HYDROCEPHALUS AND VENTRICULOMEGALY

HYDROCEPHALUS AND VENTRICULOMEGALY
Prevalence:
Hydrocephalus is found in about 2 per 1,000 births.
Ventriculomegaly is found in 1% of pregnancies at the 20-23 week scan.
Therefore the majority of fetuses with ventriculomegaly do not develop hydrocephalus.

MILD VENTRICULOMEGALY
. Mild ventriculomegaly (MVM) is defined by atrial measurements 10 to 15 mm. Measurements are obtained from an axial plane at the level of the choroid plexus.

MILD VENTRICULOMEGALY


HYDROCEPHALUS AND VENTRICULOMEGALY

1. Fetal cerebral ventricles should be measured if they subjectively appear larger than the choroid plexus (III-B).
2. Cerebral ventricles greater than or equal to 10 mm are associated with chromosomal and central nervous system pathology.
Expert review should be initiated to obtain the following: a. a detailed anatomic evaluation looking for additional
malformations or soft markers. (III-B), b. laboratory investigation for the presence of congenital
infection or fetal aneuploidy . (III-B).
3. Neonatal assessment are important because of the potential for subsequent abnormal neurodevelopment . (II-2 B).
MILD VENTRICULOMEGALY
SOGC guidelines June 2005

HOLOPROSENCEPHALY Diagnosis: In the standard transverse view of the fetal
head for measurement of the biparietal diameter there is a single dilated midline ventricle replacing the two lateral ventricles or partial segmentation of the ventricles.
The alobar and semilobar types are often associated with facial defects, such as hypotelorism or cyclopia, facial cleft and nasal hypoplasia

HOLOPROSENCEPHALY

MICROCEPHALY Microcephaly means small head and brain. Prevalence: Microcephaly is found in about 1 per 1,000
births. The diagnosis is made by the demonstration of brain abnormalit ies, such as holoprosencephaly.
In cases with apparently isolated microcephaly it is necessary to demonstrate progressive decrease in the head to abdomen circumference rat io to below the 1st centi le with advancing gestation. Such diagnosis may not be apparent before the third tr imester.
In microcephaly there is a typical disproport ion between the size of the skull and the face.

MICROCEPHALY

CHOROID PLEXUS CYSTS
Definit ion and Imaging CriteriaChoroid plexus cysts (CPCs) are small
cysts ( 3 mm) found in the choroid plexus within
the lateral cerebral ventricles at 14 to 24 weeks .
Prevalence: Choroid plexus cysts are found in about
2% of fetuses at 20 weeks of gestation but in more than 90% of cases they resolve by 26 weeks.


CHOROID PLEXUS CYSTS


Recommendations1. Isolated CPCs require no further investigation when maternal age or the serum screen equivalent is less than
the risk of a 35-year-old (II-2 E).2. Fetal karyotyping should only be offered if isolated CPCs
are found in women 35 years or older or if the maternal serum screen is positive for either trisomy 18 or 21 (II-2 A).
3. All women with fetal CPCs and additional malformation or additional soft markers should be offered referral and karyotyping (II-2 A).
CHOROID PLEXUS CYSTS
SOGC guidelines June 2005

Enlarged cisterna magna If the cisterna magna is
subjectively increased, a measurement should be taken . (III-B).
The mean diameter of a normal cisterna magna is 5 mm, 10 mm is considered an abnormality



Enlarged cisterna magna
1. An isolated enlarged cisterna magna is not an indication for fetal karyotyping (III-D).
2. With an enlarged cisterna magna, look for other anomalies, growth restriction, or abnormal amniotic fluid volume. (III-B).
3. If the enlarged cisterna magna is seen in association with other abnormal findings, fetal karyotyping should be offered . (III-B).
SOGC guidelines June 2005

It must be emphasised that prenatal testing is a two-edged tool; it can be used either with a view to allow the opportunity for prenatal counseling with a multidisciplinary team of experts to permit the planning of the mode and site of delivery, thus ensuring optimal care of the fetus and the newborn.
, or it may be used with a view to selective abortion in order to avoid the birth of a disabled child.
The tests themselves can give rise to great worry and can be traumatic for the pregnant woman, even if her baby is found to be healthy.

Amniotic fluid

Amniotic f luid Qualitative evaluation of amniotic fluid is accurate when
assessed by an experienced operator The volume of the amniotic fluid is evaluated by visually
dividing the mother's abdomen into 4 quadrants. The largest vertical pocket of fluid is measured in centimeters. The total volume is calculated by multiplying this value by 4.
Polyhydramnios is usually defined as an amniotic fluid index (AFI) more than 24 cm or a single pocket of fluid at least 8 cm in deep that results in more than 2000 mL of fluid.
Oligohydramnios is defined as an AFI less than 7 cm or the absence of a fluid pocket 2-3 cm in depth.
E-medicine 3-2006

Prenatal ultrasonography and oligohydramnios Levels less than 5 cm indicate signif icant
ol igohydramnios. Visualize the fetal kidneys, collecting
system, and bladder. If these are normal, suspect the chronic leakage of amniotic f luid.
Assess fetal growth. I f PROM or urinary tract anomalies are absent, consider placental insuff iciency and IUGR.
Uterine artery Doppler study f indings may aid in the diagnosis of placental insuff iciency.

Prenatal ultrasonography and polyhydramnios
Evaluate fetal swallowing. A decrease in fetal deglutit ion occurs in anencephaly, tr isomy 18, tr isomy 21, muscular dystrophy, and skeletal dysplasia.
Evaluate the fetal anatomy; assess for diaphragmatic hernia, lung masses, and the absence of the stomach bubble (which is associated with esophageal atresia). The double-bubble sign or a dilated duodenum suggests the possibil i ty of duodenal atresia.
An abnormally large abdominal circumference may be observed with ascites and hydrops fetalis or a macrosomic fetus; these findings are also observed in association with poorly controlled maternal diabetes.

placenta

PLACENTAL LOCALISATION
The relationship between the lower margin of the placenta and the internal os should be determined.

Definition Placenta previa is a placental
implantation that overlies or is within 2 cm of the internal cervical os.
a complete previa when it covers the os a marginal previa when the edge lies
within 2 cm of the os. Low lying when the edge is 2 to 3.5 cm
from the os.

placenta praevia
Ultrasound Findings.. The maternal urinary bladder may be used as
a landmark to identify the location of the internal cervical os.
The most common conditions that cause a false diagnosis of placenta previa are an overdistended bladder and myometrial contractions.

placenta praevia

placenta praevia


Accreta, Increta, Percreta Placenta accreta is the abnormal
adherence of part or all of the placenta with partial or complete absence of the decidua basalis.
Placenta increta is further extension of the placenta through the myometrium.
Placenta percreta is penetration of the uterine serosa.


Risk factor PP with Unscarred uterus, 1 to 5 percent One previous cesarean birth, 25% Two previous cesarean births, 40% Four or more previous cesarean births,
50 to 67 % Other risk factors include maternal age
>35 years, endometrial defects (Ascherman syndrome), and submucous leiomyomata.

The most prominent gray scale features to suggest placenta accreta are:-
• (1) loss of the normal hypoechoic retroplacental myometrial zone.
• (2) thinning or disruption of the hyperechoic uterine serosa-bladder interface.
• (3) the presence of multiple lakes that represent dilated vessels extending from the placenta through the myometrium.

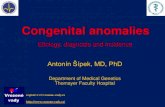
newly formed vessel + multiple placental lakes

The uterine segment is shown total ly destroyed.

the multiple layers of newly formed vessel between uterus and the bladder


Color-flow Doppler ultrasonogram demonstrating placenta percreta with bladder invasion.


Placental sizePlacentomegaly On ultrasound the placenta thickness measures
more than 5 cm. Maternal diabetes and Rh incompatabil i ty are primary causes for placentomegaly
Other causes include :Maternal anemia, a-thalassemia, Chronic intrauterine infections ,twin-twin transfusion syndrome, Congenital neoplasms and fetal malformations
SmallPlacenta: IUGR,, Intrauterine infection, Chromosomal
abnormality

Abruptio Placenta
Ultrasound Findings Upon examination of the placenta, the sonographer will notice an abnormality in the texture and size of the placenta. If a hemorrhage is present, the echogenicity depends on the age of the hemorrhage; the acute bleed is hyperechoic to isoechoic while the chronic bleed is more hypoechoic.

hydatidiform mole Ultrasound Findings uterine size larger than dates, no identifiable fetal parts,
inhomogeneous texture of the placenta that represent the multiple vesicular changes. Bilateral theca luetin cysts are seen in the ovaries.
A partial mole is associated with an abnormal fetus or fetal tissue. On ultrasound a reduced amount of amniotic fluid is noted. The placenta is thick with multiple intraplacental cystic spaces.
A coexistant mole and fetus is very rare; the mole may result from a hydatidiform degeneration of a twin fetus. This condition is more likely when two placentas are present. The abnormal placenta is hyperechoic with multiple small cysts. The coexisting fetus is live with a normal placenta.

Chorioangioma A benign vascular tumor of the placenta. Second to trophoblastic disease, chorioangioma is the
most common "tumor" of the placenta, occurring in 1% of pregnancies.
Complications include polyhydramnios, premature labor, fetal hydrops, fetal cardiomegaly, intrauterine growth retardation, and fetal demise. The maternal serum AFP may be elevated.
Ultrasound shows a circumscribed solid or complex mass that protrudes from the fetal surface of the placenta. It may be located near the umbilical cord site.

Chorioangioma

Chorioangioma

Chorioangioma

Placental grading
Grade 0 Late 1st trimester-
early 2nd trimester Uniform moderate
echogenicity Smooth chorionic
plate without indentations

Placental grading Grade 1 Mid 2nd tr imester –
early 3rd tr imester (~18-29 wks)
Subtle indentations of chorionic plate
Small, dif fuse calcif ications (hyperechoic) randomly dispersed in placenta

Placental grading Grade 2 Late 3rd tr imester
(~30 wks to delivery) Larger indentations
along chorionic plate Larger calcif ications
in a “dot-dash” configuration along the basilar plate

Placental grading Grade 3 39 wks – post dates Complete
indentations of chorionic plate through to the basilar plate creating “cotyledons”
More irregular calcif ications with signif icant shadowing