Low grade glioma
34
Low grade glioma Low grade glioma • Radiotherapy in low grade gliomas benefit with local control advantage • Patients with high risk factors need immediate radiation after surgery • RT dose of 50-54 Gy in 2 Gy/Fr • Fractionated radiosurgery in optic nerve glioma and small volume disease • RT causes cognitive function impairment, so low risk group may receive observation • Young pts, with seizures, near total excision and oligo component may be observed [email protected]
-
Upload
duttaradio -
Category
Health & Medicine
-
view
59 -
download
2
Transcript of Low grade glioma

Low grade gliomaLow grade glioma
• Radiotherapy in low grade gliomas benefit with local control advantage
• Patients with high risk factors need immediate radiation after surgery
• RT dose of 50-54 Gy in 2 Gy/Fr
• Fractionated radiosurgery in optic nerve glioma and small volume disease
• RT causes cognitive function impairment, so low risk group may receive observation
• Young pts, with seizures, near total excision and oligo component may be observed
• Patient on follow up after surgery need stringent follow up
• Patients with irregular follow up should also be treated with early RT

Low grade gliomasLow grade gliomas
A group of brain tumours: A group of brain tumours: •Astrocytoma Gr IIAstrocytoma Gr II•Oligodendroglioma Gr IIOligodendroglioma Gr II•Mixed oligoastrocytoma Gr IIMixed oligoastrocytoma Gr II
•DNET, PXA, pilocytic, SGCADNET, PXA, pilocytic, SGCA
Typically slow-growing and better prognosis than high-grade gliomasTypically slow-growing and better prognosis than high-grade gliomas

Diffuse fibrillary astrocytomas Gr IIDiffuse fibrillary astrocytomas Gr II
Adult low grade gliomasAdult low grade gliomas• Diffusely infiltrativeDiffusely infiltrative• Typically non-enhancingTypically non-enhancing
• Slow and insidious course; majority with seizuresSlow and insidious course; majority with seizures• Prognostication very difficult; some remain indolent and some recur Prognostication very difficult; some remain indolent and some recur
within short timewithin short time
• Surgery is the treatment of choiceSurgery is the treatment of choice• Surgery rarely ever totalSurgery rarely ever total
• Eventually majority (60-80%) transform into high-gradeEventually majority (60-80%) transform into high-grade
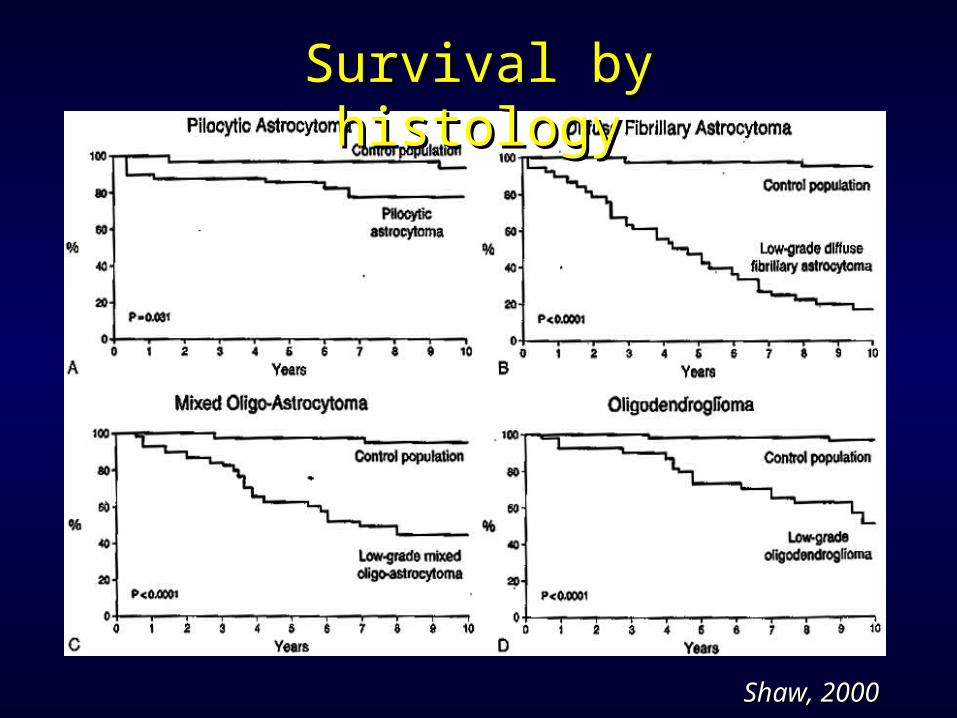
Survival by histologySurvival by histology
Shaw, 2000Shaw, 2000
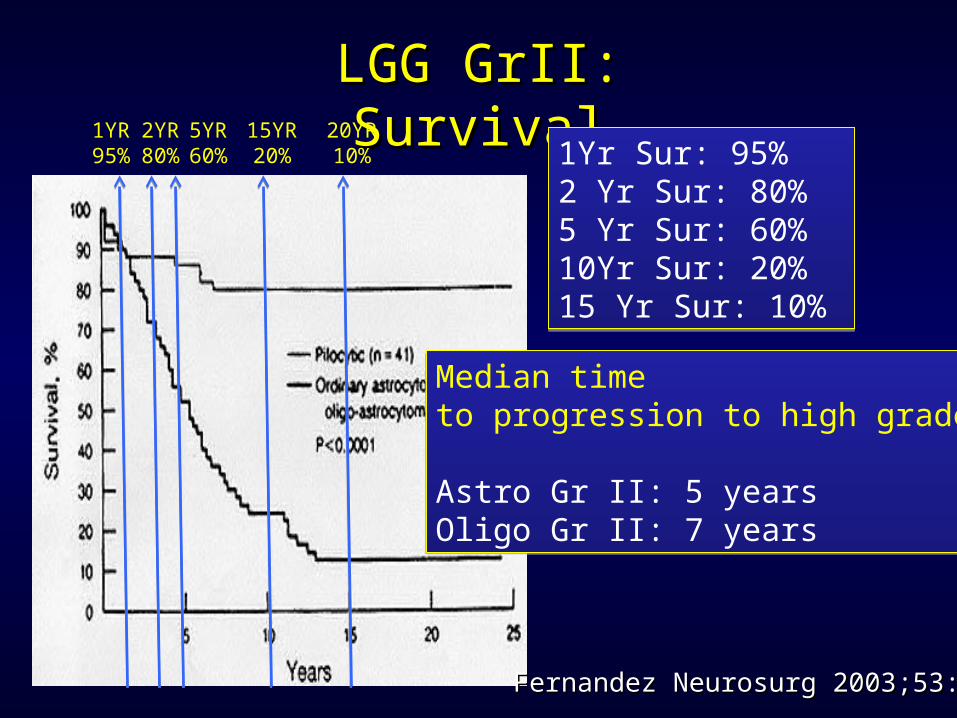
LGG GrII: SurvivalLGG GrII: Survival
1Yr Sur: 95%2 Yr Sur: 80% 5 Yr Sur: 60%10Yr Sur: 20%15 Yr Sur: 10%
1Yr Sur: 95%2 Yr Sur: 80% 5 Yr Sur: 60%10Yr Sur: 20%15 Yr Sur: 10%
Median time to progression to high grade:
Astro Gr II: 5 yearsOligo Gr II: 7 years
Median time to progression to high grade:
Astro Gr II: 5 yearsOligo Gr II: 7 years
2YR80%
1YR95%
5YR60%
15YR20%
20YR10%
Fernandez Neurosurg 2003;53:544Fernandez Neurosurg 2003;53:544

LGG Gr-II: Adjuvant therapyLGG Gr-II: Adjuvant therapy
• Majority of the LGG pts eventually receive RT when Majority of the LGG pts eventually receive RT when progressed to high gradeprogressed to high grade
• There is no debate on There is no debate on NO RT versus RTNO RT versus RT
• But, on RT But, on RT earlyearly after surgery or RT after surgery or RT at progression (late)at progression (late)
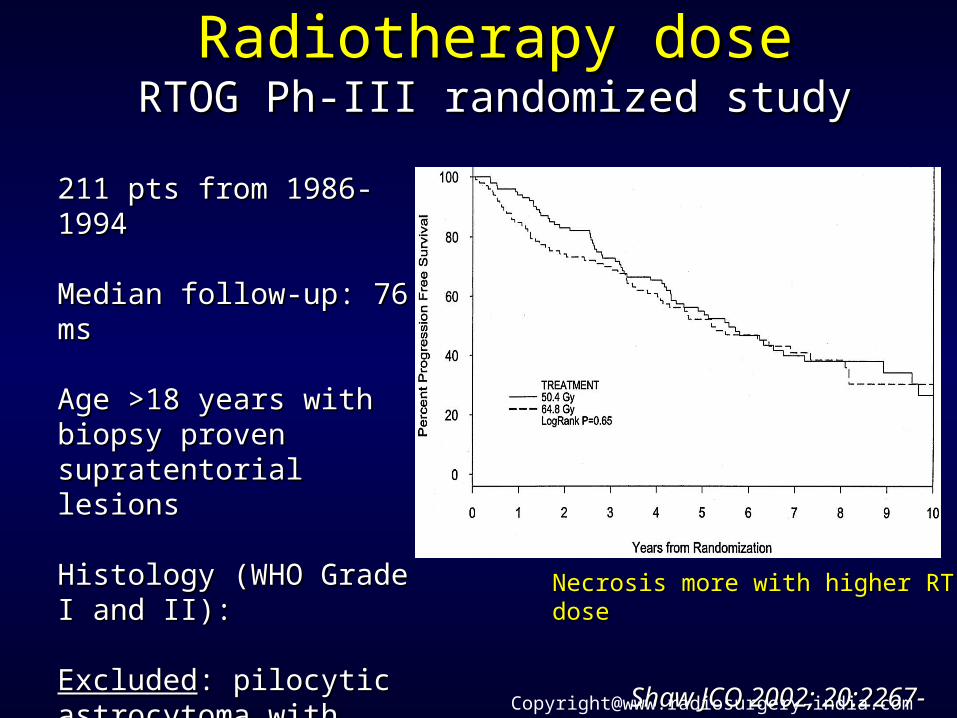
Radiotherapy doseRadiotherapy doseRTOG Ph-III randomized studyRTOG Ph-III randomized study
Necrosis more with higher RT doseNecrosis more with higher RT dose
Shaw JCO 2002; 20:2267-2276Shaw JCO 2002; 20:2267-2276
211 pts from 1986-1994211 pts from 1986-1994
Median follow-up: 76 msMedian follow-up: 76 ms
Age >18 years with biopsy Age >18 years with biopsy proven supratentorial lesionsproven supratentorial lesions
Histology (WHO Grade I and II):Histology (WHO Grade I and II):
ExcludedExcluded: pilocytic astrocytoma : pilocytic astrocytoma with gross total resection with gross total resection
RT- 50 Gy vs 64.8 GyRT- 50 Gy vs 64.8 Gy

EORTC 22844: Ph-III randomized studyEORTC 22844: Ph-III randomized study
QOL worse with higher RT doseQOL worse with higher RT dose
Karim IJROBP 1996; 36: 549-56Karim IJROBP 1996; 36: 549-56
379 pts from 1985-1991379 pts from 1985-1991
Median follow-up: 74 msMedian follow-up: 74 ms
Age 16-65 years with biopsy proven Age 16-65 years with biopsy proven supratentorial lesionssupratentorial lesions
Histology (WHO Grade I and II):Histology (WHO Grade I and II):
ExcludedExcluded: pilocytic astrocytoma with : pilocytic astrocytoma with gross total resection gross total resection
RT- 45 Gy vs 59.4 GyRT- 45 Gy vs 59.4 Gy
RT Dose: 45Gy Vs 59.4 Gy RT Dose: 45Gy Vs 59.4 Gy
Dose of RT in LGG: 45Gy/25#[email protected]
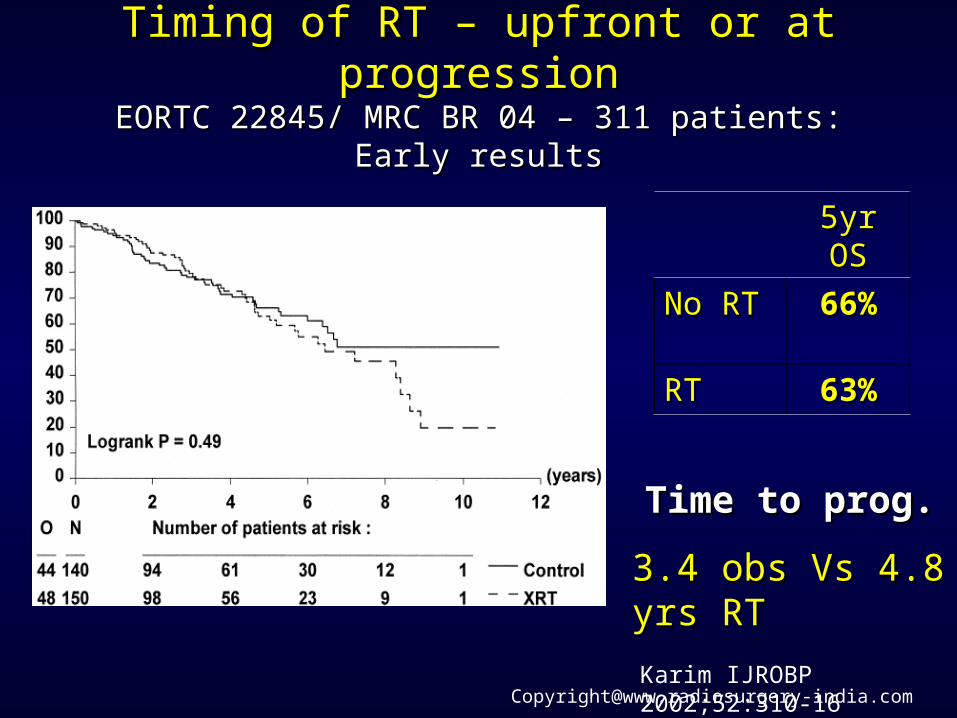
Timing of RT – upfront or at progressionTiming of RT – upfront or at progressionEORTC 22845/ MRC BR 04 – 311 patients: Early resultsEORTC 22845/ MRC BR 04 – 311 patients: Early results
5yr OS5yr OS
No RTNo RT 66%66%
RTRT 63%63%
Karim IJROBP 2002;52:310-16
Time to prog.Time to prog.
3.4 obs Vs 4.8 yrs RT3.4 obs Vs 4.8 yrs RT

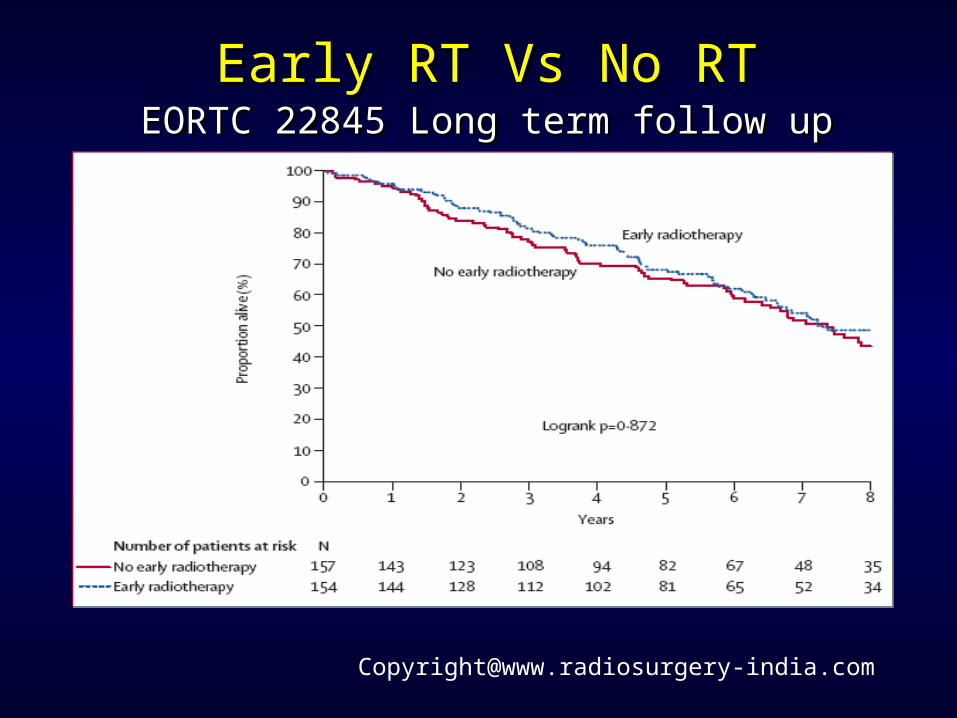
Early RT Vs No RTEarly RT Vs No RTEORTC 22845 Long term follow up (7.8 yrs)EORTC 22845 Long term follow up (7.8 yrs)
Van den Bent Lancet [email protected]
Early RT Vs No RTEarly RT Vs No RTEORTC 22845 Long term follow upEORTC 22845 Long term follow up

Early RT Vs No RTEarly RT Vs No RTEORTC 22845 Long term follow upEORTC 22845 Long term follow up
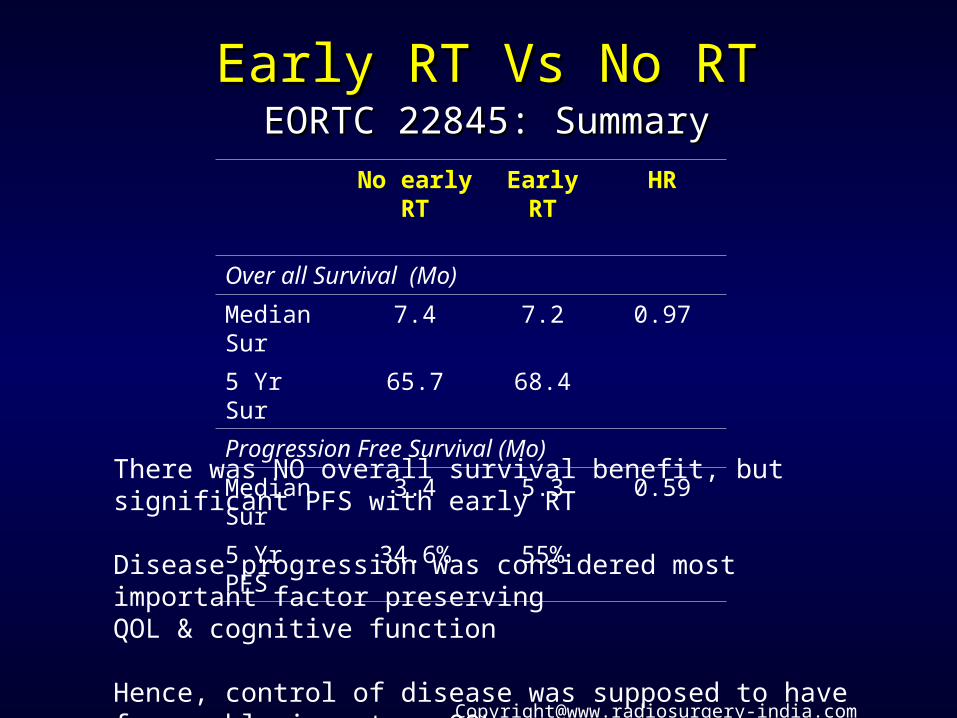
Early RT Vs No RTEarly RT Vs No RTEORTC 22845: SummaryEORTC 22845: Summary
No early RT Early RT HR
Over all Survival (Mo)
Median Sur 7.4 7.2 0.97
5 Yr Sur 65.7 68.4
Progression Free Survival (Mo)
Median Sur 3.4 5.3 0.59
5 Yr PFS 34.6% 55%
There was NO overall survival benefit, but significant PFS with early RT
Disease progression was considered most important factor preserving QOL & cognitive function
Hence, control of disease was supposed to have favourable impact on QOLHowever, in the present study there was no QOL parameter evaluation
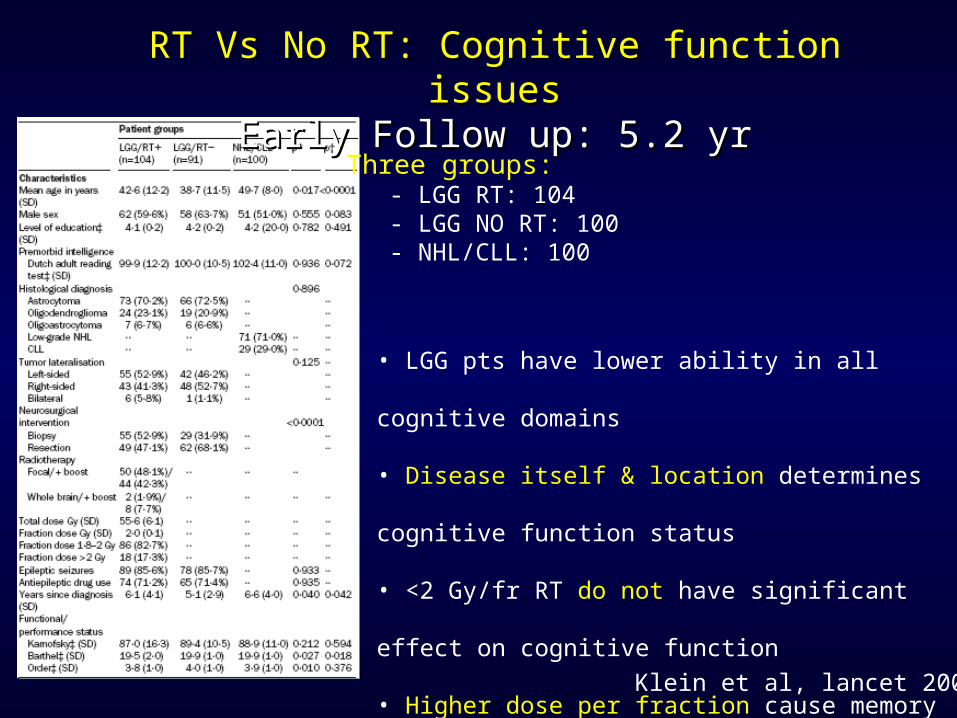
RT Vs No RT: Cognitive function issuesRT Vs No RT: Cognitive function issuesEarly Follow up: 5.2 yrEarly Follow up: 5.2 yr
Klein et al, lancet 2002
Three groups: - LGG RT: 104 - LGG NO RT: 100 - NHL/CLL: 100
• LGG pts have lower ability in all cognitive domains
• Disease itself & location determines cognitive function status
• <2 Gy/fr RT do not have significant effect on cognitive function
• Higher dose per fraction cause memory domain impairment
• Anti-epileptics cause attention & executive function deficit.
Linda Dauw et al, NEJM 2008Linda Dauw et al, NEJM 2008
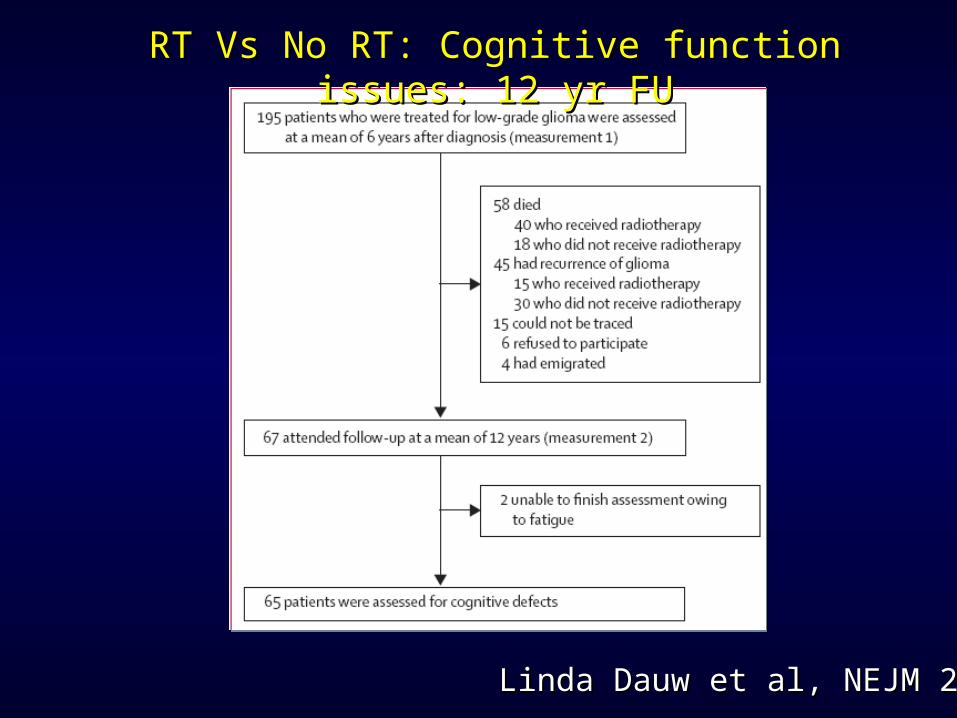
RT Vs No RT: Cognitive function issues: 12 yr FURT Vs No RT: Cognitive function issues: 12 yr FU

Lenda Dauw et al, NEJM 2008Lenda Dauw et al, NEJM 2008
RT Vs No RT: Cognitive function issues- 12 yr FURT Vs No RT: Cognitive function issues- 12 yr FU
Long term FU: There is impairment of cognitive function domain after RTEven low dose RT cause cognitive function impairment
RT in LGGRT in LGGThere is no overall Survival (OS) benefitSignificant progression free survival (PFS) benefit
But, with RT at long term there is cognitive function impairment
? Do higher transformation to high grade after RT? Hypofractionation (>2Gy/fr)? Any scope of selecting subgroup that need early RT (prognostication)

Progression to high grade after RTProgression to high grade after RT
There is a notion that after RT, there is progression to High grade
EORTC 22845 randomized study evaluated the issue
At 12 yr follow up:
Progression to high grade: In RT arm: 50% In No RT arm: 51%
No different is progression to high grade with & without RT
There is no impact of RT on progression to high gradeVan den Bent Lancet 2005

High dose per fraction (>2 Gy/Fr)High dose per fraction (>2 Gy/Fr)
EORTC 22844 & 22845 randomized study evaluated the issue
At 6 yr follow up: 1.8-2 Gy/fr RT: No impact on cognitive function >2 Gy/fr: Higher decline in memory domain
At 12 yr follow up:Cognitive function decline in both 1.8-2 Gy/fr & >2Gy/fr RTHowever, impact of High dose per fraction on cognitive function reduced
Number of pt on >2Gy/Fr is low (3%)There is no evidence of higher decline of IQ with high dose on long term FU,But >2Gy/fr in LGG should be avoided
Van den Bent Lancet 2005

RT in LGGRT in LGGThere is no overall Survival (OS) benefitSignificant progression free survival (PFS) benefit
But, with RT at long term there is cognitive function impairment
? Do higher transformation to high grade after RT? Hypofractionation (>2Gy/fr)? Any scope of selecting subgroup that need early RT (prognostication)

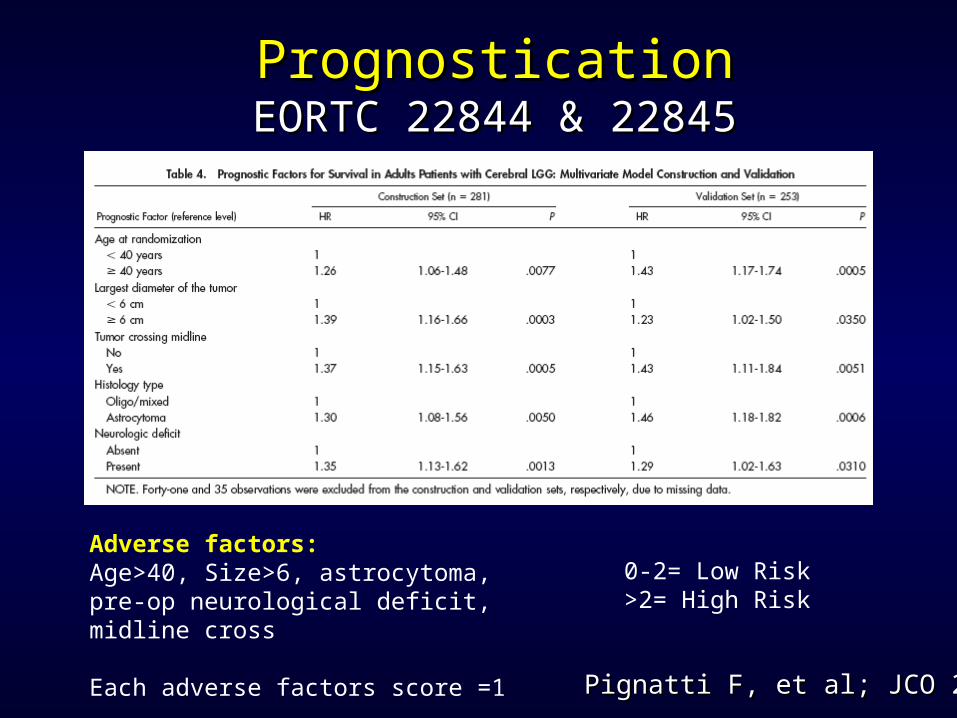
PrognosticationPrognosticationEORTC 22844 & 22845EORTC 22844 & 22845
Pignatti F, et al; JCO 2002Pignatti F, et al; JCO 2002
Analysis of factors of survival function data from largest
ph III randomized study in adult LGG
EORTC 22844 & 22845
Pt= 610
Different patient related factors were evaluated in
multivariate analysis
PrognosticationPrognosticationEORTC 22844 & 22845EORTC 22844 & 22845
Pignatti F, et al; JCO 2002Pignatti F, et al; JCO 2002
Adverse factors: Age>40, Size>6, astrocytoma, pre-op neurological deficit, midline cross
Each adverse factors score =1
0-2= Low Risk>2= High Risk

Key unfavourable variables:Key unfavourable variables:AgeAge ≥ 40 ( p = .0007) ≥ 40 ( p = .0007)HistologyHistology: Astrocytoma ( p = .005): Astrocytoma ( p = .005)Tumour crossing Tumour crossing midlinemidline ( p = .005) ( p = .005)Pre-op neurologic Pre-op neurologic deficitsdeficits ( p = .03) ( p = .03)LargeLargest diameter ≥ 6 cm ( p = .035)st diameter ≥ 6 cm ( p = .035)
Pignatti F, et al; JCO, 20:2076-2084, 2002Pignatti F, et al; JCO, 20:2076-2084, 2002
PrognosticationPrognosticationEORTC 22844 & 22845EORTC 22844 & 22845
Each unfavourable factor score =1
0-2= Low Risk>2= High Risk
MIB Index, site of disease &extent of surgery is not considered
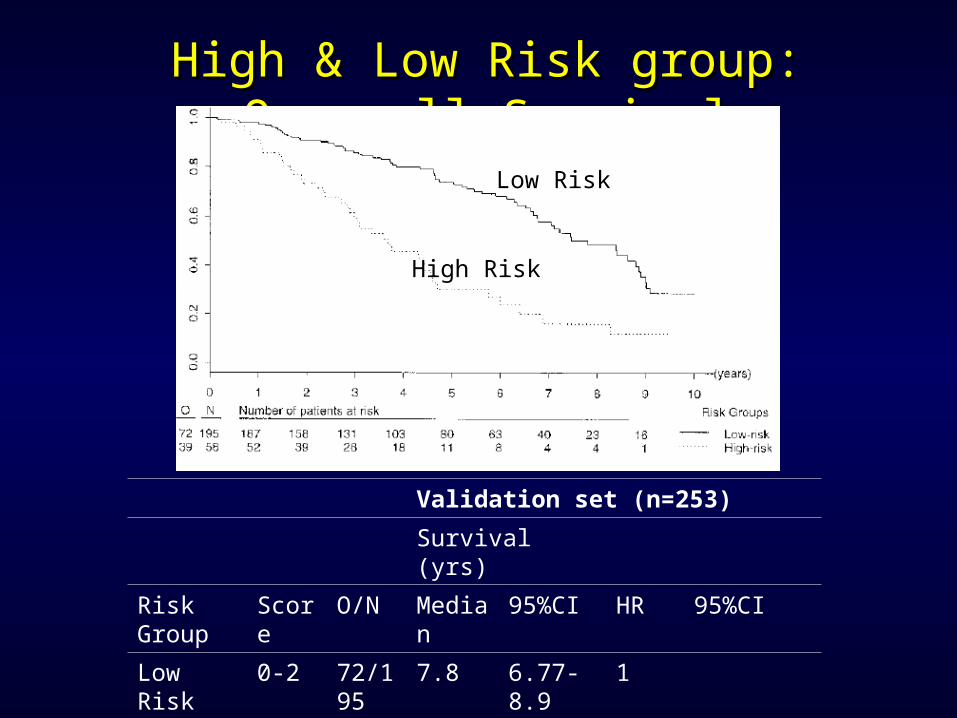
High & Low Risk group: Over all SurvivalHigh & Low Risk group: Over all Survival
Validation set (n=253)
Survival (yrs)
Risk Group Score O/N Median 95%CI HR 95%CI
Low Risk 0-2 72/195 7.8 6.77-8.9 1
High Risk 3-5 39/58 3.67 2.89-4.69 1.83 1.48-2.26
Low Risk
High Risk

RT in LGGRT in LGG
Early RT
1.High Risk group (>2 unfavourable factors)
2.Gross residual disease
3.Critical location of tumour
4.Heterogeneous enhancement on CT/MRI scan
5.Unreliable [email protected]
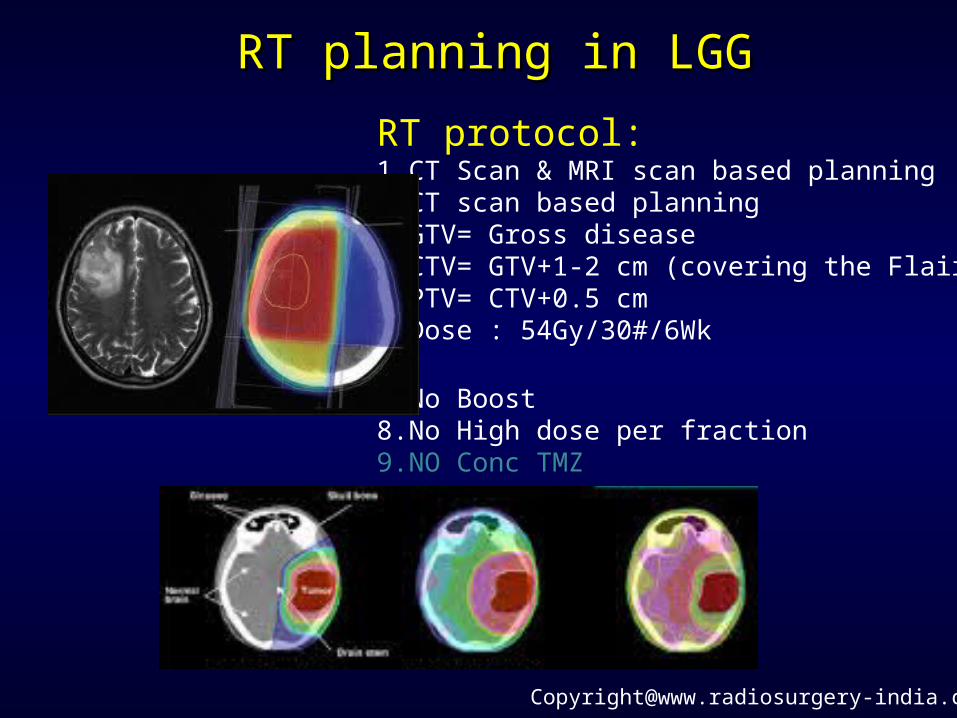
RT planning in LGGRT planning in LGG
RT protocol:1.CT Scan & MRI scan based planning2.CT scan based planning3.GTV= Gross disease4.CTV= GTV+1-2 cm (covering the Flair)5.PTV= CTV+0.5 cm 6.Dose : 54Gy/30#/6Wk
7.No Boost8.No High dose per fraction9.NO Conc TMZ
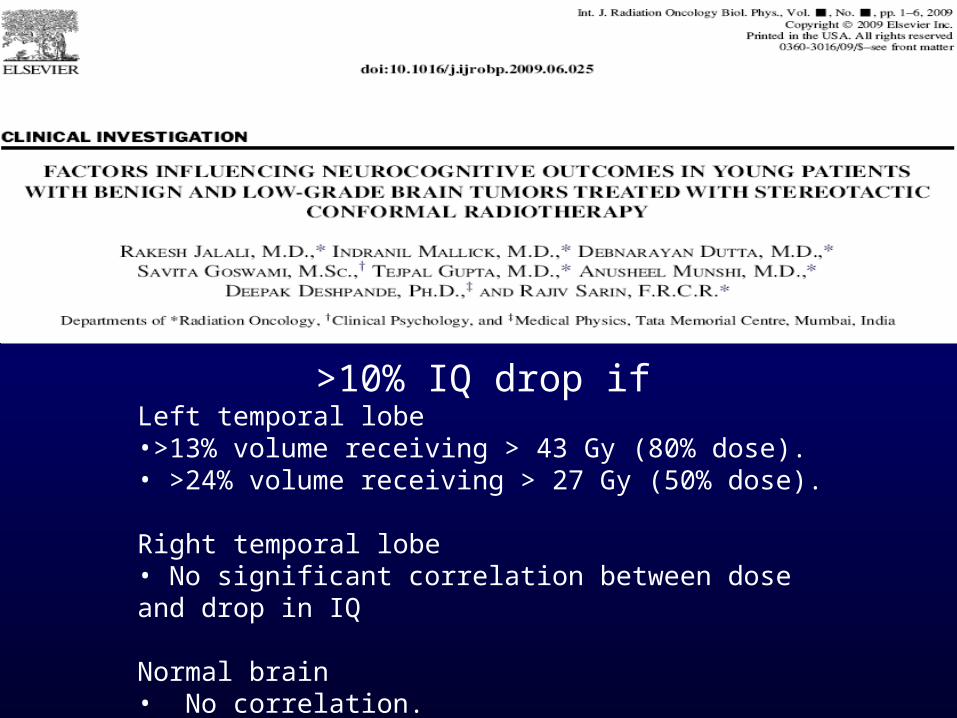
>10% IQ drop ifLeft temporal lobe •>13% volume receiving > 43 Gy (80% dose).• >24% volume receiving > 27 Gy (50% dose).
Right temporal lobe • No significant correlation between dose and drop in IQ
Normal brain • No correlation.
Factors influencing QOL scores
Apart from disease status, treatment modality and follow up,
Other factors also influence interpretation of QOL such as:
- Socio-cultutal status
- Economical status
- Educational status
QOL data should be interpreted with socio-cultural and geographical background
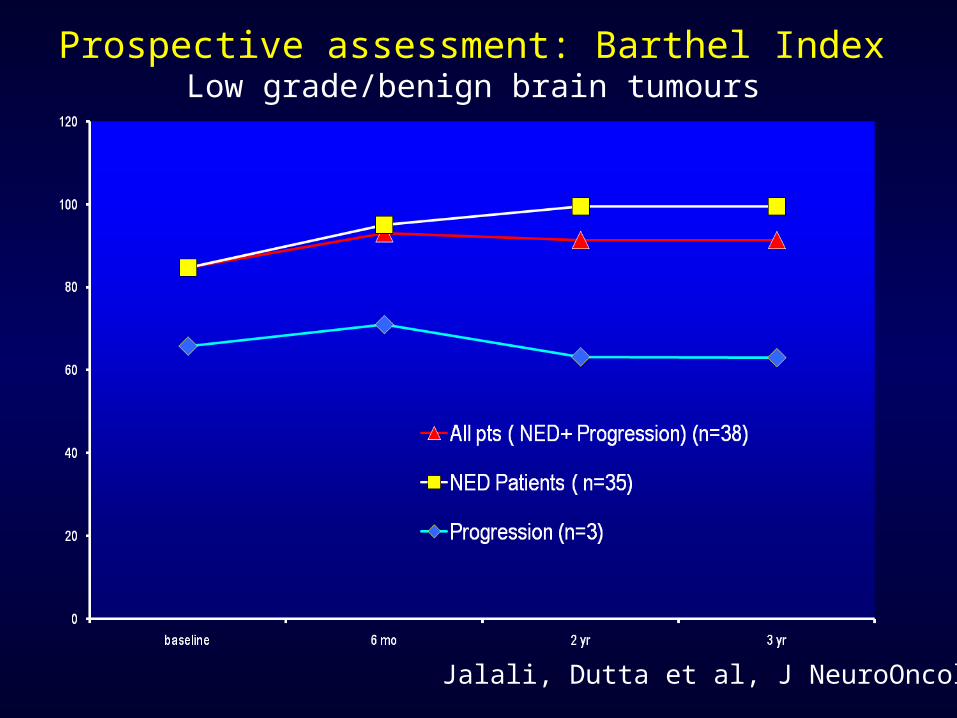
Jalali, Dutta et al, J NeuroOncol 2010
Prospective assessment: Barthel Index Low grade/benign brain tumours
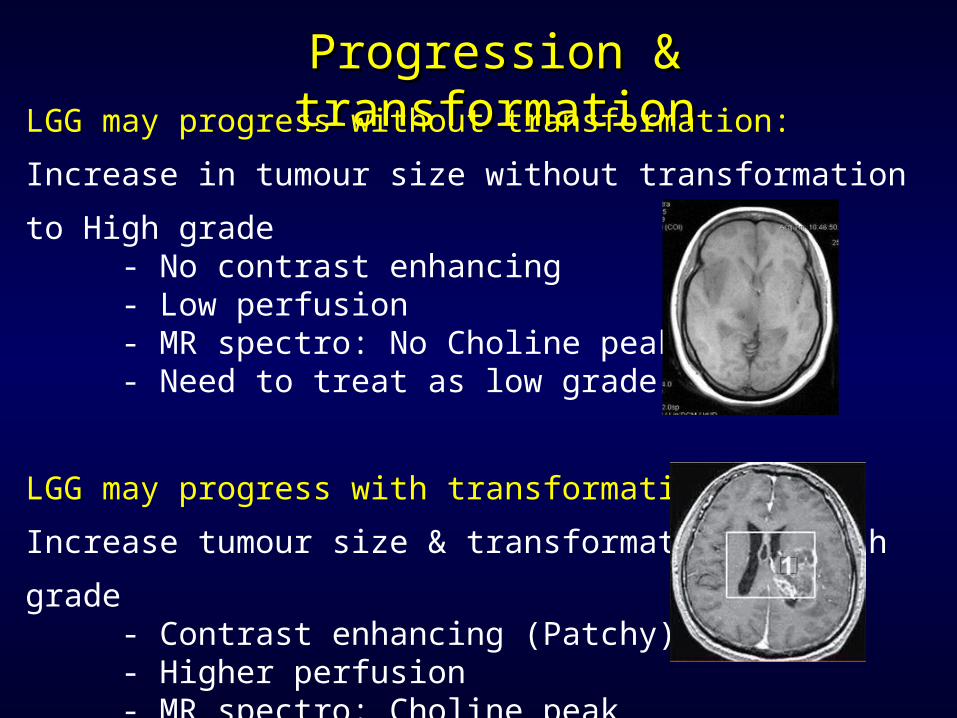
Progression & transformationProgression & transformationLGG may progress without transformation:
Increase in tumour size without transformation to High grade - No contrast enhancing - Low perfusion - MR spectro: No Choline peak - Need to treat as low grade glioma
LGG may progress with transformation:
Increase tumour size & transformation to high grade - Contrast enhancing (Patchy) - Higher perfusion - MR spectro: Choline peak - Need to treat as High grade glioma
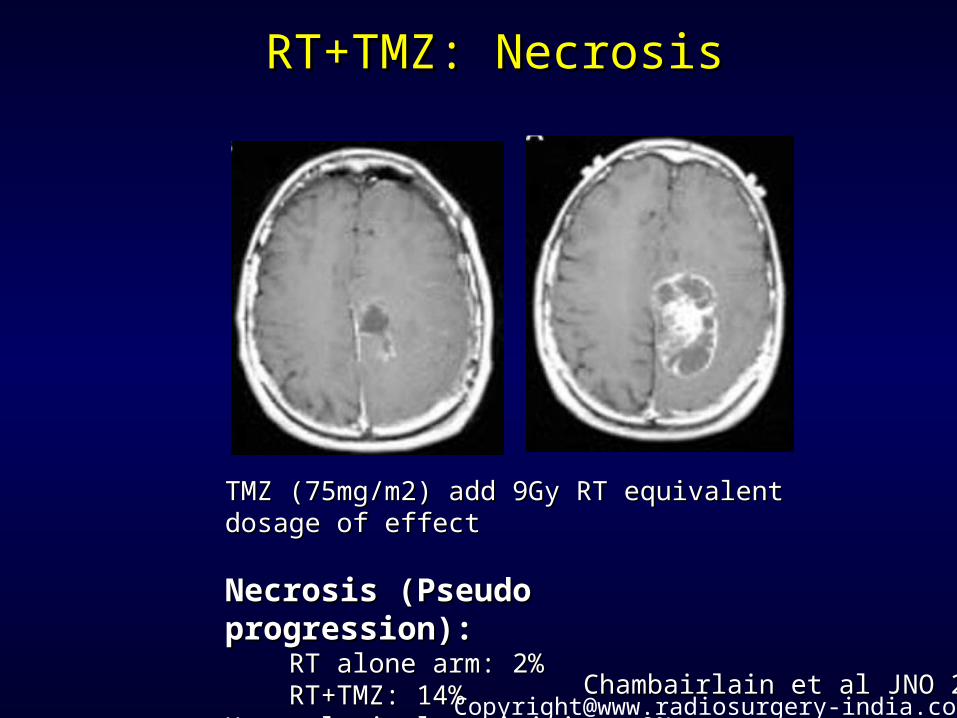
RT+TMZ: NecrosisRT+TMZ: Necrosis
Chambairlain et al JNO 2006Chambairlain et al JNO 2006
TMZ (75mg/m2) add 9Gy RT equivalent dosage of effectTMZ (75mg/m2) add 9Gy RT equivalent dosage of effect
Necrosis (Pseudo progression):Necrosis (Pseudo progression): RT alone arm: 2%RT alone arm: 2% RT+TMZ: 14%RT+TMZ: 14%Hematological toxicities: 9%Hematological toxicities: 9%

Benign/low-grade with indolent behaviourBenign/low-grade with indolent behaviourSurgery treatment of choiceSurgery treatment of choice
Completely excised/small residual - observe excellent Completely excised/small residual - observe excellent cure ratescure rates
RT only if there is gross residual/ progressionRT only if there is gross residual/ progression
Fernandez Neurosurg 2003;53:544Fernandez Neurosurg 2003;53:544
Pilocytic astrocytomasPilocytic astrocytomas
SummarySummary1. RT in LGGs have PFS benefit, no OS benefit
2. Adult LGGs with 2 or more adverse prognostic factors need early RT
3. MIB index and extent of surgery is also considered prognostic factor
4. RT dose of 50-54 Gy in 2 Gy/Fr
5. Hypofractionation (>2 Gy) not indicated
1. RT causes cognitive function impairment
2. Young pts, with seizures, near total excision and oligo component may be observed
3. Patient on follow up after surgery need stringent follow up
4. Patients with irregular follow up should also be treated with early RT