Meetings resource person X
51
1 | N ational K idney and T ransplant I nstitute “Sakit sa Bato, Sagot Nandito, NKTI Kaagapay Mo” The Executive Committee is committed to achieving its vision through organizational excellence by imbibing a Culture of Excellence where the employees’ battlecry is, “Excellence EVERYDAY!” 1.1 Senior Leadership 1.1a Vision, Values, and Mission 1.1a(1) Vision and Values. Having the National Kidney and Transplant Institute Mandate as main basis, the Vision and Mission statements are created. In order to achieve the Vision-Mission, key performance indicators (KPI) are identified based on the strategic objectives. Different initiatives to achieve the KPIs with the corresponding process owners are further assigned. Stakeholder consultation and customer feedback are considered to make a holistic performance review. The PDCA Model is applied to ensure effectiveness and efficiency. Under Plan, work system and process are in place in every section observing the total quality management principles. Upon careful review of the work system and process, they are implemented (performance) using good governance where this is the “Do” step. Checking is done through careful evaluation and customer feedback. Evaluation and feedback are reviewed and analyzed through research and development. After research and development, extensive advocacies are implemented considering social responsibility. (Fig.1.1-1) To date, a group was convened to review the current NKTI vision-mission statements. The objective is to make it more relevant to the current state of the Institution. A survey tool was provided the department chairs in order to assess if the present vision-mission statements still apply to the present set-up of NKTI. Vision and values are introduced to the new employees through various strategies. For residents, fellows and consultants, it is discussed by the deputy executive director for medical services during the annual general orientation. For new non medical staff, it is discussed during the General Orientation Program. For employees, vision and values are communicated during the Delivering Quality Service Program and 7S Workshop. Other strategies used are discussion during meetings, posting of posters on bulletin boards and other areas, website, issuance of hospital circular and publishing of the Renal Capsule. (Fig. 1.1-2) Fig.1.1-2: Vision and Values Deployment Matrix CATEGORY 1. LEADERSHIP Deployment Method Employees Customers Stakeholders Physicians’ Orientation (residents, fellows, consultants) every January by the Deputy Director for Medical Services X Employee orientation for new staff by the Human Resource Management Division, and orientation conducted by department where new staff will be assigned X Employee training particularly Stream 1 programs: Delivering Quality Service program (held every two months) 7S Workshop (held every two months) where the Chief of the Human Resource Management Division is a regular resource person X Meetings * Monthly for unit/section and department * Quarterly for medical staff X Posters at the patient care areas and bulletin board X X X Website X X X Hospital Circular initiated by the Executive Director and attested by the Deputy Executive Director X Renal Capsule initiated by the Executive Director X X X Fig.1.1-1: Leadership Model
Transcript of Meetings resource person X
1 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
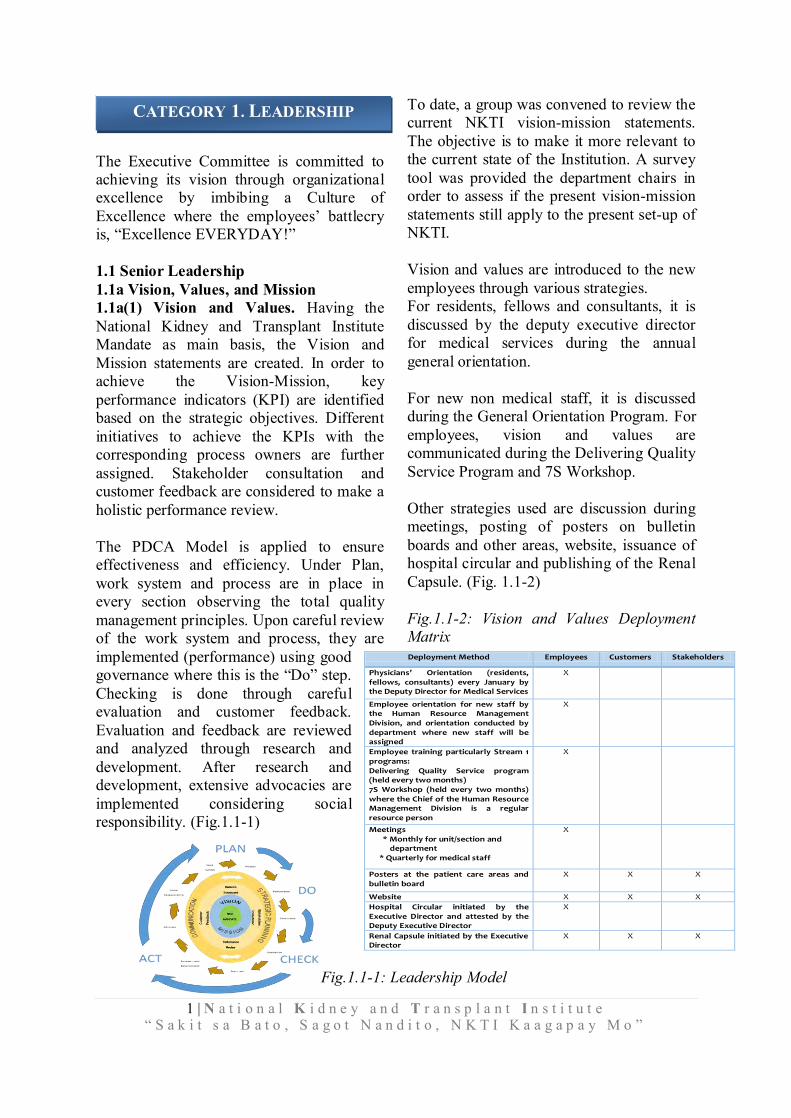
The Executive Committee is committed to achieving its vision through organizational excellence by imbibing a Culture of Excellence where the employees’ battlecry is, “Excellence EVERYDAY!” 1.1 Senior Leadership 1.1a Vision, Values, and Mission 1.1a(1) Vision and Values. Having the National Kidney and Transplant Institute Mandate as main basis, the Vision and Mission statements are created. In order to achieve the Vision-Mission, key performance indicators (KPI) are identified based on the strategic objectives. Different initiatives to achieve the KPIs with the corresponding process owners are further assigned. Stakeholder consultation and customer feedback are considered to make a holistic performance review. The PDCA Model is applied to ensure effectiveness and efficiency. Under Plan, work system and process are in place in every section observing the total quality management principles. Upon careful review of the work system and process, they are implemented (performance) using good governance where this is the “Do” step. Checking is done through careful evaluation and customer feedback. Evaluation and feedback are reviewed and analyzed through research and development. After research and development, extensive advocacies are implemented considering social responsibility. (Fig.1.1-1)
To date, a group was convened to review the current NKTI vision-mission statements. The objective is to make it more relevant to the current state of the Institution. A survey tool was provided the department chairs in order to assess if the present vision-mission statements still apply to the present set-up of NKTI. Vision and values are introduced to the new employees through various strategies. For residents, fellows and consultants, it is discussed by the deputy executive director for medical services during the annual general orientation. For new non medical staff, it is discussed during the General Orientation Program. For employees, vision and values are communicated during the Delivering Quality Service Program and 7S Workshop. Other strategies used are discussion during meetings, posting of posters on bulletin boards and other areas, website, issuance of hospital circular and publishing of the Renal Capsule. (Fig. 1.1-2) Fig.1.1-2: Vision and Values Deployment Matrix
CATEGORY 1. LEADERSHIP
Deployment Method Employees Customers Stakeholders
Physicians’ Orientation (residents, fellows, consultants) every January by the Deputy Director for Medical Services
X
Employee orientation for new staff by the Human Resource Management Division, and orientation conducted by department where new staff will be assigned
X
Employee training particularly Stream 1 programs: Delivering Quality Service program (held every two months) 7S Workshop (held every two months) where the Chief of the Human Resource Management Division is a regular resource person
X
Meetings * Monthly for unit/section and
department * Quarterly for medical staff
X
Posters at the patient care areas and bulletin board
X X X
Website X X X
Hospital Circular initiated by the Executive Director and attested by the Deputy Executive Director
X
Renal Capsule initiated by the Executive Director
X X X
Fig.1.1-1: Leadership Model

2 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
1.1a(2) Promoting Legal and Ethical Behavior. Senior leaders (SL) follow legal and government requirements. The NKTI is regulated by RA 9184 Government Procurement Reform Act as well as by accounting and auditing rules by government. The NKTI website posts annual reports, approved budget and MFO targets and awarded contracts. 1.1a(3) Creating a Sustainable Organization. Performance highlight was pegged on how an institution delivers its mandated services fostering a culture of positive customer experience and engagement. The NKTI realized that strong influencers for patient availment of the hospital’s services included to a significant extent the physician, the patient’s relatives, and their HMO.
The NKTI had created physician engagement programs that prompted loyalty to the institution. Monthly medical staff meetings where the information flowed both ways were held. Physicians and their respective departments were enjoined to plan an exhibit and put on display at the Main Lobby their services and expertise. Consultative meetings at different levels, from unit to department to administrative were held periodically and innovations and achievements were encouraged and recognized publicly during assemblies (flag ceremonies usually).
Patients’ relatives were empowered by including them in the decision-making process as it pertains to the medical care of the patient.
HMO engagement has only been recently recognized, and at the present time, the NKTI has focused on providing the HMOs with the necessary facilities for their operations.
By harnessing the capacity of the private sector to collaborate with government
institutions, the NKTI has been proactive in this partnership framework to further expand the growing healthcare need of the populace (PPP on hemodialysis, PET-CT, and Cyclotron).
Relative to organizational development and staff empowerment, the NKTI-EC ensures compliance with new performance measurement tools prescribed by the CSC and Department of Budget and Management (DBM) as to institutional major final output (MFOs) by targeting individual performance outputs as primary indicators in determining organizational performance outcome.
To strengthen institutional commitment in terms of quality and professional growth, there is a need to implement new management framework to enhance both internal and external system of the NKTI. Being the first government institution to be accredited by ISO (TUV-SUD), sustained for 12 years, the EC sought new methods to further develop its capacity and hone new methods of sustainability. Together with the assistance of Development Academy of the Philippines (DAP), necessary preparations was already jump-started in the journey towards performance excellence, dream of achieving the prestigious Philippine Academy Award. To financially sustain NKTI’s mission and achieve its vision, NKTI builds a strong financial base by delivering cost-efficient care and implementing managed growth. Its finance and administrative services make efforts increasing subsidy, strict capital expenditure prioritization, and monitoring, and maximizing high margin opportunities. All these redound to promoting satisfactory customer experience and engagement. The EC has a defined professional growth and development program centralized to the HRMD for Stream 1 programs, and through the departments for Stream 2 programs. Committee or special project assignment enhances employee learning.

3 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
To enhance competencies including leadership skills for leaders, succession planning is determined to provide training and systematically appoint persons in key positions once need is identified. 1.1b Communication and Organizational Performance 1.1b(1) Communication. The NKTI senior leaders believe that only by clearly communicating NKTI’s strategy and helping staff understand their roles in the execution of that strategy can NKTI optimize its performance while remaining a great place to work in. Hence, department and hospital team building and strategic planning sessions are held. Communication to employees of different levels is done through a general assembly once a year or more often as needed. Aside from the general assembly, there is a weekly address of the employees by the Executive Director or his designate every Monday during flag raising ceremony where inspirational messages are shared. Hospital orders, circulars, memos, etc., are sent through the hospital email system. Every year the executive director summarizes annual performance in the NKTI Annual report. For the nursing services department, an annual staff satisfaction survey is done in order to assess staff’s level of satisfaction. Annual Recognition. Senior leaders recognize outstanding performance (Best Employee and Perfect Attendance award) during Kidney month celebration held every June, as well as Loyalty awards (15, 20 and 25 years in service) during the annual hospital Christmas celebration. 1.1b(2) Focus on Action. All offices prepare action plans which are reviewed by the Internal Quality Audit team (IQA). Management review is held twice a year to revisit action plans and report on accomplishments.
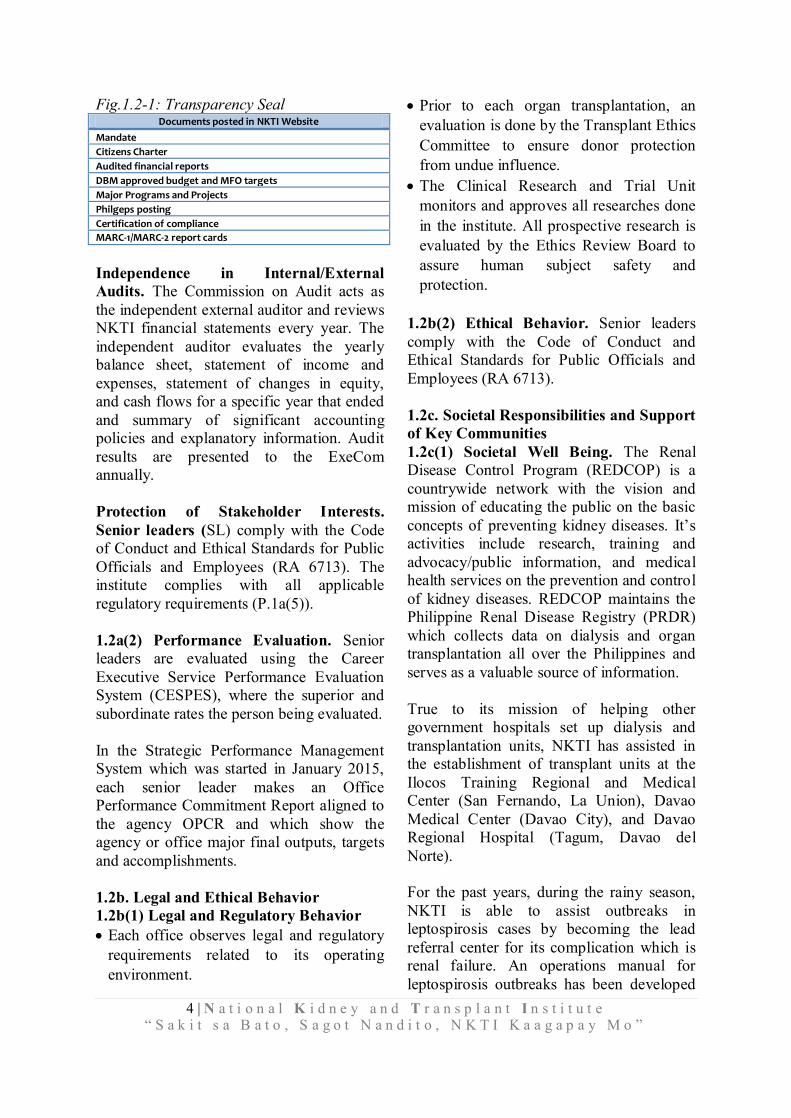
1.2 Governance and Societal Responsibilities 1.2a. Organizational Governance 1.2a(1) Governance System Accountability for management’s actions. NKTI is under the administrative supervision of the Department of Health. Executive Order No. 34 dated July 29, 1986 provides that NKTI be administered by a Board of Trustees (BOT), so that matters pertaining to budget, high end equipment, infrastructure, Public-Private Partnerships (PPP), as well as computerization projects, are referred to the BOT for final decision/approval. BOT Resolution No. 5 dated June 18,1997 authorized the Executive Director to execute specific powers and functions of 1) formulating policies, guidelines and programs to effectively implement and carry out the purposes and objectives of creating NKTI, 2) prescribing, reviewing and revising the amount of fees, charges and assessment, levied and collected for the support and maintenance of the hospital’s operations, and 3) promulgating such rules and regulations as may be necessary or proper for the effective service of powers and functions as well as the discharge of duties, responsibilities of the hospital, its officers and employees. NKTI is covered by R.A. No. 101491 (GOCC Governance Act of 2011) promoting financial viability and fiscal discipline in Government-owned and controlled corporations (GOCCs) and strengthening the role of the state in governance and management for public interest. Fiscal Accountability. The finance and budget office plans budgets for operations and reports to the Executive Director and committee. Transparency in operations and selection of and disclosure policies for Governance board members. To ensure transparency in operations the following documents are posted on the NKTI website (Fig 1.2-1).
4 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig.1.2-1: Transparency Seal Documents posted in NKTI Website
Mandate
Citizens Charter
Audited financial reports
DBM approved budget and MFO targets
Major Programs and Projects
Philgeps posting
Certification of compliance
MARC-1/MARC-2 report cards
Independence in Internal/External Audits. The Commission on Audit acts as the independent external auditor and reviews NKTI financial statements every year. The independent auditor evaluates the yearly balance sheet, statement of income and expenses, statement of changes in equity, and cash flows for a specific year that ended and summary of significant accounting policies and explanatory information. Audit results are presented to the ExeCom annually. Protection of Stakeholder Interests. Senior leaders (SL) comply with the Code of Conduct and Ethical Standards for Public Officials and Employees (RA 6713). The institute complies with all applicable regulatory requirements (P.1a(5)). 1.2a(2) Performance Evaluation. Senior leaders are evaluated using the Career Executive Service Performance Evaluation System (CESPES), where the superior and subordinate rates the person being evaluated. In the Strategic Performance Management System which was started in January 2015, each senior leader makes an Office Performance Commitment Report aligned to the agency OPCR and which show the agency or office major final outputs, targets and accomplishments. 1.2b. Legal and Ethical Behavior 1.2b(1) Legal and Regulatory Behavior Each office observes legal and regulatory
requirements related to its operating environment.
Prior to each organ transplantation, an evaluation is done by the Transplant Ethics Committee to ensure donor protection from undue influence.
The Clinical Research and Trial Unit monitors and approves all researches done in the institute. All prospective research is evaluated by the Ethics Review Board to assure human subject safety and protection.
1.2b(2) Ethical Behavior. Senior leaders comply with the Code of Conduct and Ethical Standards for Public Officials and Employees (RA 6713). 1.2c. Societal Responsibilities and Support of Key Communities 1.2c(1) Societal Well Being. The Renal Disease Control Program (REDCOP) is a countrywide network with the vision and mission of educating the public on the basic concepts of preventing kidney diseases. It’s activities include research, training and advocacy/public information, and medical health services on the prevention and control of kidney diseases. REDCOP maintains the Philippine Renal Disease Registry (PRDR) which collects data on dialysis and organ transplantation all over the Philippines and serves as a valuable source of information. True to its mission of helping other government hospitals set up dialysis and transplantation units, NKTI has assisted in the establishment of transplant units at the Ilocos Training Regional and Medical Center (San Fernando, La Union), Davao Medical Center (Davao City), and Davao Regional Hospital (Tagum, Davao del Norte). For the past years, during the rainy season, NKTI is able to assist outbreaks in leptospirosis cases by becoming the lead referral center for its complication which is renal failure. An operations manual for leptospirosis outbreaks has been developed
5 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
at the NKTI and is recognized by the DOH. This manual has been adapted by various government hospitals as part of their emergency preparedness program. 1.2c(2) Community Support. NKTI conducts activities to create public awareness not only about kidney disease but also other allied diseases such as cancer, diabetes, liver diseases etc. As per Proclamation No. 184 s.1993, as declared by President Fidel V. Ramos, to promote awareness on the fatal consequences of renal diseases and its prevention. 1) Every year in June, Kidney Month is celebrated. Public awareness about diseases of the kidney and its management are brought to the public through media guestings, hospital and mall exhibits, and medical outreaches. 2) Nutrition Month happens every July where nutrition lectures, cooking demonstrations, free blood glucose screening, lectures on various diseases, and community outreaches are held. 3) Beyond the kidneys, public awareness campaigns are held by key clinical units such as the Liver Center and the Breast Center. The Liver Center held lay fora and a public exhibit in September 2013 and a total of 173 patients were given free hepatitis B & C screening. October is Breast Cancer Awareness Month. In 2013, as part of the advocacy on breast cancer which is the leading cause of cancer in the Philippines, breast cancer related activities were held at the NKTI. These included a lecture series for employees of the NKTI and other government offices attended by almost 400 participants. Nearly 300 free breast examinations were conducted, 19 free diagnostic mammograms and 18 free diagnostic ultrasound examinations were given to patients in need. 4) As part of Health Emergency Management System, we were able to provide full support to the DOH by sending some of our paramedical and medical staff to aide our fellowmen devastated by super typhoon “Yolanda”.
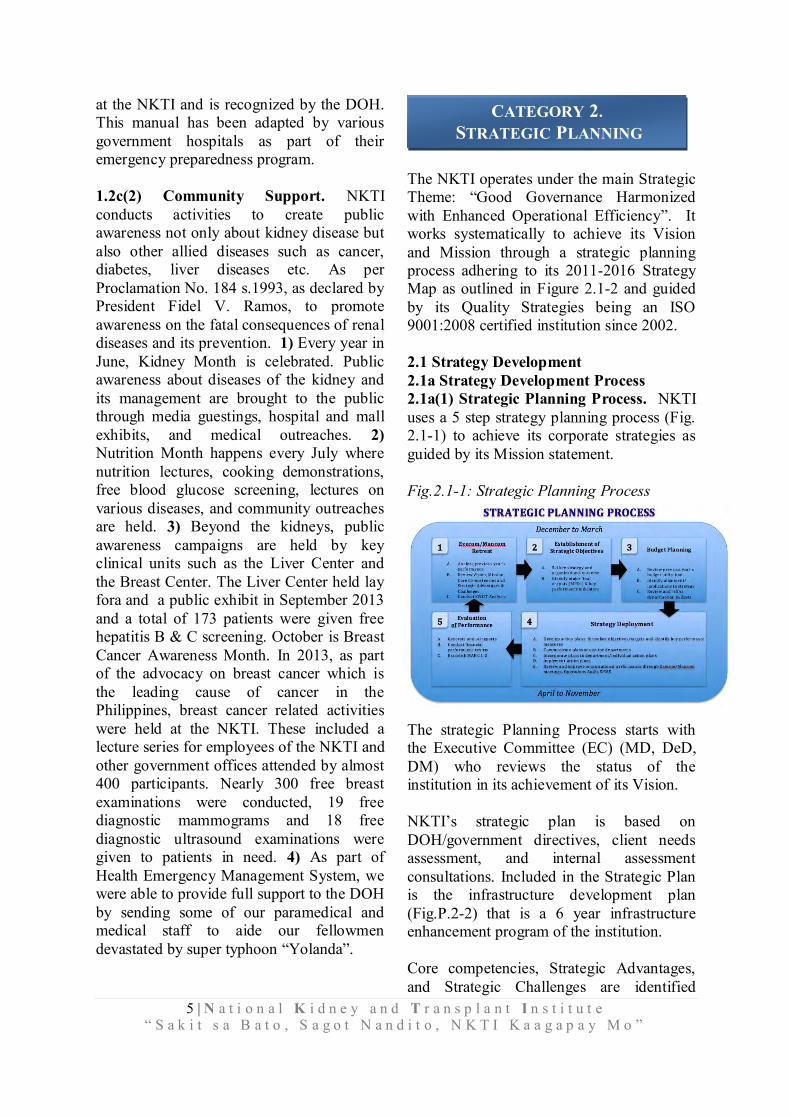
The NKTI operates under the main Strategic Theme: “Good Governance Harmonized with Enhanced Operational Efficiency”. It works systematically to achieve its Vision and Mission through a strategic planning process adhering to its 2011-2016 Strategy Map as outlined in Figure 2.1-2 and guided by its Quality Strategies being an ISO 9001:2008 certified institution since 2002. 2.1 Strategy Development 2.1a Strategy Development Process 2.1a(1) Strategic Planning Process. NKTI uses a 5 step strategy planning process (Fig. 2.1-1) to achieve its corporate strategies as guided by its Mission statement. Fig.2.1-1: Strategic Planning Process
The strategic Planning Process starts with the Executive Committee (EC) (MD, DeD, DM) who reviews the status of the institution in its achievement of its Vision. NKTI’s strategic plan is based on DOH/government directives, client needs assessment, and internal assessment consultations. Included in the Strategic Plan is the infrastructure development plan (Fig.P.2-2) that is a 6 year infrastructure enhancement program of the institution. Core competencies, Strategic Advantages, and Strategic Challenges are identified
CATEGORY 2. STRATEGIC PLANNING

6 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
during the regular ExeCom/ManCom meetings by analysis of the strengths, weaknesses, opportunities and threat of the institution. These Core Competencies, Strategic Advantages, and Strategic Challenges are summarized in Fig. P.1-2 and P.2-3. These lead to identification of blind spots and necessary revisions of the Strategic Plan. Blind spots are also basically identified through customer feedbacks, employee survey, supplier forum, and external consultant. These lead to further enhancement of the strategic plan to further cater to the needs and better service to the stakeholders. The Strategic Plan is subsequently presented to the BOT for their approval and recommendation for budget allocation by the Department of Budget and Management (DBM) (step 3) The strategic plan is then discussed with the ManCom composed of department chairmen, division heads, and unit managers who plan and align their short term and long term departmental action plans (step 4). A comparative performance report (year to year) is presented regularly at the ManCom Meeting where achievements in the previous years action plans are described and new action plans presented to the committee. Depending on the yearly performance, a new target is set and plans for enhancement are presented and approved. Action plans and projects necessitating appropriation of budget is presented to the Finance Department for budget allocation. Equipment purchases more than 1 million pesos are presented to the Capital Expenditure (CAPEX) for prioritization and approval. During the CAPEX presentation, justification for the budget is defended and includes the impact to the services of the unit, benefits to the delivery of care, and projected return of investment (ROI).
Each department subsequently deploys the action plans to its respective divisions/units for detailed planning and execution. A midyear performance evaluation is done and again presented to the ManCom to monitor accomplishment of targets of the action plans. Necessary modifications of the action plans may be done as deemed necessary and as suggested during the ManCom meeting. A year-end (step 5), performance evaluation is again presented which includes accomplishments of the previous year and financial performance review. From 2012, the institution also followed the directive of the national government on the monitoring of performance targets for the Performance Based Incentive System. MARC 1 (Fig.7.1-17,18) reflected the institutional performance for 2013 and 2014. As a result of the institute’s journey towards the PQA, a Strategic Planning Workshop was held in the first quarter of 2015 to identify the Strategic Objectives and Action Plans of the institution based on the 2011-2016 Strategy Map (Fig.2.1-2) and ISO Quality Objectives. 2.1a(2) Strategic Considerations. The NKTI works along the Vision and Mission of the national government and is directly affected by governmental policies on healthcare and delivery. Statutory rules and regulations and governmental directives have to be adhered to; if these are implemented midway in the strategic planning process, then adjustments in policies will have to be made. In general, however, governmental policies are aimed towards the effective delivery of service to the general population and uncommonly affect the overall strategic plans and the strategic planning process. The Medical Director represents the NKTI in the Board of Trustees and explains the overall strategic plan of the institution and seeks approval for its budget and implementation.

7 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Each department is tasked to conduct their own Strengths/Weaknesses/opportunities Threats (SWOT) analysis on how to further improve its delivery of services and improve financial returns for income generating centers/units. Trends in healthcare delivery, availability of new technologies, increasing utilization of facilities, and potential threats are taken into consideration in the planning process. This is participated by the members/staff and managers/heads of each respective department in their regular (at least quarterly) staff meetings. Necessary changes and modifications may be done in the exigency of an efficient service. During ManCom meetings, all cost centers are tasked to provide a semiannual income and expense report. To ensure financial stability to sustain its operations and provide funds for further institutional projects and improvements, each cost center is constantly tasked to find ways of improving its income without necessarily compromising its services and losing its competitiveness with comparable institutions. Continuous upgrade in NKTI’s facilities and services has ensured the loyalty of its stakeholders. With the expansion of the institution come problems with human resource. To address human resource problems due to restrictions of available plantilla positions (salaried personnel under government positions), positions under job order status have been created. Additional medical specialists are regularly added with proper credentialing and privileging to render specialized care to the patients. Realizing the fact that the core service of the institution is delivery of care to patients with renal disease and organ transplantation, NKTI has always looked at ways of improving its services to these patients. The hemodialysis unit has continually been improved and expanded. Units for peritoneal dialysis have been created. To render better patient service to dialysis patients, a training
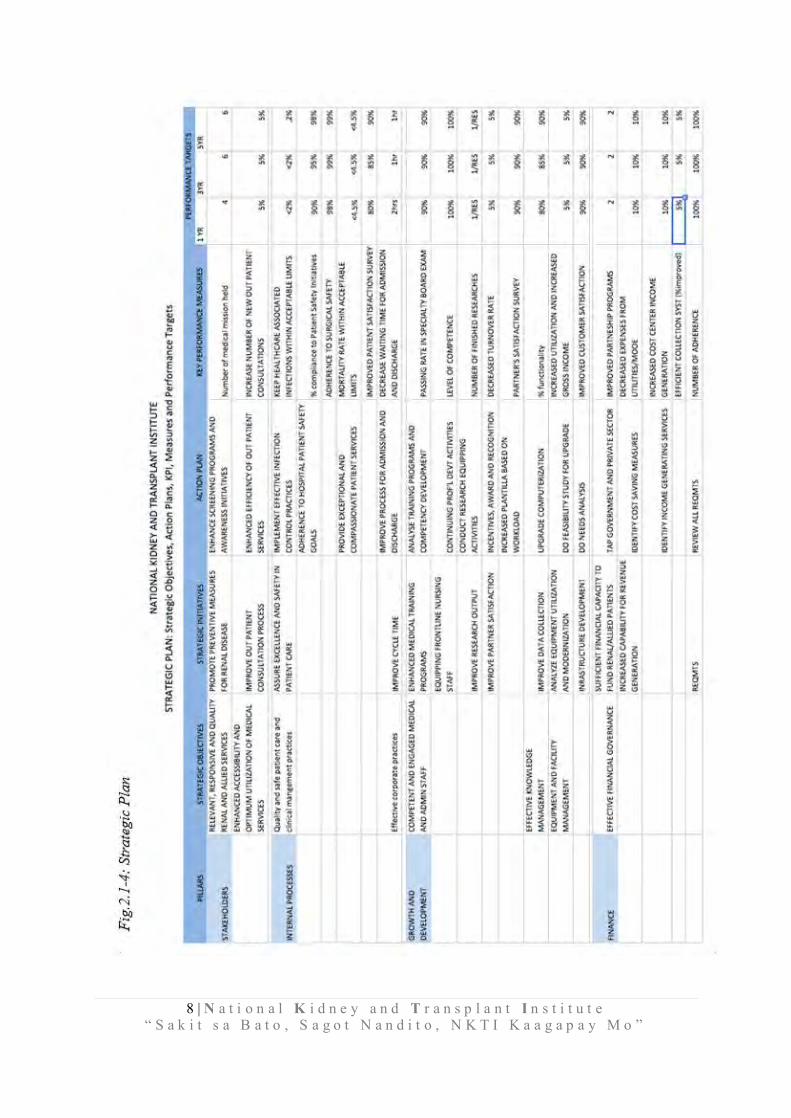
program for home peritoneal dialysis was started and effectively implemented. 2.1b Strategic Objectives 2.1b(1) Key Strategic Objectives. As part of NKTI's SPP, the ExeCom together with Department managers and heads develop, review and monitor targets through scheduled meetings (Fig.2.1-1). Likewise, each department is tasked to develop, review and monitor its own strategies, targets and accomplishment. Fig.2.1-2: NKTI Strategy Map 2011-2016
These Strategic Objectives (Fig. 2.1-4) are then deployed to each department for realigning their action plans for 2015 and beyond. Fig.2.1-3: Schedule of Strategic Activities
STRATEGIC ACTIVITIES FREQUENCY MEMBERS
Strategic Planning Workshop Once a year Medical Director; Deputy Directors; Department Heads/ Managers (DH/M)
Executive Committee (EC) Meeting
Once a month or as needed
Medical Director; Deputy Directors; Department Manager for Finance and Ancillary Services
Management Review Twice a year EC; DH/M
Management Committee Twice a month EC; DH/M
Operations Audit Twice a month Finance Heads/Ancillary Head
Departmental Meetings Once a month Department Staff
8 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
9 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
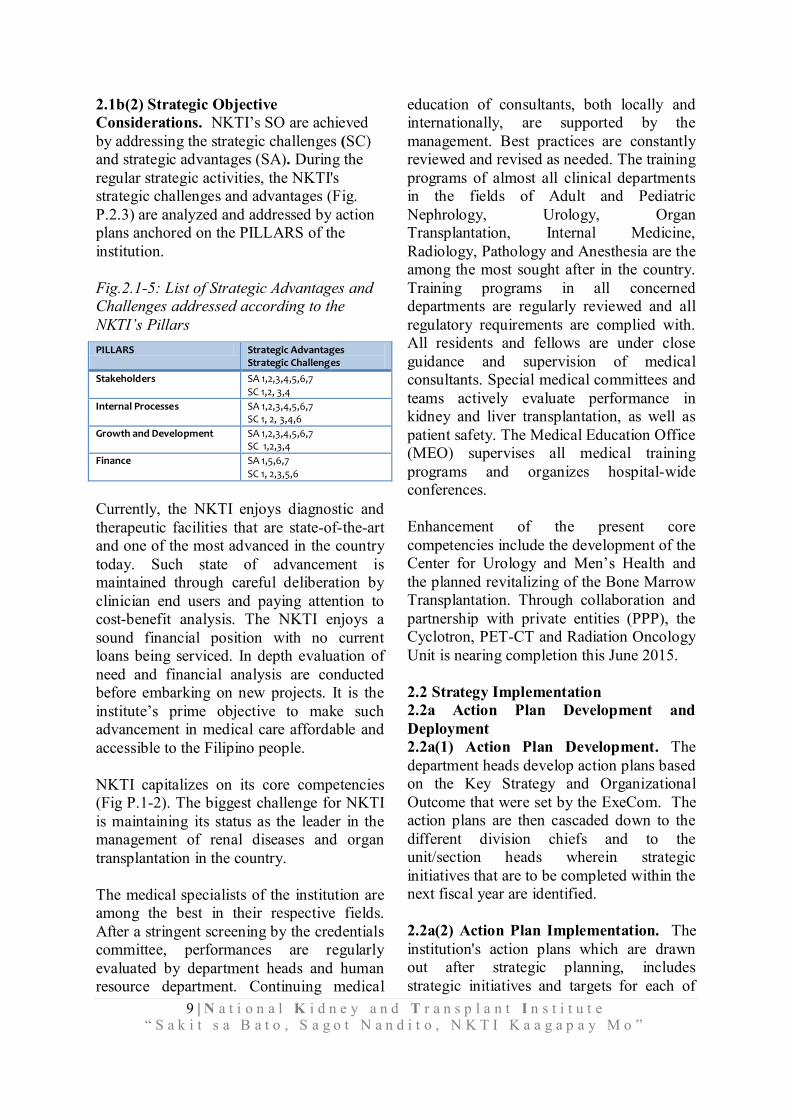
2.1b(2) Strategic Objective Considerations. NKTI’s SO are achieved by addressing the strategic challenges (SC) and strategic advantages (SA). During the regular strategic activities, the NKTI's strategic challenges and advantages (Fig. P.2.3) are analyzed and addressed by action plans anchored on the PILLARS of the institution. Fig.2.1-5: List of Strategic Advantages and Challenges addressed according to the NKTI’s Pillars PILLARS Strategic Advantages
Strategic Challenges
Stakeholders SA 1,2,3,4,5,6,7 SC 1,2, 3,4
Internal Processes SA 1,2,3,4,5,6,7 SC 1, 2, 3,4,6
Growth and Development SA 1,2,3,4,5,6,7 SC 1,2,3,4
Finance SA 1,5,6,7
SC 1, 2,3,5,6
Currently, the NKTI enjoys diagnostic and therapeutic facilities that are state-of-the-art and one of the most advanced in the country today. Such state of advancement is maintained through careful deliberation by clinician end users and paying attention to cost-benefit analysis. The NKTI enjoys a sound financial position with no current loans being serviced. In depth evaluation of need and financial analysis are conducted before embarking on new projects. It is the institute’s prime objective to make such advancement in medical care affordable and accessible to the Filipino people. NKTI capitalizes on its core competencies (Fig P.1-2). The biggest challenge for NKTI is maintaining its status as the leader in the management of renal diseases and organ transplantation in the country. The medical specialists of the institution are among the best in their respective fields. After a stringent screening by the credentials committee, performances are regularly evaluated by department heads and human resource department. Continuing medical
education of consultants, both locally and internationally, are supported by the management. Best practices are constantly reviewed and revised as needed. The training programs of almost all clinical departments in the fields of Adult and Pediatric Nephrology, Urology, Organ Transplantation, Internal Medicine, Radiology, Pathology and Anesthesia are the among the most sought after in the country. Training programs in all concerned departments are regularly reviewed and all regulatory requirements are complied with. All residents and fellows are under close guidance and supervision of medical consultants. Special medical committees and teams actively evaluate performance in kidney and liver transplantation, as well as patient safety. The Medical Education Office (MEO) supervises all medical training programs and organizes hospital-wide conferences. Enhancement of the present core competencies include the development of the Center for Urology and Men’s Health and the planned revitalizing of the Bone Marrow Transplantation. Through collaboration and partnership with private entities (PPP), the Cyclotron, PET-CT and Radiation Oncology Unit is nearing completion this June 2015. 2.2 Strategy Implementation 2.2a Action Plan Development and Deployment 2.2a(1) Action Plan Development. The department heads develop action plans based on the Key Strategy and Organizational Outcome that were set by the ExeCom. The action plans are then cascaded down to the different division chiefs and to the unit/section heads wherein strategic initiatives that are to be completed within the next fiscal year are identified. 2.2a(2) Action Plan Implementation. The institution's action plans which are drawn out after strategic planning, includes strategic initiatives and targets for each of
10 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
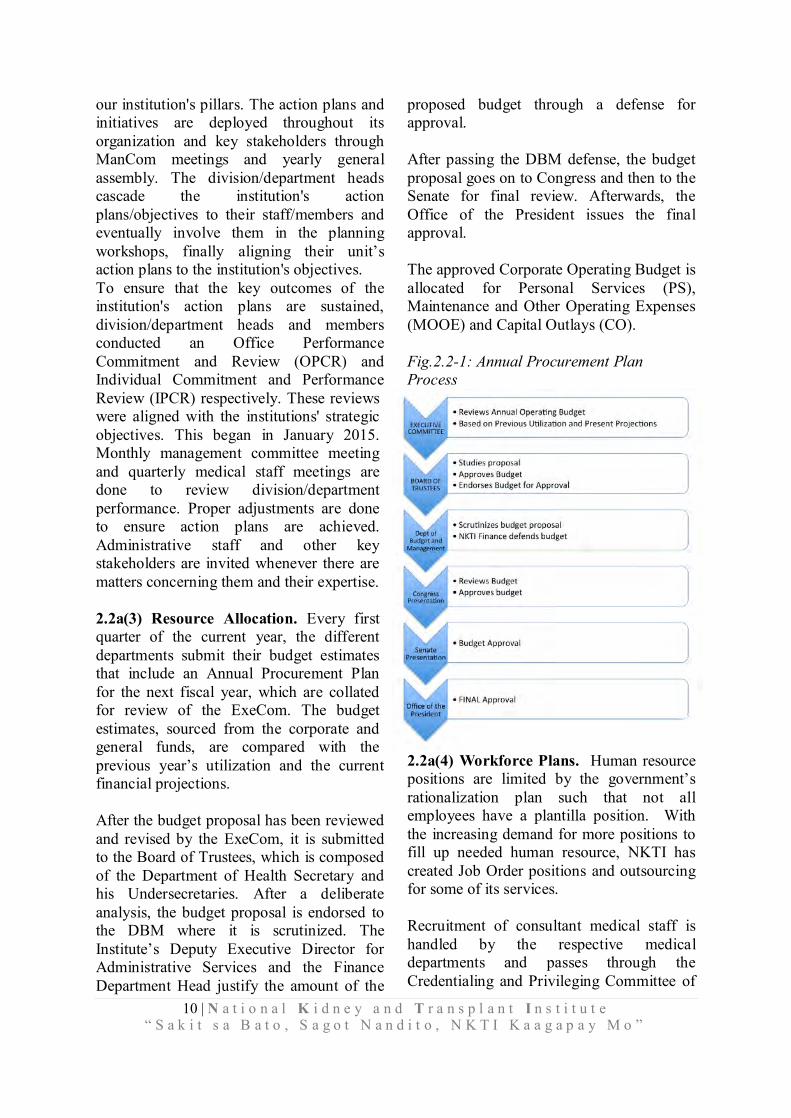
our institution's pillars. The action plans and initiatives are deployed throughout its organization and key stakeholders through ManCom meetings and yearly general assembly. The division/department heads cascade the institution's action plans/objectives to their staff/members and eventually involve them in the planning workshops, finally aligning their unit’s action plans to the institution's objectives. To ensure that the key outcomes of the institution's action plans are sustained, division/department heads and members conducted an Office Performance Commitment and Review (OPCR) and Individual Commitment and Performance Review (IPCR) respectively. These reviews were aligned with the institutions' strategic objectives. This began in January 2015. Monthly management committee meeting and quarterly medical staff meetings are done to review division/department performance. Proper adjustments are done to ensure action plans are achieved. Administrative staff and other key stakeholders are invited whenever there are matters concerning them and their expertise. 2.2a(3) Resource Allocation. Every first quarter of the current year, the different departments submit their budget estimates that include an Annual Procurement Plan for the next fiscal year, which are collated for review of the ExeCom. The budget estimates, sourced from the corporate and general funds, are compared with the previous year’s utilization and the current financial projections. After the budget proposal has been reviewed and revised by the ExeCom, it is submitted to the Board of Trustees, which is composed of the Department of Health Secretary and his Undersecretaries. After a deliberate analysis, the budget proposal is endorsed to the DBM where it is scrutinized. The Institute’s Deputy Executive Director for Administrative Services and the Finance Department Head justify the amount of the
proposed budget through a defense for approval. After passing the DBM defense, the budget proposal goes on to Congress and then to the Senate for final review. Afterwards, the Office of the President issues the final approval. The approved Corporate Operating Budget is allocated for Personal Services (PS), Maintenance and Other Operating Expenses (MOOE) and Capital Outlays (CO). Fig.2.2-1: Annual Procurement Plan Process
2.2a(4) Workforce Plans. Human resource positions are limited by the government’s rationalization plan such that not all employees have a plantilla position. With the increasing demand for more positions to fill up needed human resource, NKTI has created Job Order positions and outsourcing for some of its services. Recruitment of consultant medical staff is handled by the respective medical departments and passes through the Credentialing and Privileging Committee of

11 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
the Institution. After going through the screening process they are introduced to the medical staff during the Medical and Surgical Staff Meeting. The respective departments, based on criteria set by the respective specialty board, handle recruitment of in-training residents and fellows. They undergo rigorous training and competency development while handling patients in the Institution. The number of residents and trainees is adjusted to respond to the growing needs of the institution to render efficient, competent, and excellent healthcare services to its stakeholders. 2.2a(5) Performance Measures. The Institute follows the Performance-Based Incentive System (PBIS) that is prescribed by the National Government, wherein Major Final Outputs (MFOs) and its corresponding Performance Indicators are identified. The actual accomplishments are compared to the year-on-year targets for each performance indicator. The three Major Final Outputs are: Hospital Services, Research and Development Services, and Education and Training for Health Professionals. Below are the Performance Indicators for each MFO: Hospital Services Percentage of patients discharged as
improved Percentage of clients that rate hospital
services as satisfactory or better Percentage of triage patients with score ≥ 3
Emergency Severity Index (ESI) on the following areas ER – within 30 minutes OPD – within 2 hours
Research and Development Services Number of medical research projects
completed
Percentage of completed medical research projects published in a recognized journal of specialty societies or adopted by health sector
Percentage of research projects completed within the original proposed timeframe
Education and Training for Health Professionals Number of graduates of specialization in
nephrology and urology Percentage of trainees (medical) who
passed specialty board exams Percentage of doctors who completed the
specialization course within scheduled time
In addition to the MFOs, the performance indicators and targets pertaining to Support to Operations (STO) and General Administration and Support Services (GASS) are identified: Support to Operations (STO) Percentage of effectivity and functionality
of Hospital Information System Percentage of laboratory results given
within 3 hours (TAT) General Administration and Support Services (GASS) Budget utilization rate Total Actual Obligation (Net of PS &
Disallowed items in the COB/DBM Approved Budget (Net of PS)
Total Actual Disbursement/Total Actual Obligation Percentage of Financial statements and documents submitted within the mandated time
Financial statement submitted to COA within mandated time
2.2a(6) Action Plan Modification. The institution's planning process puts emphasis on review and revision of its action plans in response to key changes in the internal and external environments. These changes to the demands of key stakeholders (i.e. patients, physicians, suppliers, other stakeholders), need for additional personnel, need for additional equipment/technology, legislative

12 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
or regulatory changes are discussed throughout the year by ExeCom with the division/departmental heads. Whenever urgent issues requiring immediate attention arise, it is resolved by an emergency meeting called by ExeCom. Aside from the quarterly and annual performance review by the ExeCom, department/division meetings are done monthly to address performance gaps and address areas for strategic improvement. This monthly department/division performance and reports serves as feedback for ExeCom to modify some action plans. 2.2b. Performance Projections. Performance projections are based on historical trends of the Institution’s performance in general, and of the different cost centers, in particular. Considering that the income of the NKTI supports its major expenses and expansion programs, financial stability is a major outcome that is regularly assessed. Each center is tasked at the start of the year to have an annual projection of income which is usually increased by 10%-20% of the previous years income. Together with this projected income increase are measures that would be taken to achieve the projection. Benchmarking with major comparable institutions is made with regards to availability of advanced technology, efficiency of service and cost of procedures. This is analyzed by midyear and year-end to accomplishment the projected income target. Strategy modifications and corrective action plans are implemented if the performance is short of target. Since among the core competencies and pillars of the NKTI are its training programs for medical specialties, performance of the different training programs is also monitored. The projection is for the training department to have an acceptable passing in the specialty board of its graduates. Because of this, the different specialties and subspecialties recognize the NKTI as one of the best training institutions. The graduates of the different training programs of NKTI
excel in their respective specialties and have a high passing rate in their board exams. They are also now a leaders in their respective organizations and place of practice. (Fig.7.1-19). NKTI also provides specialists to the different provinces where the specific specialty is scarce or not available. (Fig.7.1-20, 21, 22, 23)
3.1 Voice of the Customer and Citizen 3.1a Customer and Citizen Listening 3.1a(1) Listening to Current Customers and Citizens. The Institute declares on its vision and mission the three mandates for Service, Training and Research. Thus, NKTI classifies its customers aligned with the expertise being availed for. NKTI listens to its current customers and citizens using various methods. Listening methods also vary across the identified life cycle and point of interaction of the customers with the services of the Insitute as appropriate. For the expertise of Service to patients, they are first sub-classified as in-patient and out-patient. During the admission / confinement period, verbalized concerns are heard through the staff in contact with the patient and are relayed to their Unit Head for actions on the matters beyond the staff’s capabilities. NKTI through its Community Relation and Marketing Services (CREAM) Service Satisfaction Assurance Unit (SSAU), following DOH prescribed format and content, has also developed different feedback gathering tools for different sets of customers. For a confined patient, the Feedback survey tool touches on more topics and mentions the different sections the patient may have had interaction with during his/her admission period. A survey called “We Hear You” is given to patients upon admission and at the Hemodialysis Unit and Peritoneal Dialysis (PD) Unit. Following discharge from the PD Unit, hospital patients
CATEGORY 3. CUSTOMER FOCUS
13 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
receive follow up calls and a 24/7 hotline is available to patients and their families for questions about PD post-hospital care, the healing process, medications, or discharge instructions. Home Visits are also one of the services conducted by the PD Unit to follow up on the condition and treatment compliance of their patients. For out-patient services with different cost centers, each has separate Feedback survey tools individualized for their offered services.
For the expertise of Training, the Institute of Advance Nursing and Allied Health Professions (IANAHP) employs continuous feedback during regular meetings and prior to start of rotation schedule. IANAHP also utilizes Kirkpatrick's training evaluation model using the four levels of learning evaluation for the purpose of program evaluation and feedback from the trainees. Nursing conventions and updates are evaluated after its conduction. Post interaction evaluation from all the different service areas availed, feedback from the social media, emails, and phone calls are the different methods used to acquire feedback from the customers. Post contact feedback allows responses being done in a reactive manner. Different policies such as Quality Procedures on Updating of Social Media Sites (CRM-WI-039) and Handling E-Mails (CRM-WI-020) have been developed. All NKTI related inquiries, compliments and complaints are logged into the Online Inquiry Logbook, provided a Ticket Number and forwarded to the consultant in-charge for responses. Feedback is given to the sender from the social media post or email upon review of response of the concerned office by the Social Media Officer of CREAM unit. The social media that NKTI has accounts in are Facebook (FB), Instagram (IG), Google+ (G+), Twitter, LinkedIn, and Foursquare.
3.1a(2) Listening to Potential Customers and Citizens. For its former customers and clients, the Institute tries to meet the present demands and being react on the concerns raised by these groups, if any. For potential customers, the NKTI has the Re-entry Project. This uses the principle of a referral system to other specialty tertiary hospitals like the Lung Center of the Philippines (LCP) and Philippine Heart Center (PHC). NKTI maintains reciprocal communication with these hospitals so they may directly refer their renal patients to NKTI for renal medical management. In like manner, the Institute will also refer to them patients requiring their respective cardiac and pulmonary expertise. This project is a form of reinforcement of different strengths of these specialty hospitals. Laboratory and Radiology Departments also benchmark the pricing schemes with other hospitals of their services for competition reasons. Listening methods across the life cycle apply to these potential patients when they get to avail our health care services. Attendees of NKTI-conducted Symposia and kidney health awareness during National Kidney Month on Malls and other Medical Missions were also sought for feedback and these are being reported to the Chairman of the respective Committees handling these proceedings and further forwarded to the Department Manager handling these committees for process improvement and planning. Informally, the Social Media Officer of CREAM reviews information from local media such as Reviewing of Newspapers (CRM-WI-021), social media (CRM-WI-039), to obtain issues concerning kidney donation, organ transplantation, dialysis, in-house doctors & staff participating in conventions, and NKTI-related activities, press releases and advertisements of NKTI and other related issues. Copies of the report are then forwarded to the Executive

14 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
CUSTOMER SEGMENT MECHANISM MEASURES USE OF INFORMATION TO EXCEED CUSTOMER
EXPECTATION
EXTERNAL CUSTOMERS
HEALTH CARE SERVICE to PATIENTS
Written feedback through survey tools, online-e-mail & Facebook
Verbalization of concerns during hospitalization
Verbal Conduct of Survey, Email,
1. Appropriateness 2. Timeliness 3. Staff Competency 4. Attitude 5. Quality of Service 6. Condition of the
Environment
1. Process & Systems Improvement
2. Policy Development 3. Strategic & Action Planning
addition and improvement
TRAINING Continuous feedback during meetings, regularly Annually, per rotation schedule, every after seminars
Personal exit interviews Evaluation tools
1. Competency Assessment 2. Passing Rate on
Consultancy Board
Training module enhancement & creation of new courses
RESEARCH None at hand
INTERNAL CUSTOMERS
MEDICAL, PARAMEDICAL PERSONNEL, & ADMINISTRATIVE EMPLOYEES
Staff satisfaction survey annually in some units and quarterly for some departments
Level of Satisfaction, Retention Rate, Reward System
1. Process & Systems Improvement
2. Policy Development
Director, Deputy Directors, Finance Manager, department /division / staff concerned for their information and action. 3.1b Determination of Customer and Citizen Satisfaction and Engagement 3.1b(1) Satisfaction and Engagement. The Patient Feedback Survey Tool measures the level of patient service satisfaction. Parts of it are the comments and recommendation encouraging inputs from the patients for improvement of services received, complaints, concerns or commendations. It is clear that the methodology for listening from the customers and determining their satisfaction is the same which is the utilization of the patient Feedback Survey Tool. The Help desk entertains more of the complaint elevated and as an information resource for customers. The Service Satisfaction Assurance Unit of CREAM handles the dissemination and collection of the patient survey tools. They encode the result and forward them to the Medical Records Division for the statistical data processing, analysis and interpretation. They report the results to the management during the Management Committee Meeting in semestral manner.
Fig. 3.1-1 Customer Satisfaction and Engagement
Determining satisfaction and engagement. Patient Feedback Survey tools are used for patient satisfaction measurement across all the units of the Institute that allow for feedback on those specific services availed. Questions for the in-patient and out-patient satisfaction surveys are tailored for the services rendered aside from the generic contents prescribed by DOH. In 2014, “likelihood to recommend” was added as an engagement and loyalty indicator.
Satisfaction/engagement surveys are collected daily, collated and analyzed monthly and reported in a semestral basis by CREAM to the Management Review. This allows identification of process improvement opportunities. SSAU also reproduces and forwards the accomplished forms to the concerned departments/ divisions/ sections/ doctors if there are major concern/complaints in the survey that needs immediate attention. Survey interpretation contains analysis that identify sections garnering passed patient satisfaction With regards to training expertise, pre-training surveys are conducted to identify specific training requirements. Suggestion for next topic of interest and necessity in the practice are being sought as included in the evaluation tool every after training
conducted. Focused Group Discussions are also venues to extract the training needs analysis of allied medical professionals. The seminar and training evaluation tools contain the level of satisfaction acquired in the attendance and participation with a rating scale used ranging from 1 to 5 score.

15 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
3.1b(2) Satisfaction Relative to Comparable Organizations. Obtaining and using comparative information. There is no data available from the Department of Health with regards to the satisfaction levels of other DOH or private hospitals in the country. The Department said that only NKTI submits patient feedback survey report to them. However, with regards to Hemodialysis and Peritoneal Dialysis Data, loyal patients indicate direct relation to satisfaction as compared to other Hemodialysis centers particularly the number of patients continuously patronizing these sections for the treatment. Listening methods are supplemented with some modalities of patient fora such as the weekly Pre-transplant patient orientation and orientation to the service policies for new patients qualified under the Medical Social Service Division. Peritoneal Dialyis and Hemodialysis patients also conduct patient meeting for feedback and update.
Training services also utilizes Focus Group Discussions among its trainees and existing Institute employees in extracting new topics and programs to be conducted.
3.1b(3) Dissatisfaction. All approaches for gathering, analyzing, and reporting patient and member satisfaction and engagement data also serve to quantify dissatisfaction (3.1b(1)). Quantitative data come in the form of low scores, and qualitative data are derived from complaints and comments, focus groups, websites, social media and through verbal or telephone comments logged in the ticketing system of addressing complaints by CREAM and under the E3N Monitoring of the Nursing Services Department. Feedback Survey in determining Dissatisfaction employs the Ticketing System of complaint management. (Fig. 3.2-3, Steps 2-3). Complaint information from dissatisfaction comments in surveys is linked with various hospital units to increase patient satisfaction 3.1b(1). Complaint reports generated from CREAM
are shared with Leaders and concerned sections monthly to identify common themes. Those reports coming from the patient care areas are reported and dealt with during the weekly Nursing Audit and improvement plans are created for corrective and preventive purposes. Those that could not be resolved through the Ticketing System are being elevated to the NCPAR Team.
3.2 Customer and Citizen Engagement 3.2a(1) Health Care Service Offerings. CREAM Office has Marketing Research and Concierge Units. Marketing Research Unit conducts periodic research in assessing customer needs while they are in the hospital apart from their illness needs. Concierge Unit assesses and determines customer needs that apart from medical considerations. These non-medical needs identified had put up the Business Center of this CREAM offering services such as photocopy, fax, and taxi companies contact for transport home.
The CREAM and Sections use the Voice of the Customer Information to identify new or improved service offerings to attract new patients. Sections such as Hemodialysis and Peritoneal Dialysis and Marketing unit of CREAM use tailored approaches, such as patient meetings, to seek feedback for satisfaction and dissatisfaction and to identify opportunities for improvement.
Data gathered by the Management on health care utilization, customer listening and learning, and patient preferences guide determination of key patient and customer requirements. During the meetings of the leaders, they discuss these data to identify differences across customer segments and stages of patients’ relationship with us. This review enables the teams to design processes that respond to changing customer needs. For example, new buildings are constructed to accommodate patients identified on the allied medical cases apart from the renal diseases mandated in the Institute. Another

16 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
instance is the PPP availment of Linear Accelerator to accommodate majority of the medical cancer patients. Project of expanding the Hemodialysis section to be big enough to accommodate the increasing number of patients.
Training Services offers Continuous Professional Development sessions during the program aside from the basic course availed. Training graduates are placed on top priority among the applicants for employment and dependent on their ranking during the training course. Integration of other modalities of training is also employed in order to facilitate active learning and experience to the trainees. 3.2a(2) Customer and Citizen Support. Information and citizen support through different methods are available in different segments of customers of the Institute. These are all available through the Web & social Media, Patient/Family Orientation and Education through Fora, Television/Radio Advocacies on special occasions, and Community Outreach Programs. Feedback survey tools are still the key medium to elicit their opinions on the products and services and support provided by the hospital in all its services and expertise.
Fig.3.2-1: Patient and Citizen Support Mechanisms
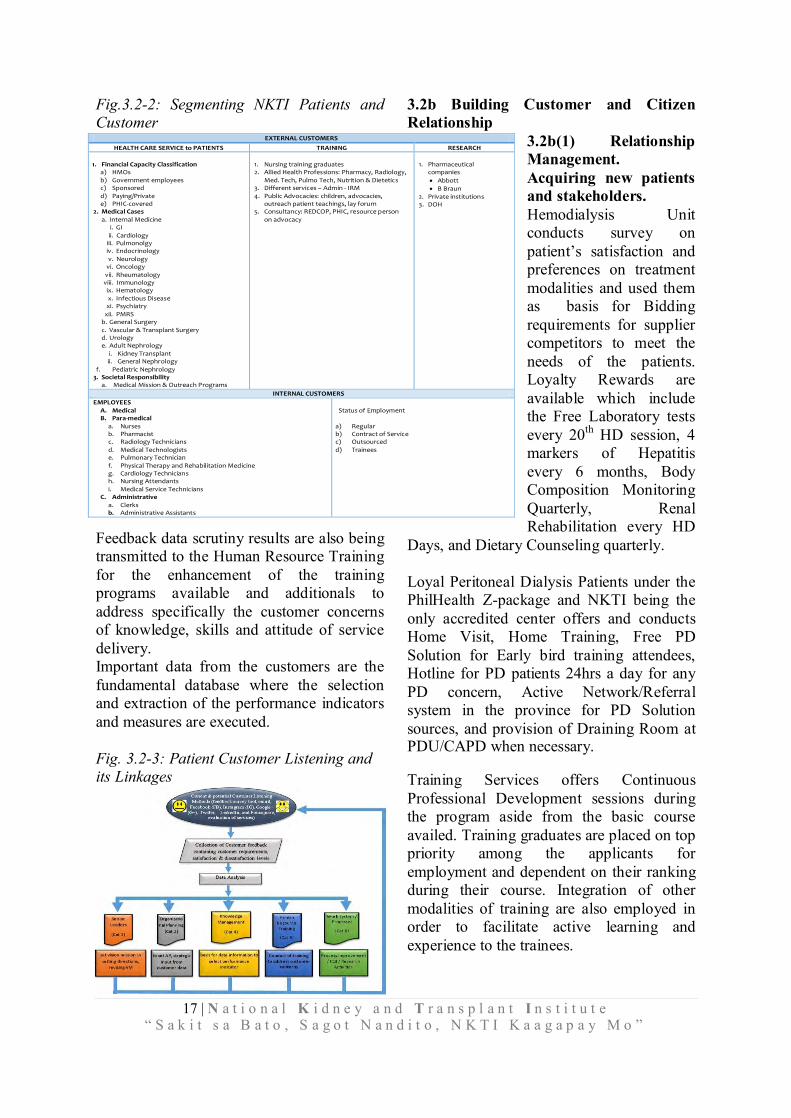
3.2a(3) Customer and Citizens Segmentation. Segmentation of the Institute’s customers is aligned with its expertise for service, training and research. Segmentation under the Service to patients includes the Financial Status, Medical Cases, In-patient and Out-patient. Training
encompasses the professionals and Research handles the pharmaceutical companies. 3.2a(4) Patient and Citizen Data Use. Patient Feedback Survey provides valuable revealing data, most highly and directly illustrating satisfaction. These data trigger service enhancement, modify work systems and process, and train people. Examples of using patient and market data to identify new segmented service offerings include:
1. 1. Building a Center for Urology and Men’s Health to accommodate patients with urologic problems that are closely linked with renal illnesses. This also shelters the Ambulatory Urology and GI endoscopy Center which caters on the outpatient surgical procedures. It also houses the iVasc Center for the Vascular Diseases determination and treatment. 2. Building of Diagnostic Center housing the state-of-the-art facilities and equipment of Radiologic Diagnostic Examinations to aid in the diagnosis of renal diseases and its allied health illnesses.
Data extracted from the listening methodologies from the current and potential customers that contain the satisfaction and dissatisfaction feedback are arranged to be analyzed. Results of this data analysis and interpretation are being fed to the management for the senior leaders to set and revise the vision and mission, and establish strategic directions Analyzed customer data are translated as direct input for the strategic planning of each department which can be evident in the setting of Action plan and performance measures.
METHOD STAKEHOLDERS SEEKING INFO.
STAKEHOLDERS UTILIZING SERVICES
Web & Social Media PT, PU, C PT, C
Patient/Family Orientation/Educ.
PT -
Television / Radio PT, PU, C -
Community Outreach PT, C PT, C
Stakeholders Key: PT = Patients & Family Members, PU = Purchasers,
C = Community Organizations
17 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
EXTERNAL CUSTOMERS
HEALTH CARE SERVICE to PATIENTS TRAINING RESEARCH
1. Financial Capacity Classification a) HMOs
b) Government employees c) Sponsored
d) Paying/Private e) PHIC-covered
2. Medical Cases
a. Internal Medicine i. GI
ii. Cardiology iii. Pulmonolgy iv. Endocrinology
v. Neurology vi. Oncology
vii. Rheumatology viii. Immunology ix. Hematology
x. Infectious Disease xi. Psychiatry
xii. PMRS b. General Surgery
c. Vascular & Transplant Surgery d. Urology e. Adult Nephrology
i. Kidney Transplant ii. General Nephrology
f. Pediatric Nephrology 3. Societal Responsibility
a. Medical Mission & Outreach Programs
1. Nursing training graduates 2. Allied Health Professions: Pharmacy, Radiology,
Med. Tech, Pulmo Tech, Nutrition & Dietetics 3. Different services – Admin - IRM
4. Public Advocacies: children, advocacies, outreach patient teachings, lay forum
5. Consultancy: REDCOP, PHIC, resource person
on advocacy
1. Pharmaceutical companies
Abbott
B Braun 2. Private institutions 3. DOH
INTERNAL CUSTOMERS
EMPLOYEES
A. Medical B. Para-medical
a. Nurses b. Pharmacist c. Radiology Technicians d. Medical Technologists e. Pulmonary Technician
f. Physical Therapy and Rehabilitation Medicine g. Cardiology Technicians h. Nursing Attendants
i. Medical Service Technicians C. Administrative
a. Clerks b. Administrative Assistants
Status of Employment
a) Regular b) Contract of Service c) Outsourced d) Trainees
Fig.3.2-2: Segmenting NKTI Patients and Customer
Feedback data scrutiny results are also being transmitted to the Human Resource Training for the enhancement of the training programs available and additionals to address specifically the customer concerns of knowledge, skills and attitude of service delivery. Important data from the customers are the fundamental database where the selection and extraction of the performance indicators and measures are executed. Fig. 3.2-3: Patient Customer Listening and its Linkages
3.2b Building Customer and Citizen Relationship
3.2b(1) Relationship Management. Acquiring new patients and stakeholders. Hemodialysis Unit conducts survey on patient’s satisfaction and preferences on treatment modalities and used them as basis for Bidding requirements for supplier competitors to meet the needs of the patients. Loyalty Rewards are available which include the Free Laboratory tests every 20th HD session, 4 markers of Hepatitis every 6 months, Body Composition Monitoring Quarterly, Renal Rehabilitation every HD
Days, and Dietary Counseling quarterly. Loyal Peritoneal Dialysis Patients under the PhilHealth Z-package and NKTI being the only accredited center offers and conducts Home Visit, Home Training, Free PD Solution for Early bird training attendees, Hotline for PD patients 24hrs a day for any PD concern, Active Network/Referral system in the province for PD Solution sources, and provision of Draining Room at PDU/CAPD when necessary.
Training Services offers Continuous Professional Development sessions during the program aside from the basic course availed. Training graduates are placed on top priority among the applicants for employment and dependent on their ranking during their course. Integration of other modalities of training are also employed in order to facilitate active learning and experience to the trainees.
18 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
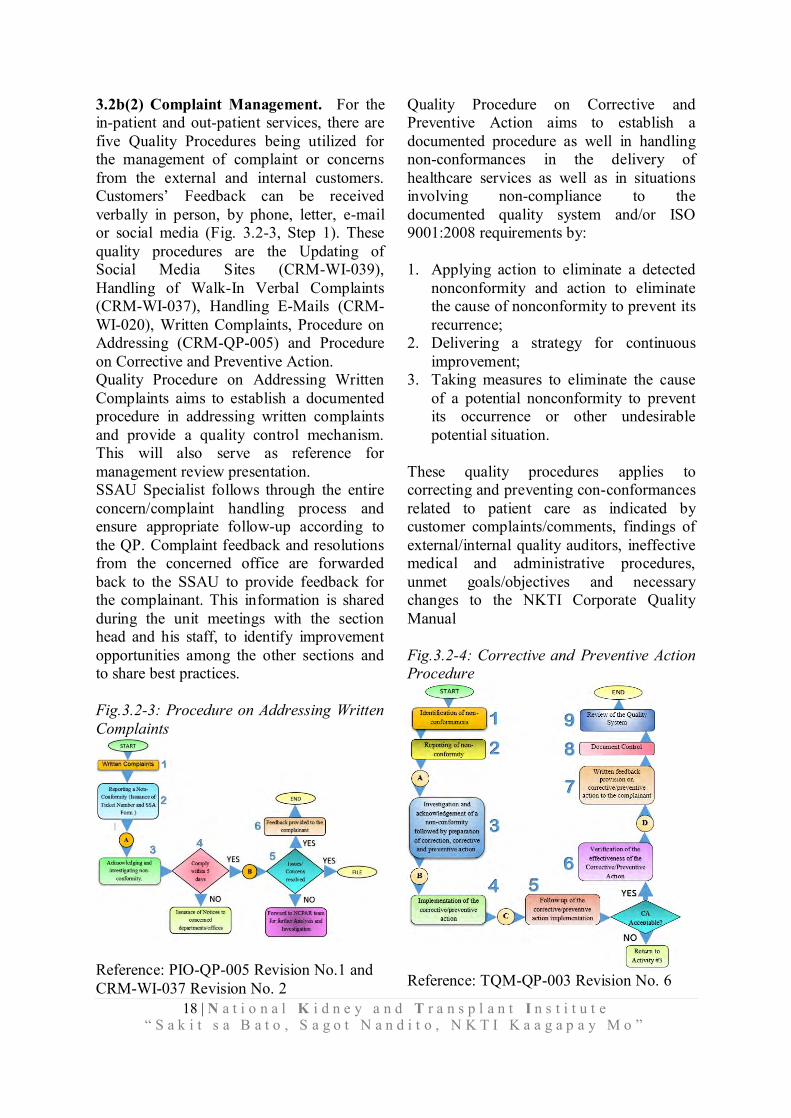
3.2b(2) Complaint Management. For the in-patient and out-patient services, there are five Quality Procedures being utilized for the management of complaint or concerns from the external and internal customers. Customers’ Feedback can be received verbally in person, by phone, letter, e-mail or social media (Fig. 3.2-3, Step 1). These quality procedures are the Updating of Social Media Sites (CRM-WI-039), Handling of Walk-In Verbal Complaints (CRM-WI-037), Handling E-Mails (CRM-WI-020), Written Complaints, Procedure on Addressing (CRM-QP-005) and Procedure on Corrective and Preventive Action. Quality Procedure on Addressing Written Complaints aims to establish a documented procedure in addressing written complaints and provide a quality control mechanism. This will also serve as reference for management review presentation. SSAU Specialist follows through the entire concern/complaint handling process and ensure appropriate follow-up according to the QP. Complaint feedback and resolutions from the concerned office are forwarded back to the SSAU to provide feedback for the complainant. This information is shared during the unit meetings with the section head and his staff, to identify improvement opportunities among the other sections and to share best practices. Fig.3.2-3: Procedure on Addressing Written Complaints
Reference: PIO-QP-005 Revision No.1 and CRM-WI-037 Revision No. 2
Quality Procedure on Corrective and Preventive Action aims to establish a documented procedure as well in handling non-conformances in the delivery of healthcare services as well as in situations involving non-compliance to the documented quality system and/or ISO 9001:2008 requirements by: 1. Applying action to eliminate a detected
nonconformity and action to eliminate the cause of nonconformity to prevent its recurrence;
2. Delivering a strategy for continuous improvement;
3. Taking measures to eliminate the cause of a potential nonconformity to prevent its occurrence or other undesirable potential situation.
These quality procedures applies to correcting and preventing con-conformances related to patient care as indicated by customer complaints/comments, findings of external/internal quality auditors, ineffective medical and administrative procedures, unmet goals/objectives and necessary changes to the NKTI Corporate Quality Manual Fig.3.2-4: Corrective and Preventive Action Procedure
Reference: TQM-QP-003 Revision No. 6
19 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
All employees are responsible for quality assurance. The Quality Management Representative (QMR) is responsible for ensuring that NKTI Quality Procedures are observed and root causes of any non-conformity are investigated and documented with appropriate corrective or preventive actions prescribed. Each department/division manager in turn is responsible for taking appropriate corrective actions in his/her area of responsibility. Non-conformance Corrective and Preventive Action Reports (NCPARs) can be directed within NKTI and to its suppliers. Initiation of an NCPAR may be proposed by anyone in the organization, but all NCPARs must be tracked and followed up. Tracking and follow-up of NCPARs is done through a computerized database administered by TQM Office. NCPAR can be used to deal with system deficiencies, ensure that problems are identified and investigated, undergo the process of root cause analysis, corrective and preventive actions must be identified, implemented, verified and validated for effectiveness. An NCPAR Team composed of a Chairperson and 4 members is organized to facilitate prompt and effective process review and implementation of the said process. In addition, Brand Development and Management Sub Unit Social Media Officer of CREAM monitors and updates the Social Media Sites where posts classified as concern or complaint of concerned persons related to NKTI are extracted. The concern/complaint is then logged into the Online Inquiry Logbook and provided with Ticket Number. This then follows the QP for Addressing Written Complaint Process to be followed through by the Social Media Officer.
NKTI mission and vision is accomplished and achieved through its ability to formulate judicious, sensible and informed decisions based on regular analysis of reliable and consistent data. 4.1 Measurement, Analysis, and Improvement of Organizational Performance 4.1a Performance Measurement. NKTI’s vision statement determines and guides the formulation of strategic objectives and action plans. Each strategic objectives has a set of performance indicators that describes the key performance measurements and traits used to measures process effectiveness and efficiencies. 4.1a(1) Performance Measures. Each department/division/office establishes its own strategic objectives and actions plans based on the institutes, strategic objectives. These, in turn, determine the selection of measures for monitoring and tracking of daily operations. Department Chairs /Division Chiefs establish the methods of data collection, targets and thresholds and accountability for results. These measures support the decision making a fundamental process of quality, efficiency, and effectiveness in each department/division/office on a continuous basis. Moreover, these measures allow changes to be made if the performance falls below the target. Overall performance of each department /division/office is reported to and reviewed by the Executive Committee (EC) or during the Management Committee (MC) meetings
CATEGORY 4. MEASUREMENT ANALYSIS, AND KNOWLEDGE
MANAGEMENT
20 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
which is done on a regular basis. This prompt action plans if necessary. The EC continue the PDCA cycle until targets are achieved.
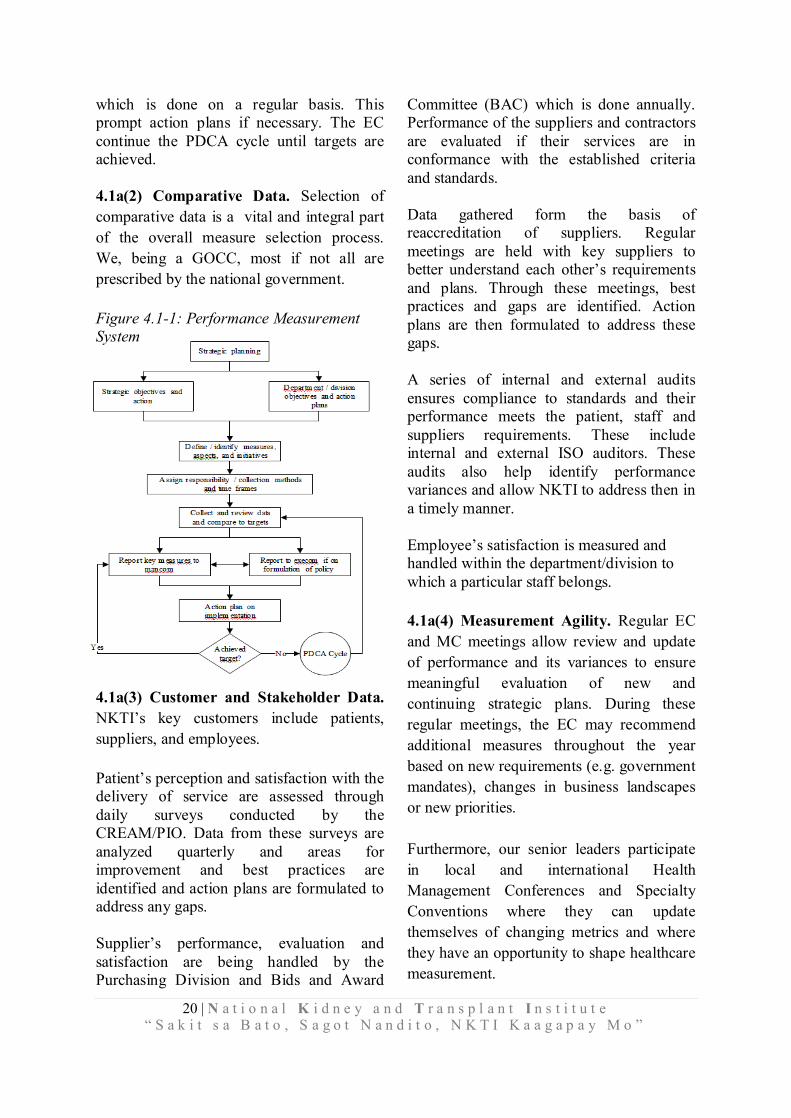
4.1a(2) Comparative Data. Selection of comparative data is a vital and integral part of the overall measure selection process. We, being a GOCC, most if not all are prescribed by the national government. Figure 4.1-1: Performance Measurement System
4.1a(3) Customer and Stakeholder Data. NKTI’s key customers include patients, suppliers, and employees. Patient’s perception and satisfaction with the delivery of service are assessed through daily surveys conducted by the CREAM/PIO. Data from these surveys are analyzed quarterly and areas for improvement and best practices are identified and action plans are formulated to address any gaps. Supplier’s performance, evaluation and satisfaction are being handled by the Purchasing Division and Bids and Award
Committee (BAC) which is done annually. Performance of the suppliers and contractors are evaluated if their services are in conformance with the established criteria and standards. Data gathered form the basis of reaccreditation of suppliers. Regular meetings are held with key suppliers to better understand each other’s requirements and plans. Through these meetings, best practices and gaps are identified. Action plans are then formulated to address these gaps. A series of internal and external audits ensures compliance to standards and their performance meets the patient, staff and suppliers requirements. These include internal and external ISO auditors. These audits also help identify performance variances and allow NKTI to address then in a timely manner. Employee’s satisfaction is measured and handled within the department/division to which a particular staff belongs. 4.1a(4) Measurement Agility. Regular EC and MC meetings allow review and update of performance and its variances to ensure meaningful evaluation of new and continuing strategic plans. During these regular meetings, the EC may recommend additional measures throughout the year based on new requirements (e.g. government mandates), changes in business landscapes or new priorities. Furthermore, our senior leaders participate in local and international Health Management Conferences and Specialty Conventions where they can update themselves of changing metrics and where they have an opportunity to shape healthcare measurement.
21 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
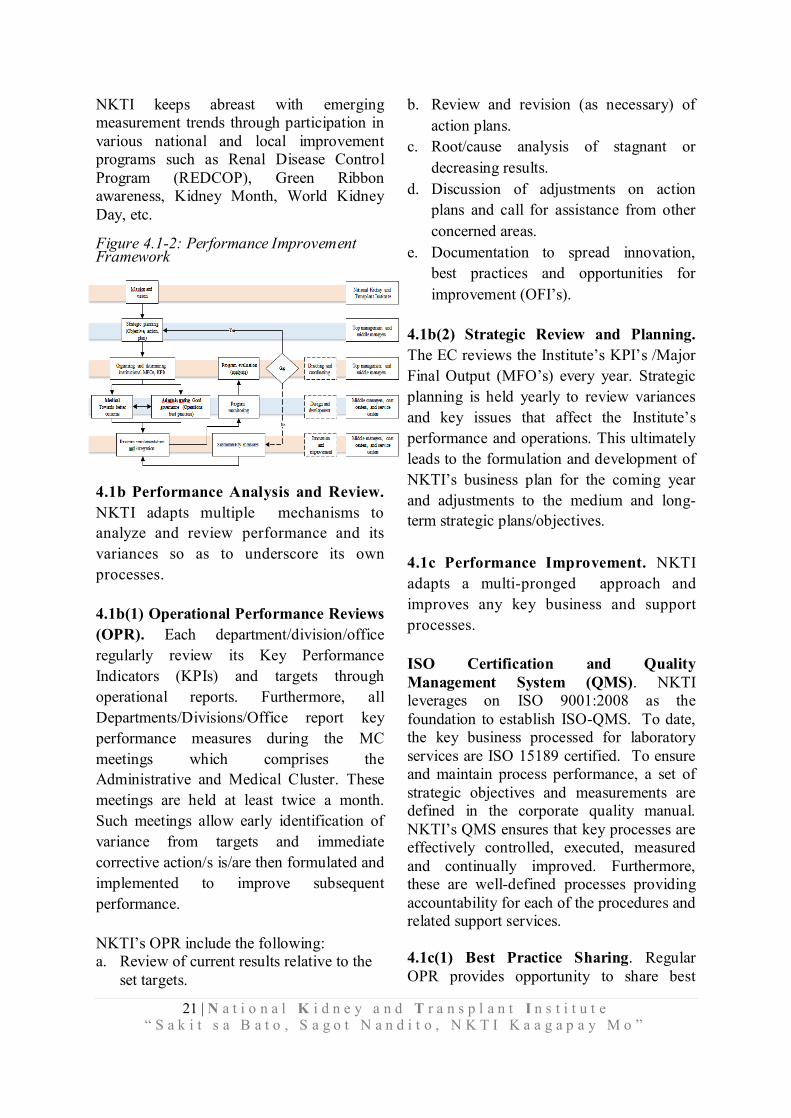
NKTI keeps abreast with emerging measurement trends through participation in various national and local improvement programs such as Renal Disease Control Program (REDCOP), Green Ribbon awareness, Kidney Month, World Kidney Day, etc. Figure 4.1-2: Performance Improvement Framework
4.1b Performance Analysis and Review. NKTI adapts multiple mechanisms to analyze and review performance and its variances so as to underscore its own processes. 4.1b(1) Operational Performance Reviews (OPR). Each department/division/office regularly review its Key Performance Indicators (KPIs) and targets through operational reports. Furthermore, all Departments/Divisions/Office report key performance measures during the MC meetings which comprises the Administrative and Medical Cluster. These meetings are held at least twice a month. Such meetings allow early identification of variance from targets and immediate corrective action/s is/are then formulated and implemented to improve subsequent performance. NKTI’s OPR include the following: a. Review of current results relative to the
set targets.
b. Review and revision (as necessary) of action plans.
c. Root/cause analysis of stagnant or decreasing results.
d. Discussion of adjustments on action plans and call for assistance from other concerned areas.
e. Documentation to spread innovation, best practices and opportunities for improvement (OFI’s).
4.1b(2) Strategic Review and Planning. The EC reviews the Institute’s KPI’s /Major Final Output (MFO’s) every year. Strategic planning is held yearly to review variances and key issues that affect the Institute’s performance and operations. This ultimately leads to the formulation and development of NKTI’s business plan for the coming year and adjustments to the medium and long-term strategic plans/objectives. 4.1c Performance Improvement. NKTI adapts a multi-pronged approach and improves any key business and support processes. ISO Certification and Quality Management System (QMS). NKTI leverages on ISO 9001:2008 as the foundation to establish ISO-QMS. To date, the key business processed for laboratory services are ISO 15189 certified. To ensure and maintain process performance, a set of strategic objectives and measurements are defined in the corporate quality manual. NKTI’s QMS ensures that key processes are effectively controlled, executed, measured and continually improved. Furthermore, these are well-defined processes providing accountability for each of the procedures and related support services. 4.1c(1) Best Practice Sharing. Regular OPR provides opportunity to share best

22 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
practices among departments/divisions/cost centers that ultimately leads to continuous improvement and innovation. During regular operations audit, each division/department/office reports monthly accomplishments, challenges encountered and how it was resolved. In this meeting, when the key performance indicators were met by the department/division/office, the EC decides on the possibility of expansion of services. Gaps are also monitored by the Middle Managers to ensure that individual outputs are aligned to action plans. Intervening variables are also identified for policy improvement. Best practices are shared with other departments and reported to MC on a quarterly basis. 4.1c(2) Future Performance. Action planning process is used to project expected levels of performance and targets of the Institute. The various data from regular conduct of OPR during MC meetings are used to project future performance and targets for the following year/s, as well as customer, supplies and other external requirements (e.g. data gathered from environmental scan, government mandates and regulations). 4.1c(3) Continuous Improvement and Innovation. OPR at every level provide opportunities to identify innovation breakthrough improvements to achieve our strategic objectives. As new strategic objective/s is/are developed and ongoing strategic objectives are modified (which is usually done on an annual basis, but new strategies can be adopted throughout the year as necessary), the concerned teams are given the responsibilities to develop action
plans to support short and long-term strategic objectives. New initiatives are cascaded to all Heads/Chiefs of the departments/divisions/offices during MC meetings which are then cascaded to the rest of the staff.
Other sources of innovative ideas include various industry or professional society conferences attended by both the medical and administrative teams, on-going market scanning, benchmarking by the various cost centers as well as from the business advisers of the Institute. New initiatives or modification of existing initiatives are likewise shared, discussed and clarified with our partners and suppliers with emphasis to their roles in effecting change and update. NKTI like any other business are under continuous pressure to improve the quality of care and achieve best health outcomes. NKTI adopted the quality management best practices to ensure that our services to patients meet the highest quality standards possible. Medical and administrative staff are committed and dedicated to continuously improve quality. When a problem or opportunity for improvement is identified, a group of employees or the concerned department/division/office clearly defines the issue, collects data and information and formulates possible solutions. Once approved, they implement the change and continuously measure if the change made an improvement. Through this process, NKTI employees are striving to our goal of “Excellence Everyday”.
23 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
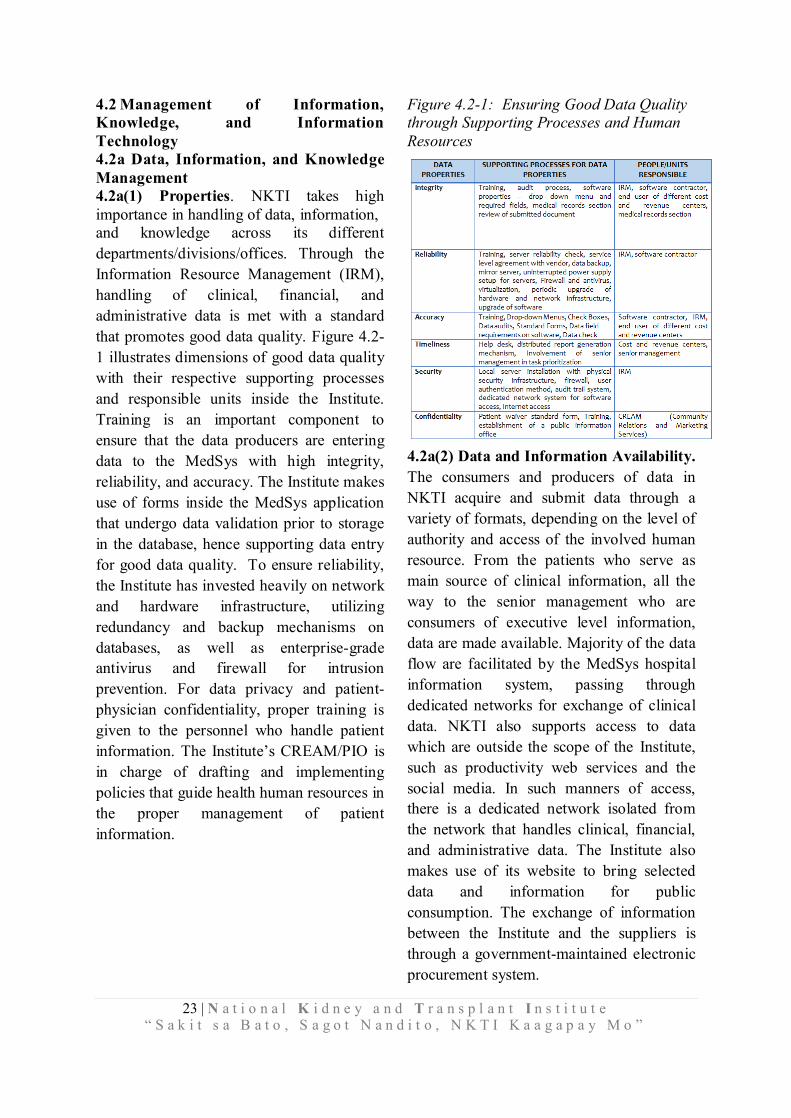
4.2 Management of Information, Knowledge, and Information Technology 4.2a Data, Information, and Knowledge Management 4.2a(1) Properties. NKTI takes high importance in handling of data, information, and knowledge across its different departments/divisions/offices. Through the Information Resource Management (IRM), handling of clinical, financial, and administrative data is met with a standard that promotes good data quality. Figure 4.2-1 illustrates dimensions of good data quality with their respective supporting processes and responsible units inside the Institute. Training is an important component to ensure that the data producers are entering data to the MedSys with high integrity, reliability, and accuracy. The Institute makes use of forms inside the MedSys application that undergo data validation prior to storage in the database, hence supporting data entry for good data quality. To ensure reliability, the Institute has invested heavily on network and hardware infrastructure, utilizing redundancy and backup mechanisms on databases, as well as enterprise-grade antivirus and firewall for intrusion prevention. For data privacy and patient-physician confidentiality, proper training is given to the personnel who handle patient information. The Institute’s CREAM/PIO is in charge of drafting and implementing policies that guide health human resources in the proper management of patient information.
Figure 4.2-1: Ensuring Good Data Quality through Supporting Processes and Human Resources
4.2a(2) Data and Information Availability. The consumers and producers of data in NKTI acquire and submit data through a variety of formats, depending on the level of authority and access of the involved human resource. From the patients who serve as main source of clinical information, all the way to the senior management who are consumers of executive level information, data are made available. Majority of the data flow are facilitated by the MedSys hospital information system, passing through dedicated networks for exchange of clinical data. NKTI also supports access to data which are outside the scope of the Institute, such as productivity web services and the social media. In such manners of access, there is a dedicated network isolated from the network that handles clinical, financial, and administrative data. The Institute also makes use of its website to bring selected data and information for public consumption. The exchange of information between the Institute and the suppliers is through a government-maintained electronic procurement system.

24 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Figure 4.2-2: Matrix for Data and Information Availability
4.2a(3) Knowledge Management. In the management of knowledge, the Institute implements a distribution and aggregation system through a local knowledge management system, hosted in the data center of the Institute. The local repositories are organized according to knowledge base and are accessible depending on the departments that would need the particular knowledge. For example, the Institute has housed a local repository for the use of a Free and Open Source Software (FOSS) document processing. This tutorial set has since been made available for all departments that are using the FOSS document processor. Identification of best practices is done through documentation of regular department, executive, and management meetings. For such best practice methods that are applicable to a wider audience, memos are issued. Implementation of best practice methods are done using change management processes, which could be either short- or long-term depending on the scope and coverage of such best practice. Fig. 4.2-3 describes the different processes used to manage knowledge from the Institute’s data and information.
Fig.4.2-3: Processes for Managing Knowledge from Data Analyzed
4.2b Management of Information Resources and Technology 4.2b(1) Hardware and Software Properties. Management of hardware and software assets are centralized through the IRM. The network administrator is in charge of ensuring reliability of the hardware and network components of the Institute. By placing monitoring systems and ensuring redundancy of access, data is ensured to be accessible at all times. A member of the IRM technical staff conducts a quarterly preventive maintenance on all computers installed in the Institute. IRM ensures that all Operating System used in the Institute are genuine (Windows, Office productivity tools), and are evaluated for software reliability. The software applications are selected based on their capacity to fulfill functions on an enterprise level. A licensed anti-virus is installed in every single computer to protect from viruses. Validity of software applications are maintained through a registry of licenses. In non-mission critical areas of the Institute, the IRM promotes the use of FOSS. This application allows the Institute to perform efficient appropriation and allocation of resources, specifically for procurement of enterprise licenses. By allotting enterprise licenses to selected departments, the Institute can procure the best of class while using FOSS alternatives for the other departments.
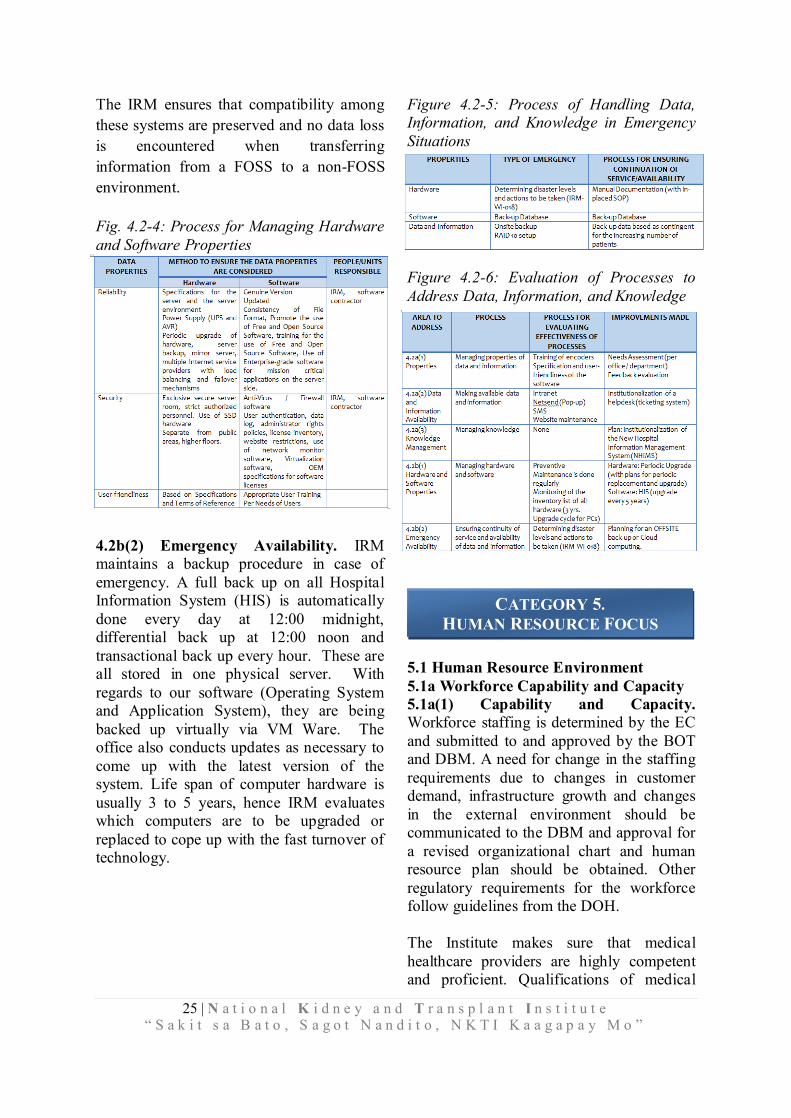
25 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
The IRM ensures that compatibility among these systems are preserved and no data loss is encountered when transferring information from a FOSS to a non-FOSS environment. Fig. 4.2-4: Process for Managing Hardware and Software Properties
4.2b(2) Emergency Availability. IRM maintains a backup procedure in case of emergency. A full back up on all Hospital Information System (HIS) is automatically done every day at 12:00 midnight, differential back up at 12:00 noon and transactional back up every hour. These are all stored in one physical server. With regards to our software (Operating System and Application System), they are being backed up virtually via VM Ware. The office also conducts updates as necessary to come up with the latest version of the system. Life span of computer hardware is usually 3 to 5 years, hence IRM evaluates which computers are to be upgraded or replaced to cope up with the fast turnover of technology.
Figure 4.2-5: Process of Handling Data, Information, and Knowledge in Emergency Situations
Figure 4.2-6: Evaluation of Processes to Address Data, Information, and Knowledge
5.1 Human Resource Environment 5.1a Workforce Capability and Capacity 5.1a(1) Capability and Capacity. Workforce staffing is determined by the EC and submitted to and approved by the BOT and DBM. A need for change in the staffing requirements due to changes in customer demand, infrastructure growth and changes in the external environment should be communicated to the DBM and approval for a revised organizational chart and human resource plan should be obtained. Other regulatory requirements for the workforce follow guidelines from the DOH. The Institute makes sure that medical healthcare providers are highly competent and proficient. Qualifications of medical
CATEGORY 5. HUMAN RESOURCE FOCUS
26 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
healthcare providers are determined by the Office of the Deputy Director for Medical Services. Once approved, they are privileged to practice in the Institute and follow a tenure of practice based on the “Rules and Regulations of the Medical Staff and Policies and Guidelines on Private Practice” and DOH guidelines of private medical practice. Nursing competency requirements are determined by the Nursing Service Office (NSO). Civil service qualification standards are followed for administrative personnel. 5.1a(2) New Members of the Organization. Recruitment and Hiring. NKTI has highly trained medical staff who are also connected with other medical training institutions. They are able to continually attract new graduates of medical subspecialty programs to apply and practice in our Institute. Other methods of recruitment include internal referrals, newspaper postings, internship or externship program and on-the-job training tie ups with the DOH, and schools of allied healthcare. For nursing and paramedical staff, the Institute offers a 4-month training known as Basic Nephrology for Nurses (BNN). Other trainings include externship for medical technologists, pharmacists, dietitians which serve as a pool of applicants for manpower requirements. Retention. The Institute promotes retention through a robust reward system in partnership with the Program on Awards and Incentives for Service Excellence (PRAISE) Committee which recognizes model employees annually, and grant loyalty and perfect attendance awards to employees.
5.1a(3) Work Accomplishment. NKTI organizes and manages employees in accomplishing the Institute’s work by preparing the Office Performance Commitment Review (OPCR) Form that is anchored to its vision and mission. OPCR
is a tool in measuring the department/division/office’s performance as well as indicator if work targets are accomplished. The OPCR is cascaded from the Institute’s Head down to the departments/divisions/offices then to each personnel in the form of Individual Performance Commitment Review (IPCR). The OPCR and IPCR together with the action plans formulated by each department/division /office have set targets and parameters to ensure that these are achieved. The IPCR which focuses on workforce performance is linked to Performance Based Bonus (PBB). PBB, which is a form of reward, motivates the accomplishment of work and in a way encourages employees to surpass what has been targeted. This is in support to DBM’s memorandum circular No. 2012-02 dated October 16, 2012. NKTI also addresses its strategic challenges through organizational performance as evident in Major Final Output Accountability Report Card I (MARC I) and Management Accountability Report Card II and (MARC II) which are displayed in the Institute’s main lobby. In addition, there is the management review which is conducted semi-annually. 5.1a(4) Human Resource Change Management. NKTI through the HRMD ensures that it will be able to respond to its current and emerging capability and capacity needs relative to workforce requirements. An Annual Procurement Program (APP) is prepared by each office to enlist all supplies, materials, and equipment which includes manpower requirement. The APP is consolidated by the Budget Office and is recommended for approval by the Executive Director. HRMD works on manpower requirement and sees to it that this is properly budgeted and workforce development is addressed. Around 5% of the Personal Services Budget (PSB) is allotted to training and development. Figure 5.1a(4)
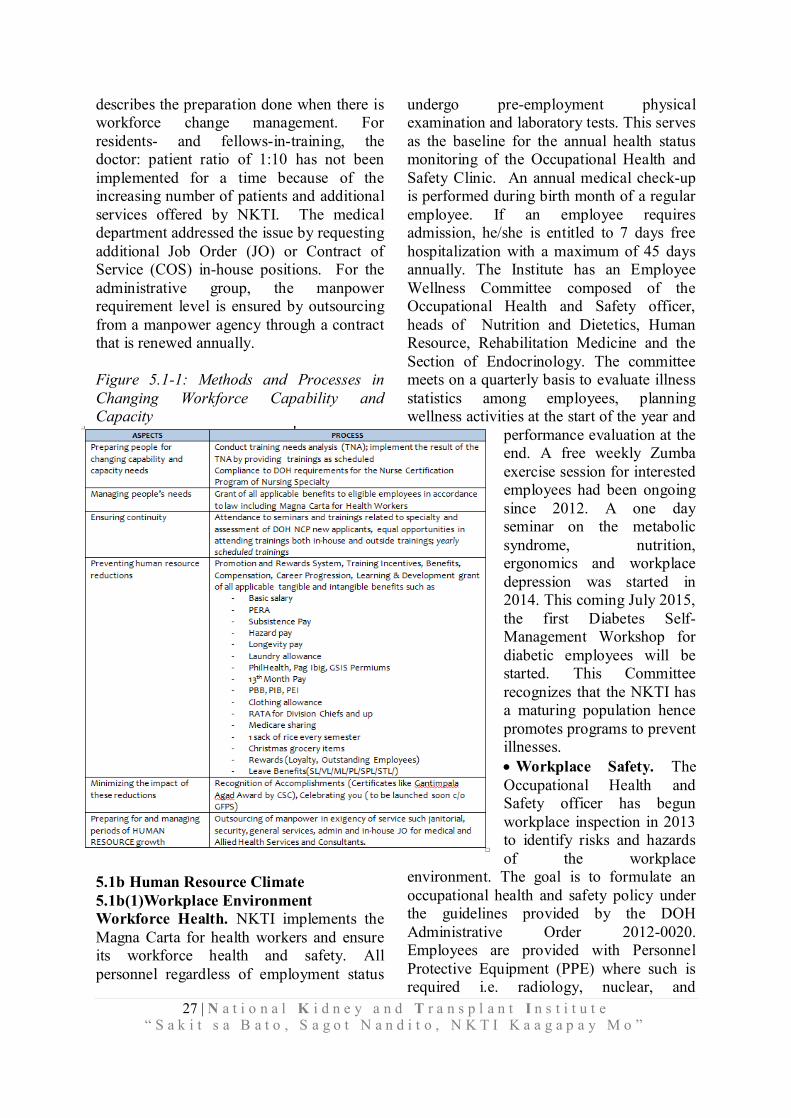
27 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
describes the preparation done when there is workforce change management. For residents- and fellows-in-training, the doctor: patient ratio of 1:10 has not been implemented for a time because of the increasing number of patients and additional services offered by NKTI. The medical department addressed the issue by requesting additional Job Order (JO) or Contract of Service (COS) in-house positions. For the administrative group, the manpower requirement level is ensured by outsourcing from a manpower agency through a contract that is renewed annually. Figure 5.1-1: Methods and Processes in Changing Workforce Capability and Capacity
5.1b Human Resource Climate 5.1b(1)Workplace Environment Workforce Health. NKTI implements the Magna Carta for health workers and ensure its workforce health and safety. All personnel regardless of employment status
undergo pre-employment physical examination and laboratory tests. This serves as the baseline for the annual health status monitoring of the Occupational Health and Safety Clinic. An annual medical check-up is performed during birth month of a regular employee. If an employee requires admission, he/she is entitled to 7 days free hospitalization with a maximum of 45 days annually. The Institute has an Employee Wellness Committee composed of the Occupational Health and Safety officer, heads of Nutrition and Dietetics, Human Resource, Rehabilitation Medicine and the Section of Endocrinology. The committee meets on a quarterly basis to evaluate illness statistics among employees, planning wellness activities at the start of the year and
performance evaluation at the end. A free weekly Zumba exercise session for interested employees had been ongoing since 2012. A one day seminar on the metabolic syndrome, nutrition, ergonomics and workplace depression was started in 2014. This coming July 2015, the first Diabetes Self-Management Workshop for diabetic employees will be started. This Committee recognizes that the NKTI has a maturing population hence promotes programs to prevent illnesses. Workplace Safety. The Occupational Health and Safety officer has begun workplace inspection in 2013 to identify risks and hazards of the workplace
environment. The goal is to formulate an occupational health and safety policy under the guidelines provided by the DOH Administrative Order 2012-0020. Employees are provided with Personnel Protective Equipment (PPE) where such is required i.e. radiology, nuclear, and
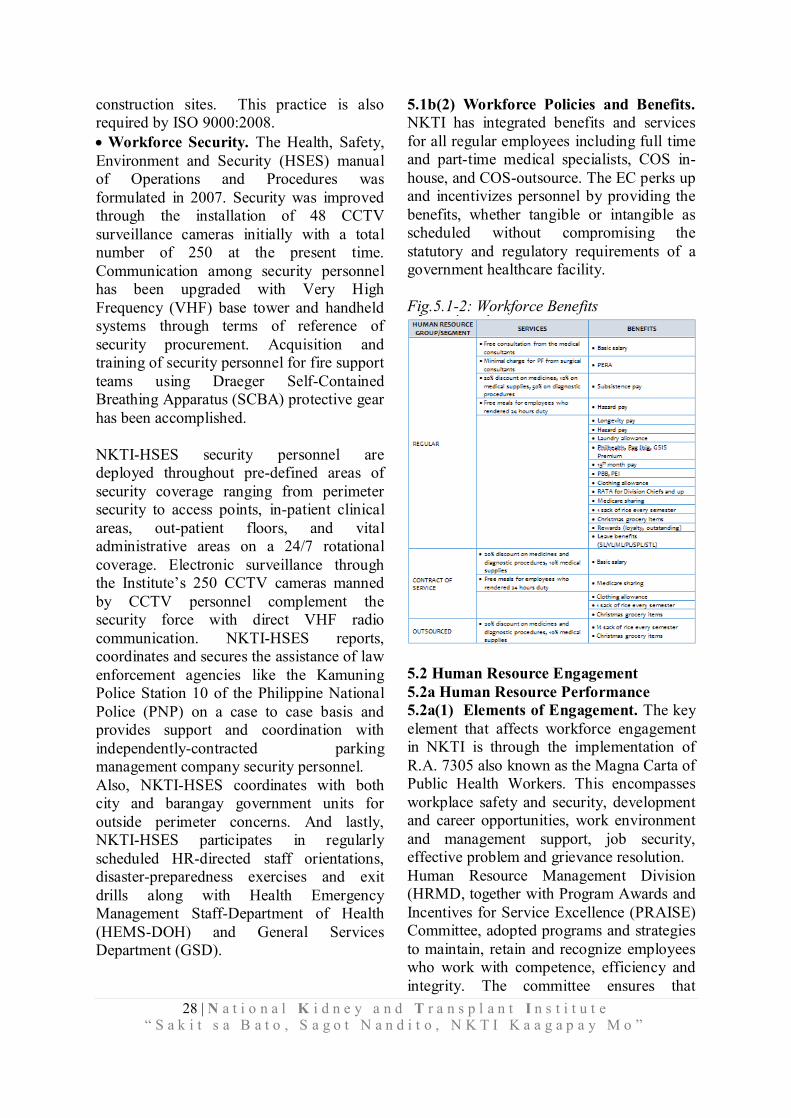
28 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
construction sites. This practice is also required by ISO 9000:2008. Workforce Security. The Health, Safety, Environment and Security (HSES) manual of Operations and Procedures was formulated in 2007. Security was improved through the installation of 48 CCTV surveillance cameras initially with a total number of 250 at the present time. Communication among security personnel has been upgraded with Very High Frequency (VHF) base tower and handheld systems through terms of reference of security procurement. Acquisition and training of security personnel for fire support teams using Draeger Self-Contained Breathing Apparatus (SCBA) protective gear has been accomplished. NKTI-HSES security personnel are deployed throughout pre-defined areas of security coverage ranging from perimeter security to access points, in-patient clinical areas, out-patient floors, and vital administrative areas on a 24/7 rotational coverage. Electronic surveillance through the Institute’s 250 CCTV cameras manned by CCTV personnel complement the security force with direct VHF radio communication. NKTI-HSES reports, coordinates and secures the assistance of law enforcement agencies like the Kamuning Police Station 10 of the Philippine National Police (PNP) on a case to case basis and provides support and coordination with independently-contracted parking management company security personnel. Also, NKTI-HSES coordinates with both city and barangay government units for outside perimeter concerns. And lastly, NKTI-HSES participates in regularly scheduled HR-directed staff orientations, disaster-preparedness exercises and exit drills along with Health Emergency Management Staff-Department of Health (HEMS-DOH) and General Services Department (GSD).
5.1b(2) Workforce Policies and Benefits. NKTI has integrated benefits and services for all regular employees including full time and part-time medical specialists, COS in-house, and COS-outsource. The EC perks up and incentivizes personnel by providing the benefits, whether tangible or intangible as scheduled without compromising the statutory and regulatory requirements of a government healthcare facility. Fig.5.1-2: Workforce Benefits
5.2 Human Resource Engagement 5.2a Human Resource Performance 5.2a(1) Elements of Engagement. The key element that affects workforce engagement in NKTI is through the implementation of R.A. 7305 also known as the Magna Carta of Public Health Workers. This encompasses workplace safety and security, development and career opportunities, work environment and management support, job security, effective problem and grievance resolution. Human Resource Management Division (HRMD, together with Program Awards and Incentives for Service Excellence (PRAISE) Committee, adopted programs and strategies to maintain, retain and recognize employees who work with competence, efficiency and integrity. The committee ensures that
29 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
incentives and awards are provided based on their performance, innovative ideas and exemplary behavior. 5.2a(2) Organizational Culture. Aligned with its vision and mission, NKTI has been active in the pursuit of quality management since the late 90’s. The Total Quality Management advocacy which was formally launched on March 28, 2001, was a defining milestone in the delivery of quality healthcare. As supported by the Institute’s “quality policy” and “quality objectives”, service quality is maintained in all areas. The pursuit of excellence and nurtured by the ISO environment has now propelled the Institution towards working for the Philippine Quality Award. The journey towards business excellence is tough but with the dedicated leaders and workforce it is an achievable prize. The Nursing Service has also been active in continuing quality initiatives (CQI) to improve the patient safety environment. The E3N Care Program (Efficient, Effective and Equitable Nursing Care Program) notably includes evaluating and monitoring the common types of patient related incidents, improving communication lines and reducing turnaround time in addressing corrective measures. The EC and MC conduct monthly meetings with the heads of the medical, nursing and administrative departments. These meetings aimed to know the accomplishments, problems and suggestions from each area. A lobby exhibit highlighting the accomplishments of each department as well as core services such as advanced surgical and diagnostic services is held every month. The Institute also celebrates the “Kidney Month” every June. In addition, outreach program such as free laboratory services, blood letting, tree planting and media collaborations are held.
Employees are allowed to form cooperatives and a collective negotiations agreement has been forged with the employee union. It is the Management’s aspiration to encourage the medical staff to let their patients avail the Institute’s services. Hence, they ensure unceasing facility and equipment enhancement and development so as to continually engage the medical practitioners in delivering the best and quality care to the patients. 5.2a(3) Performance Management. High Performance Work and Engagement. In the past, the annual employee evaluation was achieved through the Performance Evaluation System (PES). Last March 2012, the Strategic Performance Management System (SPMS) was introduced by the Civil Service Commission (CSC) and in November of 2014, the Institute’s SPMS was approved by CSC and its implementation began this year. It is envisioned that through this system employees will be able to link individual with organizational goals resulting in better performance and organizational productivity. Last January 2015, the Institute’s Office Performance Commitment Review (OPCR) and Individual Performance Commitment Review (IPCR) were finished in which office and individual performance reports were submitted to HR. Four orientation meetings were held on the SPMS to help office heads and employees accomplish their OPCRs and IPCR. It is stressed that mentoring and coaching should be ongoing for the whole year. By year end performance review will be done and evaluated based on the strategic objectives for the year. Patient, Stakeholder and Healthcare Focus. Performance monitoring ensures that improvements are always being done to improve the quality of care. Innovations and improvements lead to satisfied patients who will use the Institute’s services again if needed.

30 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Compensation, Rewards, Recognition. The PRAISE committee gives yearly awards to high performers in the organization. Good performance is also recognized through step increments for plantilla levels and continuing education is encouraged through scholarship grants. Other awards include the Loyalty, Perfect Attendance and Best Employee Award. Fig. 5.2-1: Total Performance Management Cycle
5.2b Assessment of Human Resource Engagement. 5.2b(1) Assessment of Engagement. HRMD engagement is assessed through patient admissions of active medical consultants and regular meetings such as the medical-surgical staff meetings, general assembly for employees, participation in organization events (e.g. Kidney Month, annual Christmas celebrations), individual and group interviews. A one-time project on employee engagement in April 2013 with the Ateneo’s Center of Research and Development (CORD) utilizing focus group discussions revealed that employee engagement in the Institution is driven by rewards and recognition, management support, association with a good organization, good working relationships with co-workers. 5.2b(2) Correlation with Business Results. Patient admissions and utilization of Institute’s services of active consultants reflect medical staff engagement and satisfaction with the Institute’s organization. These data are regularly discussed in the medical-surgical staff meetings with the
Executive Director and other leaders of the organization. 5.2c. Human Resource and Leader Development 5.2c(1)Learning and Development System. There are about 108 medical residents and fellows under training in the Institute. The Institution’s goal is a 90% pass rate for the subspecialty board examination. For nurses and other paramedical staff, NKTI developed and established the Institute of Advanced Nursing and Allied Health Professions (IANAHP). IANAHP is envisioned to provide and equip the nursing and paramedical staff the necessary training, exposure and skills based on globally accepted standards. Administrative staff also undergoes continuous trainings on quality customer service, gender and development, information systems and patient safety. 5.2c(2) Learning and Development Effectiveness. Medical and nursing departments have competency evaluations for their trainees. Medical subspecialty trainees take the subspecialty board examination after they complete their training in the Institute. Performance in the department is evaluated and they take the subspecialty examination after completion of the required years of training. For administrative staff, learning effectiveness is measured by the module and speakers evaluation by the participants. Likewise, the participants are given exit examinations or return demonstrations to assess and measure what they learned from the modules. In Delivering Quality Service Seminar, the Training and Development Section (TDS) are distributing Training Effectiveness Form to supervisors of the participants three months after they attended the seminar. The objectives are to assess the improvement and changes in delivering services of the

31 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
attendees and to ask training feedbacks and suggestions from the supervisors. 5.2c(3) Career Progression. The executive and management committee discusses succession planning and career progression and decides on training as appropriate.
NKTI anchors its operation on its mandate; guided by the vision, mission, and strengthened by our core competencies. Our work systems involve human resources, partners, key suppliers and contractors and other components of the supply chain needed to produce and deliver our services and support processes. 6.1 Work Systems 6.1a. Work System Design 6.1a(1) Design Concepts. NKTI designs and innovates overall work system dependent on the need of its patients and other stakeholders using a PDCA model through a cycle of learning and improvement. (Fig. 6.1-1).
It emanates from researches, new technologies, competitive market, benchmarking, and/or as required by the government anchored with its mandate and vision, mission, and objective (VMO). Our mission of healthcare, training, and research laid the foundation of our systems and processes. Each department defines its need
and designs requirements following the ISO standards. A feasibility study is presented to the EC for review and approval. If there are necessary changes and adjustments, redesigning will then be instituted. Technical Working Group (TWG) will then be created for the specificity, identification, and validation of the required needs based from the indicated requirements submitted by the department. The EC decides which system processes to outsource depending on the key considerations. External resources are utilized when the requirement exceeds internal capacity, cost capability or when the external provider can perform more efficiently and effectively in terms of preventive maintenance and machine/ equipment’ fast turn over. For example, the Institute outsources manpower services including General Services Division (GSD), Security, and Housekeeping for janitorial service and linen. (Fig. 6.1-2) Some system processes uses both internal and external resource like the Institute’s HD Center-PPP involving engagement of a private sector through a lease contract to provide top of the line and state of the art
HD equipment for the management and treatment of ESRD and other renal-related diseases. This partnership strategy allows the provision for the highest dialysis facility wherein the Institute provides the space and staffing component and wherein the winning proponent supplements the rest of the HD Center’s needs that is beyond its internal capacity such as HD machines, equipment, supplies, solutions, furniture, fixtures,
preventive maintenance, and calibration. It was the first PPP model in health care recognized globally and the country’s model for other government and private dialysis facilities. The Institute’s HD Center received an award of recognition as one of the Best Model of PPP in Health and one of the top 10 Best PPP projects by the World Bank in Washington DC, USA dated April 16, 2013.
CATEGORY 6. OPERATIONS FOCUS
Figure 6.1-1: PDCA Cycle, Work System Framework.
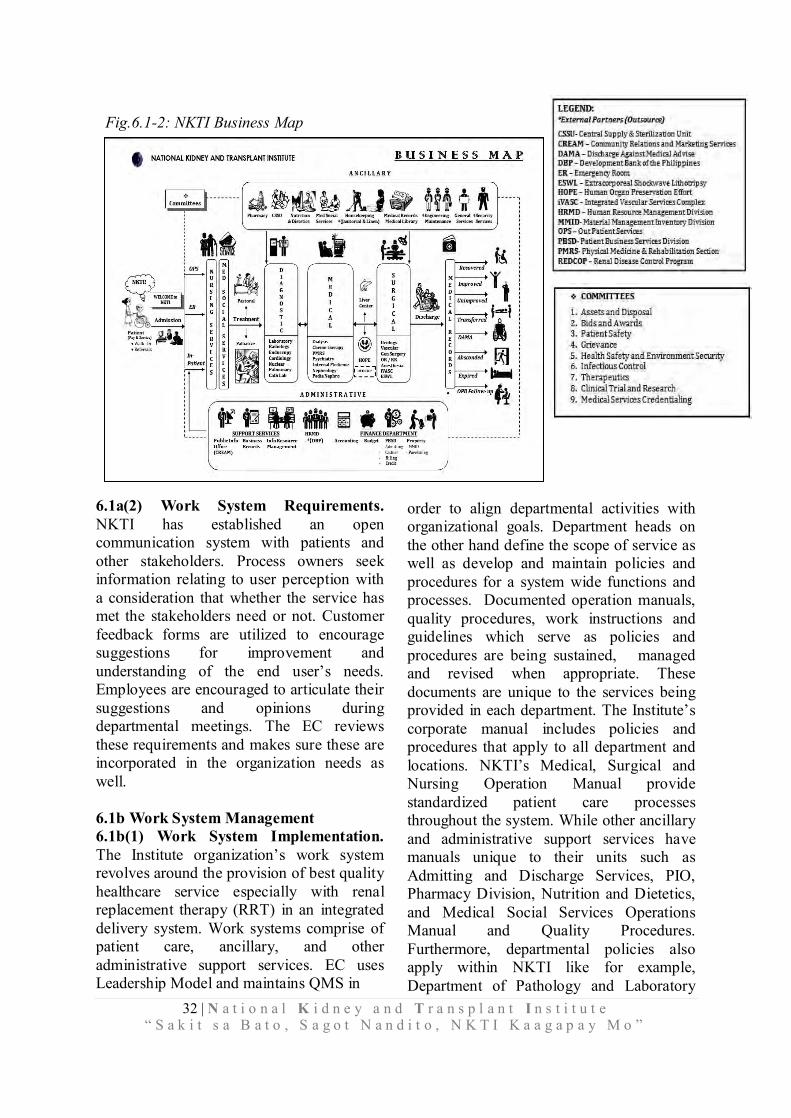
32 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
6.1a(2) Work System Requirements. NKTI has established an open communication system with patients and other stakeholders. Process owners seek information relating to user perception with a consideration that whether the service has met the stakeholders need or not. Customer feedback forms are utilized to encourage suggestions for improvement and understanding of the end user’s needs. Employees are encouraged to articulate their suggestions and opinions during departmental meetings. The EC reviews these requirements and makes sure these are incorporated in the organization needs as well.
6.1b Work System Management 6.1b(1) Work System Implementation. The Institute organization’s work system revolves around the provision of best quality healthcare service especially with renal replacement therapy (RRT) in an integrated delivery system. Work systems comprise of patient care, ancillary, and other administrative support services. EC uses Leadership Model and maintains QMS in
order to align departmental activities with organizational goals. Department heads on the other hand define the scope of service as well as develop and maintain policies and procedures for a system wide functions and processes. Documented operation manuals, quality procedures, work instructions and guidelines which serve as policies and procedures are being sustained, managed and revised when appropriate. These documents are unique to the services being provided in each department. The Institute’s corporate manual includes policies and procedures that apply to all department and locations. NKTI’s Medical, Surgical and Nursing Operation Manual provide standardized patient care processes throughout the system. While other ancillary and administrative support services have manuals unique to their units such as Admitting and Discharge Services, PIO, Pharmacy Division, Nutrition and Dietetics, and Medical Social Services Operations Manual and Quality Procedures. Furthermore, departmental policies also apply within NKTI like for example, Department of Pathology and Laboratory
Fig.6.1-2: NKTI Business Map

33 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Medicine and Nursing Services Department Special Orders which are being instituted consistently across all laboratory sections and nursing units respectively.
6.1b(2) Cost Control. NKTI controls overall work systems cost. This is by reducing errors and complaints, streamline step of work, monitoring supplies consumption, integrated 7S dissemination, and decreasing electrical and water consumptions. Prevention through personnel training are being employed and prioritized to prevent re-works. Re-training is also being utilized through Learning and Development Intervention (LDI) specifically by the Nursing Services Department to prevent variance recurrence among nurses and allied health personnel. NKTI utilizes processes and standardized best practices to reduce variations and to minimize the cost of health care while improving outcomes. An example is the implementation of the Paper Reduction Initiative Strategies initiated by the Nursing Services Department beginning last 2013. This initiative aims to sustain and achieve higher reduction in the Institute’s paper consumption relative to its cost and also to contribute to the preservation of the environment and reduction of global warming. This is done by controlling paper request from different offices/units, advocating the use of recycled papers for internal communications, and setting up of electronic forms database to reduce volume of mimeograph forms. 6.1b(3) Systems Improvement. Performance improvement initiatives are being reported by various departments, divisions, sections, units, and offices during executive and management committee meetings. This is being done monthly, quarterly, semi-annual, and annually or as required by the management. NKTI conducts an annual Internal Quality Audit (IQA) to check coherence with QM from 2009 to 2013. The Department of Pathology and Laboratory Medicine also conducts IQA
based on ISO 15189 standards. Likewise, management reviews is being conducted after every IQA. Yearly strategic planning process (SPP) is being employed to lay down scope of activities for the year as well as regular monitoring of non-conformities. 6.1c Emergency Readiness. NKTI is mandated by the Adoption and Implementation of Code Alert System for DOH Hospital during Emergencies and Disasters (AO 182 s2001). This was in response to the 1998 Lung Center Fire. There is a documented contingency plan to cover particular situations in the event of disasters and emergency which is specific to the needs of patients and stakeholders. The Institute has created different committees to take action and to ensure continuity of healthcare and support operations in the event of an emergency and result of large scale natural disaster or calamity such as earthquake, typhoon and flood, fire, power interruption, water loss, Hospital Information System (HIS) and machine downtime; and potential pandemics like leptospirosis, Middle East respiratory syndrome coronavirus (MERS-CoV), human immunodeficiency virus (HIV), and Ebola virus. These committees include Health Emergency Management Bureau (HEMB) and Health, Safety, Environment and Security (HSES). HEMB is in charge of the training of NKTI’s employees through dissemination of information and conduction of drills while HSES on the other hand is in charged for the Institute’s safety and security as well as reduction of healthcare risk. There are also emergency preparedness plans specific to the needs of the different department of the Institute (Fig.6.1-3) Employees are mandated to participate annually in staff orientation, training and drills conducted regularly by HRMD in coordination with HSES and HEMB to know how to prevent healthcare risk and respond during any emergency situation.
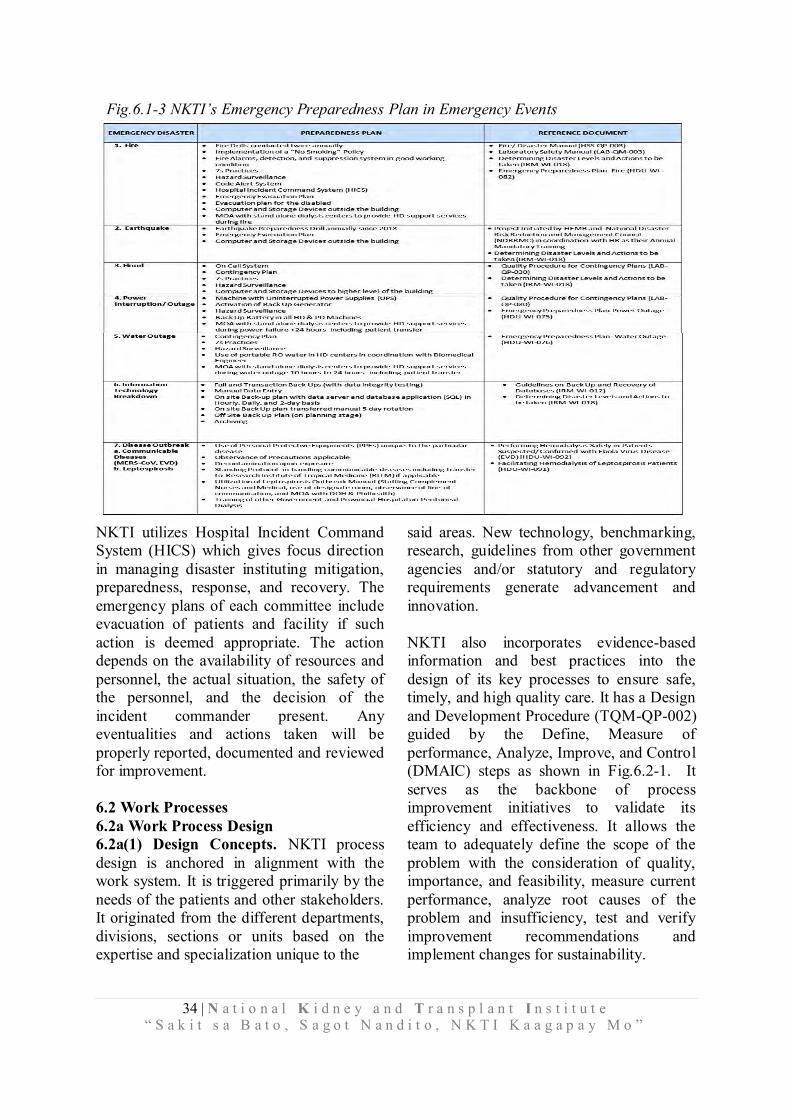
34 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
NKTI utilizes Hospital Incident Command System (HICS) which gives focus direction in managing disaster instituting mitigation, preparedness, response, and recovery. The emergency plans of each committee include evacuation of patients and facility if such action is deemed appropriate. The action depends on the availability of resources and personnel, the actual situation, the safety of the personnel, and the decision of the incident commander present. Any eventualities and actions taken will be properly reported, documented and reviewed for improvement. 6.2 Work Processes 6.2a Work Process Design 6.2a(1) Design Concepts. NKTI process design is anchored in alignment with the work system. It is triggered primarily by the needs of the patients and other stakeholders. It originated from the different departments, divisions, sections or units based on the expertise and specialization unique to the
said areas. New technology, benchmarking, research, guidelines from other government agencies and/or statutory and regulatory requirements generate advancement and innovation. NKTI also incorporates evidence-based information and best practices into the design of its key processes to ensure safe, timely, and high quality care. It has a Design and Development Procedure (TQM-QP-002) guided by the Define, Measure of performance, Analyze, Improve, and Control (DMAIC) steps as shown in Fig.6.2-1. It serves as the backbone of process improvement initiatives to validate its efficiency and effectiveness. It allows the team to adequately define the scope of the problem with the consideration of quality, importance, and feasibility, measure current performance, analyze root causes of the problem and insufficiency, test and verify improvement recommendations and implement changes for sustainability.
Fig.6.1-3 NKTI’s Emergency Preparedness Plan in Emergency Events
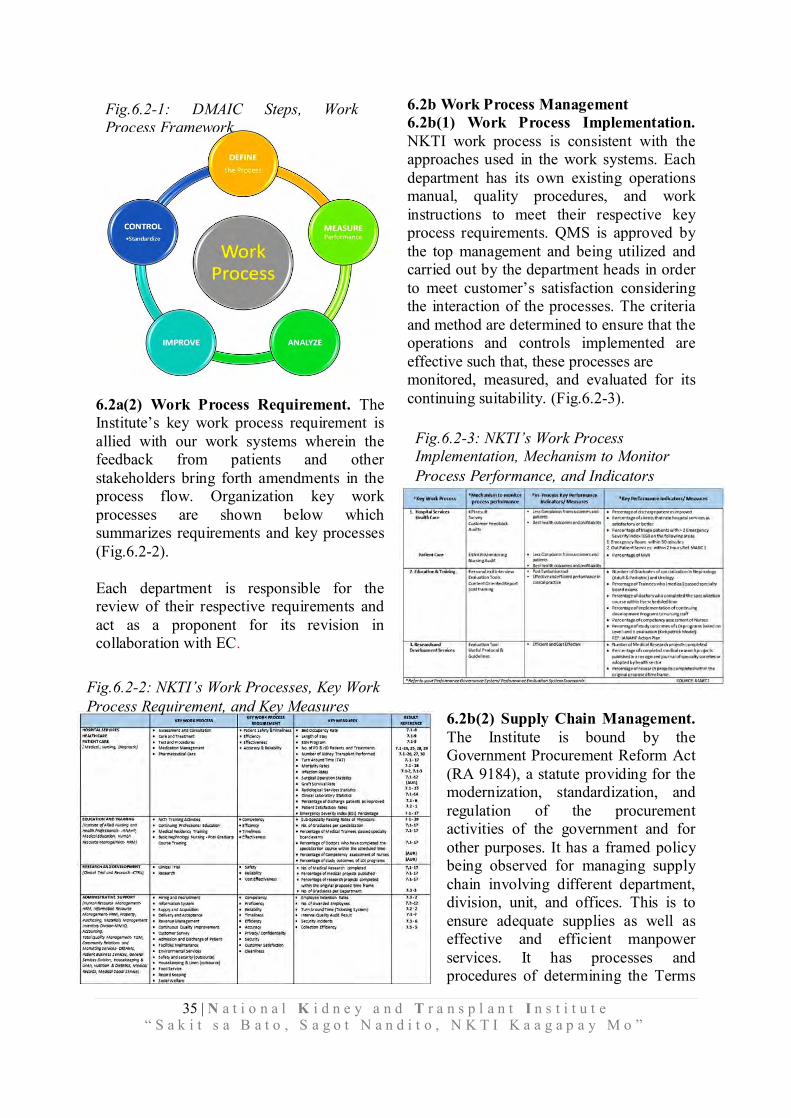
35 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
6.2a(2) Work Process Requirement. The Institute’s key work process requirement is allied with our work systems wherein the feedback from patients and other stakeholders bring forth amendments in the process flow. Organization key work processes are shown below which summarizes requirements and key processes (Fig.6.2-2). Each department is responsible for the review of their respective requirements and act as a proponent for its revision in collaboration with EC.
6.2b Work Process Management 6.2b(1) Work Process Implementation. NKTI work process is consistent with the approaches used in the work systems. Each department has its own existing operations manual, quality procedures, and work instructions to meet their respective key process requirements. QMS is approved by the top management and being utilized and carried out by the department heads in order to meet customer’s satisfaction considering the interaction of the processes. The criteria and method are determined to ensure that the operations and controls implemented are effective such that, these processes are monitored, measured, and evaluated for its continuing suitability. (Fig.6.2-3).
6.2b(2) Supply Chain Management. The Institute is bound by the Government Procurement Reform Act (RA 9184), a statute providing for the modernization, standardization, and regulation of the procurement activities of the government and for other purposes. It has a framed policy being observed for managing supply chain involving different department, division, unit, and offices. This is to ensure adequate supplies as well as effective and efficient manpower services. It has processes and procedures of determining the Terms
Fig.6.2-1: DMAIC Steps, Work Process Framework
Fig.6.2-3: NKTI’s Work Process Implementation, Mechanism to Monitor Process Performance, and Indicators
Fig.6.2-2: NKTI’s Work Processes, Key Work Process Requirement, and Key Measures
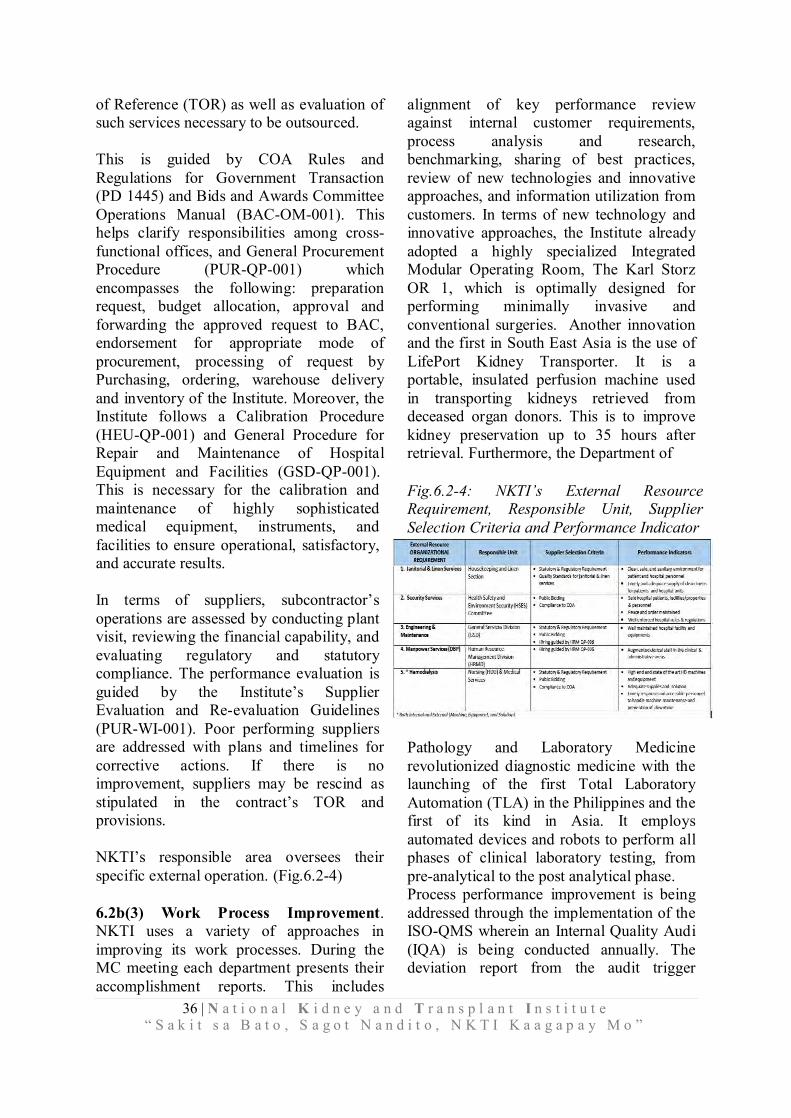
36 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig.6.2-4: NKTI’s External Resource Requirement, Responsible Unit, Supplier Selection Criteria and Performance Indicator
of Reference (TOR) as well as evaluation of such services necessary to be outsourced. This is guided by COA Rules and Regulations for Government Transaction (PD 1445) and Bids and Awards Committee Operations Manual (BAC-OM-001). This helps clarify responsibilities among cross- functional offices, and General Procurement Procedure (PUR-QP-001) which encompasses the following: preparation request, budget allocation, approval and forwarding the approved request to BAC, endorsement for appropriate mode of procurement, processing of request by Purchasing, ordering, warehouse delivery and inventory of the Institute. Moreover, the Institute follows a Calibration Procedure (HEU-QP-001) and General Procedure for Repair and Maintenance of Hospital Equipment and Facilities (GSD-QP-001). This is necessary for the calibration and maintenance of highly sophisticated medical equipment, instruments, and facilities to ensure operational, satisfactory, and accurate results. In terms of suppliers, subcontractor’s operations are assessed by conducting plant visit, reviewing the financial capability, and evaluating regulatory and statutory compliance. The performance evaluation is guided by the Institute’s Supplier Evaluation and Re-evaluation Guidelines (PUR-WI-001). Poor performing suppliers are addressed with plans and timelines for corrective actions. If there is no improvement, suppliers may be rescind as stipulated in the contract’s TOR and provisions. NKTI’s responsible area oversees their specific external operation. (Fig.6.2-4) 6.2b(3) Work Process Improvement. NKTI uses a variety of approaches in improving its work processes. During the MC meeting each department presents their accomplishment reports. This includes
alignment of key performance review against internal customer requirements, process analysis and research, benchmarking, sharing of best practices, review of new technologies and innovative approaches, and information utilization from customers. In terms of new technology and innovative approaches, the Institute already adopted a highly specialized Integrated Modular Operating Room, The Karl Storz OR 1, which is optimally designed for performing minimally invasive and conventional surgeries. Another innovation and the first in South East Asia is the use of LifePort Kidney Transporter. It is a portable, insulated perfusion machine used in transporting kidneys retrieved from deceased organ donors. This is to improve kidney preservation up to 35 hours after retrieval. Furthermore, the Department of
Pathology and Laboratory Medicine revolutionized diagnostic medicine with the launching of the first Total Laboratory Automation (TLA) in the Philippines and the first of its kind in Asia. It employs automated devices and robots to perform all phases of clinical laboratory testing, from pre-analytical to the post analytical phase. Process performance improvement is being addressed through the implementation of the ISO-QMS wherein an Internal Quality Audi (IQA) is being conducted annually. The deviation report from the audit trigger
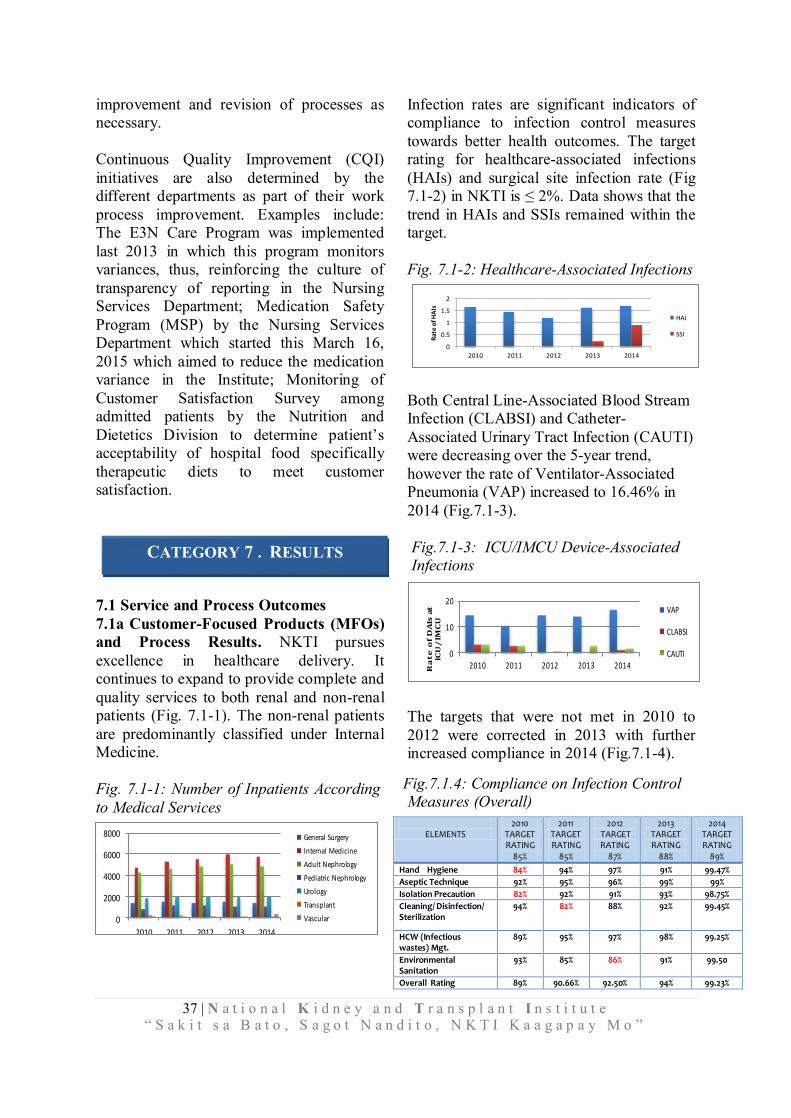
37 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
ELEMENTS
2010 TARGET RATING
85%
2011 TARGET RATING
85%
2012 TARGET RATING
87%
2013 TARGET RATING
88%
2014 TARGET RATING
89%
Hand Hygiene 84% 94% 97% 91% 99.47%
Aseptic Technique 92% 95% 96% 99% 99%
Isolation Precaution 82% 92% 91% 93% 98.75%
Cleaning/ Disinfection/ Sterilization
94% 82% 88% 92% 99.45%
HCW (Infectious wastes) Mgt.
89% 95% 97% 98% 99.25%
Environmental Sanitation
93% 85% 86% 91% 99.50
Overall Rating 89% 90.66% 92.50% 94% 99.23%
Fig.7.1.4: Compliance on Infection Control Measures (Overall)
improvement and revision of processes as necessary. Continuous Quality Improvement (CQI) initiatives are also determined by the different departments as part of their work process improvement. Examples include: The E3N Care Program was implemented last 2013 in which this program monitors variances, thus, reinforcing the culture of transparency of reporting in the Nursing Services Department; Medication Safety Program (MSP) by the Nursing Services Department which started this March 16, 2015 which aimed to reduce the medication variance in the Institute; Monitoring of Customer Satisfaction Survey among admitted patients by the Nutrition and Dietetics Division to determine patient’s acceptability of hospital food specifically therapeutic diets to meet customer satisfaction.
7.1 Service and Process Outcomes 7.1a Customer-Focused Products (MFOs) and Process Results. NKTI pursues excellence in healthcare delivery. It continues to expand to provide complete and quality services to both renal and non-renal patients (Fig. 7.1-1). The non-renal patients are predominantly classified under Internal Medicine.
Fig. 7.1-1: Number of Inpatients According to Medical Services
Infection rates are significant indicators of compliance to infection control measures towards better health outcomes. The target rating for healthcare-associated infections (HAIs) and surgical site infection rate (Fig 7.1-2) in NKTI is ≤ 2%. Data shows that the trend in HAIs and SSIs remained within the target. Fig. 7.1-2: Healthcare-Associated Infections
0
0.5
1
1.5
2
2010 2011 2012 2013 2014
Rat
e o
f HA
Is
HAI
SSI
Both Central Line-Associated Blood Stream Infection (CLABSI) and Catheter-Associated Urinary Tract Infection (CAUTI) were decreasing over the 5-year trend, however the rate of Ventilator-Associated Pneumonia (VAP) increased to 16.46% in 2014 (Fig.7.1-3). Fig.7.1-3: ICU/IMCU Device-Associated Infections
The targets that were not met in 2010 to 2012 were corrected in 2013 with further increased compliance in 2014 (Fig.7.1-4).
CATEGORY 7 . RESULTS
0
10
20
2010 2011 2012 2013 2014Ra
te
of
DA
Is a
t
ICU
/IM
CU
VAP
CLABSI
CAUTI
0
2000
4000
6000
8000
2010 2011 2012 2013 2014
General Surgery
Internal Medicine
Adult Nephrology
Pediatric Nephrology
Urology
Transplant
Vascular

38 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
98.60%
98.80%
99.00%
99.20%
99.40%
99.60%
99.80%
100.00%
100.20%
2010 2011 2012 2013 2014
Pe
rce
nt
(%)
of C
om
pli
ance
Bas
ed
on
N
o.
of
Dis
cha
rges
Medication Variance
Patient Fall
Heathcare Associated Pressure
SoresHealthcare Associated Burn
InjuryBlood-Transfusion Related Errors
Patient Complaints
Diagnostic Test-Related Errors
Fig. 7.1-5: Nursing Services E3N Care Program
The compliance to patient safety measures by the nurses is monitored using the four keys performance indicators from 2010 to 2012. In 2013, four more indicators were added. The results were high in all the indicators except for medication variance which has the least level of compliance (Fig. 7.1-5).
The percentage of patients who recovered or improved from their illnesses upon discharge shows an increase from 2010 to 2011. However, a decline was noted in 2012 (Fig. 7.1-6). The increase in 2013 and 2014 is a result of the continuous quality improvement initiatives of the healthcare team.
7.1b(1) Operational Process Effectiveness Results 7.1b(1) Operational Effectiveness. NKTI operates within the context of delivering complete hospital services in which complex processes are involved. In an effort to attain excellent quality of services, the Institute made its way towards acquiring the ISO 9001:2000 certification in 2002 that
was subsequently upgraded to 9001:2008 in 2009 (P.1a(2)). The Internal Quality Audit (IQA) Team evaluates NKTI’s compliance
with the ISO elements to ensure process effectiveness across the organization. The frequency of these is recorded annually, these showed an overall decrease in trend except for measurement, analysis and improvement (Fig. 7.1-7).
Specific hospital statistics or operational ratios are also utilized: Occupancy Rate. The trend in the adjusted bed occupancy rate declined from 2010 to 2012, however there was an increase in 2013 and 2014 of 68.91% and 69.04% respectively (Fig. 7.1-8).
Fig.7.1-8: Adjusted Occupancy Rates
Average Length of Stay. The average length of stay of service patients is relatively longer than the paying ones. This
result is based on the fact that service patients have more severe illness or/are chronic cases before they seek treatment in a tertiary specialty hospital (Fig. 7.1-9).
Fig. 7.1-6: Percent of Patients Discharged as Improved/Recovered
Fig.7.1-7: Result of Internal Quality Audit
39 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig.7.1-9: Average Length of Stay, Pay & Service
0
5
10
2010 2011 2012 2013 2014
Da
ys
Pay
Service
Patient Mix. The inpatients being seen in the Institute are classified according to their source of payment. Around 80% were private service patients and 20% were charity service patients, which are both increasing over the years (Fig. 7.1-10).
Fig.7.1-10: Number of Inpatients
Equipment Utilization Rate. The utilization rate of the Department of Radiology decreased from 2012 to 2014 by 6% (Fig. 1.1-11). This is a result of the acquisition of new equipment in 2012. Fig.7.1-11: Department of Radiology Utilization Rate
Other Operational Statistics. The volume of procedures in various areas or centers helps the management determine productivity. From 2010 to 2014, the surgical operation statistics showed a declining trend in minor surgeries while increasing medium and major surgeries. The decrease in minor surgeries was because some of the procedures such as access insertion for HD and PD were done
in the Procedure Room of the Emergency Room. (Fig. 7.1-12). Fig.7.1-12: Surgical Operation Statistics
0
2000
4000
6000
2010 2011 2012 2013 2014
Major
Medium
Minor
The volume of radiology procedures, especially x-ray and ultrasound steadily increased throughout the 5-year trend (Fig. 7.1-13).
Fig. 7.1-13: Radiology Services Statistics
0
10000
20000
30000
40000
2010 2011 2012 2013 2014
X-ray
Ultrasound
CT Scan
Mammography
MRI
Similarly, the number of procedures done at the Medical Laboratory, particularly the APCP tests, increased significantly from 668, 866 in 2010 to 915, 512 in 2013, however there is a slight decline in 2014 (Fig. 7.1-14). Fig.7.1-14: Clinical Laboratory Statistics
The volume of procedures in all ancillary laboratories also increased from 2010 to 2014 with the highest volume from the Departments of Physical Medicine and Rehabilitation and Pulmonary. (Fig. 7.1-15)
0
500000
1000000
2010 2011 2012 2013 2014
APCP Tests
Hematology
Immunology

40 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig.7.1-15: Ancillary Laboratory Statistics
For the special services, medical oncology had the highest volume with an increasing trend. Furthermore, an increasing trend in the Cardiovascular Catheterization and Radiology Unit (CCRU) was noted. This unit started its operation in 2012. For the extracorporeal shock wave lithotripsy (ESWL), a downward trend was observed from 2010 to 2014. This was because of the shifting from an old machine owned by a private partner to NKTI’s new ESWL machine. (Fig.7.1-16). Fig. 7.1-16: Special Services 7.1b(2) Emergency Preparedness. Disaster preparedness seminars are conducted annually. Since 2012, 384 employees have participated in the Fire Prevention Seminar and Drill. The Earthquake Preparedness Lecture and Drill was conducted starting 2013 with 76 attendees. Moreover, 96 employees attended the Mass Casualty Management Seminar that was initially conducted in 2014. 7.1c Strategy Implementation Results. The monitoring of the performance indicators related to the identified MFOs (2.2a(5)) is corollary of the implementation of the Performance-Based Incentive System (PBIS) for National Government Agencies and Employees that was introduced in 2012. In 2013, NKTI has qualified for the grant of the Performance-Based Bonus (PBB) for
achieving its targets and was ranked as BETTER. The rating was based on the result as shown in MARC-1 (Fig. 7.1-17)
New performance indicators were identified for FY 2014 to reinforce the effectiveness of monitoring and appraisal of NKTI’s performance especially for MFO1: Hospital Services. The 2014 MARC-1 is yet to be published, though it is evident that NKTI’s accomplishment for FY 2014 indicates good performance as it achieved most of its targets (Fig.7.1-18).
0
20000
40000
60000
80000
2010 2011 2012 2013 2014
Cardiovascular
Neurology
Nuclear Medicine
Physical Med & RehabilitationPulmonary
Vascular & Woundcare
0
5000
2010 2011 2012 2013 2014
Medical Oncology
Endoscopy
ESWL
Urodynamics
CCRU
Fig.7.1-17: MARC-1
41 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig.7.1-20: Urology Map Program
As far as Education and Training of Health Professionals is concerned, NKTI takes pride of the high passing rate of physicians on specialty boards examinations. In 2014, all departments achieved a 100% passing rate (Fig.7.1-19). Fig.7.1-19: Sub-Specialty Passing Rates of Physicians
Adult Nephrology
25% 100% 86% 100% 100%
Pediatric Nephrology
100% 100% 100% 100% 100%
Internal Medicine
100% 100% 100% 100% 100%
Pathology 100% 100% 100% 100% -
Radiology (Part I, II & III)
100% 100% 84% 100% 100%
Radiology (Utz) 100% 100% 100% 100% 100%
Radiology (MRI) 50% 75% 100% 33% 100%
Urology 100% 100% 100% - 100%
Transplant Surgery
100% 100% 100% 100% 100%
The graduates of NKTI practice their profession in different provinces in the country. They are the living proof of the quality of training they received from NKTI (Fig.7.1-20 to 21).
Fig.7.1-18: 2014 Office Performance Indicators and Targets (Accomplishment)
Fig.7.1-21: Adult Nephrology Map)
National Kidney and Transplant Institute
DEPARTMENT OF ADULT NEPHROLOGY
CAGAYAN
ILOCOS NORTE
ILOCOS SUR
ISABELA
LA UNION
BAGUIO
NUEVA VISCAYA
PANGASINAN
TARLAC NUEVA ECIJA
ZAM
BA
LES
BATAAN
PAMPANGA BULACAN
RIZAL
CAVITE LAGUNA
SORSOGON
CAMARINES SUR
MARINDUQUE
BATANGAS
ROXAS
PALAWAN
ILOILO
BACOLOD
DUMAGUETE
CEBU
BOHOL
LEYTE
SURIGAO
CAGAYAN DE ORO
OZAMIS
ILIGAN PAGADIAN
TAGUM
DAVAO
SOUTH COTABATO
ZAMBOANGA CITY
NCR
QUEZON
REGION VII (Central Visayas)
Uriel Baclayon, MD-Cebu (1986) Helen Po, MD-Cebu (1987)
Eulysses Baniga, MD-Cebu (1990) Juliet Chua Chong-Noel, MD-Cebu (1996)
Ma. Mayida Ybañez, MD-Bohol (2002) Ophelia Saad, MD-Dumaguete (2004)
German Mayo, MD-Cebu (2005) Yvette Ethel Mondano, MD-Cebu (2006)
John Li, MD-Cebu (2008) Roy Diamond Arco, MD-Dumaguete (2012)
Maria Isabel Momongan, MD-Dumaguete (2013) Catherine Rose Ti, MD-Cebu (2013) Mark Javeson Tam, MD-Cebu (2014)
REGION X (Northern Mindanao)
Philip Lazo, MD-Cagayan de Oro (1987) Sandra Oliveros, MD-Cagayan de Oro (1994)
Angelita Sy Go, MD-Ozamis City (1995) Rosalie Imelda Orejudos, MD-Iligan (2005)
Nenia May Batulayan, MD-Cagayan de Oro (2007)
REGION XI (Southern Mindanao)
Flor Jocelyn Caballes, MD-Davao (1988) Franklin Guillano, MD-Davao (2000)
Maria Theresa Bad-Ang, MD-Davao (2008) Asterio Ramiscal, MD-Tagum (2008)
Chito Cornejo, MD-Digos, Davao (2009) Clarissa Equipado, MD-Davao (2010) Bernard Ramos, MD-Davao (2010)
REGION VIII (Eastern Visayas)
Avito Salinas, MD-Leyte (1988) Olga Chavez, MD-Leyte (1998)
Joyce Rosario Matoza, MD-Leyte (2008) Rodrigo Capahi, MD-Leyte (2012)
REGION IV-A (CALABARZON)
Eugene Castillo, MD-Cavite (1990) Nathaniel Agoncillo, MD-Batangas (1992)
Rene Baltazar, MD-Laguna (1993) Ma. Gina Nazareth, MD-Batangas (1998)
Rolando Macalalag, MD-Cavite (2002) Gjay Ordinal, MD-Rizal (2002)
Virgilio Ocampo Jr., MD-Laguna (2007) Marlene Villanueva, MD-Laguna (2008)
Carmel Carlos, MD-Rizal (2009) Alvin Belen, MD-Laguna (2010)
Irene Castillo, MD-Batangas (2010) Christina Erika Basilan, MD-Quezon (2013)
Rudi Joy Laraño, MD-Laguna (2014)
REGION V (Bicol Region)
Rizalina Ramos, MD-Camarines Sur (1992) Jean Pabilonia, MD-Naga (1995)
Jose Emmanuel Cabildo, MD-Sorsogon (2006) Edwin Tan, MD-Sorsogon (2006)
Josephine Bonos, MD-Sorsogon (2014)
CAR (Cordillera Administrative Region)
Josefina Luspian, MD-Baguio (1995) Ma. Gemma Pinlac, MD-Baguio (1996)
Erwin Villar, MD-Baguio (2003) Alma Suclad, MD-Baguio (2006)
Ruchelle Marie Turqueza, MD-Baguio (2014)
REGION IX (Zamboanga Peninsula)
Jamasali Usman, MD-Zamboanga City (1995) Emerson Mondarte, MD-Pagadian (2011)
REGION I (Ilocos Region)
Wilfredo Magcalas, MD-Ilocos Norte (1997) Abraham Coquia, MD-Pangasinan (2000)
Virginia Mangati, MD-La Union (2010) Angielyn Asuncion, MD-Pangasinan (2012) Amor Rhea Quilala, MD-Ilocos Sur (2013)
REGION VI (Western Visayas)
Jerome Pepingco, MD-Bacolod (1999) Maria May Samillano, MD-Bacolod (1999)
Hazel Yadao-Oro, MD-Iloilo (2005) Leo Manuel Tumaneng, MD-Bacolod (2009)
Sheila Marie Baria, MD-Iloilo (2011) Ethel Cordero, MD-Iloilo (2011)
Marianne Diaz, MD-Roxas City (2011) Maricris Bacinillo, MD-Bacolod (2012)
Rey Isidto, MD-Iloilo (2013)
REGION XII (Central Mindanao)
Floherna Diccion, MD-South Cotabato (2014)
REGION II (Cagayan Valley)
Edmund Bautista, MD-Cagayan (2001) Frederick Parallag, MD-Cagayan (2002)
Rubylaine Par-Pinoy, MD-Nueva Viscaya (2005) Omega Mallillin, MD-Isabela (2013)
REGION III (Central Luzon)
Olivia Idio, MD-Bataan (2001) Mara Tugade, MD-Bulacan (2001)
Ma. Christina Salas, MD-Cabanatuan (2003) Diosdado Bartolo, MD-Bulacan (2006) Angelito Rioveros, MD-Bulacan (2008)
Ma. Lorelei Lucio-Tong, MD-Bataan (2009) Joy Mallari, MD-Pampanga (2009) Shalee Santos, MD-Tarlac (2011)
Marichel Pile, MD-Bulacan (2012) Maria Regina Gregorio, MD-Zambales (2014)
REGION XIII (CARAGA Region)
Romina Rusillon, MD Surigao del Norte (2004)
REGION IV-B (MIMAROPA)
Chona Tagayuna, MD-Marinduque (2006) Ruel Agni, MD-Palawan (2012)
JOLO
ARMM (Autonomous Region of Muslim Mindanao)
Mel-Hatra Arakama, MD-Jolo (2013)
Florencio Pine, MD (1984) Antonio Paraiso, MD (1984)
Delia Bayog, MD (1985) Ma. Remedios Caballero, MD (1985)
Raceme Erasmo, MD (1986) Corazon Macaraeg, MD (1990)
Albert Lu, MD (1991) Ramon Mora, MD (1991) Susan Jorge, MD (1992)
Susan Añonuevo-Dela Rama, MD (1993) Ma. Nila Lopez, MD (1994) Annfil Balista, MD (1996) Regina Ampil, MD (1997)
Rogelio Dela Cruz, MD (1997) Cipriano Famorca, Jr., MD (1997)
Melo Jane Paz, MD (1998) Concesa Casasola, MD (1999)
Lilibeth Ibbarientos, MD (1999) Alberto Frederick Celestial, MD (2000)
Elizabeth Sebastian, MD (2000) Lea Grace Vasquez, MD (2000)
Arlene Lamban, MD (2001) Ma. Cecilia Manalo, MD (2001)
Ma. Martina Alcantara, MD (2002) Glenda Eleanor Pamugas, MD (2002)
Ronald Perez, MD (2002) Maaliddin Biruar, MD (2004)
Arnel Chua, MD (2004) Hazel Daphne Niñalga, MD (2005)
Richard Hizon, MD (2007) Roland Dela Cruz, MD (2007)
Ma. Angeline Gumba, MD (2007) Arlene Muñoz, MD (2007)
Ma. Eliza Navarro, MD (2008) Czarina Kay Beltran, MD (2009)
Eric Chua, MD (2010) Nemma Evangelista, MD (2011)
Ana-Mae Quetua, MD (2012) Layla Marie Paraiso, MD (2013)
Cher Alaine Luna, MD (2014) J. Meinard Nepomuceno (2014)
NCR (National Capital Region)

42 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
As compared to the other hospitals in NCR, NKTI remained to be the frontrunner in attracting new patients for PD (Fig.7.1-24), HD (Fig.7.1-25) and kidney transplantation (KT) (Fig.7.1-26). The decreasing trend at NKTI was consistent with the nationwide decrease in the number of kidney transplants performed (Fig.7.1-27). Fig.7.1-24: Number of New Peritoneal Dialysis Patients in NCR According to Dialysis Unit
Fig.7.1-25: Number of New HD Patients in NCR According to Dialysis Unit
Fig. 7.1-26: Number of Kidney Transplants Performed in NCR According to Hospital
0
100
200
300
400
2009 2010 2011 2012 2013
CMC
CSMC
NKTI
SLMC-QC
SLMC-GC
Fig.7.1-27: Number of Kidney Transplants Performed in the Philippines
Internally, the trend in PD and HD sessions continue to increase in number from 2010 to 2014. Continuous ambulatory peritoneal dialysis (CAPD) was the sole modality used
Fig. 7.1-23: Transplant and Vascular Surgery Map
Fig. 7.1-22: Pediatric Nephrology Map
43 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
0
200
400
600
800
2010 2011 2012 2013 2014
CAPD
CIPD
CCPD
40
74
3526
0
20
40
60
80
2010 2011 2012 2013
Num
ber
of C
PAR
Form
s Us
ed
since 2013 that led to a dramatic increase in the number of CAPD trainings in 2013 and 2014 (7.1-28). Fig. 7.1-28 Number of Peritoneal Dialysis Treatments
The number of HD treatments also showed an increasing trend from 2010 to 2014 however there is a marginal decrease by 1.9% from 2013 to 2014 (Fig. 7.1-29).
Fig. 7.1-29: Number of Hemodialysis Treatments
0
20000
40000
2010 2011 2012 2013 2014
Out-Patient
In-Patient
The number of KT performed decreased by 10% from 2013 to 2014. The number of transplants from living related donor increased by 10% in 2014, while there was a decrease in the living non-related and non-living donor (Fig 7.1-30). Fig.7.1-30: Number of Kidney Transplantations
7.2 Customer-Driven and Citizen-Focused Outcomes 7.2a(1) Customer and Citizens’ Satisfaction. The increasing satisfaction rate of patients is a result of the continuous effort of NKTI to achieve the best quality of care.
Fig.7.2-1: Patient Satisfaction Survey Results
0%
50%
100%
150%
2012 2013 2014
Determining complaints or dissatisfaction is likewise important to identify areas for improvement. The number of CPAR forms issued equates to the amount of complaints received. The number of complaints decreased from 74 to 26 in 2011 to 2013 respectively. Fig. 7.2-2: Number of Corrective and Preventive Action Request Forms Issued
Ticketing system was a new approach used in 2014 to increase efficiency in addressing patient complaints, wherein a number of 70 complaints was recorded. The sudden increase in the number of complaints is a result of a more effective system in identifying them. NKTI is also recognized by other organizations for its outstanding delivery of services. This is demonstrated by the recognitions received.
Fig. 7.2-3 Awards and Recognitions AWARD/RECOGNITION
2012 1. UAE Health Foundation Prize (NKTI-REDCOP)
2011 1. 1. PSQUA Partner in Quality Award 2. 2. First Gawad Likha Kalusugan Award, Award of
Merit and Excellence (HD Center – Fresenius Medical Care)
3. 3. Quezon City Gawad Parangal as Most Outstanding Institution
0
100
200
2010 2011 2012 2013 2014
LRD
LNRD
NLD
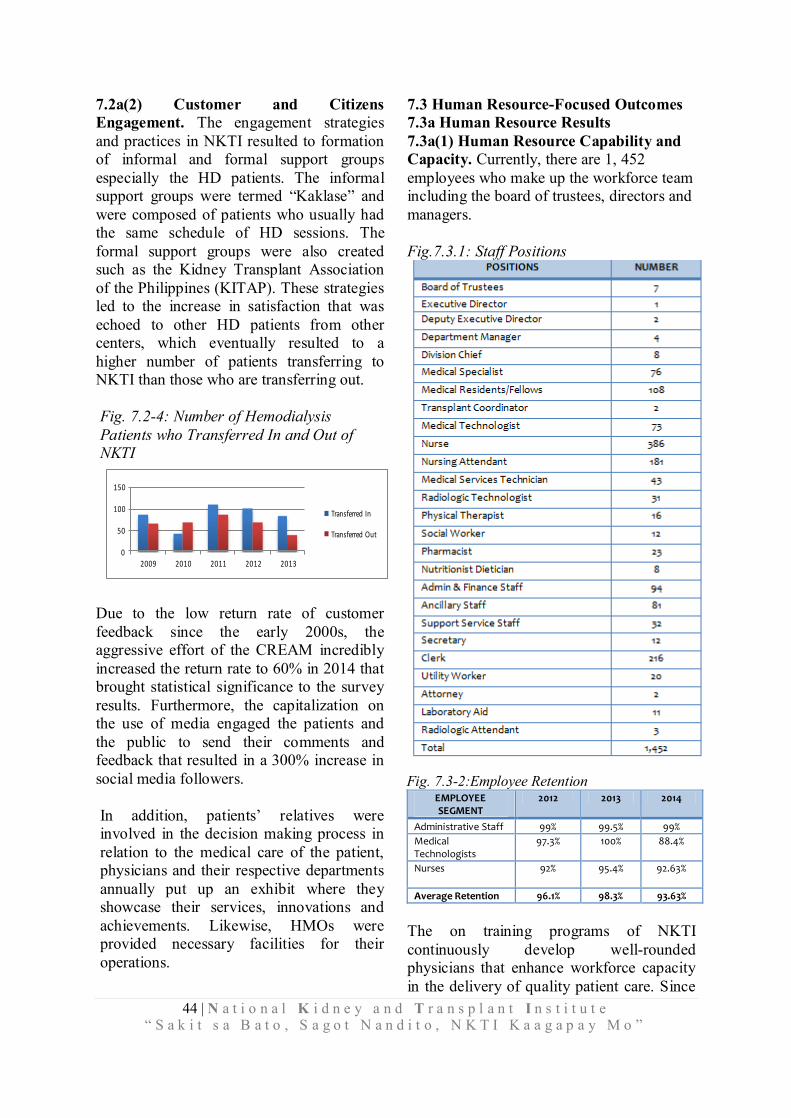
44 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
7.2a(2) Customer and Citizens Engagement. The engagement strategies and practices in NKTI resulted to formation of informal and formal support groups especially the HD patients. The informal support groups were termed “Kaklase” and were composed of patients who usually had the same schedule of HD sessions. The formal support groups were also created such as the Kidney Transplant Association of the Philippines (KITAP). These strategies led to the increase in satisfaction that was echoed to other HD patients from other centers, which eventually resulted to a higher number of patients transferring to NKTI than those who are transferring out. Fig. 7.2-4: Number of Hemodialysis Patients who Transferred In and Out of NKTI
0
50
100
150
2009 2010 2011 2012 2013
Transferred In
Transferred Out
Due to the low return rate of customer feedback since the early 2000s, the aggressive effort of the CREAM incredibly increased the return rate to 60% in 2014 that brought statistical significance to the survey results. Furthermore, the capitalization on the use of media engaged the patients and the public to send their comments and feedback that resulted in a 300% increase in social media followers. In addition, patients’ relatives were involved in the decision making process in relation to the medical care of the patient, physicians and their respective departments annually put up an exhibit where they showcase their services, innovations and achievements. Likewise, HMOs were provided necessary facilities for their operations.
7.3 Human Resource-Focused Outcomes 7.3a Human Resource Results 7.3a(1) Human Resource Capability and Capacity. Currently, there are 1, 452 employees who make up the workforce team including the board of trustees, directors and managers. Fig.7.3.1: Staff Positions The retention rate of administrative staff remained steady at 99%. Though there was a decline with the medical technologists and nurses, the average retention rate remained high from 2012 to 2014. Fig. 7.3-2:Employee Retention
EMPLOYEE SEGMENT
2012 2013 2014
Administrative Staff 99% 99.5% 99%
Medical Technologists
97.3% 100% 88.4%
Nurses
92% 95.4% 92.63%
Average Retention 96.1% 98.3% 93.63%
The on training programs of NKTI continuously develop well-rounded physicians that enhance workforce capacity in the delivery of quality patient care. Since

45 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
1983 to 2013 it has produced a total of 548 graduates. Fig.7.3-3: Number of Graduates per Department Department 2010 2011 2012 2013
Adult Nephrology 7 7 8 8
Pediatric Nephrology
2 2 3 4
Anesthesia (Fellow)
0 0 0 1
Anesthesia (Residents)
3 2 4 3
Internal Medicine
(Residents)
5 6 6 7
Oncology (Fellow) 1 1 1 2
Laboratory Medicine (Residents)
1 2 1 3
Organ Transplant 2 3 4 2
Radiology (Fellows)
0 4 2 3
Radiology (Residents)
2 3 2 4
Urology 2 2 2 3
Vascular Surgery 0 0 1 3
Total 25 32 34 43
7.3a(2) Human Resource Climate. Immunization of Hepatitis B is required among the employees and trainees who provide direct patient care such as the doctors and nurses upon entry. Furthermore, an average of 25 participants attend the zumba dance exercise that is conducted once a week as part of the wellness program. The number of employees who availed free annual physical exam steadily increased from 2012 to 2014. This is due to the collective efforts of the Employee Wellness Committee to promote its utilization to effectively assess the health status of employees. Fig. 7.3-4: Compliance to Annual Physical Examination
Due to the consistent campaign of the Infection Control Committee and Healthcare Waste Management Committee against needle stick injuries, the number of sharps or body fluids exposure of employees shows a declining trend. The highest number of 35 was recorded in 2012 but this declined to 22 in 2013 and 2014. Fig.7.3-5: Sharps/Body Fluids Exposure of Employees
The improved security system provides a more secure workplace that led to the decline in security incidents. Fig.7.3-6: Security Incidents
7.3a(3) Human Resource Engagement. The result of the FGD conducted by Ateneo CORD to assess engagement of employees shows that 50% of the respondents perceive engagement as having commitment towards their work. Also, 65% of the respondents associated going overtime as the most common action of an employee that shows engagement. Also, they identified rewards and recognition, management support, association with organization, relationships, job satisfaction, and opportunities or employee development as factors that engage them.

46 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig.7.3-7: Drivers of Engagement Rewards and Recognition 55%
Management Support 45%
Association with Org 35%
Relationships 35%
Job Satisfaction 30%
Opportunities/Employee Development 30%
Appreciation 25%
Compensation and Benefits 20%
Org’s Vision and Mission 5%
The average number of absences ranges from 16 to 18 per year. This indicator suggests that the level of absenteeism at NKTI is low. Fig. 7.3-8: Average Number of Employee Absences per Year
The number of tardiness shows a decreasing trend over the 5-year period. There was a 65% decrease from 2013 to 2014, however there were a total number of 6 employees who were issued suspension notice due to habitual tardiness. Fig. 7.3-9: Total Number of Tardiness vs. No. of Staff Who Were Issued Suspension
0
20
40
60
80
2010 2011 2012 2013 2014
The recipients of Gantimpala Agad Awards significantly increased by 66% from 2012 to 2013 but declined by 34% in 2014. The number of most outstanding employees remained at 10 over the 3-year period, while the trend of perfect attendance awardees consistently increased.
Fig. 7.3-10: Number of Awarded Employees AWARDS 2012 2013 2014
Gantimpala Agad Awards 199 590 387
Most Outstanding Employees 10 10 10
Perfect Attendance Awardees 15 16 19
Loyalty Awardees
- 20 Years 25 27 24
- 25 Years 31 61 21
- 30 Years 0 21 12
7.3a(4) Human Resource Development In Human Resource Development, employees are promoted based on human resource needs and the result of their performance evaluation. Fig.7.3-11: Number of Promotions per Year
YEAR NO. OF PROMOTIONS
2011 34
2012 16
2013 35
2014 40
All healthcare professionals are required to have licenses and certifications specific to their respective professions. The Human Resource Management Division ensures that all concerned employees comply with their professional requirements. The different departments depending on the needs of their staff also conduct seminars regularly aside from the seminars that are conducted by the HRMD. 7.4 Leadership and Governance Outcomes 7.4a Leadership, Governance, and Societal Responsibility Results 7.4a(1) Leadership. Since communication is critical in deploying the strategies set by the Executive Committee, meetings are held according to segmentation of participants.

47 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig.7.4-1: Percentage of Attendance to Meetings
Type of
Meeting
Frequency 2010 2011 2012 2013 2014
Percentage (%) of Attendance
ExeCom Monthly 92% 75% 85% 80% 82%
ManCom Monthly 80% 80% 80% 82% 83%
Operation
s Audit (FASD)
Monthly 92% 93% 93% 88% 100%
Operations Audit (Support Offices)
Monthly - 84% 91% 100% 88%
Management Review
Semi-Annual
100% 100% 90% 100% -
General Assembly
Annually 75% 75% 75% 75 75%
Medical/ Surgical Meeting
Quarterly 95% 95% 95% 95% 95%
7.4a(2) Governance. NKTI complies with Good Governance Conditions as prescribed in the Performance-Based Incentive System. In 2013, it has complied in all areas except for substantial compliance to the transparency seal. Fig:7.4-2: Management Accountability Report Card (MARC-2) MANAGEMENT ACCOUNTABILITY
REPORT CARD (MARC-2)
Good Governance
Conditions
NATIONAL KIDNEY AND TRANSPLANT INSTITUTE
2012 2013 2014 2015
Transparency Seal
Substantial Compliance
Substantial Compliance
PhilGEPS Posting
Non-Compliant
Compliant
Cash Advance
Liquidation Compliant Compliant
Citizen’s Charter
Compliant Compliant
SALN N/A Compliant
From 2008 to 2012, the number of observations reduced from 10 to 8 and best efforts are put into action to fully implement, if not partially, the recommendations of COA.
Fig.7.4-3: Number of COA Recommendations and Actions Taken
Yea
r
# o
f O
bse
rvat
ion
s
Nu
mb
er o
f
Rec
om
men
dat
ion
s
ACTIONS TAKEN
Fully
Im
ple
men
ted
Par
tial
ly
Imp
lem
ente
d
No
t Im
ple
men
ted
2008 10 30 10 5 15
2009 14 27 10 10 7
2010 10 20 14 4 2
2011 7 11 8 2 1
2012 8 12 6 4 2
7.4a(3) Law and Regulation. In 2010, NKTI was accredited by Philhealth as Center for Excellence and in 2014 it has received recognition from the same agency for being the 5th among the more than 300 hospitals accredited by PhilHealth with the least number of Return to Hospital Claims. 7.4a(4) Ethics . Several staff members were sent to undergo training on various areas of ethics. In 2013, the eleven (11) members of the Research Ethics Committee attended a total of 26 trainings. The committee reviewed and approved a total of 19 research projects out of the 20 that were submitted. In the following year, the number of researches reviewed increased to 57 with 44 approved. In relation to the Hospital Transplant Ethics Committee for Non-Living Related Donors, 94 cases were deliberated in 2013 wherein 10 out of these cases were disapproved. In 2014, 75 out of 76 cases passed the assessment. 7.4a(5) Society. Through REDCOP, several medical missions are conducted in different regions of the Philippines. The activities during the medical missions aim to identify potential renal problems of Filipinos. The most number of medical missions were done in the year 2013 (Fig.4-4).
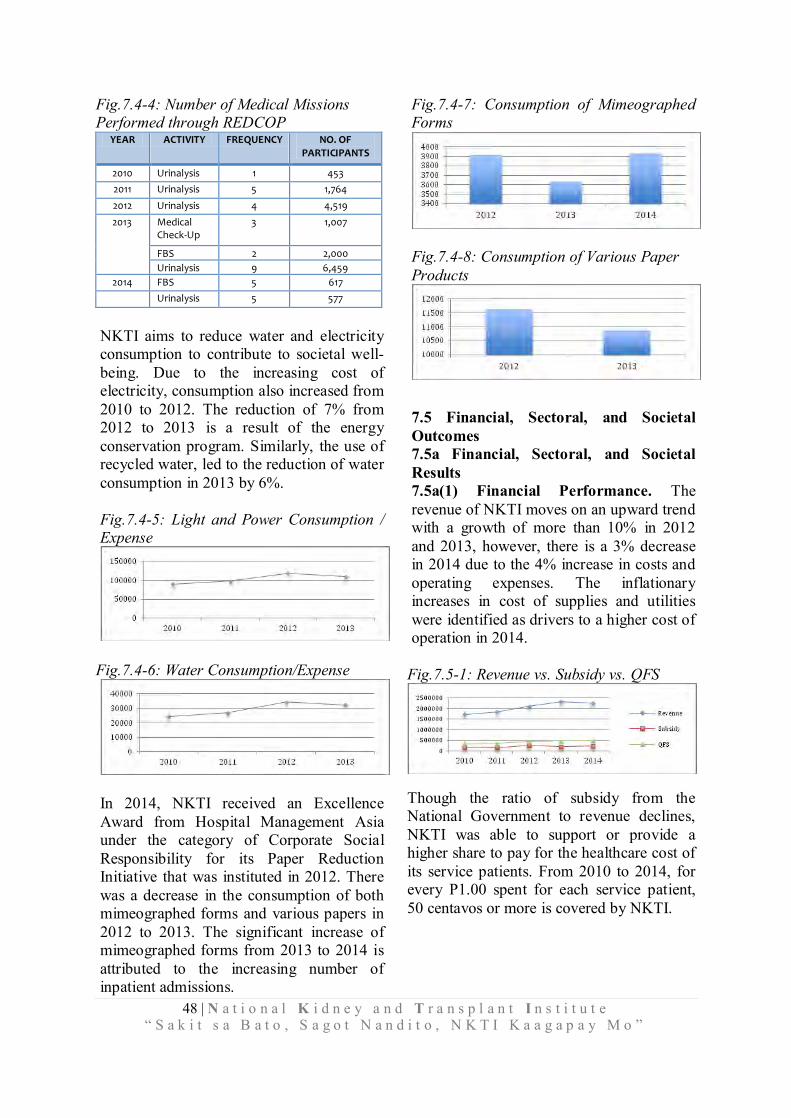
48 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig.7.4-4: Number of Medical Missions Performed through REDCOP
YEAR ACTIVITY FREQUENCY NO. OF PARTICIPANTS
2010 Urinalysis 1 453
2011 Urinalysis 5 1,764
2012 Urinalysis 4 4,519
2013 Medical Check-Up
3 1,007
FBS 2 2,000
Urinalysis 9 6,459
2014 FBS 5 617
Urinalysis 5 577
NKTI aims to reduce water and electricity consumption to contribute to societal well-being. Due to the increasing cost of electricity, consumption also increased from 2010 to 2012. The reduction of 7% from 2012 to 2013 is a result of the energy conservation program. Similarly, the use of recycled water, led to the reduction of water consumption in 2013 by 6%. Fig.7.4-5: Light and Power Consumption / Expense
Fig.7.4-6: Water Consumption/Expense
In 2014, NKTI received an Excellence Award from Hospital Management Asia under the category of Corporate Social Responsibility for its Paper Reduction Initiative that was instituted in 2012. There was a decrease in the consumption of both mimeographed forms and various papers in 2012 to 2013. The significant increase of mimeographed forms from 2013 to 2014 is attributed to the increasing number of inpatient admissions.
Fig.7.4-7: Consumption of Mimeographed Forms
Fig.7.4-8: Consumption of Various Paper Products
7.5 Financial, Sectoral, and Societal Outcomes 7.5a Financial, Sectoral, and Societal Results 7.5a(1) Financial Performance. The revenue of NKTI moves on an upward trend with a growth of more than 10% in 2012 and 2013, however, there is a 3% decrease in 2014 due to the 4% increase in costs and operating expenses. The inflationary increases in cost of supplies and utilities were identified as drivers to a higher cost of operation in 2014.
Fig.7.5-1: Revenue vs. Subsidy vs. QFS
Though the ratio of subsidy from the National Government to revenue declines, NKTI was able to support or provide a higher share to pay for the healthcare cost of its service patients. From 2010 to 2014, for every P1.00 spent for each service patient, 50 centavos or more is covered by NKTI.

49 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig.7.5-2: QFS Share: NKTI and Subsidy
50 55 63 0.57 53
50 45 37 0.43 47
0%
20%
40%
60%
80%
100%
2010 2011 2012 2013 2014
Subsidy
NKTI
The current ratio shows that there was high liquidity over the five-year period that remained within the range of the local industry average of 1.0 to 2.5. This affirms that it has the capability to meet its obligations over the coming year. However, it is important to note that there was a slight decline from 1.69 in 2013 to 1.66 in 2014 due to the increase in fixed assets. Fig. 7.5-3: Current Ratio
0
0.5
1
1.5
2
2.5
2010 2011 2012 2013 2014
The acid test ratio indicates a very good liquidity as well with P1.28 available cash ready to settle current liabilities. Fig. 7.5-4: Acid Test Ratio
0
0.5
1
1.5
2010 2011 2012 2013 2014
The approximate collection time of receivables went up from 86 days in 2010 to 101 days in 2014. Fig.7.5-5: Collection Efficiency
0
50
100
150
2010 2011 2012 2013 2014
From 2010 to 2014, the inventory days on hand indicates an increasing trend, this
means that the supplies are available up to 121 days. Fig. 7.5-6: Inventory Days on Hand
The notable decrease in fixed asset turnover is due to the acquisition of state of the art equipment and facilities improvement. The highest turn-over rate was recorded in 2013, which declined to 0.79 in 2014. Fig. 7.5-7: Fixed Asset Turnover
In 2013, NKTI has started monitoring the PhilHealth Support Value to determine the level by which PhilHealth is able to support the patients’ hospitalization through its aggressive benefit packages. In 2014, there was a 1% decrease in PhilHealth Support Value at NKTI. Fig. 7.5-8: PhilHealth Support Value
7.5a(2) Sectoral Performance. The performance of NKTI in terms of liquidity is compared with another GOCC operating in healthcare. Data shows that NKTI’s performance is better than Hospital X (Fig.7.5-9). According to Business World Magazine, Volume 28, 2014 issue, NKTI ranked 778 among the top 1,000 corporations in the Philippines.
0
50
100
150
2010 2011 2012 2013 2014
14%
13%
13%
13%
14%
14%
15%
2013 2014
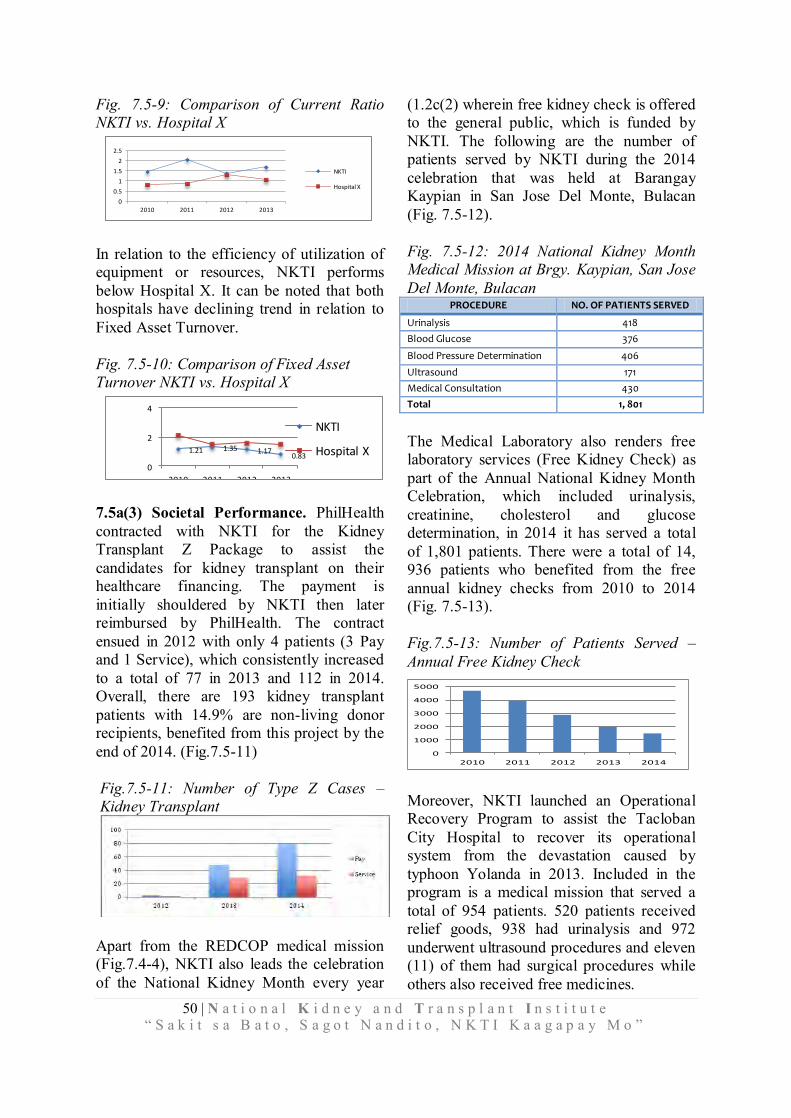
50 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”
Fig. 7.5-9: Comparison of Current Ratio NKTI vs. Hospital X
0
0.5
1
1.5
2
2.5
2010 2011 2012 2013
NKTI
Hospital X
In relation to the efficiency of utilization of equipment or resources, NKTI performs below Hospital X. It can be noted that both hospitals have declining trend in relation to Fixed Asset Turnover. Fig. 7.5-10: Comparison of Fixed Asset Turnover NKTI vs. Hospital X
1.21 1.35 1.170.83
0
2
4
2010 2011 2012 2013
NKTI
Hospital X
7.5a(3) Societal Performance. PhilHealth contracted with NKTI for the Kidney Transplant Z Package to assist the candidates for kidney transplant on their healthcare financing. The payment is initially shouldered by NKTI then later reimbursed by PhilHealth. The contract ensued in 2012 with only 4 patients (3 Pay and 1 Service), which consistently increased to a total of 77 in 2013 and 112 in 2014. Overall, there are 193 kidney transplant patients with 14.9% are non-living donor recipients, benefited from this project by the end of 2014. (Fig.7.5-11) Fig.7.5-11: Number of Type Z Cases – Kidney Transplant
Apart from the REDCOP medical mission (Fig.7.4-4), NKTI also leads the celebration of the National Kidney Month every year
(1.2c(2) wherein free kidney check is offered to the general public, which is funded by NKTI. The following are the number of patients served by NKTI during the 2014 celebration that was held at Barangay Kaypian in San Jose Del Monte, Bulacan (Fig. 7.5-12). Fig. 7.5-12: 2014 National Kidney Month Medical Mission at Brgy. Kaypian, San Jose Del Monte, Bulacan
PROCEDURE NO. OF PATIENTS SERVED
Urinalysis 418
Blood Glucose 376
Blood Pressure Determination 406
Ultrasound 171
Medical Consultation 430
Total 1, 801
The Medical Laboratory also renders free laboratory services (Free Kidney Check) as part of the Annual National Kidney Month Celebration, which included urinalysis, creatinine, cholesterol and glucose determination, in 2014 it has served a total of 1,801 patients. There were a total of 14, 936 patients who benefited from the free annual kidney checks from 2010 to 2014 (Fig. 7.5-13). Fig.7.5-13: Number of Patients Served –
Annual Free Kidney Check
Moreover, NKTI launched an Operational Recovery Program to assist the Tacloban City Hospital to recover its operational system from the devastation caused by typhoon Yolanda in 2013. Included in the program is a medical mission that served a total of 954 patients. 520 patients received relief goods, 938 had urinalysis and 972 underwent ultrasound procedures and eleven (11) of them had surgical procedures while others also received free medicines.
0
1000
2000
3000
4000
5000
2010 2011 2012 2013 2014
51 | N a t i o n a l K i d n e y a n d T r a n s p l a n t I n s t i t u t e “ S a k i t s a B a t o , S a g o t N a n d i t o , N K T I K a a g a p a y M o ”