Medicaid Waiver Update Health Care Appropriations Subcommittee January 11, 2012

MMIS Report Joint Appropriations
Subcommittee on Health and Human Services
March 14, 2013
Ed Riley
Associate Program Director
Contract Manager
NC DHHS Office of MMIS Services
Paul Guthery
Associate Program Director
Senior Program Manager
NC DHHS Office of MMIS Services

NCMMIS Program Purpose Replacement MMIS Project (NCTracks)
◦ Design, develop and install a componentized, integrated, multi-payer Replacement Medicaid Management Information System (MMIS) and Fiscal Agent operations
◦ Facilitate provider enrollment and consolidate claims processing activities for multiple DHHS health plans Division of Medical Assistance – Medicaid & Health Choice Division of Mental Health, Developmental Disabilities, and Substance Abuse Services Division of Public Health Office of Rural Health and Community Care
◦ Coordinate processing among the payers to ensure the proper assignment of the payer, benefit plan, and pricing methodology for each service on a claim
3/14/2013 2 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

NCMMIS Program Purpose Reporting & Analytics Project
◦ Design, develop and install a state-of-the-art Data Warehouse, and reporting solution that meets not only current DHHS needs, but provides a platform for changes leading to future growth with enhanced self-service by the end-user community
◦ Surveillance Utilization Review System (SURS) – Detection of fraud and abuse
◦ Decision Support System (DSS) – Healthcare data analytics to empower more informed policy decisions
3/14/2013 3 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

NCMMIS Program Purpose Business Process Automation System Project
◦ Identify and execute the procurement and implementation of a Business Process Automation System and associated business services for the DHHS Division of Health Service Regulation (DHSR)
◦ Satisfy the information sharing requirements with the Replacement MMIS in the area of provider eligibility
◦ Provide automation, using a common database, to support the business functions of DHSR
Certificate of Need
Construction
Licensure and Certification
Health Care Personnel Registry
Center for Aide Regulation and Education
3/14/2013 4 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Advantages of the Replacement MMIS Multi-payer system consolidating claims processing for multiple
DHHS divisions, ensuring the proper assignment of payer, health plan, benefit plan, and pricing methodology for each claim line
Provider Web Portal ◦ Provider Enrollment
◦ Changes to Provider enrollment information
◦ Recipient Enrollment and Service Limits
◦ Electronic Claims Submission
◦ Fee Schedules and Rates
◦ Prior Approval Inquiry and Request
◦ Claims Status Information
◦ Retrieval of Remittance Advices
◦ Online access to training information
3/14/2013 5 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services
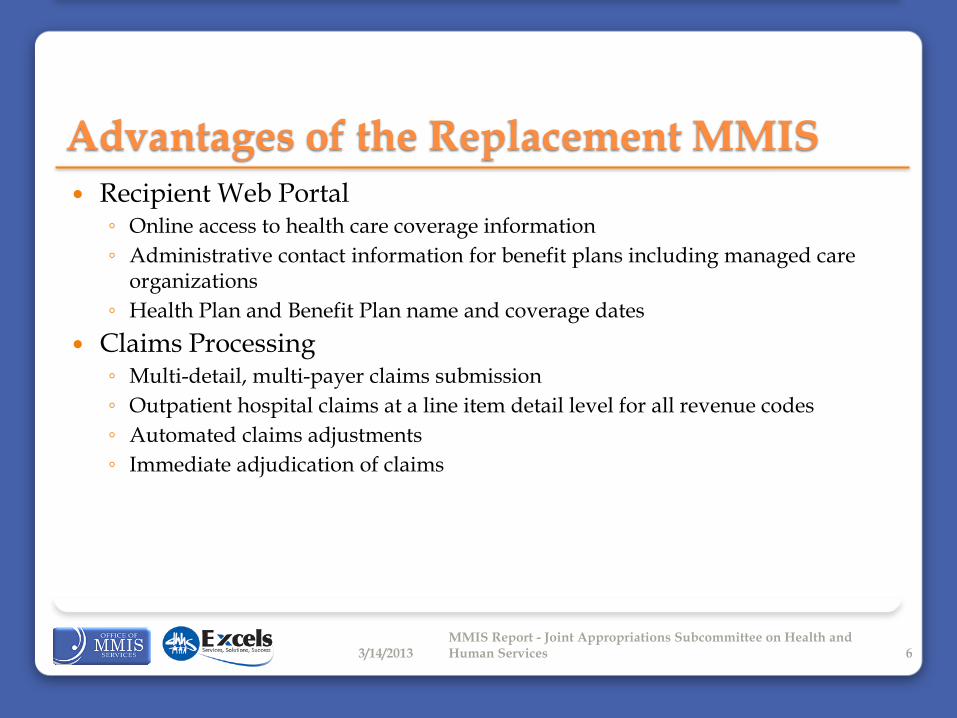
Advantages of the Replacement MMIS Recipient Web Portal
◦ Online access to health care coverage information
◦ Administrative contact information for benefit plans including managed care organizations
◦ Health Plan and Benefit Plan name and coverage dates
Claims Processing ◦ Multi-detail, multi-payer claims submission
◦ Outpatient hospital claims at a line item detail level for all revenue codes
◦ Automated claims adjustments
◦ Immediate adjudication of claims
3/14/2013 6 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

MMIS Legacy System Synchronization Modifications to the legacy solutions continued after the system
freeze date
Limitations to the level of change that can be made to the system once final testing began while maintaining quality ◦ System soft freeze began on March 2, 2012 – Hard freeze began on May 31, 2012
◦ User Acceptance Testing (UAT) began August 29, 2012
◦ Changes approved after freeze date not available for current UAT
3/14/2013 7 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

MMIS Legacy System Synchronization CSC Contract Amendment #3 created to allow for the development
and testing of the most critical of these changes ◦ Additional capacity for change allocated
◦ Move Operational Readiness Date from March 1, 2013 to July 1, 2013 to accommodate additional Medicaid changes
◦ Maintain July 1, 2013 Operational Start
◦ Use capacity originally allocated to ICD-10 (International Classification of Diseases 10th
Revision)
Federally required compliance date moved from October 1, 2013 to October 1, 2014
Work continues on ICD-10 in preparation for system changes
◦ Additional Final Integration and User Acceptance Testing Period
April / May 2013
Overlap additional testing with the execution of Provider Operational Preparedness (POP)
3/14/2013 8 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

MMIS Legacy System Synchronization Additional Synchronization Gap Less Critical Functionality
◦ Additional CSRs are currently in the CSC backlog to be implemented that will not be addressed by July 1, 2013
◦ The first two post operational start software releases are scheduled for:
October 1, 2013
January 1, 2014
◦ Workarounds required until the implementation of functionality
3/14/2013 9 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Workarounds Strategy Workgroup currently developing workarounds for 288 change
requests ◦ 120 Customer Service Requests (CSRs)
◦ 168 State Memoranda
The workaround strategies can be broadly grouped by the following categories:
Change policy, business rules, and/or claims filing instructions
Manual intervention performed by CSC, the State, or other vendor
Pay and chase or report
Monitor impacts
Cancel original change request
Suspend specific task in Division operations
Workgroup to complete identification of workarounds by March 18
Work beginning to define impacts and communications
3/14/2013 10 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Replacement MMIS Schedule
System Hard Freeze
Items added or extended ffected by Contract Amendment 3 shown in crosshatched shading
Fiscal Agent Operations
Sep Oct Nov Dec
2012
Feb Mar Apr May Jun Jul Aug
2013
JulJan Sep Oct Nov Dec
Additional UAT
Aug
PST Extended
UAT Extended
Mar Apr May JunFeb Nov Dec
2014
May Jun Jul Aug Sep OctJan Feb Mar Apr
Target for 2nd Release
Target for 1st Release
Build System Integration Testing
Additional Final Integration
Test (FIT) / PST
Provider Operational
Preparedness
UAT for
Providers
Production Simulation Testing
(PST)
User Build Acceptance Test (UBAT)
System Soft Freeze
FIT
FSIT
User Acceptance Testing
BSIT
CMS Certification
3/14/2013 11 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

User Acceptance Test (UAT) Results User Acceptance Test Cases Completed by the State: 1,980
Test Cases with no outstanding defects: 1,751 (88.4%)
Total defects discovered during UAT: 1,520 ◦ Initial UAT period (8/29/2012 – 1/16/2013)
Severity Exit Threshold
Discovered Resolved Open
1. System-wide Failure 0 33 33 0
2. Inconsistent Results 10% (83) 839 761 78
3. Workaround Exists 25% (134) 537 452 85
4. Cosmetic n/a 96 51 45
5. Working as Designed n/a 15 1 14
Total n/a 1,520 1,298 222
3/14/2013 12 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Overall Program Budget
3/14/2013 13 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Vendor Cost Savings - MMIS Over the five year operations & maintenance phase, the CSC
contract cost will save on average $3 million per month over expected future costs of existing contracts that will be retired when NCTracks is implemented.
The state appropriations savings over that same five year period is expected to average over $900,000 per month.
Systems to be retired by NCTracks: ◦ MMIS – HP
◦ IPRS – HP
◦ Pharmacy Prior Authorization Call Center – Xerox
◦ Smart PA – Xerox
◦ POMCS– DHHS
3/14/2013 14 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

CSC Contract - MMIS
Vendor Amendment Cost State Share
CSC
Development1 Base 77,960,715$ 9,901,010.81$
Ops & Maintenance Base 187,243,759$ 51,023,924.33$
Development Amend # 1 -$ -$
Ops & Maintenance Amend # 1 -$ -$
Development Amend # 2 152,754,523$ 18,025,033.71$
Ops & Maintenance2 Amend # 2 66,921,800$ 18,236,190.50$
Development Amend # 3 N/A N/A
Ops & Maintenance Amend # 3 N/A N/A
Total
Development 230,715,238$ 27,926,045$
Ops & Maintenance 254,165,559$ 69,260,115$
NCMMIS+ ProgramContract Amendments
1 Although not included in the initial contract; $ 22M was budgeted for changes
and approved by CMS. 2 Two additional years of operations were added to the contact.
3/14/2013 15 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Program Risks and Issues Based on analysis by an outside consultant, Susan Young, the following risks and
mitigation strategies have been identified:
Risk Mitigation Strategy
Stakeholder Engagement A supplementary communications approach has been developed and a resource allocated to integrate the specific plans into the overall program and management routines
Program Planning, Execution and Monitoring
The MMIS Program has now been aligned under the DHHS CIO, and availability of critical resources has been secured
Organizational Change Enablement
An external consultant will be engaged to drive our development of Division business processes and facilitate additional preparations for user testing and transition
Change Management A hard freeze has been placed on further changes to the legacy and new systems. A team has been formed to identify gaps and define interim processes
Overall Implementation Strategy
Resources will be reallocated to support deployment planning efforts and bring focus to the most significant levers for the success of the initiative.
Test Planning and Execution Critical resources to support testing cycles have been secured. Additional business process activities will make user testing and readiness assessments more effective
3/14/2013 16 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Program Risks and Issues As reported by CSC in their 2/14/2013 report to the NCMMIS+ Steering Committee
Risk Mitigation Strategy
Provider Conversion A number of data quality issues have been identified during PST and UAT that impact claims adjudication. The State and CSC have made good progress. 2 outstanding issues remain, 3 issues require data clean up and one potential workaround has been identified
Taxonomy The current design requires a taxonomy at level 3 for professional providers and some may have credentials only to a level 2. CSC has determined the effort required to make the required modifications and will work with the State to determine how to implement by operational start.
Interfaces CSC is still working through interface files from the State so end to end testing can occur during the extended PST. 8 interfaces will be tested during the May PST.
Legacy CSR Workarounds There are approximately 120 Legacy CSRs and 168 State memoranda that will not be in NC Tracks at operational start. OMMISS and DMA are evaluating the workarounds with a 3/18/2013 completion target. Any impact to CSC operations must be reviewed and determined after that date.
3/14/2013 17 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Appendix
3/14/2013 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services 18

CMS Certification Review of the MMIS and operations
◦ CMS Certification Checklists
State requests certification after the closeout of two fiscal quarters ◦ Operational start on July 1, 2013
◦ North Carolina can request certification after closing out the quarter ending December 31, 2013
Following the request, CMS and the State begin planning one week on-site certification review ◦ Document collection and preparation
One week on-site visit typically at least one year after operational start
Based on the information collected, CMS may issue findings and require the State to take remedial action
3/14/2013 19 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

CMS Certification Financial Impact
◦ On the first day of operations, the Federal match for operations is 50%
◦ Upon certification the Federal match for operations improves to 75%
◦ When certification is achieved, the difference between the 50% and 75% Federal match is paid retroactively back to the day the system is deemed by CMS to be the system of record
3/14/2013 20 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Testing Participation CSC Staff
◦ Build System Integration Testing
◦ Final Integration Testing
◦ Final System Integration Testing
◦ Production Simulation Testing
OMMISS Staff ◦ User Build Acceptance Testing
◦ User Acceptance Testing
◦ Review of CSC Conducted Testing
Division Testing ◦ 46 participants from the DHHS divisions
◦ Participants from DMA, DMH/DD/SAS, DPH
3/14/2013 21 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Testing Participation Providers
◦ User Acceptance Testing for Providers
◦ Worked with 25 Provider Associations for nominees
◦ 37 Providers nominated by 8 associations participated over six weeks
3/14/2013 22 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Transition Planning Deployment Planning Approach
Iteration Content
Initial Framework (Delivered 11/26/2012)
Establishes the concept, structure, and layout of the deliverable, with a focus on the introductory information, high-level activity/task and schedule definition, establishment of assumptions and constraints, templates and integration with related documents.
Iteration 2 (Delivered 2/15/2013)
Focuses on the detailed rollout and deployment schedule/activities, post deployment activities, organization rolls and responsibilities, continued refinement of assumptions and constraints, populating the templates, and details of the back out plan.
Iteration 3 (Delivery 3/31/2013)
Continued expansion of the detailed rollout and deployment schedule/activities, expansion of the post deployment activities, finalization of the organization rolls and responsibilities, continued refinement of assumptions and constraints, continued refinement of the back out plan details.
Final Iteration (Delivery 5/31/2013)
Wrap-up of the detailed rollout and deployment schedule/activities, wrap-up of the post deployment activities, wrap-up of assumptions and constraints, wrap-up of the back out plan details.
3/14/2013 23 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Budget Update Overall Program Budget and Budget for Each Project
◦ Initial
◦ Current
◦ Reasons for Changes
◦ Operations and Maintenance Costs
◦ Sources of Funding
3/14/2013 24 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Replacement MMIS Budget
3/14/2013 25 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Reason for Changes to the Replacement MMIS Budget 1. Schedule slipped 22 months; functionality has been added.
Reasons for slippage: • Over estimation of the degree of fit with the baseline solution from CSC
• Estimated 73% reuse – Realized 32% reuse
• Approximately 200 legacy change requests that were not included in the original scope were added to the design
• Federal Scope Expansion:
• HIPAA 5010
• ICD-10
• National Correct Coding Initiative (NCCI)
• Healthcare Reform
• State Legislation: SL 2010 and SL 2011 changes
• Added four months of Provider Operational Preparedness
3/14/2013 26 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Reason for Changes to the Replacement MMIS Budget 2. Added 22 months to the development phase impacting the
Independent Verification and Validation (IV&V) and Testing vendors’ contracts; and internal labor and project support costs
3. Revised estimate of the resources needed to manage vendors and to begin the next MMIS procurement cycle
4. Added 22 months to early operations (provider enrollment, credentialing and verification) and for drug utilization review; also realized a larger number of providers enrolling in Medicaid
3/14/2013 27 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Reporting & Analytics Budget
3/14/2013 28 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Reason for Changes to the Reporting & Analytics Budget 1. Due to the MMIS project being extended 22 months, the R&A
project needed to be extended as R&A is dependent upon data from the Replacement MMIS. Also developed and implemented the Surveillance Utilization Review System (SURS) to operate with legacy data
2. Added 22 months to the development phase impacting IV&V and Testing vendor contracts
3. Although the development phase was extended, the staffing level required to support this R&A project was initially overestimated
3/14/2013 29 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Business Process Automation System (BPAS) Budget
Initial Current Reason Federal State Share
Development 6,167,739$ 8,565,102$ 4,697,413$ 3,780,389$
Vendor Costs
GLS 4,205,970$ 4,205,970$ 2,102,985$ 2,102,985$
IV&V and Testing 174,601$ 174,601$ 87,301$ 87,301$
Internal Costs 1,787,168$ 4,184,531$ 1 2,507,127$ 1,677,404$
Ops & Maintenance 6,119,699$ 8,119,699$ -$ 8,119,699$
Vendor Costs 4,846,779$ 4,846,779$ -$ 4,846,779$
Internal Costs 1,272,920$ 3,272,920$ 1 -$ 3,272,920$
Total 12,287,438$ 16,684,801$ 4,697,413$ 11,900,088$
Business Process Automation System (BPAS) Project
Budget
3/14/2013 30 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Reason for Changes to the BPAS Budget 1. Staffing levels were initially underestimated and required
hardware and software was omitted from the initial budget
3/14/2013 31 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Program Level Project
Initial Current Reason Federal State Share
Development 9,721,297$ 15,803,746$ 13,828,278$ 1,975,468$
Vendor Costs -$
Internal Costs 9,721,297$ 15,803,746$ 1 13,828,278$ 1,975,468$
Certification 1,430,271$ 2,440,790$ 2,135,691$ 305,099$
Vendor Costs -$ -$ -$ -$
Internal Costs 1,430,271$ 2,440,790$ 2 2,135,691$ 305,099$
Total 11,151,568$ 18,244,536$ 15,963,969$ 2,280,567$
Program-Level Project
Budget
3/14/2013 32 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Reason for Changes to the Program-Level Budget 1. The project length was extended by 22 months, additional staffing
hours were required due to the extended schedule
2. Updated staffing requirements for the first year of operations to support maintenance and federal certification activities
3/14/2013 33 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Contract Amendments
Contract Amendments ◦ By Project and vendor
◦ Cost Increase associated with each
3/14/2013 34 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Truven Contract – Reporting & Analytics
Vendor Amendment Cost State Share
Truven
Development Base 6,877,113$ 687,711$
Ops & Maintenance Base 43,428,927$ 10,857,232$
Development Amend # 1 -$ -$
Ops & Maintenance Amend # 1 -$ -$
Development CSR 787 1,511,370$ 151,137$
Development Amend # 2 1,441,798$ 1,297,618$
Ops & Maintenance Amend # 2 20,851,305$ 5,212,826$
Development Amend # 3 -$ -$
Ops & Maintenance Amend # 3 -$ -$
Total
Development 9,830,281$ 2,136,467$
Ops & Maintenance 64,280,232$ 16,070,058$
NCMMIS+ ProgramContract Amendments
3/14/2013 35 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

GLS Contract – Business Process Automation System (BPAS)
Vendor Amendment Cost State Share
GLS
Development Base 5,515,494$ 2,757,747$
Ops & Maintenance Base 3,537,255$ 1,768,628$
Development Amend # 1 -$ -$
Ops & Maintenance Amend # 1 -$ -$
Total
Development 5,515,494$ 2,757,747$
Ops & Maintenance 3,537,255$ 1,768,628$
NCMMIS+ ProgramContract Amendments
3/14/2013 36 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services

Maximus Contract – Independent Verification and Validation (IV&V)
Vendor Amendment Cost State Share
Maximus
Development Base 2,549,968$ 267,747$
Ops & Maintenance Base 378,796$ 94,699$
Development Amend # 1 -$ -$
Ops & Maintenance Amend # 1 -$ -$
Development Amend # 2 1,459,752$ 153,274$
Ops & Maintenance Amend # 2 507,640$ 126,910$
Total
Development 4,009,720$ 421,021$
Ops & Maintenance 886,436$ 221,609$
NCMMIS+ ProgramContract Amendments
3/14/2013 37 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services
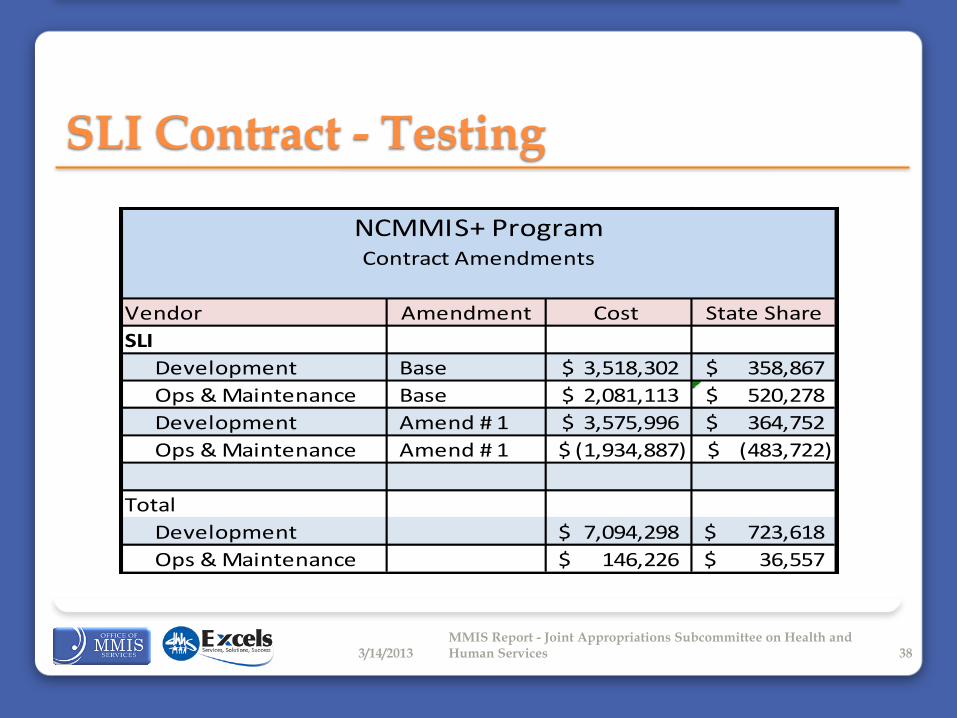
SLI Contract - Testing
Vendor Amendment Cost State Share
SLI
Development Base 3,518,302$ 358,867$
Ops & Maintenance Base 2,081,113$ 520,278$
Development Amend # 1 3,575,996$ 364,752$
Ops & Maintenance Amend # 1 (1,934,887)$ (483,722)$
Total
Development 7,094,298$ 723,618$
Ops & Maintenance 146,226$ 36,557$
NCMMIS+ ProgramContract Amendments
3/14/2013 38 MMIS Report - Joint Appropriations Subcommittee on Health and Human Services