2-ischemia 1

of 12
-
Upload
abdallah-essam-al-zireeni -
Category
Documents
-
view
228 -
download
0
Transcript of 2-ischemia 1
-
8/2/2019 2-ischemia 1
1/12
CVS disordersPage 1
CVS disordersaboutisToday's lecture
:)1(Ischemia
Anatomical and Physiological Introduction:-
Heart arteries are mainly 2 and they arise from the
ascending aorta (which is the largest art. In human) and
supply the myocardium with oxygenated blood:
1- Left Coronary art. Divides into:
-anterior interventricular branch.
-circumflex branch.
2- Right Coronary art. Divides into:
- posterior interventricular branch.
-marginal branch (left and right).
Drainage of veins through the Coronary sinus (a
vascular sinus which is a thin-walled sinus with no
smooth muscles) which drains the blood to the
right atrium.
(Note: that these arteries or this system of arteries
oS.vascularity of the heartreferred to as theis
thatswhy we explained them to get the idea about
how ischemia occurs).
Normal coronary blood flow:
The resting coronary blood flow= 225ml/min
-
8/2/2019 2-ischemia 1
2/12
CVS disordersPage 2
(Relaxed situation e.g: sleeping)
In strenuous exercise = increase three to
four folds.
(Sometimes up to 7 folds)
Now the question is, when does perfusion
occur? during the systole or the diastole?
Systolic pressure is created from the
contraction of the left ventricle (phase of
contraction).
Diastolic pressure is created from the
recoil of the aorta (phase of relaxation).
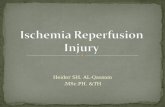
During systole: arteries (the
subendocardial arteries) of the heart willofperfusionso most of thebe compressed
.diastoleoccurs duringheart
As you see in the following diagram:
Systole BF is 100 ml/minute.
-
8/2/2019 2-ischemia 1
3/12
CVS disordersPage 3
Diastole BF is 300 ml/minute.
What controls the coronary blood flow and all
arteries of the body in general?
The need or the increased demand that increases
the blood supply.
if there's imbalance between the supplyOtherwise (
ae demand) it's going to be consideredand th
Ischemia.which is called(defect )disorder
Blood flow is controlled mainly by:-
Metabolic (activities) regulation: if it is increased then
the BF will increase. (Blood flow through the coronary
system is regulated almost entirely by local arterial
vasodilatation in response to cardiac muscles' needfor nutrients which leads to increased contraction so
there will be an Increase in the rate of coronary
blood flow).
Nervous regulation: sympathetic stimulationincreases the heart rate and contractility, so it will
increase the cardiac output which means increased
coronary blood flow.
-
8/2/2019 2-ischemia 1
4/12
CVS disordersPage 4
Now let us start with pathophysiology:-
:Ischemia
There are two important subjects placed
under or related to ischemia generally:
-Ischemia.
-Necrosis.
Now what do we mean by Ischemia?
It's the lack of oxygen due to inadequate perfusion
of the myocardium, which causes imbalance
between oxygen supply and demand.
Specifically: when there's a constriction, a
narrowing or a subdivision (partial occlusion) in
the arteries which supply the heart (coronary
arteries).
The other part is necrosis (myocardial infarction):
When there's complete occlusion of the blood
vessel (not partial).
Then the myocytes beyond the occlusion will die
and it might be fatal (this leads to a state of
necrosis).
-
8/2/2019 2-ischemia 1
5/12
CVS disordersPage 5
Ischemia equation :
e.g u need 10 liters, and
blood supplies only 8 liters (this leads to ischemia).
-Causes of myocardial ischemia:
The most common cause is Coronary atherosclerosis
(This means blockage of arteries):
Thickening or narrowing of the wall of the arteries
due to accumulation of fatty materials such as
cholesterol (most common in old people).
Epicardial coronary arteries are the major site.
Major risk factors that cause atherosclerosis
(precipitating factors):
Increase in LDL (low density lipoprotein). Decrease in HDL (high density lipoprotein). Cigarette smoking. Hypertension. DM (Diabetes mellitus).
*Additional note: low density lipoprotein means bad cholesterol and HDL means good
cholesterol.
-
8/2/2019 2-ischemia 1
6/12
CVS disordersPage 6
We all know that smoking, hypertension, etc are
common causes, but what is the mechanism?
Because all these things lead to destruction or injury tothe endothelial (has to be smooth) layer of the arteries
which leads to aggregation of clotting factors (platelets)
due to the fragility of its surface (no luminar flow).
This mechanism is similar to getting injured or having an
external cut, this leads to rough (fragile) surface and
aggregation of clotting factors.*remember that a blood vessel consists of 3 layers: tunica interna (endothelial), tunica
media, tunica externa.
*there are 2 type of blood flow: luminar flow (steady or smooth state) and turbulent
flow.
Normal function of vascular endothelium:-Local control of vascular tone.
-Maintenance of an anticoagulant surface.-Defense against inflammatory cells.Loss of these defensesleads to:-Inappropriate constriction.
-Luminal clot formation.-Abnormal interactions with blood monocytes &
platelets.
- Now the occlusion is caused either by Thrombosis or
Embolism, but what the difference?
-
8/2/2019 2-ischemia 1
7/12
-
8/2/2019 2-ischemia 1
8/12
CVS disordersPage 8
The Location of the obstruction Influences the quantity
of myocardial ischemia, Determines the severity of the
clinical manifestations which means that if the occlusion
was in a major artery then the effect will be major (the
heart will be affected so much, massive destruction of
cells leads to massive dead myocytes) but if the artery is
small the complication will be less (why? Because there
are fewer amounts of dead cells).Collateral circulation:
Before that there's a question: If a young man had a
myocardial infarction he would die but an old or a
middle- aged man wouldn't?
Due to the collateral circulation that is only formed
in old people and athletes.
Which means that an area (the same one) supplied
by many arteries (network of blood vessels), it is
not opened in young people (except athletes) but
opens when we get older.
*in athletes because they have a high demand
(cardiomegaly).
-
8/2/2019 2-ischemia 1
9/12
CVS disordersPage 9
If heart rate is less than 60 it's a disorder which is
called brady cardi but in athletes it's not (their heart
size is larger = cardiomegaly) normal to have HR
-
8/2/2019 2-ischemia 1
10/12
CVS disordersPage 10
3) Cell membrane function:
-Leakage of potassium and uptake of sodium by
myocytes.4) Electrical function:-ECG changes:Repolarization abnormalities.Transient ST segment depression.
-Electrical instability:Ventricular tachycardia and fibrillation.
Later on when we discuss arrhythmia we will know
that one of its important causes is ischemia and
massive myocardial infarction (it may lead toventricular fibrillation which is fatal).
-angina
There are 2 types:
-unstable angina:
which is misdiagnosed betweenunstable angina and acute MI (myocardial infarction)
both of them are Acute coronary syndromes (symptoms:
retrosternal severe chest pain near to the left hand).
We can differentiate between them by ECG, we have to
do blood tests, ckmp, troponine (will be +ve for MI
-
8/2/2019 2-ischemia 1
11/12
CVS disordersPage 11
patients andve for unstable angina patients) next lecture
we will discuss it in details.
-Stable angina: chronic artery disease.Characteristics:Heaviness, Pressure, Squeezing,Smothering and choking pain.
Causes:
-CAD (coronary artery disease).- Aortic valve disease.
- Hypertrophic cardiomyopathy.
History:
A man > 50 years.
A woman > 60 years.
Pain with physical & emotional exertion.
Lasts to 5-10 min (relieved by vasodilators).
But how does the pain occur or start? Radiating pain to the left
shoulder, both arms, back, interscapular region, root of the neck,
jaw and teeth. but you need to know any other symptoms that
are not related to the heart in diagnosing angina or MI
-
8/2/2019 2-ischemia 1
12/12
CVS disordersPage 12
(e.g abdominal pain) otherwise, you might kill the patient
because you will forget or misdiagnose that he has angina and
you will give him another treatment for another disease (that
you had in mind).
Both types have the same cause (narrowing and
constriction of the coronary artery) but the stable is
relieved by Vasodilators (nitro-peceline sublingual,
nitrates, -adrenergic blockers, Calcium, antagonists and
Antiplatelet drugs). Occurs mainly after doing exercises
especially when the demand becomes more than thesupply, which leads to a severe chest pain but signs and
symptoms will be subsided by Vasodilators. But in
unstable pain will not be subsided by Vasodilators.
*tread-mill or stress test: to know if your heart is doing well (220- the
age) e.g ( your age is 20 then 220-20=200 this means that your HR after
doing exercises should reach 200 without feeling any chest pain
otherwise there would be a disorder).
Why are these patients given analgesics (morphine or opium) or
as we call them painkillers?
Because the heart pain is very severe (painful).
THE END