Opioid Analgesics - cmaav.mx · OPIOID ANALGESICS Peter J. Pascoe, BVSc Opioid analgesics have...
16
MANAGEMENT OF PAIN 0195-5616/00 $15.00 + .OO OPIOID ANALGESICS Peter J. Pascoe, BVSc Opioid analgesics have provided the most consistent and effective analgesia for many years and are still the best drugs available for pain control in small animals. There are at least three different opiate receptors, and they each have different roles to play in the activities of the nervous system. Although the receptors are generally classified as mu, kappa, and delta, it is becoming obvious that there are several subtypes of each of these receptors and that the expression of these receptors varies according to the location of the tissue. The mu receptors have been divided into mu-1, mu-2, and mu-3, but recent molecular biology techniques suggest that there may be at least seven subtypes of this receptor. These receptors are distributed throughout the body; thus, drugs acting at these receptors are likely to have effects on many different organs and systems. The drugs we use have different affinities for these receptors, and t h s explains some of the differences between the available drugs. Drugs such as morphine, oxymorphone, fentanyl, hydromorphone, and meperidine are opioid agonists and act mainly at the mu receptors, where they have a high affinity.The agonist- antagonists (butorphanol, nalbuphine, buprenorphine, pentazocine) are able to reverse some of the effects of the pure agonists but are still capable of producing analgesia by themselves. The receptor activity of these drugs is varied; for example, butorphanol seems to act at the kappa receptors and as a mu antago- nist, whereas buprenorphine is a kappa antagonist but has high affinity for mu receptors, although it only has moderate receptor activity and is classified as a partial agonist. It should be recognized that these drugs do tend to antagonize the pure agonists, and care must be taken not to mix these two classes of opioids unless reversal of the agonist is intended. The antagonists include naloxone, naltrexone, and nalmefene. These drugs reverse the actions of both mu and kappa agonists, although their activity is more potent at the mu receptor. The opioids can be used by systemic administration or can be applied more directly to the tissues or the spinal receptors by injecting the drug epidurally or intrathe- cally. From the Department of Surgical and Radiological Sciences, School of Veterinary Medicine, University of California, Davis, California VETERINARY CLINICS OF NORTH AMERICA: SMALL ANIMAL PRACTICE VOLUME 30 * NUMBER 4 - JULY 2000 757
Transcript of Opioid Analgesics - cmaav.mx · OPIOID ANALGESICS Peter J. Pascoe, BVSc Opioid analgesics have...
MANAGEMENT OF PAIN 0195-5616/00 $15.00 + .OO
OPIOID ANALGESICS
Peter J. Pascoe, BVSc
Opioid analgesics have provided the most consistent and effective analgesia for many years and are still the best drugs available for pain control in small animals. There are at least three different opiate receptors, and they each have different roles to play in the activities of the nervous system. Although the receptors are generally classified as mu, kappa, and delta, it is becoming obvious that there are several subtypes of each of these receptors and that the expression of these receptors varies according to the location of the tissue. The mu receptors have been divided into mu-1, mu-2, and mu-3, but recent molecular biology techniques suggest that there may be at least seven subtypes of this receptor. These receptors are distributed throughout the body; thus, drugs acting at these receptors are likely to have effects on many different organs and systems. The drugs we use have different affinities for these receptors, and th s explains some of the differences between the available drugs. Drugs such as morphine, oxymorphone, fentanyl, hydromorphone, and meperidine are opioid agonists and act mainly at the mu receptors, where they have a high affinity. The agonist- antagonists (butorphanol, nalbuphine, buprenorphine, pentazocine) are able to reverse some of the effects of the pure agonists but are still capable of producing analgesia by themselves. The receptor activity of these drugs is varied; for example, butorphanol seems to act at the kappa receptors and as a mu antago- nist, whereas buprenorphine is a kappa antagonist but has high affinity for mu receptors, although it only has moderate receptor activity and is classified as a partial agonist. It should be recognized that these drugs do tend to antagonize the pure agonists, and care must be taken not to mix these two classes of opioids unless reversal of the agonist is intended. The antagonists include naloxone, naltrexone, and nalmefene. These drugs reverse the actions of both mu and kappa agonists, although their activity is more potent at the mu receptor. The opioids can be used by systemic administration or can be applied more directly to the tissues or the spinal receptors by injecting the drug epidurally or intrathe- cally.
From the Department of Surgical and Radiological Sciences, School of Veterinary Medicine, University of California, Davis, California
VETERINARY CLINICS OF NORTH AMERICA: SMALL ANIMAL PRACTICE
VOLUME 30 * NUMBER 4 - JULY 2000 757
758 PASCOE
SYSTEMIC INJECTION
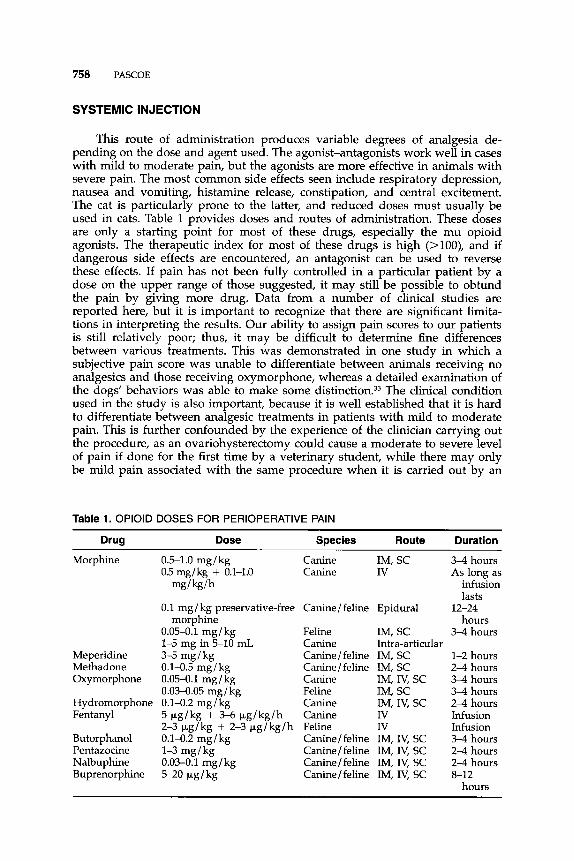
This route of administration produces variable degrees of analgesia de- pending on the dose and agent used. The agonist-antagonists work well in cases with mild to moderate pain, but the agonists are more effective in animals with severe pain. The most common side effects seen include respiratory depression, nausea and vomiting, histamine release, constipation, and central excitement. The cat is particularly prone to the latter, and reduced doses must usually be used in cats. Table 1 provides doses and routes of administration. These doses are only a starting point for most of these drugs, especially the mu opioid agonists. The therapeutic index for most of these drugs is high (>loo), and if dangerous side effects are encountered, an antagonist can be used to reverse these effects. If pain has not been fully controlled in a particular patient by a dose on the upper range of those suggested, it may still be possible to obtund the pain by giving more drug. Data from a number of clinical studies are reported here, but it is important to recognize that there are significant limita- tions in interpreting the results. Our ability to assign pain scores to our patients is still relatively poor; thus, it may be difficult to determine fine differences between various treatments. This was demonstrated in one study in which a subjective pain score was unable to differentiate between animals receiving no analgesics and those receiving oxymorphone, whereas a detailed examination of the dogs' behaviors was able to make some di~tinction.3~ The clinical condition used in the study is also important, because it is well established that it is hard to differentiate between analgesic treatments in patients with mild to moderate pain. T h s is further confounded by the experience of the clinician carrying out the procedure, as an ovariohysterectomy could cause a moderate to severe level of pain if done for the first time by a veterinary student, while there may only be mild pain associated with the same procedure when it is carried out by an
Table 1. OPlOlD DOSES FOR PERIOPERATIVE PAIN
Drug Dose Species Route Duration
Morphine
Meperidine Methadone Oxymorphone
Hydromorphone Fentanyl
Butorphanol Pentazocine Nalbuphine Buprenorphine
0.5-1.0 mg/kg Canine IM, SC 0.5 mg/kg + 0.1-1.0 Canine Iv
mg/kg/h
morphine 0.1 mg/ kg preservative-free Canine/feline Epidural
0.054.1 mg/kg Feline IM, sc 1-5 mg in5-10 mL Canine Intra-articular 3-5 mg / kg Canine/feline IM, SC 0.14.5 mg/kg Canine/feline IM, SC 0.05-0.1 mg/kg Canine IM, N, SC 0.034.05 mg/kg Feline IM, SC 0.1-0.2 mg/kg Canine IM, IV, SC 5 pg/kg + 3 4 bg/kg/h Canine Iv 2-3 pg / kg + 2-3 pg / kg / h Feline Iv 0.14.2 mg/kg Canine/feline IM, Iv, SC 1-3 mg/kg Canine/feline IM, Iv, SC 0.03-0.1 mg/kg Canine / feline IM, IV, SC 5-20 pg/kg Canine/feline IM, IV, SC
3-4 hours As long as
infusion lasts
hours 3 4 hours
1-2 hours 2 4 hours 3 4 hours 3-4 hours 2 4 hours Infusion Infusion 3-4 hours 2 4 hours 2-4 hours
hours
12-24
8-12
OPIOID ANALGESICS 759
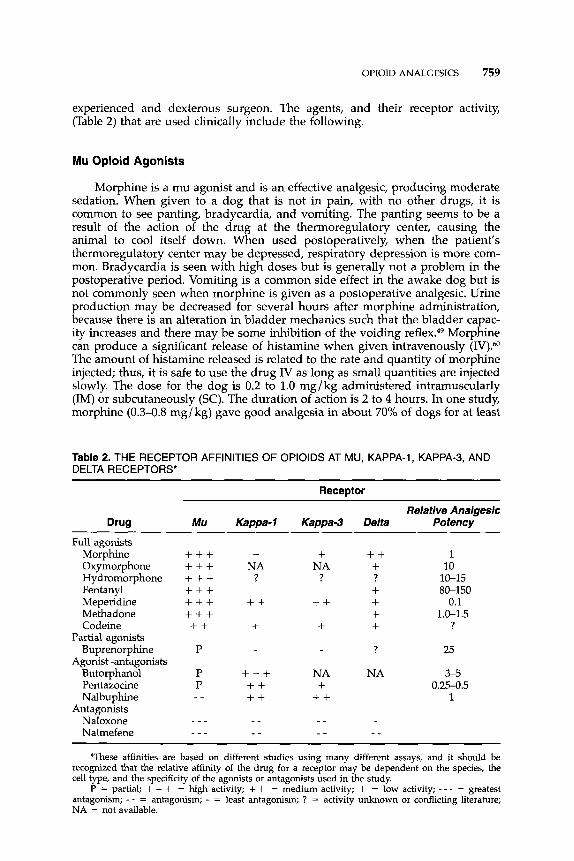
experienced and dexterous surgeon. The agents, and their receptor activity, (Table 2) that are used clinically include the following.
Mu Opioid Agonists
Morphine is a mu agonist and is an effective analgesic, producing moderate sedation. When given to a dog that is not in pain, with no other drugs, it is common to see panting, bradycardia, and vomiting. The panting seems to be a result of the action of the drug at the thermoregulatory center, causing the animal to cool itself down. When used postoperatively, when the patient’s thermoregulatory center may be depressed, respiratory depression is more com- mon. Bradycardia is seen with high doses but is generally not a problem in the postoperative period. Vomiting is a common side effect in the awake dog but is not commonly seen when morphine is given as a postoperative analgesic. Urine production may be decreased for several hours after morphine administration, because there is an alteration in bladder mechanics such that the bladder capac- ity increases and there may be some inhibition of the voiding Morphine can produce a significant release of histamine when given intravenously (IV)?O The amount of histamine released is related to the rate and quantity of morphme injected; thus, it is safe to use the drug IV as long as small quantities are injected slowly. The dose for the dog is 0.2 to 1.0 mg/kg administered intramuscularly (IM) or subcutaneously (SC). The duration of action is 2 to 4 hours. In one study, morphine (0.3-0.8 mg/kg) gave good analgesia in about 70% of dogs for at least
Table 2. THE RECEPTOR AFFINITIES OF OPlOlDS AT MU, KAPPA-I, KAPPA-3, AND DELTA RECEPTORS*
Receptor
Relative Analgesic Drug Mu Kappa-1 Kappa-3 Delta Potency
Full agonists Morphine Oxymorphone Hydromorphone Fentanyl Meperidine Methadone Codeine
Partial agonists Buprenorphine
Agonist-antagonists Butorphanol Pentazocine Nalbuphine
Antagonists Naloxone Nalmefene
+ + + + + + + + + + + + + + + + + + + + P
P P
_ _
- - _ - - _
+ NA
?
+ + +
+ + + + + + + _ - - -
+ NA
?
+ + +
NA +
+ + _ _ _ -
+ + + ? + + + + ?
NA
- -
1 10
10-15 80-150
0.1 1.0-1.5
?
25
3-5 0.25-0.5
1
These affinities are based on different studies using many different assays, and it should be recognized that the relative affinity of the drug for a receptor may be dependent on the species, the cell type, and the specificity of the agonists or antagonists used in the study.
P = partial; + + + = high activity; + + = medium activity; + = low activity; - - - = greatest antagonism; - - = antagonism; - = least antagonism; ? = activity unknown or conflicting literature; NA = not available.
760 PASCOE
4 hours after a variety of orthopedic surgeries." In another study in dogs, it gave adequate analgesia (0.3 mg/ kg IM) in most cases over a 7-hour assessment period after arthrotomy.l0 At 0.15 mg/kg N, morphine gave less than 4 hours of analgesia in six dogs after left lateral thoracotomy, and five of the six dogs had received additional doses of morphine by this time.59 Morphine has also been used as a continuous IV infusion in dogs at a rate of 0.1 to 1.0 mg/kg/h (I have generally found 0.2 mg/kg/h to be effective) after a 0.3 to 0.5 mg/kg dose IM or IV. Cats can be given 0.05 to 0.1 mg/kg IM or SC, and it should not be given IV unless it is diluted and given slowly.
Meperidine is less potent than morphine, and it produces less sedation but has similar side effects. Panting is rare after administration of meperidine, but this drug is even more likely to cause histamine release and should not be used IV. It has a short duration of action and provides 0.5 to 2.0 hours of pain relief. This can be an advantage when it is necessary to reassess the degree of pain within a short period so as to understand the progression of a condition (eg , abdominal pain), but it limits the drug's potential as a long-term analgesic. In one clinical trial, approximately 70% of the dogs had no analgesia at 90 minutes after receiving meperidine (3.5 mg/kg) just before or just after the end of anesthesia.m In another study, the dogs receiving meperidine (5 mg/kg IM) at the end of surgery had lower pain scores than the controls at 1 hour but not at 2 hours.45 In this study, the dogs receiving the same treatment before the begin- ning of surgery had pain scores similar to those of the controls until 4 hours after the procedure (ovariohysterectomy). From 8 to 20 hours after the procedure, these dogs had lower scores, supporting the concept of preemptive analgesia." After ovariohysterectomy in cats, there seemed to be no difference in pain scores or further analgesic requirements between the meperidine (5 mg/kg IM) group and the control gr0up.6~ The dose in the dog and cat is 3 to 5 mg/kg IM or SC.
Oxymorphone (Numorphan) is approximately 10 times as potent as mor- phine, with a similar duration of action. When given at the end of an operation, a delay in recovery is expected, because oxymorphone does produce some sedation. Using this technique usually allows a smooth transition from anesthe- sia to recovery, however. Oxymorphone does not cause histamine release but may produce respiratory depression when given during anesthesia. It is rare for a dog to vomit or exhibit respiratory depression after oxymorphone administra- tion in the postoperative period. In a study comparing IM oxymorphone (0.2 mg/ kg) with epidural oxymorphone after left lateral thoracotomy, the dogs receiving IM oxymorphone had higher pain scores, heart rates, blood pressures, and respiratory rates at 1 hour, and by 4 hours, all 8 dogs had been treated with further doses of oxymorphone (IV) and withdrawn from the study, suggesting a 1- to 4-hour duration of action. In another study, the mean duration of analgesia after pelvic or hind limb orthopedic surgery (0.15 mg/kg IM) was 5 h 0 ~ r s . l ~ A study comparing various analgesics showed inadequate analgesia in 1 of 6 dogs after shoulder ar thr~tomy.~~ The duration of analgesia was at least 2 to 3 Pain scores were lower for dogs treated with oxymorphone (0.05 mg/kg IM) 1 hour after surgery in comparison with animals treated with butorphanol but the scores were similar thereafter. Conversely, 10 of 17 dogs treated with oxymorphone did not require further analgesics by 12 hours com- pared with 13 of 18 dogs treated with butorphanol.51 The dose of oxymorphone in the dog is 0.05 to 0.2 mg/kg IM or SC; in the cat, it is 0.03 to 0.05 mg/kg IM or SC. For severe to excruciating pain, an IV bolus titrated to effect is recom- mended, with a similar dose given over 1 to 2 hours as a constant-rate infusion. When titrating the drug, it should be remembered that it takes 6 to 8 minutes to reach peak effect. Intermittent boluses may be given for breakthrough pain.
OPIOID ANALGESICS 761
Methadone (Dolophine) is 1.0 to 1.5 times as potent as morphine and has similar analgesic properties. In people, it is used because of its greater duration of effect, but this has not been demonstrated in the dog and cat. Clinically, it seems to give good analgesia for moderate pain for at least 4 hours. Methadone does not cause histamine release and can be given IV if a more rapid onset is needed. One study reported an initial dose of methadone at 1 mg/ kg (N) given before the start of surgery followed by subsequent doses at 0.25 to 0.5 mg/kg. Profound analgesia lasted for 120 to 180 minutes.2l In cats, analgesia lasted from 1.5 to 6.5 hours after doses at 0.1 to 0.5 mg/kg?O The recommended dose range is 0.1 to 0.5 mg/kg IM or SC.
Hydromorphone (Dilaudid) is a mu agonist with a potency approximately five to seven times that of morphine. It induces a greater degree of sedation than oxymorphone and has a slightly shorter duration of action. It is not thought to release histamine when given IV. The dose range is 0.1 to 0.4 mg/ kg IV, IM, or SC in cats and dogs.
Fentanyl (Sublimaze) is a potent agonist with a relatively short duration of action. For this reason, it has not been used widely for the management of pain in the dog and cat. Because it has a relatively rapid onset of action (2-3 minutes), an IV bolus may be used to control severe pain (up to 20 pg/kg). It is also feasible to use it as an infusion to provide a continuous level of analgesia. Because respiratory depression with opioids can be profound, an animal on such an infusion should be monitored at all times. In dogs, an infusion could start with a 3- to 5-pg/kg bolus followed by an infusion of 3 to 6 pg/kg/h. In cats, about half of this is used as a bolus of 2 to 3 p,g/ kg with an infusion of 2 to 3 pg/ kg/h. Other congeners of fentanyl (sufentanil, alfentanil, and remifentanil) may be useful in this context, but they are currently quite expensive in North America.
Kappa Opioid Agonists-Mu Antagonists
Butorphanol (Torbugesic) is an agonist-antagonist, and its actions are slightly different than those of the other opioids. With increasing dosage, there is a ceiling effect on respiratory depression such that further increases in dose do not increase respiratory depression. Its potential as an addictive drug is much less than that of other opioids, and it is included as an antitussive in some human cough medicines. This drug causes mild sedation and seems to have a duration of activity of at least 2 hours or longer in some cases. Butorphanol has 7 to 10 times the receptor binding potency when compared with morphine but does not seem to be as effective an analgesic in cases with severe pain. Butorpha- no1 does not cause histamine release when injected IV. In an experimental study of analgesia in the cat, a dose of 0.1 mg/kg IV gave a longer duration of analgesia (at least 6 hours) than higher doses. When given SC, 0.8 mg/kg was required to produce the same duration and consistency of analgesia.63 This research demonstrates that there is a ceiling effect to the analgesia of this drug and that as the dose is increased, the antagonist properties may reverse some of the agonist activity. In another study, butorphanol (0.5 mg/kg) failed to give complete analgesia in 2 of 12 dogs at 15 minutes postoperatively, and it wore off by 90 minutes in dogs given the drug after anesthesia but had a longer duration of action if given during anesthesia (50% no analgesia at 90 minutes).78 In cats undergoing orthopedic surgery, 0.3 mg/kg IV gave less analgesia in the early postoperative period than ketoprofen (2 mg / kg IV).29 Dogs undergoing hind limb orthopedic surgery had higher pain scores at 1 hour when receiving
762 PASCOE
butorphanol than dogs receiving ketoprofen and oxymorphone or oxymorphone alone, but only 5 of 18 dogs received supplemental analgesics over the first 12 hours compared with 7 of 17 dogs receiving oxymorphone?6 A study comparing analgesic therapies showed inadequate analgesia with butorphanol (0.4 mg / kg IM) in 40% of the dogs after laparotomy and in 80% of the dogs after shoulder arthr~tomy.~~ The duration of analgesia was about 2 hours after laparotomy and less than 1 hour after shoulder surgeTy.S1 The dose in the dog is 0.1 to 0.4 mg/ kg IM, SC, or IV; it is 0.1 to 0.8 mg/kg IM, SC, or IV in the cat.
Pentazocine (Talwin) is another agonist-antagonist that is less potent than morphine and does not work well as a mu antagonist. It is considered to be a short-acting drug, but in one study, it had a similar duration of action to morphine (i.e., at least 4 h0urs),~3 whereas 1 of 12 dogs had no analgesia at 15 minutes postoperatively, and there was no analgesia by 180 minutes in another
The dose in the dog and cat is I to 3 mg/kg IM, SC, or IV. The higher dose (3 mg/kg) given IV to cats may produce marked ataxia, and the animals may seem to be apprehensive or frightened.
Nalbuphine (Nubain) is an agonist-antagonist. It is a kappa agonist and a mu antagonist. It is more potent as an antagonist than any of the other com- monly used mixed agonist-antagonist drugs. In postoperative analgesic trials in people, it was as effective as pentazocine or meperidine. This drug does not produce much sedation and has a minimal effect on respiration. As is the case with most of the opioids, it has a minimal effect on the cardiovascular system.& The dose in dogs and cats is 0.03 to 0.1 mg/kg IM, SC, or IV (W injections may be slightly painful). In cats, doses from 0.75 to 3.0 mg/kg were equally effective for visceral analgesia and produced no behavioral side effe~ts.6~
Partial Mu Opioid Agonist-Kappa Antagonist
Buprenorphine (Buprenex) is also an agonist-antagonist. It has strong affin- ity for mu receptors and also has kappa antagonist properties. It is a partial agonist, meaning that it does not induce the same degree of effect as a full agonist such as morphine. The association with mu receptors is slow in onset, and the peak effect of the drug does not occur until about 45 to 60 minutes after IV administration. The strong affinity for mu receptors means that it is hard to reverse the effects of buprenorphine. If naloxone is ineffective in reversing respiratory depression caused by buprenorphine, it is suggested that doxapram be used for temporary reversal. The dissociation from the mu receptors is also slow. The main advantage of this drug is that it has a potential 8- to 12-hour duration of action; however, in practice, its duration of action rarely exceeds 6 hours. Buprenorphine produces moderate sedation when used in the postopera- tive period. When given at 10 pg/kg in dogs 30 minutes before the end of anesthesia, it gave good analgesia at 15 minutes, but only half of the dogs were pain-free at 45 minutes, although some dogs still had some analgesia at 4
Of the drugs tested in that trial, it also induced the greatest sedation. In another study, buprenorphine (7-20 pg/kg) gave less analgesia than either morphine or pentazocine during the first 4 hours after orthopedic In cats given 6 p,g/kg, there were no differences in pain scores between the control group and the buprenorphine group during the 18-hour study period after ovariohy~terectomy.~~ Buprenorphine is only effective for treating mild to moder- ate pain. Increasing the dose significantly above that recommended may result in reduced analgesic effect, whch is difficult to treat with a pure opioid because of avid receptor blockade. The dose in the dog and cat is 5 to 20 kg/kg IM, SC,
OPIOID ANALGESICS 763
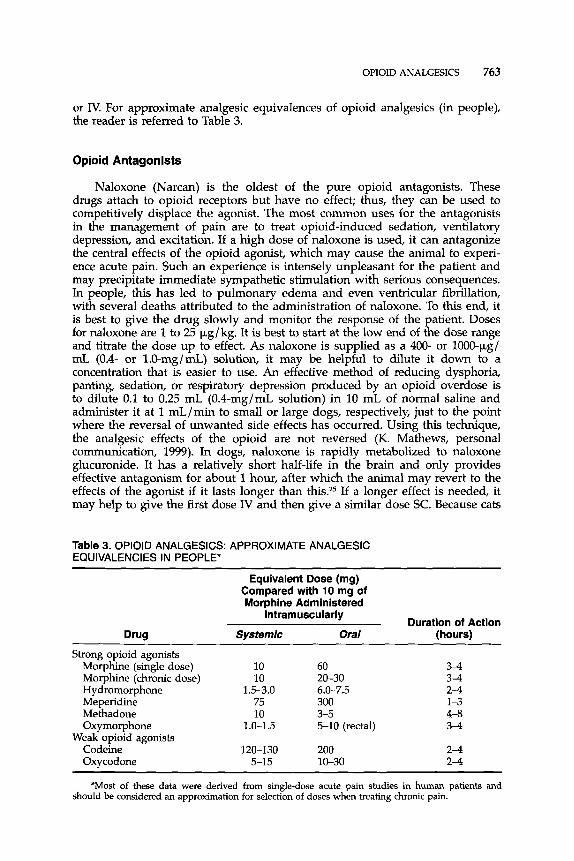
or Iv. For approximate analgesic equivalences of opioid analgesics (in people), the reader is referred to Table 3.
Opioid Antagonists
Naloxone (Narcan) is the oldest of the pure opioid antagonists. These drugs attach to opioid receptors but have no effect; thus, they can be used to competitively displace the agonist. The most common uses for the antagonists in the management of pain are to treat opioid-induced sedation, ventilatory depression, and excitation. If a high dose of naloxone is used, it can antagonize the central effects of the opioid agonist, which may cause the animal to experi- ence acute pain. Such an experience is intensely unpleasant for the patient and may precipitate immediate sympathetic stimulation with serious consequences. In people, this has led to pulmonary edema and even ventricular fibrillation, with several deaths attributed to the administration of naloxone. To this end, it is best to give the drug slowly and monitor the response of the patient. Doses for naloxone are 1 to 25 kg/kg. It is best to start at the low end of the dose range and titrate the dose up to effect. As naloxone is supplied as a 400- or lOOO-k.g/ mL (0.4- or 1.0-mg/mL) solution, it may be helpful to dilute it down to a concentration that is easier to use. An effective method of reducing dysphoria, panting, sedation, or respiratory depression produced by an opioid overdose is to dilute 0.1 to 0.25 mL (O.Crng/mL solution) in 10 mL of normal saline and administer it at 1 mL/min to small or large dogs, respectively, just to the point where the reversal of unwanted side effects has occurred. Using this technique, the analgesic effects of the opioid are not reversed (K. Mathews, personal communication, 1999). In dogs, naloxone is rapidly metabolized to naloxone glucuronide. It has a relatively short half-life in the brain and only provides effective antagonism for about 1 hour, after whch the animal may revert to the effects of the agonist if it lasts longer than this.25 If a longer effect is needed, it may help to give the first dose IV and then give a similar dose SC. Because cats
Table 3. OPlOlD ANALGESICS: APPROXIMATE ANALGESIC EQUIVALENCIES IN PEOPLE"
Equivalent Dose (mg) Compared with 10 mg of Morphine Administered
Intramuscularly Duration of Action
Drug Systemic Oral (hours)
Strong opioid agonists Morphine (single dose) 10 60 3-4 Morphine (chronic dose) 10 20-30 3-4 Hydromorphone 1.5-3.0 6.0-7.5 2-4
Methadone 10 3-5 4-8 Oxymorphone 1.0-1.5 5-10 (rectal) 3-4
Oxycodone 5-15 10-30 2-4
Meperidine 75 300 1-3
Weak opioid agonists Codeine 120-130 200 2-4
'Most of these data were derived from single-dose acute pain studies in human patients and should be considered an approximation for selection of doses when treating chronic pain.
764 PASCOE
are deficient in glucuronyl transferase, it would be expected that naloxone might have a longer half-life in cats, but no direct comparison data are available.
Nalmefene (Revex) is also a pure opioid antagonist and has been developed because of its longer half-life. It is used for the same purposes as naloxone and can produce similar side effects if given rapidly. In a clinical trial, it reversed the effects of oxymorphone and lasted long enough so that there was minimal resedation through a 4-hour observation period.= In a study of the pharmacoki- netics of naloxone in dogs, the longer duration of effect of nalmefene was only apparent in the terminal elimination phase, because the elimination half-times and mean residence times were similar.n Nalmefene is also metabolized via glucuronidation and could have a longer duration of action in cats. Recom- mended doses for people start at 0.25 pg/kg for reversal of respiratory depres- sion. A dose of 30 pg/kg was used in the previously discussed clinical trial." As is the case with naloxone, it is probably best to start with a low dose and titrate the drug to effect.
ORAL ADMINISTRATION
Opioids are metabolized in the liver; thus, there is a significant loss of the drug before it gets to the brain. Hydromorphone has a bioavailability of about 60% given orally and can be a useful analgesic (0.2-0.6 mg/kg administered every 6-8 hours). Oxycodone is twice as potent as morphine with a 3- to 6-hour duration in people. It seems to be effective in dogs at 0.3 mg/kg (increase if required) administered every 6 to 8 hours, and it may be given with a nonsteroi- dal anti-inflammatory analgesic (K. Mathews, personal communication, 1999). Codeine has an oral-to-parenteral ratio of 6.5% in dogs, which is about one tenth of that in In people, approximately 10% of codeine is metabolized to morphine, and it is thought that most of the analgesic action of codeine comes from this conversion. In the dog and cat, less than 1.5% is converted to morphine, and the intrinsic analgesic action of codeine is thought to be 10w.~ In a tooth pulp assay in dogs, 4 mg/kg of codeine SC was equivalent to about 0.15 mg/ kg of morphine.@
An oral sustained-release morphine has recently been studied in dogs, and the drug was absorbed over approximately 6 hours with a 20% bioavailability. The terminal elimination half-life for this preparation was 8 to 10 hours, sug- gesting that it could be given twice a day at a dose of 2 to 5 mg/kg. The oral administration of the morphine was associated with vomiting in several dogs.*Vu
The author has also used oral butorphanol in dogs, assuming that the bioavailability is on the order of 20% to 30% (0.5-2.0 mg/kg). This has been given every 6 to 8 hours.
RECTAL ADMINISTRATION
Both morphine and hydromorphone are available in suppository form. The uptake of either drug is highly dependent on rectal content and the formulation of the drug3, 35. but its bioavailability is similar to that of orally administered drug, and it may have a longer duration of action." This route of administration has been used in people for perioperative analgesia! A study in dogs found little advantage for rectal administration over reported values for oral uptake? The bioavailability of the morphine was 20%, and this study suggests that rectal
OPIOID ANALGESICS 765
administration in dogs does not avoid first-pass metabolism, thus limiting the advantage of using this route to those cases where oral administration is difficult or impossible.
TRANSDERMAL ADMINISTRATION
Highly lipid-soluble drugs such as fentanyl can be absorbed through the skin, and transdermal delivery systems have recently been developed for people. The transdermal patches consist of a drug reservoir containing fentanyl, alcohol gelled together with hydroxyethyl cellulose, and an ethylene-vinyl acetate copol- ymer membrane that controls the rate of delivery of fentanyl to the skin. The currently available patches (Duragesic, Janssen Pharmaceutical, Titusville, NJ) are available in 4 sizes, releasing fentanyl at the rates of 25, 50, 75, and 100 pg/ h and with surface areas of 10, 20, 30, and 40 cm2 containing 2.5, 5.0, 7.5, and 10.0 mg of fentanyl, respectively.
Fentanyl is a schedule I1 drug; as such, it is subject to all the usual regula- tions. The company marketing these patches specifically states that they are not for perioperative use because they were licensed for human cancer patients. As there are significant dangers to people exposed to this drug, it is important that veterinarians prescribing these patches for patients outside their clinic have an understanding of the environment in which the dog or cat is living. A young child could tear a patch off a dog and get enough exposure to fentanyl by licking the patch or sticking it on hmself or herself to cause death.34 An addict might try to extract the fentanyl from the patch; t h s has caused a number of deaths in people, because there is a large quantity of the drug present in the patch.5O
The initial absorption rate is relatively slow, and it takes approximately 6 to 24 hours for the drug to reach peak plasma concentrations in cats and dogs, respectively. In dogs, there are two studies suggesting that it takes 12 to 24 hours to reach peak effect.26,43,66 In cats, the peak values may be reached sooner, but in one study, the cats had significant concentrations of fentanyl measured at time 0.65 In another study in cats, a patch releasing fentanyl at a rate of 25 pg/ h produced plasma values of 0.32 t 0.37 ng/mL at 8 hours, rising to 0.55 2 0.19 ng/mL at 16 hours. The 50-pg/h patch produced concentrations of 0.27 ? 0.20 ng/mL and 0.66 & 0.23 ng/mL at 8 and 16 hours, respectively (JE Ilkiw, personal communication, 1998). Once the peak value is obtained, the plasma concentrations remain fairly constant until removal of the patch (or until the reservoir runs out). In the canine studies, the patches were removed at 72 hours, whereas in one feline study, the patches were left on until 104 hours with maintenance of plasma concentrations. In the above feline study, the 50-pg/h patch maintained plasma concentrations above 0.2 ng/mL for up to 6 days, whereas the 25-pg/ h patch plasma concentrations decreased below the detect- able limit by 60 hours (JE Ilkiw, personal communication, 1998). After removal of the patch, plasma concentrations decay more slowly than after IV administration because there is thought to be a reservoir of drug in the dermis that continues to be absorbed. This decay time is more rapid in dogs than it is in people.26, 66
In human beings, it takes 12 to 24 hours for concentrations to decay below a therapeutic value, whereas such decay is on the order of 2 to 12 hours in 31,43 Bioavailability of fentanyl from this system is high (>90%), and there seems to be little degradation of the drug by the skin or its microflora.76 Several studies have demonstrated the effectiveness of the system as a contribution to postoperative analgesia in people, but it is not being advocated as a sole
766 PASCOE
approach to pain management.13, 32, 46 I n people, there have been a number of fatalities caused by heating the patch. This has occurred when a patient has been lying on a heating pad, which increases the rate of absorption of fentanyl from the patch. One study in dogs (weighing 22 2 7 kg) found comparable levels of analgesia after ovariohysterectomy between a fentanyl patch (50 Fg/h) and oxymorphone (approximately 0.05 mg/kg IM as a preanesthetic and at 6, 12, and 18 hours).44 Plasma fentanyl concentrations were about 1.2 ng/mL. For analgesia, it is suggested that the plasma concentration should exceed 1 ng/mL based on human studies. Another study suggests that transdermal fentanyl is more effective than epidural morphine in dogs undergoing orthopedic surgery.61 The transdermal fentanyl provided poor control of pain in the immediate post- operative period, however, and there were no significant differences in pain scores at any specific time point even though the cumulative pain score was higher over 48 hours for the dogs in which morphine was administered epidur- ally.61 Dose recommendations are as follows:
Cats: 25-50 pg/h Dogs: 3-10 kg = 25 pg/h
10-20 kg = 50 Fg/h
>30 kg = 100 pg/h 20-30 kg = 75 Fg/h
In one study, investigators were not able to show a difference in plasma concentrations between the 75- and IOO-Fg/h patchesz6 When using these patches, it is extremely important not to cut them. The diffusion of fentanyl into the animal is limited by the membrane on the patch, and direct exposure to the gel can cause rapid uptake. If it is necessary to use a small area, the covering on the front surface of the patch can be peeled back and cut so that only one half or one quarter of the patch is stuck to the skin. A variety of sites have been used for these patches, but all the previously discussed studies were carried out with the patches applied to the lateral thorax or the back of the neck. It is not clear how the uptake of the drug might be affected by sites on the back or the leg, although it is likely that these other sites work well, as the rate-limiting membrane in the patch should provide the most consistent barrier to absorption. Before applying these patches, the skin should be gently cleaned with water and allowed to dry. Soap or detergent should not be used, as any residue may prevent the patch from sticking and increases the likelihood of a skin reaction. Once the area has been prepared, the patch is applied firmly and held for about 2 minutes. We prefer to apply a bandage over the patch to decrease the likeli- hood of the patch being removed by a person or the animal. The bandage is labeled with the size of the patch and the time and date of application.
LOCAL ADMINISTRATION
Recently, it has been demonstrated that there are opioid receptors on noci- ceptive nerve terminals that are activated by trauma or inflarnmati~n.~~ This leads to the possibility of occupying these receptors to cause hyperpolarization of the peripheral nerve endings. One piece of evidence for this activity is stress- induced analgesia in the inflamed (Freund’s adjuvant) hind paw of rats. It has been shown that this effect can be abolished by local administration of mu- and delta-receptor antagonists but not kappa antagonists. The effect is also dimin-
OPIOID ANALGESICS 767
ished if the rats are treated with cyclosporine A or irradiation to suppress the immune A source of the peripheral analgesia is thought to be the immune cells that can synthesize opioid peptides. In an induced model of arthritis in dogs, there was a 50-fold increase in morphine binding sites in synovial membrane, and the specifics of the binding tests suggested the mu3 binding site found on immune cells.41
This knowledge has been put to use for intra-articular analgesia, where morphine has been ~ s e d . 3 ~ Joshi et aljs used 5 mg of morphine in 25 mL of saline given into the knee joint of people after arthroscopy. In this study, they found that the analgesia lasted for about 18 hours and that the quality of analgesia was better than that of the control group, which was receiving IV meperidine. They also state that it is important to keep a tourniquet on for at least 10 minutes after injection of the opioid. Another study compared the effect of 1 mg of morphine in 40 mL of saline intra-articularly versus the same dose given IV after arthroscopic knee surgery.72 Analgesia was much better in the group receiving intra-articular morphine. Heard et aP6 suggested that intra- articular bupivacaine gave better analgesia than morphine, but it is not stated in the materials and methods section of their report whether they used a tourniquet. Another study found no beneficial effect with morphine and tourni- quet application for up to 16 Although not confirmed by every study, it seems that most investigators suggest that a combination of morphine and bupivacaine provides the best approach.*, Is, 40 In one canine study, the addition of morphme to intra-articular bupivacaine did nothing to improve the postopera- tive pain scores.62 In another study, intra-articular morphme was as effective as epidural morphine at controlling postoperative pain after stifle arthr~tomy.'~ We have used this intra-articular technique for surgical procedures of the elbow and usually place a catheter in the joint during closure of the surgical wound. After the surgery is finished, we place a tourniquet above the elbow and inflate i; to 300 mm Hg. Morphine (1.0 mg in 5 mL of saline) is injected into the joint, and the tourniquet is left on for 10 minutes. At this time, the tourniquet is released and the catheter is pulled from the joint.
EPIDURAL OR INTRATHECAL ADMINISTRATION
Because there are opioid receptors in the spinal cord, these drugs can be applied directly to these receptors. Ths has led to a tremendous increase in the use of opioids by this route, as smaller doses can be used and the systemic effects can be minimized. Morphine has been the most commonly used drug to date and is the most useful in a veterinary environment because it has a longer duration of action than the more lipid-soluble opioids. Morphine has been used in dogs9, 56, 75 and cats.30 Other opioids have been used for epidural or intrathecal administration, and there is thought to be an inverse relation between lipid solubility and potency. For example, the median effective dose of fentanyl versus morphine was 85.0 versus 15.8 nrnol (24.3 vs 5.3 pg) in a rat model using the percentage of inhibition of C-fiber activity. In th s experiment, IV fentanyl was more effective than intrathecal fentanyl, with 10 pg IV inducing almost complete inhibition of C-fiber activity. The median effective doses for meperidine and methadone in these experiments were 115 and 204 nmol, respectively (these drugs are highly s o l ~ b l e ) . ' ~ ~ ~ ~ Oxymorphone has been used in dogs at 0.1 mg/ kg epidurally with long-lasting (at least 10 hours) beneficial effe~ts.5~ According
768 PASCOE
to Plummer et al,”’ intrathecal oxymorphone was slightly more potent than morphine in the rat hot plate test and equally potent in the tail flick test. Although oxymorphone is about 10 times more potent than morphine, its lipid solubility is higher by systemic administration, which cancels its potency when given intrathecally.
Despite this theoretic relationship, the doses of drugs like fentanyl and sufentanil that are used for intrathecal or epidural administration in people are far lower than the morphine dose. For example, sufentanil has been used at 50 pg epidurally with an infusion of 5 pg/h (total dose per adult human patient) with similar analgesia to morphine at 5 mg and 0.5 rng/h.” Fentanyl at 100 pg plus an infusion of 100 pg/h epidurally gave plasma concentrations similar to those of IV fentanyl (same doses) with no apparent difference in analgesia after knee Combinations of opioids have also been used with the intent of decreasing the latency without sacrificing the duration of action. In one study, a combination of fentanyl (25 pg) and morphine (0.25 mg) was given to women in labor with a decrease in pain scores within 5 minutes and lasting through to perineal distention?’ Despite some of these results, there is evidence suggesting that the more potent and lipophilic opioids are of little or no benefit epidurally, because most of their analgesic effect is the result of systemic absorption and action in the brain7
EPIDURAL AND INTRATHECAL OPlOlDS WITH LOCAL AN ESTH ETlCS
When combined with local anesthetics, there may be further potentiation of the opioid analgesia without an increased duration of motor blockade from the local anesthetic.’ Ths effect has been used extensively by combining morphine with bupivacaine. The combination seems to be chemically compatiblea and causes no neurotoxic effects even when given for prolonged In human studies, the bupivacaine-morphine combination is often given as a bolus fol- lowed by an infusion (e.g., 100 mg of bupivacaine plus 2 mg of morphine followed by 1 mg/h of bupivacaine and 0.2 mg/h of morphine)? In this study comparing bupivacaine, morphine, and the combination after hysterectomy in women, the combination provided the best analgesia, but the analgesia thus provided was not statistically different from that of morphine alone. Both groups receiving morphine had more nausea and vomiting, and there was delayed bowel function and urinary retention? Other studies in human patients have also shown no benefit from the addition of the local anesthetic compared with the opioid alone.“ l5 In another study, there was no difference between pain scores at rest, but the morphine-bupivacaine combination gave greater analgesia during movement and coughing after major abdominal surgery compared with morphine a10ne.16 Recent work in dogs has shown a benefit of this combination3’ as well as a benefit of bupivacaine with oxyrn~rphone.’~ In both studies, the combination provided the greatest postoperative pain relief. When using mor- phine with different local anesthetics, it has been found that 2-chloroprocaine inhibits the action of morphinez7 and fentanyl but not butorphanol.l2 The mecha- nism for t h s inhibitory effect is not understood.
This author has used the combination of morphine and bupivacaine, and early experience was negative in that four animals went lame on the leg not involved in the surgery (all recovered) and two animals developed respiratory
OPIOID ANALGESICS 769
paralysis. All these animals received high volumes of local anesthetic with morphine. Since adjusting the dose to a maximum of 6 mL, no more similar complications have been seen. If this combination is being used postoperatively via an epidural catheter, the concentration of the bupivacaine should be limited to 0.1% to 0.125% to minimize the motor effects of the drug.
SUMMARY
Opioids are useful and potent drugs for the management of pain in small animal patients. They have a wide therapeutic index and can be given by a number of different routes. Some of these techniques (e.g., epidural and intra- articular) allow for the production of profound analgesia in a localized area of the body while limiting the dose and the side effects, and others provide a noninvasive method for the delivery of continuous analgesia (e.g., transdermal administration).
References
1. Akerman B, Arwestrom E, Post C: Local anesthetics potentiate spinal morphine anti- nociception. Anesth Analg 67943, 1988
2. Asantila R, Eklund P, Rosenberg P H Continuous infusion of bupivacaine and mor- phine for postoperative analgesia after hysterectomy. Acta Anaesthesiol Scand 35:513, 1991
3. Babul N, Darke AC, Anslow JA, et al: Pharmacokinetics of two novel rectal controlled- release morphine formulations. J Pain Symptom Manage 7400,1992
4. Badner NH, Reimer EJ, Komar WE, et al: Low dose bupivacaine does not improve postoperative epidural fentanyl analgesia in orthopedic patients. Anesth Analg 72:337, 1991
5. Barnhart MD, Hubbell JAE, Muir WW, et al: Pharmacokinetics, pharmacodynamics, and analgesic effects of morphine after rectal, intramuscular, and intravenous adminis- tration in dogs. Am J Vet Res 61:24, 2000
6. Beaver WT, Feise GA: A comparison of the analgesic effect of oxymorphone by rectal suppository and intramuscular injection in patients with postoperative pain. J Clin Pharmacol 17276, 1977
7. Bernards C M Epidural and intrathecal opioids: Which drugs should we choose and how should they be used? In Annual Refresher Course Lectures, American Society of Anesthesiologists, Dallas, 1999, p 266
8. Boden BP, Fassler S, Cooper S, et al: Analgesic effect of intraarticular morphine, bupivacaine, and morphine / bupivacaine after arthroscopic knee surgery. Arthroscopy 10:104, 1994
9. Bonath KH, Saleh AS: Long term pain treatment in the dog by peridural morphine [abstract]. In Proceedings of the Second International Congress of Veterinary Anesthe- sia, Sacramento, CA, 1985, p 161
10. Brodbelt DC, Taylor I'M, Stanway G W A comparison of pre-operative morphine and buprenorphine for post operative analgesia for arthrotomy in the dog [abstract]. J Vet Anaesth 2442, 1997
11. Bruera E, Belzile M, Neumann CM, et al: Twice-daily versus once-daily morphine sulphate controlled-release suppositories for the treatment of cancer pain. A random- ized controlled trial. Support Care Cancer 7280, 1999
12. Camann WR, Hartigan I'M, Gilbertson LI, et al: Chloroprocaine antagonism of epidural opioid analgesia: A receptor-specific phenomenon? Anesthesiology 73:860, 1990
13. Caplan RA, Ready LB, Oden RV, et al: Transdermal fentanyl for postoperative pain management. A double-blind placebo study. JAMA 261:1036, 1989
770 PASCOE
14. Cribb PH, Vesal N: Post-operative analgesic and cardiopulmonary effects of intramus- cular oxymorphone, epidural oxymorphone, epidural oxymorphone and epidural med- etomidine in dogs: A comparative study [abstract]. J Vet Anaesth 2231, 1995
15. Cullen ML, Staren ED, El-Ganzouri A, et al: Continuous epidural infusion for analgesia after major abdominal operations: A randomized, prospective, double-blind study. Surgery 98:718, 1985
16. Dahl JB, Rosenberg J, Hansen B, et al: Differential analgesic effects of low dose epidural morphine and morphine-bupivacaine at rest and during mobilization after major abdominal surgery. Anesth Analg 74362, 1992
17. Day TK, Pepper WT, Tobias TA, et al: Comparison of intra-articular and epidural morphine for analgesia following stifle arthrotomy in dogs. Vet Surg 24:522, 1995
18. De Andres J, Valaia J, Barrera L, et al: Intra-articular analgesia after arthroscopic knee surgery: Comparison of three different regimens. Eur J Anaesthesiol 15:10, 1998
19. Dickenson A, Sullivan A, McQuay H: Intrathecal etorphine, fentanyl and buprenor- phine on spinal nociceptive neurones in the rat. Pain 42227, 1990
20. Dobromylskyj P: Assessment of methadone as an anaesthetic premedicant in cats. J Small h i m Pract 34:604, 1993
21. Dobromylskyj P: The pharmacokinetics of methadone during the perioperative period [abstract]. J Vet Anaesth 20:45, 1993
22. Dohoo SE, Tasker RA: Pharmacokinetics of oral morphine sulfate in dogs: A compari- son of sustained release and conventional formulations. Can J Vet Res 61:251, 1997
23. Dohoo S, Tasker RA, Donald A Pharmacokinetics of parenteral and oral sustained- release morphine sulphate in dogs. J Vet Pharmacol Ther 17426, 1994
24. Dyer RA, Anderson BJ, Michell WL, et al: Postoperative pain control with a continuous infusion of epidural sufentanil in the intensive care unit: A comparison with epidural morphine. Anesth Analg 71:130, 1990
25. Dyson DH, Doherty T, Anderson GI, et al: Reversal of oxymorphone sedation by naloxone, nalmefene, and butorphanol. Vet Surg 19:398, 1990
26. Egger CM, Duke T, Archer J, et al: Comparison of plasma fentanyl concentrations by using three transdermal fentanyl patch sizes in dogs. Vet Surg 27159, 1998
27. Eisenach JC, Schlairet TJ, Dobson CE, et al: Effect of prior anesthetic solution on epidural morphine analgesia. Anesth Analg 73:119, 1991
28. Findlay JW, Jones EC, Welch RM: Radioimmunoassay determination of the absolute oral bioavailabilities and 0-demethylation of codeine and hydrocodone in the dog. Drug Metab Dispos 7310, 1979
29. Fonda D, Perini A Ketoprofen versus butorphanol efficacy in postsurgical control of pain in cats [abstract]. J Vet Anaesth 2232, 1995
30. Golder FJ, Pascoe PJ, Bailey CS, et al: The effect of epidural morphine on the minimum alveolar concentration of isoflurane in cats. J Vet Anaesth 25:52, 1998
31. Gourlay GK, Kowalski SR, Plummer JL, et al: The efficacy of transdermal fentanyl in the treatment of postoperative pain: A double-blind comparison of fentanyl and placebo systems. Pain 40:21, 1990
32. Gourlay GK, Kowalski SR, Plummer JL, et al: The transdermal administration of fentanyl in the treatment of postoperative pain: Pharmacokinetics and pharmacody- namic effects. Pain 37193, 1989
33. Hardie E, Hansen B, Carroll G: Behavior after ovariohysterectomy in the dog: What’s normal? Appl Anim Behav Sci 51:111, 1997
34. Hardwick W, King W, Palmisano P: Respiratory depression in a child unintentionally exposed to transdermal fentanyl patch. South Med J 90:962, 1997
35. Hayazaki T, Mori T, Kurono S A study on morphine preparations. Report I- Pharmacokinetics of morphine after single oral and rectal administration of controlled release morphine sulphate and morphine hydrochloride in dogs. The Clinical Report 25:7, 1991
36. Heard SO, Edwards T, Ferrari D, et al: Analgesic effect of intraarticular bupivacaine or morphine after arthroscopic knee surgery: A randomized, prospective, double-blind study. Anesth Analg 74:822, 1992
37. Hendrix PK, Raffe MR, Robinson EP, et al: Epidural administration of bupivacaine,
OPIOID ANALGESICS 771
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
morphine, or their combination for postoperative analgesia in dogs. J A W 209:598, 1996 Joshi GP, McCarroll SM, Cooney CM, et al: Intra-articular morphine for pain relief after knee surgery. J Bone Joint Surg Br 74:749, 1992 Kalso E, Tramaer M, Carroll D, et al: Pain relief from intra-articular morphine after knee surgery: A qualitative systematic review. Pain 71:127, 1997 Karlsson J, Rydgren B, Eriksson B, et al: Postoperative analgesic effects of intra- articular bupivacaine and morphine after arthroscopic cruciate ligament surgery. Knee Surg Sports Traumatol Arthrosc 3:55, 1995 Keates HL, Cramond T, Smith MT Intraarticular and periarticular opioid binding in inflamed tissue in experimental canine arthritis. Anesth Analg 89:409, 1999 Klinken C: Effects of tourniquet time in knee arthroscopy patients receiving intraarticu- lar morphine combined with bupivacaine. Certified Registered Nurse Anesthetist 637, 1995 Kyles AE, Papich M, Hardie EM: Disposition of transdermally administered fentanyl in dogs. Am J Vet Res 57715, 1996 Kyles AE, Hardie EM, Hansen BD, et al: Comparison of transdermal fentanyl and intramuscular oxymorphone on post-operative behaviour after ovariohysterectomy in dogs. Res Vet Sci 65245, 1998 Lascelles BD, Cripps PJ, Jones A, et al: Post-operative central hypersensitivity and pain: The pre-emptive value of pethidine for ovariohysterectomy. Pain 73:461, 1997 Latasch L, Luders S: Transdermal fentanyl against postoperative pain. Acta Anaesthe- siol Belg 40113, 1989 Leighton BL, DeSimone CA, Norris MC, et al: Intrathecal narcotics for labor revisited: The combination of fentanyl and morphine intrathecally provides rapid onset of profound, prolonged analgesia. Anesth Analg 69:122, 1989 Loper KA, Ready LB, Downey M, et al: Epidural and intravenous fentanyl infusions are clinically equivalent after knee surgery. Anesth Analg 7072, 1990 Malinovsky JM, Le Normand L, Lepage JY, et al: The urodynamic effects of intravenous opioids and ketoprofen in humans. Anesth Analg 87456, 1998 Marquardt K, Tharratt R Inhalation abuse of fentanyl patch. J Toxicol Clin Toxicol 3275, 1994 Mathews KA, Paley DM, Foster RA, et al: A comparison of ketorolac with flunixin, butorphanol, and oxymorphone in controlling postoperative pain in dogs. Can Vet J 37557, 1996 Matsumoto Y, Watanabe Y, Yamamoto I, et al: Difference in rectal absorption of morphine from hollow-type and conventional suppositories in rabbits. Biol Pharm Bull 16:150, 1993 McQuay HJ, Sullivan AF, Smallman K, et al: Intrathecal opioids, potency and lipophil- icity. Pain 36:111, 1989 Neels JT Compatibility of bupivacaine hydrochloride with hydromorphone hydrochlo- ride and morphine sulfate. American Journal of Hospital Pharmacy 492149, 1992 Pascoe PJ, Dyson DH: Analgesia after lateral thoracotomy in dogs. Epidural morphine vs. intercostal bupivacaine. Vet Surg 22:141, 1993 Pibarot P, Dupuis J, Grisneaux E, et al: Comparison of ketoprofen, oxymorphone hydrochloride, and butorphanol in the treatment of postoperative pain in dogs. JAVMA 211:438, 1997 Plummer JL, Cmielewski PL, Remolds GD, et al: Influence of polarity on dose response relationships of intrathecal opiiids in rats. Pain 40:339, 1990
58. Popilskis S, Kohn DF, Laurent L, et al: Efficacy of epidural morphine versus intrave- nous morphine for post-thoracotomy pain in dogs. J Vet Anaesth 20:21, 1993
59. Popilskis S, Kohn D, Sanchez JA, et al: Epidural vs. intramuscular oxymorphone analgesia after thoracotomy in dogs. Vet Surg 20:462, 1991
60. Robinson EP, Faggella AM, Henry DP, et al: Comparison of histamine release induced by morphine and oxymorphone administration in dogs. Am J Vet Res 49:1699, 1988
61. Robinson TM, Kruse-Elliott KT, Markel MD, et al: A comparison of transdermal fentanyl versus epidural morphine for analgesia in dogs undergoing major orthopedic surgery. J Am h i m Hosp Assoc 35:95, 1999
772 FASCOE
62. Sammarco JL, Conzemius MG, Perkowski SZ, et al: Postoperative analgesia for stifle surgery: A comparison of intra-articular bupivacaine, morphine, or saline. Vet Surg 25:59, 1996
63. Sawyer DC, Rech RH: Analgesia and behavioral effects of butorphanol, nalbuphine, and pentazocine in the cat. J Am Anim Hosp Assoc 23:438, 1987
64. Sawyer DC, Anderson DL, Scott JB: Cardiovascular effects and clinical use of nalbuph- ine in the dog. Proceedings of the Association of Veterinary Anaesthetists of Great Britain and Ireland 10:215, 1982
65. Scherk-Nixon M: A study of the use of a transdermal fentanyl patch in cats. J Am Anim Hosp Assoc 32:19, 1996
66. Schultheiss PJ, Morse BC, Baker W H Evaluation of a transdermal fentanyl system in the dog. Contemporary Topics 34:75, 1995
67. Sjoauberg M, Karlsson PA, Nordborg C, et al: Neuropathologic findings after long- term intrathecal infusion of morphine and bupivacaine for pain treatment in cancer patients. Anesthesiology 76:173, 1992
68. Skingle M, Tyers ME: Further studies on opiate receptors that mediate antinociception: Tooth pulp stimulation in the dog. Br J Pharmacol 70:323, 1980
69. Slingsby LS, Lane EC, Mears ER, et al: Postoperative pain after ovariohysterectomy in the cat: A comparison of two anaesthetic regimens. Vet Rec 143:589, 1998
70. Slingsby LS, Waterman-Pearson AE: Comparison of pethidine, buprenorphine and ketoprofen for postoperative analgesia after ovariohysterectomy in the cat. Vet Rec 143:185, 1998
71. Stein C: Peripheral mechanisms of opioid analgesia. Anesth Analg 76:182, 1993 72. Stein C, Comisel K, Haimerl E, et al: Analgesic effect of intraarticular morphine after
arthroscopic surgery. N Engl J Med 325:1123, 1991 73. Taylor I'M, Houlton JEF Post-operative analgesia in the dog: A comparison of mor-
phine, buprenorphine and pentazocine. J Small Anim Pract 25:437, 1984 74. Torske KE, Dyson DH, Pettifer G: End tidal halothane concentration and postoperative
analgesia requirements in dogs: A comparison between intravenous oxymorphone and epidural bupivacaine alone and in combination with oxymorphone. Can Vet J 39:361, 1998
75. Valverde A, Dyson DH, McDonell WN, et al: Use of epidural morphine in the dog for pain relief. Vet Comp Orthop Traumatol 2:55, 1989
76. Varvel JR, Shafer SL, Hwang SS, et al: Absorption characteristics of transdermally administered fentanyl. Anesthesiology 70:928, 1989
77. Veng-Pedersen P, Wilhelm JA, Zakszewski TB, et al: Duration of opioid antagonism by nalmefene and naloxone in the dog: An integrated pharmacokmetic/ pharmacody- namic comparison. J Pharm Sci 841101, 1995
78. Waterman AE, Kalthum W Use of opioids in providing postoperative analgesia in the dog: A double-blind trial of pethidine, pentazocine, buprenorphine, and butorphanol. In Short CE, Van Poznack A (eds): Animal Pain. New York, Churchill Livingstone, 1992, p 466
79. Yeh SY, Woods LA Excretion of codeine and its metabolites by dogs, rabbits and cats. Archives Internationales de Pharmacodynamie et de Therapie 191:231, 1971
Address reprint requests to
Peter J. Pascoe, BVSc University of California School of Veterinary Medicine
Department of Surgical and Radiological Sciences Schml of Veterinary Medicine
Davis, CA 95616
e-mail: [email protected]