
Mechanical ventilator weaning and Physiotherapist...
65
MECHANICAL VENTILATOR AND WEANING FROM MECHANICAL VENTILATOR Mr.Sakol Patcharapanyawat BMC’s Chest PT
Transcript of Mechanical ventilator weaning and Physiotherapist...
MECHANICAL VENTILATOR
AND
WEANING
FROM
MECHANICAL VENTILATOR
Mr.Sakol Patcharapanyawat
BMC’s Chest PT
Contents
- Basic respiratory system Mechanics
- Basic Physiology of gas Exchange
- Assessment and management in respiratory
insufficiency
- Mechanical ventilator (Mode and Weaning process)
Factors Contributing to
understand to Mechanical
Ventilator
Atmosphere
Tissue cell
Alveoli of lungs
Pulmonary
circulation
Systemic
circulation
CO2 O2
Food + O2 CO2 + HO2 + ATP
O2
CO2
CO2
O2
1
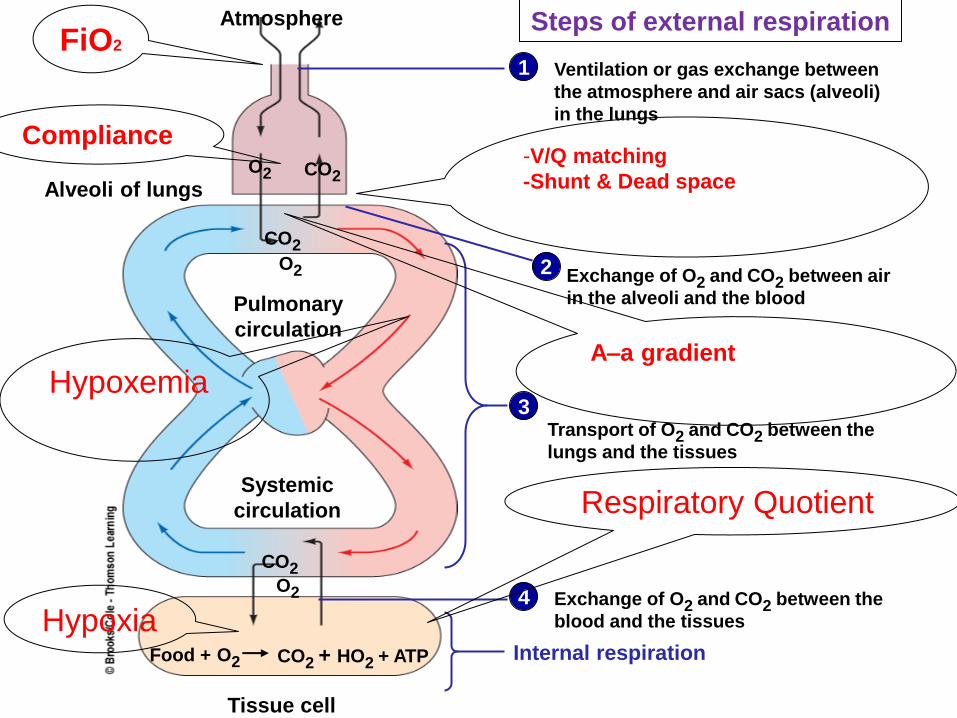
Steps of external respiration
Ventilation or gas exchange between
the atmosphere and air sacs (alveoli)
in the lungs
Exchange of O2 and CO2 between air
in the alveoli and the blood
Transport of O2 and CO2 between the
lungs and the tissues
Exchange of O2 and CO2 between the
blood and the tissues
Internal respiration
2
3
4
FiO2
Compliance
Respiratory Quotient
-V/Q matching
-Shunt & Dead space
A–a gradient
Hypoxemia
Hypoxia
http://www.aic.cuhk.edu.hk/web8/mechanical_ventilation.htm
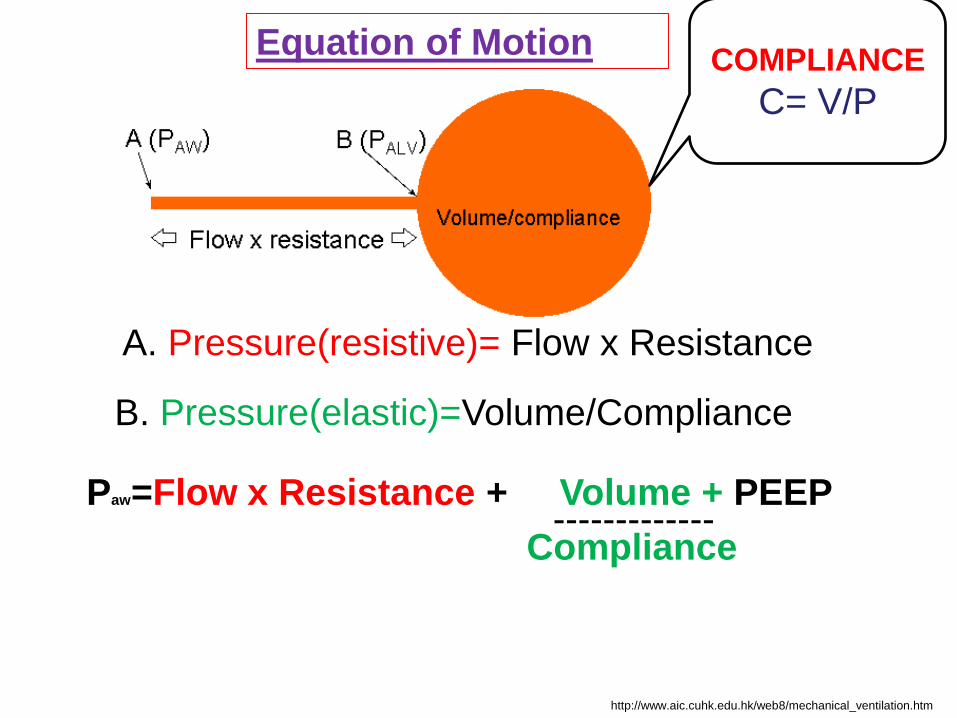
Paw=Flow x Resistance + Volume + PEEP
Compliance -------------
Equation of Motion
A. Pressure(resistive)= Flow x Resistance
B. Pressure(elastic)=Volume/Compliance
COMPLIANCE
C= V/P
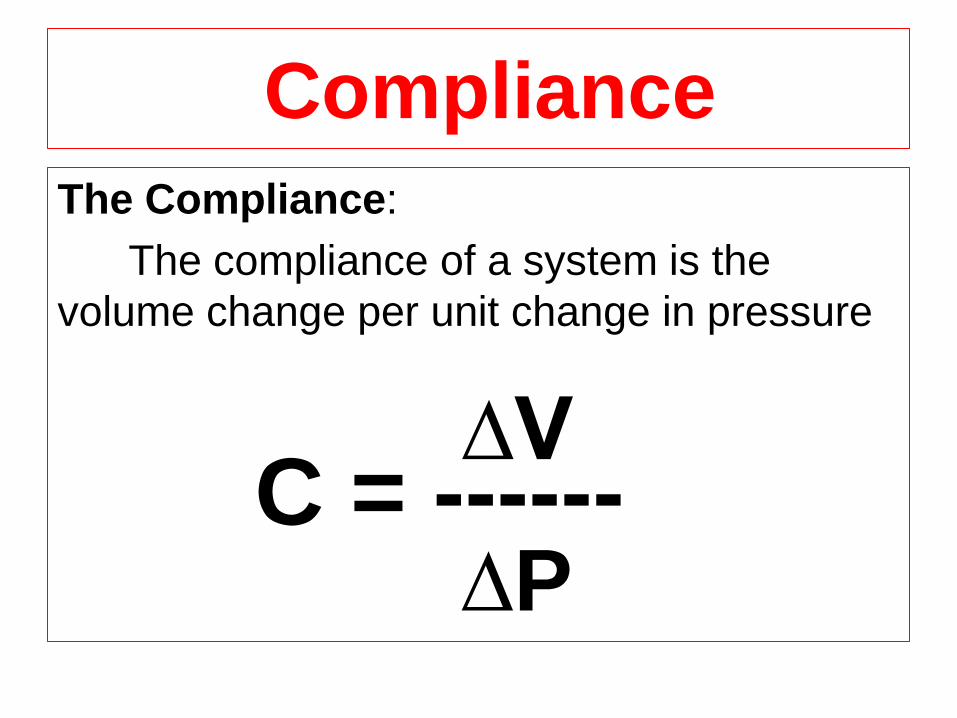
Compliance
The Compliance:
The compliance of a system is the
volume change per unit change in pressure
C = ------ ∆V
∆P
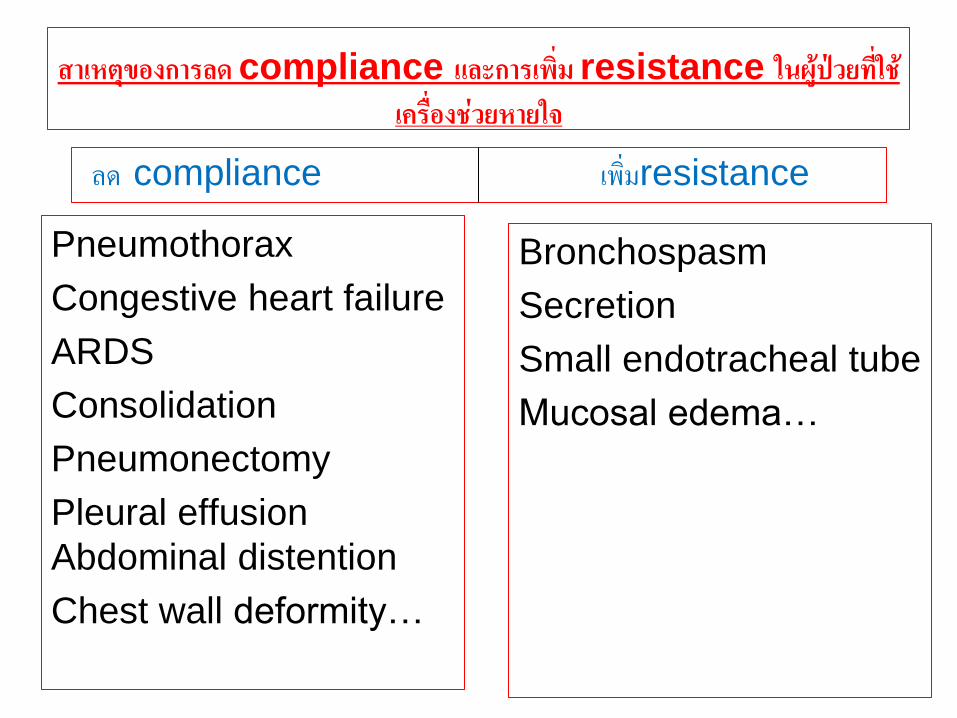
สาเหตของการลด compliance และการเพม resistance ในผปวยทใช
เครองชวยหายใจ
Pneumothorax
Congestive heart failure
ARDS
Consolidation
Pneumonectomy
Pleural effusion
Abdominal distention
Chest wall deformity…
Bronchospasm
Secretion
Small endotracheal tube
Mucosal edema…
ลด compliance เพมresistance
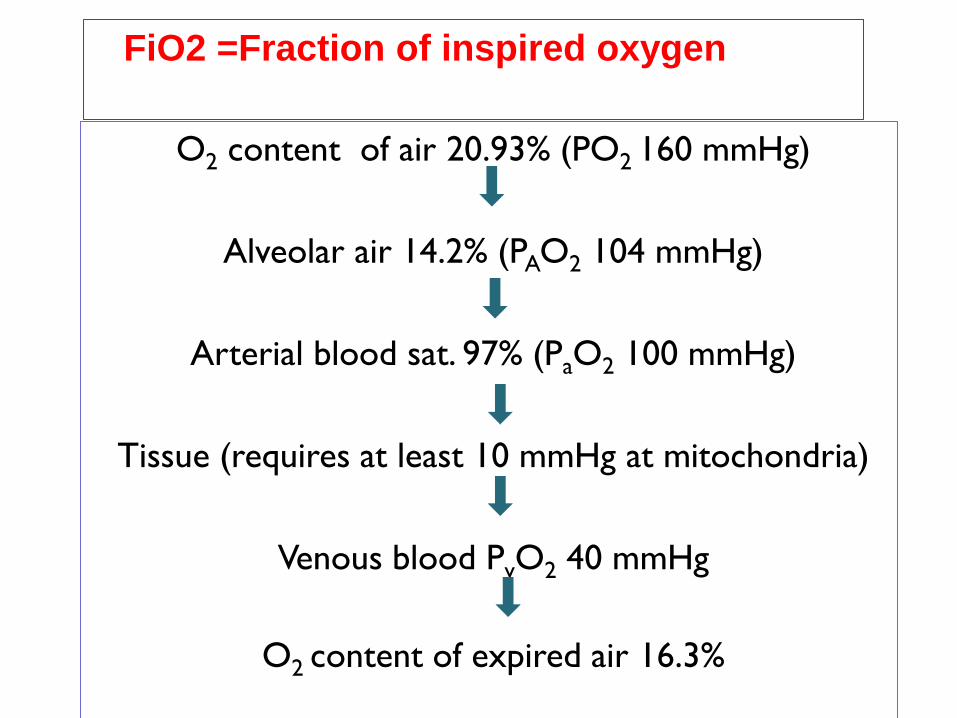
FiO2 =Fraction of inspired oxygen
O2 content of air 20.93% (PO2 160 mmHg)
Alveolar air 14.2% (PAO2 104 mmHg)
Arterial blood sat. 97% (PaO2 100 mmHg)
Tissue (requires at least 10 mmHg at mitochondria)
Venous blood PvO2 40 mmHg
O2 content of expired air 16.3%
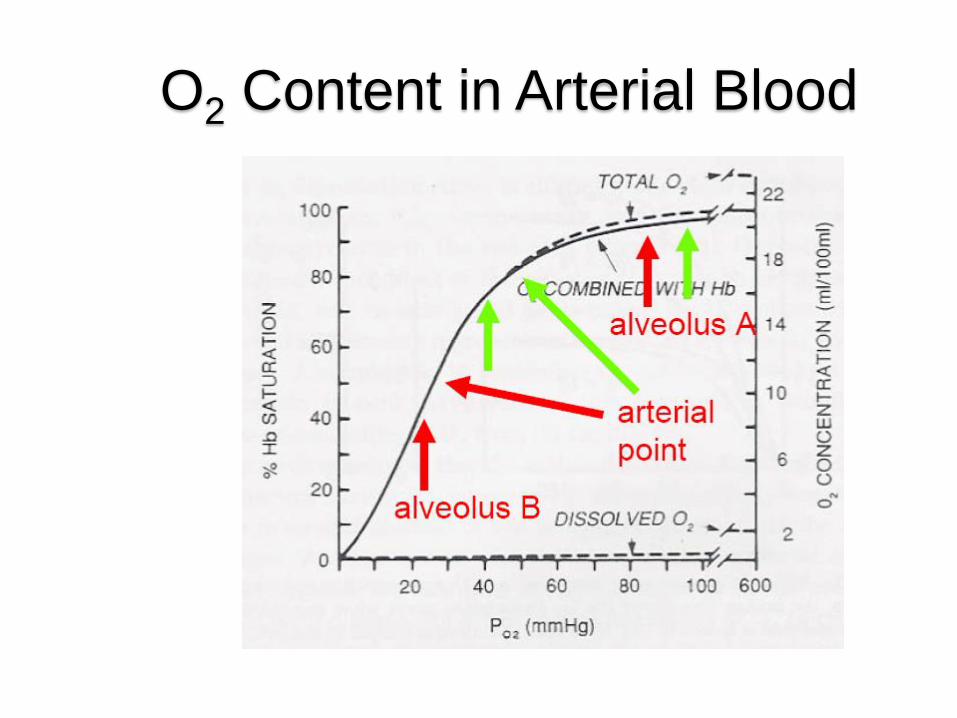
O2 Content in Arterial Blood
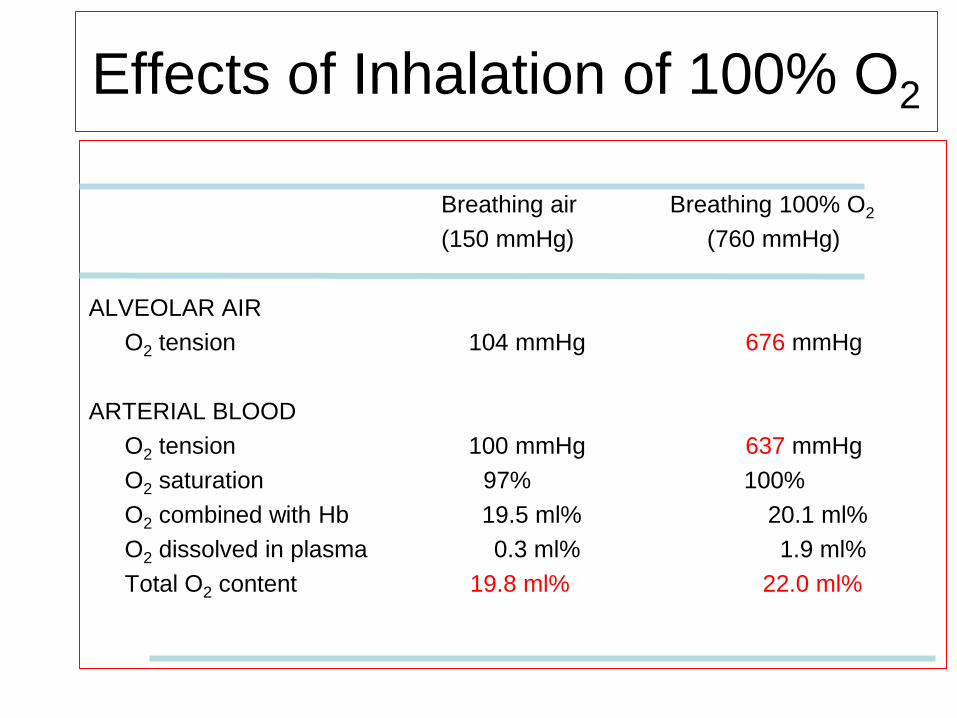
Effects of Inhalation of 100% O2
Breathing air Breathing 100% O2
(150 mmHg) (760 mmHg)
ALVEOLAR AIR
O2 tension 104 mmHg 676 mmHg
ARTERIAL BLOOD
O2 tension 100 mmHg 637 mmHg
O2 saturation 97% 100%
O2 combined with Hb 19.5 ml% 20.1 ml%
O2 dissolved in plasma 0.3 ml% 1.9 ml%
Total O2 content 19.8 ml% 22.0 ml%
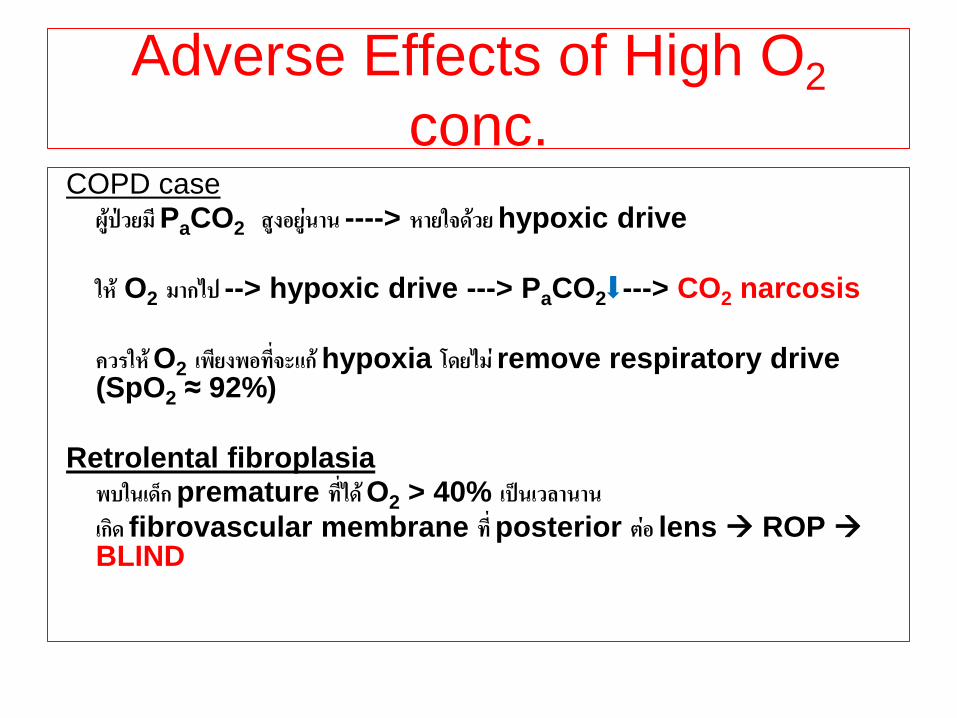
Adverse Effects of High O2
conc. COPD case ผปวยม PaCO2 สงอยนาน ----> หายใจดวย hypoxic drive
ให O2 มากไป --> hypoxic drive ---> PaCO2 ---> CO2 narcosis
ควรให O2 เพยงพอทจะแก hypoxia โดยไม remove respiratory drive
(SpO2 ≈ 92%)
Retrolental fibroplasia พบในเดก premature ทได O2 > 40% เปนเวลานาน
เกด fibrovascular membrane ท posterior ตอ lens ROP BLIND
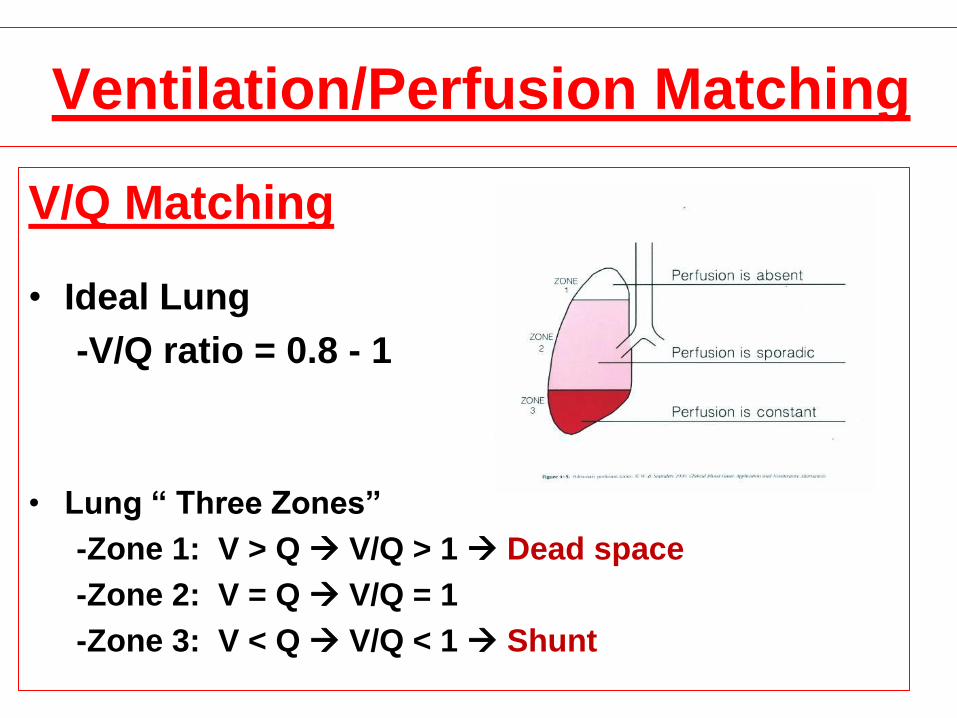
Ventilation/Perfusion Matching
V/Q Matching
• Ideal Lung
-V/Q ratio = 0.8 - 1
• Lung “ Three Zones”
-Zone 1: V > Q V/Q > 1 Dead space
-Zone 2: V = Q V/Q = 1
-Zone 3: V < Q V/Q < 1 Shunt
SHUNT AND DEAD SPACE ?
Dead Space
#Non-gas exchanging
Areas –or
#Areas of the lungs
Normally involved in gas
Exchange ,however blocked
or
Impaired blood flow
preventing this.
Shunt
Results from anything
that interferes with the
Movement of air down
to the gas exchanging
areas.
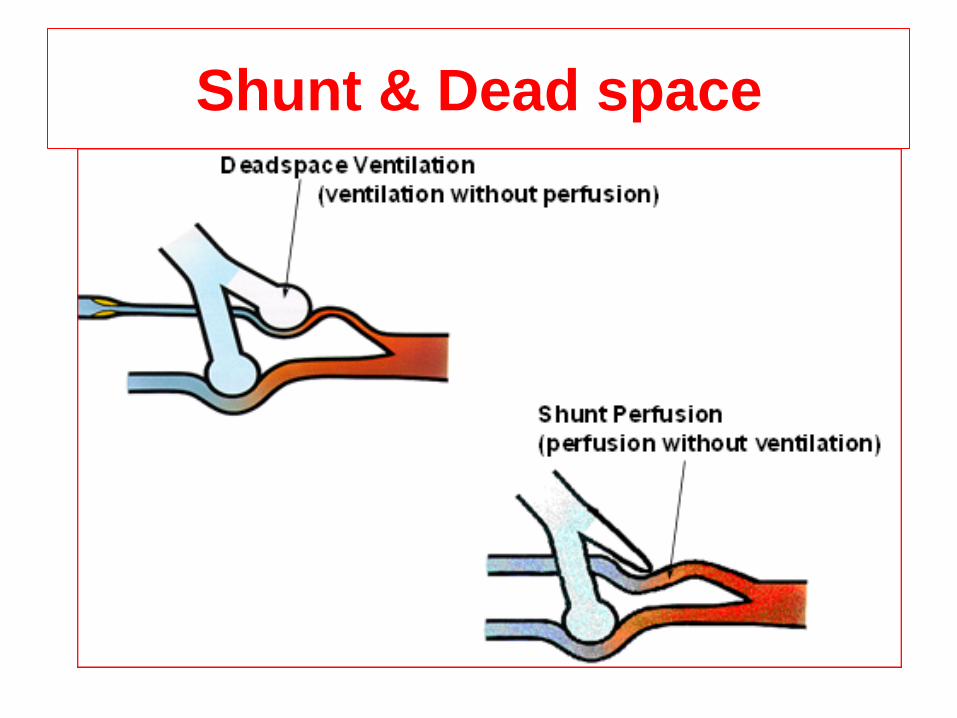
Shunt & Dead space
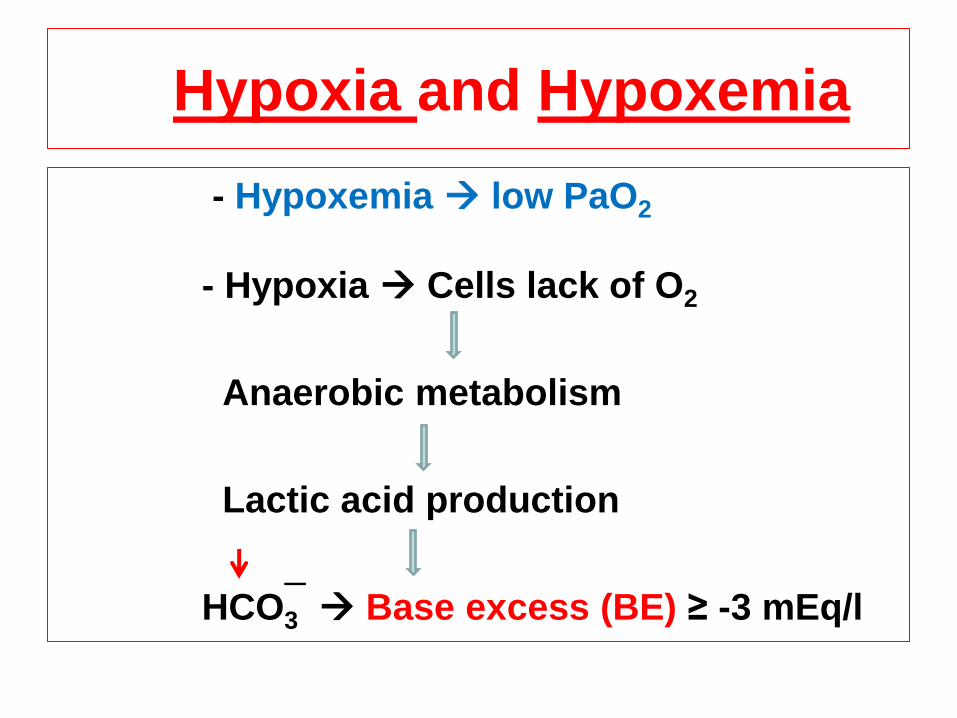
Hypoxia and Hypoxemia
- Hypoxemia low PaO2
- Hypoxia Cells lack of O2
Anaerobic metabolism
Lactic acid production
HCO3 Base excess (BE) ≥ -3 mEq/l
_
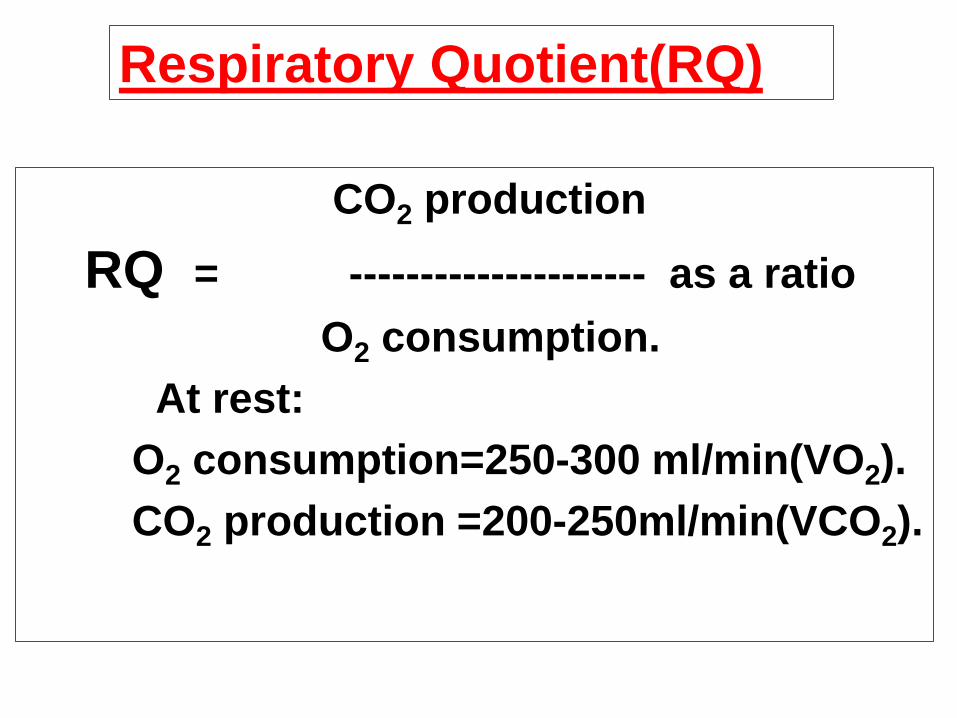
CO2 production
RQ = --------------------- as a ratio
O2 consumption.
At rest:
O2 consumption=250-300 ml/min(VO2).
CO2 production =200-250ml/min(VCO2).
Respiratory Quotient(RQ)
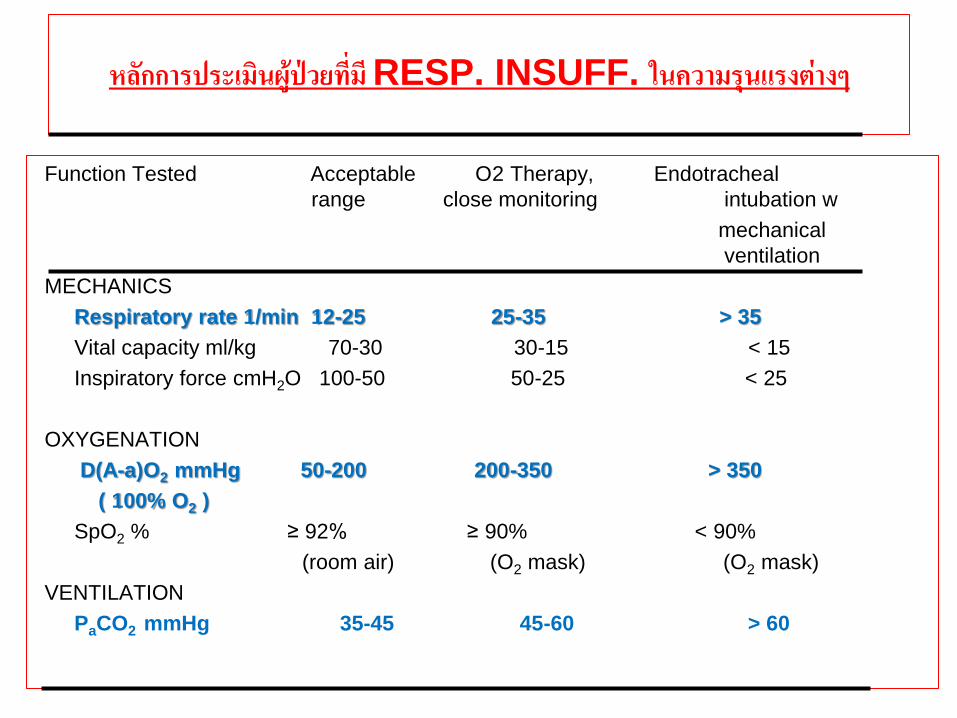
หลกการประเมนผปวยทม RESP. INSUFF. ในความรนแรงตางๆ
Function Tested Acceptable O2 Therapy, Endotracheal
range close monitoring intubation w
mechanical
ventilation
MECHANICS
Respiratory rate 1/min 12-25 25-35 > 35
Vital capacity ml/kg 70-30 30-15 < 15
Inspiratory force cmH2O 100-50 50-25 < 25
OXYGENATION
D(A-a)O2 mmHg 50-200 200-350 > 350
( 100% O2 )
SpO2 % ≥ 92% ≥ 90% < 90%
(room air) (O2 mask) (O2 mask)
VENTILATION
PaCO2 mmHg 35-45 45-60 > 60
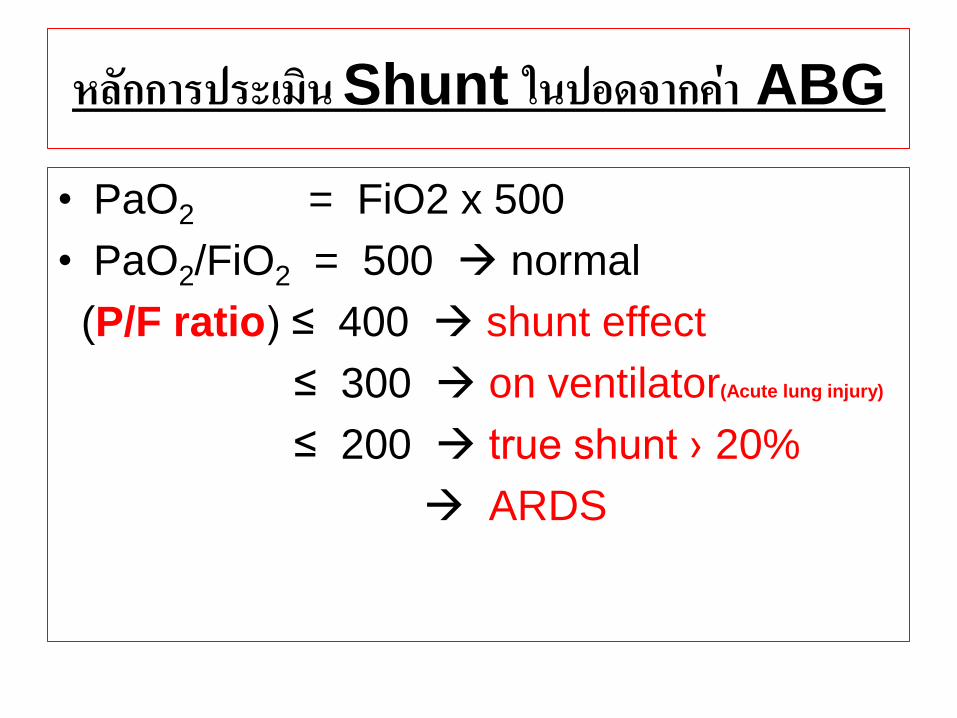
หลกการประเมน Shunt ในปอดจากคา ABG
• PaO2 = FiO2 x 500
• PaO2/FiO2 = 500 normal
(P/F ratio) ≤ 400 shunt effect
≤ 300 on ventilator(Acute lung injury)
≤ 200 true shunt › 20%
ARDS
Definition of Weaning
The transition process from
total ventilatory support
to spontaneous breathing.
This period may take many forms ranging
from abrupt withdrawal to gradual
withdrawal from ventilatory support.
CPG : Weaning(1)
หลกการพจารณากอนการหยาเครองชวยหายใจ -หมดขอบงชทตองใชเครองชวยหายใจ -อาการทางคลนคหรอภาพ Chest X-Rayดขน
-STABLE HEMODYNAMIC -ไมมความผดปกตของกรดดาง รวมทงระดบ Mg,PO4,K
-ไมมความเจบปวด -ไมม active GI bleeding, Hyper/hypothyroid
-สภาวะทางโภชนาการคงท
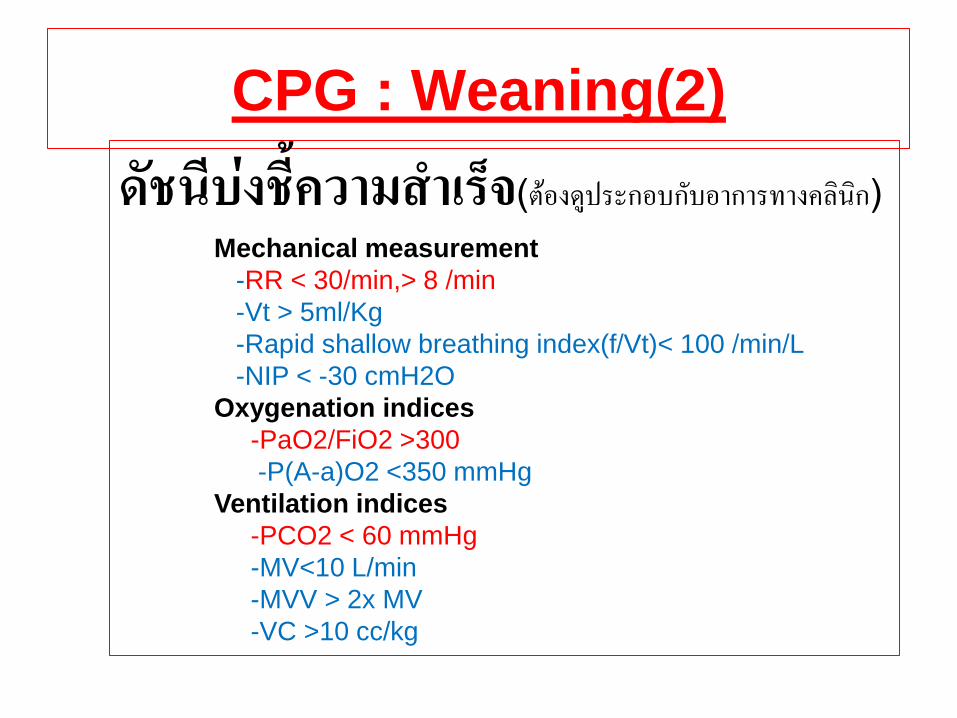
CPG : Weaning(2)
ดชนบงชความส าเรจ(ตองดประกอบกบอาการทางคลนก) Mechanical measurement
-RR < 30/min,> 8 /min
-Vt > 5ml/Kg
-Rapid shallow breathing index(f/Vt)< 100 /min/L
-NIP < -30 cmH2O
Oxygenation indices
-PaO2/FiO2 >300
-P(A-a)O2 <350 mmHg
Ventilation indices
-PCO2 < 60 mmHg
-MV<10 L/min
-MVV > 2x MV
-VC >10 cc/kg
MECHANICAL VENTILATOR
What is mechanical ventilator?
Definition
Mechanical ventilator is the use of a mechanical
device (machine) to inflate and deflate the lungs.
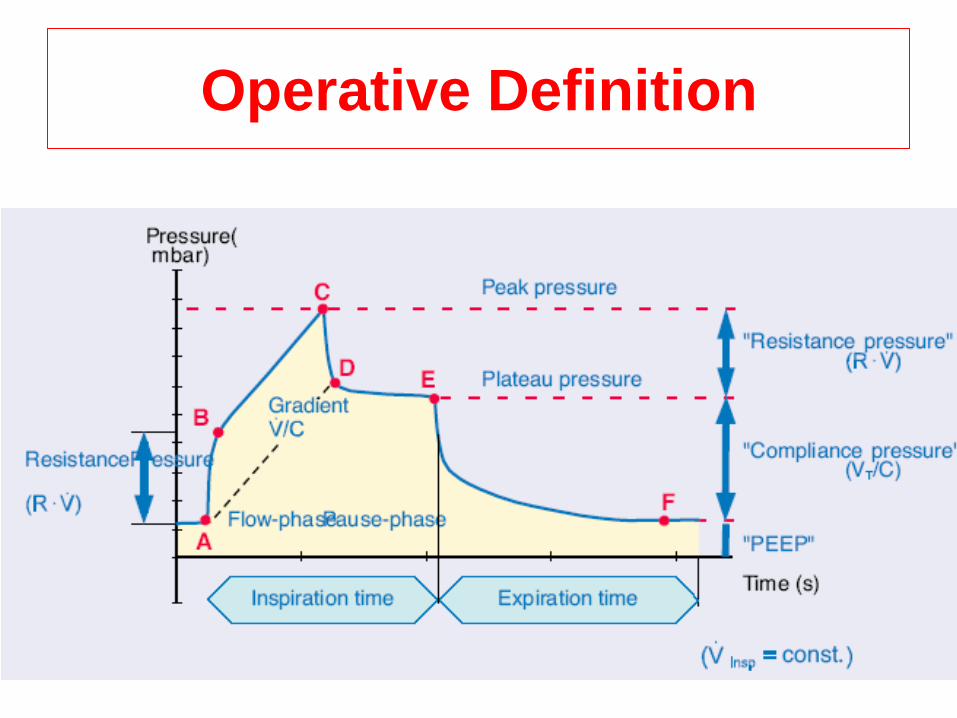
Operative Definition
1. Tidal volume (Vt) คอ ปรมาตรอากาศทไหลเขาออกจากปอดผปวยตอการหายใจ1 ครง วดไดจากลมทออกจากเครองทต าแหนง expiratory value
2. Minute volume (MV) คอ ปรมาณลมหายใจออกทงหมดใน 1 นาท มหนวยเปน (L/min) (MV = Vt X RR) 3.Peak Inspiratory Pressure (PIP, Ppeak) คอ คาความดนในหลอดลมทวดไดสงสดในจงหวะการหายใจเขา หรออาจเรยก peak airway pressure
4.Plateau Pressure (Ppla) คอ คาความดนในจงหวะสนสดการหายใจเขาแลวคางไว บงชถงความยดหยนของเนอปอด
Operative Definition
Phases of breath
• Start inspiration-------Trigger
• Sustain inspiration------ Limit
• End inspiration--------Cycling
• Sustain Expiratory-----Base line
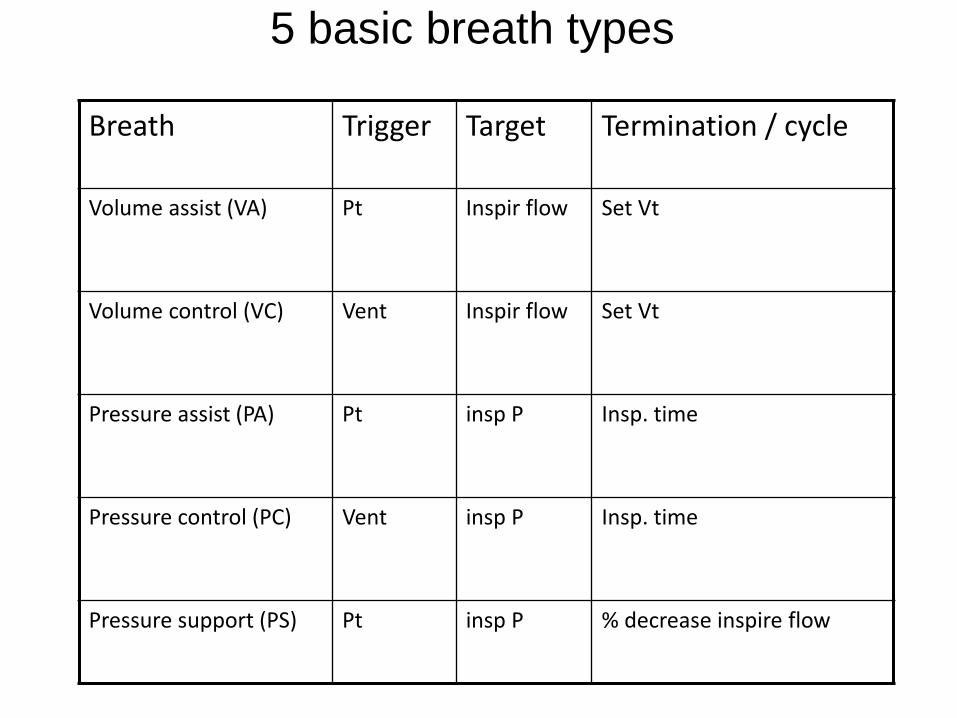
5 basic breath types
Breath Trigger Target Termination / cycle
Volume assist (VA)
Pt Inspir flow Set Vt
Volume control (VC)
Vent Inspir flow Set Vt
Pressure assist (PA)
Pt insp P Insp. time
Pressure control (PC)
Vent insp P Insp. time
Pressure support (PS) Pt insp P % decrease inspire flow
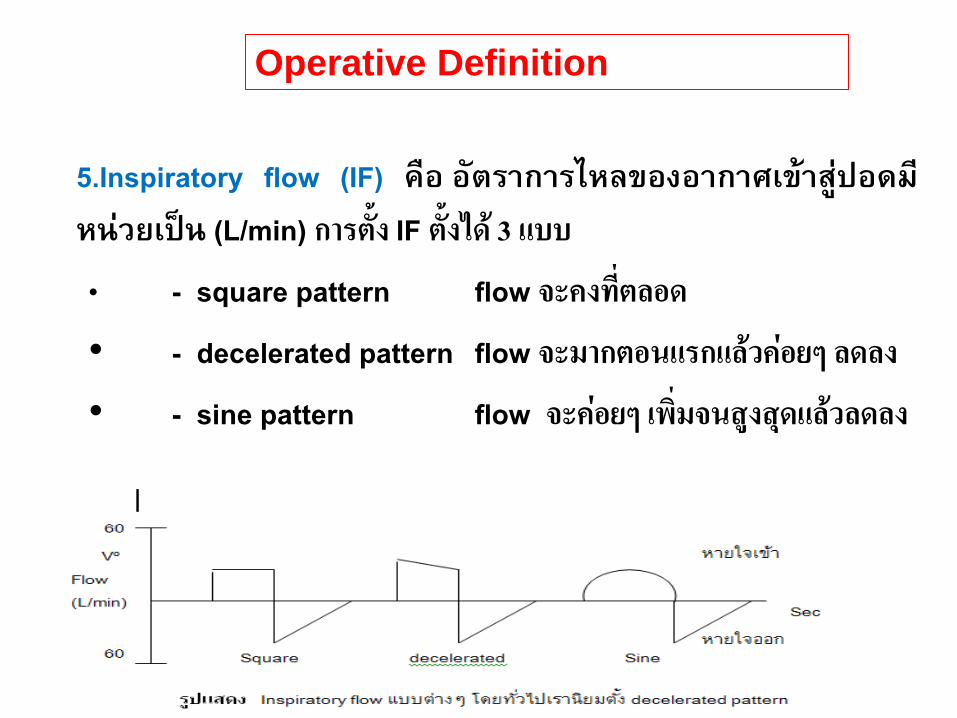
5.Inspiratory flow (IF) คอ อตราการไหลของอากาศเขาสปอดมหนวยเปน (L/min) การตง IF ตงได 3 แบบ
• - square pattern flow จะคงทตลอด
• - decelerated pattern flow จะมากตอนแรกแลวคอยๆ ลดลง
• - sine pattern flow จะคอยๆ เพมจนสงสดแลวลดลง
Operative Definition
6.Airway resistance คอ แรงตานในหลอดลม ซงถาวดจากเครองชวยหายใจมกจะรวมแรงตานในทอชวยหายใจเขาไปดวย วดโดยการใชสตร P peak – P pla มหนวยเปน Cm H2O
IF
ในทางปฏบตเวลาวดเราจะตงเครองชวยหายใจ โดยใช constant flow ท 60 L/ min ซงจะท าให IF = 1 L/sec ท าใหเวลาวด airway resistance จะค านวณงายโดยเอา Ppeak ลบ Ppla ไดคาออกมาเลย
7. I : E ratio คอ สดสวนของเวลาทหายใจเขา (I) ตอเวลาทหายใจออก (E) การหาปกต I : E จะนอยกวา 1 เสมอ ยกเวน กรณพเศษทเราตองการตงเวลาการหายใจเขาใหนานกวาปกตในผปวยท hypoxemia ท refractory ตอวธการหายใจทวไป
8.Sensitivity (S) คอ คาความไวของเครองทก าหนดใหผปวยตองออกแรงเพอกระตน(trigger) ใหมการหายใจเขา 9. Positive end expiratory pressure (PEEP) คอ การก าหนดใหมแรงดนบวกในตอนหายใจออก ท าใหมลมคางอยบางสวนในปอด
Operative Definition
Operative Definition
10.ลกษณะการหายใจ
- Assist ventilation (A) คอ การหายใจแรงดนบวก โดยใหผปวยเปนผกระตนการหายใจเขา - Control ventilation (C) คอ การหายใจแบบแรงดนบวก โดยเครองเปนตวก าหนดการหายใจทกครง ดงนน RR เครอง = RR ผปวย - Assist/ control ventilation (A/C) คอ การหายใจผสมผสานของ 2 วธขางตน คอ เครองจะหายใจใหผปวยเทากบ RR ทตง แตในบางจงหวะ ถาผปวยหายใจไดเองและมแรงดงมากกวา Sensitivity ทตงไว เครองกจะท างานเพมได
Operative Definition
Common modes of ventilation
1. Continuous mandatory ventilation (CMV) เครองเปนตวก าหนดลมทกครงของการหายใจ โดยอาจเปนแบบ A, C, A/C กได
2. Synchronous mandatory ventilation (SIMV) เครองเปนตวก าหนดลมเขาปอดเปนครงคราวสลบกบการหายใจโดยผปวยเปนคนเรมตน
3. Pressure Control ventilation (PCV) เครองจะใหแรงดนบวกเขาโดยการควบคมใหผปวยหมดแบบ control มกใชใน ARDS รนแรง ท airway pressure สงมาก
4. Pressure support ventilation (PSV) เครองจะใหแรงดนบวกเขาแตการควบคมเวลาในการหายใจเขาออกผปวยจะเปนผก าหนดเพยงแตตงระดบความดนไวเทานน
5. Continuous positive airway pressure (CPAP) คอ การหายใจทผปวยตองออกแรงหายใจเอง แตเครองจะชวยโดยการอดลมเขาในทอเพอรกษาระดบแรงดนบวกตลอดทงการหายใจเขาและออก
Types of Ventilator
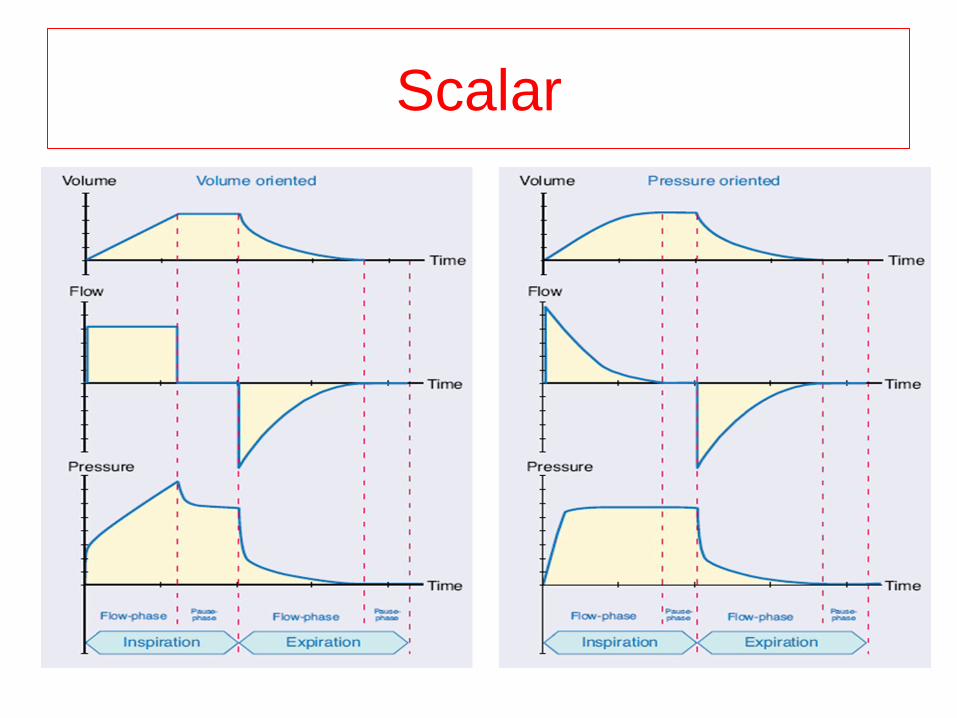
Waveforms Scalar:
Pressure – time
Volume – time
Flow – time
Loops: Pressure – volume
Volume – Flow
Flow – pressure
Trends:
Scalar
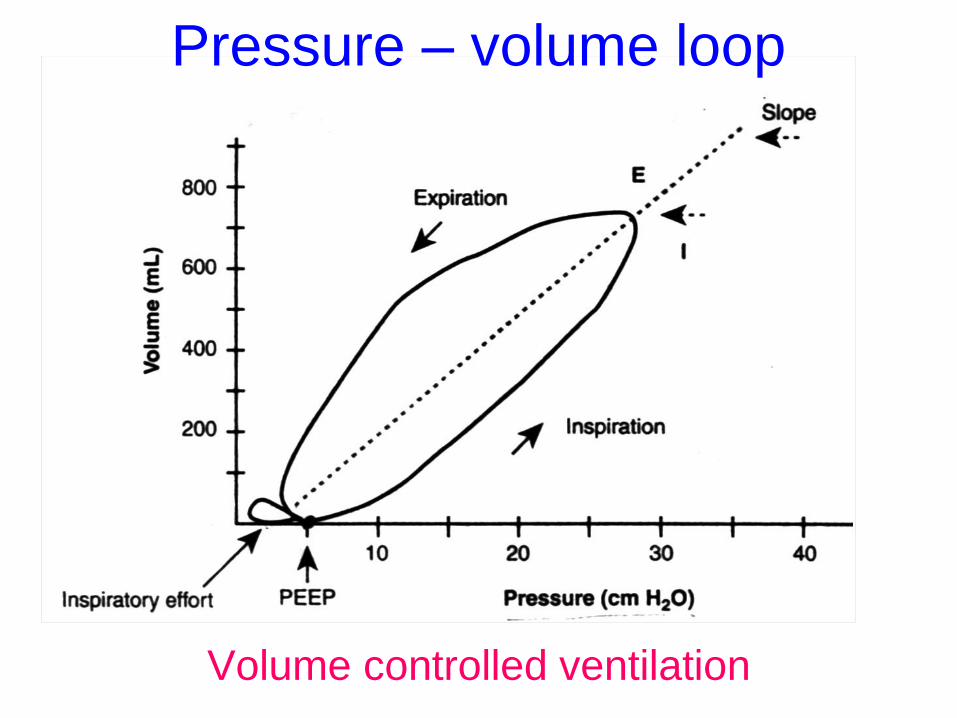
Pressure – volume loop
Volume controlled ventilation
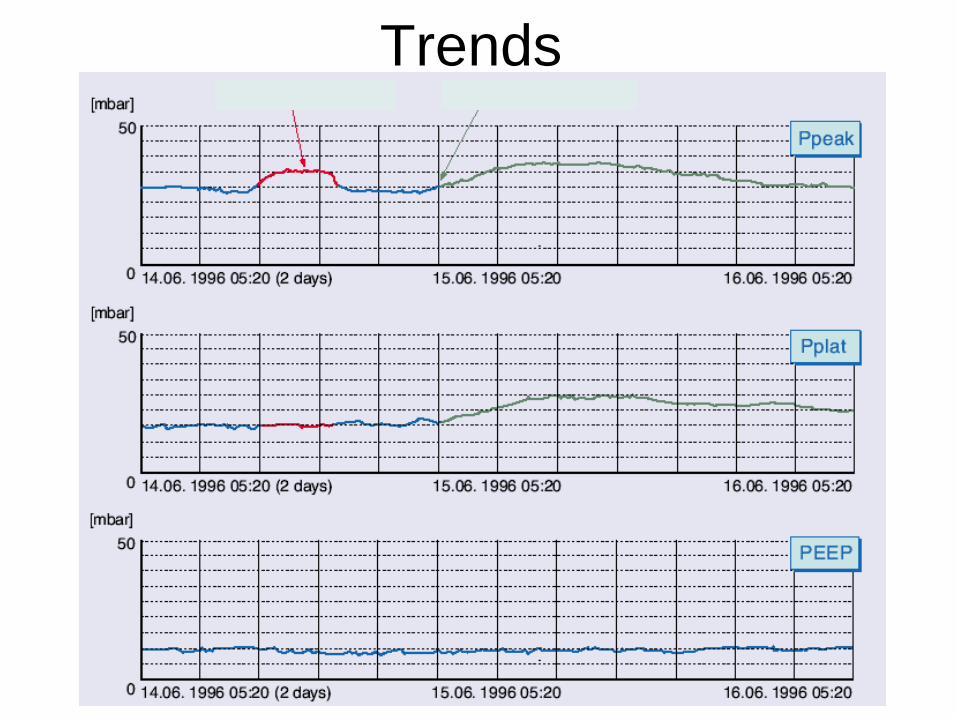
Trends
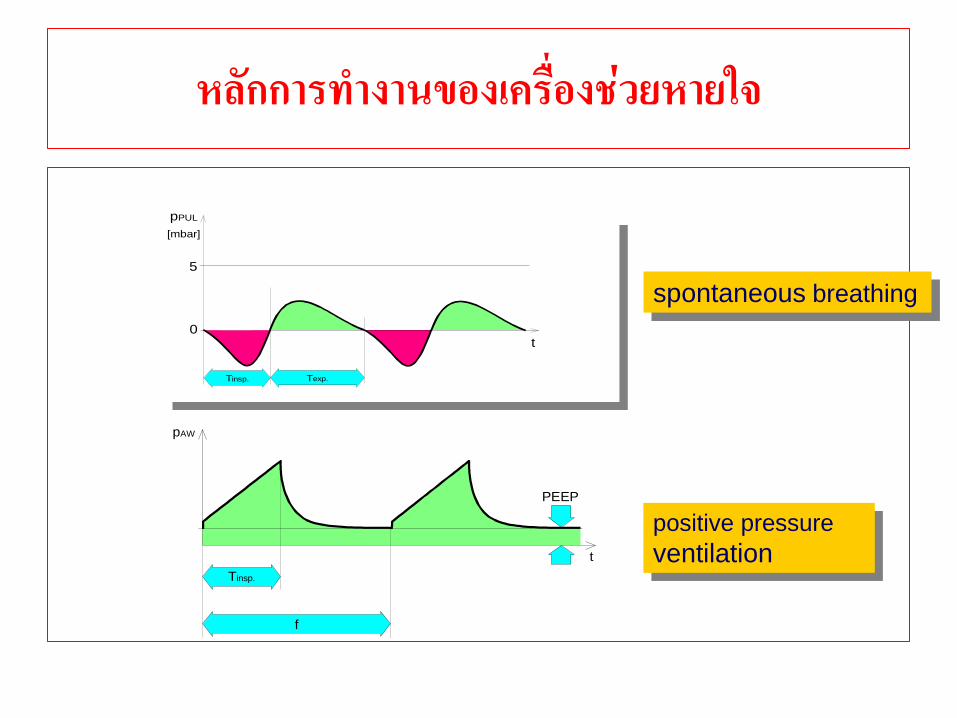
หลกการท างานของเครองชวยหายใจ
spontaneous breathing
f
t
pAW
PEEP
Tinsp.
positive pressure
ventilation
t
Tinsp. Texp.
5
0
[mbar]
pPUL
ชนดของเครองชวยหายใจ
แบงไดเปน 3 แบบตามการสนสดของการหายใจเขา(Cycle)
1.Volume cycle ventilator เครองชวยหายใจชนดนการหายใจเขาจะสนสดลงเมอไดปรมาตรตามทตงไว เปลยนเปนการหายใจออกทนท 2. Pressure cycle ventilator เครองชวยหายใจชนดนการหายใจเขาจะสนสดลงเมอไดรบความดนตามทตงไว เครองชวยหายใจชนดน 3. Time cycle ventilator เครองชวยหายใจชนดนใชระยะเวลาในการหายใจเขาเปนตวสนสดระยะเวลาการหายใจเขา เมอครบเวลาตามทตงไวแลวจะสนสดการหายใจเขาเปนหายใจออกทนท *** Dual Control เครองชวยหายใจทประกอบดวย Pressure control และ Volume control รวมกน ความดนในการหายใจเขาระหวางการหายใจแตละครงจะปรบเปลยนไปโดยอตโนมต
ชนดของเครองชวยหายใจ
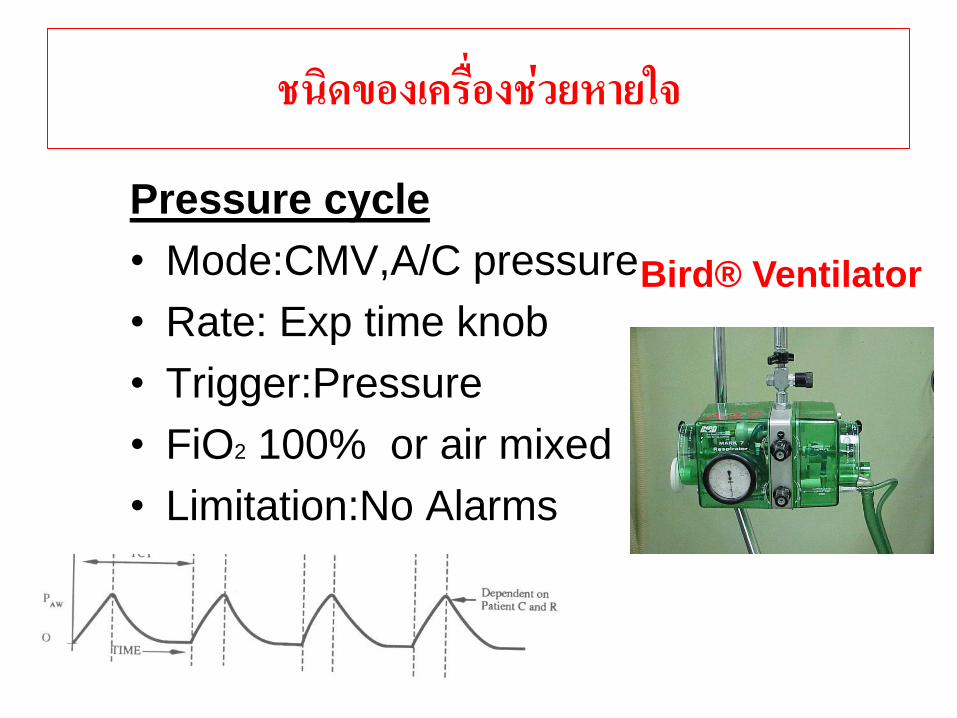
Pressure cycle
• Mode:CMV,A/C pressure
• Rate: Exp time knob
• Trigger:Pressure
• FiO2 100% or air mixed
• Limitation:No Alarms
Bird® Ventilator
ชนดของเครองชวยหายใจ
Volume cycle

ชนดของเครองชวยหายใจ
Time cycle
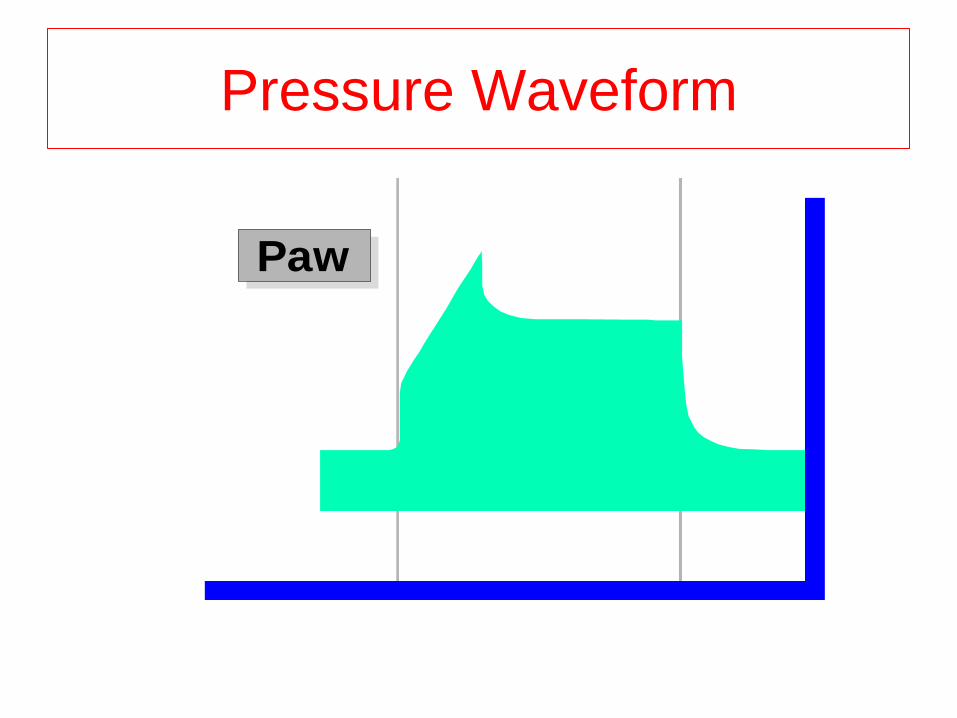
Pressure Waveform
Paw
Modes of Mechanical
Ventilation
and
Step of Weaning.
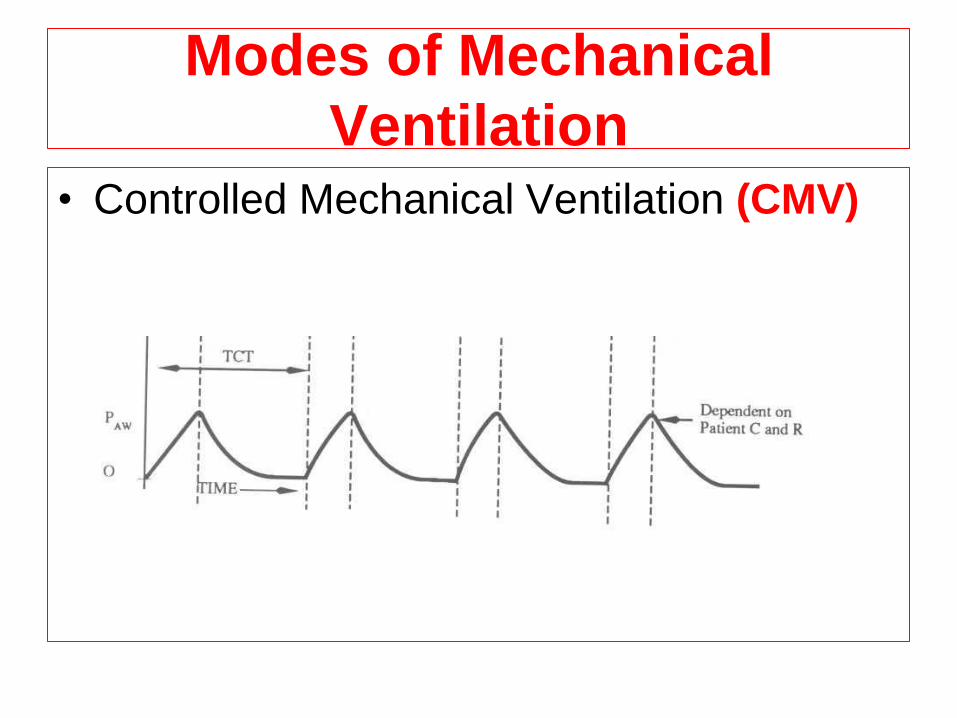
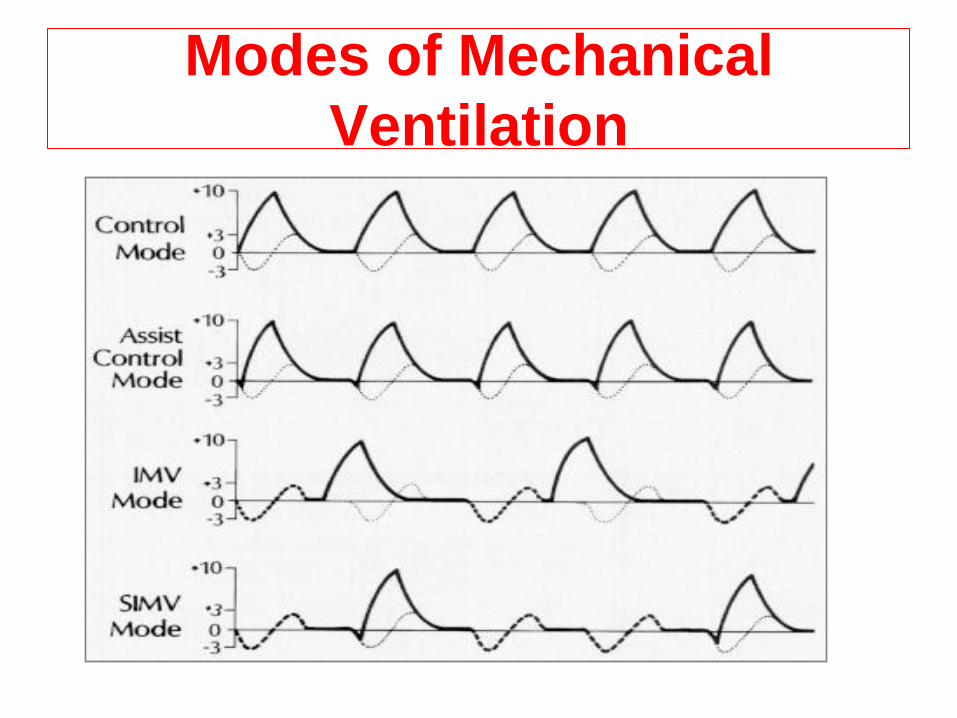
Modes of Mechanical
Ventilation • Controlled Mechanical Ventilation (CMV)
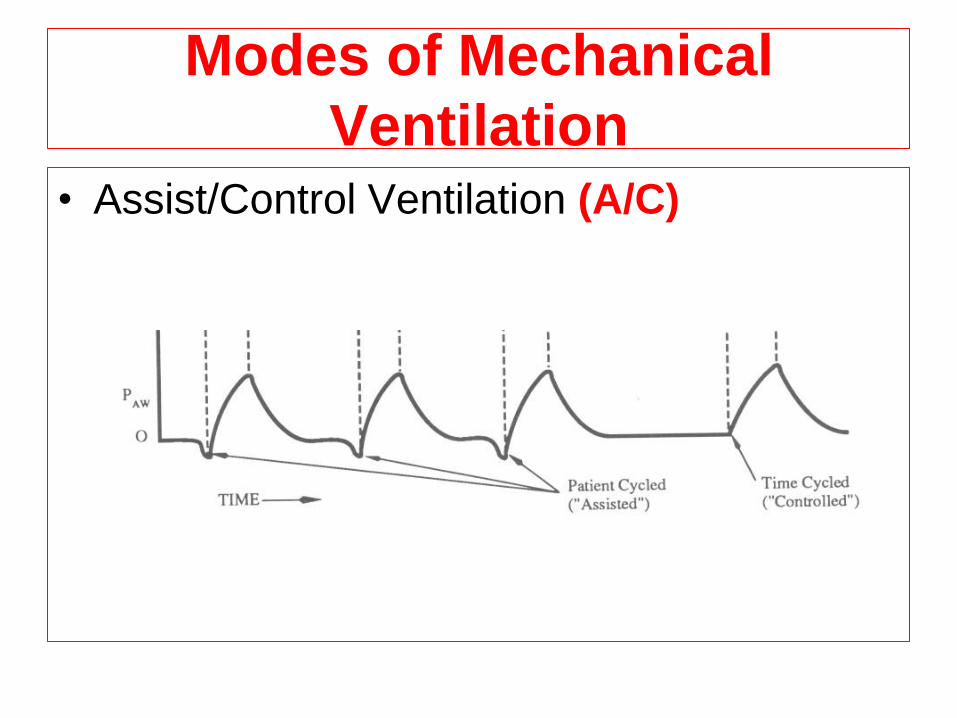
Modes of Mechanical
Ventilation • Assist/Control Ventilation (A/C)
Weaning Process
• CMV A/C T-piece extubation
O2 mask room air
• Prolonged ventilated: A/CT-piece
A/CT-piece…
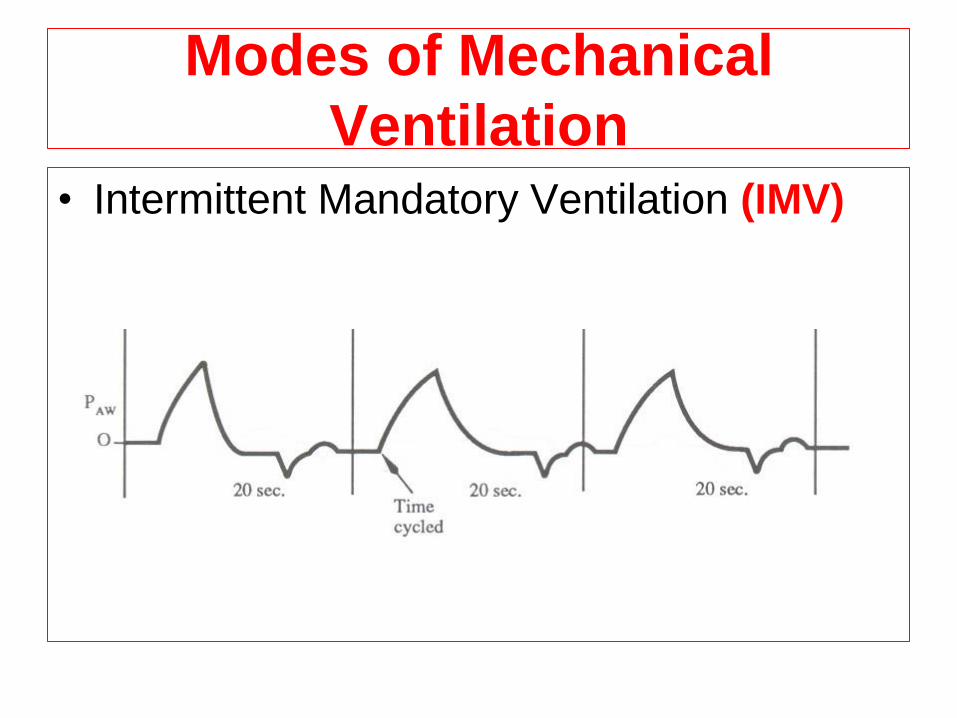
Modes of Mechanical
Ventilation • Intermittent Mandatory Ventilation (IMV)
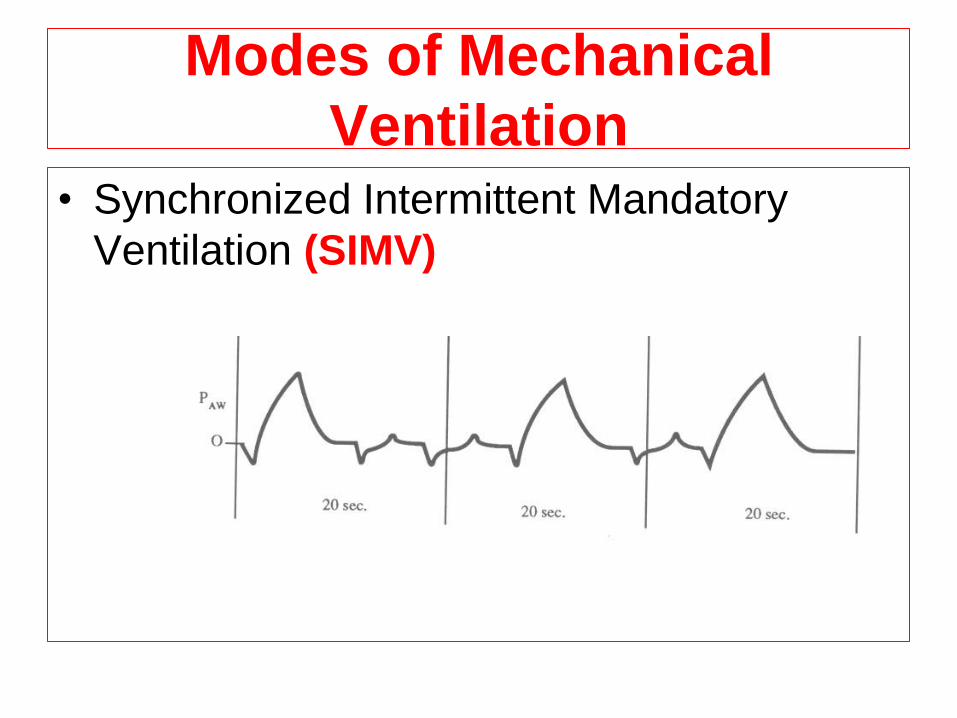
Modes of Mechanical
Ventilation • Synchronized Intermittent Mandatory
Ventilation (SIMV)
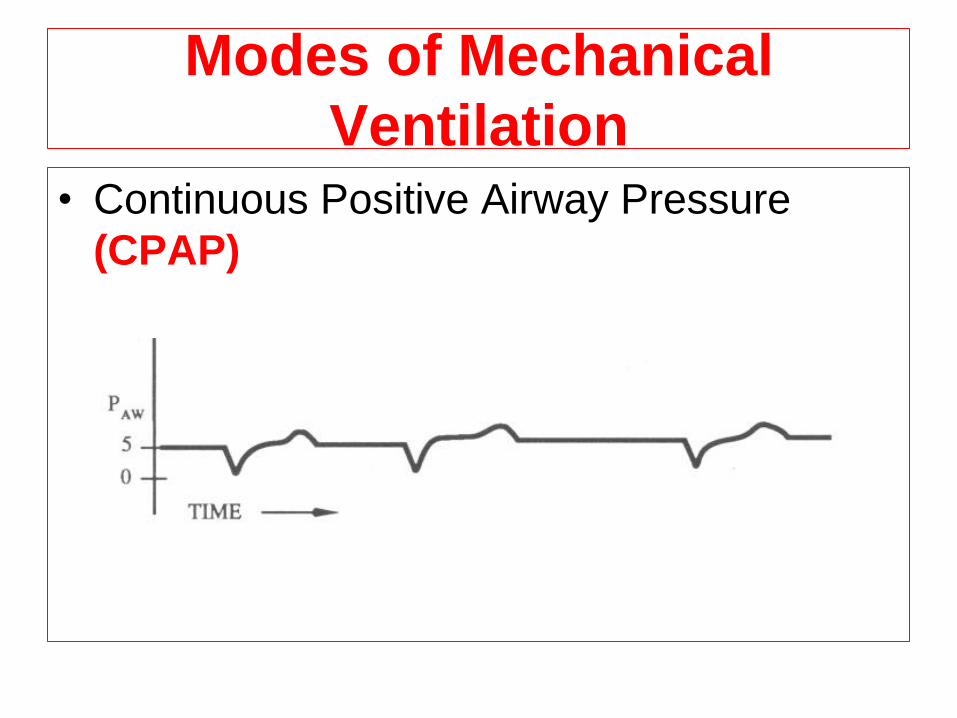
Modes of Mechanical
Ventilation • Continuous Positive Airway Pressure
(CPAP)
Modes of Mechanical
Ventilation
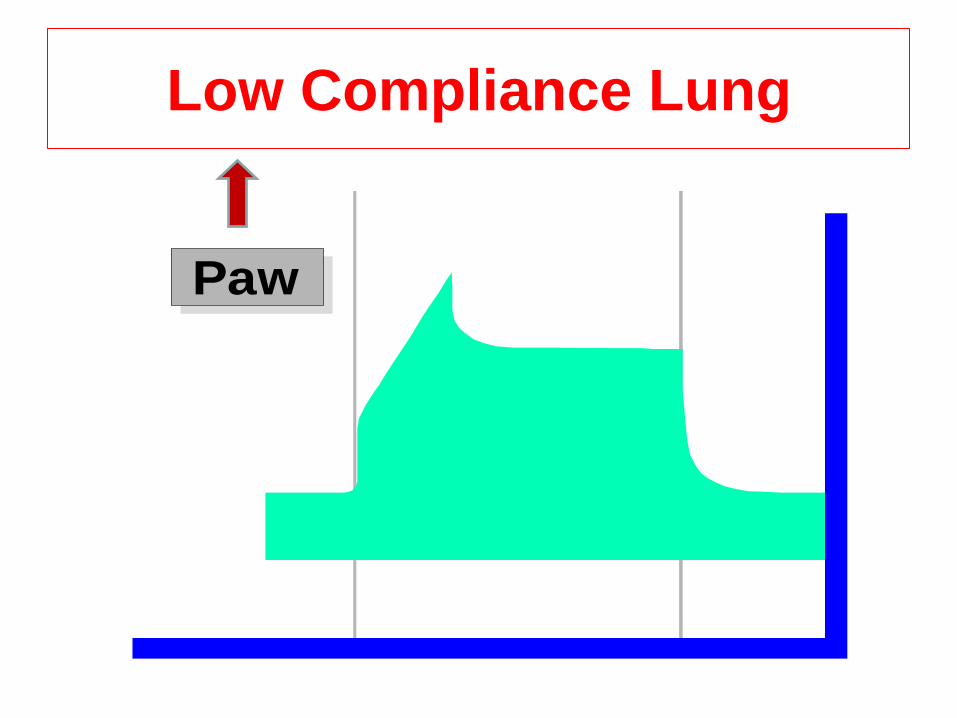
Low Compliance Lung
Paw
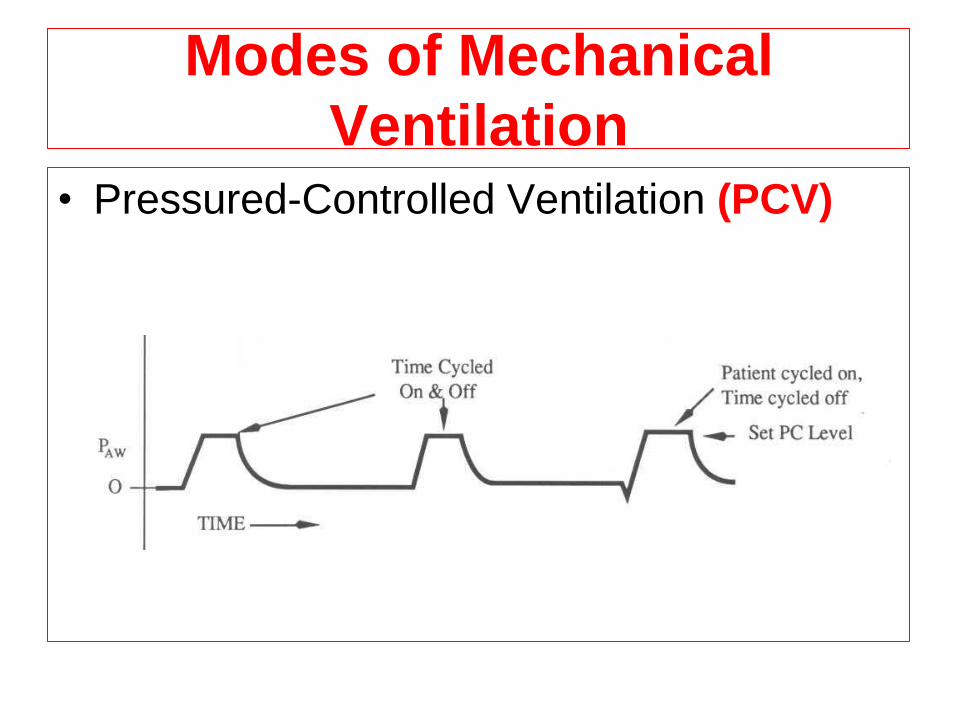
Modes of Mechanical
Ventilation • Pressured-Controlled Ventilation (PCV)
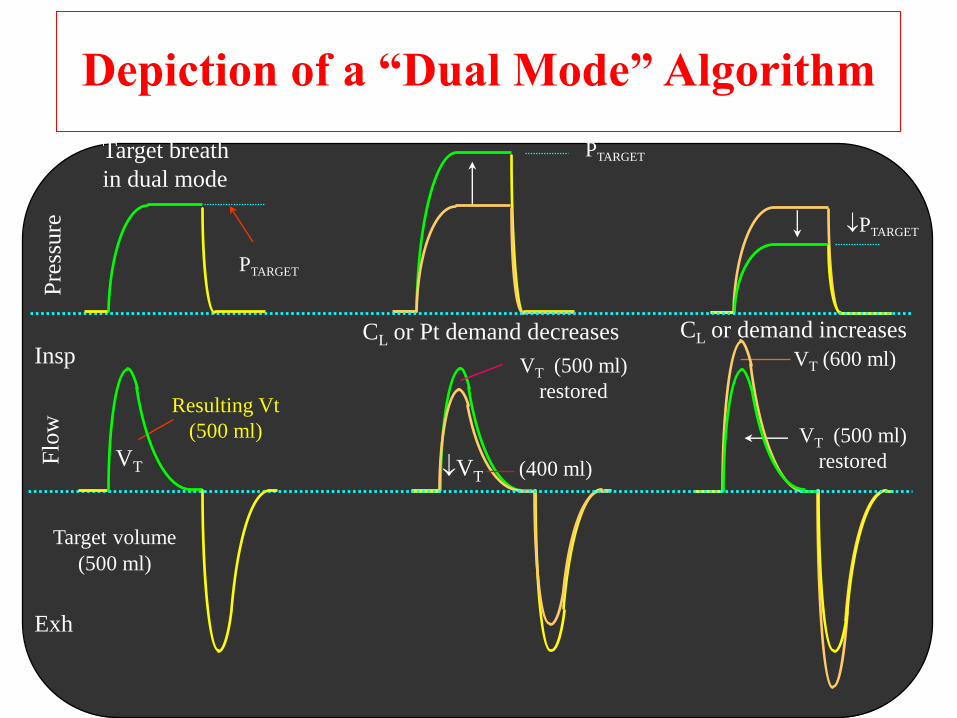
Depiction of a “Dual Mode” Algorithm
CL or Pt demand decreases CL or demand increases
VT (500 ml)
restored
VT (600 ml)
PTARGET
PTARGET
PTARGET
VT (500 ml)
restored
Resulting Vt
(500 ml)
Flo
w
Pre
ssure
Insp
Exh
VT (400 ml)
Target breath
in dual mode
Target volume
(500 ml)
VT
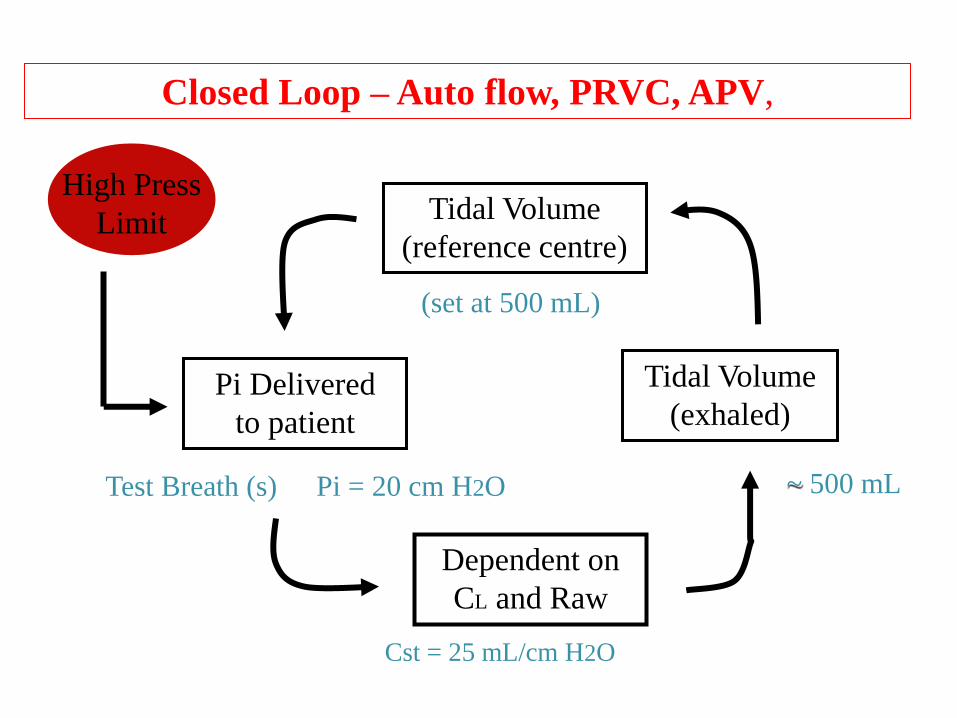
High Press
Limit Tidal Volume
(reference centre)
Tidal Volume
(exhaled)
Dependent on
CL and Raw
Pi Delivered
to patient
Closed Loop – Auto flow, PRVC, APV,
Cst = 25 mL/cm H2O
(set at 500 mL)
Test Breath (s) ~ 500 mL Pi = 20 cm H2O
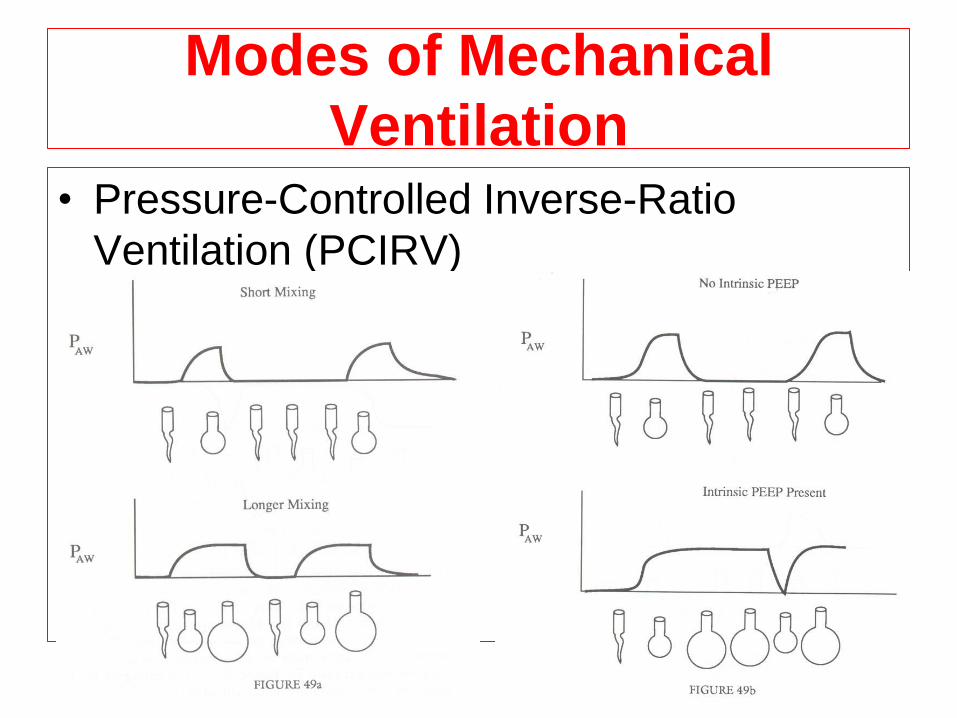
Modes of Mechanical
Ventilation • Pressure-Controlled Inverse-Ratio
Ventilation (PCIRV)
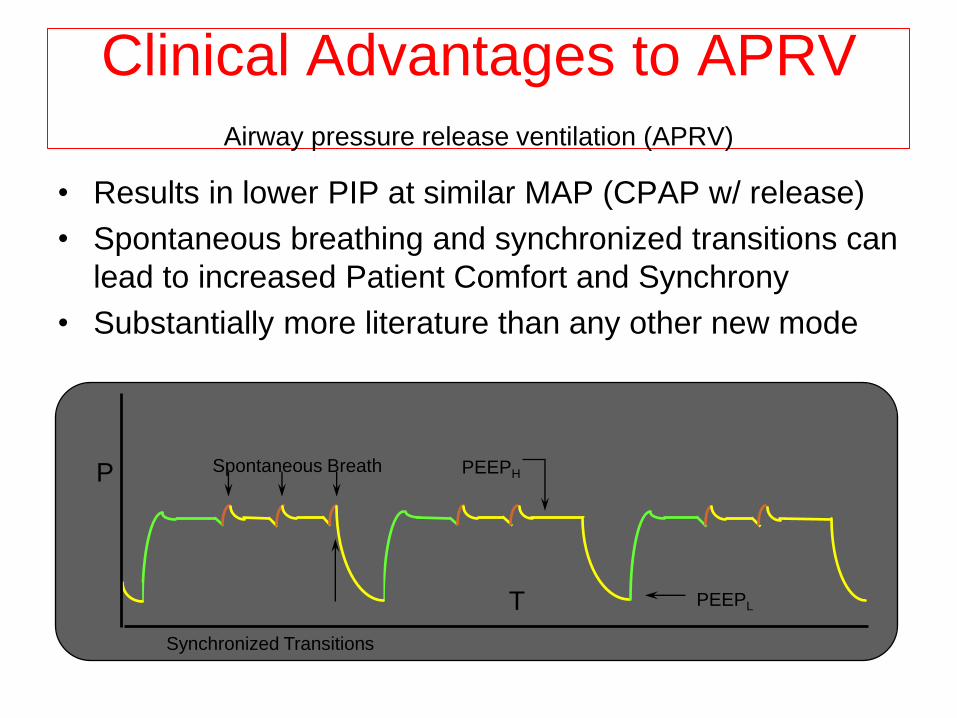
Clinical Advantages to APRV
Airway pressure release ventilation (APRV) • Results in lower PIP at similar MAP (CPAP w/ release)
• Spontaneous breathing and synchronized transitions can
lead to increased Patient Comfort and Synchrony
• Substantially more literature than any other new mode
Synchronized Transitions
Spontaneous Breath P
T
PEEPH
PEEPL
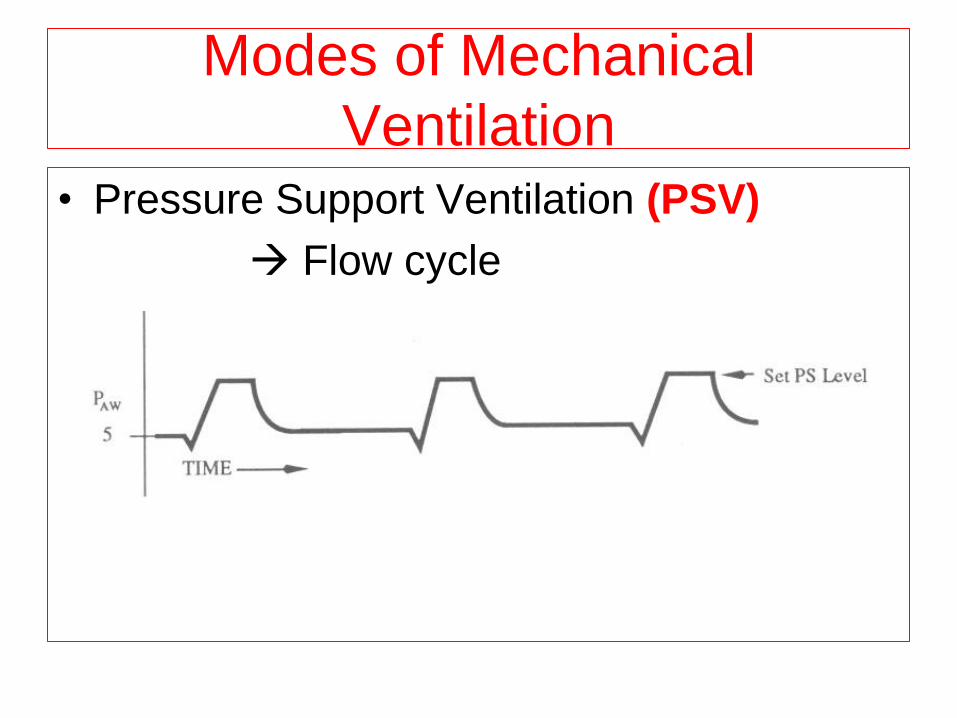
Modes of Mechanical
Ventilation • Pressure Support Ventilation (PSV)
Flow cycle
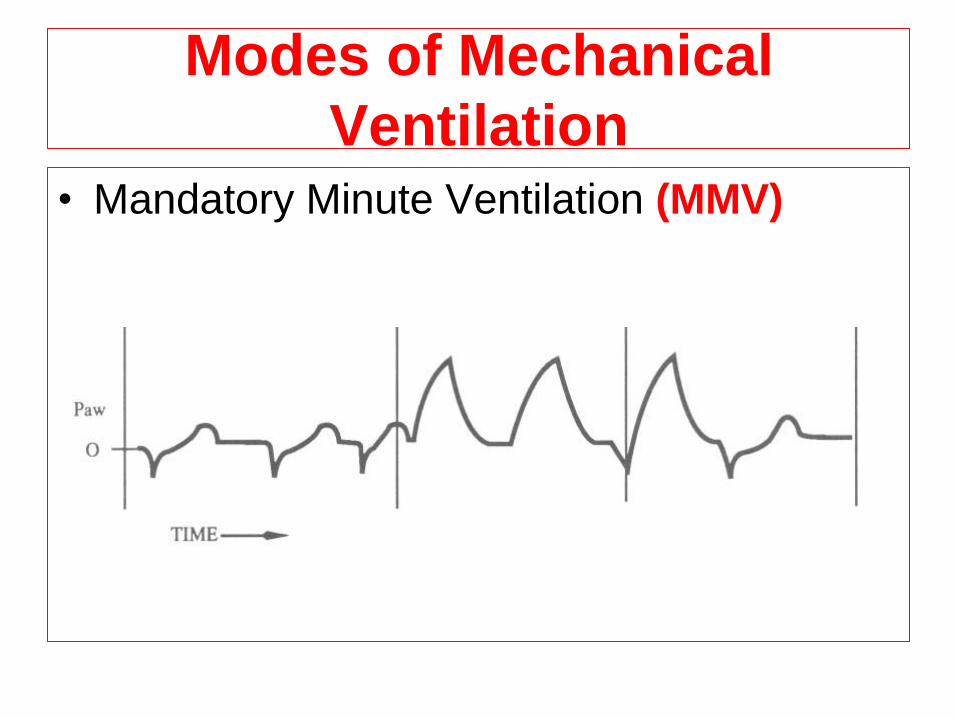
Modes of Mechanical
Ventilation • Mandatory Minute Ventilation (MMV)
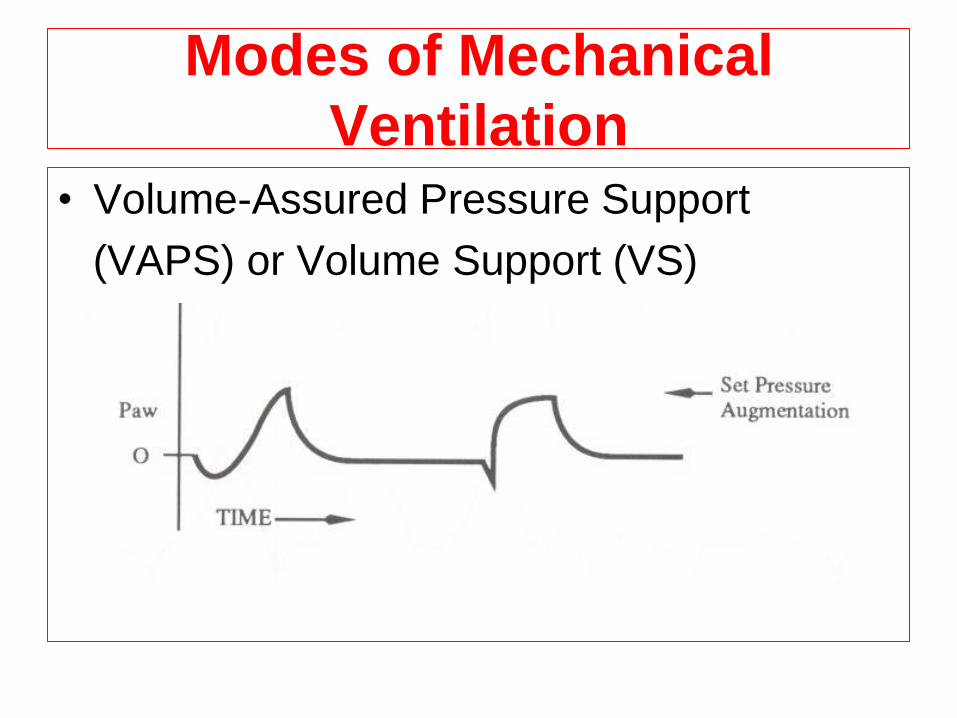
Modes of Mechanical
Ventilation • Volume-Assured Pressure Support
(VAPS) or Volume Support (VS)
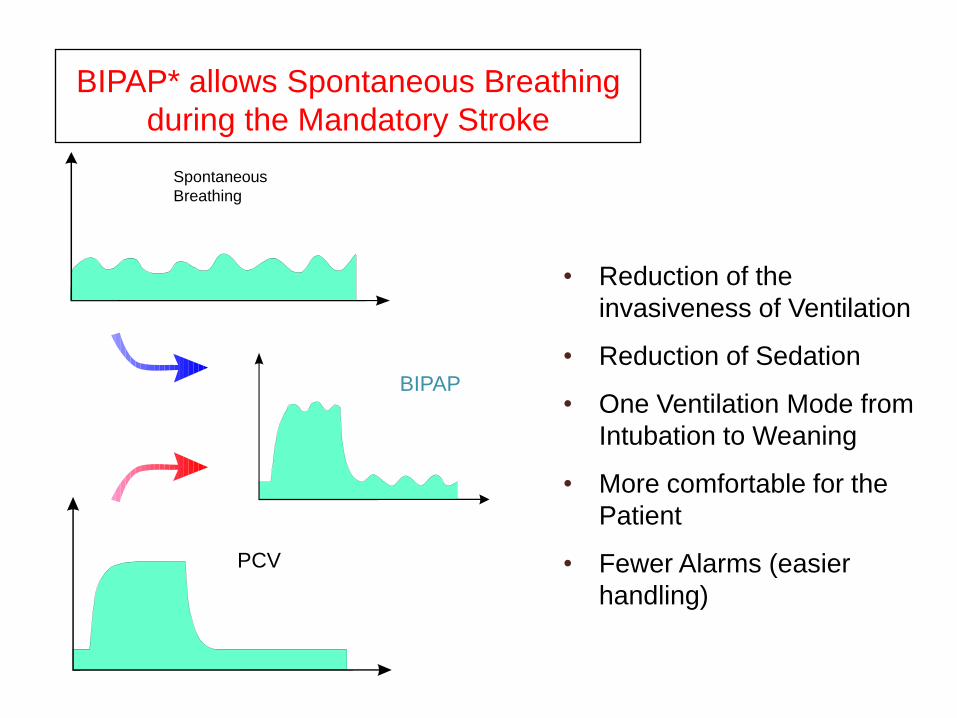
BIPAP* allows Spontaneous Breathing
during the Mandatory Stroke
• Reduction of the
invasiveness of Ventilation
• Reduction of Sedation
• One Ventilation Mode from
Intubation to Weaning
• More comfortable for the
Patient
• Fewer Alarms (easier
handling)
PCV
Spontaneous
Breathing
BIPAP
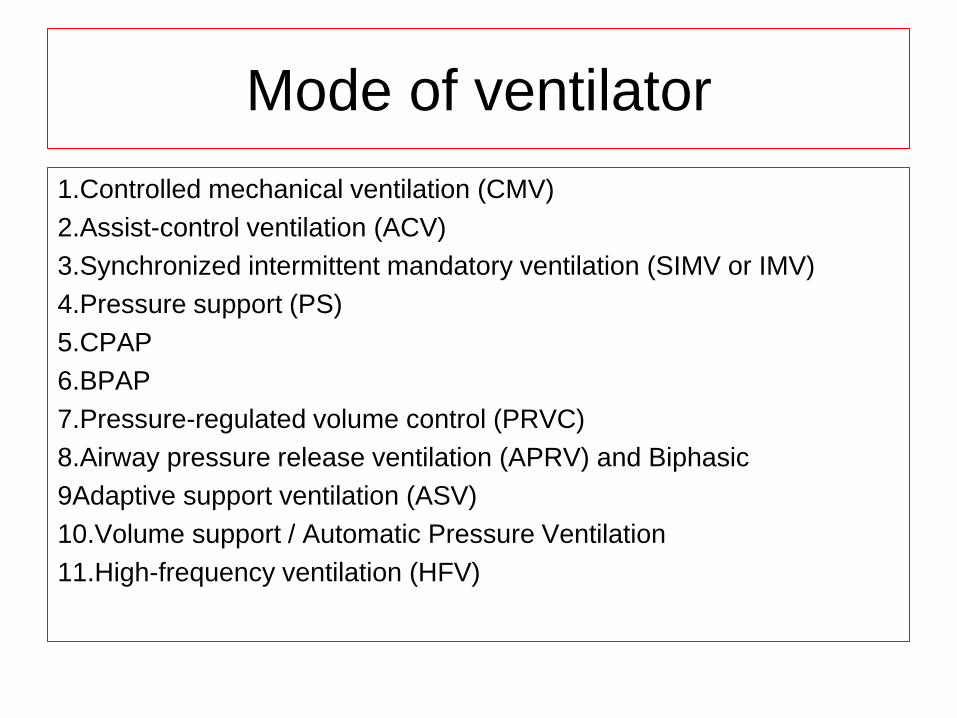
Mode of ventilator
1.Controlled mechanical ventilation (CMV)
2.Assist-control ventilation (ACV)
3.Synchronized intermittent mandatory ventilation (SIMV or IMV)
4.Pressure support (PS)
5.CPAP
6.BPAP
7.Pressure-regulated volume control (PRVC)
8.Airway pressure release ventilation (APRV) and Biphasic
9Adaptive support ventilation (ASV)
10.Volume support / Automatic Pressure Ventilation
11.High-frequency ventilation (HFV)
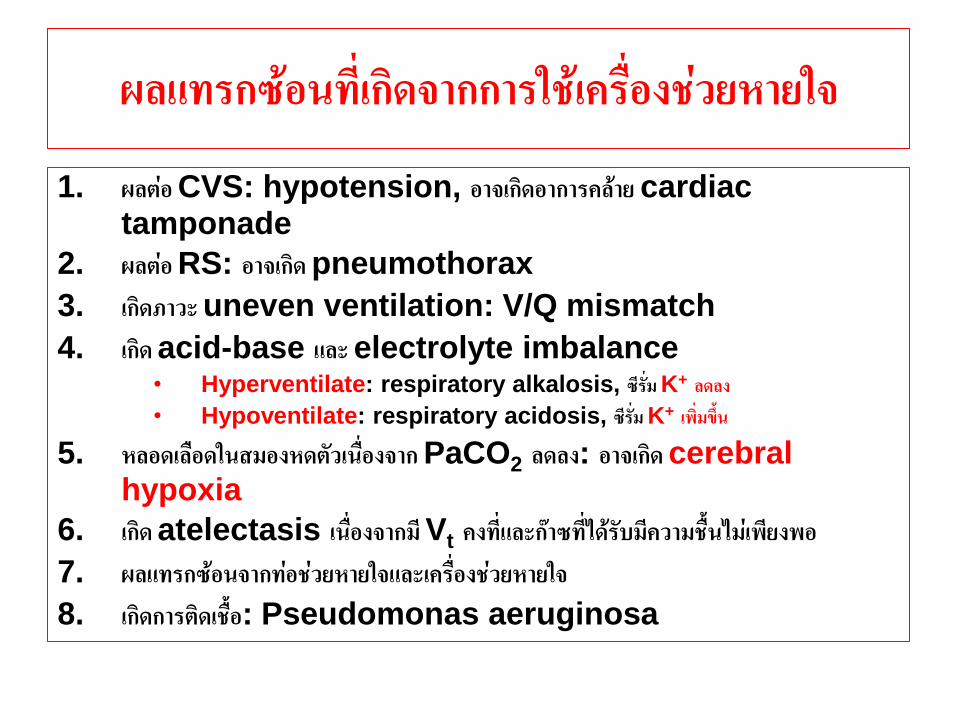
ผลแทรกซอนทเกดจากการใชเครองชวยหายใจ
1. ผลตอ CVS: hypotension, อาจเกดอาการคลาย cardiac tamponade
2. ผลตอ RS: อาจเกด pneumothorax
3. เกดภาวะ uneven ventilation: V/Q mismatch
4. เกด acid-base และ electrolyte imbalance • Hyperventilate: respiratory alkalosis, ซรม K+ ลดลง • Hypoventilate: respiratory acidosis, ซรม K+ เพมขน
5. หลอดเลอดในสมองหดตวเนองจาก PaCO2 ลดลง: อาจเกด cerebral hypoxia
6. เกด atelectasis เนองจากม Vt คงทและกาซทไดรบมความชนไมเพยงพอ 7. ผลแทรกซอนจากทอชวยหายใจและเครองชวยหายใจ 8. เกดการตดเชอ: Pseudomonas aeruginosa
ผลของการใชเครองชวยหายใจตอ Physiology ของรางกาย
1. ท าใหความดนในทางเดนหายใจและชองอกสงขน
2. ผปวยใชแรงในการหายใจลดลง 3. ท าใหหลอดลมขยายตว 4. สามารถเปลยนแปลงคา mechanical ventilatory
pattern ตามทตองการ 5. ปรบคา Vt ได และท าใหการกระจายของ ventilation ดขน
6. Cardiac output จะลดลงเนองจาก venous return ลดลง 7. Intracranial pressure จะสงขน
8. Urine output ลดลง เนองจากมการหลง ADH มากขน
9. ผลตอสภาพจตใจ: หวาดกลว วตกกงวล นอนไมหลบ ซมเศรา PU
การดแลผปวยทใชเครองชวยหายใจ
1. ปองกนการตดเชอ: physical therapy, humidification, secretion drainage & suction with aseptic technique
2. ระวงการตดเชอจากสงแวดลอม: สมผสโดยตรงจากบคคล 3. การจดทาผปวย: postural drainage, ใหอยในทานงบาง 4. ใหมการหายใจลก (sigh) เปนครงคราว: 6-8 ครง/ชวโมง 5. การดดเสมหะ: แตละครงไมเกน 10 วนาท, กอนและหลงตองให O2 เสมอ 6. ปองกน peptic ulcer: antacid, H2 antagonist
7. ปองกน gastric distention & ileus: ใส NG tube
8. ค านงถงเรอง nutrition: high protein, carbohydrate & vitamins
References
• Civetta,Taylor&Kirby’s Manual of Critical care.Andrea gabrielli
A.Joseph layon Mihae yu.
• Fundamental in critical care.รองศาสตราจารยนายแพทยเอกรนทร ภมพเชฐ
• http://wn.com/respiratory_care_and_mechanical_ventilation By
Thepakorn Sathitkarnmanee MD.
• http://wn.com/Mechanical_ventilation_-12_Auto_flow_English

THANK YOU


















