Opioid analgesics
56
-
Upload
ryma-chohan -
Category
Health & Medicine
-
view
167 -
download
1
Transcript of Opioid analgesics

Analgesics
Drugs that relief pain without loss of
conciousness.
Opioid or Narcotic analgesics
Non-opioid or NSAIDS
Basic Pharmacology of Opoid
Analgesic
Source
Opium (Morphine Source) is obtained from Poppy, Papaver somniferum and P album.
Poppy seed pod exudes white substance that turns into brown gum i.e crude opium
Morphine is present in high concentration (10%).
Codeine is commercially synthesized from Morphine
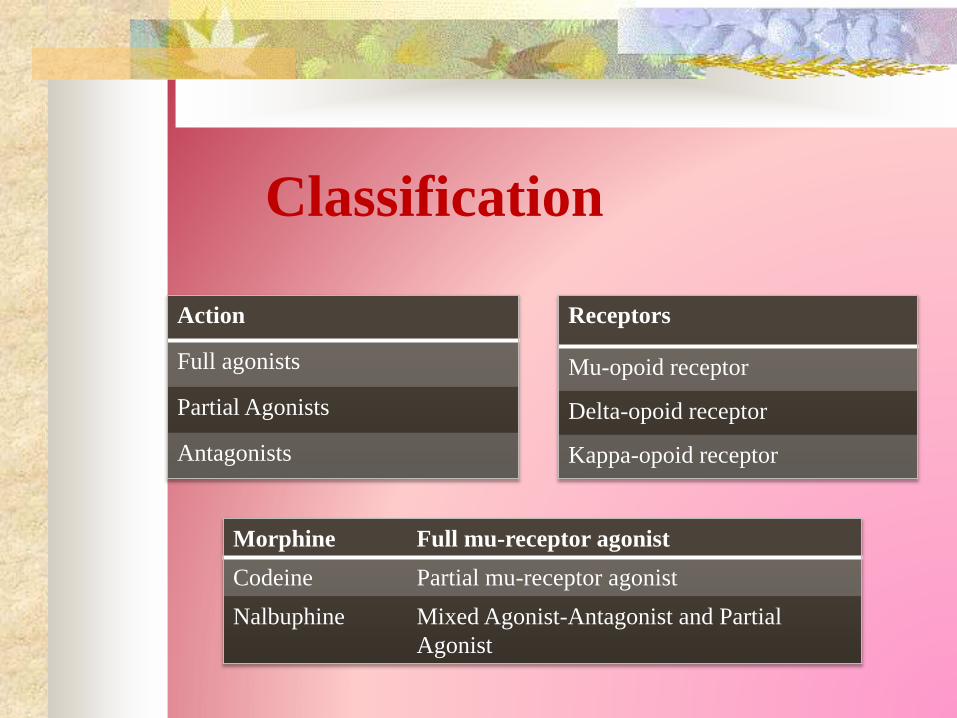
Classification
Action
Full agonists
Partial Agonists
Antagonists
Receptors
Mu-opoid receptor
Delta-opoid receptor
Kappa-opoid receptor
Morphine Full mu-receptor agonist
Codeine Partial mu-receptor agonist
Nalbuphine Mixed Agonist-Antagonist and Partial
Agonist
Chemistry
Substitution of allyl group on the nitrogen of
morphine and addition of single hydroxyl group
Form naloxone(strong mu-
receptor antagonist)
Certain opoid analgesics modified in liver
form compounds with greater analgesic action
Most of the synthetic opoids are simpler
molecules
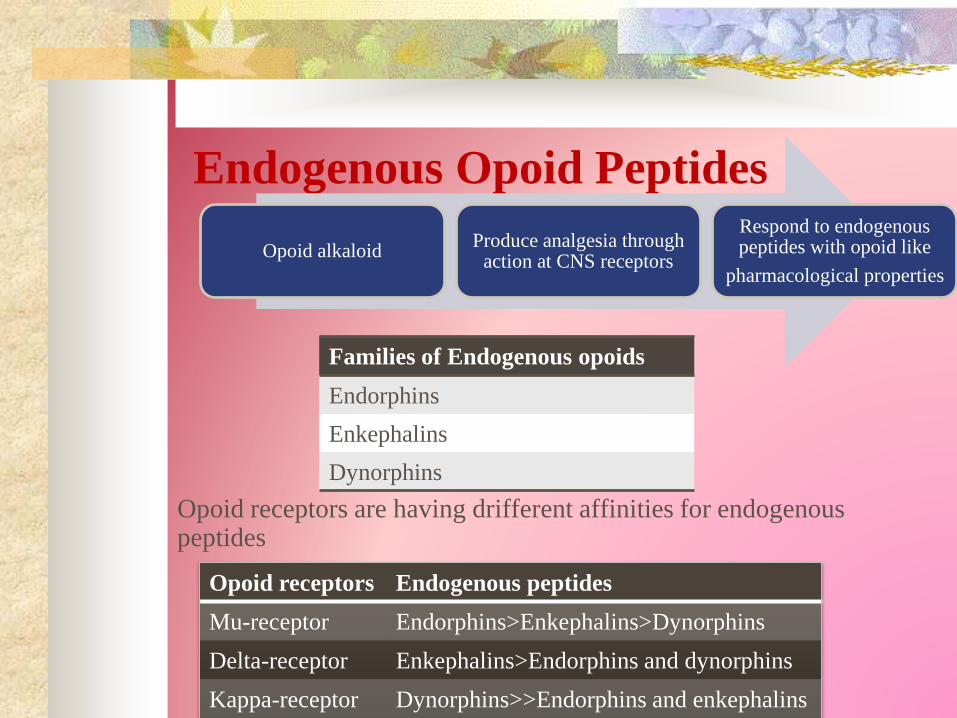
Endogenous Opoid Peptides
Opoid receptors are having drifferent affinities for endogenous peptides
Opoid receptors Endogenous peptides
Mu-receptor Endorphins>Enkephalins>Dynorphins
Delta-receptor Enkephalins>Endorphins and dynorphins
Kappa-receptor Dynorphins>>Endorphins and enkephalins
Families of Endogenous opoids
Endorphins
Enkephalins
Dynorphins
Opoid alkaloidProduce analgesia through
action at CNS receptors
Respond to endogenous peptides with opoid like
pharmacological properties

Endogenous peptides are derived from three
precursor proteins:
Prepro-opiomelanocortin(POMC)
Preproenkephalin(Proenkephalin A)
Preprodynorphin(Proenkeohalin B)
POMC contains Preproenkephalin contains Preprodynorphin contains
Met-enkephalin sequence Six copies of met enkephalin active opoid peptides containg
leu-enkephalin sequence
Beta-endorphin one copy of leu-enkephalin Active peptides are dynorphin
A, dynirohin B and alpha and
beta-nonendorphins
nonopoind peptides including
adenocorticotropic hormone,
Beta-lipotropin, melanocyte
stimulating hormone
met and leu have slightly high
affinity for delta then mu
receptor
Dynorphin A found in dorsal horn of
spinal cord play role in sensitization of
nociceptive neurotransmission.
Increased dynorphin causing increase pain and
long lasting hyperalgesia due to tissue injury and
inflammation
Endogenous opoid precursor molecule and
endopmorphins are present at CNS sites that have been
implicated with pain modulation
Pronociceptive action of dynorphin
independent of opoid receptor…..but dependent on
bradykinin receptor activation
Endogenous peptides, endomorphin-1 and endomorphin-
2 selectively activate central and peripheral mu-opoid
receptors
Pharmacokinetics
Absorption Opioid agonist are well absorbed when given by
subcutaneous,intramuscular and oral route.
Oral route needs high dose as compared to parenteralroute
Certain analgesics such as codeine and oxycodoneare effective orally because they have reduced first-pass metabolism.
Other routes includes oral mucosa via lozenges and transdermal via transdermal patches.
Recently an iontophoretics transdermal system has been introduced.
Distribution
All opioids bind to plasma proteins with varying
affinity.
The drugs rapidly leave the blood compartment
and localize in highest concentrations in tissues.
Drug concentrations in skeletal muscle may be
much lower, but this tissue serves as the main
reservoir because of its greater bulk.
Metabolism
The opioids are converted in large part to polar
metabolites (mostly glucuronides).
Morphine is metabolized to M3G and M6G.
M3G, a compound with neuroexcitatory property
and M36, a compound with analgesic property.
Esters are rapidly hydrolyzed by tissue esterases
e.g remifentanil.
Heroin (diacetylmorphine) is hydrolyzed to
monoacetylmorphine and finally to morphine,
which is then conjugated with glucuronic acid.
Cont…
Hepatic oxidative metabolism is the primary route of
degradation of the phenylpiperidine opioids.
The P450 isozyme CYP3A4 metabolizes fentanyl by
N-dealkylation in the liver.
Codeine, oxycodone, and hydrocodone undergo
metabolism in the liver by P450 isozyme CYP2D6.
Metabolic disposition of naloxone is chiefly by
glucronides conjugation like that of the agonist .
Excretion
Polar metabolites, including glucuronide
conjugates of opioid analgesics, are excreted
mainly in the urine.
Small amounts of unchanged drug may also be
found in the urine.
Glucuronide conjugates are also found in the bile.
Enterohepatic circulation represents only a small
portion of the excretory process.
Pharmacodynamics
Mechanism of Action• Opioid agonists produce analgesia by binding to
specific G protein-coupled receptors
• Receptors located primarily in brain and spinalcord regions (transmission and modulation of pain).
Receptor Types
• Multiple receptor subtypes have been proposedbased on pharmacologic criteria, including
o µ1,µ2
o δ1,δ2
o κ1,κ2,κ3
Pharmacodynamics
Opioid receptors form a family of proteins that physically couple to G-proteins
This interaction affect ion channel gating
1. They close voltage-gated Ca2+ channels on presynaptic nerve terminals and thereby reduce transmitter release
2. They hyperpolarize and thus inhibit postsynaptic neurons by opening K+ channels.
gg
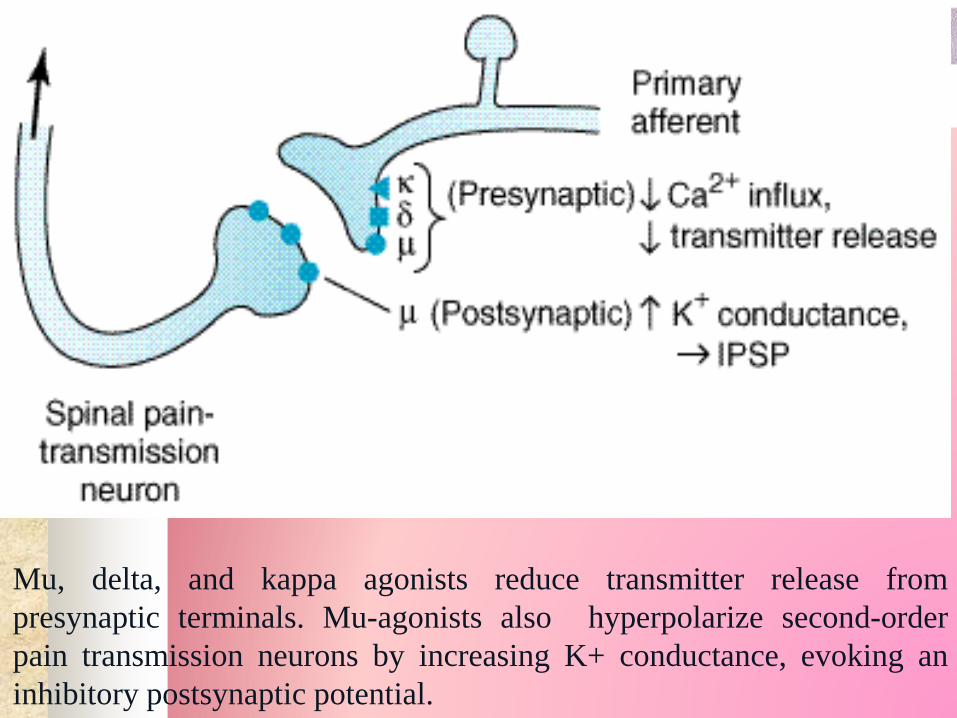
Mu, delta, and kappa agonists reduce transmitter release from
presynaptic terminals. Mu-agonists also hyperpolarize second-order
pain transmission neurons by increasing K+ conductance, evoking an
inhibitory postsynaptic potential.
Tolerance and Physical Dependence
Tolerance
With frequently repeated administration of therapeutic doses of morphine there is a gradual loss in effectiveness
Physical dependence
Occurrence of a characteristic withdrawal when the drug is stopped or an antagonist is administered.
Organ System Effects
Central Nervous System Effects
Analgesia:
Opioids reduce both sensory and affective aspects
of pain.
Specially affective aspects.
Euphoria:
IV morphine – euphoria…reduce anxiety and
distress

Sedation:
Drowsiness
Clouding of mentation
Induce more sleep in elders than youngs
Morphine + sedative-hypnotics = Deep sleep
Phenanthrene derivatives > synthetic agents
Morphine disrupts REM and Non-REM sleep
patterns

Repiratory Depression:
Direct action on brain stem respiratory centre
Increases alveolar CO2
Respiratory rate = 3-4 beats/min
Cough supression:
Cough treatment
Ventilation via endotracheal tube – codiene
Secretion Airway obstruction
Miosis:
Induce pupillary constriction in awake state
Block pupillary reflex dilation during anasthesia
Nausea and Vomiting:
Opioids activates CTZ in area prostema of
medulla
Temperature:
Endogenous opioids – maintain body temperature
Morphine – hyperthermia
K- agonists - hypothermia
Peripheral Effects CVS:
No direct effect on heart (cardiac rhythm)
Morphine – release of histamines – peripheral
vasodilation- preload, ionotropy & chronotropy
– cardioprotective
GIT:
Stomach- motility tone HCL secretion
Intestine- resting tone with spasm – constipation

Biliary tract:
Contracts biliary smooth muscles – biliary colic
Renal:
Depress renal function – renal plasma flow –
ADH release – Na+ reabsorbtion – urinary
retention
Uterus:
uterine tone –prolong labour
Neuroendocrine:
+ release of ADH, prolactin and somatotropins
- release of LH
Skin:
Histamine release – dilation of cutaneous blood
vessels – flushing, warming of skin
Miscellaneous:
Opioids modulate immune system
Lymphocyte proliferation
Antibody production
Chemotaxis
Leucocyte migration- opioid peptides –
inflammatory pain.
CLINICAL PHARMACOLOGY

ANALGESIA:
• Relieve constant pain.
• In cancer, terminal illness, labor, renal and biliary colic
pain.
• Sustained release dosage forms MSContin and
OXYContin.
• In GIT disturbances we use fentanyl transdermal or
transmucosal patches.
• Amphetamine.
• Morphine and mepridine in labor.
• Strong opiod agonist for renal and biliary pain.
• Nalaxone – antagonist
ACUTE PULMONARY EDEMA:
Morpine and furosemide are used.
Furosemide when only pulmonary edema.
Morphine (IV) when pulmonary edema with myocardial
ischemia as decreases anxiety, cardiac preload and
afterload.
COUGH:
Low dose like 15mg codeine.
Diminished use.
DIARRHEA:
Paregoric, diphenoxylate and loperamide.
Not used when infection is there..
SHIVERING:
Mepridine - more pronounced effect.
Alpha-2 adrenoreceptor.
ANESTHESIA:
Along with analgesic opiods have sedative and anxiolytic
property.
Direct action on superficial nerves of dorsal horn of spinal
cord through epidural and subarachanoid route.
Epidural route is preferred – morphine.
Nalaxone – Antagonist.
CVS surgery.
Thoracic and upper abdominal surgery
local anesthetic + fentanyl
thoracic epidural catheter
Continuous infusion.
ADVERSE EFFECTS OF OPIOD ANALESICS:
Respiratory depression
Nausea
Vomiting
Constipation
Itching around nose
Postural hypotention
Hypovolemia
Restlessness
Tremulousness
Hyperactivity
Increased intracranial pressure
Urinary retention
Urticaria (spinal and parenteral administration)
TREATMENT:
Antagonist – nalaxone (IV).
Reverse coma due to opiods only.
CONTRAINDICATIONS:USE OF PURE AGONIST WITH WEAK PARTIAL
AGONIST
Morphine + pentazocine.
Diminished analgesia and withdrawl effects.
USE IN PATIENTS WITH HEAD INJURY:
Respiratory depression – CO2 retention – cerebral vasodilation – brain function alters.
USE DURING PREGNANCY:
Physical dependence and withdrawl effects with 6mg heroin daily.
Irritability, shrill crying, diarrhea, seizure with 12mg heroin.
Treated with diazepam, methadone & camphorated tincture of opium.

USE IN PATIENTS WITH IMPAIRED PULMONARY
FUNCTION:
Respiratory failure.
USE IN PATIENTS WITH IMPAIRED HEPATIC
FUNCTION:
Effects drug metabolism.
USE IN PATIENTS WITH IMPAIRED RENAL
FUNCTION:
Increased half life and accumulation of active
glucoronide metabolites.
USE IN PATIENTS WITH ENDOCRINE DISEASES:
Prolonged and exaggerated response to opiods.
DRUG INTERACTIONS:SEDATIVE – HYPNOTICS:
Increased CNS depression
Increased respiratory depression
ANTIPSYCHOTICS TRANQUILIZERS:
Increased sedation
Respiratory depression
Anti-muscarinic CVS effects
Alpha blocking CVS effects
MAO INHIBITORS:
Hyperpyrexic coma
Hypertension

SPECIFIC AGENTS
Strong agonists
Phenanthrenes
Phenyl
Heptyl
amines
Morphinans
Phenyl
piperidines

PhenanthrenesThis class includes drugs as Morphine,
hydromorphone and oxymorphone.
Strong mu-R agonist although shows
binding affinity to other opioid receptors.
Heroin:
It is also called diamorphine ,
diacetylmorphine.
It is potent and fast acting.
More effective than morphine in relieving
pain by IM route.
PhenylheptylaminesThis class includes agents such as Methadone.
Potent mu-R agonist.
Exists as racemic mixture i.e. in form of D
and L isomers of methadone.
Can block NMDA and Monoaminergic
reuptake transporter thus helpful in
treatment of neuropathic pain.
Methadone-Clinical uses Used in treatment of opioid abuse. Treatment of mild to severe pain. For detoxification of heroin dependent
addict it is given 5-10 mg orally two to three times a day for 2-3 days.
Its use as analgesic has increased due to less effect on CNS functions compared to Morphine.
Phenylpiperidines This class include Fentanyl and its subgroup
includes agents like sufentanil, alfentanil, remifentanil.
Sufentanil is 5 to 7 times more potent than fentanyl.
Alfentanil is less potent than fentanyl but rapidly acting and with shorter duration of action.
Remifentanil is rapidly metabolized by blood and tissue esterases thus exhibiting shorter half life.
Meperidine:
Shows anti-Muscarinic effects which can
be a contraindication in case of
tachycardia.
Negative inotropic action on heart.
Can produce seizures
Due to increased side effect profile its
rarely used as an analgesic.
MILD TO MODERATE OPIOID AGONISTS
Phenantherenes Phenylpiperidines Phenantherenes
Phenantherenes
CODIENE, DIHYDROCODEINE,
HYDROCODONE:
Are less efficious than morphine.
OXYCODONE:
Semisynthetic derivative of codeine that acts as
a narcotic analgesic’ more potent.
COMBINATION:
Hydrocodone/oxycodone with acetaminophen=> for
treatment of mild to moderate pain, used orally
Phenylheptylamines
PROPOXYPHENE:
Chemically related to methadone
Low analgesic properties
Low efficiancy
Phenylpiperidines
Diphenoxylate
loperamide
Used as Anti-diarrheal agents.
Diphenoxylate is used in combination with
atropine.
DOSE: two tablets to start and then one
tablet after each diarrheal stole.
OPIODS WITH MIXED RECEPTOR FUNCTIONS
Phenantherenes Benzomorphans Morphinans
PhenantherenesNALBUPHINE:
K-receptor agonist
u-receptor antagonist
Given parenterally
Causes such
respiratory
depression which cannot
Be reversed by naloxone.
BUPRENORPHINE:
• Partial u agonist
• K-antgonist
• Slow dissociation
from u-receptorslong
duration of action
• Used for
detoxification
• Maintaince of heroin
abuse

Morphinans
BUTORPHANOL:
K-receptor agonist
Partial u-receptor
agonist/antagonist.
Produces analgesia
equivalent to nalbuphine
and buprinorphine.
PENTAZOCIN:
• K-receptor agonist
u- antagonist/ partial
antagonist.
• Orally or parenterally.
• No sub cutaneous
injection becaucse of
irritant properties.
Benzomorphans
AntagonistsNaloxone
Naltrexone
Nalmefene
They are receptor antagonist that acts on opioid receptors (µ, ,k).
These agents in the treatment of opioid overdose
Clinical Uses
NALOXONE Initial dose: 0.1 to 0.4mg IV
for life threatning CNS and
respiratory depression
NALTREXONEUsed in maintainence
programs
Blocks heroin effects
upto 48hours
FDA approved for
alcohol abuse
Used to prevent relapse
of alcohol drinking
Effective for weight lose
When you do not succeed in taking giant steps on the road to your goal, be satisfied with little steps,
and wait patiently till the time that you are able to run, or better still, to fly.
Be satisfied to be a little bee in the hive who will soon become a big bee capable of making
honey…
Thank you …
56