Congenital Cardiovascular Anomalies

of 36
Transcript of Congenital Cardiovascular Anomalies
-
7/28/2019 Congenital Cardiovascular Anomalies
1/36
Congenital Cardiovascular
Anomalies
dr. Herlina Dimiati, SpA (K)
SMF / Bagian Kardiologi Pediatrik
RSU Dr. Zainal Abidin
Fakultas Kedokteran Universitas Syiah Kuala
Banda Aceh
-
7/28/2019 Congenital Cardiovascular Anomalies
2/36
Classification of CHDs
1. Structural heart defects due to
abnormal development of the heart
during the first 2 months after conception
2. Functional heart defects
ex: congenital heart block
1. Positional heart defects ex: dextrocardia
-
7/28/2019 Congenital Cardiovascular Anomalies
3/36
Dextrocardia
May occur: With Situs Inversus: carries
a slightly increased risk ofheart defects (~ 5 10%associated with other
CHDs)
Without Situs Inversus:carries a greatly increasedrisk of associated heartdefects (~95% associatedwith other CHDs)
Both conditions areEXTREMELY rare
Situs Inversus
-
7/28/2019 Congenital Cardiovascular Anomalies
4/36
Classifications of
Structural Congenital Heart Defects
Increased
Pulmonary
Blood Flow
Decreased
Pulmonary
Blood Flow
Obstruction to
Systemic Blood
Flow
PDAASD
VSD
AV Canal
Total Anomalous
Pulmonary Venous
Return
Truncus Arteriosis
Tetralogy of FallotTransposition of the
Great Arteries
Pulmonary Stenosis
Pulmonary Atresia
Tricuspid Atresia
Coarctation of theAorta
Aortic Stenosis
Hypoplastic Left
Heart Syndrome
Mitral Stenosis
-
7/28/2019 Congenital Cardiovascular Anomalies
5/36
Shunts
Right to Left vs. Left to Right
Right to left shunt: un-oxygenated blood is
shunted from the right side of the heart to the left
side, and then enters the systemic circulation.
Left to right shunt: a portion of the oxygenated
blood is shunted from the left side of the heart to
the right side and enters the pulmonarycirculation, increasing the work load for the right
heart
-
7/28/2019 Congenital Cardiovascular Anomalies
6/36
Cyanotic vs. Acyanotic
Acyanotic (usually left to right shunts):
PDA, ASD, VSD
Cyanotic (right to left shunts):
TOF, Transposition of the Great Arteries, HypoplasticLeft Heart
O2 Sat less than 95%
Child may have chronic hypoxia
Caused by: Decreased pulmonary blood flowand/or-- Right-to-left shunting: de-oxygenated blood is shunted from the right side of the heart to the
left side without traveling though the pulmonary circulation, and blood ejected from the left
side of the heart to the systemic circulation is only partly oxygenated
-
7/28/2019 Congenital Cardiovascular Anomalies
7/36
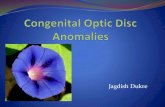
Most Common Congenital Heart
Defects
9%10%
12%
10%15%
44%
Atrioventricular Septal
Defect
Coarctation of theAorta
Tetralogy of Fallot
Transposition of the
Great Arteries
Ventricular Septal
Defects
All other congenital
heart defects
These account for 85% of all
CHDs:
-
7/28/2019 Congenital Cardiovascular Anomalies
8/36
Some Statistics
Most common birth defect 30% of all
congenital birth defects
(36,000/yr in the United States)
Most common cause of infant death for children
dying as the result of a birth defect
In the US over 130,000 hospitalizations/year are
related to CHD
-
7/28/2019 Congenital Cardiovascular Anomalies
9/36
Etiology of CHD
Unknown in most cases
Incidence of CHD in children is slightly
increased if a sibling or parent has CHD
Gender Factors
Environmental Factors
Genetic Factors
-
7/28/2019 Congenital Cardiovascular Anomalies
10/36
Gender Factors
Occur equally among males and females,
but
More common in males:
aortic stenosis, coarctation of the aorta
More common in females:
PDAs, ASDs
-
7/28/2019 Congenital Cardiovascular Anomalies
11/36
Environmental Factors
Maternal Infections: Rubella: PDA, pulmonary stenosis, VSD, ASD
Maternal Drugs:
Lithium: Tricuspid valve abnormalities, Ebsteins Anomaly
Thalidomide
Possibly related to CHDs: Dilantin & Cocaine Alcohol abuse: VSD
Maternal Disease:
Diabetes: transportation of the great vessels, VSD, situs inversus,single ventricle, hypoplastic left ventricle
SLE: Congenital heart block
-
7/28/2019 Congenital Cardiovascular Anomalies
12/36
Genetic Factors
Trisomy 21 (Downs Syndrome):
A-V canal defects, VSD
XO (Turners Syndrome):coarctation of the aorta, aortic stenosis
Osteogenesis Imperfecta:
Aortic incompetence
Marfan Syndrome:
Aortic dilatation, aortic & mitral incompetence
-
7/28/2019 Congenital Cardiovascular Anomalies
13/36
The good news is--
From 1991 2001 deaths related to CHD
declined 28% due to improvements in surgical
techniques and medical management
-
7/28/2019 Congenital Cardiovascular Anomalies
14/36
Prevention of CHD
Not possible in most cases
But -- there are actions a woman can take to
reduce her risk of having a child with CHD:
Abstain from alcohol during pregnancy
Be immunized against rubella before conception
If diabetic, maintain tight control of blood sugars
Folic acid 400 mcg/daily before conception may help
to prevent CHD (unproven)
If there is a family history of CHD seek genetic
counseling prior to conception
-
7/28/2019 Congenital Cardiovascular Anomalies
15/36
Signs/Symptoms of CHD
Murmurs
Cyanosisworsens with crying or other exertion
Respiratory distress
Signs of poor perfusion, such as slow capillary
refill, diminished peripheral pulses
Fatigue commonly observed during feedings in
newborns or during play in children Failure to thrive
-
7/28/2019 Congenital Cardiovascular Anomalies
16/36
Embryonic Heart Development
The heart develops in the embryo duringpost-conception weeks 3 - 8
-
7/28/2019 Congenital Cardiovascular Anomalies
17/36
Beginning Development
Early week 3 post-conception: heart begins as 2
endothelial tubes
Mid-week 3 : endothelial tubes fuse to form a
tubular structure 28 days following conception: the single-
chambered heart begins pumping blood
-
7/28/2019 Congenital Cardiovascular Anomalies
18/36
Week 4
Heart has:
single outflow tract, the truncus arteriosus (divides to
form aorta & pulmonary veins)
Single inflow tract, the sinus venosus (divides to formthe superior and inferior vena cavae)
Single atrium
Single ventricle
AV canal begins to close
-
7/28/2019 Congenital Cardiovascular Anomalies
19/36
Weeks 5 - 7
Week 5
AV canal closure
complete
Formation of atrial andventricular septums
Heart growing rapidly,
and folds back on itself to
form its completed
anatomic shape
Week 7
Ventricular septum fully
developed
Coronary Sinus forms Outflow tracts (aorta &
pulmonary truck) fully
separated
-
7/28/2019 Congenital Cardiovascular Anomalies
20/36
8 Weeks After Conception
By the end of the 8th week after conception the
fetus has a fully developed 4-chambered heart
-
7/28/2019 Congenital Cardiovascular Anomalies
21/36
Fetal Circulation
Before birth the placenta provides the
oxygen needed by the developing fetus
the lungs receive only enough blood to
perfuse the lung tissues due to highpulmonary vascular resistance & fetal
vascular shunts
-
7/28/2019 Congenital Cardiovascular Anomalies
22/36
-
7/28/2019 Congenital Cardiovascular Anomalies
23/36
Fetal Circulation
Arterial blood in the fetus:
enters the fetal circulation via the umbilical vein:
passes through the ductus venosus and enters the
inferior vena cava flows into the right atrium and passes through the
foramen ovale into the left side of the heart
passes from the right side of the heart, through the
ductus arteriosus to enter the systemic circulation,bypassing the pulmonary circulation
-
7/28/2019 Congenital Cardiovascular Anomalies
24/36
Fetal Circulation
Venous blood in the fetus:
returns to the placenta through the 2 umbilical
arteries
-
7/28/2019 Congenital Cardiovascular Anomalies
25/36
After Birth
Lungs distend with air and pulmonary
vascular resistance falls. Pulmonary
blood flow increases
The foramen ovale and ductus venosususually close during the first day of life
The ductus arteriosus usually closes
during the first 24 72 hours of life
-
7/28/2019 Congenital Cardiovascular Anomalies
26/36
Common Congenital Heart
Anomalies
-
7/28/2019 Congenital Cardiovascular Anomalies
27/36
Patent Ductus Arteriosus (PDA)
Usually closes within 24 to 72 hours after birth
Closure of the ductus may be delayed, or not
occur at all in preterm infants
Patent PDA causes increased pulmonary bloodflow, pulmonary congestion, increases the
workload of the right ventricle; causes increased
pulmonary venous return and increases
workload of the right ventricle
-
7/28/2019 Congenital Cardiovascular Anomalies
28/36
PDA
-
7/28/2019 Congenital Cardiovascular Anomalies
29/36
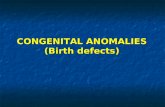
Coarctation of the Aorta
Localized narrowing of
the aorta
More common in males
than females
Associated with Turners
Syndrome
Most common clinical
sign: weak pulses &
decreased blood
pressure in the lower
extremities
-
7/28/2019 Congenital Cardiovascular Anomalies
30/36
VSD
Most common
congenital heart
defect
May occur alone, orwith other
abnormalities
About one-third of
small VSDs will close
spontaneously
-
7/28/2019 Congenital Cardiovascular Anomalies
31/36
Truncus Arteriosus
Truncus fails to dividecompletely duringfetal life, leaving aconnection between
the aorta andpulmonary arteries
Mixed oxygenatedand de-oxygenatedblood exits the heartand enters thesystemic circulation
-
7/28/2019 Congenital Cardiovascular Anomalies
32/36
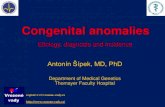
Tetralogy of Fallot
TOF = Ventricular septal
defect
Aorta position is
shifted to the right andover-rides the VSD
Stenosis of thepulmonary outflow
tract, often involvingthe pulmonary valve
Hypertrophy of theright ventricle
-
7/28/2019 Congenital Cardiovascular Anomalies
33/36
Transposition of the Great Vessels
The aorta originates from
the right ventricle; the
pulmonary artery
originates in the left
ventricle A PDA is necessary for
these infants to survive
until they can have
corrective surgery More common in infants
of diabetic mothers
-
7/28/2019 Congenital Cardiovascular Anomalies
34/36
Hypoplastic Left Heart
Fatal without early
surgical intervention
-
7/28/2019 Congenital Cardiovascular Anomalies
35/36
TAPVR
The pulmonary veins,
instead of being
connected to the left
ventricle, areconnected to the right
ventricle or superior
vena cava, and return
oxygenated blood tothe right side of the
heart.
-
7/28/2019 Congenital Cardiovascular Anomalies
36/36
AV Canal
Includes:
ASD
VSD
Abnormalities of theMitral and/or Tricuspid
valves
Greater incidence inchildren with Downs
Syndrome