insight review articles The immunopathogenesis of sepsiscbsg/Materials/Cohen_nature01326.pdf ·...
7
insight review articles NATURE | VOL 420 | 19/26 DECEMBER 2002 | www.nature.com/nature 885 S epsis describes a complex clinical syndrome that results from a harmful or damaging host response to infection. As a result of a concerted effort to understand the underlying pathogenetic mechanisms, there have been significant advances that have illuminated not just the process of sepsis, but also fundamental principles governing bacterial–host interactions. Unfortunately, attempts to translate these observations into improved clinical outcomes proved unsuccessful and led to considerable frustration. But in the past year, four major clinical trials that are based on somewhat different strategies have shown that it is possible to significantly reduce the mortality from sepsis and septic shock, and it is therefore timely to review these developments, both in basic science and its clinical applications. Sepsis develops when the initial, appropriate host response to an infection becomes amplified, and then dysregulated. Clinically, the onset is often insidious: features may include fever, mental confusion, transient hypotension, diminished urine output or unexplained thrombocytopenia. If untreated, the patient may develop respiratory or renal failure, abnormal- ities of coagulation, and profound and unresponsive hypoten- sion. A recent epidemiological study from North America found that the incidence was approximately 3.0 cases per 1,000 population, which translates into an annual burden of approx- imately 750,000 cases. The overall mortality is approximately 30%, rising to 40% in the elderly and is 50% or greater in patients with the more severe syndrome, septic shock 1 . It is worth emphasizing that these figures represent mortality rates in patients admitted to hospital intensive care units and given antibiotics and the best available supportive care. The commonest sites of infection are the lungs, abdominal cavity, the urinary tract and primary infections of the blood stream. A microbiological diagnosis is made in about half the cases; Gram-negative bacteria account for about 60% of cases, Gram-positive for the remainder 1,2 . Microbial components that initiate injury Determining the structural components of bacteria that are responsible for initiating the septic process has been impor- tant not only in understanding the underlying mechanisms, but also in identifying potential therapeutic targets. These bacterial motifs, which are recognized by the innate immune system, have been called pathogen-associated molecular patterns (PAMPs) 3 , although it might be more accurate to call them microorganism-associated molecular patterns as it is by no means clear how the host distinguishes between signals from pathogens rather than commensals. In Gram-negative bacteria, lipopolysaccharide (LPS; known also as endotoxin) has a dominant role. The outer membrane of Gram-negative bacteria is constructed of a lipid bilayer, separated from the inner cytoplasmic mem- brane by peptidoglycan. The LPS molecule is embedded in the outer membrane and the lipid A portion of the molecule serves to anchor LPS in the bacterial cell wall. Biophysical studies on the three-dimensional conforma- tion adopted by different lipid A partial structures have revealed that, under physiological conditions, the most active forms assume the shape of a truncated cone, whereas inactive molecules prefer a lamellar structure and become progres- sively more cylindrical 4 . These conformational changes seem to correlate with the ability to activate host cell membranes. There is no endotoxin in Gram-positive bacteria, but their cell walls do contain peptidoglycan and lipoteichoic acid, and several investigators have identified structural components that account for their biological activity 5,6 . Both peptidoglycan and lipoteichoic acid can bind to cell- surface receptors and are pro-inflammatory 7 , although they are much less active, on a weight-for-weight basis, than LPS. Their role in the pathogenesis of clinical sepsis remains uncertain because there are no convincing clinical data to show that they are present in the circulation at concentra- tions comparable to those used in the experimental setting. However, an important feature of Gram-positive cells is the production of potent exotoxins, some of which are implicated in septic shock. The best known examples are the toxic shock syndromes caused by toxic shock syndrome toxin-1 (TSST-1)-producing strains of Staphylococcus aureus and the pyrogenic exotoxins from Streptococcus pyogenes. Toxic shock syndromes are among the most acute and most severe forms of septic shock. They frequently occur without warning in otherwise healthy individuals and the mortality can be as high as 50%. These Gram-positive exotoxins are of great interest because they exhibit the properties of superantigens, that is, they are able to bind promiscuously to major histocompatibility complex class II and a restricted repertoire of T-lymphocyte receptor (TCR) Vb domains. In so doing they cause massive T-cell activa- tion and release of pro-inflammatory lymphokines 8 , suggesting a plausible role for these toxins as a cause of the profound shock that is seen in patients with toxic shock. Detailed structural analyses have been done for many bacterial superantigens, and the crystal structures of several staphylococcal and streptococcal toxins have been elucidated 9 . Interestingly, sequence variability in the amino-terminal domain dictates varying affinities for specific human leukocyte antigen (HLA) class II alleles; for instance, the strep- The immunopathogenesis of sepsis Jonathan Cohen Brighton & Sussex Medical School, Westlain House, Falmer, Brighton BN1 9PH UK (e-mail: [email protected]) Sepsis is a condition that results from a harmful or damaging host response to infection. Many of the components of the innate immune response that are normally concerned with host defences against infection can, under some circumstances, cause cell and tissue damage and hence multiple organ failure, the clinical hallmark of sepsis. Because of the high mortality of sepsis in the face of standard treatment, many efforts have been made to improve understanding of the dysregulation of the host response in sepsis. As a result, much has been learnt of the basic principles governing bacterial–host interactions, and new opportunities for therapeutic intervention have been revealed. © 2002 Nature Publishing Group
Transcript of insight review articles The immunopathogenesis of sepsiscbsg/Materials/Cohen_nature01326.pdf ·...

insight review articles
NATURE | VOL 420 | 19/26 DECEMBER 2002 | www.nature.com/nature 885
Sepsis describes a complex clinical syndromethat results from a harmful or damaging hostresponse to infection. As a result of a concertedeffort to understand the underlyingpathogenetic mechanisms, there have been
significant advances that have illuminated not just theprocess of sepsis, but also fundamental principlesgoverning bacterial–host interactions. Unfortunately,attempts to translate these observations into improvedclinical outcomes proved unsuccessful and led toconsiderable frustration. But in the past year, four majorclinical trials that are based on somewhat differentstrategies have shown that it is possible to significantlyreduce the mortality from sepsis and septic shock, and it istherefore timely to review these developments, both inbasic science and its clinical applications.
Sepsis develops when the initial, appropriate host responseto an infection becomes amplified, and then dysregulated.Clinically, the onset is often insidious: features may includefever, mental confusion, transient hypotension, diminishedurine output or unexplained thrombocytopenia. If untreated,the patient may develop respiratory or renal failure, abnormal-ities of coagulation, and profound and unresponsive hypoten-sion. A recent epidemiological study from North Americafound that the incidence was approximately 3.0 cases per 1,000population, which translates into an annual burden of approx-imately 750,000 cases. The overall mortality is approximately30%, rising to 40% in the elderly and is 50% or greater inpatients with the more severe syndrome, septic shock1. It isworth emphasizing that these figures represent mortality ratesin patients admitted to hospital intensive care units and givenantibiotics and the best available supportive care. The commonest sites of infection are the lungs, abdominal cavity,the urinary tract and primary infections of the blood stream. Amicrobiological diagnosis is made in about half the cases;Gram-negative bacteria account for about 60% of cases,Gram-positive for the remainder1,2.
Microbial components that initiate injuryDetermining the structural components of bacteria that areresponsible for initiating the septic process has been impor-tant not only in understanding the underlying mechanisms,but also in identifying potential therapeutic targets. Thesebacterial motifs, which are recognized by the innateimmune system, have been called pathogen-associated molecular patterns (PAMPs)3, although it might be moreaccurate to call them microorganism-associated molecularpatterns as it is by no means clear how the host distinguishesbetween signals from pathogens rather than commensals.
In Gram-negative bacteria, lipopolysaccharide (LPS;known also as endotoxin) has a dominant role. The outermembrane of Gram-negative bacteria is constructed of alipid bilayer, separated from the inner cytoplasmic mem-brane by peptidoglycan. The LPS molecule is embedded inthe outer membrane and the lipid A portion of the moleculeserves to anchor LPS in the bacterial cell wall.
Biophysical studies on the three-dimensional conforma-tion adopted by different lipid A partial structures haverevealed that, under physiological conditions, the most activeforms assume the shape of a truncated cone, whereas inactivemolecules prefer a lamellar structure and become progres-sively more cylindrical4. These conformational changes seemto correlate with the ability to activate host cell membranes.
There is no endotoxin in Gram-positive bacteria, buttheir cell walls do contain peptidoglycan and lipoteichoicacid, and several investigators have identified structuralcomponents that account for their biological activity5,6.Both peptidoglycan and lipoteichoic acid can bind to cell-surface receptors and are pro-inflammatory7, although theyare much less active, on a weight-for-weight basis, than LPS.Their role in the pathogenesis of clinical sepsis remainsuncertain because there are no convincing clinical data toshow that they are present in the circulation at concentra-tions comparable to those used in the experimental setting.
However, an important feature of Gram-positive cells isthe production of potent exotoxins, some of which areimplicated in septic shock. The best known examples are thetoxic shock syndromes caused by toxic shock syndrometoxin-1 (TSST-1)-producing strains of Staphylococcusaureus and the pyrogenic exotoxins from Streptococcus pyogenes. Toxic shock syndromes are among the most acuteand most severe forms of septic shock. They frequentlyoccur without warning in otherwise healthy individuals andthe mortality can be as high as 50%. These Gram-positiveexotoxins are of great interest because they exhibit the properties of superantigens, that is, they are able to bindpromiscuously to major histocompatibility complex class IIand a restricted repertoire of T-lymphocyte receptor (TCR)Vb domains. In so doing they cause massive T-cell activa-tion and release of pro-inflammatory lymphokines8, suggesting a plausible role for these toxins as a cause of theprofound shock that is seen in patients with toxic shock.
Detailed structural analyses have been done for many bacterial superantigens, and the crystal structures of severalstaphylococcal and streptococcal toxins have been elucidated9.Interestingly, sequence variability in the amino-terminaldomain dictates varying affinities for specific human leukocyte antigen (HLA) class II alleles; for instance, the strep-
The immunopathogenesis of sepsisJonathan Cohen
Brighton & Sussex Medical School, Westlain House, Falmer, Brighton BN1 9PH UK (e-mail: [email protected])
Sepsis is a condition that results from a harmful or damaging host response to infection. Many of thecomponents of the innate immune response that are normally concerned with host defences against infectioncan, under some circumstances, cause cell and tissue damage and hence multiple organ failure, the clinicalhallmark of sepsis. Because of the high mortality of sepsis in the face of standard treatment, many effortshave been made to improve understanding of the dysregulation of the host response in sepsis. As a result,much has been learnt of the basic principles governing bacterial–host interactions, and new opportunities fortherapeutic intervention have been revealed.
© 2002 Nature Publishing Group

Several other bacterial components have been shown to have pro-inflammatory activity and to be able to induce shock in experimentalsystems. These include cell-wall structures such as flagellin15 andcurli16, and unmethylated CpG sequences in naked bacterial DNA17.Receptors for some of these elements have been identified among thefamily of Toll-like proteins that are now known to be crucial in thecellular recognition of microbial structures18.
Host recognition of microbial componentsThe CD14–LBP complexThe inability to identify an ‘LPS receptor’ was for many years a barrierto understanding how Gram-negative bacteria initiated the septicresponse, but in a series of elegant studies it was shown that activationof host cells was dependent on the presence of LPS-binding protein(LBP) and the opsonic receptor CD14 (ref. 19). Although CD14 wasoriginally identified as the essential co-receptor that mediated LPSactivation of monocytes, subsequent work has shown that it also par-ticipates in the activation by Gram-positive cell-wall componentssuch as peptidoglycan20, mediates macrophage apoptosis21, and isimportant in shuttling LPS between serum proteins that have thecapacity to bind LPS, such as LBP and serum lipoproteins22. Mem-brane bound CD14 (mCD14) is a glycosylphosphatidylinositol-linked molecule anchored in the cell surface, but it is also found in thecirculation as soluble CD14 (sCD14). Many cells that are constitu-tively CD14 negative, such as dendritic cells, fibroblasts, smoothmuscle cells and vascular endothelium, are still able to respond to LPSby interacting with sCD14. sCD14 is found in the serum of healthyindividuals but levels rise in sepsis23, and antibody to CD14 protectsprimates from lethal endotoxin shock24.
Toll-like receptorsAlthough the discovery of CD14 represented a significant step for-ward in understanding host responses to LPS, the fact that mCD14had no intracellular tail meant that it remained unclear how ligationof the LPS–LBP complex led to cellular activation. This uncertaintywas resolved by the discovery of the family of Toll-like receptors
insight review articles
886 NATURE | VOL 420 | 19/26 DECEMBER 2002 | www.nature.com/nature
tococcal superantigen SPEA (for streptococcal pyrogenic exotoxin A)shows significantly greater affinity for HLA-DQ than HLA-DR. Thesedifferences may in part explain the remarkable selectivity of the toxicshock syndromes: although staphylococcal and streptococcal strainsbearing superantigen genes are widespread and indeed frequently causeinfections, toxic shock syndromes are relatively uncommon.
Although experimental and epidemiological studies providesome support for the view that these superantigenic toxins are thecause of the toxic shock syndromes10, it is by no means clear that it istheir superantigenicity per se that is responsible. For instance, despitemany data that implicate the streptococcal toxin SPEA11, this is in facta relatively weak superantigen compared to the more recentlydescribed toxin streptococcal mitogenic exotoxin Z (SMEZ)12. Yet inexperimental models in which HLA-DQ transgenic mice are chal-lenged with strains of S. pyogenes in which smez is disrupted, there isno effect on survival despite a profound reduction in pro-inflamma-tory activity13. These findings are important because there is consid-erable interest in devising therapeutic strategies that are targeted atGram-positive infections and the toxic shock syndromes, and it is notclear whether these strategies should be aimed at the superantigenic-ity, or at other pro-inflammatory properties of the toxins.
There are also data that suggest that superantigenic toxins fromGram-positive bacteria induce hypersensitivity to LPS. The staphy-lococcal toxin TSST-1 enhances the susceptibility of rabbits to a lethalinjection of LPS by a factor of approximately 50,000, and co-injectionof LPS and TSST-1 induces tumour-necrosis factor-a (TNF-a) levelssignificantly higher than injection of similar doses of either toxinalone. Mice with severe combined immunodeficiency, lacking B andT lymphocytes, are resistant to this effect, but regain sensitivity whenreconstituted with T-cells, and the mechanism seems to be dependent on enhanced production of interferon-g (IFN-g) fromtoxin-activated T cells14. This interaction between superantigens andLPS might in part explain the devastating nature of the toxic shocksyndromes. It could also have therapeutic implications, as it might beadvantageous to target LPS even if the infection is apparently causedexclusively by Gram-positive bacteria.
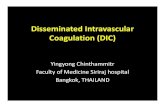
Figure 1 Cell-surface recognition oflipopolysaccharide (LPS). The principal mechanism bywhich LPS is sensed is via an LPS-binding protein(LBP)–LPS complex and then signalling through theToll-like receptor 4 (TLR4)–MD-2 complex. However,other cell surface molecules also sense LPS; theseinclude the macrophage scavenger receptor (MSR),CD11b/CD18 and ion channels. Intracellularsignalling depends on binding of the intracellular TLRdomain, TIR (Toll/IL-1 receptor homology domain), toIRAK (IL-1 receptor-associated kinase), a process thatis facilitated by two adapter proteins, MyD88 (myeloiddifferentiation protein 88) and TIRAP (TIR domain-containing adapter protein; also called MyD88-adapter-like protein or Mal), and inhibited by a thirdprotein Tollip (Toll-interacting protein). Note that thereis also an MyD88-independent pathway by whichTIRAP/Mal signals through an RNA-dependent proteinkinase (PKR) and interferon regulatory factor (IRF)-3.Recently it has been proposed that cells may also beable to respond to LPS by intracellular receptorscalled NOD proteins (for nucleotide-bindingoligomerization domain). NOD1 (also called caspase-recruitment domain 4) was identified originally on thebasis of structural homology to the apoptosisregulator, Apaf-1. The NOD proteins have some similarities to the resistance (R) genes in plants that are involved in pathogen recognition; in common with TLRs and R genes, NODshave leucine-rich repeats. Expression of NOD1 and NOD2 confer responsiveness to Gram-negative LPS but not to lipoteichoic acid, which is found in Gram-positive bacteria. Themechanism by which NOD may recognize LPS in the cytosol is unknown.
MD-2 MyD88IRAK
TRAF6
TollipTIRAP/Mal
MSR
CD11b/CD18
IRF3
PKRIKKcomplex
IκB
NFκB
K+ channel
?
?
? ?
Cytokines and effector molecules
MAPK
NOD1
NOD2
TLR4
CD14
LBP
LPS
TIR
© 2002 Nature Publishing Group

insight review articles
NATURE | VOL 420 | 19/26 DECEMBER 2002 | www.nature.com/nature 887
(TLRs)25,26. Over a remarkably short period of time, studies of innateimmunity in Drosophila revealed the existence of a proteolytic cascade that yielded ligands for cellular receptors that could distinguish bacterial from fungal infection. It was shown subse-quently that there were striking similarities between this system andthe interleukin (IL)-1 signalling system in mammals. This in turn ledto the identification of human TLRs27 and the discovery that a TLRwas the long-sought co-receptor for LPS28.
A family of (currently) ten TLRs has been identified with a widerange of ligand specificity including bacterial, fungal and yeast proteins25,29. Thus, TLR4 is the LPS receptor, TLR2 is predominantlyresponsible for recognizing Gram-positive cell-wall structures30,TLR5 is the receptor for flagellin31 and TLR9 recognizes CpG elements in bacterial DNA18. An additional cell-surface molecule,MD-2, has been identified that is required for activation of TLR4 (ref.32). MD-2 knockout mice do not respond to LPS and survive endotoxic shock. The role of MD-2 seems to be that of positioningTLR4 correctly on the cell surface, as in MD-2–/– embryonic fibrob-lasts TLR4 remained within the Golgi and failed to appear on the cell surface33.
The notion of a ‘monogamous’ association between one particu-lar TLR and its microbial ligand, as in the case of LPS and TLR4, is inreality an oversimplification. For instance, TLR2 can be activated bycell-wall components of both yeast and mycobacteria. Further com-plexity is introduced into the system by the fact that TLRs seem to beable to combine to form a repertoire capable of distinguishing closelyrelated ligands34, and there is at least preliminary evidence that polymorphisms in Toll-family proteins might provide part of the
explanation for the enormous variability in individual responses towhat seem to be similar infective challenges35,36.
Signalling pathways activated by TLRs have been dissected ingreat detail, and show a remarkable degree of homology with the Tollactivation pathway in Drosophila37. TLRs have an intracellulardomain that is homologous with the IL-1 receptor and the IL-18receptor. Adapter proteins facilitate binding to IL-1 receptor-associ-ated kinase, which in turn induces TNF receptor-associated factor-6,leading to nuclear translocation of nuclear factor-kB (NF-kB) andultimately to activation of cytokine gene promoters (Fig. 1).Although this model is based on LPS signalling of TLR4, a similar —although not identical — process is involved in the activation ofTLR2 by Gram-positive bacteria.
Other host signal molecules that respond to bacteriaA further layer of complexity has been provided by the discovery thatthere are several additional pathways by which cells recognize micro-bial components. Peptidoglycan-recognition proteins (PGRPs) wereidentified in moths and subsequently a family of PGRP genes wasfound in Drosophila38 and in humans39. Different PGRPs can distin-guish between Gram-positive40 and Gram-negative bacteria41,42. InDrosophila, they seem to act by regulating activation of Relish, amember of the NF-kB family43, although the precise mechanism bywhich they are sensed at the cell surface remains unknown.
The triggering receptor expressed on myeloid cells (TREM-1) andthe myeloid DAP12-associating lectin (MDL-1) are two recentlyidentified receptors involved in monocytic activation and inflamma-tory response. TREM-1 is upregulated in the presence of variousmicroorganisms44, although the ligand for TREM-1 is unknown.When mononuclear cells are exposed to a combination of LPS and anantibody to TREM-1, there is a synergistic effect and enhanced production of pro-inflammatory cytokines. But if a fusion protein ofTREM-1 and the Fc portion of IgG is used to compete with cell-bound receptor, LPS-induced cytokine production is downregulatedand mice can be protected from death up to 4 hours after a lethalinjection of LPS45. This is a therapeutic effect that will have obviousimplications if it can be reproduced in clinical studies.
Finally, there is the recent description of the monocytic intracel-lular proteins NOD1 and NOD2 (for nucleotide-binding oligomer-ization domain), which seem to have the ability to bind and to conferresponsiveness to LPS46, suggesting that this might be yet another waycells respond to the presence of bacteria47. Genotypic variations inNOD2 are associated with distinct clinical phenotypes of Crohn’s disease48, prompting speculation that other NOD genotypes mightbe associated with phenotypic variations in LPS responsiveness.
Signal amplificationFollowing the initial host–microbial interaction there is widespreadactivation of the innate immune response, the purpose of which is tocoordinate a defensive response involving both humoral and cellularcomponents. Mononuclear cells play a key role, releasing the classicpro-inflammatory cytokines IL-1, IL-6 and TNF-a, but in additionan array of other cytokines including IL-12, IL-15 and IL-18, and ahost of other small molecules (Table 1).
TNF-a and IL-1 are the prototypic inflammatory cytokines thatmediate many of the immunopathological features of LPS-inducedshock49. They are released during the first 30–90 minutes after expo-sure to LPS and in turn activate a second level of inflammatory cas-cades including cytokines, lipid mediators and reactive oxygenspecies, as well as upregulating cell adhesion molecules that result inthe initiation of inflammatory cell migration into tissues. The factthat anti-TNF or anti-IL-1 strategies failed to prevent death in septicpatients is probably related more to the difficulty of designing clinicaltrials in these patients, rather than an intrinsic flaw in the scientificrationale50. One practical problem is that patients often come tomedical attention relatively late in the disease, and blocking theseearly cytokines may simply be too late. High mobility group B1
Enhanced formationof fibrin blood clots
PAI-1Tissue factor
+Factor VIIaFactor X
Factor XaFactor Va
Protein C
Prothrombin
Thrombin
Increasedfibrinogen
aPC
Plasminogenactivators
Plasminogen
Plasmin
Fibrin
Impairedfibrinolysis
FDP
Thrombosis of small vessels
Impaired tissue perfusion
Sepsis
Procoagulant pathways Anticoagulant pathways
–
–
–
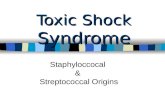
Figure 2 Sepsis disturbs the normal homeostatic balance between procoagulant andanticoagulant mechanisms. Tissue factor expression is enhanced leading to increasedproduction of prothrombin that is converted to thrombin, and that in turn generatesfibrin from fibrinogen. Simultaneously, levels of the plasminogen-activator inhibitor-1(PAI-1) are increased, resulting in impaired production of plasmin and thus failure ofnormal fibrinolytic mechanisms by which fibrin is converted to degradation products(FDP). Sepsis also causes a fall in the levels of the natural anticoagulant protein C (andalso antithrombin and the tissue factor pathway inhibitor, TFPI, not shown). Theactivated form of protein C, aPC, dissociates from the endothelial protein C receptor toinactivate factors Va and VIIa and inhibit PAI-1 activity; hence reduced levels of proteinC result in further procoagulant effect. The net result is enhanced formation of fibrinclots in the microvasculature, leading to impaired tissue oxygenation and cell damage.
© 2002 Nature Publishing Group

pathway inhibitor. These natural anticoagulants are of particularinterest because in addition to their effect on thrombin generation,they also have anti-inflammatory properties, including effects onrelease of monocyte-derived TNF-a by inhibiting activation of thetranscription factors NF-kB and activator protein (AP)-1 (ref. 60).
Particular attention has focused on Protein C, which is convertedto the activated form (aPC) when thrombin complexes with throm-bomodulin, an endothelial transmembrane glycoprotein. Once aPCis formed it dissociates from an endothelial protein C receptor(EPCR) before binding protein S, resulting in inactivation of factorsVa and VIIIa and thus blockade of the coagulation cascade. It hasbeen shown recently that aPC uses EPCR as a co-receptor for cleavageof protease-activated receptor 1 (PAR1). Gene profiling showed thatPAR1 signalling could account for the activation of aPC-inducedprotective genes, including the immunomodulatory monocytechemoattractant protein-1 (MCP-1), suggesting a role for PAR-1activation in protection from sepsis61. In septic patients, aPC levelsare reduced and expression of endothelial thrombomodulin andEPCR are impaired62, providing some support for the notion thatreplacement of aPC might have therapeutic value.
The counter-inflammatory response — modifier or mediator?The profound pro-inflammatory response that occurs in sepsis is bal-anced by an array of counter-regulatory molecules that attempt torestore immunological equilibrium. In this sense, the counter-inflammatory response is seen as a ‘modifier’ — both appropriate andbeneficial. Counter-inflammatory cytokines include antagonists suchas the soluble TNF receptors and IL-1 receptor antagonist, decoyreceptors such as IL-1 receptor type II, inactivators of the complement
insight review articles
888 NATURE | VOL 420 | 19/26 DECEMBER 2002 | www.nature.com/nature
(HMGB1) has recently been identified as a cytokine-like product ofmacrophages that appears much later after LPS stimulation and mayrepresent a more tractable target for intervention51.
HMGB1 is a non-histone chromosomal protein that is abundant-ly distributed and exists in nuclear, cytoplasmic and membrane-bound forms. It participates in stabilizing nucleosomes, facilitatesgene transcription and modulates the activity of steroid hormonereceptors. When mice were injected with LPS, HMGB1 serum con-centrations rose after a delay of about 24 hours, long after the initialpeak of IL-1 and TNF-a had declined. Importantly, mice could berescued from LPS-induced shock by administering an antibody toHMGB1, even when this was provided up to 2 hours after the lethalinjection52. Subsequently it was shown that patients with sepsis haveelevated serum levels of HMGB1, and that higher levels are associatedwith an increased mortality, suggesting that clinical intervention byblocking or neutralizing HMGB1 might be a viable option.
Another macrophage-derived cytokine that has been identified asa potential therapeutic target in sepsis is macrophage migrationinhibitory factor (MIF). Mice with a targeted disruption of the MIFgene are resistant to LPS-induced shock53 and antibody to MIF is fullyprotective, even in the more demanding caecal ligation and puncturemodel that resembles clinical peritonitis54. MIF also seems to mediateshock caused by Gram-positive bacteria, such as the toxic shock syndrome associated with S. aureus55, suggesting that anti-MIFstrategies might have broad application in septic patients. MIF has acurious relationship with glucocorticoids, which are normallythought of as being anti-inflammatory, as low doses of glucocorti-coids paradoxically induce macrophage MIF. Once released, MIFthen acts as a pro-inflammatory agent, over-riding the ability of glu-cocorticoids to prevent shock in animal models of sepsis56. How thiscomplex relationship manifests in a clinical setting is of particularinterest in the light of the recent studies demonstrating a protectiveeffect of low-dose steroids in patients with severe sepsis.
These pro-inflammatory cytokines are important because they inturn are responsible for orchestrating a complex network of sec-ondary responses (for a review, see ref. 49). A good example of this isprovided by IL-18, a cytokine that induces production of interferon-g (IFN-g). In human mononuclear cells, IFN-g upregulates surfaceexpression of TLR4, MD-2 and MyD88, and counteracts the LPS-induced downregulation of TLR4 (ref. 57). It has long beenknown that IFN-g sensitizes human mononuclear cells to the effectsof LPS, and these new findings suggest strongly that this effect isprobably mediated through upregulation (or at least, prevention ofdownregulation) of TLR4.
The coagulation cascadeCytokines are also important in inducing a procoagulant effect insepsis. Disorders of coagulation are common in sepsis, and 30–50%of patients have the more severe clinical form, disseminated intravas-cular coagulation58. Coagulation pathways are initiated by LPS andother microbial components, inducing expression of tissue factor onmononuclear and endothelial cells. Tissue factor in turn activates aseries of proteolytic cascades, which result in the conversion of prothrombin to thrombin, which in turn generates fibrin from fibrinogen. Simultaneously, normal regulatory fibrinolytic mecha-nisms (fibrin breakdown by plasmin) are impaired because of highplasma levels of plasminogen-activator inhibitor type-1 (PAI-1) thatprevent the generation of plasmin from the precursor plasminogen.The net result is enhanced production and reduced removal of fibrinleading to the deposition of fibrin clots in small blood vessels, inade-quate tissue perfusion and organ failure (Fig. 2).
Pro-inflammatory cytokines, in particular IL-1 and IL-6, arepowerful inducers of coagulation, and conversely, IL-10 regulatescoagulation by inhibiting the expression of tissue factor on mono-cytes (for a review, see ref. 59). An additional cause of the procoagu-lant state in sepsis is the downregulation of three naturally occurringanticoagulant proteins — antithrombin, protein C and tissue factor
Neutrophils Monocytes
Complement
ChemotaxisLysosomal enzymes
Cytokines
Lipid mediatorsOxygen radicals
Coagulopathy Fever Vasodilation Capillary leak
Sepsis and multiple organ failure
IncreasedTF and PAI-1
Procoagulant effect
LPS and otherbacterial components
Endothelium
Microvascular occlusion Vascular instability
Figure 3 Pathogenetic networks in shock. Lipopolysaccharide (LPS) and othermicrobial components simultaneously activate multiple parallel cascades thatcontribute to the pathophysiology of adult respiratory distress syndrome (ARDS) andshock. The combination of poor myocardial contractility, impaired peripheral vasculartone and microvascular occlusion leads to tissue hypoperfusion and inadequateoxygenation, and thus to organ failure.
© 2002 Nature Publishing Group

insight review articles
NATURE | VOL 420 | 19/26 DECEMBER 2002 | www.nature.com/nature 889
cascade and the anti-inflammatory cytokines, of which the prototypeis IL-10. In concert with this, the host response to injury includes pro-found changes in metabolic activity (increased cortisol productionand release of catecholamines), induction of acute-phase proteins,and endothelial activation with upregulation of adhesion moleculesand release of prostanoids and platelet-activating factor (PAF).
Another facet of downregulation of immunity that occurs in sep-sis is the development of lymphocyte apoptosis. Extensive lympho-cyte apoptosis is seen in animal models of sepsis and is also present inseptic patients, although interestingly, much less so in critically illnon-septic controls63. Septic patients are usually lymphopenic, andsubset analysis of autopsy tissue samples has shown that there is selec-tive depletion of B and CD4+ lymphocytes64. This process and itsfunctional consequences are viewed as part of a more general state ofimmunosuppression, characterized by T-cell hyporesponsivenessand anergy, which occurs to some extent in most septic patients, andwhich is seen as a counter-balancing response (and sometimes, over-response) to the initial pro-inflammatory state.
It is because of this over-response that some investigators view thecounter-inflammatory response as the cause of an inadequate hostdefence against infection and hence a potential ‘mediator’ of sepsis andprogressive organ failure. Several have pursued the notion that reversalof this immunosuppressive state might be of therapeutic value. Forinstance, mice transfected with the human gene bcl-2 that overexpress
the anti-apoptotic protein Bcl-2 are protected from death after caecalligation and puncture65, and patients that received IFN-g in a small non-randomized clinical study showed upregulation of HLA-DR on theirmonocytes and a better-than-anticipated survival66.
Role of genetic susceptibility in the pathogenesis of sepsisAmong this vast array of host molecules that orchestrate the responseto sepsis there are many examples of genetic variability that influencephysiological activity. For example, there has been great interest inexploring the possibility that a polymorphism in the TNF promoterthat results in significantly higher TNF levels might be associatedwith a worse outcome from sepsis. Several of these associations havebeen studied67 (Table 2) and at least in some cases the evidence seemsconvincing. Of particular interest was the recent report that muta-tions in TLR4 are associated with an increased susceptibility toGram-negative sepsis36.
Mechanisms of organ failureThe ultimate cause of death in patients with sepsis is multiple organ failure. Typically, patients will first develop a single organ failure — for instance, respiratory failure requiring mechanical ventilation — and then if the disease remains unchecked, will progressively develop failure of other organ systems. There is a closerelationship between the severity of organ dysfunction on admissionto an intensive care unit and the probability of survival, and betweenthe numbers of organs failing and the risk of death. If four or fiveorgans fail the mortality is greater than 90%, irrespective of treatment.
The pathogenesis of organ dysfunction is multifactorial andincompletely understood. Tissue hypoperfusion and hypoxia aredominant factors (Fig. 3). The mechanisms involve widespread fib-rin deposition causing microvascular occlusion, the development oftissue exudates further compromising adequate oxygenation, anddisorders of microvascular homeostasis resulting from the elabora-tion of vasoactive substances such as PAF, histamine and prostanoids.Cellular infiltrates, particularly neutrophils, damage tissue directlyby releasing lysosomal enzymes and superoxide-derived free radi-cals. TNF-a and other cytokines increase the expression of theinducible nitric oxide synthase and increased production of nitricoxide causes further vascular instability and may also contribute tothe direct myocardial depression that occurs in sepsis68.
The tissue hypoxia that develops in sepsis is reflected in the oxygendebt — that is, the difference between oxygen delivery and oxygenrequirements. The extent of the oxygen debt is related to the outcomefrom sepsis, and strategies designed to optimize oxygen delivery tothe tissues can improve survival. In addition to hypoxia, cells may bedysoxic — that is, unable to properly utilize available oxygen. Recentdata suggest that this may be another consequence of excess nitricoxide production, because skeletal muscle biopsies from septic
Table 1 Macrophage products implicated in the pathogenesis of sepsis
Mediators Typical effects
CytokinesIl-1, IL-6, IL-12, IL-15, Activate neutrophils, lymphocytes and vascular IL-18, TNF-a, MIF, endothelium; upregulate cellular adhesion molecules; HMGB1, IL-10 induce prostaglandins, nitric oxide synthase and
acute-phase proteins; induce fever. Note that IL-10 is predominantly a negative regulator of these effects
ChemokinesIL-8, MIP-1a, MIP-1b, Mobilize and activate inflammatory cells, especially MCP-1, MCP-3 neutrophils; activate macrophages
Lipid mediatorsPlatelet-activating factor, Activate vascular endothelium; regulate vascularprostaglandins, tone; activate extrinsic coagulation cascadeleukotrienes, thromboxane, tissue factor
Oxygen radicalsSuperoxide and hydroxyl Antimicrobial properties; regulation of vascular toneradicals, nitric oxide
Upon activation by microbial components, macrophages release a diverse range of products; thetable lists the principal among them that are implicated in the pathogenesis of sepsis. Most ofthese products have multiple targets and cause effects through several parallel mechanisms. Forinstance, nitric oxide has direct antimicrobial properties, can modify vascular tone (and hencetissue oxygenation), and also causes macrophage apoptosis. Furthermore, many macrophageproducts are involved in the regulation of each other. Thus, TNF-a upregulates tissue factor andnitric oxide synthase, IL-18 induces IFN-g, which in turn further activates macrophages, while IL-10 is a global suppressor of macrophage function. These highly complex and tightly regulatednetworks make it difficult to predict the consequences of blocking or inhibiting just one pathway.
Table 2 Summary of genetic polymorphisms that have been explored in patients with sepsis and meningococcal disease
Host factor Genetic association Clinical effect
Tumour-necrosis factor-a (TNF-a) TNF2 allele Increased serum levels of TNF associated with non-survival in sepsisG308A mutation in TNF promoter
Lymphotoxin-a (TNF-b) TNFB2 allele Increased levels of lymphotoxin associated with sepsis in trauma patients
Interleukin-1 receptor antagonist (IL-1Ra) ILRN*2 allele Associated with increased levels IL-1b and more severe sepsis. Homozygotes for ILRN*2 and TNFB2 have a higher mortality from sepsis
Factor V Leiden FVL Possibly a mild effect on the severity of meningococcal disease
Tissue plasminogen activator (t-PA) Insertion/deletion polymorphism No effect in meningococcal disease
Plasminogen-activator inhibitor 1 (PAI-1) 4G/5G insertion/deletion polymorphism 4G/4G haplotype associated with increased levels of PAI-1 and increased severity of meningococcal disease
FCgRIIa (CD32) R131 allotype More severe outcome from meningococcal disease
Lipopolysaccharide-binding protein (LBP) and Various No statistically significant effect in sepsisbactericidal/permeability-increasing protein (BPI)
CD14 C(-159)T promoter polymorphism Increased susceptibility to septic shock and death
Toll-like receptor 4 (TLR4) Asp299Gly allele Significant association with septic shock, and in particular Gram-negative sepsis
It should be noted that not all these associations have been confirmed independently, and the significance of the findings is influenced by the precise patient population studied and the methods used.Other host factors (for instance, mannan binding protein) are known to be important in the response to specific infections, but have not yet been studied specifically in sepsis; yet others (for example,nitric oxide synthase) have been suggested to be important, but clinical data are lacking.
© 2002 Nature Publishing Group

insight review articles
890 NATURE | VOL 420 | 19/26 DECEMBER 2002 | www.nature.com/nature
patients show evidence of impaired mitochondrial respiration,which is inhibited by nitric oxide69.
Therapeutic approachesDespite the extraordinary developments in understanding theimmunopathology of sepsis, therapeutic advances have beenpainfully slow. However, in the past 12 months several clinical trialshave finally shown that it is possible to reduce mortality in patientswith sepsis. Interestingly, each has been based on a different aspect ofthe pathology described above.
The critical importance of tissue oxygenation was addressed by astudy in which patients in the earliest stages of sepsis were treated byaggressive management with fluids, blood transfusion and inotropicagents to optimize haemodynamic function70. An alternative approachwas taken by van den Berghe and co-workers, who studied the effect ofrigorous control of blood glucose levels. Hyperglycaemia and insulinresistance are common in critically ill patients, even if they have not pre-viously had diabetes, and these authors showed that intensive insulintherapy could substantially reduce mortality71. The mechanism of thisstriking effect is not absolutely clear, although it is of interest that thegreatest reduction in mortality involved deaths due to multiple-organfailure in patients with a proven septic focus, perhaps suggesting that itwas related to the better control of the initial infective process.
The third study to show significant benefit was a trial of low-dosecorticosteroids. Earlier trials using very high doses of steroids, basedon the premise that sepsis represented an uncontrolled inflammatoryresponse, had failed to show any survival benefit. But Annane andcolleagues had noted that patients in the advanced stages of septicshock had relative adrenal insufficiency and reasoned that low-dosereplacement steroids might be beneficial. In a phase III trial in highlyselected patients, they found that low doses of hydrocortisone andfludrocortisone did indeed reduce the mortality substantially72. Butdoubts remain about the precise mechanism of this effect and it ispossible that the benefit derives, at least in part, from the immuno-suppressive effects of the hydrocortisone.
Disordered coagulation is important in sepsis, and the fourthstudy examined the effects on the course of sepsis of replacing aPC. Arandomized controlled trial of aPC therapy resulted in a significantsurvival benefit in treated patients73, although interestingly the effectwas equally marked in patients whose protein C levels were notdepressed. This suggests that the therapeutic effect was attributablein part to the immunosuppressive effects of protein C60, and not justto its anticoagulant properties.
Improved understanding of the immunopathology of sepsis hasfacilitated many other approaches, and several additional strategies areat various stages of development. These include therapies aimed at bacterial targets, for example novel anti-endotoxin molecules such asbactericidal/permeability-increasing protein, or modified lipopro-teins, both of which absorb and neutralize LPS, as well as very recentreports that oxidized phospholipids can interfere with binding of LPSto LBP74, and strategies aimed at Gram-positive toxins, including competitive antagonists of superantigen-binding sites. There are alsoinvestigations aimed at host molecules, such as PAF-receptor antago-nists, and a variety of targets in the coagulation cascade. For the clinicalinvestigator, the challenge will be the design of studies with sufficientpower to determine the potential value of these new therapies. As fatality rates drop with the use of low-dose steroids, aPC and the othermeasures described above, it will become increasingly difficult to carryout studies on a heterogeneous population of patients with sepsis. Theway forward is likely to lie in identifying clinically relevant endpointsother than death (for instance, reduced incidence of organ failure),and/or identifying more homogeneous subgroups of patients in whomto study specifically targeted therapeutic interventions. ■■
doi:10.1038/nature01326
1. Angus, D. C. et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome,
and associated costs of care. Crit. Care Med. 29, 1303–1310 (2001).
2. Alberti, C. et al. Epidemiology of sepsis and infection in ICU patients from an international
multicentre cohort study. Intensive Care Med. 28, 108–121 (2002).
3. Janeway, C. A. Jr & Medzhitov, R. Introduction: the role of innate immunity in the adaptive immune
response. Semin. Immunol. 10, 349–350 (1998).
4. Seydel, U., Oikawa, M., Fukase, K., Kusumoto, S. & Brandenburg, K. Intrinsic conformation of lipid
A is responsible for agonistic and antagonistic activity. Eur. J. Biochem. 267, 3032–3039 (2000).
5. Majcherczyk, P. A. et al. Digestion of Streptococcus pneumoniae cell walls with its major peptidoglycan
hydrolase releases branched stem peptides carrying proinflammatory activity. J. Biol. Chem. 274,
12537–12543 (1999).
6. Morath, S., Geyer, A. & Hartung, T. Structure–function relationship of cytokine induction by
lipoteichoic acid from Staphylococcus aureus. J. Exp. Med. 193, 393–397 (2001).
7. Wang, J. E. et al. Peptidoglycan and lipoteichoic acid from Staphylococcus aureus induce tumor
necrosis factor alpha, interleukin 6 (IL-6), and IL-10 production in both T cells and monocytes in a
human whole blood model. Infect. Immun. 68, 3965–3970 (2000).
8. Lavoie, P. M., Thibodeau, J., Erard, F. & Sekaly, R. P. Understanding the mechanism of action of
bacterial superantigens from a decade of research. Immunol. Rev. 168, 257–269 (1999).
9. Papageorgiou, A. C. & Acharya, K. R. Microbial superantigens: from structure to function. Trends
Microbiol. 8, 369–375 (2000).
10.Kotb, M. Bacterial pyrogenic exotoxins as superantigens. Clin. Microbiol. Rev. 8, 411–426 (1995).
11.Norrby-Teglund, A. et al. Evidence for superantigen involvement in severe group A streptococcal
tissue infections. J. Infect. Dis. 184, 853–860 (2001).
12.Muller-Alouf, H. et al. Pyrogenicity and cytokine-inducing properties of Streptococcus pyogenes
superantigens: comparative study of streptococcal mitogenic exotoxin Z and pyrogenic exotoxin A.
Infect. Immun. 69, 4141–4145 (2001).
13.Unnikrishnan, M. et al. The bacterial superantigen streptococcal mitogenic exotoxin Z is the major
immunoactive agent of Streptococcus pyogenes. J. Immunol. 169, 2561–2569 (2002)
14.Dinges, M. M. & Schlievert, P. M. Role of T cells and gamma interferon during induction of
hypersensitivity to lipopolysaccharide by toxic shock syndrome toxin 1 in mice. Infect. Immun. 69,
1256–1264 (2001).
15.Eaves-Pyles, T. et al. Flagellin, a novel mediator of salmonella-induced epithelial activation and
systemic inflammation: IkBa degradation, induction of nitric oxide synthase, induction of
proinflammatory mediators, and cardiovascular dysfunction. J. Immunol. 166, 1248–1260 (2001).
16.Herwald, H. et al. Activation of the contact-phase system on bacterial surfaces—a clue to serious
complications in infectious diseases. Nature Med. 4, 298–302 (1998).
17.Sparwasser, T. et al. Bacterial DNA causes septic shock. Nature 386, 336–337 (1997).
18.Bauer, S. et al. Human TLR9 confers responsiveness to bacterial DNA via species-specific CpG motif
recognition. Proc. Natl Acad. Sci. USA 98, 9237–9242 (2001).
19.Wright, S. D., Ramos, R. A., Tobias, P. S., Ulevitch, R. J. & Mathison, J. C. CD14, a receptor for
complexes of lipopolysaccharide (LPS) and LPS binding protein. Science 249, 1431–1433 (1990).
20.Pugin, J. et al. CD14 is a pattern recognition receptor. Immunity 1, 509–516 (1994).
21.Devitt, A. et al. Human CD14 mediates recognition and phagocytosis of apoptotic cells. Nature 392,
505–509 (1998).
22.Yu, B., Hailman, E. & Wright, S. D. Lipopolysaccharide binding protein and soluble CD14 catalyze
exchange of phospholipids. J. Clin. Invest. 99, 315–324 (1997).
23.Landmann, R. et al. Increased circulating soluble CD14 is associated with high mortality in Gram-
negative septic shock. J. Infect. Dis. 171, 639–644 (1995).
24.Leturcq, D. J. et al. Antibodies against CD14 protect primates from endotoxin-induced shock. J. Clin.
Invest. 98, 1533–1538 (1996).
25.Aderem, A. & Ulevitch, R. J. Toll-like receptors in the induction of the innate immune response.
Nature 406, 782–787 (2000).
26.Vasselon, T. & Detmers, P. A. Toll receptors: a central element in innate immune responses. Infect.
Immun. 70, 1033 (2002).
27.Medzhitov, R., Preston-Hurlburt, P. & Janeway, C. A. Jr A human homologue of the Drosophila Toll
protein signals activation of adaptive immunity. Nature 388, 394–397 (1997).
28.Poltorak, A. et al. Defective LPS signaling in C3H/HeJ and C57BL/10ScCr mice: mutations in Tlr4
gene. Science 282, 2085–2088 (1998).
29.Opal, S. M. & Huber, Ch. Bench-to-bedside review: Toll-like receptors and their role in septic shock.
Crit. Care 6, 125–136 (2002).
30.Takeuchi, O. et al. Differential roles of TLR2 and TLR4 in recognition of gram-negative and gram-
positive bacterial cell wall components. Immunity 11, 443–451 (1999).
31.Hayashi, F. et al. The innate immune response to bacterial flagellin is mediated by Toll- like receptor 5.
Nature 410, 1099–1103 (2001).
32.Shimazu, R. et al. MD-2, a molecule that confers lipopolysaccharide responsiveness on Toll-like
receptor 4. J. Exp. Med. 189, 1777–1782 (1999).
33.Nagai, Y. et al. Essential role of MD-2 in LPS responsiveness and TLR4 distribution. Nature Immunol.
3, 667–672 (2002).
34. Ozinsky, A. et al. The repertoire for pattern recognition of pathogens by the innate immune system is
defined by cooperation between toll-like receptors. Proc. Natl Acad. Sci. USA 97, 13766–13771 (2000).
35.Lorenz, E., Mira, J. P., Cornish, K. L., Arbour, N. C. & Schwartz, D. A. A novel polymorphism in the
Toll-like receptor 2 gene and its potential association with staphylococcal infection. Infect. Immun.
68, 6398–6401 (2000).
36.Lorenz, E., Mira, J. P., Frees, K. L. & Schwartz, D. A. Relevance of mutations in the TLR4 receptor in
patients with gram-negative septic shock. Arch. Intern. Med. 162, 1028–1032 (2002).
37.Bowie, A. & O’Neill, L. A. The interleukin-1 receptor/Toll-like receptor superfamily: signal generators
for pro-inflammatory interleukins and microbial products. J. Leukoc. Biol. 67, 508–514 (2000).
38.Werner, T. et al. A family of peptidoglycan recognition proteins in the fruit fly Drosophila
melanogaster. Proc. Natl Acad. Sci. USA 97, 13772–13777 (2000).
39.Liu, C., Xu, Z., Gupta, D. & Dziarski, R. Peptidoglycan recognition proteins: a novel family of four
human innate immunity pattern recognition molecules. J. Biol. Chem. 276, 34686–34694 (2001).
40.Michel, T., Reichhart, J. M., Hoffmann, J. A. & Royet, J. Drosophila Toll is activated by Gram-positive
bacteria through a circulating peptidoglycan recognition protein. Nature 414, 756–759 (2001).
41.Gottar, M. et al. The Drosophila immune response against Gram-negative bacteria is mediated by a
peptidoglycan recognition protein. Nature 416, 640–644 (2002).
42. Ramet, M., Manfruelli, P., Pearson, A., Mathey-Prevot, B. & Ezekowitz, R. A. Functional genomic analysis
of phagocytosis and identification of a Drosophila receptor for E. coli. Nature 416, 644–648 (2002).
© 2002 Nature Publishing Group

insight review articles
NATURE | VOL 420 | 19/26 DECEMBER 2002 | www.nature.com/nature 891
43.Choe, K. M., Werner, T., Stoven, S., Hultmark, D. & Anderson, K. V. Requirement for a peptidoglycan
recognition protein (PGRP) in Relish activation and antibacterial immune responses in Drosophila.
Science 296, 359–362 (2002).
44.Bouchon, A., Dietrich, J. & Colonna, M. Inflammatory responses can be triggered by TREM-1, a
novel receptor expressed on neutrophils and monocytes. J. Immunol. 164, 4991–4995 (2000).
45.Bouchon, A., Facchetti, F., Weigand, M. A. & Colonna, M. TREM-1 amplifies inflammation and is a
crucial mediator of septic shock. Nature 410, 1103–1107 (2001).
46. Inohara, N., Ogura, Y., Chen, F. F., Muto, A. & Nunez, G. Human Nod1 confers responsiveness to
bacterial lipopolysaccharides. J. Biol. Chem. 276, 2551–2554 (2001).
47. Inohara, N., Ogura, Y. & Nunez, G. Nods: a family of cytosolic proteins that regulate the host response
to pathogens. Curr. Opin. Microbiol. 5, 76–80 (2002).
48.Hampe, J. et al. Association of NOD2 (CARD 15) genotype with clinical course of Crohn’s disease: a
cohort study. Lancet 359, 1661–1665 (2002).
49.Dinarello, C. A. Proinflammatory and anti-inflammatory cytokines as mediators in the pathogenesis
of septic shock. Chest 112, 321S–329S (1997).
50.Cohen, J. Adjunctive therapy in sepsis: a critical analysis of the clinical trial programme. Br. Med. Bull.
55, 212–226 (1999).
51.Yang, H., Wang, H. & Tracey, K. J. HMG-1 rediscovered as a cytokine. Shock 15, 247–253 (2001).
52.Wang, H. et al. HMG-1 as a late mediator of endotoxin lethality in mice. Science 285, 248–251 (1999).
53.Bozza, M. et al. Targeted disruption of migration inhibitory factor gene reveals its critical role in
sepsis. J. Exp. Med. 189, 341–346 (1999).
54.Calandra, T. et al. Protection from septic shock by neutralization of macrophage migration inhibitory
factor. Nature Med. 6, 164–170 (2000).
55.Calandra, T., Spiegel, L. A., Metz, C. N. & Bucala, R. Macrophage migration inhibitory factor is a
critical mediator of the activation of immune cells by exotoxins of Gram-positive bacteria. Proc. Natl
Acad. Sci. USA 95, 11383–11388 (1998).
56.Calandra, T. et al. MIF as a glucocorticoid-induced modulator of cytokine production. Nature 377,
68–71 (1995).
57.Bosisio, D. et al. Stimulation of toll-like receptor 4 expression in human mononuclear phagocytes by
interferon-gamma: a molecular basis for priming and synergism with bacterial lipopolysaccharide.
Blood 99, 3427–3431 (2002).
58.Levi, M. & ten Cate, H. Disseminated intravascular coagulation. N. Engl. J. Med. 341, 586–592 (1999).
59.Van der Poll, T., de Jonge, E., Levi, M. & van Deventer, S. J. Pathogenesis of DIC in sepsis. Sepsis 3,
103–110 (1999).
60.Okajima, K. Regulation of inflammatory responses by natural anticoagulants. Immunol. Rev. 184,
258–274 (2002).
61.Riewald, M., Petrovan, R. J., Donner, A., Mueller, B. M. & Ruf, W. Activation of endothelial cell
protease activated receptor 1 by the protein C pathway. Science 296, 1880–1882 (2002).
62.Faust, S. N. et al. Dysfunction of endothelial protein C activation in severe meningococcal sepsis. N.
Engl. J. Med. 345, 408–416 (2001).
63.Hotchkiss, R. S. et al. Apoptotic cell death in patients with sepsis, shock, and multiple organ
dysfunction. Crit. Care Med. 27, 1230–1251 (1999).
64.Hotchkiss, R. S. et al. Sepsis-induced apoptosis causes progressive profound depletion of B and CD4+
T lymphocytes in humans. J. Immunol. 166, 6952–6963 (2001).
65.Hotchkiss, R. S. et al. Prevention of lymphocyte cell death in sepsis improves survival in mice. Proc.
Natl Acad. Sci. USA 96, 14541–14546 (1999).
66.Döcke, W.-D. et al. Monocyte deactivation in septic patients: restoration by IFN-g treatment. Nature
Med. 3, 678–681 (1997).
67.Stuber, F. Effects of genomic polymorphisms on the course of sepsis: is there a concept for gene
therapy? J. Am. Soc. Nephrol. 12(Suppl. 17), S60–S64 (2001).
68.Landry, D. W. & Oliver, J. A. The pathogenesis of vasodilatory shock. N. Engl. J. Med. 345, 588–595
(2001).
69.Brealey, D. et al. Association between mitochondrial dysfunction and severity and outcome of septic
shock. Lancet 360, 219–223 (2002).
70.Rivers, E. et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N. Engl.
J. Med. 345, 1368–1377 (2001).
71.Van den Berghe, G. et al. Intensive insulin therapy in critically ill patients. N. Engl. J. Med. 345,
1359–1367 (2001).
72.Annane, D. et al. Effects of treatment with low doses of hydrocortisone and fludrocortisone on
mortality in patients with septic shock. J. Am. Med. Assoc. 288, 862–871 (2002).
73.Bernard, G. R. et al. Efficacy and safety of recombinant human activated protein C for severe sepsis.
N. Engl. J. Med. 344, 699–709 (2001).
74.Bochkov, V. N. et al. Protective role of phospholipid oxidation products in endotoxin-induced tissue
damage. Nature 419, 77–81 (2002).
© 2002 Nature Publishing Group











![Division of Public Health Services...Syndrome [Treponema pallidum] Tetanus [Clostridium tetani] Toxic-Shock Syndrome (TSS) [streptococcal or staphylococcal] Trichinosis [Trichinella](https://static.fdocuments.us/doc/165x107/600aad0a71e3742d46221fb0/division-of-public-health-services-syndrome-treponema-pallidum-tetanus-clostridium.jpg)