Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering – MIRACL: Rationale and Results...
29
Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering – MIRACL: Rationale and Results A Slide Lecture Kit
-
Upload
marilyn-johns -
Category
Documents
-
view
224 -
download
5
Transcript of Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering – MIRACL: Rationale and Results...

Myocardial Ischemia Reduction with Aggressive Cholesterol
Lowering – MIRACL:Rationale and Results
A Slide Lecture Kit
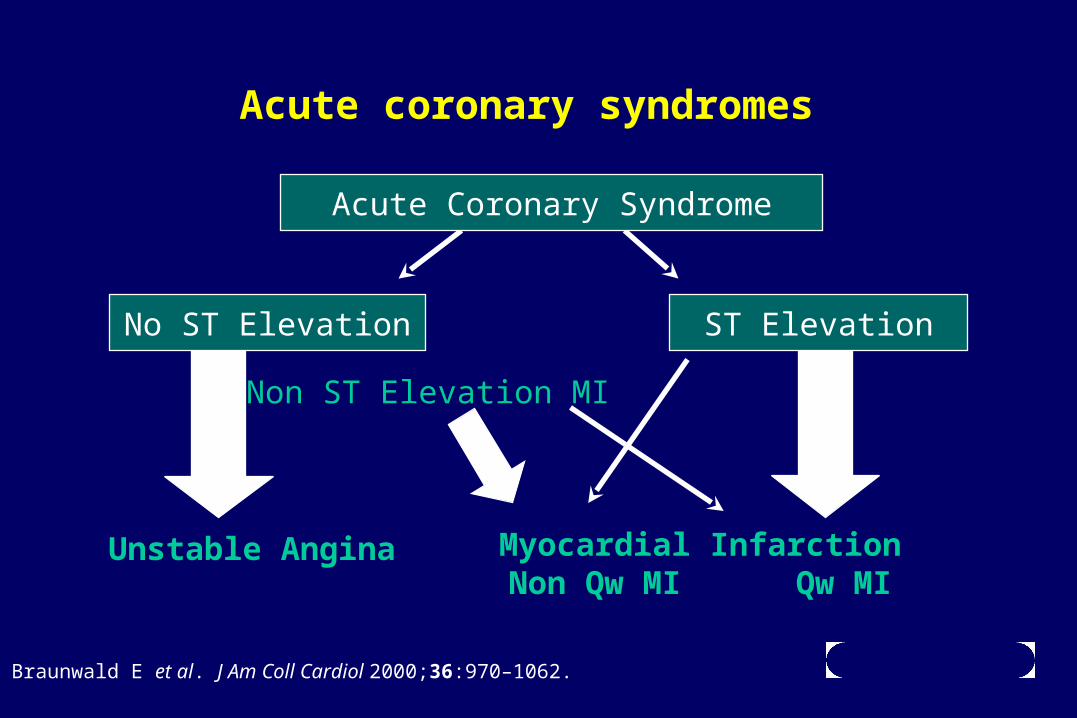
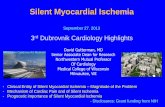
Acute coronary syndromes
Acute Coronary Syndrome
No ST Elevation ST Elevation
Unstable Angina Myocardial InfarctionNon Qw MI Qw MI
Non ST Elevation MI
Braunwald E et al. J Am Coll Cardiol 2000;36:970–1062.

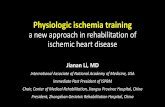
Outcomes in primary prevention, stable and unstable coronary disease
Dea
th/n
on
fata
l MI (
%)
Months of follow-up
Unstable angina/non-Q-wave MI (FRISC II)
16
12
8
4
0
0 2 4 6 8 10 12
Stable angina (SAPAT)
Wallentin L et al. Lancet 2000;356:9–16.Juul-Moller S et al. Lancet 1992;340:1421–1425.Shepherd J et al. N Engl J Med 1995;333:1301–1307.
Primary prevention (WOSCOPS)
Unstable angina: prognosis
• Patients with unstable angina have a far worseshort-term prognosis than do patients with stable angina
• Despite recent advances in therapy, the relative risk of death or nonfatal MI in patients with unstable angina versus those with stable disease is higher over the first year
Braunwald E et al. J Am Coll Cardiol 2000;36:970–1062.Wallentin L et al. Lancet 2000;356:9–16.Juul-Moller S et al. Lancet 1992;340:1421–1425.

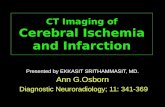
Early secondary prevention trials only focussed on long-term event reductions in stable patients
1.00
0.95
0.90
0.85
0.80
0.00
0 1 2 3 4 5 6
Pro
po
rtio
n a
liv
e
Risk reduction, 30%Log-rank p=0.0003
Simvastatin
Placebo
4S
0
0
Fa
tal
CH
D/n
on
fata
lM
I (%
)
5
10
15
20
1 2 3 4 5 6 7
Risk reduction, 24%p<0.001
Pravastatin
Placebo
LIPID
0 1 2 3 4 5 6
15
10
5
0
Fa
tal
CH
D/n
on
fata
lM
I (%
)
Risk reduction, 24%p=0.003
Pravastatin
Placebo
CARE
Years4S Study Group. Lancet 1994;344:1383–1389.Sacks FM et al. N Engl J Med 1996;335:1001–1009.LIPID study group. N Engl J Med 1998;339:1349–1357.

MIRACL: addressed a treatment gapAcute coronary
event
MIRACL
4S3
AFCAPS / TexCAPS/WOSCOPS
CARE1/LIPID2
4 moNo history of CAD Unstable CAD
Randomization:24–96 h
3 mo
t=0
6 moRandomization:
CARE - 3–20 moLIPID - 3–36 mo
Randomization:>6 mo
Stable CAD
Primary prevention Secondary prevention
Schwartz GG et al. Am J Cardiol 1998;81:578–581.Duration of follow-up: 15.0 years; 26.1 years; 35.4 years.
MIRACL: central hypothesis
Early, rapid, and profoundcholesterol lowering therapy with
atorvastatin can reduce early recurrent ischemic events in patients with unstable
angina or non-Q-wave acute MI
Schwartz GG et al. Am J Cardiol 1998;81:578–581.

MIRACL: inclusion criteria
• Unstable Angina– Hospitalization with 15 min or more chest pain or discomfort within
24 h of admission, together with one of the following:–Dynamic or interval ECG changes–New wall motion changes on echo and/or positive perfusion
defect–Abnormally elevated Troponin-T or -I
• Absence of new/presumed new Q-waves (30 m sec)
• Non-Q-wave MI– Hospitalization with chest pain (15 min or more) within 24 h– Elevated CK or Troponin (>2 x ULN)
Schwartz GG et al. Am J Cardiol 1998;81:578–581.Data on file, Pfizer Inc.
MIRACL: exclusion criteria
• Serum cholesterol levels >7 mmol/L (>8 mmol/L in Poland and South Africa)
• Coronary revascularization planned/anticipated
• Recent Q-wave MI <1 month
• Recent CABG (<3 months) or PTCA (<6 months)
• LBBB or paced ventricular rhythm; severe CHF
• Concurrent lipid-lowering therapy (except niacin)
Schwartz GG et al. Am J Cardiol 1998;81:578–581.Data on file, Pfizer Inc.

MIRACL: exclusion criteria (cont’d)
• Vitamin E (except at doses 400 IU daily)
• Drugs associated with rhabdomyolysis
• Severe anemia; renal or hepatic dysfunction
• Brittle type 1 diabetes
• Pregnancy/lactation
Schwartz GG et al. Am J Cardiol 1998;81:578–581.
MIRACL: study design
• Randomized, double-blind, placebo-controlled
• Intention-to-treat
• 16-week follow-up
• 3086 patients
• Enrollment: June 1997–September 1999
• Last patient completed in January 2000
Schwartz GG et al. Am J Cardiol 1998;81:578–581.Data on file, Pfizer Inc.

MIRACL: study design (cont’d)
Hospitalizationfor
unstable anginaor non-Q MI
n=3086Randomized
24–96 hoursafter admission
Placebo + diet
Atorvastatin 80 mg + diet
16 weeks
Assessments conducted at weeks 0, 2, 6 and 16
Schwartz GG et al. Am J Cardiol 1998;81:578–581.

MIRACL: primary efficacy measure
Time to first event:• Death (any cause)
• Nonfatal MI
• Resuscitated cardiac arrest
• Worsening angina with new objective evidence of ischemia requiring urgent rehospitalization
Schwartz GG et al. Am J Cardiol 1998;81:578–581.
MIRACL: secondary efficacy measures
• Occurrence of
– Individual components of the primary efficacy measure
– Stroke
– Myocardial revascularization (CABG or PTCA)
– Worsening congestive heart failure
– Worsening angina without new objective evidence of ischemia
• Percent change from baseline in lipids (TC, LDL-C, HDL-C, TG) at end of study
Schwartz GG et al. Am J Cardiol 1998;81:578–581.Data on file, Pfizer Inc.

MIRACL: statistical assumptions/analyses
• Overall primary end point rate = 13%
• Sample size = 3000 (80% power to detect 25% reduction in primary end points)
• Due to interim analyses, significance level = 0.049 for primary efficacy measure
• All analyses by intention to treat
• All end points adjudicated by blinded committee
• Time-to-event analysis: Cox Proportional Hazards
• End point occurrence: Cochran-Mantel-Haenszel
• Lipid analyses: ANCOVA
Data on file, Pfizer Inc.
• Investigators at 122 sites in 19 countries
• Committees– Steering– Blinded End point– Data Monitoring and Safety
• Core laboratories– ECG– Clinical chemistry
• Investigators at 122 sites in 19 countries
• Committees– Steering– Blinded End point– Data Monitoring and Safety
• Core laboratories– ECG– Clinical chemistry
MIRACL: study organization
Schwartz GG et al. Am J Cardiol 1998;81:578–581.Data on file, Pfizer Inc.
MIRACL: study organization (cont’d)
Co-Principal Investigators• Anders Olsson, MD• Gregory Schwartz, MD
Steering Committee• Anders Olsson, MD• Gregory Schwartz, MD• Michael Ezekowitz, MD• Peter Ganz, MD• Michael Oliver, MD• David Waters, MD• Andreas Zeiher, MD
St. Louis Core ECG Lab• Bernard Chaitman, MD
Data Monitoring and Safety Committee• Eliott Rapaport, MD (Chair)• Paul Armstrong, MD• Antonio Gotto Jr, MD• Stuart Pocock, PhD
End point Committee• Peter Stone, MD (Chair)• Merill Knudtson, MD• Jean-Marc LaBlanche, MD• Herbert Levine, MD• Christopher O’Connor, MD• Blair O’Neill, MD
Data on file, Pfizer Inc.

MIRACL: baseline characteristicsDemographics
Placebo AtorvastatinCharacteristic (n=1548) (n=1538)
Gender
Male, n (%) 1020 (65.9) 992 (64.5)
Female, n (%) 528 (34.1) 546 (35.5)
Race
White, n (%) 1324 (85.5) 1317 (85.6)Black, n (%) 44 (2.8) 51 (3.3)Asian, n (%) 58 (3.7) 40 (2.6)Other, n (%) 122 (7.9) 130 (8.5)
Age (years), Median 65 66
Min–Max 26–94 30–93
Mean (SE) 65 (0.30) 65 (0.30)
Data on file, Pfizer Inc.

MIRACL: baseline characteristicsDemographics (cont’d)
Placebo AtorvastatinCharacteristic [n (%)] (n=1548) (n=1538)
Current smokers 430 (27.8) 429 (27.9)
Past MI 392 (25.3) 382 (24.8)Q-wave 191 (12.3) 180 (11.7)
Revascularization 173 (11.2) 153 (9.9)CABG 121 (7.8) 112 (7.3)PTCA 52 (3.4) 41 (2.7)
Inclusion eventUnstable angina 705 (45.5) 726 (47.2)Non-Q-wave acute MI 843 (54.5) 812 (52.8)
Data on file, Pfizer Inc.

MIRACL: concurrent medicationsaccording to treatment group
Medications during and/or following Placebo Atorvastatinhospitalization for Index Event [n (%)] (n=1548) (n=1538)
Aspirin 1412 (91.2) 1400 (91.0)Platelet GPIIb/IIIa RAs 19 (1.2) 14 (0.9)Other antiplatelet agents 176 (11.4) 176 (11.3)Heparin 1154 (74.6) 1147 (74.6)Oral anticoagulants (coumarites) 129 (8.3) 119 (7.7)Fibrinolytic agents 137 (8.9) 109 (7.1) Nitrates 1396 (90.2) 1389 (90.3)Beta-blockers 1200 (77.5) 1192 (77.5)Calcium-channel blockers 745 (48.1) 735 (47.8)ACE inhibitors or ARBs 769 (49.7) 746 (48.5)Digoxin 171 (11.1) 182 (11.8)
Data on file, Pfizer Inc.

Baseline End of studyMean of both groups Placebo Atorvastatin
mg/dL mg/dL (% change)
Total cholesterol 206 217 147 (+ 7%) (- 27%)
LDL cholesterol 124 135 72(+ 12%) (- 40%)
HDL cholesterol 46 46 48(+ 4%) ( + 5%)
Triglycerides 182 187 139(+ 9%) (- 16%)
MIRACL: plasma lipids
Data on file, Pfizer Inc.
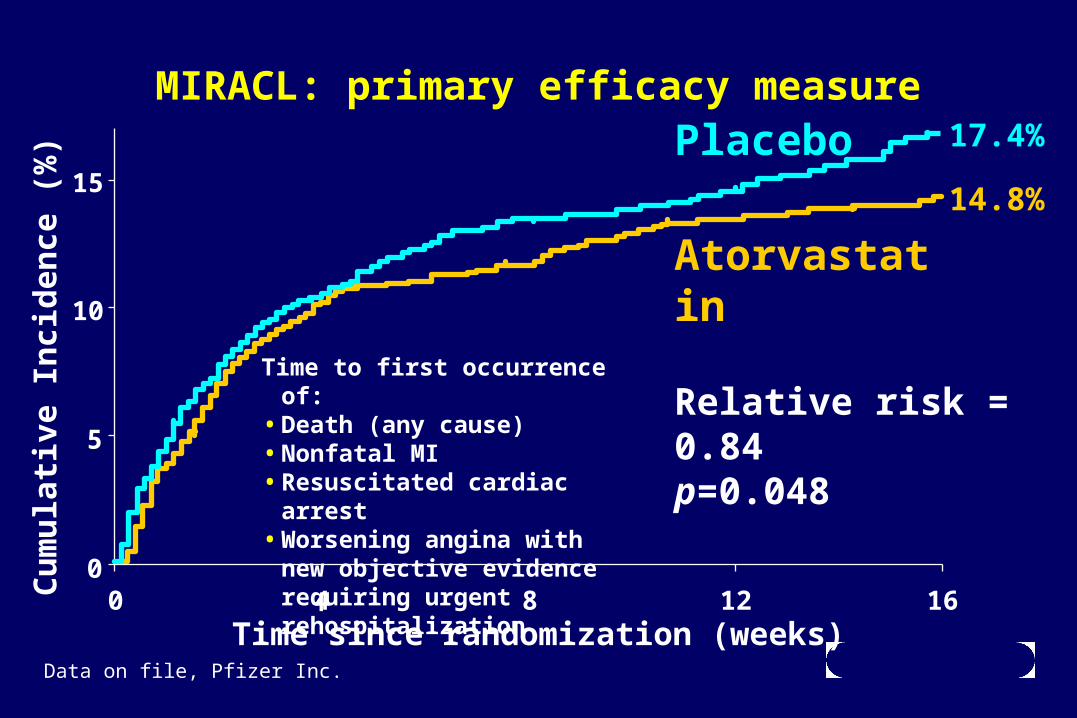
MIRACL: primary efficacy measure
Relative risk = 0.84p=0.048
Atorvastatin
Placebo
0
5
10
15
0 4 8 12 16Time since randomization (weeks)
Cu
mu
lati
ve I
nci
den
ce (
%)
Time to first occurrence of:• Death (any cause)• Nonfatal MI• Resuscitated cardiac arrest• Worsening angina with new
objective evidence requiring urgent rehospitalization
17.4%
14.8%
Data on file, Pfizer Inc.

MIRACL: worsening angina with new objective evidence of ischemia requiring urgent rehospitalization
0
3
6
9
0 4 8 12 16
Time since randomization (weeks)
Cu
mu
lati
ve I
nci
den
ce (
%)
Relative risk = 0.74p=0.02
Atorvastatin
Placebo 8.4%
6.2%
Data on file, Pfizer Inc.
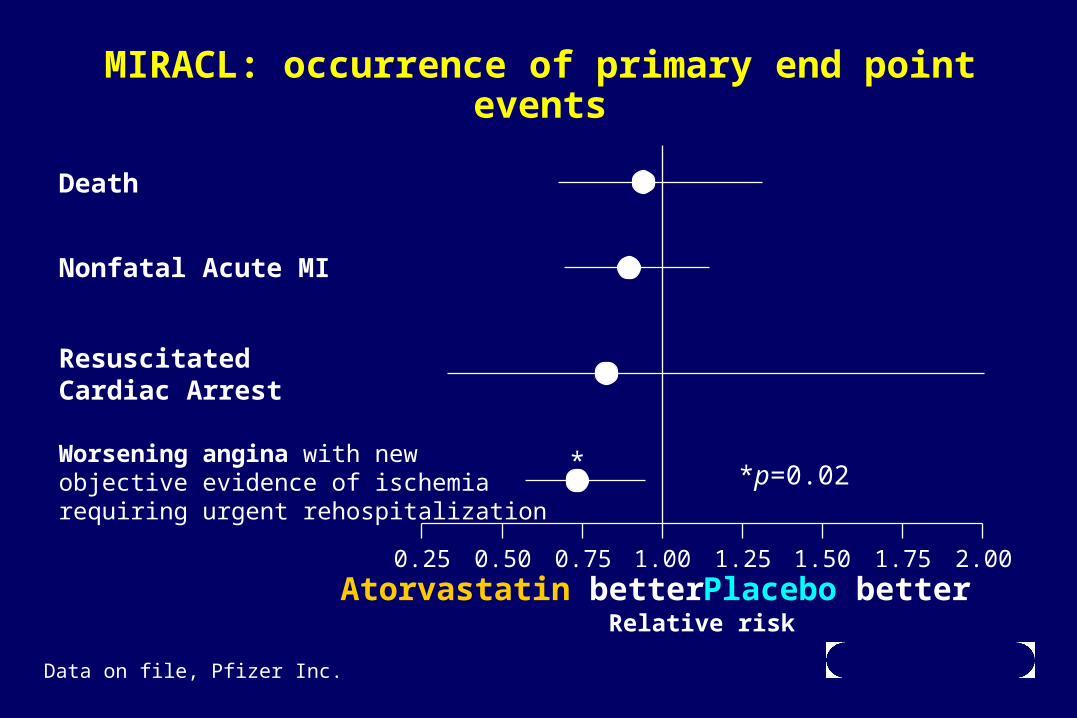
MIRACL: occurrence of primary end point events
*p=0.02
0.25 0.50 0.75 1.00 1.25 1.50 1.75 2.00Atorvastatin better Placebo better
Relative risk
Death
Nonfatal Acute MI
ResuscitatedCardiac Arrest
Worsening angina with newobjective evidence of ischemiarequiring urgent rehospitalization
*
Data on file, Pfizer Inc.

* Patients may experience more than one revascularization and/or more than one secondary clinical end point.
† p=0.045 vs placebo; ‡ p=0.021 vs placebo
MIRACL: occurrence of secondaryclinical end points
Placebo AtorvastatinSecondary end point [n (%)] (n=1548) (n=1538)
Revascularization* 250 (16.1) 254 (16.5)Catheter based 143 (9.2) 150 (9.8)CABG 110 (7.1) 106 (6.9)
Fatal + Nonfatal Stroke 24 (1.6) 12 (0.8)†
Nonfatal stroke 22 (1.4) 9 (0.6)‡
New or worsening CHF 43 (2.8) 40 (2.6)Worsening angina w/o new objectiveevidence of ischemia 106 (6.8) 91 (5.9)
Data on file, Pfizer Inc.
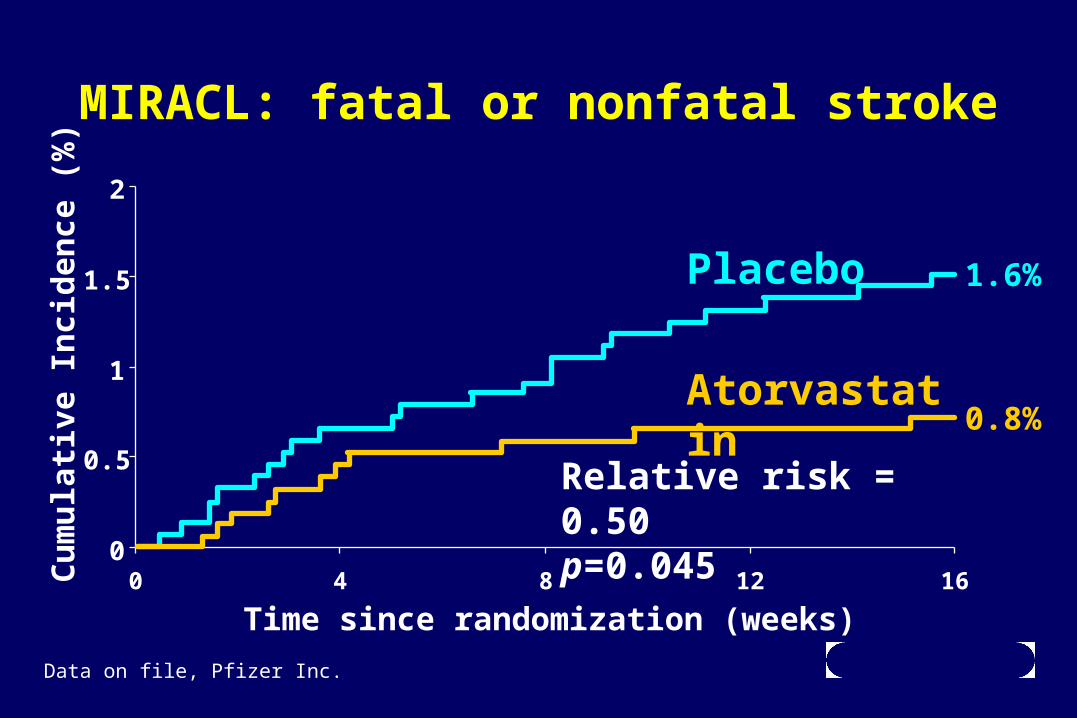
MIRACL: fatal or nonfatal stroke
0
0.5
1
1.5
2
0 4 8 12 16
Time since randomization (weeks)
Cu
mu
lati
ve I
nci
den
ce (
%)
Relative risk = 0.50p=0.045
Atorvastatin
Placebo 1.6%
0.8%
Data on file, Pfizer Inc.

MIRACL: compliance with intended treatment
Placebo Atorvastatin(n=1548) (n=1538)
Mean duration of compliance 99 days 98 days
Premature discontinuation 10.3% 11.2%
Reasons for discontinuation:nonfatal AE 1.5% 2.1%nonfatal ischemic event 0.6% 0.5%other 8.2% 8.6%
No. of patients lost to follow-up 4 8
Data on file, Pfizer Inc.
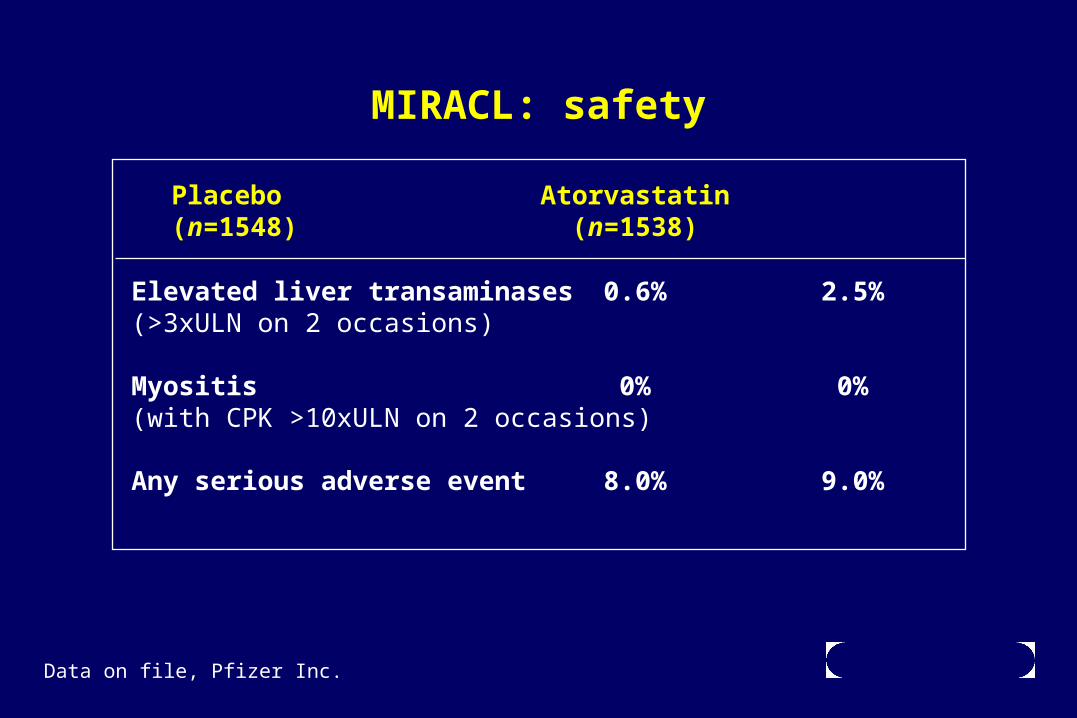
MIRACL: safety
Placebo Atorvastatin(n=1548) (n=1538)
Elevated liver transaminases 0.6% 2.5%(>3xULN on 2 occasions)
Myositis 0% 0%(with CPK >10xULN on 2 occasions)
Any serious adverse event 8.0% 9.0%
Data on file, Pfizer Inc.

MIRACL: conclusions
• Early, rapid, and profound cholesterol lowering therapy with atorvastatin reduced early recurrent ischemic events in patients with unstable angina or non-Q-wave acute MI
• Atorvastatin reduced the incidence of recurrent ischemic events within 16 weeks
• Treatment was generally well tolerated
Data on file, Pfizer Inc.