Physiopathology of idiopathic nephrotic syndrome: lessons from glucocorticoids and epigenetic...
8
REVIEW Physiopathology of idiopathic nephrotic syndrome: lessons from glucocorticoids and epigenetic perspectives Valéry Elie & May Fakhoury & Georges Deschênes & Evelyne Jacqz-Aigrain Received: 24 March 2011 /Revised: 30 May 2011 /Accepted: 2 June 2011 /Published online: 28 June 2011 # IPNA 2011 Abstract Idiopathic nephrotic syndrome (INS) has been studied for decades in attempt to understand the physio- pathological mechanisms explaining the disease. It is recognized as a multifactorial disease, with immunological components targeting kidney functions. Many hypotheses have been discussed or tested, including the role of a circulating factor, polymorphisms of genes implicated in lymphocyte maturation and differentiation, and DNA epigenetic modifications. In the present review, the data supporting these different (and probably combinatorial) hypotheses have been reviewed in order to identify and discuss the possible pathways implicated in the physiopa- thology of INS. Keywords Epigenetics . Glucocorticoids . Kidney disease . Nephrotic syndrome . Proteinuria . Pediatric . Idiopathic nephrotic syndrome . INS Introduction Idiopathic nephrotic syndrome (INS) is the most prevalent kidney disease in children. Described as a rare and complex disease, INS is clinically defined by the triad of massive proteinuria (>50 mg/kg/day), edema and hypoalbuminemia (<30 g/l), linked to glomerular damage. The complexity of the disease relies on its definition that regroups a large diversity of patterns, all resulting in massive proteinuria. Two major groups of INS can be defined: the genetically determined forms, including the congenital Finnish type NS [1] (excluded from the scope of this review) and the acquired nephrotic syndromes. Histologically, three patterns are observed: minimal change nephrotic syndrome (MCNS), focal segmental glomerulosclerosis (FSGS) and mesangial proliferative glomerulonephritis (MPGN), where MCNS is the most prevalent histological pattern [2]. All these forms share a common feature, which is a podocyte foot process effacement, with a structural disorganization of the glomerular filtration barrier leading to proteinuria. However, the mechanisms underlying these structural changes are poorly understood, and seem quite different from these diverse forms. Historically, management of nephrotic syndrome is based on guidelines from the International Study of Kidney Disease in Children (ISKDC)[3] and the Arbeitsgemein- schaft für Padiatrische Nephrologie (APN)[4]. INS is often completely reversible after initiation of treatment based on oral glucocorticoids (GC)[5]. However, the evolution is characterized by a succession of remissions and relapses, often extended over several years before definitive cure. At the first manifestation of nephrotic syndrome, patients receive daily prednisone therapy for 4 to 6 weeks, for a cumulative dose of 3,000–4,000 mg/m 2 , depending on the V. Elie : M. Fakhoury : E. Jacqz-Aigrain (*) Department of Pediatric Pharmacology and Pharmacogenetics, Clinical Investigation Center CIC Inserm 9202, Hôpital Robert Debré, 48 Boulevard Sérurier, 75935 Paris Cedex 19, France e-mail: [email protected] M. Fakhoury : E. Jacqz-Aigrain Clinical Investigation Center (CIC) INSERM 9202, Hôpital Robert Debré, 48 Boulevard Sérurier, 75935 Paris Cedex 19, France G. Deschênes Department of Pediatric Nephrology, Hôpital Robert Debré, 48 Boulevard Sérurier, 75935 Paris Cedex 19, France Pediatr Nephrol (2012) 27:1249–1256 DOI 10.1007/s00467-011-1947-1
Transcript of Physiopathology of idiopathic nephrotic syndrome: lessons from glucocorticoids and epigenetic...

REVIEW
Physiopathology of idiopathic nephrotic syndrome:lessons from glucocorticoids and epigenetic perspectives
Valéry Elie & May Fakhoury & Georges Deschênes &
Evelyne Jacqz-Aigrain
Received: 24 March 2011 /Revised: 30 May 2011 /Accepted: 2 June 2011 /Published online: 28 June 2011# IPNA 2011
Abstract Idiopathic nephrotic syndrome (INS) has beenstudied for decades in attempt to understand the physio-pathological mechanisms explaining the disease. It isrecognized as a multifactorial disease, with immunologicalcomponents targeting kidney functions. Many hypotheseshave been discussed or tested, including the role of acirculating factor, polymorphisms of genes implicated inlymphocyte maturation and differentiation, and DNAepigenetic modifications. In the present review, the datasupporting these different (and probably combinatorial)hypotheses have been reviewed in order to identify anddiscuss the possible pathways implicated in the physiopa-thology of INS.
Keywords Epigenetics . Glucocorticoids . Kidney disease .
Nephrotic syndrome . Proteinuria . Pediatric .
Idiopathic nephrotic syndrome . INS
Introduction
Idiopathic nephrotic syndrome (INS) is the most prevalentkidney disease in children. Described as a rare and complexdisease, INS is clinically defined by the triad of massiveproteinuria (>50 mg/kg/day), edema and hypoalbuminemia(<30 g/l), linked to glomerular damage. The complexity ofthe disease relies on its definition that regroups a largediversity of patterns, all resulting in massive proteinuria.
Two major groups of INS can be defined: the geneticallydetermined forms, including the congenital Finnish type NS[1] (excluded from the scope of this review) and theacquired nephrotic syndromes. Histologically, three patternsare observed: minimal change nephrotic syndrome(MCNS), focal segmental glomerulosclerosis (FSGS) andmesangial proliferative glomerulonephritis (MPGN), whereMCNS is the most prevalent histological pattern [2]. Allthese forms share a common feature, which is a podocytefoot process effacement, with a structural disorganization ofthe glomerular filtration barrier leading to proteinuria.However, the mechanisms underlying these structuralchanges are poorly understood, and seem quite differentfrom these diverse forms.
Historically, management of nephrotic syndrome isbased on guidelines from the International Study of KidneyDisease in Children (ISKDC)[3] and the Arbeitsgemein-schaft für Padiatrische Nephrologie (APN)[4]. INS is oftencompletely reversible after initiation of treatment based onoral glucocorticoids (GC)[5]. However, the evolution ischaracterized by a succession of remissions and relapses,often extended over several years before definitive cure. Atthe first manifestation of nephrotic syndrome, patientsreceive daily prednisone therapy for 4 to 6 weeks, for acumulative dose of 3,000–4,000 mg/m2, depending on the
V. Elie :M. Fakhoury : E. Jacqz-Aigrain (*)Department of Pediatric Pharmacology and Pharmacogenetics,Clinical Investigation Center CIC Inserm 9202,Hôpital Robert Debré,48 Boulevard Sérurier,75935 Paris Cedex 19, Francee-mail: [email protected]
M. Fakhoury : E. Jacqz-AigrainClinical Investigation Center (CIC) INSERM 9202,Hôpital Robert Debré,48 Boulevard Sérurier,75935 Paris Cedex 19, France
G. DeschênesDepartment of Pediatric Nephrology, Hôpital Robert Debré,48 Boulevard Sérurier,75935 Paris Cedex 19, France
Pediatr Nephrol (2012) 27:1249–1256DOI 10.1007/s00467-011-1947-1

treatment protocol (60 mg/m2/day for 4 weeks recommendedby the “Société de Néphrologie Pédiatrique” and 2 mg/kg perday for 6 weeks, recommended by ISKDC/APN studies,never exceeding 60 mg/day) followed by 4–6 weeks onalternate therapy (1.5 mg/kg ISKDC/APN, maximum 40 mg).Remission (defined by proteinuria/creatininuria <0.1 g/mmol)is usually obtained within 4 weeks of daily GC therapy and inthis case, the INS is classified as steroid-sensitive (SSNS). Incases of relapse during the alternate therapy, treatment isrestarted at the first dose [5]. If remission cannot beachieved within 4 weeks, INS is classified as steroid-sensitive but remains dependant on GC administration(SDNS). If remission cannot be obtained under GCtreatment, the INS is classified as steroid-resistant (SRNS)and treatment associated to anti-calcineurin immunosup-pressants, usually cyclosporin.
Under treatment, clinical signs progressively decreasewhile podocyte foot process effacement completelyreverses. Morbidity of INS relies on its chronicity,complicated with irreversible sequelaes resulting fromsteroid administration, systemic bacterial infection, orvascular thrombosis.
Precise epidemiological data on INS are limited [6, 7].Its incidence depends on age, ethnicity, sex, and livingenvironment [6] and interestingly, there is a huge differencein the average length of the disease according to the age ofonset, ranging from 11.5 years when the disease starts at2 years of age, and 1.5 years when it appears after 14 yearsof age [8].
Many hypotheses have been made on the physiopa-thology of INS, but none fully explains the occurrence ofthe disease. The triggers, patients’ immune specificitiesand the molecular mechanisms explaining glomerularchanges, are poorly understood, though, SSNS isconsidered as a complex multifactorial disease, with animmunological component. Various hypotheses include aT-lymphocyte helper 2 (Th2) polarization and regulatoryT-cells (Tregs)[9, 10], DNA hypersensitivity affectingT-cell differentiation, and epigenetic modifications of
glucocorticoids [11]. All are discussed in the presentreview, focusing on MCNS and presented in Table 1.
Glucocorticoids and nephrotic syndrome
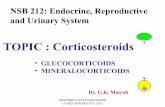
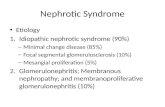
GCs are mainly known for their anti-inflammatory andimmunosuppressive properties, acting on lymphocytes andinflammatory cells through the inhibition of the NF-κBtranscription factor pathway [12]. GCs also act on a widediversity of target cells (dendritic, epithelial, and endothe-lial cells) mainly by inhibition of pro-inflammatory cyto-kine gene transcription [13] (Fig. 1) and more interestingly,by inhibition of production and proliferation functions(through apoptosis) of helper, cytotoxic, and suppressiveT-cells. In addition to the genomic effect on target genetranscription, GCs exert a rapid non-genomic effect viadirect interaction of the active glucocorticoid receptor (GR)with target proteins such as NF-κB [12] (Fig. 2). Thus,GC’s high efficacy in reversing INS symptoms pledges infavor of an immune system deregulation, especially of T-cell and NF-κB pathways. Moreover, the quick protein-uria remission induced by GCs is in favor of a non-genomic effect of GCs on these pathways. As aconsequence, most of the studies have tried to identifyphysiopathological mechanisms of INS towards T-lymphocyte pathways.
Nephrotic syndrome: an immune disease?
Involvement of the immune system in the physiopathologyof INS is highly suspected since efficient treatment withglucocorticoids and immunosuppressants have a profoundeffect on immune cells.
The central role of GCs in reversing clinical symptomssuggests that INS is an immunological disease, with thekidney being the target of a trigger circulating factor, notyet identified, but obviously secreted by immune cells [14].
Table 1 Hypotheses on idiopathic nephrotic syndrome
Hypothesis Pre-clinical and/or clinical data Reference
T cell dysfunction and cytokine Efficacy of GCs on NS thymic dysregulationcirculating factor (T-cell secreted)
[9, 14, 19, 31, 34, 35]
B cells and immunoglobulins Rituximab efficacy on SDNS and SRNS circulatingfactor (B-cells secreted) RAG hypomorphic mutations
[16, 30, 39]
Immature immune cells CD34+ cells injection in NOD/SCID micethymic dysregulation
[18, 24]
NF-κB pathway Glucocorticoids efficacy, non-genomic effects [9, 18]
Viral infection First outbreak of INS often associated with viral infection [17, 65]
Podocyte dysfunction Enzymatic disturbances, protein expressionalterations (c-mip, angptl4, GPC5)
[47, 49, 50, 52, 53]
1250 Pediatr Nephrol (2012) 27:1249–1256

Moreover, not only GCs but also calcineurin inhibitors(CI), cyclosporin, and tacrolimus, indicated immune cellsas key effectors in INS. Used in the treatment of SDNS andSRNS, they demonstrated efficacy in reducing proteinuriathrough inhibition of the adaptive immune response [15]. Inaddition, mycophenolic acid, also active in INS, acts byinhibiting lymphocyte proliferation and B-cell productionof immunoglobulins [15], whose depletion from plasmaleads to a reduction in proteinuria.
Recently, the anti-CD20 monoclonal antibody rituximabhas shown an unexpected efficacy in SDNS and SRNS,inducing rapid and long-term remission even inmultirelapsingpatients who did not respond to treatments primarily active onT-cells (including cyclosporin, cyclophosphamide, tacrolimus,prednisone). CD20 is largely expressed on B-lymphocytesand rituximab treatment resulted in a complete depletion ofcirculating B-lymphocytes, but had no effect on B-cellprecursors or differentiated B-cell (plasma cell) populations
[16]. Altogether, these data suggest that not only T-cells butalso B-cells or B-cell products might be implicated in thecausal mechanism of INS through abnormal regulation ofT-cell function by circulating B-cells or communicationbetween B and T cells. However, T-cells still remain themajor cell subtype investigated and implication of B-cells inINS needs to be investigated more deeply.
As prior infection of upper airways has been recognizedas a factor associated with SSNS and steroid-dependency ofthe disease, it is hypothesized that SSNS might be anacquired kidney disease [17]. Recently, transcriptionaldifferences in T-cells from nephrotic patients in remissioncompared to T-cells from non-affected patients, sampledaway from any infection, reported different expressionprofiles of proteins involved in the regulation of apoptosisand activation of the transcription factor NF-κB [9, 18].The NF-κB pathway has been reported to be deregulated inMCNS patient T-cells. Relapsing patients showed increasedactivation of the NF-κB pathway persisting during theactive phase of the disease but repressed in remission [9].IκBKβ, an NF-κB pathway key regulator, and interestingly,sCD25, a T-cell activation marker, were overexpressedduring relapses [18]. Moreover, numerous cases of MCNSoccurring with Hodgkin’s disease, known to be a T-celldisorder, have been observed [19, 20].
Two additional proteins, c-maf (proto-oncogen) andTc-mip (form of c-mip resulting from alternative splicing)were also implicated. The c-maf protein is involved in thepolarization inhibition of T-cells towards Th1 phenotypeand is reported to be highly expressed only in patients withfrequent relapses [21], which is consistent with the Th2
Fig. 1 Glucocorticoids effects and target cells
Fig. 2 Schematic immunosup-pressive and anti-inflammatorymechanisms of action ofglucocorticoids on T-cells
Pediatr Nephrol (2012) 27:1249–1256 1251

polarization of T-cells recurrently observed in INS [22].Similarly, Tc-mip is implicated in c-maf activation andhighly expressed in MCNS Th2 CD4+ T-cells, while totallyabsent in non-nephrotic patients [21]. These findings areconcordant with the observed abnormal RNA processingand altered expression of serin-rich proteins, involved inmRNA splicing, within MCNS T-cells [23] suggesting thatMCNS T-cell dysfunction might be associated with abnormalmRNA splicing/transcription machinery (Table 1).
Relapse was also associated with induction of L-selectinand T-lymphocyte maturation-associated proteins, markersof T-cell differentiation and recent emigrant/naive T-cells,suggesting a thymic deregulation of apoptosis precursors inMCNS [18]. This hypothesis was strengthened by datafrom a mouse model of INS, where injection of CD34+ stemcells from affected patients induced albuminuria with podo-cyte foot process effacement, arguing for a role of immaturecells more than mature peripheral cells [24]. Also, a stem cellmobilization, decrease in CD19+ cells, and increase inNatural Killer (NK) cells were reported in SSNS duringrelapse [25], thus indicating an autoimmune disease targetingthe podocytes.
The thymus is the primary lymphoid organ implicated inT-cell differentiation and establishment of self-tolerance.Thymic nurse cells (TNC) interact with immature thymo-cytes responsible for their differentiation and selection.TNCs express self-antigens whose intrathymic transcriptionis regulated by the AutoImmune REgulator protein (AIRE),which is expressed in peripheral CD4+ T-cells and at a highlevel in antigen- and IL2-stimulated T-cells [26]. AIRE hasbeen implicated in autoimmune diseases and most interest-ingly, loss of AIRE-dependent expression of a peripheraltissue antigen makes it a target of B and T-cells [27].
Immune deregulation is also supported by regulatory FoxP3T-cells (Tregs), critical in the transfer of immune tolerance,especially self-tolerance. Injection of Foxp3-positive T-cellsled to marked reductions in disease severity in animal modelsof asthma, renal disease, and multiple sclerosis [28], and moststrikingly, these FoxP3 Tregs were found to be decreased inpediatric primary nephrotic syndrome [29].
Circulating factor
The potential role of a circulating factor secreted by immunecells was suggested by Shalhoub [14] in 1974. Indeed, T-cellsand B-cells together might prompt the formation of cytokinesand immunoglobulins. However, all the studies trying toconfirm this attractive hypothesis failed to clearly identifyany circulating factor and therefore generated additionalhypotheses on what this factor might be [30, 31].
Such a circulating factor is highly suspected, as proteinuriaand NS rapidly reappear after kidney graft revascularization in
patients with a secondary steroid-resistant form of INS. Thereappearance of INS after kidney graft was first observed in1972 [32] with numerous additional studies establishing anaverage recurrence rate of 30%. Plasmapheresis efficiency inresolving disease progression and proteinuria [33], as well asthe induction of proteinuria after injection of rats withsupernatant from in vitro cultures of T-cell hybridomas fromINS patients [34], are both additional arguments in favor of acirculating factor (Table 1). Moreover, the search for thiscirculating factor identified diverse cytokine expressionmodifications (IL-4, IL-13) associated with MCNS,however, it still remains unclear whether these are a cause ora consequence of the disease [35].
The presence of immunoglobulins in the mesangium ofalmost half of the patients with INS, persistence of a deficit inIgG in remission evoking an alteration of their metabolism,and observations of MCNS in pathologies associated withmonoclonal light chains highly suggest a potential implicationof immunoglobulins and/or of defective machinery leading toabnormal immunoglobulins [30].
From that perspective, two proteins have interestingroles in immunoglobulin synthesis. Lymphocyte develop-ment involves Immunoglobulin V(D)J gene rearrangementresulting in a wide immune repertory by allelic exclusion. Ithas been demonstrated that IgK rearrangement is regulatedby NF-κB coordinating recombinase activator gene (RAG)expression [36]. RAG1 and RAG2 expression is restrictedto immature lymphocytes and the RAG1/2 complex isimplicated in the formation of diverse immunoglobulinsand T-cell receptors [37]. RAG1 mutations are oftenassociated with severe combined immune deficiency(SCID) and Omenn syndrome. These conditions arecharacterized by the lack of T and/or B-cells, but somehypomorphic mutations still allow the development of aresidual differentiation of T and/or B-cells [38]. Theseparticular cases of SCID are also characterized by thepresence of autoreactive T-cells and NK cells in peripheralblood, and some patients present a severe associatedCytomegalovirus (CMV) infection [39].
Proteins of the Interferon Regulatory Family (IRF) havean important role in B and T-cell differentiation andmaturation, especially the IRF4 protein that acts as atranscription factor in lymphocyte differentiation and isexpressed in B-cells (pre-B, B, and plasma-cells) andmature T-cells. In mature B-cells, IRF4 regulates Ig classswitch recombination and plasma cell differentiation [40].IRF4 also regulates the expression of a subset of Th2lymphocytes, specifically increasing their IL-4 and IL-10production, but does not induce other Th2 cytokines, whereasIRF4-deficient T-cells secrete decreased levels of Th2cytokines[41]. Interestingly, IL10 has been described as apotential factor in steroid resistance [42]. Additionally,Foxp3 Tregs might regulate the expression of IRF4 [43].
1252 Pediatr Nephrol (2012) 27:1249–1256

Nephrotic syndrome, a podocytopathy?
Apart from genetically determined forms of nephrotic syn-drome directly affecting podocyte structure and proteins likeFinnish-type NS, INS has always been thought to be animmune disease due to GC action on immune cells. Recently,new evidence of a direct effect of GCs on podocytes hasemerged, bringing new insight into nephrotic syndromephysiopathology [44, 45]. GRs have been found in podocytesand in addition to immune cells, their direct action resulted ina protective effect on podocytes, even in mice podocytes,enhancing their recovery via actin filament stabilization [44]and preventing PAN-induced apoptosis [46]. Moreover, adirect effect of cyclosporin has been demonstrated on thepodocyte actin cytoskeleton through inhibiting phosphoryla-tion of synaptopodin, a key protein involved in themaintenance of the glomerular basement membrane and stressfibers [47], suggesting that proteinuria could be a conse-quence of an enzymatic disturbance of the podocyte [48].
However, Shimada et al. proposed that INS could be a“two-hit” podocyte immune disorder, implicating both CD80expression deregulation on podocytes and dysfunctional Tregs[49]. More strikingly, the c-mip protein discovered in a T-celltranscriptome study has also been identified in podocytes ofaffected patients and its induction is closely related to theoccurrence of MCNS [20]. C-mip abundance increases in thepodocytes of patients with MCNS and induced proteinuria[50]. In vitro, the c-mip protein was also found to interactand inhibit the NF-κB transcription factor pathway inperipheral blood mononuclear cells, but not in podocytes[51], showing that more information is needed on thepotential effect of GCs on the c-mip protein.
Lately, a new podocyte-secreted substance has beenimplicated in the occurrence of SSNS proteinuria.Angiopoietin-like-4 (angptl4) is a podocyte-secreted glyco-protein and a mice model overexpressing angptl4 developsproteinuria and foot process effacement, which is reversible
after angptl4 expression normalization [52]. Furthermore,with the emergence of new technologies like genome-wideassociation studies (GWAS), researchers have found newleads that were not suspected. Indeed, glypicans, cell-surfaceheparin sulfate proteoglycans, were found to be associatedwith the occurrence of acquired nephrotic syndrome andpredominantly expressed and localized at podocyte cellsurface membranes [53]. Glypicans are implicated in severalsignal transduction pathways, and can also capture and holdvarious exogenous and endogenous products. Okamoto et al.suggested a role for the GPC5-FGF2 pathway in thepathogenesis of nephrotic syndrome, but also proposed thatsome unknown glypican-trapped molecules can induceand/or amplify podocyte injury [53]. Interestingly, thefindings about both GPC5 and angptl4 implicate thepodocyte but are also in favor of a circulating factor.
The epigenetic hypothesis
Epigenetics is the study of inherited modifications in geneexpression and phenotype caused by mechanisms otherthan changes in the underlying DNA sequence.
Unlike genetic polymorphisms, non-genetic partial andreversible DNA modifications can occur. From this point ofview, epigenetics is not only critical for generating diversityin cell types but is also important for maintaining thestability and integrity of the expression profiles of differentcell types. It has been described as a trigger factor in thedifferent steps of neoplastic progression [54] and associatedwith altered expression of key genes involved in cellgrowth and differentiation in diseases like cancer [55].
Epigenetic regulation is continuous throughout life withpermissive and suppressive factors controlling gene expres-sion, but epigenetic marks can spill over to the nextgeneration, resulting in a real inheritance of acquiredgenome modifications that can be potentially reversible
Fig. 3 Chromatin and histonemodifications
Pediatr Nephrol (2012) 27:1249–1256 1253

[56, 57]. Complex epigenetic modifications involve threemechanisms regulated by distinct but coupled pathways[58]: changes in DNA methylation by the DNA methyl-transferases (DNMTs), chromatin, and histone modificationby either histone acetyltransferases (HATs) or histonedeacetylases (HDAC) and gene silencing through RNAinterference (RNAi) [59] (Fig. 3). A high degree ofmethylation across the genome confers long-term epigeneticsilencing, whereas chromatin and histone modificationsinvolve mechanisms continuously packing and unpackingthe genome, ultimately regulating gene expression byrendering them accessible/inaccessible to the transcriptionmachinery. Epigenetic status varies with age as age-dependentepigenetic changes in the level of methylated cytosine invarious tissues have been reported [60]. The epigenome ishighly influenced by environmental factors, such as toxins ornutriment, and dietary modifications can have a profoundeffect on DNA methylation.
One of the most striking examples of such an environ-mental impact is the methylation modification of the GRassociated with altered histone acetylation observed in thehippocampus of rat pups in response to maternal groomingthat persists into adulthood. HDAC inhibitor injectionremoved the differences in histone acetylation and DNAmethylation, as well as in GR expression, suggesting acausal relationship between epigenomic state and GRexpression in the offspring [61]. Similarly, the epigeneticstatus of the disease gene(s) might be misregulated to someextent from birth, but well tolerated by the cell, delayingthe age of onset of a disease or resulting clinically inremission and relapse episodes [56] as observed in INS.
In addition, hormone-induced epigenetic changes have animpact on gene expression by changing chromatin conforma-tion and may trigger the disease process contributing, by thismechanism, to sex susceptibility to complex diseases [62].
Recently, epigenetics has been implicated in chronickidney diseases [63]. Increases or decreases in theexpression of specific proteins in INS, during relapse orin remission has previously been described. Modulation ofprotein expression is largely the result of epigenetics,thereby evoking this mechanism in the physiopathologyof INS as already suggested in pathologies such as COPD(chronic obstructive pulmonary disease) and severe asthma[64], also suggested in schizophrenia, where epigeneticchanges result in remission/relapse cycles during diseaseprogression [56].
Furthermore, the GC mechanism of action involveschanges in histone acetylation in order to regulate inflam-matory and anti-inflammatory genes through HDAC2.Deacetylated GR inhibits NF-κB-activated inflammatorygenes through interaction with the NF-κB complex [64].Such epigenetic action of GCs might reverse epigeneticanomalies, triggering INS.
The first outbreak of nephrotic syndrome is often associatedwith a viral infection of the upper airways [65]. A deregulationof the NF-κB pathway has been ruled out, while it has beendemonstrated that a viral infection could lead to DNAmodifications in infected cells (through an epigeneticmechanism, by the cells themselves or even by the virus) inan attempt to escape the immune system[66, 67]. Moreover,the IL-4 gene in Th2 IL-4-producing and non-producing cellshas differential levels of CpG methylation and histoneacetylation [68], where IL-4 is an important cytokine thatpromotes IgG and IgE class-switch recombination.
Recent data has suggested that changes in DNAhypersensitivity related to altered methylation patterns andhistone acetylation occur at the specific IL-10 locus duringT-cell differentiation into Th2 cells and in IL-10-producingTregs enabling optimal IL-10 gene expression, probablyresulting from epigenetic modification. Similar results werefound for other Th2 cytokines in human cells [69].
Conclusions
Nephrotic syndrome is a multifactorial disease and acomplex area of research that for decades has been anintriguing subject for clinicians and researchers, leading toa multitude of hypotheses trying to explain its occurrenceand childhood specificity.
These hypotheses include three probably interactingmechanisms implicated in the occurrence of the disease:(a) deregulation mechanisms of genes implicated in thematuration and differentiation process of lymphocytes,especially T-cells in patients presenting a steroid sensitivenephrotic syndrome, (b) abnormalities of podocyte proteinsleading to cytoskeleton modifications, and (c) probableimpact of DNA epigenome modifications in infected cellsafter viral infection. The field of epigenetics and the recentadvances in genome-wide association studies should opennew possible perspectives in identifying the physiopatho-logical mechanisms of the disease.
Conflict of interest The authors have no conflicts of interest.
References
1. Niaudet P (2004) Genetic forms of nephrotic syndrome. PediatrNephrol 19:1313–1318
2. Habib R, Kleinknecht C (1971) The primary nephrotic syndromeof childhood. Classification and clinicopathologic study of 406cases. Pathol Annu 6:417–474
3. International Study of Kidney Disease In Children (1978)Nephrotic syndrome in children: prediction of histopathologyfrom clinical and laboratory characteristics at time of diagnosis.Kidney Int 13:159–165
1254 Pediatr Nephrol (2012) 27:1249–1256

4. Arbeitsgemeinschaft für Pädiatrische Nephrologie (1988) Shortversus standard prednisone therapy for initial treatment ofidiopathic nephrotic syndrome in children. Lancet 1:380–383
5. Hodson EM, Alexander SI (2008) Evaluation and management ofsteroid-sensitive nephrotic syndrome. Curr Opin Pediatr 20:145–150
6. McKinney PA, Feltbower RG, Brocklebank JT, Fitzpatrick MM(2001) Time trends and ethnic patterns of childhood nephroticsyndrome in Yorkshire, UK. Pediatr Nephrol 16:1040–1044
7. Schlesinger ER, Sultz HA, Mosher WE, Feldman JG (1968) Thenephrotic syndrome. Its incidence and implications for thecommunity. Am J Dis Child 116:623–632
8. Trompeter RS, Lloyd BW, Hicks J, White RH, Cameron JS (1985)Long-term outcome for children with minimal-change nephroticsyndrome. Lancet 1:368–370
9. Sahali D, Pawlak A, Le Gouvello S, Lang P, Valanciuté A, RemyP, Loirat C, Niaudet P, Bensman A, Guellaen G (2001)Transcriptional and post-transcriptional alterations of IkappaBalphain active minimal-change nephrotic syndrome. J Am Soc Nephrol12:1648–1658
10. Araya C, Diaz L, Wasserfall C, Atkinson M, Mu W, Johnson R,Garin E (2009) T regulatory cell function in idiopathic minimallesion nephrotic syndrome. Pediatr Nephrol 24:1691–1698
11. Weaver ICG (2009) Epigenetic effects of glucocorticoids. SeminFetal Neonatal Med 14:143–150
12. Barnes PJ (2010) Mechanisms and resistance in glucocorticoidcontrol of inflammation. J Steroid Biochem Mol Biol 120:76–85
13. Adcock IM (2000) Molecular mechanisms of glucocorticosteroidactions. Pulm Pharmacol Ther 13:115–126
14. Shalhoub RJ (1974) Pathogenesis of lipoid nephrosis: a disorderof T-cell function. Lancet 2:556–560
15. Ulinski T, Aoun B (2010) Pediatric idiopathic nephrotic syn-drome: treatment strategies in steroid-dependent and steroid-resistant forms. Curr Med Chem 17:847–853
16. Sellier-Leclerc A, Macher M, Loirat C, Guérin V, Watier H,Peuchmaur M, Baudouin V, Deschênes G (2010) Rituximabefficiency in children with steroid-dependent nephrotic syndrome.Pediatr Nephrol 25:1109–1115
17. Yap HK, Han EJ, Heng CK, GongWK (2001) Risk factors for steroiddependency in children with idiopathic nephrotic syndrome.Pediatr Nephrol 16:1049–1052
18. Mansour H, Cheval L, Elalouf J, Aude J, Alyanakian M,Mougenot B, Doucet A, Deschênes G (2005) T-cell transcriptomeanalysis points up a thymic disorder in idiopathic nephroticsyndrome. Kidney Int 67:2168–2177
19. Audard V, Larousserie F, Grimbert P, Abtahi M, Sotto J, Delmer A,Boue F, Nochy D, Brousse N, Delarue R, Remy P, Ronco P, SahaliD, Lang P, Hermine O (2006) Minimal change nephroticsyndrome and classical Hodgkin's lymphoma: report of 21 casesand review of the literature. Kidney Int 69:2251–2260
20. Audard V, Zhang S, Copie-Bergman C, Rucker-Martin C, Ory V,Candelier M, Baia M, Lang P, Pawlak A, Sahali D (2010)Occurrence of minimal change nephrotic syndrome in classicalHodgkin lymphoma is closely related to the induction of c-mip inHodgkin-Reed Sternberg cells and podocytes. Blood 115:3756–3762
21. Grimbert P, Valanciute A, Audard V, Pawlak A, Le Gouvelo S,Lang P, Niaudet P, Bensman A, Guellaën G, Sahali D (2003)Truncation of C-mip (Tc-mip), a new proximal signaling protein,induces c-maf Th2 transcription factor and cytoskeleton reorgani-zation. J Exp Med 198:797–807
22. Yap HK, Cheung W, Murugasu B, Sim SK, Seah CC, Jordan SC(1999) Th1 and Th2 cytokine mRNA profiles in childhoodnephrotic syndrome: evidence for increased IL-13 mRNA expressionin relapse. J Am Soc Nephrol 10:529–537
23. Grimbert P, Audard V, Valanciute A, Pawlak A, Lang P, GuellaënG, Sahali D (2005) Abnormal RNA processing and altered
expression of serin-rich proteins in minimal-change nephroticsyndrome. Pediatr Res 57:133–137
24. Sellier-Leclerc A, Duval A, Riveron S, Macher M, Deschenes G,Loirat C, Verpont M, Peuchmaur M, Ronco P, Monteiro RC,Haddad E (2007) A humanized mouse model of idiopathicnephrotic syndrome suggests a pathogenic role for immaturecells. J Am Soc Nephrol 18:2732–2739
25. Lapillonne H, Leclerc A, Ulinski T, Balu L, Garnier A,Dereuddre-Bosquet N, Watier H, Schlageter M, Deschênes G(2008) Stem cell mobilization in idiopathic steroid-sensitivenephrotic syndrome. Pediatr Nephrol 23:1251–1256
26. Nagafuchi S, Katsuta H, Koyanagi-Katsuta R, Yamasaki S, InoueY, Shimoda K, Ikeda Y, Shindo M, Yoshida E, Matsuo T, Ohno Y,Kogawa K, Anzai K, Kurisaki H, Kudoh J, Harada M, Shimizu N(2006) Autoimmune regulator (AIRE) gene is expressed in humanactivated CD4+ T-cells and regulated by mitogen-activated proteinkinase pathway. Microbiol Immunol 50:979–987
27. Gavanescu I, Kessler B, Ploegh H, Benoist C, Mathis D (2007)Loss of Aire-dependent thymic expression of a peripheral tissueantigen renders it a target of autoimmunity. Proc Natl Acad SciUSA 104:4583–4587
28. Long E, Wood KJ (2007) Understanding FOXP3: progresstowards achieving transplantation tolerance. Transplantation84:459–461
29. Shao XS, Yang XQ, Zhao XD, Li Q, Xie YY, Wang XG, Wang M,Zhang W (2009) The prevalence of Th17 cells and FOXP3regulate T cells (Treg) in children with primary nephroticsyndrome. Pediatr Nephrol 24:1683–1690
30. Deschênes G, Doucet A (2009) Free immunoglobulin light chains:a role in minimal change disease. Biosci Hypotheses 2:135–142
31. Garin EH (2000) Circulating mediators of proteinuria in idiopathicminimal lesion nephrotic syndrome. Pediatr Nephrol 14:872–878
32. Hoyer JR, Vernier RL, Najarian JS, Raij L, Simmons RL, MichaelAF (2001) Recurrence of idiopathic nephrotic syndrome afterrenal transplantation. J Am Soc Nephrol 12:1994–2002
33. Cochat P, Kassir A, Colon S, Glastre C, Tourniaire B, Parchoux B,Martin X, David L (1993) Recurrent nephrotic syndrome aftertransplantation: early treatment with plasmaphaeresis and cyclo-phosphamide. Pediatr Nephrol 7:50–54
34. Koyama A, Fujisaki M, Kobayashi M, Igarashi M, Narita M(1991) A glomerular permeability factor produced by human Tcell hybridomas. Kidney Int 40:453–460
35. Ikeuchi Y, Kobayashi Y, Arakawa H, Suzuki M, Tamra K,Morikawa A (2009) Polymorphisms in interleukin-4-related genesin patients with minimal change nephrotic syndrome. PediatrNephrol 24:489–495
36. Vanden Berghe W, Ndlovu N, Hoya-Arias R, Dijsselbloem N, GerloS, Haegeman G (2006) Keeping up NF-[kappa]B appearances:epigenetic control of immunity or inflammation-triggered epige-netics. Biochem Pharmacol 72:1114–1131
37. Alt FW, Rathbun G, Oltz E, Taccioli G, Shinkai Y (1992) Functionand control of recombination-activating gene activity. Ann NYAcad Sci 651:277–294
38. Corneo B, Moshous D, Güngör T, Wulffraat N, Philippet P, LeDeist FL, Fischer A, de Villartay JP (2001) Identical mutations inRAG1 or RAG2 genes leading to defective V(D)J recombinaseactivity can cause either T-B-severe combined immune deficiencyor Omenn syndrome. Blood 97:2772–2776
39. de Villartay J, Lim A, Al-Mousa H, Dupont S, Déchanet-Merville J, Coumau-Gatbois E, Gougeon M, Lemainque A,Eidenschenk C, Jouanguy E, Abel L, Casanova J, Fischer A, LeDeist F (2005) A novel immunodeficiency associated withhypomorphic RAG1 mutations and CMV infection. J Clin Invest115:3291–3299
40. Klein U, Casola S, Cattoretti G, Shen Q, Lia M, Mo T, Ludwig T,Rajewsky K, Dalla-Favera R (2006) Transcription factor IRF4
Pediatr Nephrol (2012) 27:1249–1256 1255

controls plasma cell differentiation and class-switch recombination.Nat Immunol 7:773–782
41. Lee GR, Fields PE, Flavell RA (2001) Regulation of IL-4 geneexpression by distal regulatory elements and GATA-3 at thechromatin level. Immunity 14:447–459
42. Barnes PJ, Adcock IM (2009) Glucocorticoid resistance ininflammatory diseases. Lancet 373:1905–1917
43. Zheng Y, Chaudhry A, Kas A, deRoos P, Kim JM, Chu T,Corcoran L, Treuting P, Klein U, Rudensky AY (2009) RegulatoryT-cell suppressor program co-opts transcription factor IRF4 tocontrol T(H)2 responses. Nature 458:351–356
44. Ransom RF, Lam NG, Hallett MA, Atkinson SJ, Smoyer WE (2005)Glucocorticoids protect and enhance recovery of cultured murinepodocytes via actin filament stabilization. Kidney Int 68:2473–2483
45. Schönenberger E, Ehrich JH, Haller H, Schiffer M (2011) Thepodocyte as a direct target of immunosuppressive agents. NephrolDial Transplant 26:18–24
46. Wada T, Pippin JW, Marshall CB, Griffin SV, Shankland SJ (2005)Dexamethasone prevents podocyte apoptosis induced by puromy-cin aminonucleoside: role of p53 and Bcl-2-related familyproteins. J Am Soc Nephrol 16:2615–2625
47. Faul C, Donnelly M, Merscher-Gomez S, Chang YH, Franz S,Delfgaauw J, Chang J, Choi HY, Campbell KN, Kim K, Reiser J,Mundel P (2008) The actin cytoskeleton of kidney podocytes is adirect target of the antiproteinuric effect of cyclosporine A. NatMed 14:931–938
48. Mundel P, Reiser J (2010) Proteinuria: an enzymatic disease of thepodocyte? Kidney Int 77:571–580
49. Shimada M, Araya C, Rivard C, Ishimoto T, Johnson RJ, GarinEH (2011) Minimal change disease: a “two-hit” podocyte immunedisorder? Pediatr Nephrol 26:645–649
50. Zhang S, Kamal M, Dahan K, Pawlak A, Ory V, Desvaux D, AudardV, Candelier M, BenMohamed F, Mohamed FB, Matignon M,Christov C, Decrouy X, Bernard V, Mangiapan G, Lang P, GuellaënG, Ronco P, Sahali D (2010) c-mip impairs podocyte proximalsignaling and induces heavy proteinuria. Sci Signal 3:ra39
51. Kamal M, Pawlak A, BenMohamed F, Valanciuté A, Dahan K,Candelier M, Lang P, Guellaën G, Sahali D (2010) C-mip interactswith the p85 subunit of PI3 kinase and exerts a dual effect onERK signaling via the recruitment of Dip1 and DAP kinase.FEBS Lett 584:500–506
52. Clement LC, Avila-Casado C, Macé C, Soria E, Bakker WW, KerstenS, Chugh SS (2011) Podocyte-secreted angiopoietin-like-4 mediatesproteinuria in glucocorticoid-sensitive nephrotic syndrome. Nat Med17:117–122
53. Okamoto K, Tokunaga K, Doi K, Fujita T, Suzuki H, Katoh T,Watanabe T, Nishida N, Mabuchi A, Takahashi A, Kubo M,
Maeda S, Nakamura Y, Noiri E (2011) Common variation inGPC5 is associated with acquired nephrotic syndrome. Nat Genet43:459–463
54. Feinberg AP, Ohlsson R, Henikoff S (2006) The epigeneticprogenitor origin of human cancer. Nat Rev Genet 7:21–33
55. EstellerM (2008) Epigenetics in cancer. N Engl JMed 358:1148–115956. Wong AHC, Gottesman II, Petronis A (2005) Phenotypic differences
in genetically identical organisms: the epigenetic perspective. HumMol Genet 14 Spec No 1:R11–R18
57. Feinberg AP (2007) Phenotypic plasticity and the epigenetics ofhuman disease. Nature 447:433–440
58. Li E (2002) Chromatin modification and epigenetic reprogrammingin mammalian development. Nat Rev Genet 3:662–673
59. Rodenhiser D, Mann M (2006) Epigenetics and human disease:translating basic biology into clinical applications. CMAJ 174:341–348
60. Fraga MF, Ballestar E, Paz MF, Ropero S, Setien F, Ballestar ML,Heine-Suñer D, Cigudosa JC, Urioste M, Benitez J, Boix-ChornetM, Sanchez-Aguilera A, Ling C, Carlsson E, Poulsen P, Vaag A,Stephan Z, Spector TD, Wu Y, Plass C, Esteller M (2005)Epigenetic differences arise during the lifetime of monozygotictwins. Proc Natl Acad Sci USA 102:10604–10609
61. Szyf M, Weaver ICG, Champagne FA, Diorio J, Meaney MJ(2005) Maternal programming of steroid receptor expression andphenotype through DNA methylation in the rat. Front Neuro-endocrinol 26:139–162
62. Migeon BR (2008) X inactivation, female mosaicism, and sexdifferences in renal diseases. J Am Soc Nephrol 19:2052–2059
63. Dwivedi RS, Herman JG, McCaffrey TA, Raj DSC (2011) Beyondgenetics: epigenetic code in chronic kidney disease. Kidney Int79:23–32
64. Barnes PJ (2009) Targeting the epigenome in the treatment ofasthma and chronic obstructive pulmonary disease. Proc AmThorac Soc 6:693–696
65. MacDonald NE, Wolfish N, McLaine P, Phipps P, Rossier E (1986)Role of respiratory viruses in exacerbations of primary nephroticsyndrome. J Pediatr 108:378–382
66. Stram Y, Kuzntzova L (2006) Inhibition of viruses by RNAinterference. Virus Genes 32:299–306
67. Maekawa M, Watanabe Y (2007) Epigenetics: relations to diseaseand laboratory findings. Curr Med Chem 14:2642–2653
68. Guo L, Hu-Li J, Zhu J, Watson CJ, Difilippantonio MJ, PannetierC, Paul WE (2002) In TH2 cells the Il4 gene has a series ofaccessibility states associated with distinctive probabilities of IL-4production. Proc Natl Acad Sci USA 99:10623–10628
69. Adcock IM, Tsaprouni L, Bhavsar P, Ito K (2007) Epigeneticregulation of airway inflammation. Curr Opin Immunol 19:694–700
1256 Pediatr Nephrol (2012) 27:1249–1256