La Stipsi severa: attualità terapeutiche · La Stipsi severa: attualità terapeutiche Verona,...
43
La Stipsi severa: attualità terapeutiche Verona, 14-15 giugno 2012 Eziopatogenesi e clinica Fabrizio Bonfante
-
Upload
truongngoc -
Category
Documents
-
view
217 -
download
0
Transcript of La Stipsi severa: attualità terapeutiche · La Stipsi severa: attualità terapeutiche Verona,...

La Stipsi severa: attualità
terapeutiche Verona, 14-15 giugno 2012
Eziopatogenesi e clinica
Fabrizio Bonfante

Chronic constipation
Constipation is divided, with considerable
overlap, into issues of stool consistency
(hard, painful stools) and issues of
defecatory behavior (infrequency,
difficulty in evacuation, straining during
defecation)


Rome III Definition of Chronic Constipation
Must include 2 or more of the following:
a. Straining during at least 25% of defecations
b. Lumpy or hard stools in at least 25% of defecations
c. Sensation of incomplete evacuation for at least 25% of
defecations
d. Sensation of ano-rectal obstruction for at least 25% of
defecations
e. Manual maneuvers to facilitate at least 25% of defecations
f. Fewer than 3 defecations per week
• Loose stools are rarely present without the use of laxatives • There are insufficient criteria for IBS Longstreth et al., Gastroenterology 2006; 130(5):1480-91

Functional Bowel Disorders
Longstreth G et al, Gastroenterology 2006

Constipation Symptoms in a Patient Perspective Survey
%
n= 557
Johanson JF & Kralstein J. APT 2007;25:599-608
%

“Easy“ Chronic constipation

Myths and misconceptions in Constipation
Constipation is caused by inadequate dietary fiber intake
Increased dietary fiber relieves symptoms
Constipation is caused by inadequate fluid intake
Increased fluid intake is a helpful treatment
Constipation is caused by inadequate psysical exercise
Constipation is caused by a long colon
Laxatives cause enteric neural damage
Muller-Lissner SA et al, Am J gastroenterol 2005

Non tutte le stipsi sono uguali…

Severe chronic constipation

What mean “severe constipation” ?
• Impairment of work (69%), and social and personal life (73%)
• Almost half (47%) unsatisfied with current treatment
– For the majority (82%), due to lack of efficacy
Johanson et al. Aliment Pharmacol Ther 2007; 25: 599
80
79
66
50
52
75
50
50
67
71
60
44
Ineffective relief of bloating
Lack of predictability
Ineffective relief of multiple symptoms
Ineffective relief of constipation
OTC laxatives (n=146) Prescription laxatives (n=42) Fibre (n=68)
Patients (%)
557 eligible participants:
243 men and 314 women,
≥18 years old;
Rome II criteria;
45-question survey

Wald et al., APT 2007;26:227-36
* P<0.05 in constipated vs not constipated
Effect of constipation on QoL - 13.875 adults in 7 Countries -
Physical Scale
SF-36 Score
*
*
*
*
*
35 40 45 50 55
MSC
MH
RE
SF
VI
Mental Scale
SF-36 Score
*
*
*
*
*
• PF = Physical
functioning
• RP = Role Physical
• BP = Bodily Pain
• GH = General Health
• VT = Vitality
• SF = Social
functioning
• RE = Role Emotional
• MH = Mental Health
Constipated
Not Constipated
effect on QoL osteoarthritis, chronic allergies, diabetes, GERD, heart disease, depression

Chronic constipation
Primary constipation
Secondary constipation

Secondary constipation
Organic lesions
Medication
Neurologic Disorders
Endocrinologic or metabolic disorders
Connective tissue disorders
Muscolar disorders
Psychological issue e/o eating disorders

Medication
Antidepressants
Psychotropic drugs
Anticholinergics
Opioids
Calcium channel blockers
NSAIDs

Neurological disorders
Stroke
Hirschprung disease
Parkinson disease
Multiple sclerosis
Diabetic autonomic neuropathy
Spinal cord lesion
Chagas disease
Endocrinological or metabolic
disorders
Hypercalcemia
Hyperparathyroidism
Hypokaliemia
Hypothiroidism
Addison disease
Porphyria
Diabetes mellitus

Primary and Secondary Forms of Chronic Constipation
Iantorno et al. Dig Dis Sci. 2007;52:317–320
466 patients* with chronic constipation† referred to a gastroenterology referral unit
54% secondary
Including:
• Pharmacology (27%)
• Endocrine disorders (16%)
• Psychiatric disorders (13%)
46% primary
*382 women, 82 men; age range, 18–83 years, referred over a 10-year period to a centre in Buenos Aires, Argentina
† Defined using Rome I criteria
76,3%
8,4%
10,7%
4,7% Pelvic floor disorder
Slow transit constipation
IBS-C (normal transit)
Normal transitconstipation
Primary chronic constipation
Classification
Normal transit constipation
Slow transit constipation
Pelvic floor dysfunction or outlet
obstruction

Normal transit
Stool passage in colon at a normal rate
Overlap with IBS – constipation
Difficult evacuation :
– Bloating
– Straining
– Hard stools

Outlet obstruction
Anorectal manometry

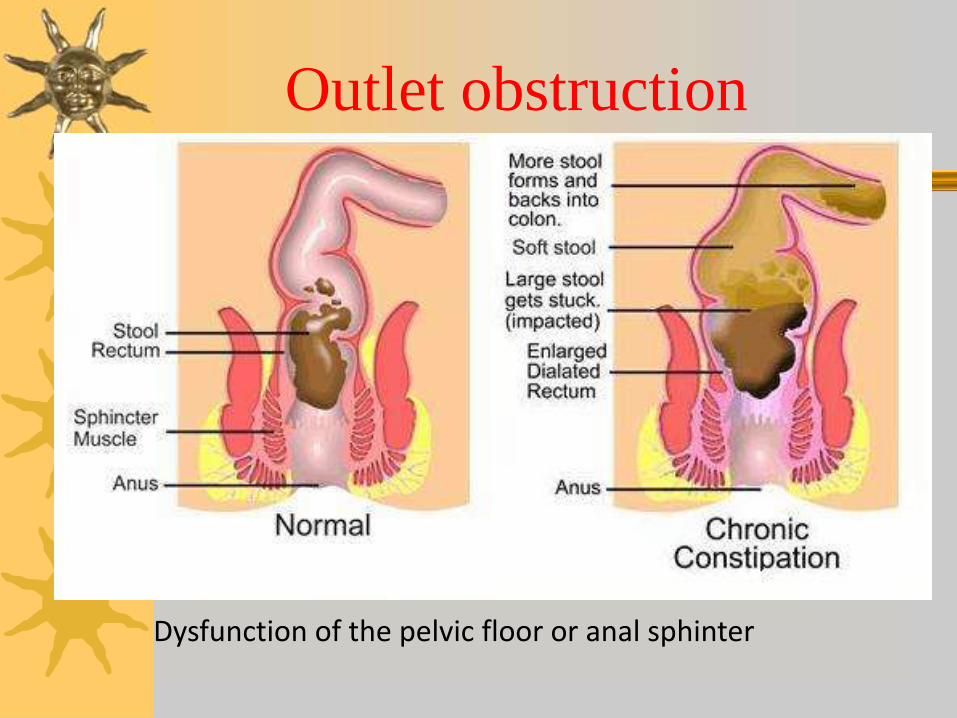
Outlet obstruction
Dysfunction of the pelvic floor or anal sphinter

Defecation disorders
Impaired rectal contraction
Paradoxical anal contraction
Inadequate anal relaxation
Lack of coordination (or dyssynergia)
Impaired rectal sensation
Structural abnormalities

Structural abnormalities
Rectal prolapse and or intussusceptions
Rectocele
Excessive perineal descent

Slow transit constipation (STC)
Impaired phasic colonic motor activity
Infrequent bowel movements
Lack of an increase in motor activity after :
– meal
– cholinergic agents
– awakening in the morning
No answer to rectal balloon distension


Dinning PG et al., WJG 2010;116:5162-72
High Amplitude Propagated Contractions
in Healthy Controls

24-hr Spatiotemporal Maps of Colonic Propagating Sequences
Dinning PG et al., WJG 2010;116:5162-72

Enteric nervous system
(the brain of the gut)
– Bowel movement
– Fluid secretion
– Blood flow

Linden & Farrugia, 2008
GI Control Mechanisms
Enteric neurons
Inter. Cajal cells Enteric glia cells Smooth muscle
changes ?
and Related Abnormalities in STC
Reviewed by Di Nardo & De Giorgio, et al. Aliment Pharmacol Ther, 2008;28:25-42

Serotonin (5-HT)
95% of serotonin in the
human body is found in
the digestive tract
Necessary for
communication between
brain and the gut

Peristalsis & Related Neuronal Circuitries
modified from Tonini et al. Neuroscience 1996;73:287-97
Ascending reflex contraction
Descending reflex relaxation
Excitatory motor neuron
Inhibitory motor neuron
Sensory neuron
ACh/TK NO/VIP/(ATP)
ACh/TK ACh/TK
Intraluminal content
Fibre colinergiche
Fibre adrenergiche

5-HT signaling

Dysfunction of the 5-HT signaling
• 5-HT availability
• 5-HT reuptake
• 5-HT receptor mechanisms e/o density
5-HT4 receptor agonists
stimulate acetylcholine secretion, thus display prokinetic activity (as tegaserod and prucalopride).

Impaired motility in
slow transit constipation
HAPCs are decreased in amplitude and
frequency • Abnormalities of the myenteric plexus
• Reduction of argyrophilic neurons and axons
• Increase in the number of variably sized nuclei within ganglia
Reduced volume of interstizial cells of Cajal
Reduced number of enteric glial cells
Dysfunction of the 5-HT signaling

Vi ringrazio per l’attenzione


Enteric glial cells (EGC)
Mechanical supporters
Promoting synaptic communication by neurotrophic factor release
Involving in enteric neurotransmission
– Glutamatergic signaling
– Nitrergic neurotransmission
Outlet obstruction
Dysfunction of the pelvic floor or anal sphinter

Defecation disorders
Impaired rectal contraction
Paradoxical anal contraction
Inadequate anal relaxation
Lack of coordination (or dyssynergia)
Impaired rectal sensation
Structural abnormalities

Neurotransmitters
The functions of enteric and extrinsic neurons are regulated by these neurotransmitters:
– noradrenalin
– acetylcholine
– opioids
– serotonin
– somatostatin
– CCK
– substance-P
– VIP
– neuropeptide-Y

Structural abnormalities
Rectal prolapse and or intussusceptions
Rectocele
Excessive perineal descent