Management of Malaria Dr M Ridwanur Rahman Professor (Medicine), ShSMC, Dhaka Member, Malaria...
44
Management of Malaria Dr M Ridwanur Rahman Professor (Medicine), ShSMC, Dhaka Member, Malaria Research Group, Ctg
-
Upload
ariel-dalton -
Category
Documents
-
view
224 -
download
6
Transcript of Management of Malaria Dr M Ridwanur Rahman Professor (Medicine), ShSMC, Dhaka Member, Malaria...

Management of Malaria
Dr M Ridwanur Rahman
Professor (Medicine), ShSMC, Dhaka
Member, Malaria Research Group, Ctg

THE BURDEN OF MALARIA
>100 countries in the world are malarious >2 billion people are exposed to the risk of
malaria infection annually. Residents of non-endemic areas also have,
Travel malariaAirport malaria
High Risk Groups Young children (6 months - 5 years) -Pregnant women (primigravids) -Non-immune migrants (Military personnel,
expatriates, tourists, refugees).

High Risk Malaria Areas in Bangladesh

Case Load: Malaria in Bangladesh, 1963 – 1998

Clinical Malaria - Treatment
Non falciparum malaria- Uncomplicated
Uncomplicated Malaria (falciparum)
Severe (Complicated) Malaria

Malaria Case Fatality Rates
Severe malaria 10-40%
Moderately severe malaria 3%
Uncomplicated malaria <1%

Relationship between life cycle & clinical features
Cycle/feature Vivax/ovale Malariae Falciparum
Incubation 8-25 days 15-30 days 8-25 days
Asexual cycle 48 hrs, synchronus
72 hrs, synchronus
<48 hrs, asynchronus
Periodicity of fever
Tertian Quartan Aperiodic
Exo-erythrocytic
Persist as hypnozoites
None None
Delayed onset common rare Rare
Relapses Common upto 2 years
Recrudescence many years
Recrudescence upto 1 year

Clinical Features Fever- classically intermittent & periodic 3 stages described Asymptomatic apyrexial intervals Malaise, Headache, bodyache & vomiting Cough & mild diarrhoea- children Jaundice relatively common- falciparum No specific physical sign Liver & spleen- enlarge & tender Anaemia frequent in falciparum

D/D in uncomplicated disease
Flue like illness’ Enteric feversRTI’s UTI Dengue SSTI Others

Diagnosis
High index of suspicion- H/O chance of contact, absence of symptom/signs of other disease, characteristic C/F
Blood slide examination Dipstick Tests Other tests- to exclude other D/D,
e.g., urine R/M/E, CBC, CXR etc.

Classification of antimalarial drugs based on chemical structures
4-aminoquinolines e.g. chloroquine, hydroxychloroquine, amodiaquine
8-aminoquinolnes e.g. primaquine 2,4-diaminopyrimidine e.g. pyrimethamine Arylaminoalcohols e.g. quinine, mefloquine, lumefantrine Acridine derivatives e.g. quinacrine, mepacrine, pyronaridine Biguanides e.g. chloroguanide, chloroproguanil Suphonamides and sulphones e.g. sulphadoxine and dapsone
respectively Phenanthrene methanols e.g. halofanthrine Naphthoquinones e.g. atovaquone Artemisinins e.g. dihydroartemisinin, artesunate, artemether,
arteether, e.t.c.

FACTORS THAT GOVERN CHOICE OF DRUGS
Parasite species
Local Level of resistance to drugs
Patient’s general health and medical
history. Availability of medication in the country
of prescription.
Intended use (prophylactic or
therapeutic).

Drug resistant Malaria
Resistance is the ability of an organism to survive or multiply despite presence of the drug – exhibited by falciparum only
CQ, S/P resistance in Bangladesh May have reduced sensitivity to Q & M Bangladesh is a multi-drug resistant
falciparum area

Factors aiding Resistance in
malaria parasites. Indiscriminate drug useSub-optimal dosagesNon compliance with treatment
courseLow quality drugsFake and substandard drugs

WHO Treatment Guidelines
Artemisinin-based Combination Therapies (ACTs) should be first line treatment for falciparum malaria everywhere.
This should ideally be formulated in fixed dose combinations when possible.
Therapeutic options for ACT -Artesunate-SP -Artemether-lumefantrine -Artesunate-amodiaquine -Artesunate-mefloquine -Dihydroartemisinin-piperaquine

What are Artemisinins ?
Artemisinin derivatives
Methyl Ether
Hemisuccinate
Ethyl Ether
Arteether Artemether
Artesunate
Dihydroartemisin
Qinghaosu ("ching-how-soo")

40
60
80
100
Year
Cured (%)
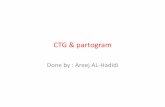
Mefloquine15
Mefloquine25
Mefloquine +
artesunate
Treatment efficacy at Thai-Burmese border
First demonstration project in Thailand

Widespread use of 1st line Rx withArtemisinin-basedCombination Therapy
Improve clinical cure ratesDelay emergence of resistanceReduce transmission
Cost effective
Artemisinin-based combination therapy in uncomplicated malaria

Treatment of Uncomplicated MalariaNon-Falciparum-
- Chloroquine 25 mg/kg over 3 days, (Tab 4-4-2, adults)
- & primaquine 15 mg/d, 14 days Falciparum- ACT
Co-artem - 6 doses
2nd line- Alternative ACT, Q7T7 or Q7D7

What to give in pregnancy ?
In 1st trimester Quinine + Clindamycin 7 days
In 2nd and 3rd trimesters Any ACT combination as per rec. or Artesunate + Clindamycin 7 days or Quinine + Clindamycin 7 days
Lactating women same ACT

CLASSIFICATION OF THERAPEUTIC RESPONSE (WHO 2004)
3 Categories Early treatment failure (ETF)
Late treatment failure (LTF) Late clinical failure Late parasitological failure
Adequate clinical and parasitological response (ACPR)

Severe & Complicated Malaria (SCM)
Falciparum malaria Children, pregnant & short term
travel/resident – endemic zones Severe symptoms Life threatening in the absence
of early effective treatment Medical emergency

Table-1 Types of Severe Manifestations (n=829)
Type SCM (Major) Full Recovery
DeathN (%, CFR)
Others 2 TotalN (%)
CNS Manifestations 304 39 (31) 19 362 (44)
Unrousable Coma 86 36 (27) 10 132 (16)
Impaired Consciousness 185 2 (1) 8 195 (24)
Convulsion 33 1 (3) 1 35 (4)
Severe Prostation 193 0 4 197 (24)
Hyper-parasitaemia 172 0 6 178 (22)
Severe Anamia 51 0 16 67 (8)
Hyperpyrexia 14 1 (7) 0 15 (2)
Others 7 0 3 10
Total n (row%) 741 (89) 40 (4.8) 48 (6) 829

SCM – Other Manifestations
Acute renal failure Pulmonary Oedema Haemoglobinuria Hypoglycaemia DIC Jaundice Multi-organ involvement/failure
May occur singly, often in combination

Management (SCM)
• Medical Emergency • Appropriate anti-parasitic
Treatment • Crucial General Management • Identification & management
of complications

Treatment of severe falciparum malaria
Any of the following antimalarial medicines are recommended
–Artesunate i.v. or i.m –artemether i.m. –quinine (i.v. infusion or i.m. injection).
Full course of ACT or quinine + clindamycin or doxycycline when patient can tolerate oral treatment

Artemisinins parenteral
αβ Arteether – 150 mg (2ml) i.m od x 3 days or 3 mg/kg od i.m. x 3 days
Artesunate 2.4 mg/kg i.v. or i.m. given on admission (time = 0), then at 12 h and 24 h, then once a day
Artemether 3.2 mg/kg i.m. given on admission then 1.6 mg/kg per day is an acceptable alternative to quinine i.v infusions
Rectal artemisinins are not as effective

Quinine parenteral
A loading dose of quinine of 20 mg salt/kg bw. 10 mg/kg 8th hrly i.v infusion
Rate-controlled i.v. infusion is the preferred route of quinine admin.
If this cannot be given safely, then i.m. injection is a satisfactory alternative.
Rectal admin. is not effective Quinidine can substitute quinine

Quinine vs Artemesinin’s
• Artemesinins are more effective than Quinine in terms of survival (MRG, contributed)
• No significant difference in coma resolution time & fever clearance time
• Parasite clearance time faster with A’s • Hypoglycaemia & cardiotoxicity less A’s • ? Uterine contractions more with Q’s • ? Neurologic sequelae more with A’s
(animals)

Cerebral Malaria – D/D
Meningitis Encephalitis Sepsis Fever in CNS Disease Fever in Organ failure Typhoid encephalopathy Metabolic/Toxic encephalopathy

Severe Anaemia
• More in children & pregnant population
• Transfuse if Hb <6.0 g/dl • Fresh whole blood or packed cells • Include the transfusion volume in
I/O calculation • Use frusemide if volume over load

Acute Renal Failure• Continuous Catheter • Correct dehydration • Use bolus frusemide 20-40 mg IV • Monitor hourly urine output, if <17 ml/hr
established ARF • Control fluid input if established ARF • Referral to renal replacement facility • Pt. Unlikely to die if dialysis facility
available

Hypoglycaemia
• Frequent in young children, pregnant women & during quinine Rx
• Intervened on suspicion- most important being deterioration of consciousness & convulsion
• Bolus 25% glucose 50 cc • Follow with IV infusion of 5%/10%
glucose • Continue monitoring for recurrence

Metabolic Acidosis
• Look for dehydration & hypovolaemia • Isotonic IV infusion, avoid fluid overload • Monitor BP, urine volume & JVP • Improve oxygenation by
- clearing airway
- oxygen inhalation
- support ventilation, if necessary

Pulmonary Oedema• Very serious, mortality >50% • Frequent in ARF, pregnancy, severe
anaemia, & at extremes of ages • Prop up position & oxygen inhalation • Stop IV fluid & give IV frusemide (40-200
mg) • Sequential torniquette application• Haemofiltration • Mechanical ventilation • Withdraw blood by venesection

Circulatory Collapse
• Often associated with gm –ve septicaemia • Common sites- lung, urinary tract,
meningitis, IV lines & injection sites • Take blood culture, start broad-spectrum
antibiotics (Amoxy + Genta) • Maintain adequate hydration & output • Dopamine may be given

Spontaneous bleeding & DIC
• Spontaneous bleeding from DIC is uncommon but serious complication
• Thrombocytopenia is common but rarely causes bleeding
• Transfuse fresh blood, clotting factors or platelets as required
• If PT or PTT prolonged, Inj. Vit. K 10 mg may be given

Haemoglobinuria• G6PD deficiency or malaria itself- not
quinine• Continue appropriate antimalarial if
parasitaemia present • Transfuse fresh whole blood to Hct >20% • Monitor JVP/CVP to avoid fluid overload
& hypovolaemia • Give frusemide 20 mg IV • Monitor renal function & consider dialysis
if required

Nursing Care• As important as anti-parasitic Rx • Meticulous nursing care to
- maintain clear airway
- prevent aspiration pneumonia
- prevent pressure sores • Careful intake-output chart • Rate of infusion checked frequently • Temperature >1020F reduced by tepid sponging &
fanning • Change in level of consciousness, behaviour &
occurrence of convulsion reported

SCM Management – Common errors Misjudgement of severity Delay in starting treatment Failure to provide nursing care Inappropriate rate of infusion Delay in correcting hypoglycaemia Failure to control convulsions Unnecessary continuation of treatment Failure to evaluate con-comitant
conditions

Prevention of Malaria death
Pre-hospital treatment
- IM Quinine
- Artesunate Suppository (MRG received BMJ group award for Best Research Paper of the Year 2010)
Chemoprophylaxis / IPT
Malaria Vaccine

DRUGS FOR CHEMOPROPHYLAXIS
Pyrimethamine – Limited efficacy Proguanil – 200mg daily- Limited efficacy
Doxycycline – Travelers 200mg daily. Not in children or pregnant women
Malarone (Atovaquone/proguanil) – very effective, good safety margin but expensive ($32 – 35
USD/dose)
Mefloquine – 250mg weekly (T1/2 too long, neuro-psychiatric AE)
Chloroquine/Amodiaquine Not recommended as it is used in Rx Resistance emerged Bone marrow suppression with amodiaquine

Conclusion
Malaria has no characteristic clinical feature
High index of suspicion is the key Early diagnosis & Prompt &
appropriate treatment (EDPT) – 1st contact
Death is avoidable with early effective treatment & meticulous followup