Chronic limb ischemia
11
CHRONIC LOWER LIMB ISCHEMIA
-
Upload
dr-slayer -
Category
Health & Medicine
-
view
184 -
download
5
Transcript of Chronic limb ischemia
CHRONIC LOWER LIMB ISCHEMIA
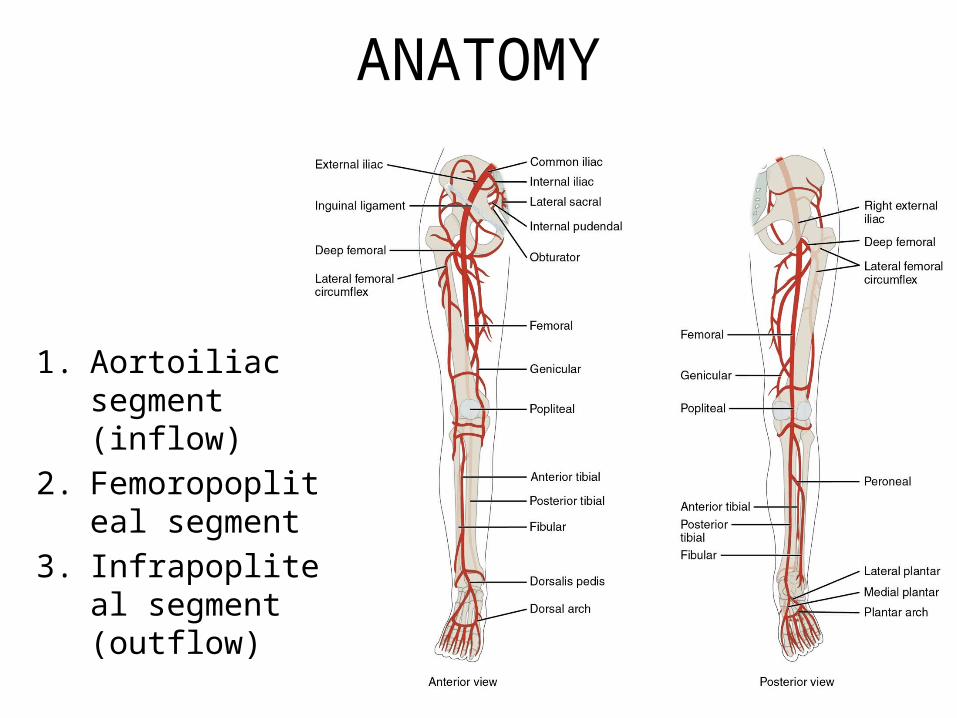
ANATOMY
1. Aortoiliac segment (inflow)
2. Femoropopliteal segment
3. Infrapopliteal segment (outflow)
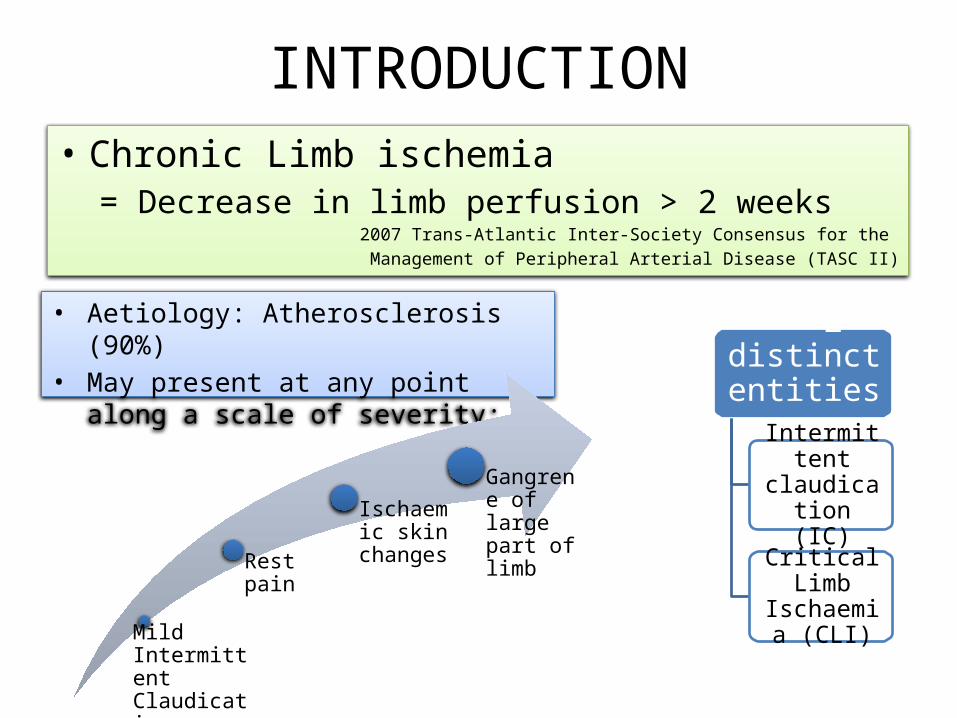
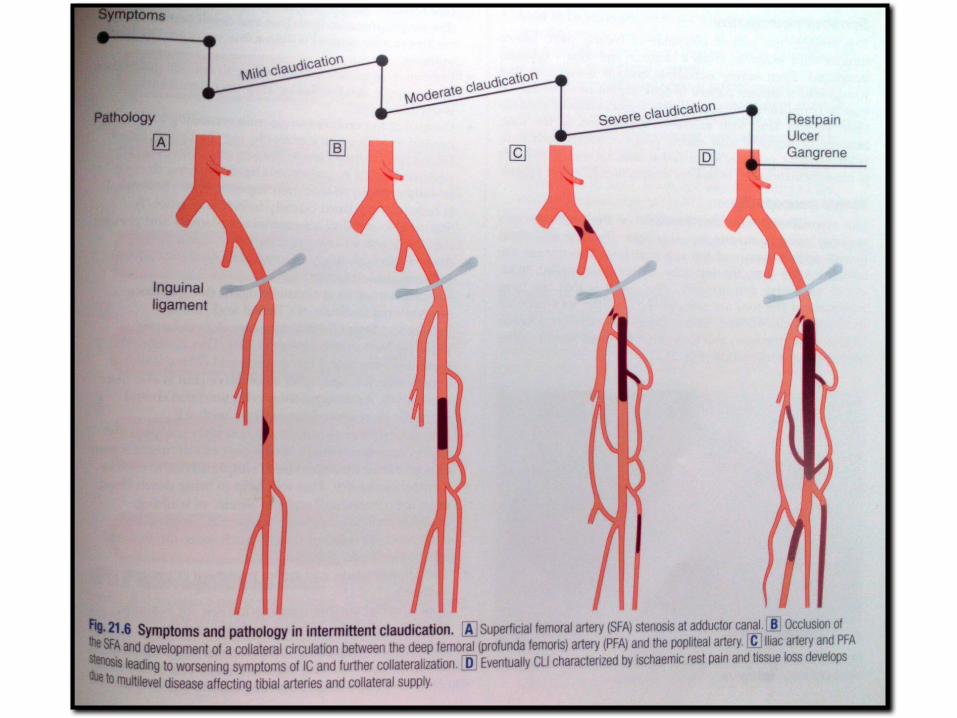
INTRODUCTION• Chronic Limb ischemia
= Decrease in limb perfusion > 2 weeks2007 Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II)
• Aetiology: Atherosclerosis (90%)• May present at any point along a scale of
severity:
Mild Intermittent Claudication
Rest pain
Ischaemic skin changes
Gangrene of large part of limb
** 2 distinct entities:
Intermittent claudication
(IC)
Critical Limb Ischaemia
(CLI)
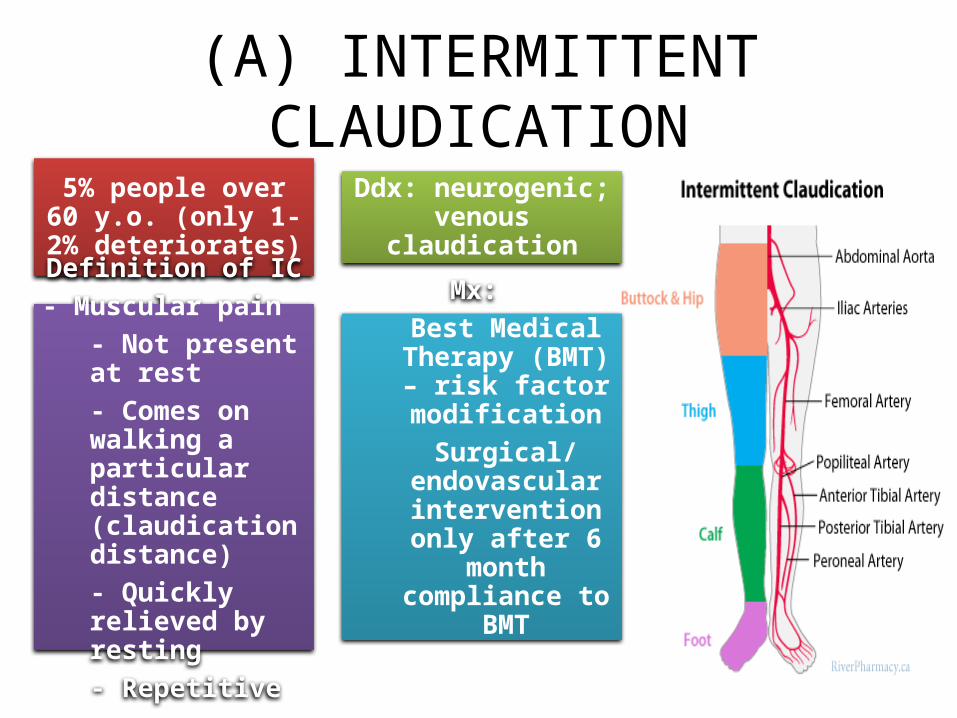
(A) INTERMITTENT CLAUDICATION5% people over 60 y.o.
(only 1-2% deteriorates)
Ddx: neurogenic; venous claudication
Definition of IC- Muscular pain
- Not present at rest- Comes on walking a particular distance (claudication distance)- Quickly relieved by resting- Repetitive
Mx: Best Medical
Therapy (BMT) – risk factor
modificationSurgical/
endovascular intervention only
after 6 month compliance to BMT
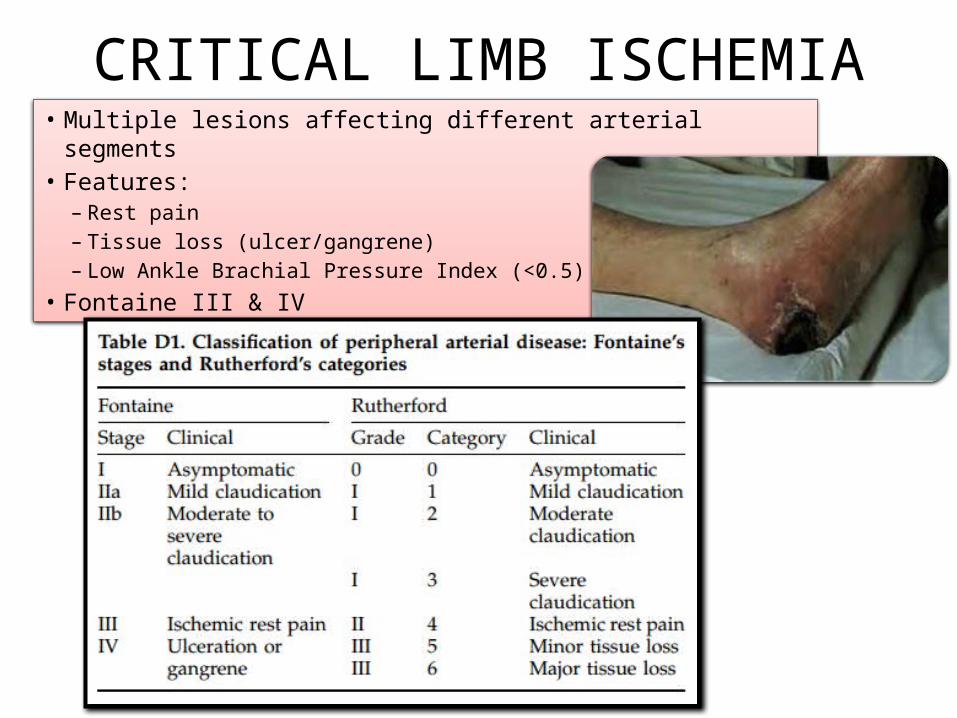
CRITICAL LIMB ISCHEMIA• Multiple lesions affecting different arterial segments• Features:
– Rest pain– Tissue loss (ulcer/gangrene)– Low Ankle Brachial Pressure Index (<0.5)
• Fontaine III & IV
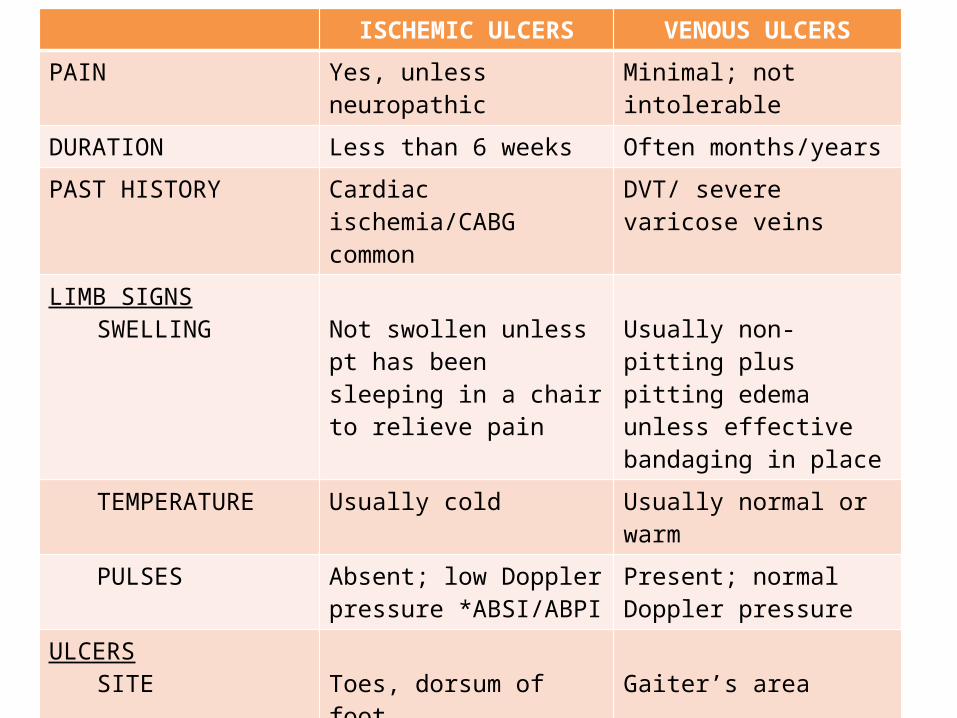
ISCHEMIC ULCERS VENOUS ULCERS
PAIN Yes, unless neuropathic Minimal; not intolerable
DURATION Less than 6 weeks Often months/years
PAST HISTORY Cardiac ischemia/CABG common
DVT/ severe varicose veins
LIMB SIGNSSWELLING Not swollen unless pt has
been sleeping in a chair to relieve pain
Usually non-pitting plus pitting edema unless effective bandaging in place
TEMPERATURE Usually cold Usually normal or warm
PULSES Absent; low Doppler pressure *ABSI/ABPI
Present; normal Doppler pressure
ULCERSSITE Toes, dorsum of foot Gaiter’s area
MARGIN Punched out Irregular with blue margin & growing epithelium
BASE Destroy deep fascia & may expose tendons, with poor granulation
Beefy red, shallow and never penetrate deep fascia, pale granulation tissue
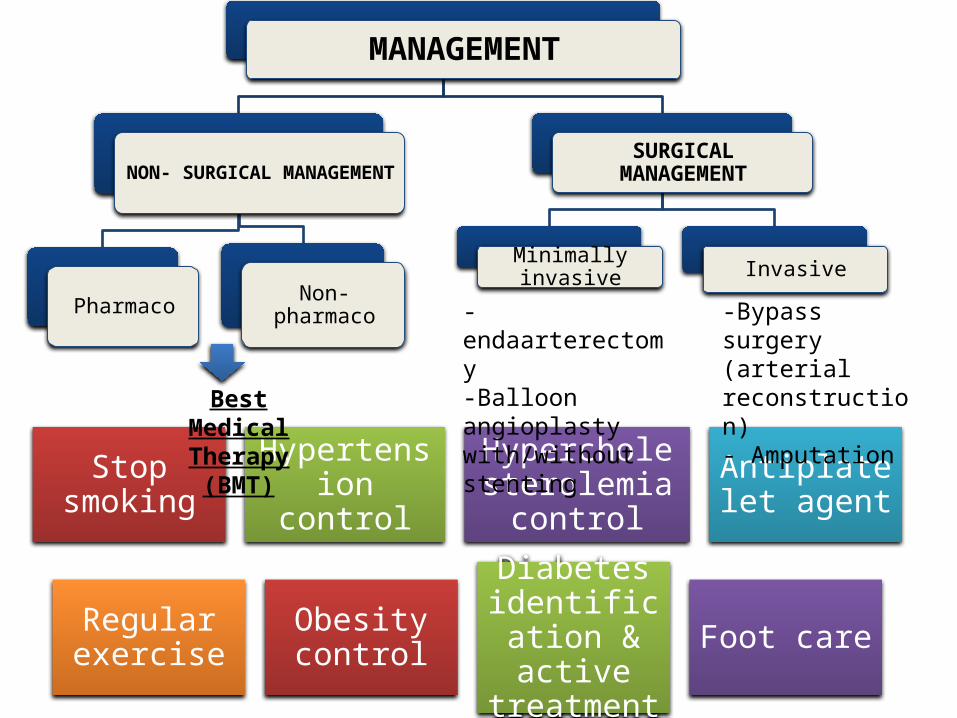
MANAGEMENT
NON- SURGICAL MANAGEMENT
Pharmaco Non-pharmaco
SURGICAL MANAGEMENT
Minimally invasive Invasive
Stop smoking
Hypertension control
Hypercholesterolemia control
Antiplatelet agent
Regular exercise
Obesity control
Diabetes identification
& active treatment
Foot care
Best Medical Therapy (BMT)
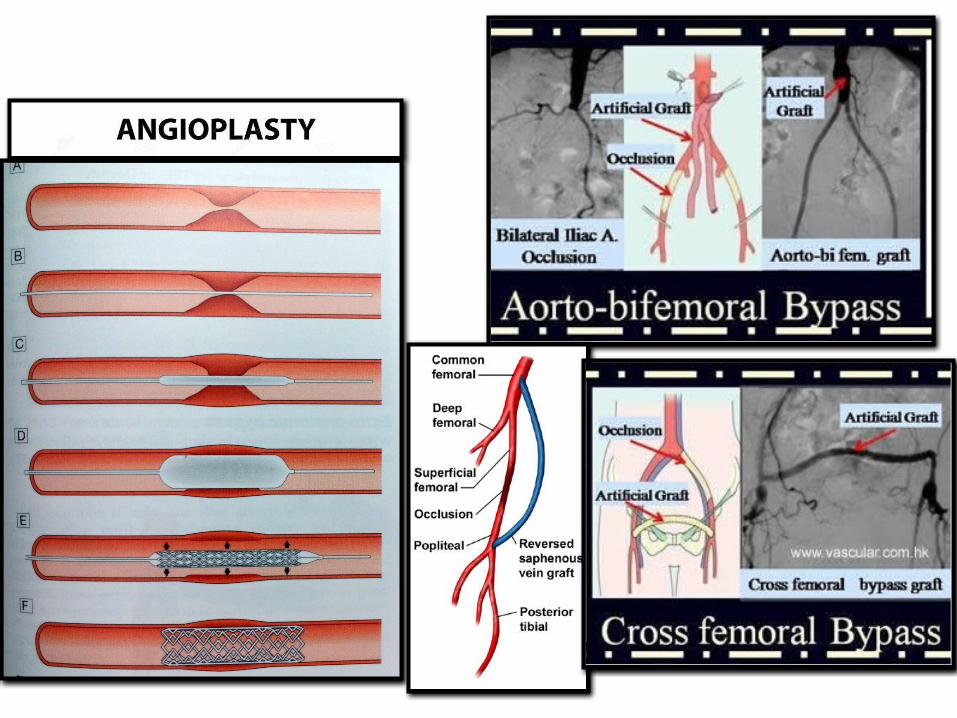
-endaarterectomy-Balloon angioplasty with/without stenting
-Bypass surgery (arterial reconstruction)- Amputation
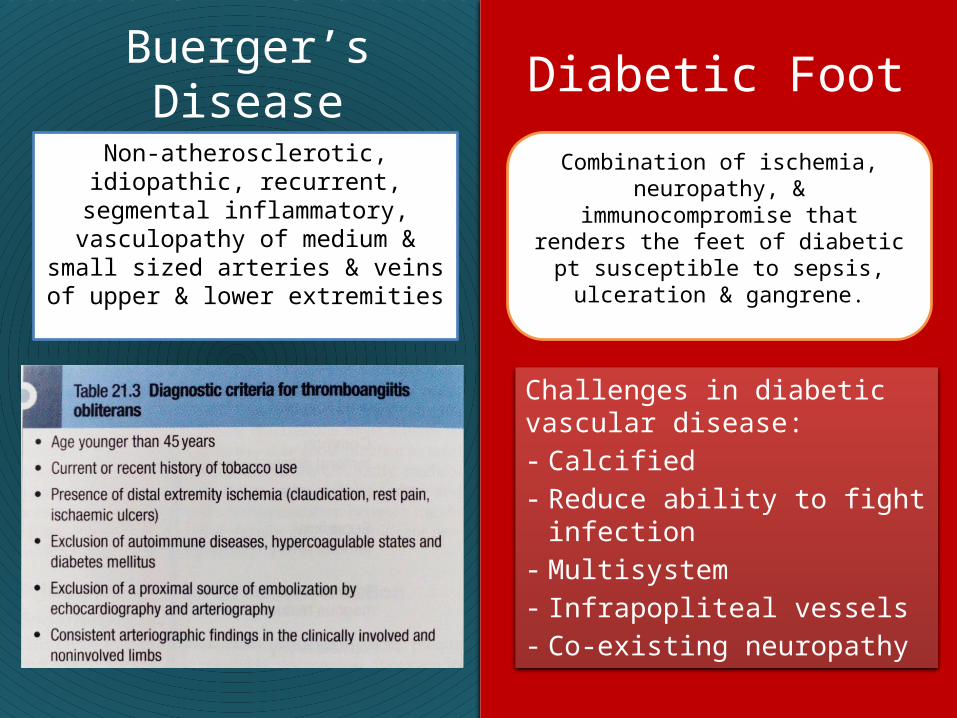
Buerger’s DiseaseNon-atherosclerotic, idiopathic,
recurrent, segmental inflammatory, vasculopathy of
medium & small sized arteries & veins of upper & lower extremities
Diabetic FootCombination of ischemia,
neuropathy, & immunocompromise that renders the feet of diabetic pt susceptible to sepsis, ulceration & gangrene.
Challenges in diabetic vascular disease:- Calcified- Reduce ability to fight infection- Multisystem - Infrapopliteal vessels- Co-existing neuropathy
REFERENCES• Principles & Practice of Surgery• Essentials Surgery• Inter-Society Consensus for the Management of Peripheral Arterial
Disease (TASC II), L. Norgren et. al., Eur J Vasc Endovasc Surg Vol 33, Supplement 1, 2007
• Review Articles: Critical limb ischemia, Varu et. al., Journal of Vascular Surgery, 2010
• Chronic lower limb ischemia, J.D. Beard, BMJ 2000