KNEE JOINT(ANATOMY)

of 5
-
Upload
ojambo-flavia -
Category
Documents
-
view
214 -
download
0
Transcript of KNEE JOINT(ANATOMY)
-
7/30/2019 KNEE JOINT(ANATOMY)
1/5
1
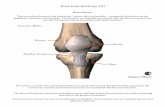
THE KNEE JOINT
The knee joint is a compound, condylar synovial joint, in which more than two
bones are involved in its formation. Three bones make up the knee joint, namely
(i) patella (ii) distal end of femur and (iii) proximal end of tibia. The fibula doesnot contribute to the knee joint. The knee joint is the largest and most elaborate in
the body. It is primarily a hinge joint, allowing only flexion and extension. [It can
allow some degree of rotation when flexed, but not when fully extended].
Articular surfaces
These are formed by the femoral condyles, the patella and the tibial condyles. All
articular surfaces are covered by articular cartilage. The patella articulates only
with the femur. The femoral condyles articulate with the tibial condyles. However,
these surfaces are not congruent. Thus the presence of two menisci renders thesesurfaces congruent.
Two major components can be recognized within the knee joint. These are:
(A) The femoropatellar joint
(B) The femorotibial joint
However, these two joints are continuous with each other.
(A) Femoropatellar joint
This is formed between the femoral trochlear and the patella. The latter is the
largest sesamoid bone in the body. The patellas anterior surface is roughened for
the attachment of the quadriceps femoris tendon and patella ligament inferiorly.
The posterior surface is smooth, being covered by hyaline cartilage, and exhibits a
vertical midline ridge. The patella runs along the trochlear groove during flexion
and extension of the knee joint. Hence the patella acts as a pulley, increasing the
mechanical advantage of the quadriceps femoris muscle during extension of the
knee joint. The patella ligament is considered to be the tendon of insertion of thequadriceps femoris muscle. This ligament attaches to the tibial tuberosity of the
tibia.
(B) The femorotibial joint
-
7/30/2019 KNEE JOINT(ANATOMY)
2/5
2
This is constituted by the condyles of the femur and the condyles of the tibia.
Interposed between the condyles are two fibrocartilage discs, called the medial and
lateral menisci. Each meniscus is C-shaped, having a thick convex peripheral
border, and a thin concave central border. [The outer curved border of eachmeniscus is attached to the joint capsule by the loose coronary ligament]. The
lateral meniscus is a more sharply curved C than the medial meniscus. The thin
tips of each meniscus are attached to the intercondylar area of the tibia. The
anterior convex margins of both menisci are attached to each other by a transverse
ligament. [In addition, the outer margin of the medial meniscus is firmly attached
to the deep surface of the tibial collateral ligament]. The menisci may contribute
to weight-bearing, but their main function is to increase congruity of the apposing
articular surfaces. [The inner concave margins and both the upper and lower
surfaces of the menisci project freely into the joint cavity]. A narrow posterior
meniscofemoral ligament connects the posterior convex surface of the lateralmeniscus to the medial femoral condyle. It runs just posterolateral to the posterior
cruciate ligament.
The Joint cavity and joint capsule
The joint capsule is attached along the articular margins of the femoral condyles
medially and laterally. It also attaches just above the intercondylar notch
posteriorly. Anteriorly, the joint cavity communicates with the suprapatellar
bursa. The latter lies between the distal end of the femur and the quadricepsfemoris muscle and tendon. The suprapatellar bursa is a good site for obtaining
synovial fluid samples or relieving severe swelling of the joint (say, when
inflamed). This archieved by inserting a needle along either the lateral or medial
margin of the patella.
Two other bursae may exist. These are the prepatellar and infrapatellar bursae.
The prepatellar bursa is subcutaneous, lying just anterior to the patella. When this
bursa is inflamed, there is pain and reduced mobility of the joint. The condition is
known as the housemaids knee. The infrapatellar bursa lies between the
patellar ligament and the proximal end of tibia. Both the prepatellar andinfrapatellar bursae do not communicate with the joint cavity. Also, distal to the
patella, the fibrous and synovial layers of the capsule are separated by the
intracapsular fat body.
Other ligaments
-
7/30/2019 KNEE JOINT(ANATOMY)
3/5
3
(a) Collateral ligaments
There are collateral ligaments namely, the fibular (lateral) and the tibial (medial)
collateral ligaments.
(i) The fibular collateral ligament is a strong, rounded cord. It extends from the
lateral femoral epicondyle to the head of the fibula. It is separated fro the lateral
meniscus by the tendon of the popliteus muscle. The fibular collateral ligament is
rarely damaged.
(ii) The tibial collateral ligament is a broad, flattened ligament. Hence it is much
weaker than the fibular collateral ligament and so it is more often damaged. It
extends from the femoral epicondyle to just below the medial condyle of tibia.
Collateral ligaments reinforce the medial and lateral aspects of the knee joint,helping to prevent side movements.
(b) Cruciate ligaments
These are (i) the anterior and (ii) posterior cruciate ligaments. They are
centrally-placed ligaments and are covered by a synovial membrane. They are two
strong bands which cross each other as they extend between the femur and tibia,
hence the name cruciate (Crux = Cross). These ligaments are named according to
their attachment to tibia. The anterior cruciate ligament extends from the anteriortibial intercondylar area to the medial surface of the lateral condyle of femur. Thus
it runs posterosuperiorly. The posterior cruciate ligament extends from the
posterior tibial intercondylar area to the lateral surface of the medial condyle of
femur. Thus it runs anterosuperiorly. The anterior cruciate ligament is always
lateral to the posterior one. The two cruciate ligaments provide stability to the knee
joint. The anterior cruciate ligament prevents forward sliding of the tibia on the
femur. Likewise, the posterior cruciate ligament prevents backward sliding of the
tibia on the femur. Rupture of these ligaments can be diagnosed by testing for these
movements when the knee is flexed. In this position, when rupture has occurred,
the leg will be able to slide excessively forward or backward with respect to thefemur. The condition is known as the drawer sign.
Movements
-
7/30/2019 KNEE JOINT(ANATOMY)
4/5
4
The overall movements of the knee joint are flexion and extension. In addition,
there is slight medial rotation of the femur with respect to the tibia. This occurs as
the joint becomes fully extended. In a relaxed standing position, the knee joint is
actually slightly hyper-extended, and the knee is said to be in a locked position.
Under these circumstances, the muscles of the thigh and leg can relax, so that thisposition can be maintained with minimum expenditure of energy.
Blood and nerve supply to the knee
Blood supply is derived from the superior, middle and inferior genicular branches
of the femoral and popliteal arteries. These branches form a rich anastomosis
around the knee joint. This anastomosis forms an important collateral circulation
that may serve to bypass the main vessels when these become narrowed or
occluded.
Innervation of the knee joint is from the nearby somatic nerves. These are the
sciatic, femoral and obturator nerves.
The popliteal fossa
This is a depression situated just posterior to the knee. It is a diamond-shaped area
through which important nerves and vessels pass from the thigh to the leg.
Boundaries of the popliteal fossa
The fossa is bounded inferiorly by the lateral and medial heads of the
gastrocnemius muscles. Superiorly, it is bounded by the biceps femoris muscle on
the lateral side, and the margins of the semimembranosus and semitendinosus
muscles on the medial side. The roof is formed by the deep fascia of the thigh
(fascia lata). The floor is formed by the posterior aspect of the distal end of the
femur and the popliteus muscle.
Contents of the popliteal fossa
(a) Vessels of the popliteal fossa
-
7/30/2019 KNEE JOINT(ANATOMY)
5/5
5
The popliteal artery is the continuation of the femoral artery. The name changes
after the femoral artery emerges from the adductor hiatus (of the adductor canal)
enter the fossa. The popliteal artery terminates by dividing into the anterior and
posterior tibial arteries. Within the fossa, it gives off two superior, one middleand two inferior genicular arteries. A popliteal pulse can be felt within the fossa.
The popliteal vein runs upward through the popliteal fossa and then enters the
adductor hiatus. Within the popliteal fossa, it receives the small saphenous vein
and the veins corresponding to the branches of the popliteal artery.
(b) Nerves
The sciatic nerve may divide into its two major branches anywhere in the posterior
thigh. However, this division often occurs as the sciatic nerve enters the poplitealfossa. The two branches are the tibial nerve and the common fibular (peroneal)
nerve. Within the fossa the tibial nerve nerve gives off muscular branches and a
medial sural cutaneous branch. The muscular branches supply the gastrocnemius,
popliteus and soleus muscles.
The common fibular (peroneal) nerve also gives off the lateral sural cutaneous
nerve. A communicating branch from the lateral sural cutaneous nerve joins the
medial sural cutaneous nerve to form the definitive sural nerve.
Other contents of the popliteal fossa
The remaining space of the fossa is filled with fat. Several lymph nodes are
embedded in this fat.