
Joachim Eberle Head of R&D, Roche Centralized Diagnosticsf4b29427-a641-42fc... · • Pipeline &...
14
Roche Oncology Event, June 19, 2006 Workshop Roche Diagnostics and Biomarker Development Joachim Eberle Head of R&D, Roche Centralized Diagnostics 2 Biomarkers and Roche Making a Diagnostics test Current Programs
Transcript of Joachim Eberle Head of R&D, Roche Centralized Diagnosticsf4b29427-a641-42fc... · • Pipeline &...

Roche Oncology Event, June 19, 2006
WorkshopRoche Diagnostics and Biomarker Development
Joachim EberleHead of R&D, Roche Centralized Diagnostics
2
Biomarkers and Roche
Making a Diagnostics test
Current Programs

Roche Oncology Event, June 19, 2006
3
Why is Roche interested in Biomarkers?
• Patients & Clinicians– early detection can increase chance of cure– patients can be selected to maximize
benefit and minimize toxicity• Payers
– optimized therapy allows more efficient use of straining healthcare budgets
– increased cost benefit per patient to reach “threshold”
• Regulatory– patient selection may be essential to gain
regulatory approval• Pipeline & Positioning
– allows us to make better development and portfolio decisions
5
Like
lihoo
d tr
eatm
ent
succ
ess
lower
higher
higherCost Effectiveness
treating patients that will benefit - not treating those that will not
Genom
ics
Prot
eom
ics
Future
4
Prognostic
Biological markers or “Biomarkers”Tests measuring a persons health status
Predict the likely response to a drug to discriminate “responders” from “non-responders”
Once disease state established, predict the probable course of the disease (“slow” vs. “fast” progressors)
Monitor efficacy of treatment or recurrence of disease
Discriminate “healthy” from asymptomatic “disease” state. Often used to screen large populations
Gene setup predisposes for disease - may or may not result in actual development of the disease
Risk Assessment / Predisposition
Therapy Monitoring
Screening / Early Detection
Patient Stratification/ Therapy selection

Roche Oncology Event, June 19, 2006
5
Risk Assessment
Screening / Early Detection
Normal - Pre-cancer - Early cancer - Carcinoma-Metastasis - Recurrence
Adjuvant Therapy Palliative Therapy
Personalized Treatment (Stratification)
Adaptationof Therapy
Potential use of Biomarkers in Oncology
Prognosis / Therapy Selection
Monitoring Recurrence, Therapy
Curative Intervention
Tum
or M
ass
(Cel
ls)
108
104
Cancer Progression
6
Biomarkers and Roche
Making a Diagnostics test
Current Programs
Roche Oncology Event, June 19, 2006
7
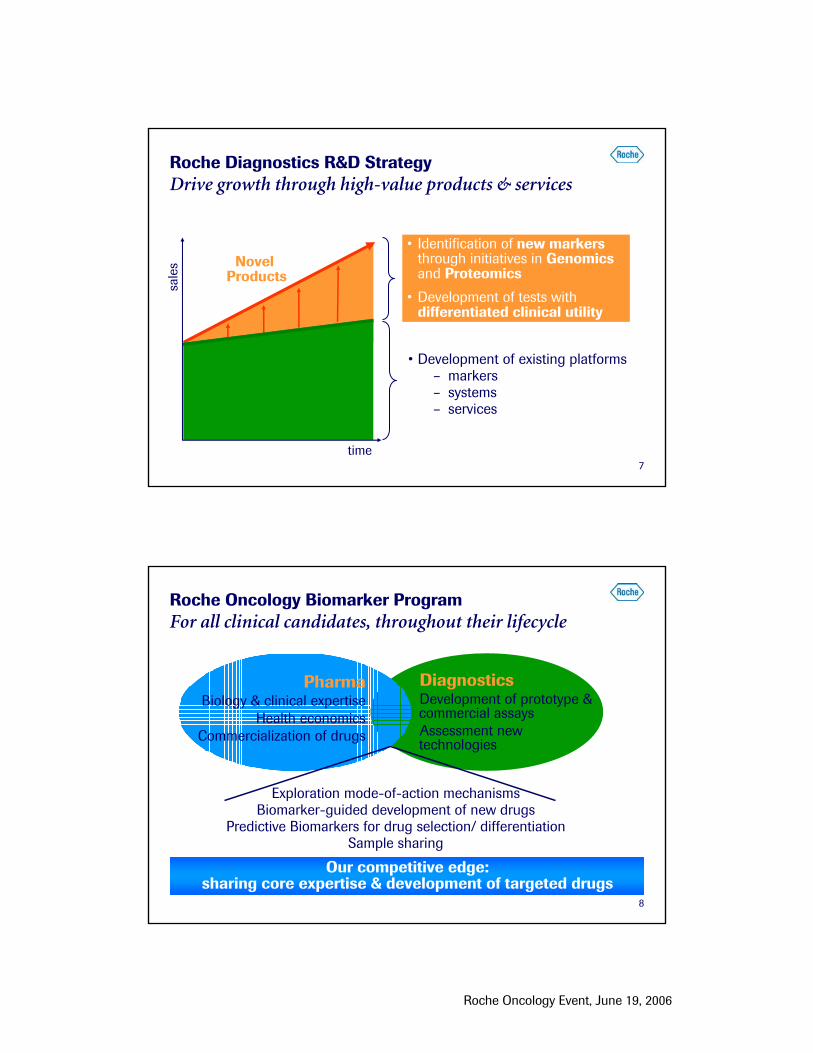
Roche Diagnostics R&D StrategyDrive growth through high-value products & services
• Development of existing platforms– markers – systems– services
time
sale
s
• Identification of new markersthrough initiatives in Genomicsand Proteomics
• Development of tests with differentiated clinical utility
Novel Products
8
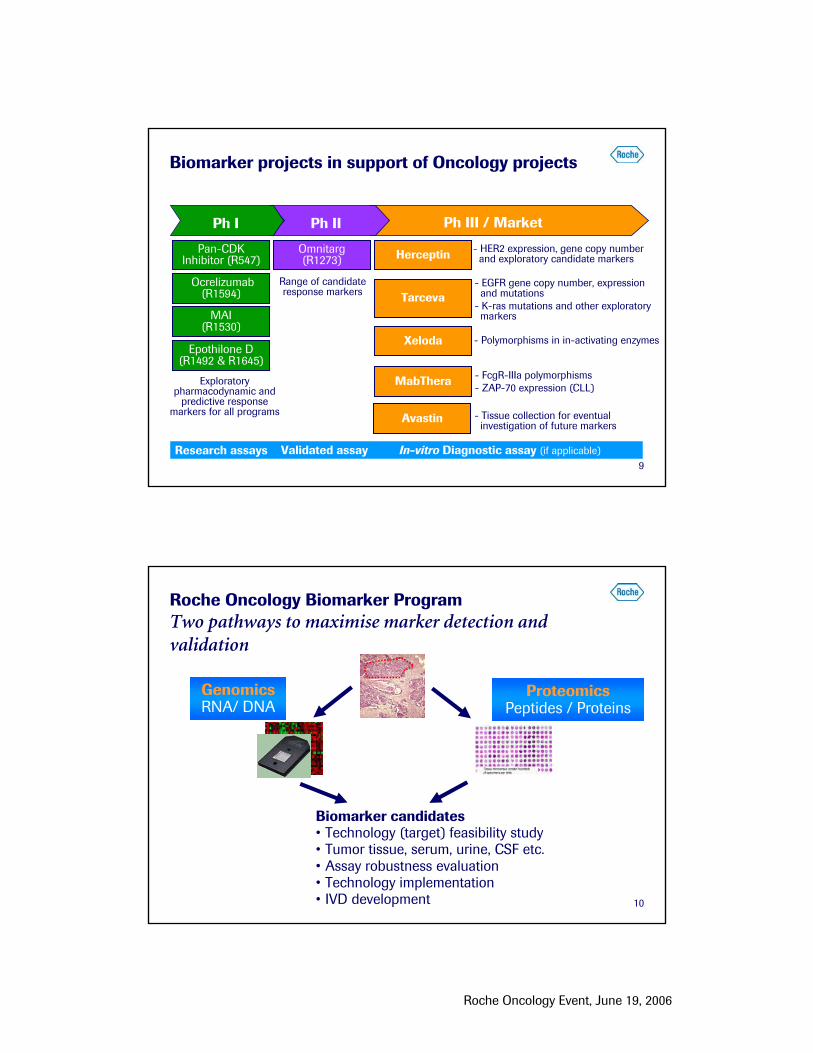
Roche Oncology Biomarker Program For all clinical candidates, throughout their lifecycle
DiagnosticsDevelopment of prototype &commercial assaysAssessment new technologies
Exploration mode-of-action mechanismsBiomarker-guided development of new drugs
Predictive Biomarkers for drug selection/ differentiationSample sharing
PharmaBiology & clinical expertise
Health economicsCommercialization of drugs
Our competitive edge: sharing core expertise & development of targeted drugs
Roche Oncology Event, June 19, 2006
9
Herceptin
Tarceva
Xeloda
MabThera
Avastin
Pan-CDKInhibitor (R547)
Ocrelizumab(R1594)
MAI (R1530)
Epothilone D(R1492 & R1645)
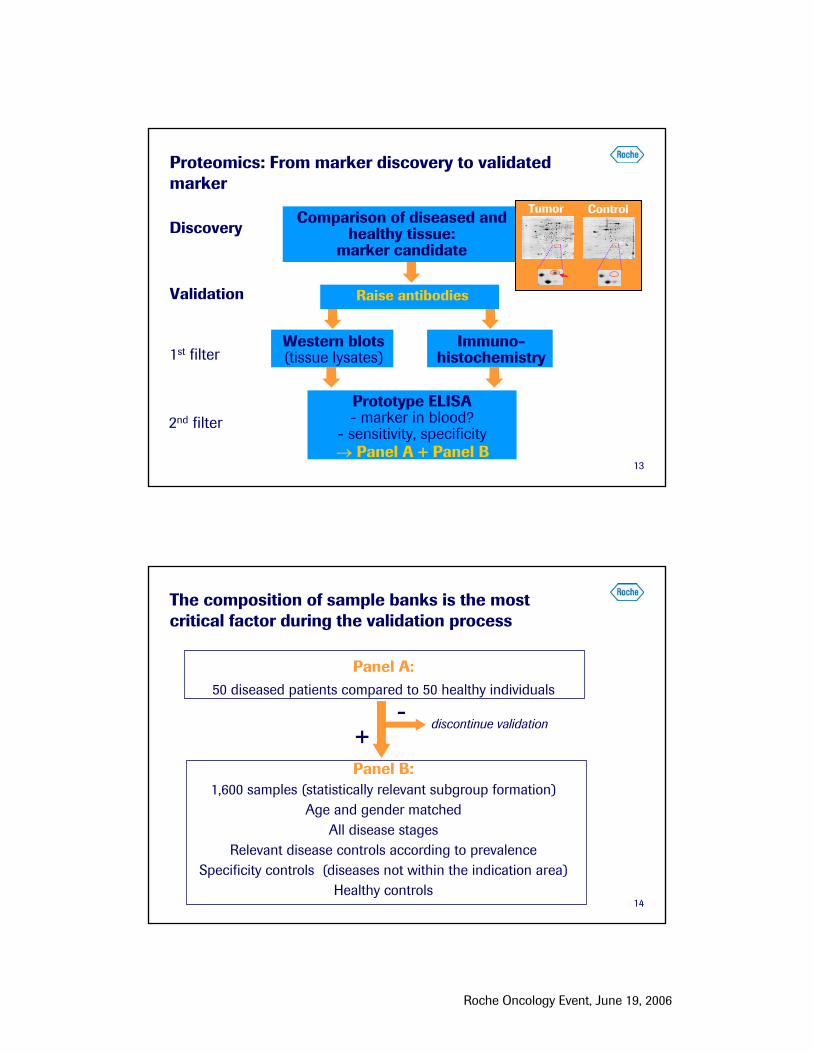
Biomarker projects in support of Oncology projects
Research assays Validated assay In-vitro Diagnostic assay (if applicable)
Ph II Ph III / MarketPh I
- HER2 expression, gene copy numberand exploratory candidate markers
- EGFR gene copy number, expressionand mutations
- K-ras mutations and other exploratorymarkers
- Polymorphisms in in-activating enzymes
- FcgR-IIIa polymorphisms- ZAP-70 expression (CLL)
Omnitarg(R1273)
Range of candidate response markers
- Tissue collection for eventualinvestigation of future markers
Exploratory pharmacodynamic and
predictive response markers for all programs
10
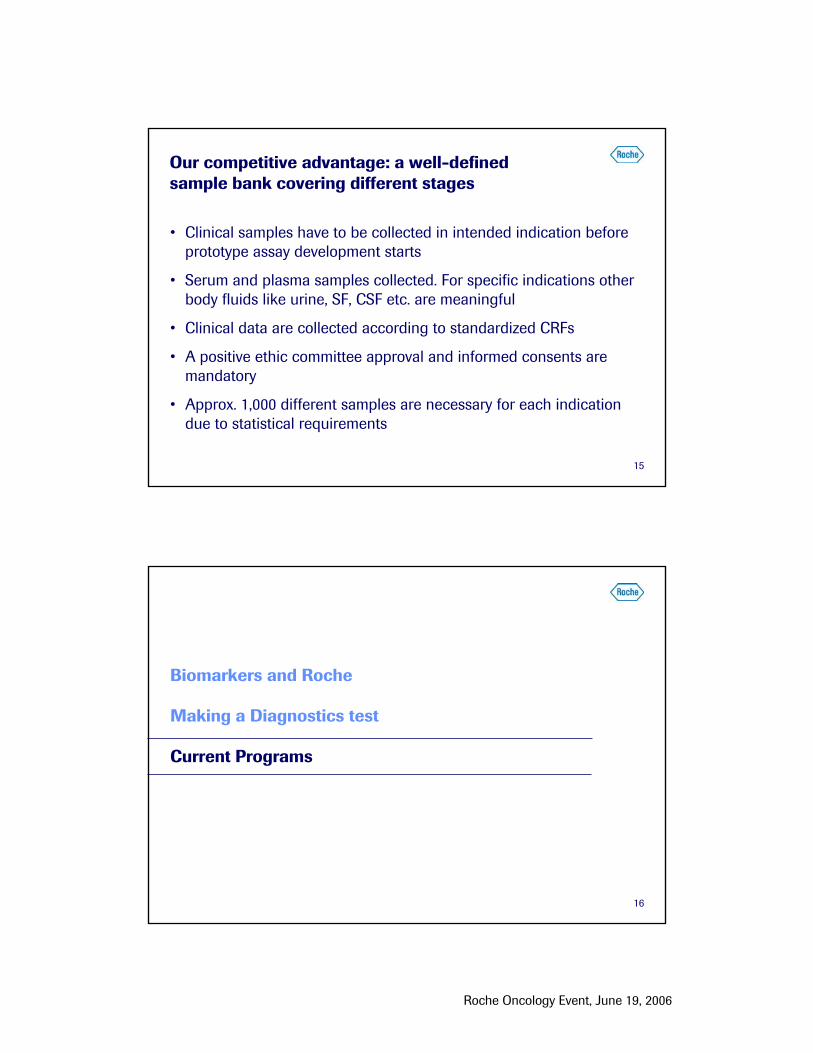
GenomicsRNA/ DNA
ProteomicsPeptides / Proteins
Biomarker candidates• Technology (target) feasibility study• Tumor tissue, serum, urine, CSF etc. • Assay robustness evaluation• Technology implementation • IVD development
Roche Oncology Biomarker Program Two pathways to maximise marker detection and validation

Roche Oncology Event, June 19, 2006
11
Bladder
Lung
Liver
Blood / bone marrow
Prostate
Colon
Breast
MonitoringTherapy
predictionRelapse
predictionClassificationScreeningCancer site
Research program based on clinical need, medical value and technology match
P
#targets 1000 – 100,0001-10
G
MicroarraysTaqMan/ PCR Elecsys IMPACT (Protein Array)
P
1- 3 Up to 20
P
P
P G
G
G
G
Genomics Proteomics
PG P
G
P P
G
G
P
P G
G G
GG P P
G
12
From diagnostic marker candidate to a product Three development phases
• Internal R&D• External R&D • Co-operations• In-licensing • Markers in
public domain
Phase I:IdentifyingCandidates
2 Years
Marker Candidate100 candidates
Phase II:Prototype
Development
• Antibody dev.• Pre-validation• Prototype assays• Validation
studies on sample panels
1-1.5 Years
Validated Candidate20 candidates
• Test development• Platform • Manufacturing• Clinical trials • Registration• Marketing
Phase III:Product
Development
3 Years
Commercial Product~5 potential markers
Roche Oncology Event, June 19, 2006
13
Comparison of diseased and healthy tissue:
marker candidateDiscovery
1st filterWestern blots (tissue lysates)
Immuno-histochemistry
Raise antibodiesValidation
Tumor Control
Proteomics: From marker discovery to validated marker
2nd filterPrototype ELISA- marker in blood?
- sensitivity, specificity→ Panel A + Panel B
14
The composition of sample banks is the most critical factor during the validation process
Panel A:50 diseased patients compared to 50 healthy individuals
Panel B:1,600 samples (statistically relevant subgroup formation)
Age and gender matched All disease stages
Relevant disease controls according to prevalenceSpecificity controls (diseases not within the indication area)
Healthy controls
+-
discontinue validation
Roche Oncology Event, June 19, 2006
15
Our competitive advantage: a well-defined sample bank covering different stages
• Clinical samples have to be collected in intended indication before prototype assay development starts
• Serum and plasma samples collected. For specific indications other body fluids like urine, SF, CSF etc. are meaningful
• Clinical data are collected according to standardized CRFs
• A positive ethic committee approval and informed consents are mandatory
• Approx. 1,000 different samples are necessary for each indication due to statistical requirements
16
Biomarkers and Roche
Making a Diagnostics test
Current Programs

Roche Oncology Event, June 19, 2006
17
Overview: blood-based screening test programsDual development genomic and proteomic targets
> 90lung
no program> 20 candidate markersprostate
> 13discovery underwaybreast
> 12 22 candidate markerscolorectal
Protein markersMethylated DNA markersCancer
7 CRC & 2 Breast markers currently in validation
18
Colorectal cancer (CRC) screening Highly curable when diagnosed in early stage
Less than 40 % CRC detected at early stages
Urgent need for screening markers in body fluids indicating early stage disease
colon
small intestine
rectum
Location
Stage at first diagnosis:5-year survival:
Stage IV Distant
metastases
17 %5 %
Stage IIIRegional
lymph node involvement
28 %55 %
Stage I + IIRestricted
to gut
55 %90 %

Roche Oncology Event, June 19, 2006
19
Risk population ( > 50 yrs or symptoms orfamily history)
unsatisfactory as first-line screening assay
- highly invasive- poor acceptance- not useful as general
screening method
Sensitivity close to 100 %
Specificity 100 %
Sensitivity* 25-50 %(number of true CRC positives detected by the assay)
Specificity* 80-95 %(number of true negatives correctly identified)
Colonoscopy
FOBT(fecal occultblood test)
Confirmation by Biopsy
Current CRC screening algorithmsIssues with sensitivity, specificity &/ or compliance
* FOBT sensitivity: Collins et al. Annals Internal Medicine 2005; 142: 81 Imperiale et al. NEJM 2004; 351:2704
20
CRC Results: Final diagnostic test most likely will be a combination of markers
• Identified differences between "healthy" and diseased tissue
• Differences could be confirmed in serum using prototype ELISA
• Combinations of markers increases sensitivity
• Continue validation of additional markers
• Clinical validation underway
Receiver Operator Curves (ROC)of different markers:
AUC = area under the curve
Sens
itivi
ty %
0204060801000
20
40
60
80
100
Specificity %
CRC1 Marker(AUC= 0,801)[most significantsingle parameter]
INDEX CRC(AUC= 0,938)
Contribution by additional 13potential tumor markers

Roche Oncology Event, June 19, 2006
21
Morphology Cytogenetics Immunophenotyping
Cytochemistry FISH Molecular Biology
61-90 %
70-90 %
75-92 %
80-90 %
76-95 %
83-90 %
Current standards in diagnosis of leukemiaVarying reproducibility rates of gold standards
• No single test currently sufficient to establish diagnosis• Current tests subjective, with up to 7 days turnaround• Lack standardization & automation - need highly skilled staff
22
Genomics program: Leukemia microarrayImproved diagnosis enables better treatment
• Heterogeneous disease caused by genetic abnormalities
• Distinction between chronic, acute and sub-classifications essential for successful treatment
– ~20 subgroups
AmpliChip Leukemia• single assay for sub-classification of major leukemia classes• potential to replace other methods/ technologies• research program ’05/ ’06
del(17p)del(13q)
Others
t(9;22)
t(9;22)t(11q23)/ MLL
t(8;14)T-ALL
T-ALL corticalt(1;19)
t(12;21)Hyperdiploid
ALL Others
t(8;21)t(11q23)/ MLLt(15;17)inv(16)ComplexNormal + Others
ALLALL
nBMnBM
NLNL
MDSMDS
Others
CLLCLL
AMLAML
CMLCML
Roche Oncology Event, June 19, 2006
23
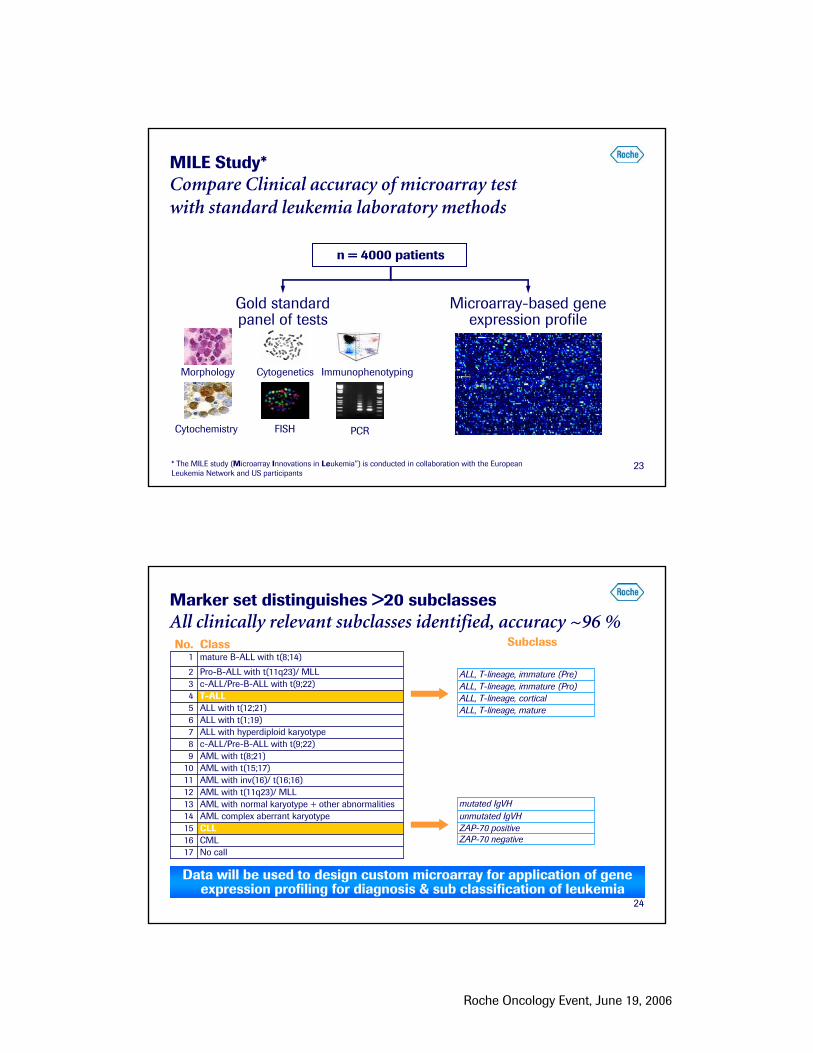
Gold standard panel of tests
Morphology Cytogenetics Immunophenotyping
FISHCytochemistry PCR
Microarray-based gene expression profile
n = 4000 patients
* The MILE study (Microarray Innovations in Leukemia”) is conducted in collaboration with the European Leukemia Network and US participants
MILE Study*Compare Clinical accuracy of microarray test with standard leukemia laboratory methods
24
Marker set distinguishes >20 subclasses All clinically relevant subclasses identified, accuracy ~96 %
Subclass
Data will be used to design custom microarray for application of gene expression profiling for diagnosis & sub classification of leukemia
CML16CLL15AML complex aberrant karyotype14AML with normal karyotype + other abnormalities13AML with t(11q23)/ MLL12
c-ALL/Pre-B-ALL with t(9;22)8AML with t(8;21)9AML with t(15;17)10AML with inv(16)/ t(16;16)11
ALL with hyperdiploid karyotype7ALL with t(1;19)6ALL with t(12;21)5
Pro-B-ALL with t(11q23)/ MLL2c-ALL/Pre-B-ALL with t(9;22)3
No call17
T-ALL4
mature B-ALL with t(8;14)1ClassNo.
ALL, T-lineage, matureALL, T-lineage, corticalALL, T-lineage, immature (Pro)ALL, T-lineage, immature (Pre)
ZAP-70 negativeZAP-70 positiveunmutated IgVHmutated IgVH
Roche Oncology Event, June 19, 2006
25
Summary
• Biomarkers are becoming a requirement in future healthcare
• Biomarker discovery is similar to drug development in timelines and success
• New assays most likely a combination of markers
• Roche has extensive joint program for all drugs throughout theirlifecycle
• Our strategy should provide Roche competitive edge in developinginnovative products and services
26
Appendix

Roche Oncology Event, June 19, 2006
27
MILE study inter-lab dataHigh inter- and intra-laboratory reproducibility
Data from the training phase (proficiency testing) using all genes represented on HG-U133 Plus 2.0 array
High correlation and concordance ensures high quality data
Reproducibility and concordanceInter-site comparison
28
2007 2008 2009
New Cancer marker launches
Bladder cancer monitoring test
Leukemia microarray (classification) Research use
AmpliChip p53 test (mutational analysis) Research use
Screening test for colorectal cancer
Cobas TaqMan
Methylation on Cobas TaqMan
Microarray
Breast relapse prediction test (p53)
Lymphoma (classification)Impact (Protein Array)
Screening test for prostate and breast cancer
Breast cancer therapy (p53)
Launch dates are estimates only; US launches may be later than indicated
2006



![Concerto in D minor for two violins and strings [BWV 1043] · e f g g g g g g j j j j j j j j pqp p j p p j j j pqp p j j m m pup k p p p p p j j j j j j t pqp p pqp p j j j j j p](https://static.fdocuments.us/doc/165x107/5b798ec17f8b9a534c8d8ff7/concerto-in-d-minor-for-two-violins-and-strings-bwv-1043-e-f-g-g-g-g-g-g-j.jpg)














