
Pattern and implication of lymphatic drainage in renal tumors 4.7/14… · Interaortocaval 42 %...
19
Pattern and implication of lymphatic drainage in renal tumors Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU Tel Aviv, July 4, 2018
Transcript of Pattern and implication of lymphatic drainage in renal tumors 4.7/14… · Interaortocaval 42 %...

Pattern and implication of lymphatic
drainage in renal tumors Axel Bex, MD, PhD
The Netherlands Cancer Institute
FOIU Tel Aviv,
July 4, 2018

Financial and Other Disclosures Off-label use of drugs, devices, or other agents: None or FILL IN HERE; including your
local regulatory agency, such as FDA, EMA, etc.
Data from IRB-approved human research is presented [or state: “is not”]
2
I have the following financial interests or
relationships to disclose: Disclosure code
Pfizer C, S
Roche C
Genentech C
Ipsen C
Novartis C
BMS C


Recommendations from EAU guidelines on
RCC – updated 2014
• For T1 RCCs, nephron-sparing surgery should be performed whenever possible.
Open partial nephrectomy currently remains the standard. A
• Laparoscopic radical nephrectomy is recommended in T2 renal cell cancer when nephron-
sparing surgery is not suitable B
• Extended lymphadenectomy does not improve survival and can be restricted to staging purposes. A
• Adrenalectomy is generally not recommended except when a normal adrenal gland cannot be excluded
by imaging and palpation. B
• Patients with small tumours and/or significant comorbidity who are unfit for surgery should be considered
for an ablative approach
(eg, cryotherapy and radiofrequency ablation). A
EAU Guidelines on RCC – 2014 update, Ljungberg et al, Eur Urol 67:913-24, 2015
• For T1 RCCs, nephron-sparing surgery should be performed whenever possible.
Open partial nephrectomy currently remains the standard. A
• Laparoscopic radical nephrectomy is recommended in T2 renal cell cancer when nephron-
sparing surgery is not suitable B
• Extended lymphadenectomy does not improve survival and can be restricted to staging purposes. A
• Adrenalectomy is generally not recommended except when a normal adrenal gland cannot be excluded
by imaging and palpation. B
• Patients with small tumours and/or significant comorbidity who are unfit for surgery should be considered
for an ablative approach
(eg, cryotherapy and radiofrequency ablation). A
But……..
• The patient who can potentially be
cured by LND has very early lymph
node metastasis and no systemic
disease
Canfield et al., J Urol 175:864-869, 2006

Capitanio et al., BJU Int 112: E59-66, 2013
• 1983 patients with cT any cNany cMany
• Prevalence of nodal metastases 6.1 %
• Accuracy 86.9 %
Preoperative nomogram to predict nodal metastases

Is there a template for lymph node
dissection in RCC ?
Hadley et al, Urologic Oncology 2009
N=31 patients with N+ >1 cm
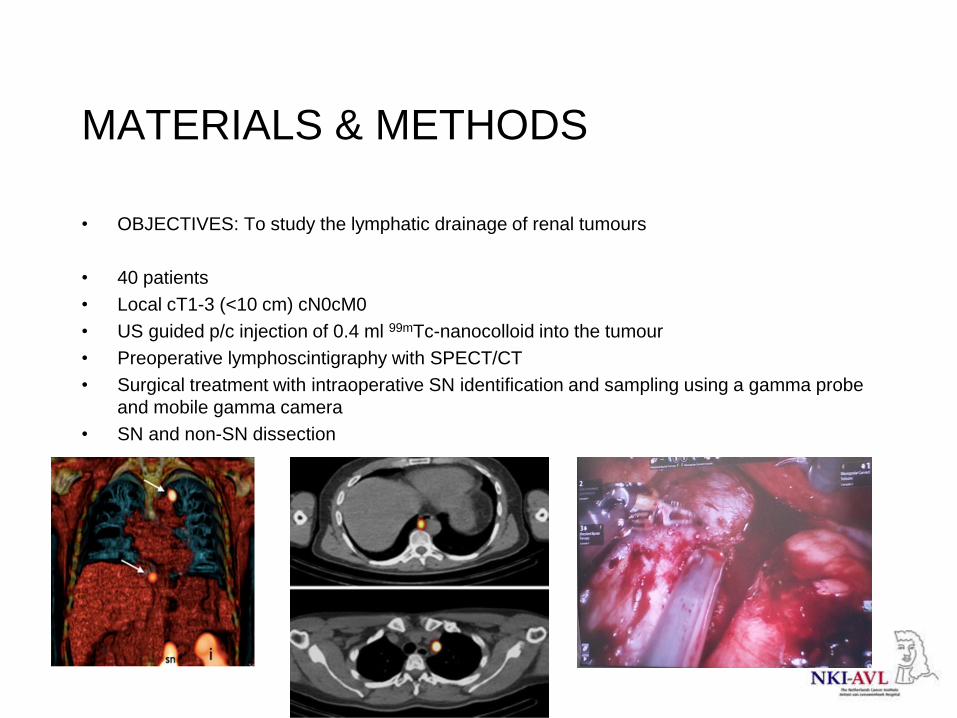
MATERIALS & METHODS
• OBJECTIVES: To study the lymphatic drainage of renal tumours
• 40 patients
• Local cT1-3 (<10 cm) cN0cM0
• US guided p/c injection of 0.4 ml 99mTc-nanocolloid into the tumour
• Preoperative lymphoscintigraphy with SPECT/CT
• Surgical treatment with intraoperative SN identification and sampling using a gamma probe
and mobile gamma camera
• SN and non-SN dissection

Contralateral paraaortic SN location
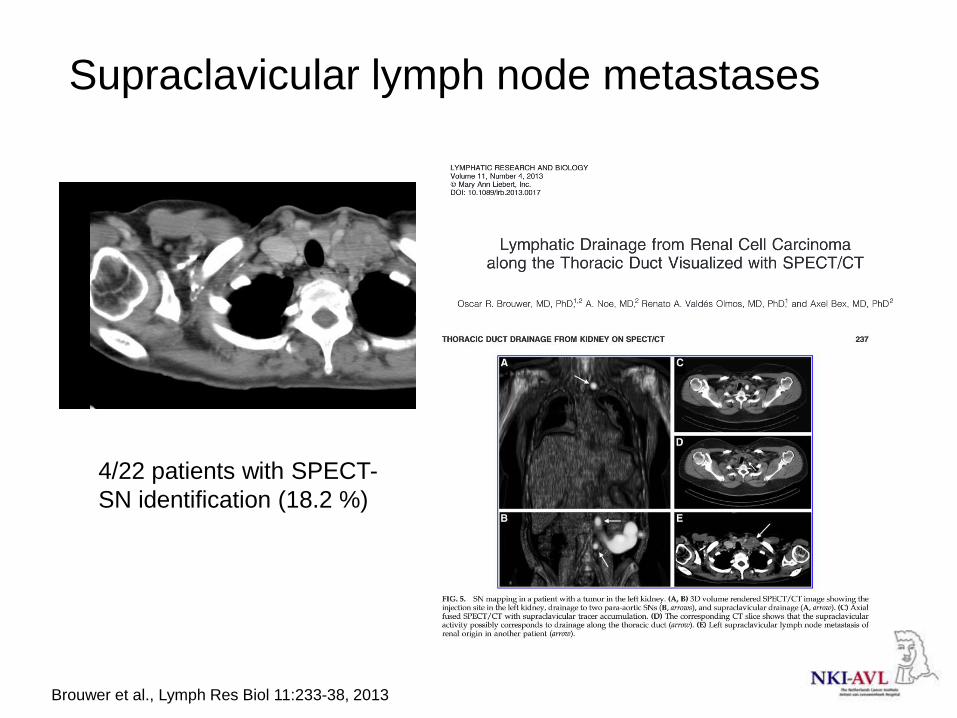
Supraclavicular lymph node metastases
4/22 patients with SPECT-
SN identification (18.2 %)
Brouwer et al., Lymph Res Biol 11:233-38, 2013

65% inside
LND
templates
35%
outside
from which
20% in
thoracic
area
Kuusk et al., J Urol 2018

Parker was the first to describe connections
to the thoracic duct
Parker 1935

1969 - A lymphographic and
histopathological investigation in RCC
• N=22 patients undergoing nephrectomy
• 7 (32 %) metastasis in lumbar and
ipsilateral iliac nodes
• 1 supraclavicular node
• Poor correlation of lymphography with
nodal metastasis but contrast filling of
mediastinal nodes observed
Hulten et al., Scand J Urol Nephrol 3:129-33, 1969


5 of 13 right side, 3 of 13 left side
Assouad et al., Lymphology 39:26-32, 2006
Direct drainage into the thoracic duct without
intervening lymph nodes

Distribution of lymph node metastases –
an autopsy study
• n= 1001 patients with metastatic RCC
Location %
neck + clavicle 20.7 %
mediastinum 10.3 %
hilus of lungs 66.2 %
hilus of kidney 7 %
paraaortal 26.8 %
retroperitoneal 36 %
mesenterial 14.4 %
Saitoh et al. J Urol 1982

Distribution of lymph node metastasis
• Imaging study on 28 patients with cN1 identified from
101 with RCC
Location Percentage (left/right
combined
Distant lymphadenopathy
without hilar
lymphadenopathy
29 %
Interaortocaval 42 %
retroaortocaval 46 %
suprahilar 30 %
Hadley et al. Urol Oncol 2009

Paraaortic TD subclavian vein lung mediastinal nodes
Brouwer et al, Assoud et al

Implications
• The pattern of lymphatic spread in RCC
is very unpredictable
• The true rate of single early occult LN
metastasis is unknown but seems low
• The sentinel node concept should be
studied in clinically high-risk cN0
patients or used for translational
research purposes


















